Back to Journals » Drug Design, Development and Therapy » Volume 16
Added Syrup as a Flavoring to Oral Midazolam Intravenous Solution Premedication Improves Tolerability in Pediatric Patients
Authors Xue Q, Xia J ![]() , Lu J, Shen X
, Lu J, Shen X
Received 9 January 2022
Accepted for publication 13 April 2022
Published 28 April 2022 Volume 2022:16 Pages 1211—1216
DOI https://doi.org/10.2147/DDDT.S357660
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tuo Deng
Qineng Xue,* Junming Xia,* Jin Lu, Xia Shen
Department of Anesthesiology, Eye & and ENT Hospital, Fudan University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xia Shen, Department of Anesthesiology, Eye & and ENT Hospital, Fudan University, 83 Fenyang Road, Shanghai, 200031, People’s Republic of China, Tel +86-21-64377134, Fax +86-21-64373416, Email [email protected]
Purpose: To investigate the tolerability of midazolam intravenous (IV) solution by masking its bitter taste through the addition of syrup.
Methods: In the waiting area before surgery at our institution, Eye and ENT Hospital, from May to November of 2021, pediatric patients scheduled for anterior ear fistula removal or eardrum catheterization were randomly assigned to receive a mixture of IV midazolam and water (Group C) or IV midazolam and syrup (Group S) in equal volumes. We measured the difference between the groups in terms of drug tolerability with a 5-point facial hedonic scale given to every patient, parent, and nurse involved in the study. Secondary outcomes included sedation and anxiety levels, which were assessed at separation from the parents and general anesthesia induction via a mask.
Results: In total, 180 patients were enrolled. The facial hedonic scales were higher in Group S as evaluated by the children (p=0.046), parents (p=0.020), and nurses (p=0.026). More patients were willing to take the same solution again in Group S than in Group C (p=0.024). The levels of sedation and anxiety at two timepoints were similar between the groups (all p> 0.05). No adverse events were noted preoperatively.
Conclusion: The tolerability of IV midazolam administered orally was increased in a pediatric population by adding syrup. The sedative and anxiolytic effects were comparable for both midazolam mixtures.
Trial Registry Number: China Clinical Research Information Service, ChiCTR2000040229.
Keywords: oral midazolam, pediatric preoperative sedation, pediatric preoperative anxiety
Introduction
Preoperative sedation may be prescribed to children to minimize separation anxiety, decrease their fear of strangers and the unknown, facilitate a smoother induction of anesthesia, or reduce the risk of postoperative maladaptive behavior.1 Midazolam can be administered intravenously, intranasally, or orally, depending on the preoperative circumstances of the patient. It is most commonly given orally prior to the induction of anesthesia.2–4 However, when given alone, the bitter taste of midazolam limits its clinical utility in the pediatric population.5,6
Various flavorings have been used to mask the bitter taste of orally administered midazolam and improve its tolerability.5–7 In the United Kingdom, midazolam hydrochloride syrup is dispensed at a 2 mg/mL concentration.8 This oral formula is not available in China, and the midazolam intravenous (IV) formulation—a bitter-tasting drug—is used for oral administration in our institution. Because children are naturally fond of sugar, and because syrup is commercially available in China, we aimed to assess whether syrup added as a flavoring to oral IV midazolam could improve its tolerability in clinical administration.
Methods
This prospective randomized study was conducted from May to November 2021 in the otologic center of our institution. The Hospital Ethics Committee (Shanghai EYE & ENT Hospital) approved the study. The study was registered with the China Clinical Research Information Service (ChiCTR2000040229). Written informed parental or guardian consent and assent from the child (where appropriate) were obtained before enrollment in the study. Patients aged 3 to 10 years who were scheduled for anterior ear fistula removal or eardrum catheterization were given the midazolam IV preparation orally in the waiting area. A lollipop was awarded to the patient after administration, and they were allowed to consume it in that moment. Exclusion criteria included: allergy to the study drug or syrup, cognitive or motor developmental delay, type 1 diabetes mellitus, or declining to participate.
Vanilla-flavored commercial syrup (Kerry Ingredients, Malaysia, SKU#11023852) or water was added to the midazolam IV preparation (5 mg/5 mL, Jiangsu Nhwa Pharmaceutical, Xuzhou, China) in equal volumes for a final concentration of 0.5 mg/mL. The mixtures were prepared just before administration by the treating anesthesiologist, who was independent of the research team.
In the waiting area, 0.25 mg/kg midazolam mixed in equal volumes of water (Group C) or syrup (Group S) was randomly (computer-generated) administered by an anesthesia nurse, who was also independent of the research team and data collection. Parental presence was allowed during administration of the midazolam preparation. Pulse oximetry was utilized throughout the procedure to monitor heart rate and oxygen saturation and enable any necessary resuscitative measures as required in the Guidelines for Nonoperating Room Anesthetizing Locations.9
An investigator recorded whether the whole dose was swallowed, partially expelled, or completely refused by the patient. For the drug tolerability assessment, each child was asked immediately after administration to record how much they liked the sample by placing a mark on a 5-point facial hedonic scale (ranging from 1, disliked very much, to 5, liked very much).10 This scale has been commonly used for taste evaluation in children aged 3–12 years and for parental evaluation of children aged 4–16 years.10 Each patient was also asked if they would be happy to take the drug again if required. Next, the 5-point hedonic scales were provided to the parent or guardian and nurse to fill in, separately, based on their observation of the child’s reaction to the taste of the assigned mixture. The treating anesthesiologist was free to administer dexmedetomidine 0.3 μg/kg intranasally if the patient instantly expelled the dose.
The sedative effect of midazolam was measured using the Ramsay sedation scale (RSS) 20 min after drug administration. This scale includes the following categories: 1, anxious, restless, or agitated; 2, cooperative; 3, responds to commands only; and 4–6, different levels of unconsciousness, where 6 indicates no response to a light glabellar tap or loud auditory stimulus. Higher scores denote higher levels of sedation.11 Then, the patient was taken to the operating room (OR) by the treating anesthesiologist. The anxiolytic effect of midazolam was assessed at separation from parents and anesthesia induction by a 4-point system (1, poor, afraid, combative, crying; 2, fair, moderate expressions of fear, not combative; 3, good, slight expressions of fear; 4, unafraid, cooperative, calm), where a higher score indicated greater drug effect. The score was then classified into two groups, where a score of 3 or 4 was labeled satisfactory and a score of 1 or 2 was labeled unsatisfactory.12
Statistical Analysis
Salman et al presented a child-reported mean (standard deviation [SD]) score of the 5-point facial hedonic scale of 1.71 (1.13) for the midazolam IV formulation.13 We conservatively assumed that a 30% improvement to this score for midazolam and syrup mixture would be clinically significant. Sample size calculations revealed that 90 subjects per group were required to achieve a power of 85% with a type 1 error of 0.05. The data are reported as mean (SD) unless otherwise noted. An unpaired Student’s t-test was used to analyze parametric data, and χ2 or Fisher’s exact test was applied to examine nominal data. The significance threshold was set at 0.05.
Results
In total, 192 patients were identified as eligible for enrollment. Twelve patients did not qualify for participation because their parents refused to allow their children to take the sedative. The remaining 180 patients finished the study (Figure 1). The patient characteristics were not significantly different between groups (Table 1).
 |
Table 1 Demographics Characteristics |
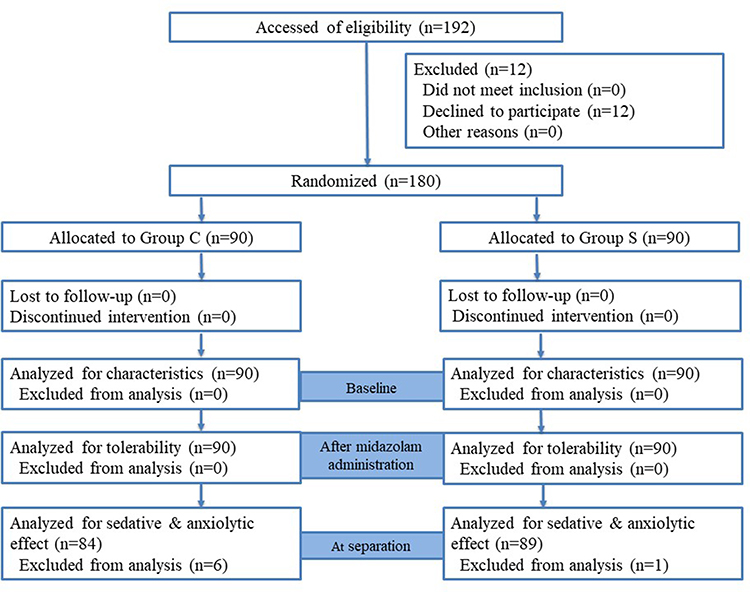 |
Figure 1 CONSORT flow diagram. We randomized 180 patients. Abbreviations: C, control group; S, syrup group. |
More patients were able to fully ingest the midazolam mixture in Group S compared with Group C (89 patients vs 84 patients, p=0.114). Three patients in Group C refused to swallow the mixture after a taste, and three expelled the dose immediately. One patient in Group S expelled the dose (Table 2).
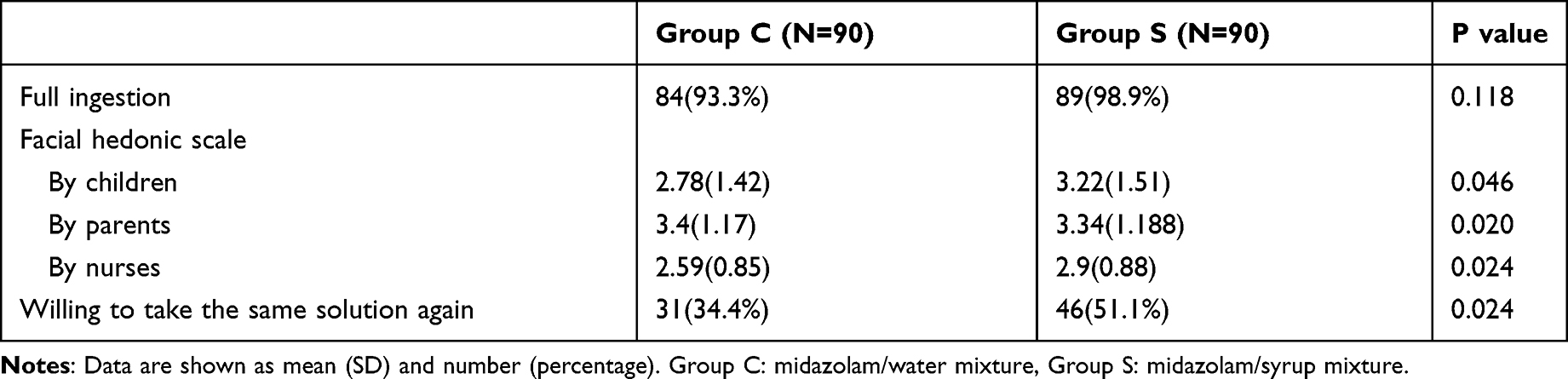 |
Table 2 Midazolam Mixture Tolerability |
Group S had significantly improved scoring on the 5-point facial hedonic scale compared with that of Group C, for the children (p=0.046), parents (p=0.020), and nurses (p=0.026). The children’s, parents’, and nurses’ scores in Group S were 3.22 (1.51), 3.34 (1.11), and 2.88 (0.88), respectively, and in Group C were 2.78 (1.46), 2.94 (1.17), and 2.59 (0.85), respectively. As shown in Table 2, there were 31 pediatric patients in Group C and 46 pediatric patients in Group S who expressed willingness to take the same solution again (p=0.024).
In Group C, 80 patients had an RSS score of 2, and 4 patients had a score of 3. In Group S, 1 patient had an RSS score of 1, 80 patients had a score of 2, and 3 patients had a score of 3. The median (IQR) RSS scores were comparable between the two groups (2 [2,2] in Group C vs 2[2,2] in Group S, p=0.439). Regarding the anxiolytic effect of midazolam, when the children were taken from their parents and guardians into the OR unit., 84 (100%, n=84) patients in Group C and 85 (95.5%, n=89) in Group S showed satisfactory responses. The difference was not statistically significant (p=0.121). At anesthesia induction, 78 (92.9%) patients in Group C and 77 (86.5%) in Group S had satisfactory anxiolysis levels (p=0.172; Table 3).
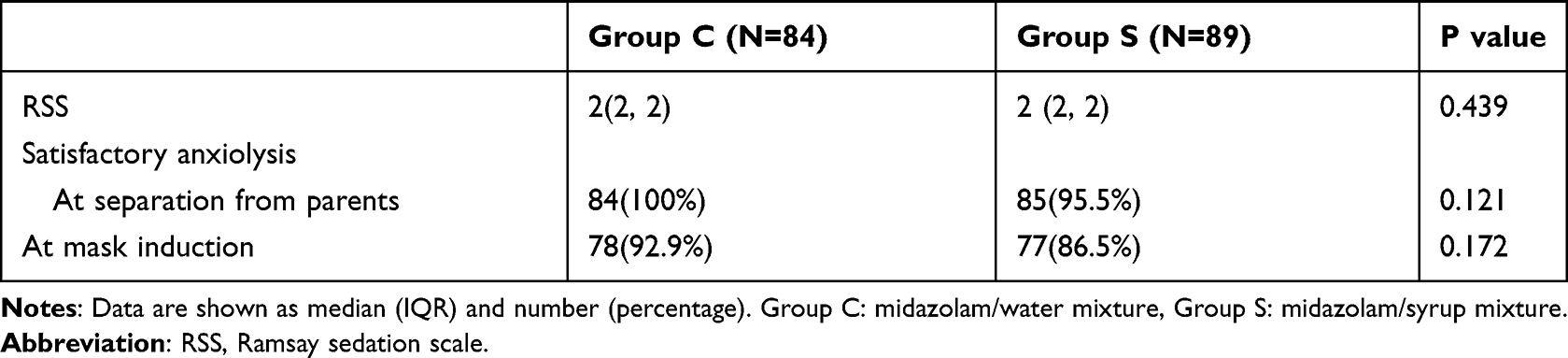 |
Table 3 Sedative and Anxiolytic Effect of Midazolam Mixture |
Discussion
This study presented evidence that adding flavored syrup to the midazolam IV preparation for oral administration improves tolerability. In addition, most patients in both groups attained a satisfactory level of anxiolysis at separation from parents and anesthesia induction.
Flavored preparation of midazolam—such as the midazolam hydrochloride syrup used in the United Kingdom8 and chocolate-flavored midazolam tablet in Australia—helps increase compliance with its oral premedication.13 Unfortunately, only the IV midazolam formulation is currently available in China. When administered orally and alone, the IV midazolam is bitter and poorly tolerated by some patients.13–15 We sought a simple way to improve its tolerability by adding syrup, a commercially available product in China. Furthermore, considering that children are naturally fond of sugar, every patient was awarded a lollipop and was allowed to lick it after midazolam administration. The following findings show that adding syrup to the midazolam IV formulation did improve its tolerability in this study population. First, there was a trend that more patients in Group S achieved full ingestion of the midazolam mixture, suggesting that the tolerability of orally ingested medications is impacted by flavor (not the drug itself), as children commonly spit out or vomit drugs that taste unpleasant. Second, children, parents, and nurses all scored the midazolam/syrup mixture significantly better on the 5-point facial hedonic scale. Finally, more children in Group S said that they would be willing to take the solution a second time. The results of the current study add to those of previous, similar studies that have examined whether adding flavoring to oral midazolam premedication improves tolerability in pediatric patients.5–7
The dosage of midazolam used for sedative premedication ranged from 0.2 to 1.5 mg/kg.1,12,16 Some studies have reported that small doses of midazolam (0.25–0.5 mg/kg) are highly effective and that little advantage is gained from increasing the dose (0.75–1.5 mg/kg).1,16 Marshall et al found that 39% of patients achieved satisfactory sedation within 20 min following a 0.25 mg/kg oral midazolam dose.12 Standard practice at our facility is to administer 0.25–0.5 mg/kg to a maximum of 15 mg. In our study, we found that most patients had an RSS score of 2 when assessed 20 min after midazolam administration, and the sedative effect was comparable between the two groups. Still, the patients showed similar anxiolytic effects of midazolam at separation from parents and anesthesia induction. The finding confirmed that this dose of midazolam (0.25 mg/kg) is safe for patients and the flavoring of the syrup improved its acceptance without impeding the sedative effects.17
This study had some limitations. First, separation anxiety is stronger in younger children. Those aged 3–10 years may be too broad of an age range. Second, we did not record the patients’ history of previous hospitalization. It is well known that children having repeat procedures can be more or less anxious, depending on age.18 Third, the effect of the nil per os (fasting) time was not considered. Generally, the longer the nil per os time, the more irritable a child becomes. Finally, we did not measure parental anxiety. It is also well recognized that higher levels of parental anxiety can cause higher levels of anxiety in the child.19
Conclusion
The current study provided evidence that adding syrup as a flavoring for oral midazolam premedication improves its tolerability in pediatric patients. The syrup did not prevent the sedative and anxiolytic effects of the midazolam. Because adding oral syrup is an easy task to add to our usual standard of care, it may facilitate the preoperative sedation of children.
Data Sharing Statement
The datasets used or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethical Standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional guidelines on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Acknowledgments
The authors thank the anesthesiologists, surgeons, and anesthesia assistants who participated in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Manso MA, Guittet C, Vandenhende F, Granier LA. Efficacy of oral midazolam for minimal and moderate sedation in pediatric patients: a systematic review. Paediatr Anaesth. 2019;29(11):1094–1106. doi:10.1111/pan.13747
2. Day PF, Power AM, Hibbert SA, et al. Effectiveness of oral midazolam for paediatric dental care: a retrospective study in two specialist centres. Eur Arch Paediatr Dent. 2006;7:228–235. doi:10.1007/BF03262557
3. Kain ZN, Caldwell-Andrews AA, Krivutza DM, Weinberg ME, Wang SM, Gaal D. Trends in the practice of parental presence during induction of anesthesia and the use of preoperative sedative premedication in the United States, 1995-2002: results of a follow-up national survey. Anesth Analg. 2004;98(5):1252–1259. doi:10.1213/01.ANE.0000111183.38618.D8
4. Kain ZN, Mayes LC, Bell C, Weisman S, Hofstadter MB, Rimar S. Premedication in the United States: a status report. Anesth Analg. 1997;84(2):427–432. doi:10.1213/00000539-199702000-00035
5. Goho C. Oral midazolam-grapefruit juice drug interaction. Pediatr Dent. 2001;23:365–366.
6. Isik B, Baygin O, Bodur H. Effect of drinks that are added as flavoring in oral midazolam premedication on sedation success. Pediatr Anesth. 2008;18:494–500. doi:10.1111/j.1460-9592.2008.02462.x
7. Brosius KK, Bannister CF. Midazolam premedication in children: a comparison of two oral dosage formulations on sedation score and plasma midazolam levels. Anesth Analg. 2003;96:392–395. doi:10.1213/00000539-200302000-00017
8. Yuen VM, Bailey CR. Premedication in children: does taste matter? Anaesthesia. 2018;73:1453–1456. doi:10.1111/anae.14379
9. Statement on Nonoperating Room Anesthetizing Locations. Approved by the ASA House of Delegates on October 19, 1994, last amended on October 16, 2013, and reaffirmed on October 17, 2018. Available from: https://www.asahq.org//statement-on-nonoperating-room-anesthetizing-locations.pdf.
10. Davies EH, Tuleu C. Medicines for children: a matter of taste. J Pediatr. 2008;153:e1–2. doi:10.1016/j.jpeds.2007.12.033
11. Ramsay M, Savege T, Simpson B, Goodwin R. Controlled sedation with alphaxalone- alphadolone. BMJ. 1974;2(5920):656. doi:10.1136/bmj.2.5920.656
12. Marshall J, Rodarte A, Blumer J, et al. Pediatric pharmacodynamics of midazolam oral syrup. J Clin Pharmacol. 2000;40:578. doi:10.1002/j.1552-4604.2000.tb05983.x
13. Salman S, Tang EKY, Cheung LC, et al. A novel, palatable paediatric oral formulation of midazolam: pharmacokinetics, tolerability, efficacy and safety. Anaesthesia. 2018;73:1469–1477. doi:10.1111/anae.14318
14. Almenrader N, Passariello M, Coccetti B, Haiberger R, Pietropaoli P. Premedication in children: a comparison of oral midazolam and oral clonidine. Pediatr Anesth. 2007;17(12):1143–1149. doi:10.1111/j.1460-9592.2007.02332.x
15. Bromfalk Å, Myrberg T, Walldén J, Engström Å, Hultin M. Preoperative anxiety in preschool children: a randomized clinical trial comparing midazolam, clonidine, and dexmedetomidine. Paediatr Anaesth. 2021;2:45. doi:10.1111/pan.14279
16. Cray SH, Dixon JL, Heard CM, et al. Oral midazolam premedication for pediatric day case patients. Paediatr Anaesth. 1996;6:265–270. doi:10.1111/j.1460-9592.1996.tb00448.x
17. Cote CJ, Cohen IT, Suresh S, et al. A comparison of three doses of a commercially prepared oral midazolam syrup in children. Anesth Analg. 2002;94(1):
18. Horbatch F, Hruschak J, Hall M, et al. Conducting EEG research in clinically anxious preschoolers: a pilot study and preliminary recommendations. Dev Psychobiol. 2021;63(7):e22183. doi:10.1002/dev.22183
19. Sadhasivam S, Cohen LL, Hosu L, et al. Real-time assessment of perioperative behaviors in children and parents: development and validation of the perioperative adult child behavioral interaction scale. Anesth Analg. 2010;110(4):1109–1115. doi:10.1213/ANE.0b013e3181d2a509
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.