Back to Journals » Journal of Inflammation Research » Volume 19
Acute Generalized Exanthematous Pustulosis: An Integrated Study of 503 Cases with Emphasis on Drug Culprits, Clinical Features, Diagnosis and Treatment
Authors Lv X ![]() , Song Z
, Song Z ![]() , Xia W, Zhu L, Ruan S, Lin M
, Xia W, Zhu L, Ruan S, Lin M ![]() , Huang J, Chen H, Chen L, Cheng B
, Huang J, Chen H, Chen L, Cheng B
Received 2 December 2025
Accepted for publication 10 February 2026
Published 26 February 2026 Volume 2026:19 580633
DOI https://doi.org/10.2147/JIR.S580633
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Anish R. Maskey
Xiaoqing Lv,1– 4,* Ziping Song,1– 4,* Wenxuan Xia,1– 4,* Li Zhu,1– 4 Shifan Ruan,5 Min Lin,1– 4 Jinwen Huang,1– 4 Huayu Chen,1– 4 Lihong Chen,1– 4 Bo Cheng1– 4
1Department of Dermatology, The First Affiliated Hospital of Fujian Medical University, Fuzhou, Fujian, 350000, People’s Republic of China; 2Institute of Dermatology and Venereology, Fujian Medical University, Fuzhou, Fujian, 350000, People’s Republic of China; 3Fujian Dermatology and Venereology Research Institute, The First Affiliated Hospital, Fujian Medical University, Fuzhou, Fujian, 350000, People’s Republic of China; 4Department of Dermatology, Aoti Campus of The First Affiliated Hospital of Fujian Medical University, Fuzhou, Fujian, 350000, People’s Republic of China; 5School of Medicine, Fuzhou University, Fuzhou, Fujian, 350000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lihong Chen, Department of Dermatology, The First Affiliated Hospital of Fujian Medical University, 20 Chazhong Road, Fuzhou, Fujian, 350000, People’s Republic of China, Tel +86 13799913399, Email [email protected] Bo Cheng, Department of Dermatology, The First Affiliated Hospital of Fujian Medical University, 20 Chazhong Road, Fuzhou, Fujian, 350000, People’s Republic of China, Tel +86 13859024296, Email [email protected]
Background: Acute generalized exanthematous pustulosis (AGEP) is a drug-induced severe cutaneous adverse reaction (SCAR) characterized by an acute extensive erythematous pustular eruption. Integrated analyses including Asian cohorts remain scarce.
Methods: A total of 503 AGEP cases were analyzed by combining two distinct, routinely-collected data cohorts: (1) a literature-derived cohort (PubMed, Embase, Web of Science, and CNKI) and (2) a hospital-based clinical cohort from a tertiary-care center in China. The hospital cohort data were collected retrospectively from January 2015 to July 2025. Demographic, etiologic, clinical, laboratory and therapeutic characteristics were summarized. Drugs were stratified by median latency (3 days) into short- versus long-latency groups to explore class-specific patterns.
Results: Drugs triggered 94.6% of cases, mainly β-lactam antibiotics (20.7%), non-β-lactam antibiotics (16.3%), and hydroxychloroquine (10.4%). With a 3-day median latency threshold, antibiotic-related reactions showed short latency, whereas antimalarials, analgesics, and antifungals exhibited longer latency. Hospitalization occurred in 75.1%, and systemic involvement in 20.2% (mostly hepatic or renal). Mucosal lesions were infrequent (oral 8.7%, genital 1.8%). Among those tested, patch tests were positive in 71.6%. Systemic corticosteroids were the mainstay (63.8%) of treatment, with cyclosporine (3.7%) and intravenous immunoglobulin (2.5%) used as adjuncts. A few refractory cases received biologics, including IL-17 inhibitors (eg secukinumab, brodalumab) and IL-36 receptor blockade (spesolimab), achieving partial or complete response. Eight deaths (1.6%) were documented, mainly among older, comorbid, polymedicated patients.
Conclusion: AGEP displays distinct drug class–specific latency signatures and occasional systemic morbidity. We propose a conceptual AGEP causality triage framework integrating latency and allergologic evidence to enhance culprit identification in polypharmacy settings. Given the mechanistic involvement of the IL-36-Th17/IL-17 axis, biologic agents targeting IL-17 or IL-36 pathways show promise in severe or corticosteroid-refractory AGEP, warranting confirmation in larger prospective studies.
Keywords: acute generalized exanthematous pustulosis, AGEP, adverse drug reaction, retrospective cohort, literature review
Introduction
Acute generalized exanthematous pustulosis (AGEP) is a severe cutaneous adverse reaction (SCAR), most commonly induced by medications, although infections, ultraviolet radiation (photoinduction), vaccinations, exposure to certain substances, and even arthropod bites have also been reported. Its annual incidence is estimated at 1–5 cases per million individuals.1 Although AGEP is rare, its acute presentation often necessitates hospitalization and intensive supportive care, imposing a substantial clinical and economic burden. Clinically, AGEP presents with an acute exanthem that often starts in flexures in a symmetric distribution, which may evolve into erythroderma. Localized exanthematous pustulosis (ALEP) has also been reported and almost always involves a single region like the face, neck, or chest. Other sites, including the extremities, have also been reported.2 It is characterized by the rapid eruption of multiple, pinpoint, non-follicular, sterile pustules arising on an erythematous and edematous base. The rash resolves with extensive psoriasiform desquamation. Targetoid lesions, with incipient necrosis, can coexist with AGEP, especially on the legs.3–5 Itch, pain, and tenderness may also occur, and patients frequently experience fever, malaise, and leukocytosis. The EuroSCAR scoring system is widely used as a diagnostic tool, yet misclassification still occurs in daily practice, particularly in differentiating AGEP from generalized pustular psoriasis (GPP).6 This distinction can be very challenging or impossible as histopathological features are usually similar in both. Eosinophils and sparse necrotic keratinocytes can support the diagnosis, while AGEP generally resolves much more rapidly than GPP. AGEP generally has a favorable prognosis and reported mortality is below 5%, with fatal outcomes typically attributable to multiorgan failure and disseminated intravascular coagulation. Patients with comorbidities and those with diffuse or mucosal involvement are at greatest risk.7 To date, no clinical trials have specifically evaluated targeted therapies for AGEP. Management is primarily supportive, and may include topical corticosteroids, antipyretics, and antihistamines. In severe cases, systemic corticosteroids can be administered.8 The clinical spectrum of AGEP has been described in preliminary studies, including a single-center inpatient cohort from France (83 cases),9 a multinational case series (297 cases),10 and a US multicenter retrospective study (340 cases).11 However, this work was limited to regional populations or relied solely on published reports without primary patient-level data. Building on this work, the present study integrates a larger dataset, incorporating cases from our institution and additional data from China, with the aim of validating established clinical features and identifying new associations in a broader patient population.
Methods
Study Design and Patient Population
This study, conducted as a retrospective case series, collected data from two distinct sources: a literature-based cohort and a hospital-based cohort. The literature-based cohort was assembled through a systematic review of case reports published before July 2025, sourced from the PubMed, Embase, Web of Science, and China National Knowledge Infrastructure (CNKI) databases. A comprehensive search strategy was employed, using a combination of keywords such as: (“acute generalized exanthematous pustulosis ”[MeSH Terms] OR “AGEP” [All Fields]) combined with relevant terms for case reports. For PubMed, Embase, and Web of Science, only publications in English were included, while for CNKI, only publications in Chinese were included. The inclusion of multiple databases was to minimize publication bias and ensure a comprehensive review of the literature. The hospital-based cohort was established by utilizing detailed medical records of patients diagnosed with AGEP from the dermatology inpatient department of the First Affiliated Hospital of Fujian Medical University (FJMU), China, from January 22, 2015, to July 1, 2025.
Ethical Considerations
The hospital-based cohort study was approved by the Ethics Committee of the First Affiliated Hospital of Fujian Medical University (MTCA, ECFAH Of FMU [2015]084-2). Written informed consent was obtained from all patients in the hospital-based cohort. This study was conducted in accordance with the Declaration of Helsinki.
Inclusion and Exclusion Criteria
All cases from both hospital and literature cohorts were screened based on predefined criteria. The process of identifying and selecting cases from the literature followed the PRISMA guidelines, and a detailed flowchart will be presented in Figure 1.
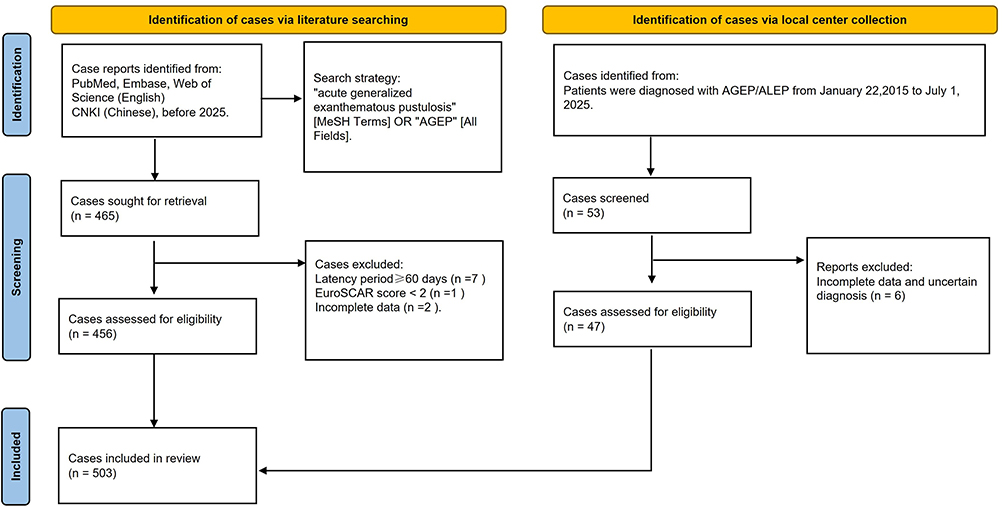 |
Figure 1 Flowchart of the study. |
Inclusion Criteria: 1) A confirmed diagnosis of AGEP, including ALEP; 2) Available data at the individual patient level, containing sufficient information for a comprehensive analysis of patient characteristics, clinical findings, laboratory results, and suspected causative agents; 3) Cases of AGEP caused by any etiology, including drugs, insect bites, dyes, or infective agents, were included.
Exclusion Criteria: 1) Cases with an unclear or suspected diagnosis of AGEP; 2) Cases with significant missing data that would preclude accurate or complete extraction of key variables.
Clinical Data Collection
Two independent researchers extracted data from the medical records and literature. Any discrepancies were resolved by consensus or through consultation with a third senior researcher. The following variables were extracted and defined: patient characteristics (age, sex, history of drug allergy, and comorbidities), suspected causes of AGEP, number of suspected drugs and time to onset of symptoms, clinical characteristics (presence of fever (>38°C), extent of skin involvement, systemic involvement, and hospitalization status), laboratory parameters (white blood cell count, absolute neutrophil count, absolute eosinophil count, serum sodium, potassium, and calcium), results of patch tests (positive/negative), with the total number of patients who underwent testing documented, Histopathological findings from skin biopsies, treatment and outcome.
The following assumptions were made to standardize the data collection process. When a patient’s age was reported within a 10-year range, such as “in their 60s”, the midpoint of the decade was used (eg, 65 years). Race and country of origin were not collected in this study. In the absence of an explicit mention or indication of systemic involvement or other specific medical history, it was assumed that these conditions were not present. For ambiguous but informative descriptions, the following conversions were applied: “a few hours” or “several hours” was coded as 0.5 days; “less than 24 h” as 1 day; and “a few days” as 3 days. Cases with completely non-quantifiable descriptions remained as missing data. When a drug was administered multiple times, the onset was calculated from the date of the first administration. Performance of a percutaneous test was recorded as a patch test. Time to onset was recorded in days.
Statistical Analysis
Statistical analysis was performed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA) and Microsoft Excel version 2019 MSO (Microsoft Corp., Redmond, WA, USA). Descriptive statistics were used to summarize the data. Continuous variables were expressed as mean ± standard deviation (SD) for normally distributed data or median [interquartile range, IQR] for non-normally distributed data. Categorical variables were presented as counts and percentages [n (%)].
Results
Patient Demographics and Clinical Characteristics
The final analytic cohort of 503 patients was established by combining cases from the literature-based cohort (initial n=465) and the hospital-based cohort (initial n=53), as described in the Methods section. A total of 15 cases were excluded from both cohorts (9 from the literature and 6 from the hospital) due to insufficient data quality, uncertain diagnosis, or failure to meet the predefined inclusion criteria (such as a latent period exceeding 60 days or EuroSCAR score <2). The detailed selection process, including filtering based on data quality and availability, is presented in Figure 1. The mean age was 46.0 ± 22.0 years (range: infancy to 92 years), and males represented 33.4% (n = 168), with pediatric patients (18 years) comprising 12.7% (Supplementary Tables S1 and S2). Comorbidities were present in 38.6% (n = 194), most commonly hypertension (10.1%), cardiovascular disease (7.6%), diabetes (6.6%), and psoriasis (4.0%) (Table 1). A prior history of drug allergy was reported in 7.2% (n = 36). Histories of other severe cutaneous adverse reactions were rare: drug reaction with eosinophilia and systemic symptoms (DRESS) in eight patients (1.6%) and Stevens-Johnson syndrome/toxic epidermal necrolysis (SJS/TEN) in three patients (0.6%). These findings indicate that AGEP can affect both previously sensitized and naïve individuals.
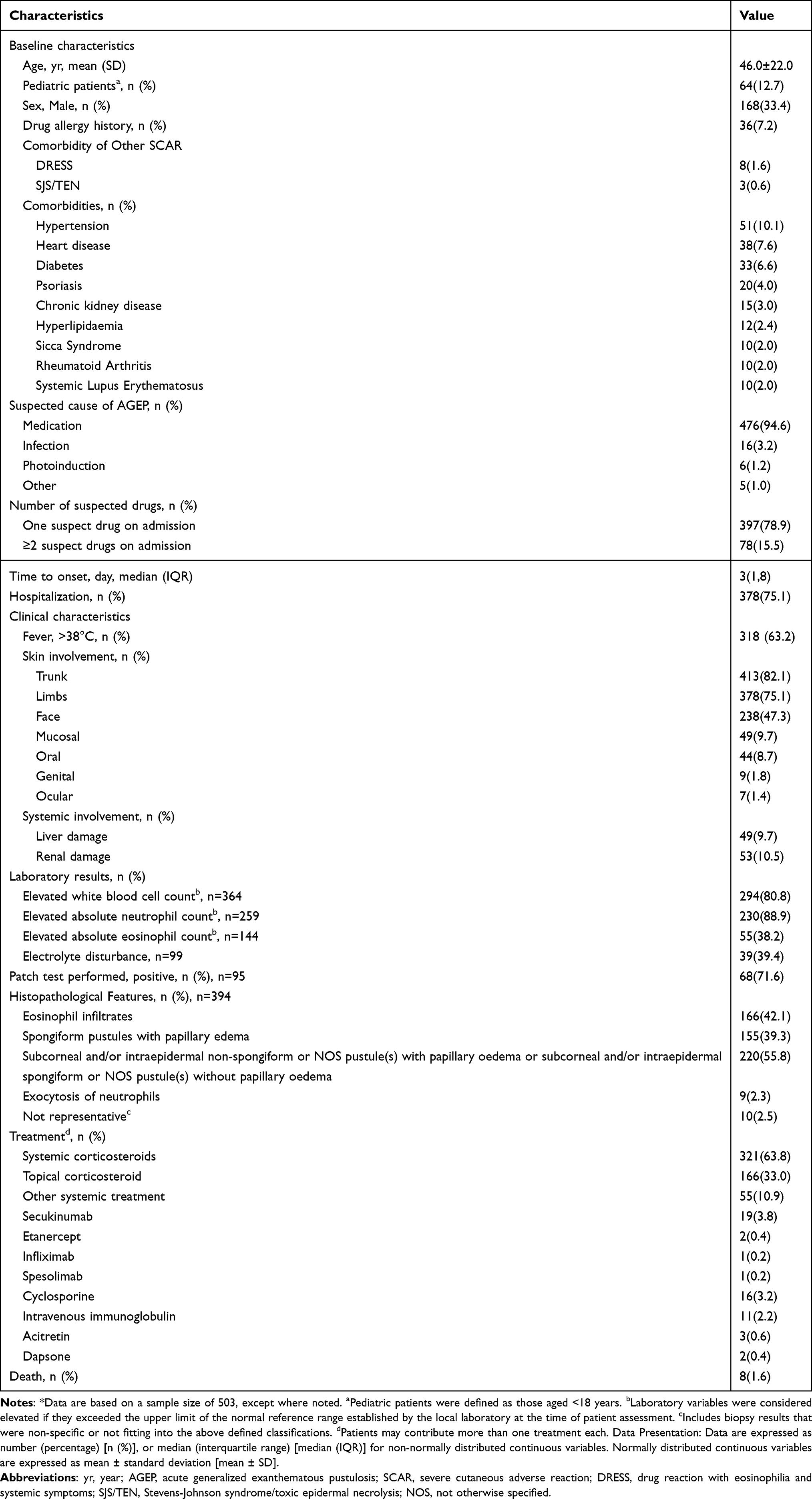 |
Table 1 Demographic, Clinical, Laboratory, and Treatment Characteristics of Patients with Acute Generalized Exanthematous Pustulosis (n = 503)* |
Etiology of AGEP
Drugs were the primary trigger, accounting for 94.6% of cases (n = 476), while infections (3.2%, n = 16), photoinduction (1.2%, n = 6), were uncommon (Table 1). Most drug-induced cases could be attributed to a single culprit agent (78.9%, n = 397), whereas 15.5% (n = 78) involved more than one potentially responsible drug. β-lactam antibiotics were the leading drug category (20.7%, n = 119), with amoxicillin and amoxicillin–clavulanic acid most frequently reported. Non–β-lactam antibiotics (16.3%, n = 94) and antimalarials (10.4%, n = 60), mainly hydroxychloroquine, were also common. Analgesics (8.9%), antitumor or immunosuppressive drugs (8.7%), and contrast media (7.0%) contributed to a smaller fraction (Table 2 and Figure 2). These results reflect the predominance of commonly used antibiotics and antimalarials in AGEP causation.
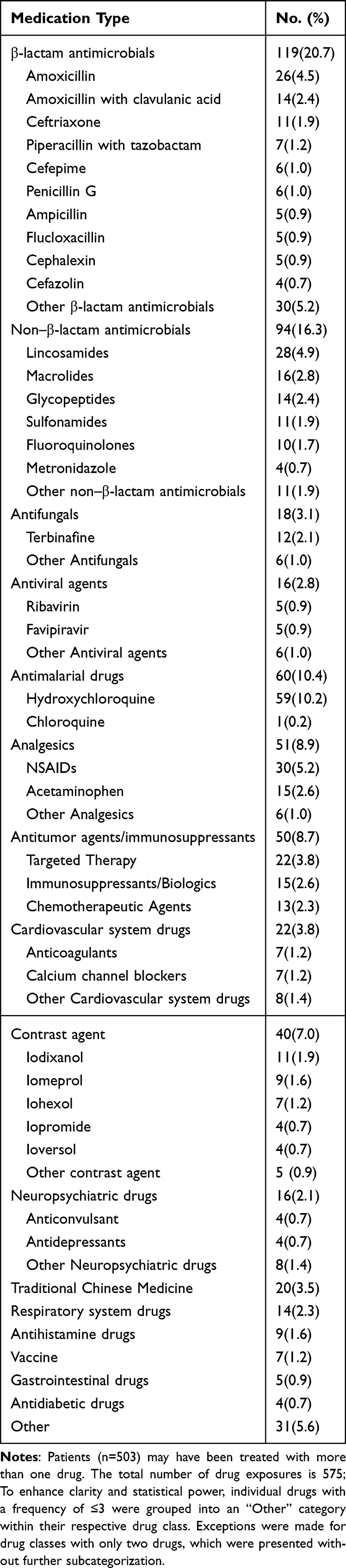 |
Table 2 Characteristics of Reported Suspect Drugs for Acute Generalized Exanthematous Pustulosis |
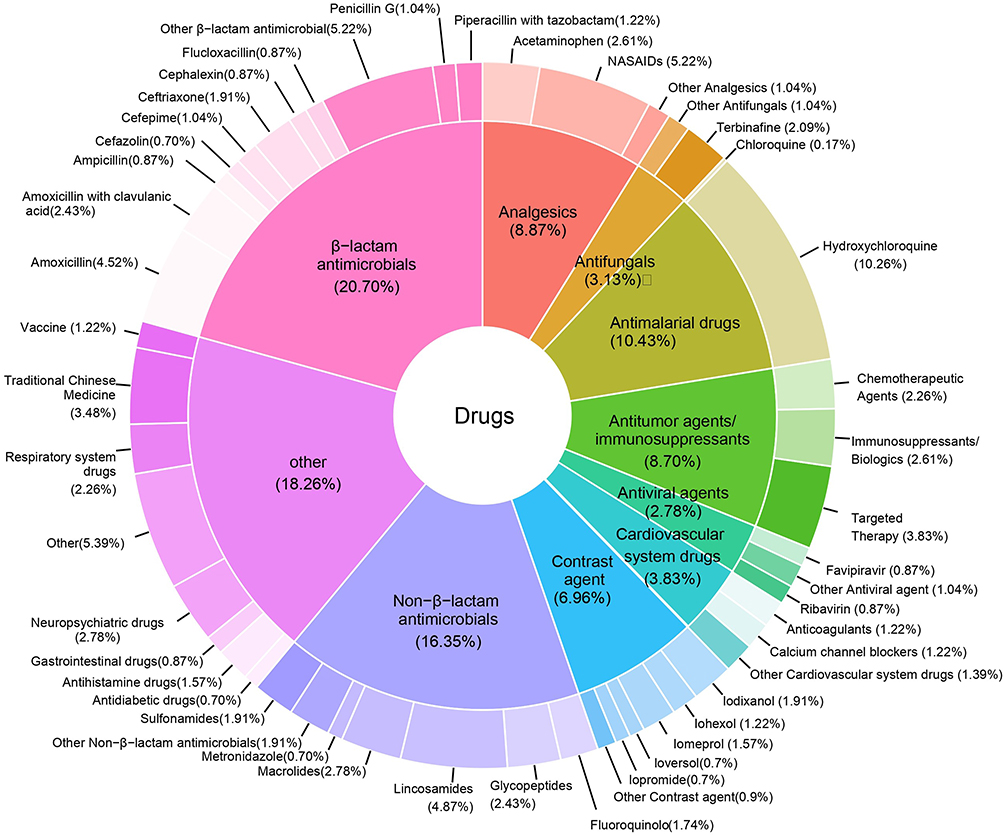 |
Figure 2 Doughnut charts illustrating the culprit drugs in AGEP cases at our center and literature. |
Clinical Features and Laboratory Findings
The median latency from exposure to symptom onset was 3 days (IQR 1-8), consistent with the typically rapid onset of AGEP. Based on the median latency period of all drugs (3 days), we defined a threshold to categorize the drugs into long and short latency periods. The results, as shown in the Figure 3, reveal that certain drug categories, such as antimalarial drugs, analgesics, and antifungals, exhibited significant differences in latency periods within the population.
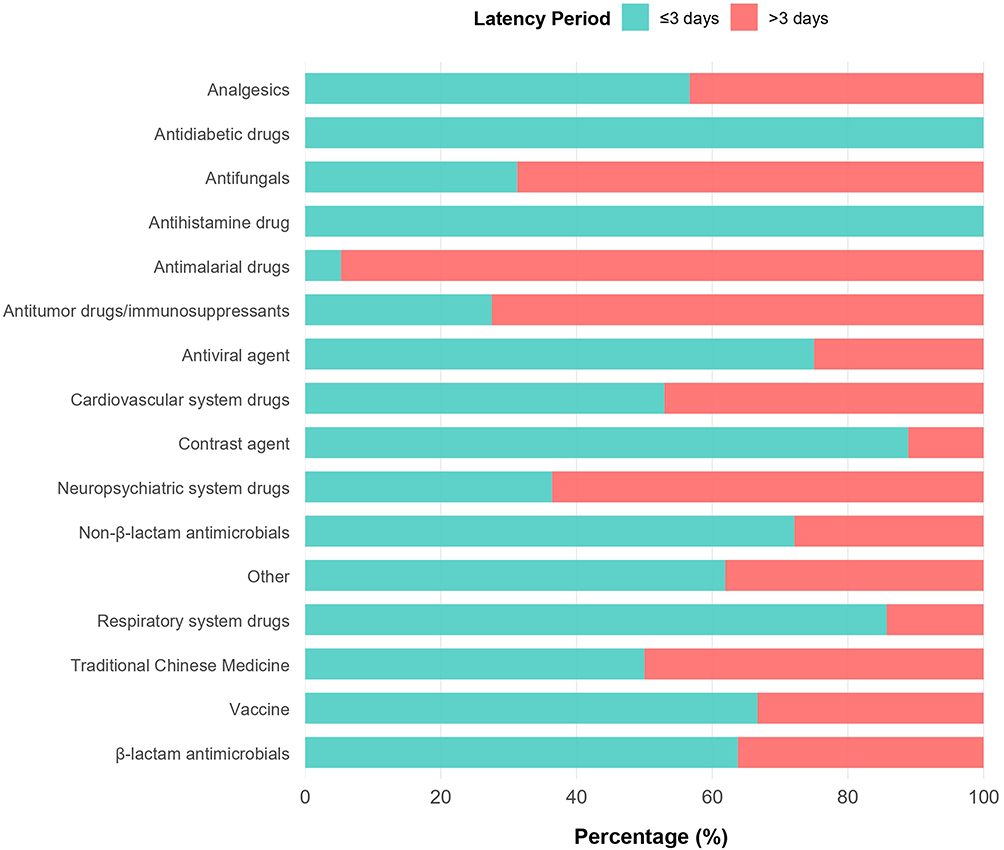 |
Figure 3 Latency Periods of Suspected Drugs in AGEP Patients. Notes: Analysis restricted to cases with a single suspected culprit drug; patients with ≥2 suspected drugs were excluded to reduce confounding. |
Hospitalization was required in 75.1% of cases (n = 378). Fever occurred in 63.2% (n = 318). Cutaneous lesions predominantly affected the trunk (82.1%) and limbs (75.1%), with facial involvement in 47.3%. Mucosal lesions were uncommon (oral, 8.7%; genital, 1.8%). Extensive involvement consistent with erythroderma was rare (1.2%). A detailed breakdown of involved body sites is provided in Supplementary Table S3. Systemic involvement was reported in 20.2% of patients, most frequently hepatic (9.7%) and renal (10.5%). Laboratory abnormalities included leukocytosis (80.8%), neutrophilia (88.9%), eosinophilia (38.2%), and electrolyte disturbances (39.4%). Histopathology (n = 398) typically showed subcorneal or intraepidermal pustules, with dermal edema in nearly half of specimens. Only 95 patients underwent patch testing, but the positive rate was high (71.6%).
Treatment and Outcomes
Treatment was predominantly corticosteroid-based: 63.8% received systemic corticosteroids, and 33.0% received topical corticosteroids. Other interventions included cyclosporine (3.7%), intravenous immunoglobulin (2.5%), and biologics such as secukinumab (3.8%). Details of systemic corticosteroid regimens (agent, route, and starting dose, where reported) are provided in Supplementary Table S4.
Overall, eight patients died (1.6%). Notably, two deaths occurred among the six patients with erythroderma (2/6, 33.3%), accounting for 25.0% (2/8) of all fatal cases. Deceased patients were older (median age 71 years) and had significant comorbidities, including malignancy, severe infection, or critical illness (Table 3). All fatal cases involved exposure to multiple drugs, particularly broad-spectrum antimicrobials and targeted therapies. Causes of death included multiple organ failure (n = 3), sepsis (n = 3), pulmonary embolism (n = 1), and myocardial infarction (n = 1). Although the absolute numbers are small, this pattern suggests that very extensive skin involvement, advanced age, comorbidities, and polypharmacy may be associated with an increased risk of mortality.
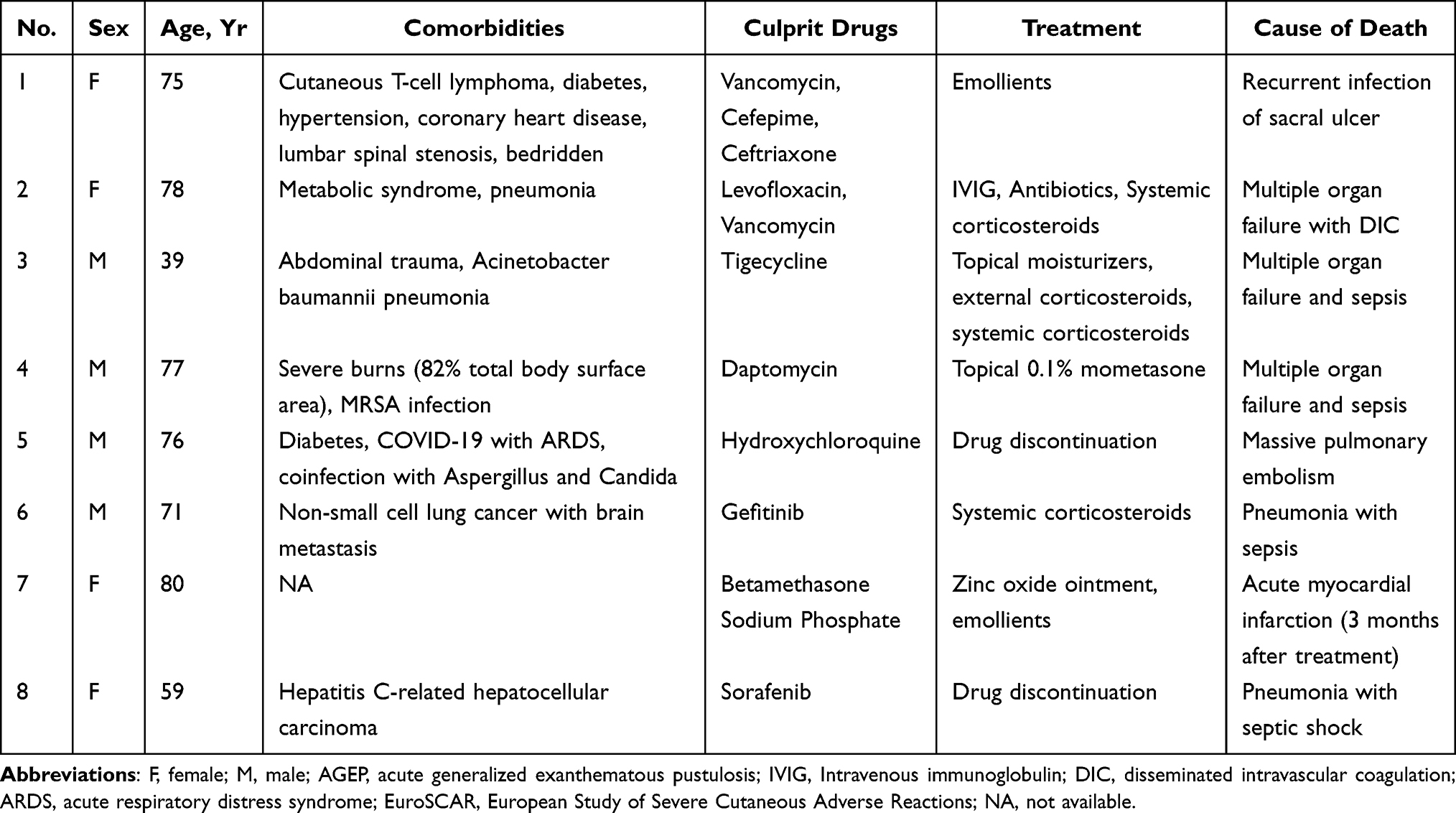 |
Table 3 Information on Deceased Patients with AGEP in This Study (n=8) |
Discussion
AGEP is an uncommon but prototypical T cell–mediated type IV hypersensitivity reaction, most frequently triggered by drugs. The immunopathogenesis of AGEP involves activation of drug-specific T cells and cytokine cascades such as the IL-36/Th17–IL-8 axis. However, current mechanistic and epidemiologic evidence has been derived mainly from Western populations, and data from Asian cohorts remain limited. To bridge this gap, we conducted an aggregated analysis of 503 patients by integrating published cases from both international and Chinese databases (including CNKI) together with case data from a tertiary-care hospital in China. This comprehensive dataset broadens the geographic scope of AGEP research and provides a more inclusive overview of its clinical spectrum.
The demographic characteristics of patients in this case series were generally comparable to those reported in other observational studies. A female predominance was observed, consistent with previous evidence.12 The mean age in our cohort was 46 years, lower than the 51.7–62 years reported in other observational and multicenter studies.11,13–15 AGEP was overwhelmingly drug-induced (94.6%), with β-lactams (20.7%), non-β-lactam antibiotics (16.3%), and hydroxychloroquine (10.4%) as the most frequently implicated agents. Regarding clinical manifestations, 63.2% of patients developed fever, a proportion similar to the 64.3% reported in a multinational study in 2022.10 Skin lesions predominantly involved the trunk, extremities, and face. Mucosal involvement was uncommon, most commonly the oral mucosa followed by the genital mucosa. Previous reports have noted that even severe AGEP cases may present with vesicles, bullae, or a positive Nikolsky sign, which necessitates careful differentiation from SJS/TEN.16 Such cases may represent either an extreme phenotype of AGEP or a true overlap syndrome. EuroSCAR scoring and histopathology can aid in distinguishing between these entities. Overlap is rare: in our cohort, only 3 cases of AGEP overlapped with SJS/TEN, whereas 8 cases overlapped with DRESS.
With respect to systemic involvement, 9.7% of patients developed liver injury and 10.5% developed kidney injury in our cohort. In comparison, a US study of 340 patients reported hepatic dysfunction and acute kidney injury in 8.4% and 7.8% of cases, respectively.11 The same study also identified frequent comorbidities among AGEP patients, including diabetes, renal impairment, prior psoriasis, and allergic disorders.11 In our data, additional comorbidities were observed, such as hypertension, cardiovascular disease, hyperlipidemia, Sjögren’s syndrome, and rheumatoid arthritis. Laboratory abnormalities were consistent with previous reports, including leukocytosis with neutrophilia, elevated C-reactive protein (CRP), and mild eosinophilia in approximately one-third to one-half of cases. Notably, among the 99 patients with available electrolyte data, 39.4% exhibited electrolyte imbalances. A recent retrospective study likewise reported that a substantial proportion of AGEP patients had electrolyte abnormalities—an observation that has been rarely mentioned in earlier literature.17
AGEP typically presents with an abrupt onset. In both our cohort and a US study of 340 patients,11 the median latency was 3 days, which was adopted as the threshold for stratified analysis. Distinct class-related differences were observed: most antibiotics clustered in the short-latency group, whereas antimalarials (notably hydroxychloroquine), analgesics, and antifungals were enriched in the long-latency group. A French single-center study also described this pattern, reporting that β-lactams and contrast media typically induced AGEP within ≤2 days, whereas hydroxychloroquine was associated with substantially longer latencies.9 This distribution is biologically plausible. β-lactams are characterized by short plasma half-lives (2 h) and multiple daily dosing, which enables rapid attainment of sensitizing concentrations.18 In contrast, hydroxychloroquine has a terminal half-life of 40–60 days, requiring 2–3 weeks of tissue accumulation to reach steady-state concentrations, consistent with its longer latency.19 Moreover, exposure patterns may also influence onset: classical immunologic concepts indicate that re-exposure often triggers faster and more severe reactions, as documented in SJS/TEN and DRESS.20 Likewise, clinical improvement after drug withdrawal (dechallenge) is a recognized cornerstone in both the WHO-UMC causality categories and the Naranjo scale.21 Collectively, these findings support the integration of latency and exposure characteristics into causality assessment for AGEP.
Previous studies have shown that more than half of AGEP patients were exposed to multiple drugs before disease onset.10 In such complex medication settings, certain agents may covalently bind to host proteins, forming hapten–protein adducts that activate the immune system and trigger AGEP,12 supporting the biological plausibility of multi-drug hypersensitivity. However, although co-sensitization by multiple agents has been reported, its overall frequency appears relatively low; in most instances, overlapping exposures or incomplete evidence complicate causality assessment. In our analysis, drugs with chronic use or poor temporal correlation were excluded, yet 15.5% of cases still retained two plausible culprit drugs—likely an overestimation driven by diagnostic uncertainty rather than true dual causality. These findings should therefore be interpreted with caution and underscore that, in the setting of polypharmacy, reliance solely on clinical judgment is insufficient, highlighting the need for a structured and reproducible approach to causality assessment. However, unlike SJS/TEN, for which the ALDEN algorithm is widely adopted, AGEP lacks a dedicated causality tool. Patch testing, although recommended to identify culprit drugs, is often limited by timing constraints (must be performed after recovery) and carries a potential risk of relapse, resulting in limited utilization (approximately 20% of published cases). To address this gap, we propose an AGEP Causality Triage (ACT) framework, inspired by the logic of ALDEN, as a heuristic bedside tool. ACT encourages clinicians to consider several key dimensions when evaluating drug causality—timing concordance (eg, patient-level vs class-typical latency, with 3 days as a reference), known drug association strength (as reflected in pharmacovigilance warnings by the EMA and FDA), exposure characteristics (dose, re-exposure, dechallenge evidence), exclusion of alternative causes, and supportive allergologic findings (patch or lymphocyte transformation tests). However, it currently serves as a conceptual framework rather than a quantitative tool, as specific scoring criteria and weighting systems remain to be established.
AGEP is driven by drug-specific T cells that release IL-8/CXCL8 and GM-CSF, inducing neutrophil recruitment and sterile pustule formation. Recent studies further implicate IL-36 overexpression and Th17/IL-17 activation as amplifiers of this inflammatory cascade.22,23 In rare cases, loss-of-function mutations in IL36RN disrupt the negative regulation of IL-36 signaling, predisposing to persistent inflammation and pustular eruptions.24 Collectively, these findings place AGEP within the IL-36–Th17/IL-17–IL-8 axis, a pathway shared with other IL-36–related pustular dermatoses such as generalized pustular psoriasis.25
Building on these mechanistic insights, we next examined real-world treatment patterns and therapeutic outcomes. In our cohort of 503 patients, most received systemic and/or topical corticosteroids, while smaller proportions were treated with cyclosporine, intravenous immunoglobulin, or biologics. The relatively high rate of systemic corticosteroid use likely reflects inclusion of more severe hospitalized cases. Corticosteroids remain the mainstay of therapy, yet their variable efficacy and potential adverse effects in refractory cases highlight the need for targeted, mechanism-based approaches.
Given the central role of the IL-36–Th17/IL-17–IL-8 axis, cytokine-targeted biologics—particularly IL-17 and IL-36 inhibitors—represent promising candidates. IL-17 blockade can reduce IL-8 production, limit neutrophil recruitment, and accelerate pustule resolution. Supporting this, clinical observations suggest that IL-17 inhibitors combined with corticosteroids may achieve faster improvement than corticosteroids alone.17 Upstream inhibition of IL-36 signaling may offer additional benefit, particularly in patients harboring variants. Overall, IL-17/IL-36-targeted biologics appear biologically plausible and clinically promising, especially for severe or steroid-refractory AGEP. However, current evidence is confined to small case series and individual reports. Large, multicenter, biomarker-stratified studies are warranted to validate the efficacy, safety, and long-term outcomes of these targeted therapies.
In our study, the hospitalization rate for AGEP was 75.1%, with 8 deaths (1.6%) recorded. This mortality rate lies at the lower end of the range reported in previous studies (typically <5%),26 indicating that although AGEP is generally considered a self-limiting condition, it can still be associated with severe outcomes in certain vulnerable populations. Fatal cases predominantly occurred in older patients with multiple comorbidities receiving polypharmacy, and the immediate causes of death were most commonly sepsis and multiorgan failure. Notably, several patients exhibited a temporal dissociation in which cutaneous lesions had markedly improved before subsequent death. This pattern supports the notion that AGEP may act as a marker of underlying host frailty or share common risk factors with adverse outcomes—such as infection susceptibility, limited organ reserve, or drug–drug interactions—rather than serving as a direct cause of death. In other words, AGEP may co-occur with and amplify adverse outcomes, but causal attribution is inherently challenging in the context of multimorbidity and polypharmacy. Moreover, incomplete follow-up data and limited reporting timeframes may further lead to over- or underestimation of mortality rates.
As a retrospective study integrating data not originally collected for research purposes, our findings are subject to inherent limitations. These include: (1) Heterogeneous and incomplete reporting: key variables (severity, selected labs, follow-up/time to remission, and systemic corticosteroid regimen details) were often missing, introducing information/selection bias and limiting treatment–outcome comparisons; (2) Potential misclassification: variable diagnostic standards and multi-drug exposures may have affected case and trigger classification; (3) Residual confounding: important patient-level factors (eg, genetics, complete chronic co-medications) were unavailable; (4) Time-related bias: reporting and diagnostic practices may have evolved over the long study period.
Conclusion
This study analyzed 503 AGEP cases, representing one of the largest datasets to date and offering a comprehensive overview of its clinical spectrum. The major strengths lie in the large, diverse sample and the introduction of a structured approach for drug causality assessment. However, as the data were mainly retrospective, incomplete records on disease severity, laboratory results, and follow-up may have introduced information and selection bias. In conclusion, this study defines the drug spectrum and clinical features of AGEP, providing a basis to enhance clinical recognition, guide rational drug withdrawal, and promote biomarker- and pharmacokinetics-based precision management.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Contributions
Xiaoqing Lv: Formal Analysis, Investigation, Data Curation, Writing – Original Draft Preparation, and Visualization. Ziping Song: Formal Analysis, Investigation, Data Curation, Writing – Original Draft Preparation, and Visualization. Wenxuan Xia: Formal Analysis, Investigation, Data Curation, Writing – Original Draft Preparation, and Visualization. Li Zhu: Investigation, Visualization, Validation, and Writing – Review & Editing. Shifan Ruan: Investigation, Resources, Validation, and Writing – Review & Editing. Min Lin: Investigation, Resources, Validation, and Writing – Review & Editing. Jinwen Huang: Investigation, Resources, Validation, and Writing – Review & Editing. Huayu Chen: Investigation, Resources, Validation, and Writing – Review & Editing. Lihong Chen: Conceptualization, Methodology, Writing – Review & Editing, Supervision, and Project Administration. Bo Cheng: Conceptualization, Methodology, Writing – Review & Editing, Supervision, and Project Administration. All authors have agreed on the final version of the manuscript for publication, have agreed on the journal to which the paper is submitted, and have agreed to be accountable for the work published.
Funding
This work was supported by the Fujian Provincial Health Technology Project [No.2020CXA034]; the Joint Funds for the Innovation of Science and Technology, Fujian Province [No.2020Y9120]; and the Key Discipline Construction Program of Traditional Chinese Medicine in Fujian Province.
Disclosure
The authors declare that there is no conflict of interest regarding the publication of this article.
References
1. Sidoroff A, Halevy S, Bavinck JN, Vaillant L, Roujeau JC. Acute generalized exanthematous pustulosis (AGEP)--a clinical reaction pattern. J Cutan Pathol. 2001;28(3):113–13. doi:10.1034/j.1600-0560.2001.028003113.x
2. Safa I, Ines L, Noureddine L, et al. Acute localized exanthematous pustulosis: clinical features, pathophysiology, and therapy. Dermatol Ther. 2021;34(5):e15087. doi:10.1111/dth.15087
3. Duman H, Topal IO, Kocaturk E, Cure K, Mansuroglu I. Acute generalized exanthematous pustulosis induced by hydroxychloroquine: a case with atypical clinical presentation. An Bras Dermatol. 2017;92(3):404–406. doi:10.1590/abd1806-4841.20175561
4. Lin JH, Sheu HM, Lee JY. Acute generalized exanthematous pustulosis with erythema multiforme-like lesions. Eur J Dermatol. 2002;12(5):475–478.
5. Kostopoulos TC, Krishna SM, Brinster NK, Ortega-Loayza AG. Acute generalized exanthematous pustulosis: a typical presentations and outcomes. J Eur Acad Dermatol Venereol. 2015;29(2):209–214. doi:10.1111/jdv.12721
6. Parisi R, Shah H, Navarini AA, et al. Acute generalized exanthematous pustulosis: clinical features, differential diagnosis, and management. Am J Clin Dermatol. 2023;24(4):557–575. doi:10.1007/s40257-023-00779-3
7. Szatkowski J, Schwartz RA. Acute generalized exanthematous pustulosis (AGEP): a review and update. J Am Acad Dermatol. 2015;73(5):843–848. doi:10.1016/j.jaad.2015.07.017
8. Tetart F, Walsh S, Milpied B, et al. Acute generalized exanthematous pustulosis: European expert consensus for diagnosis and management. J Eur Acad Dermatol Venereol. 2024;38(11):2073–2081. doi:10.1111/jdv.20232
9. Weiss M, Assier H, Hotz C, et al. Acute generalized exanthematous pustulosis: clinico-biological profile and inducing drugs in 83 patients. J Eur Acad Dermatol Venereol. 2023;37(6):e776–e778. doi:10.1111/jdv.18940
10. Vallejo-Yagüe E, Martinez-De la Torre A, Mohamad OS, Sabu S, Burden AM. Drug triggers and clinic of acute generalized exanthematous pustulosis (AGEP): a literature case series of 297 patients. J Clin Med. 2022;11(2). doi:10.3390/jcm11020397
11. Creadore A, Desai S, Alloo A, et al. Clinical characteristics, disease course, and outcomes of patients with acute generalized exanthematous pustulosis in the US. JAMA Dermatol. 2022;158(2):176–183. doi:10.1001/jamadermatol.2021.5390
12. Martinez-De la Torre A, van Weenen E, Kraus M, Weiler S, Feuerriegel S, Burden AM. A network analysis of drug combinations associated with acute generalized exanthematous pustulosis (AGEP). J Clin Med. 2021;10(19):4486. doi:10.3390/jcm10194486
13. Barbaud A, Collet E, Milpied B, et al. A multicentre study to determine the value and safety of drug patch tests for the three main classes of severe cutaneous adverse drug reactions. Br J Dermatol. 2013;168(3):555–562. doi:10.1111/bjd.12125
14. Thienvibul C, Vachiramon V, Chanprapaph K. Five-year retrospective review of acute generalized exanthematous pustulosis. Dermatol Res Pract. 2015;2015:260928. doi:10.1155/2015/260928
15. Daq O, Yeo YW, Choo KJL, Pang SM, Oh CC, Lee HY. Acute generalized exanthematous pustulosis: epidemiology, clinical course, and treatment outcomes of patients treated in an Asian academic medical center. JAAD Int. 2021;3:1–6. doi:10.1016/j.jdin.2020.12.004
16. Moreno-Arrones OM, Carrillo-Gijon R, Sendagorta E, Rios-Buceta L. Acute generalized exanthematous pustulosis simulating Stevens-Johnson syndrome/toxic epidermal necrolysis associated with the use of vismodegib. JAAD Case Rep. 2018;4(2):123–125. doi:10.1016/j.jdcr.2017.08.001
17. Lv XQ, Ruan SF, Chen JW, et al. Evaluation of combination therapy with secukinumab and systemic corticosteroids for acute generalized exanthematous pustulosis: a retrospective cohort study. J Am Acad Dermatol. 2025;93(4):1075–1077. doi:10.1016/j.jaad.2025.05.1419
18. Smith PW, Zuccotto F, Bates RH, et al. Pharmacokinetics of β-lactam antibiotics: clues from the past to help discover long-acting oral drugs in the future. ACS Infect Dis. 2018;4(10):1439–1447. doi:10.1021/acsinfecdis.8b00160
19. Rapparini L, Cedirian S, La Placa M, Piraccini BM, Raschi E, Starace M. Safety of hydroxychloroquine: what a dermatologist should know. Am J Clin Dermatol. 2025;26(2):251–264. doi:10.1007/s40257-025-00919-x
20. Peter JG, Lehloenya R, Dlamini S, et al. Severe delayed cutaneous and systemic reactions to drugs: a global perspective on the science and art of current practice. J Allergy Clin Immunol Pract. 2017;5(3):547–563. doi:10.1016/j.jaip.2017.01.025
21. More SA, Atal S, Mishra PS. Inter-rater agreement between WHO- Uppsala Monitoring Centre system and Naranjo algorithm for causality assessment of adverse drug reactions. J Pharmacol Toxicol Methods. 2024;127:107514. doi:10.1016/j.vascn.2024.107514
22. Stadler PC, Oschmann A, Kerl-French K, et al. Acute generalized exanthematous pustulosis: clinical characteristics, pathogenesis, and management. Dermatology. 2023;239(3):328–333. doi:10.1159/000529218
23. Meier-Schiesser B, Feldmeyer L, Jankovic D, et al. Culprit drugs induce specific IL-36 overexpression in acute generalized exanthematous pustulosis. J Invest Dermatol. 2019;139(4):848–858. doi:10.1016/j.jid.2018.10.023
24. Navarini AA, Valeyrie-Allanore L, Setta-Kaffetzi N, et al. Rare variations in IL36RN in severe adverse drug reactions manifesting as acute generalized exanthematous pustulosis. J Invest Dermatol. 2013;133(7):1904–1907. doi:10.1038/jid.2013.44
25. Benezeder T, Bordag N, Woltsche J, et al. IL-36-driven pustulosis: transcriptomic signatures match between generalized pustular psoriasis (GPP) and acute generalized exanthematous pustulosis (AGEP). J Allergy Clin Immunol. 2025;155(6):1913–1927. doi:10.1016/j.jaci.2025.01.046
26. Fernando SL, Li J, Toon CW, Weir C. Acute generalized exanthematous pustulosis to a novel oral anticoagulant (apixaban). Ann Allergy Asthma Immunol. 2021;127(5):588–589. doi:10.1016/j.anai.2021.07.022
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.