")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Acute Effects of Intravenous Sub-Anesthetic Doses of Ketamine and Intranasal Inhaled Esketamine on Suicidal Ideation: A Systematic Review and Meta-Analysis
Authors Chen CC, Zhou N, Hu N, Feng JG , Wang XB
Received 20 December 2022
Accepted for publication 3 March 2023
Published 14 March 2023 Volume 2023:19 Pages 587—599
DOI https://doi.org/10.2147/NDT.S401032
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yuping Ning
Cheng-Chuan Chen,1,* Na Zhou,2,* Na Hu,1 Jian-Guo Feng,1 Xiao-Bin Wang1
1Department of Anesthesiology, The Affiliated Hospital of Southwest Medical University, Luzhou, Sichuan Province, People’s Republic of China; 2School of Nursing, Southwest Medical University, Luzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiao-Bin Wang, Department of Anesthesiology, The Affiliated Hospital of Southwest Medical University, Luzhou, Sichuan Province, People’s Republic of China, Tel +86 13708280087, Fax +86 830-3161222, Email [email protected]
Purpose: Suicide is a major public health concern with currently no validated and efficacious treatments approved. Preliminary evidence suggests that intravenous ketamine has rapid and sustained antidepressant effects, making it a candidate with therapeutic potential for depressed patients at risk for suicide. We conducted a meta-analysis to evaluate the efficacy of ketamine and esketamine in reducing suicidal ideation (SI), as well as their respective onset and duration of action.
Data Sources: We searched PubMed, Embase, Ovid, Cochrane, and Web of Science databases for studies published from inception to September 29, 2022.
Study Eligibility Criteria: We conducted a systematic review of all parallel randomized controlled trials (RCTs) examining the effect and duration of ketamine or esketamine on SI. Our primary outcome measure was the Suicide Scale score, which was measured using the Scale for Suicidal Ideation (SSI), Beck Scale for Suicide Ideation (BSS), Beck Depression Inventory (BDI), or Modified Scale for Suicidal Ideation (MSSI). To obtain effect sizes (Cohen’s d), we calculated the difference in Suicide Scale scores before and after administration in each group.
Results: Our study showed that intravenous sub-anesthetic doses of ketamine and intranasal inhaled esketamine had a significant anti-SI effect. Specifically, ketamine produced a large degree of anti-SI effect within the 4– 6 hours (Cohen’s d = 1.16, 95% CI: 0.50, 1.81) and a medium-large degree in the 24 hours (Cohen’s d = 0.95, 95% CI: 0.48, 1.41). Esketamine, on the other hand, produced a small-medium degree of anti-SI effect within the 4– 6 hours timeframe (Cohen’s d = 0.26, 95% CI: 0.09, 0.44) and the 24 hours (Cohen’s d = 0.30, 95% CI: 0.17, 0.47).
Conclusion: Intravenous sub-anesthetic doses of ketamine and intranasal inhaled esketamine could reduce SI within 4 hours and last for 24 hours.
Keywords: ketamine, esketamine, suicide ideation, depressive disorder
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Manu has been published for this article.
Introduction
The World Health Organization (WHO) recently reported that although the global suicide rate has fallen sharply since 2000, it has risen in some regions, such as the United States, where suicide rates for men and women have increased by 26% and 38%, respectively.1 This demonstrates that suicidal behavior remains a global health problem that places a huge economic and emotional burden on the world.2 Suicidal behavior includes suicidal ideation (SI), suicide plan, and suicide attempt. Among them, SI is the most sensitive predictor.3 Current treatment for patients with acute SI usually consists of cognitive behavioral therapy, psychological treatment, and medication-assisted treatment, which have been proven to be effective in reducing SI.4–6 However, their efficacy in crisis situations has yet to be determined. It has been suggested that patients with major depression or SI may require rapid-acting anti-SI medications for effective treatment.7
Recent studies have found that the commonly used anesthetic ketamine has rapid and long-lasting antidepressant and anti-SI effects, making it a hot topic. Ketamine has multiple effects by binding to NMDA, AMPA, GABA receptors, and various ion channels.8 However, a proportion of patients with major depressive disorder (MDD) have psychotic features, such as bipolar disorder, presenting as psychotic treatment-resistant depression (TRD) and unresponsive to recommended therapeutic interventions. Fortunately, ketamine appears to ameliorate the symptoms of depression at subanesthetic doses among individuals with MDD.9 This follows extensive research on the racemic ketamine as well as (R)-ketamine (arketamine) and (S)-ketamine (esketamine) enantiomers. Consequently, esketamine was recently approved by the US Food and Drug Administration (FDA) for the acute management of MDD, depressive symptoms in adults with MDD with acute SI or behavior (MDSI), and as an adjunctive psychiatric indication for the treatment of MDD with a psychiatric emergency (MDD-PE).10,11 Several RCTs and meta-analysis have reported that ketamine and esketamine have a good safety and tolerability profile in MDD or TRD, with rapid and effective antidepressant and anti-SI effects.12–14 Given the findings of the above mentioned studies, there is growing interest in exploring whether ketamine and esketamine can be used to rescue patients with acute SI.
However, evidence-based treatments on the role of ketamine and esketamine in reducing SI and suicidal behavior remain inadequate. Therefore, we performed a meta-analysis to assess the effect of ketamine/esketamine on SI by comparing the degree of remission of SI in patients in the intervention and control groups.
Methods
Search Strategy and Eligibility Criteria
The protocol for this study is registered with PROSPERO (CRD42022363936). We followed PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) guidelines and searched the PubMed, Embase, Ovid, Cochrane, and Web of Science databases for MeSH terms “ketamine” or “esketamine” and “suicidal ideation” (Supplementary Material). We searched for studies published from inception to September 29, 2022. In addition to open-label trials and crossover trials, any double-blind clinical trial evaluating ketamine versus placebo could initially be included.
We only included parallel RCTs. The included population consisted of men and women between the ages of 18 and 80 years. Patients had a clinically assessed Suicide Scale (SSI/BDI) and Depression Scale (HAMD/MARDS) or a history of MDD with clinically significant SI consistent with a DSM-IV (Diagnostic and Statistical Manual of Mental Disorders) diagnosis. Psychiatric illness (such as schizophrenia or schizoaffective disorder), acute medical comorbidities, and serious substance use disorders (ketamine or other substances) were exclusion criteria.
If study data are incomplete, we will contact the corresponding author for additional information. After removing duplicates and carefully reading the full text, we ultimately included 17 RCTs for the study.15–31 Two reviewers (CCC and NZ) independently screened the titles, abstracts, and full texts against the eligibility criteria. A consensus was reached through follow-up discussions.
Data Extraction
We assessed the anti-SI effect of ketamine/esketamine by comparing whether patients in the intervention group experienced greater declines in scores than those in the control group. The 17 included RCTs used the MADRS, MARDS-ITEM-10, QIDS-SR, SSI, MSI, BDI, BSS, BHI, C-SSRS, HDRS, and HAMD-ITEM-24 scale score to assess patient SI. We calculated baseline minus endpoint values for each group of Suicide Scale score in all included RCTs and extracted data as mean ± standard deviation (MD ± SD). When study authors provided MD and SD change values in graphical form, we collected data using GetData software. Meanwhile, when the MD and SD change scores were not provided by the study authors, we calculated the MD and SD of the mean change in depression scores using the following formulas:


The data conversion formulas we used are all from Luo.32 Articles will be excluded if the research does not contain available data or computations.
Risk of Bias Assessment
We assessed risk of bias by using the Cochrane Collaboration’s “risk-of-bias” tool,33 which examines potential selection bias, performance bias, detection bias, attrition bias, reporting bias, and other biases. Two reviewers (CCC and NZ) independently assessed the risk of bias of each included trial, and we consulted a third reviewer (XBW) to resolve any disagreements.
Statistical Analyses
All statistical analyses were performed using R version 4.2.1. Given that the scales used to assess changes in SI varied across studies, we used Cohen’s d as an indicator of effect size to compare all studies based on the same measure to measure changes in SI comparing baseline and endpoint. All studies compared relative efficacy using different drug/dose/duration pooled effect sizes. The combined effect size results are shown in a forest plot. For Cohen’s d score, d < 0.2, 0.2–0.8, d > 0.8 means small, medium, and large effects.
Heterogeneity was quantified using the I2 statistic. For the I2 statistic, 25% = low heterogeneity, 50% = moderate heterogeneity, and 75% = high heterogeneity.34 In this study, we used afixed-effects model for studies with I2<50% and arandom-effects model for studies with I2>50%. When results showed high levels of heterogeneity, sensitivity analyses and meta-regression were used to examine sources of heterogeneity. We plotted funnel plots and assessed their symmetry using Egger’s test for publication bias.35
Results
Search Results
The process of including studies is shown in the PRISMA flowchart (Figure 1). An initial search identified 377 publications. In addition, 5 studies from other sources were identified. After removing 112 duplicate articles, there were 270 remaining articles, of which 152 were excluded because they did not meet the RCT study design, and 32 were excluded because their abstracts did not match their titles. In the end, 29 articles were read and evaluated in their entirety. Seven publications were removed after full-text screening because complete data were not available, and five review articles were removed because full text was not available. We used the remaining 17 articles for further analyses.
 |
Figure 1 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) study selection flow diagram. |
Study Characteristics
The pooled total sample of all RCTs included 1224 participants (n = 615 received racemic ketamine/esketamine, n = 609 received saline or midazolam). Fourteen studies in the ketamine and control groups used DSM-IV/DSM-V diagnosed or previously diagnosed depression, 2 studies used SSI/BSI > 3 as inclusion criteria, and 1 study included cancer patients with depression. In terms of scales, 12 studies administered multiple SI scales (Beck Suicidal Ideation Scale-BSS/I; Suicidal Ideation Scale-SSI; Columbia Suicide Severity Rating Scale-c-SSRS; Beck Despair Scale-BHI), and 7 trials used single items from the Depression Inventory (item 10 on the Montgomery-Åsberg Depression Rating Scale [MADRS]; item 3 on the 17-item Hamilton Depression Rating Scale [HAM-D]; item 12 on the Quick Inventory of Depressive Symptomatology-Self Report [QIDS-SR]; and/or item 9 on the Beck Depression Inventory [BDI]). In terms of administration, 12 studies used intravenous (IV) ketamine, 3 studies used intranasal inhaled (IN) esketamine, 1 study used IN ketamine and 1 study used oral (PO) and intramuscular (IM) ketamine. All 12 studies in the IV ketamine group received 0.5 mg/kg IV ketamine. The IN esketamine group used esketamine 80 mg and 1 study used IN ketamine 40 mg. The remaining 2 studies used 1 mg/kg PO ketamine or 0.5 mg/kg IM. In the control group, 8 studies were given midazolam, 8 studies were given the same volume of normal saline, and 1 study compared by electroconvulsive shock therapy . The general characteristics of the included studies are listed in Table 1.
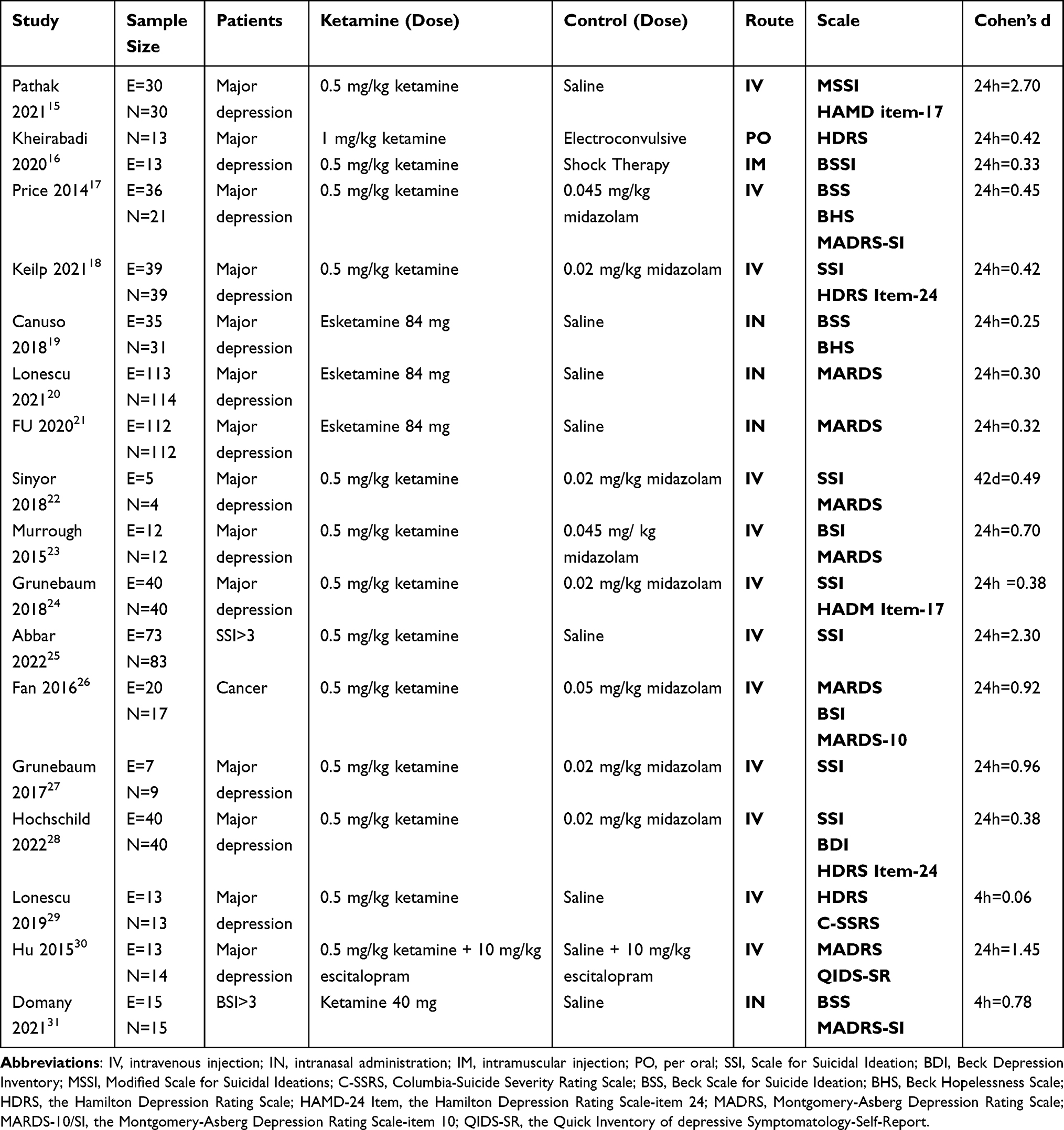 |
Table 1 Summary of Study Characteristics |
Bias Assessment
The results of the Cochrane risk of bias assessment are shown in Figure 2. The overall quality of the studies included in the meta-analysis was classified as moderate to high quality.
 |
Figure 2 No significant high risk of bias assessed by Cochrane bias tool. |
Heterogeneity and Publication Bias
Figure 3 is a forest plot of the total effect size across all studies, with an overall heterogeneity of I2 = 87%, which is highly heterogeneous. Due to the significant heterogeneity across these studies, we performed subgroup analysis, sensitivity analysis, and meta-regression analysis to explore the sources of heterogeneity.
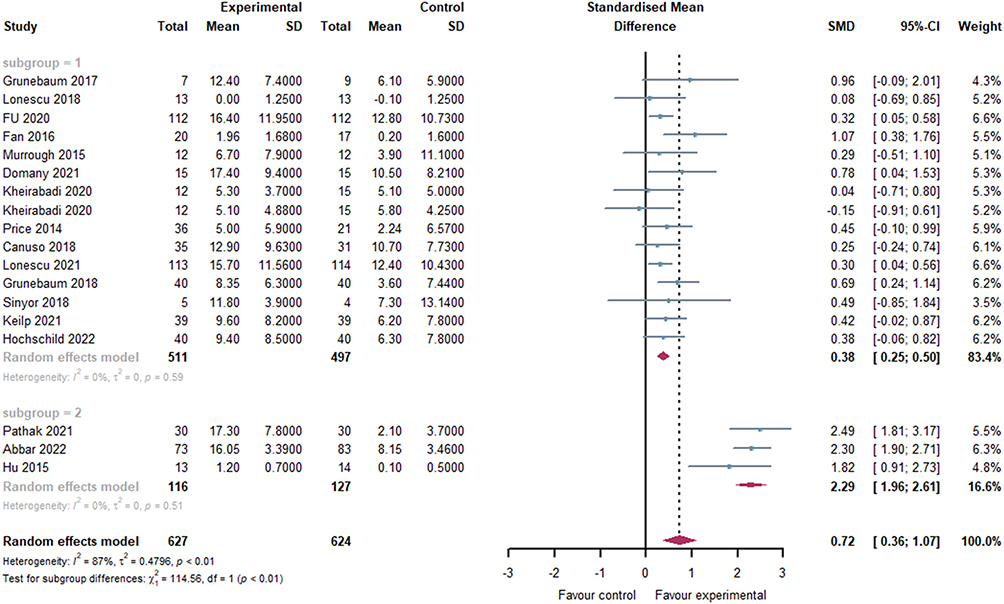 |
Figure 3 All studies were included, grouped by degree of heterogeneity. Cohen’s d changes between ketamine/esketamine-treated and control group. Squares indicate effect sizes for individual arithmetic cases, diamonds indicate effect sizes for combined results. |
We used sensitivity analysis (Figure 4) and meta-regression (Figure 5) with random-effects models to examine sources of heterogeneity. Sensitivity analysis results showed that three studies15,25,30 had a significant effect on the overall effect size. Meta-regression results indicated that there was also significant heterogeneity between studies using the MSSI scale and other studies, so we performed separate subgroup analysis for these 3 studies. Heterogeneity between the remaining 14 studies and this subset of 3 studies was 0% (P>0.05), and it can be assumed that there is no heterogeneity among these studies. Despite strong heterogeneity among some studies, we observed in the sensitivity analysis that excluding these 3 studies alone had no significant effect on the total effect size (Cohen’s dsum = 0.72, 95% CI: 0.36, 1.07). Furthermore, the design and population of these studies did not differ significantly from other studies. Meanwhile, we also plotted funnel plots and used Egger’s test to assess publication bias. The asymmetry of the funnel plot can be observed in Figure 6, and we calculated P = 0.6056 (t = 0.53, df = 18) using Egger’s method, indicating that none of the included RCTs had significant publication bias. For these reasons, instead of excluding these 3 studies, we subsequently performed subgroup analysis to avoid heterogeneity, and we do not discuss heterogeneity in the subsequent forest diagrams.
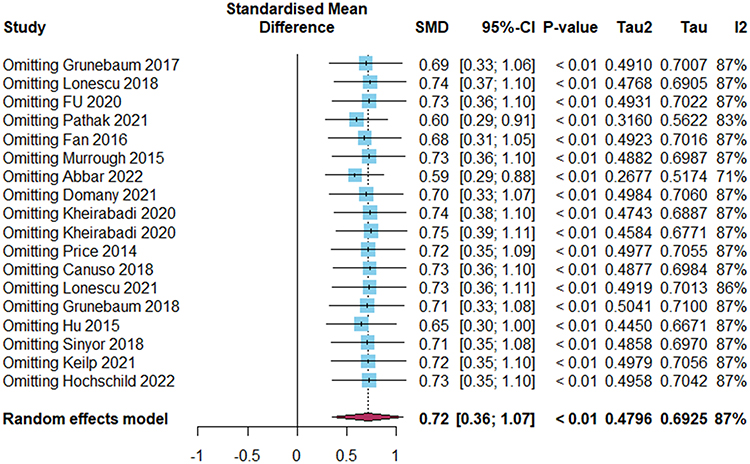 |
Figure 4 Sensitivity analysis revealed that 3 studies (Abbar 2022/ Pathak 2021/HU 2015) had a insignificant effect on the overall effect size. |
 |
Figure 5 Meta-regression identified 3 studies as a source of heterogeneity. |
 |
Figure 6 The standard error of the funnel plot was observed by Cohen’s d. |
In conclusion, various ketamine/esketamine regimens remain moderately effective against the effects of SI. We did not analyze these 3 studies individually in subsequent subgroups (However, sensitivity analyses and meta-regressions were also performed for each subgroup and reached the same conclusions).
Anti-SI Effects of Different Uses of Ketamine
Total Efficacy of Ketamine/Esketamine on Anti-SI
The forest plot (Figure 3) summarizing the anti-SI effect size of ketamine and esketamine for all administration and time points. The primary efficacy endpoint was improvement in SI compared with control groups. We analyzed 3 studies with large heterogeneity between different groups. Results showed that ketamine/esketamine had a medium effect on reducing the suicide scores compared with midazolam or placebo (Cohen’s d = 0.72, 95% CI: 0.36, 1.07). It has been shown to have anti-SI effects.
Effects of Ketamine/Esketamine on Anti-SI at Different Durations
We divided ketamine group into 3 subgroups according to time point (4–6 hours, 24 hours, >24 hours) and esketamine into 2 subgroups (4–6 hours, 24 hours). The time effect of anti-SI ketamine/esketamine was analyzed by comparing the difference in treatment effect at each time point. The forest plot of the ketamine group in Figure 7 showed that ketamine produced a large degree of anti-SI effect in both the 4–6 hours subgroup (Cohen’s d = 1.16, 95% CI: 0.50, 1.81) and a medium-large degree of the 24 hours subgroup (Cohen’s d = 0.95, 95% CI: 0.48; 1.41). In the 24 hours-7 days subgroup (Cohen’s d=2.01, 95% CI: −0.31, 4.33), the relationship between ketamine and SI was not statistically significant. Figure 8 demonstrate the effect sizes of esketamine at 4-6 hours (Cohen’s d = 0.26, 95% CI: 0.09, 0.44) and 24 hours (Cohen’s d = 0.30, 95% CI: 0.13, 0.47).
 |
Figure 7 Forest plot showing all ketamine studies grouped by timepoint. Cohen’s d changes between ketamine-treated and control group. Squares indicate effect sizes for individual arithmetic cases, diamonds indicate effect sizes for combined results. |
 |
Figure 8 Forest plot showing all esketamine studies grouped by time. Cohen’s d changes between esketamine-treated and control group. Squares indicate effect sizes for individual arithmetic cases, diamonds indicate effect sizes for combined results. |
Differences in Anti-SI Effect Between Ketamine and Esketamine
We performed subgroup analysis according to different methods of administration (0.5 mg/kg IV ketamine or IN esketamine 80 mg/40 mg) with a duration of action of 4hours/24hours. Two studies on intramuscular/oral ketamine were not included because the number of similar studies was too small. Figure 9 summarizes the effect sizes. The effect size for all responses for all methods used was Cohen’s d = 0.81 (95% CI, 0.41, 1.21). The effect size was large for IV ketamine 4 hours/24 hours (Cohen’s d = 0.96, 95% CI: 0.48, 1. 44) and medium-small for IN esketamine (Cohen’s d = 0.30, 95% CI: 0.13, 0.47).
 |
Figure 9 Includes forest plots for all studies, grouped by drug. |
Discussion
According to the results of the meta-analysis, the sub-anesthetic dose of ketamine infusion can significantly reduce SI in patients compared with midazolam/saline. The effects first appeared within 4 hours of administration and lasted for 24 hours, providing evidence of the rapid effects of ketamine on mood. However, ketamine had no statistically significant effect after 24 hours, suggesting that the effect may be transient, and other authors have reported similar results.36–38 But there are also studies showing that ketamine can rapidly reduce SI in depressed patients within 1 day and 1 week.39,40 The antidepressant effect of ketamine was reported to start after 2 hours and last for 1 week. Combined with results from other meta-analysis, the anti-SI and antidepressant effects of ketamine and esketamine appear to be synchronous.41 This is because when SI decreased, depression scores also decreased. However, the mechanisms underlying ketamine’s anti-SI and antidepressant effects are unclear, and there is no evidence that ketamine’s anti-SI effects depend on its antidepressant effects. Whether ketamine’s effects on SI are partially independent of its effects on mood remains to be determined. Therefore, whether ketamine has long-term anti-SI effects after 24 hours requires further study.
We included 4 studies of IN esketamine in addition to IV ketamine. Back in 2019, the FDA approved IN esketamine to treat patients with depression, with a statement that it could be used in severely depressed patients with significant SI. Esketamine also has some anti-SI effects. However, esketamine is not independently approved as an anti-SI drug. There have been few studies using esketamine alone to reduce SI, so its use/dose, onset/maintenance duration, and effectiveness compared with IV ketamine are unclear. According to our limited data, IN esketamine 40/84 mg showed a small-to-medium effect on SI within 24 hours (Cohen’s d = 0.30, 95% CI: 0.13, 0.47). The use and dosage of esketamine in 4 studies were consistent with guideline recommendations, and despite some limitations, we can still conclude that 40/84 mg esketamine administered within 24 hours has some anti-SI effect. However, it is important to emphasize that although the effect size of sub-anesthetic doses of IV ketamine was greater than that of IN esketamine, we cannot conclude that sub-anesthetic doses of IV ketamine over 24 hours were superior to IN esketamine because of the lack of RCTs directly comparing the effectiveness of them.
Combining studies of forest plots, we identified large heterogeneity (I2 = 87%). To explore the sources of heterogeneity, we applied sensitivity analysis and meta-regression and identified several study design features that explained the significant heterogeneity within and between studies. Double blinding is one of the basic principles of RCTs, and the Pathak 2021 study only treated single-blind patients, so poor study design may be a source of heterogeneity. The Abbar 2022 study had a large effect on the overall effect size, but we cannot simply treat it as a source of heterogeneity. This is because this was a large, multicentre study involving seven French academic hospitals. The inclusion criteria for the study were very strict, and all patients were admitted with SI. In contrast, most other studies included patients with MDD or abnormal suicide scores, which could explain their heterogeneity. However, the rigorous research design and large sample size of this study may better reflect the anti-suicide effect of ketamine. In contrast to other experimental studies, HU included IV escitalopram 10mg daily and escitalopram 10mg daily + IV ketamine 0.5 mg/kg as inclusion criteria for MDD patients and controls.30 Because escitalopram has antidepressant effect, it acts synergistically with ketamine to enhance efficacy. This could explain the heterogeneity of the studies. In conclusion, although the three studies produced a greater impact on the total effect size. But these studies had a relatively complete study design and meet the inclusion criteria, ultimately, we approached these studies by only going to subgroup analysis.
Although ketamine infusion is generally safe for MDD, some safety concerns such as arterial hypertension, dissociation, and simulated mental activity can be observed in studies.42 This has raised concerns about the safety of ketamine in treating depressed patients with these psychiatric and somatic comorbidities. Szarmach conducted an observational study of IV ketamine in TRD patients with mild cardiovascular disease, epilepsy, metabolic derangements, and other somatic comorbidities. An observational study of IV ketamine in TRD with comorbidities such as epilepsy and metabolic disorders has shown increased HR and RR during treatment but no worsening of the cardiovascular, metabolic, or epilepsy-related disease.43 The side effects were mild or moderate, well tolerated, and transient and all side effects disappeared within 4 hours after administration. Similar conclusions were also drawn from the study by Short.44 Psychotic depression is a subtype of MDD characterized by mood-related hallucinations or delusions. The lifetime prevalence of MDD with psychotic features ranges from 0.35% to 1% in the general population.45 Although treatments are approved for MDD associated with psychiatric disorders, some TRD patients do not respond to recommended therapeutic interventions.46 Wegielnik included patients with MDD and psychiatric illness or bipolar disorder and found that ketamine had good safety and efficacy for TRD patients with major depressive disorder and psychiatric comorbidity.11 TRD with psychotic comorbidities was safe and well tolerated, consistent with previous results.47 Based on the above studies, the safety of using ketamine for depression in specific populations also seems reasonable. This group of patients may benefit more from ketamine than conventional drugs, but large clinical trials are still needed to confirm this.
In addition to ketamine, traditional antidepressants also show some anti-SI effects.48 Although the mechanism of anti-SI of traditional antidepressants has not been confirmed, the combined use of ketamine/esketamine may produce synergistic effects through different mechanisms of action, resulting in superior clinical efficacy. As noted above, the combination of escitalopram with ketamine resulted in a larger effect size for this study, suggesting that the combination of old and new drugs exerted a stronger anti-SI effect. This also provides a basis for combining ketamine with other drugs. We believe that it is difficult to treat suicidal behavior or SI with one drug alone. However, the combination of drugs can both enhance the treatment effect and reduce the dose of individual drugs, thereby reducing the side effects of the drugs, perhaps also accelerating the onset of action or prolonging the maintenance of ketamine and esketamine. Therefore, we hope that more studies on ketamine/esketamine combined with other anti-suicide drugs will be conducted in the future to further reduce the global suicide rate and ease the social burden.
In summary, current research on anti-SI still has many deficiencies. Our results demonstrate the therapeutic potential of ketamine and esketamine on SI and provide evidence-based medical evidence for the treatment of anti-SI.
Limitations and Future Directions
Our meta-analysis has some limitations. First, the number of included RCTs was insufficient to allow us to draw strong conclusions about differences in efficacy of different doses/durations, especially for esketamine. In addition, two studies of esketamine were ASPIRE I and ASPIRE II studies, and the other study was conducted by the same team, which may increase the risk of publication bias. Second, there is a lack of RCTs of ketamine versus esketamine, making it difficult to directly compare the efficacy and safety of ketamine versus esketamine. Third, the inclusion criteria of existing studies were all based on MDD. Due to the homogeneity of the inclusion criteria, we could not ascertain from the included studies the anti-SI effect and safety of ketamine/esketamine in patients with other somatic comorbidities/psychiatric comorbidities (bipolar disorder/compulsive-compulsive disorder). Equally, the inclusion criteria for RCTs in this article did not specify gender/age for screening. Therefore, more RCTs are needed to investigate how the antidepressant effects and anti-SI of ketamine or esketamine differ in these populations. Fourth, the current tools for measuring the level of SI are scales such as SSI/BSI/BHI. Due to scale inconsistency, multiple scales could be used to address SI across multiple RCT outcomes. The scoring standards/total scores of different scales are different, the comparison between samples is difficult, and the heterogeneity between groups increases. Although the short-term effects of ketamine and esketamine on SI were assessed in the included RCTs, long-term use of these drugs predisposes to certain medical conditions (mental disorders, cystitis). Therefore, finding potent metabolites or important antidepressant targets of ketamine or esketamine or the mechanism of their antidepressant/anti-SI effects is of great significance for the development of safer drugs in the future.
Conclusion
In conclusion, our meta-analysis supports that intravenous sub-anesthetic doses of ketamine and intranasal inhaled esketamine have the effect on anti-SI within 4 hours and last for 24 hours. These results suggest that ketamine/esketamine holds promise as a potential fast-acting therapy for patients at risk of suicide. However, the side effects limit its clinical application. It is urgent to further study the anti-SI/depression mechanism of ketamine/esketamine, minimize its side effects, and provide new options for acute anti-SI clinical application.
Funding
This work was supported by the Department of Science & Technology of Sichuan Province (Grant No. 2020YJ0493, 2022YFS0632), and the scientific research project of the Luzhou municipal government–Southwest Medical University (2021LZXNYD-Z06).
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. World Health Statistics 2022: Monitoring Health for the Sdgs, Sustainable Development Goals. Geneva: World Health Organization; 2022.
2. World Health Organization. Preventing suicide: a global imperative. World Health Organization; 2014. Available from: http://www.who.int/iris/handle/10665/131056.
3. Beck AT, Brown G, Berchick RJ, Stewart BL, Steer RA. Relationship between hopelessness and ultimate suicide: a replication with psychiatric outpatients. Am J Psychiatry. 1990;147(2):190–195. doi:10.1176/ajp.147.2.190
4. Miller JN, Black DW. Bipolar disorder and suicide: a review. Curr Psychiatry Rep. 2020;22(2):6. doi:10.1007/s11920-020-1130-0
5. Serafini G, Costanza A, Aguglia A, et al. Overall goal of cognitive-behavioral therapy in major psychiatric disorders and suicidality: a narrative review. Med Clin North Am. 2023;107(1):143–167. doi:10.1016/j.mcna.2022.05.006
6. Klonsky ED, May AM, Saffer BY. Suicide, suicide attempts, and suicidal ideation. Annu Rev Clin Psychol. 2016;12:307–330. doi:10.1146/annurev-clinpsy-021815-093204
7. Malhi GS, Bassett D, Boyce P, et al. Royal Australian and New Zealand College of psychiatrists clinical practice guidelines for mood disorders. Aust NZ J Psychiatry. 2015;49(12):1087–1206. doi:10.1177/0004867415617657
8. Zanos P, Moaddel R, Morris PJ, et al. NMDAR inhibition-independent antidepressant actions of ketamine metabolites. Nature. 2016;533(7604):481–486. doi:10.1038/nature17998
9. Bahji A, Vazquez GH, Zarate CJ. Comparative efficacy of racemic ketamine and esketamine for depression: a systematic review and meta-analysis. J Affect Disord. 2021;278:542–555. doi:10.1016/j.jad.2020.09.071
10. Ohnishi T, Wakamatsu A, Kobayashi H. Different symptomatic improvement pattern revealed by factor analysis between placebo response and response to Esketamine in treatment resistant depression. Psychiatry Clin Neurosci. 2022;76(8):377–383. doi:10.1111/pcn.13379
11. Gałuszko-Węgielnik M, Chmielewska Z, Jakuszkowiak-Wojten K, Wiglusz MS, Cubała WJ. Ketamine as add-on treatment in psychotic treatment-resistant depression. Brain Sci. 2023;13(1):142. doi:10.3390/brainsci13010142
12. Serafini G, Howland RH, Rovedi F, Girardi P, Amore M. The role of ketamine in treatment-resistant depression: a systematic review. Curr Neuropharmacol. 2014;12(5):444–461. doi:10.2174/1570159X12666140619204251
13. Ortiz V, Costa CR, Fofo H, Fernandez SP, Barik J. Nicotinic receptors promote susceptibility to social stress in female mice linked with neuroadaptations within VTA dopamine neurons. Neuropsychopharmacol. 2022;47(9):1587–1596. doi:10.1038/s41386-022-01314-4
14. Fedgchin M, Trivedi M, Daly EJ, et al. Efficacy and safety of fixed-dose esketamine nasal spray combined with a new oral antidepressant in treatment-resistant depression: results of a randomized, double-blind, active-controlled study (TRANSFORM-1). Int J Neuropsychopharmacol. 2019;22(10):616–630. doi:10.1093/ijnp/pyz039
15. Pathak U, Ahuja S, Dwivedi R, et al. Antisuicidal efficacy of ketamine infusion in suicidal patients of depressive disorder. Indian J Psychiat. 2021;63(5):483. doi:10.4103/indianjpsychiatry.indianjpsychiatry_80_21
16. Kheirabadi D, Kheirabadi GR, Mirlohi Z, Tarrahi MJ, Norbaksh A. Comparison of rapid antidepressant and antisuicidal effects of intramuscular ketamine, oral ketamine, and electroconvulsive therapy in patients with major depressive disorder. J Clin Psychopharm. 2020;40(6):588–593. doi:10.1097/JCP.0000000000001289
17. Price RB, Iosifescu DV, Murrough JW, et al. Effects of ketamine on explicit and implicit suicidal cognition: a randomized controlled trial in treatment-resistant depression. Depress Anxiety. 2014;31(4):335–343. doi:10.1002/da.22253
18. Keilp JG, Madden SP, Marver JE, et al. Effects of ketamine versus midazolam on neurocognition at 24 hours in depressed patients with suicidal ideation. J Clin Psychiatry. 2021;82:6. doi:10.4088/JCP.21m13921
19. Canuso CM, Singh JB, Fedgchin M, et al. Efficacy and safety of intranasal esketamine for the rapid reduction of symptoms of depression and suicidality in patients at imminent risk for suicide: results of a double-blind, randomized, placebo-controlled study. Am J Psychiatry. 2018;175(7):620. doi:10.1176/appi.ajp.2018.17060720
20. Ionescu DF, Fu D, Qiu X, et al. Esketamine nasal spray for rapid reduction of depressive symptoms in patients with major depressive disorder who have active suicide ideation with intent: results of a phase 3, double-blind, randomized study (ASPIRE II). Int J Neuropsychoph. 2021;24(1):22–31. doi:10.1093/ijnp/pyaa068
21. Fu DJ, Ionescu DF, Li X, et al. Esketamine nasal spray for rapid reduction of major depressive disorder symptoms in patients who have active suicidal ideation with intent: double-blind, randomized study (ASPIRE I). J Clin Psychiatry. 2020;81:3. doi:10.4088/JCP.19m13191
22. Sinyor M, Williams M, Belo S, et al. Ketamine augmentation for major depressive disorder and suicidal ideation: preliminary experience in an inpatient psychiatry setting. J Affect Disord. 2018;241:103–109. doi:10.1016/j.jad.2018.07.073
23. Murrough JW, Soleimani L, Dewilde KE, et al. Ketamine for rapid reduction of suicidal ideation: a randomized controlled trial. Psychol Med. 2015;45(16):3571–3580. doi:10.1017/S0033291715001506
24. Grunebaum MF, Galfalvy HC, Choo TH, et al. Ketamine for rapid reduction of suicidal thoughts in major depression: a midazolam-controlled randomized clinical trial. Am J Psychiatry. 2018;175(4):327–335. doi:10.1176/appi.ajp.2017.17060647
25. Abbar M, Demattei C, El-Hage W, et al. Ketamine for the acute treatment of severe suicidal ideation: double blind, randomised placebo controlled trial. BMJ. 2022:e067194. doi:10.1136/bmj-2021-067194
26. Fan W, Yang H, Sun Y, et al. Ketamine rapidly relieves acute suicidal ideation in cancer patients: a randomized controlled clinical trial. Oncotarget. 2017;8(2):2356–2360. doi:10.18632/oncotarget.13743
27. Grunebaum MF, Ellis SP, Keilp JG, et al. Ketamine versus midazolam in bipolar depression with suicidal thoughts: a pilot midazolam-controlled randomized clinical trial. Bipolar Disord. 2017;19(3):176–183. doi:10.1111/bdi.12487
28. Hochschild A, Keilp JG, Madden SP, Burke AK, Mann JJ, Grunebaum MF. Ketamine vs midazolam: mood improvement reduces suicidal ideation in depression. J Affect Disorders. 2022;300:10–16. doi:10.1016/j.jad.2021.12.055
29. Ionescu DF, Bentley KH, Eikermann M, et al. Repeat-dose ketamine augmentation for treatment-resistant depression with chronic suicidal ideation: a randomized, double blind, placebo controlled trial. J Affect Disord. 2019;243:516–524. doi:10.1016/j.jad.2018.09.037
30. Hu YD, Xiang YT, Fang JX, et al. Single i.v. ketamine augmentation of newly initiated escitalopram for major depression: results from a randomized, placebo-controlled 4-week study. Psychol Med. 2016;46(3):623–635. doi:10.1017/S0033291715002159
31. Domany Y, Mccullumsmith CB. Single, fixed-dose intranasal ketamine for alleviation of acute suicidal ideation. an emergency department, trans-diagnostic approach: a randomized, double-blind, placebo-controlled, proof-of-concept trial. Arch Suicide Res. 2022;26(3):1250–1265. doi:10.1080/13811118.2021.1878078
32. Luo D, Wan X, Liu J, Tong T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res. 2018;27(6):1785–1805. doi:10.1177/0962280216669183
33. Higgins JP, Altman DG, Gøtzsche PC, et al. The Cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi:10.1136/bmj.d5928
34. Cochrane handbook: general methods for Cochrane reviews; 2023. Available from: https://handbook-5-1.cochrane.org/chapter_9/9_5_heterogeneity.html.
35. Sterne J, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi:10.1136/bmj.l4898
36. Abdallah CG, Roache JD, Gueorguieva R, et al. Dose-related effects of ketamine for antidepressant-resistant symptoms of posttraumatic stress disorder in veterans and active duty military: a double-blind, randomized, placebo-controlled multi-center clinical trial. Neuropsychopharmacol. 2022;47(8):1574–1581. doi:10.1038/s41386-022-01266-9
37. Xiong J, Lipsitz O, Chen-Li D, et al. The acute antisuicidal effects of single-dose intravenous ketamine and intranasal esketamine in individuals with major depression and bipolar disorders: a systematic review and meta-analysis. J Psychiatr Res. 2021;134:57–68. doi:10.1016/j.jpsychires.2020.12.038
38. Averill LA, Averill CL, Gueorguieva R, et al. mTORC1 inhibitor effects on rapid ketamine-induced reductions in suicidal ideation in patients with treatment-resistant depression. J Affect Disord. 2022;303:91–97. doi:10.1016/j.jad.2022.01.104
39. Wilkinson ST, Ballard ED, Bloch MH, et al. The effect of a single dose of intravenous ketamine on suicidal ideation: a systematic review and individual participant data meta-analysis. Am J Psychiatry. 2018;175(2):150–158. doi:10.1176/appi.ajp.2017.17040472
40. Witt K, Potts J, Hubers A, et al. Ketamine for suicidal ideation in adults with psychiatric disorders: a systematic review and meta-analysis of treatment trials. Aust NZ J Psychiatry. 2020;54(1):29–45. doi:10.1177/0004867419883341
41. Marcantoni WS, Akoumba BS, Wassef M, et al. A systematic review and meta-analysis of the efficacy of intravenous ketamine infusion for treatment resistant depression: January 2009 - January 2019. J Affect Disord. 2020;277:831–841. doi:10.1016/j.jad.2020.09.007
42. Daly EJ, Trivedi MH, Janik A, et al. Efficacy of esketamine nasal spray plus oral antidepressant treatment for relapse prevention in patients with treatment-resistant depression: a randomized clinical trial. JAMA Psychiat. 2019;76(9):893–903. doi:10.1001/jamapsychiatry.2019.1189
43. Szarmach J, Cubała WJ, Włodarczyk A, Gałuszko-Węgielnik M. Somatic comorbidities and cardiovascular safety in ketamine use for treatment-resistant depression. Medicina. 2021;57:3. doi:10.3390/medicina57030274
44. Short B, Fong J, Galvez V, Shelker W, Loo CK. Side-effects associated with ketamine use in depression: a systematic review. Lancet Psychiat. 2018;5(1):65–78. doi:10.1016/S2215-0366(17)30272-9
45. Jääskeläinen E, Juola T, Korpela H, et al. Epidemiology of psychotic depression - systematic review and meta-analysis. Psychol Med. 2018;48(6):905–918. doi:10.1017/S0033291717002501
46. Rothschild AJ. Challenges in the treatment of major depressive disorder with psychotic features. Schizophr Bull. 2013;39(4):787–796. doi:10.1093/schbul/sbt046
47. Souza-Marques B, Telles M, Leal GC, et al. Esketamine for unipolar major depression with psychotic features: a retrospective chart review and comparison with nonpsychotic depression. J Clin Psychopharmacol. 2022;42(4):408–412. doi:10.1097/JCP.0000000000001571
48. Yang P, Yang M, Li P, et al. A meta-analysis of 5-hydroxytryptamine receptor 1B polymorphisms with risk of major depressive disorder and suicidal behavior. Front Psychiatry. 2021;12:696655. doi:10.3389/fpsyt.2021.696655
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.