Back to Journals » Journal of Pain Research » Volume 18
Acupuncture Therapy for Extremity Musculoskeletal Pain: A Clinically Focused Evidence Synthesis with Therapeutic Implications
Authors Zhu F ![]() , Chen Y, Zhu Y
, Chen Y, Zhu Y ![]() , Bai Z
, Bai Z ![]() , Yan H
, Yan H
Received 3 July 2025
Accepted for publication 17 October 2025
Published 24 October 2025 Volume 2025:18 Pages 5541—5554
DOI https://doi.org/10.2147/JPR.S551446
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Houman Danesh
Fenglin Zhu, Yetong Chen, Yang Zhu, Zhenmin Bai, Huipin Yan
School of Sports Medicine and Rehabilitation, Beijing Sport University, Beijing, People’s Republic of China
Correspondence: Zhenmin Bai, School of Sports Medicine and Rehabilitation, Beijing Sport University, Beijing, People’s Republic of China, Email [email protected] Huipin Yan, School of Sports Medicine and Rehabilitation, Beijing Sport University, Beijing, People’s Republic of China, Email [email protected]
Background: Extremity musculoskeletal pain (EMP) is a major contributor to chronic pain and disability worldwide, often involving tendinopathies, enthesopathies, and myofascial pain syndromes. Conventional treatments such as medications, injections, and physical therapy frequently provide only partial or short-term relief. Acupuncture, widely practiced in clinical settings, has been proposed as a safe and effective alternative or adjunctive therapy.
Methods: A comprehensive search of PubMed, Embase, and the Cochrane Library identified studies published from January 2015 to June 2024. Eligible publications included randomized controlled trials (RCTs), systematic reviews, or meta-analyses involving adults with EMP and reporting pain or function as primary outcomes. Nineteen studies (10 RCTs, 9 reviews) met the inclusion criteria and were narratively synthesized.
Results: For lateral epicondylitis (LE), manual acupuncture provided short-term benefit, while dry needling demonstrated superior long-term effects. Evidence for carpal tunnel syndrome (CTS) was insufficient, with mixed findings and high risk of bias. In patellofemoral pain syndrome (PFPS), trigger point dry needling showed short-to-medium term pain relief, though its added value in multimodal therapy was inconsistent. For plantar heel pain syndrome (PHPS), both electroacupuncture and dry needling produced significant improvements in pain and function, with benefits sustained beyond three months.
Conclusion: Acupuncture appears to be a safe, low-risk therapy for EMP, with strongest evidence for PHPS and LE, limited support for PFPS, and insufficient evidence for CTS. Clinically, acupuncture should be considered as part of comprehensive multimodal strategies, tailored to patient needs and preferences. Future research should focus on large-scale, standardized RCTs, direct comparisons between acupuncture modalities, and inclusion of regional and non-English studies to strengthen the global evidence base.
Keywords: extremity musculoskeletal pain, plantar heel pain syndrome, lateral epicondylitis, patellofemoral pain syndrome, carpal tunnel syndrome, acupuncture therapy
Introduction
Extremity musculoskeletal pain (EMP) of the extremities is one of the most common causes of chronic pain and disability worldwide. It substantially reduces quality of life, impairs physical function, and generates significant socioeconomic burdens on healthcare systems.1,2 Unlike axial conditions such as low back or neck pain, EMP refers to pain originating from the muscles, tendons, entheses, joints, or related soft tissues of the upper and lower limbs. Typical examples include tendinopathies (eg, lateral epicondylitis [LE], plantar heel pain syndrome [PHPS]), enthesopathies, and myofascial pain syndromes, which pose unique diagnostic and therapeutic challenges.3
Conventional management strategies include pharmacological interventions (eg, nonsteroidal anti-inflammatory drugs [NSAIDs], acetaminophen, and corticosteroid injections) and non-pharmacological approaches such as physical therapy, exercise-based rehabilitation, manual therapy, and ultrasound therapy. While these treatments can provide short-term relief, their long-term effectiveness is often limited, and adverse effects are common. For example, NSAIDs are associated with gastrointestinal and cardiovascular risks,4 while corticosteroid injections may accelerate tissue degeneration with repeated use.5 Similarly, physical therapy interventions, though widely employed, show variable efficacy and high recurrence rates, particularly in conditions like patellofemoral pain syndrome (PFPS).6 These limitations highlight the need for alternative or adjunctive therapies.
Acupuncture, originating in traditional Chinese medicine, has emerged as a promising non-pharmacological therapy for musculoskeletal disorders. It is widely practiced worldwide and increasingly incorporated into mainstream clinical care.7 Proposed mechanisms include modulation of central pain pathways, anti-inflammatory effects, and improvements in local blood circulation, alongside direct effects on myofascial trigger points.8–11 Accumulating evidence from clinical studies suggests that acupuncture may provide meaningful pain relief and functional improvement in EMP.12,13
Several systematic reviews have previously examined acupuncture for musculoskeletal pain of the extremities,12 such as LE,14 carpal tunnel syndrome (CTS),15 patellofemoral pain syndrome (PFPS),16 and PHPS,17 but many are now outdated or limited in scope. Earlier reviews often did not distinguish between different acupuncture modalities (manual acupuncture, electroacupuncture, and dry needling), and few provided condition-specific recommendations for extremity pain. This underscores the need for an updated synthesis of the evidence.
Therefore, this review synthesizes randomized controlled trials and systematic reviews published between 2015 and 2024 to evaluate the clinical efficacy of acupuncture for EMP. By analyzing condition-specific outcomes and integrating practical considerations, we aim to provide clinicians with updated, evidence-informed guidance for tailoring acupuncture as part of comprehensive pain management strategies.
Literature Search
To update the current clinical evidence regarding the effects of acupuncture on musculoskeletal pain of the extremities, we performed a comprehensive search of PubMed, Embase, and Cochrane Library for studies published between January 2015 and June 2024. The search terms included “acupuncture”, “electroacupuncture”, “manual acupuncture”, “dry needling”, “lateral epicondylitis”, “carpal tunnel syndrome”, “patellofemoral pain”, “plantar heel pain syndrome”, “plantar fasciitis”, and “musculoskeletal pain”. Only English-language publications were considered.
Inclusion Criteria
Studies were included if they met all of the following requirements:
- Randomized controlled trials (RCTs), systematic reviews, or meta-analyses;
- Adult participants (≥18 years) with a clinical diagnosis of one of the following extremity musculoskeletal pain conditions: LE, CTS, PFPS, PHPS, or PF;
- Sample size ≥25 participants per trial arm;
- At least one control group (eg, sham acupuncture, waiting list, active therapy, or routine care);
- Reported pain intensity or functional outcomes as a primary endpoint;
- Adequate description of acupuncture intervention, with reporting aligned with STRICTA recommendations (eg, modality, point selection, treatment frequency, duration).
Exclusion Criteria
Studies were excluded if they met any of the following:
- Non-English publications;
- Case reports, conference abstracts, editorials, or narrative commentaries;
- Studies focusing on laser acupuncture or moxibustion;
- Studies without clinical outcome data related to pain or function;
- Pediatric or adolescent populations (<18 years);
- Studies not involving the target conditions of this review, ie, LE, CTS, PFPS, PHPS, or PF.
A total of 496 records were initially identified. After title and abstract screening, studies that did not meet the inclusion criteria were excluded, including those irrelevant to extremity musculoskeletal pain, studies with designs other than randomized controlled trials, systematic reviews, or meta-analyses, pediatric populations, non-English publications, or interventions involving laser acupuncture or moxibustion. Potentially eligible articles underwent full-text review, resulting in 19 studies that met all predefined inclusion and exclusion criteria for final synthesis.
Results
A systematic screening process identified ten randomized controlled trials18–27 and nine review articles28–36 that fulfilled the predefined inclusion criteria. These included patients who were diagnosed with lateral epicondylitis, carpal tunnel syndrome, patellofemoral pain knee, and plantar heel pain syndrome/plantar fasciitis conditions. Tables 1–4 summarizes the key characteristics of the included studies, encompassing study design, sample size, intervention protocols, assessment timepoints, outcome measures, and primary findings.
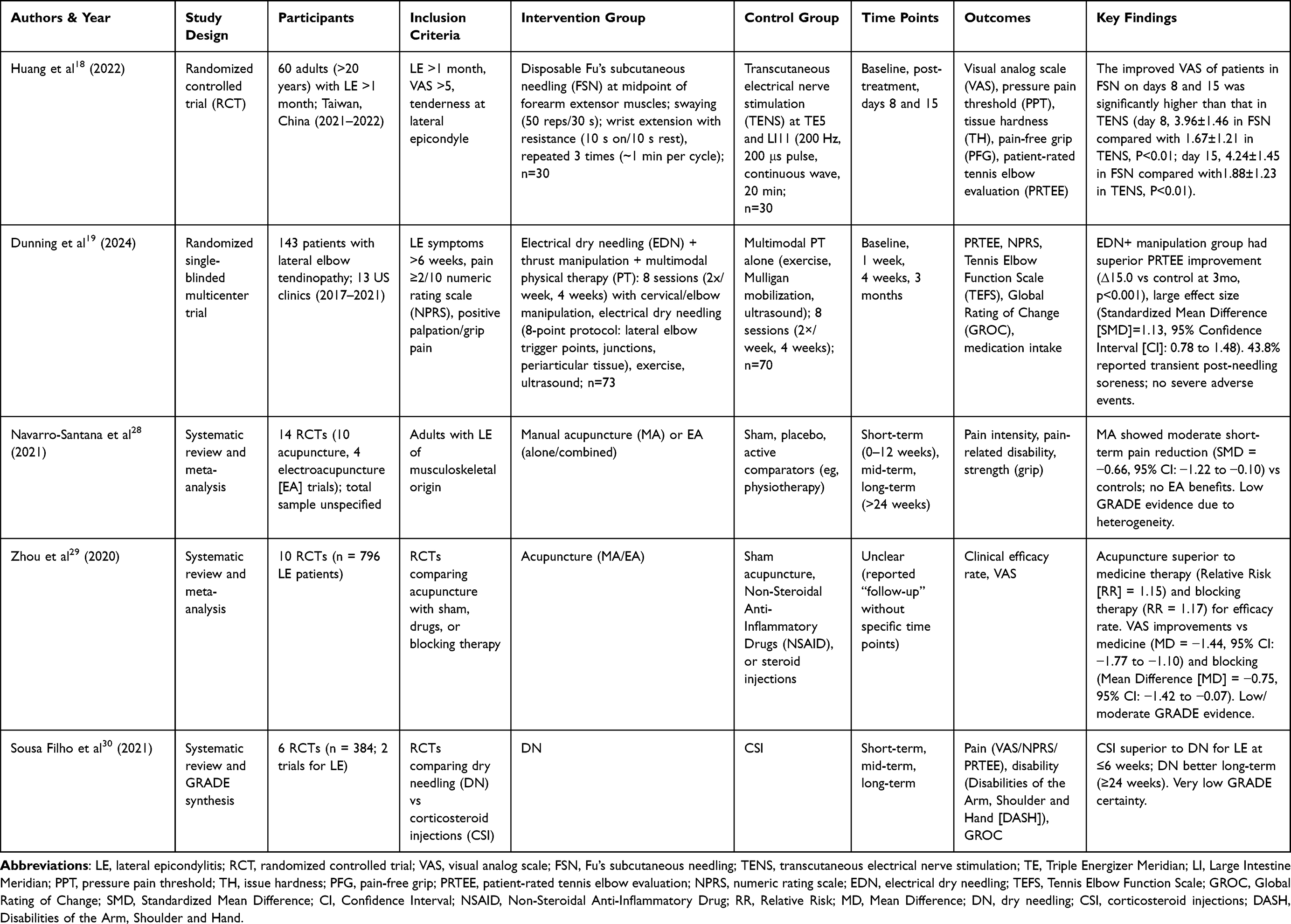 |
Table 1 Evidence Table on Acupuncture Therapy for Lateral Epicondylitis (LE) |
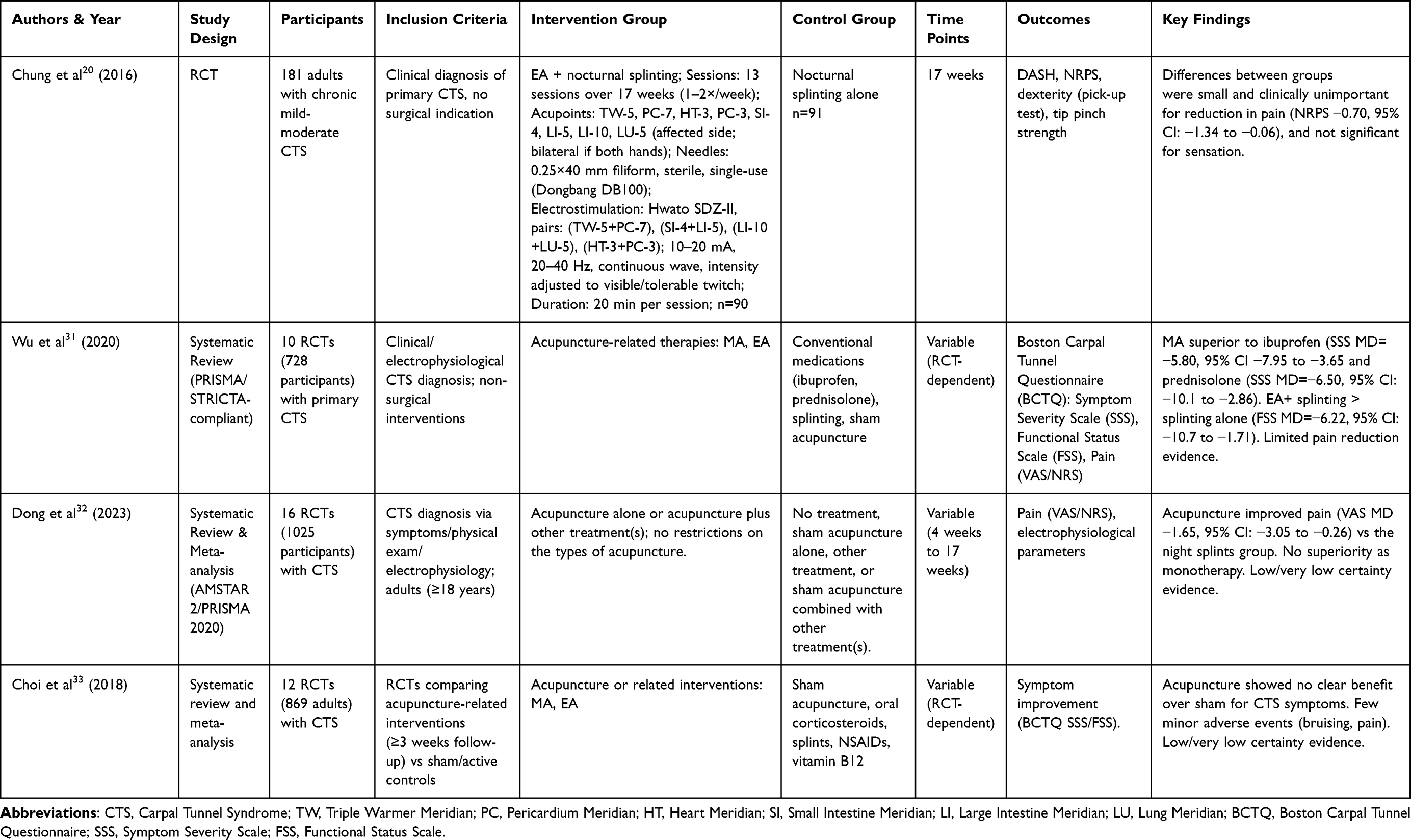 |
Table 2 Evidence Table on Acupuncture Therapy for Carpal Tunnel Syndrome (CTS) |
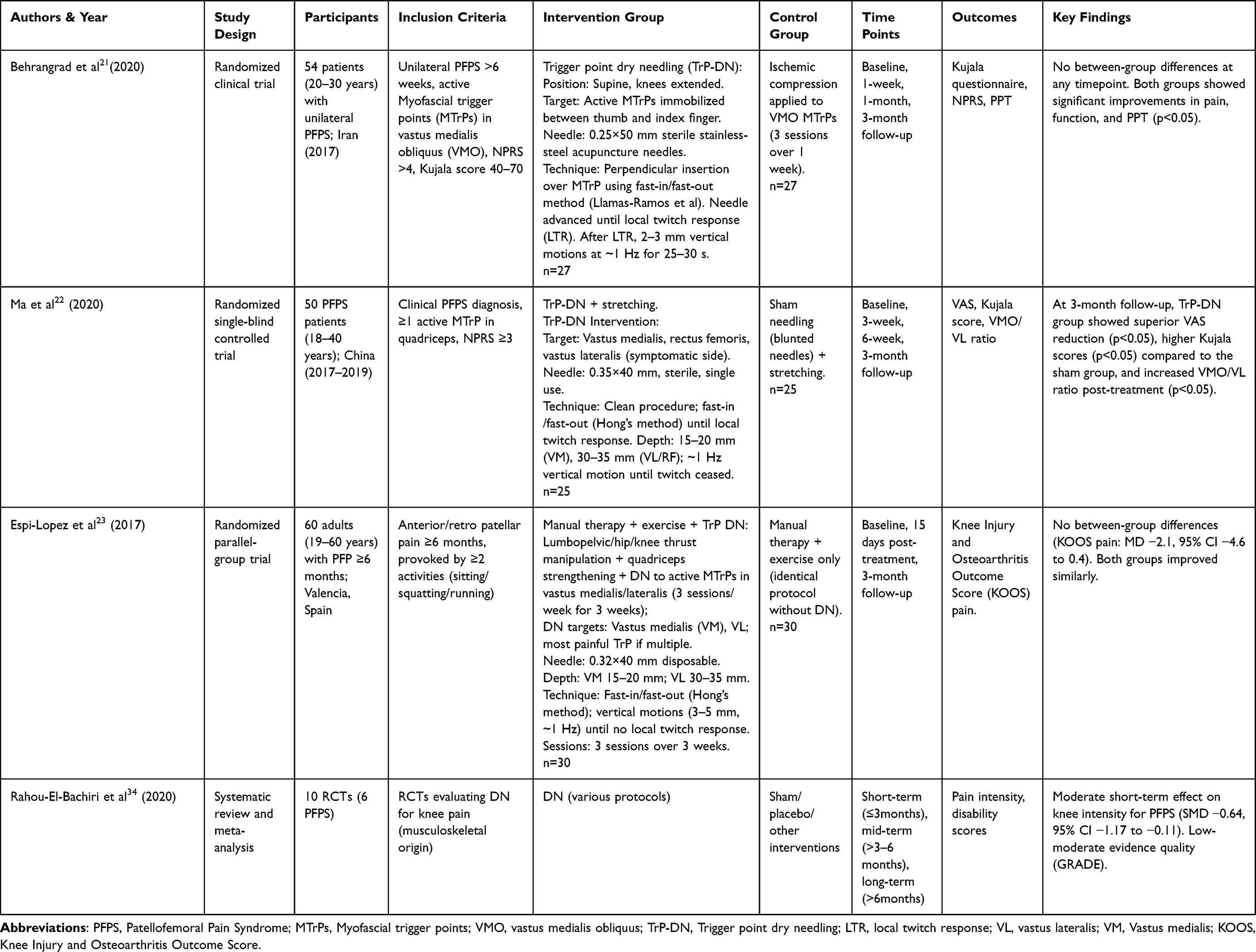 |
Table 3 Evidence Table on Acupuncture Therapy for Patellofemoral Pain Syndrome (PFPS) |
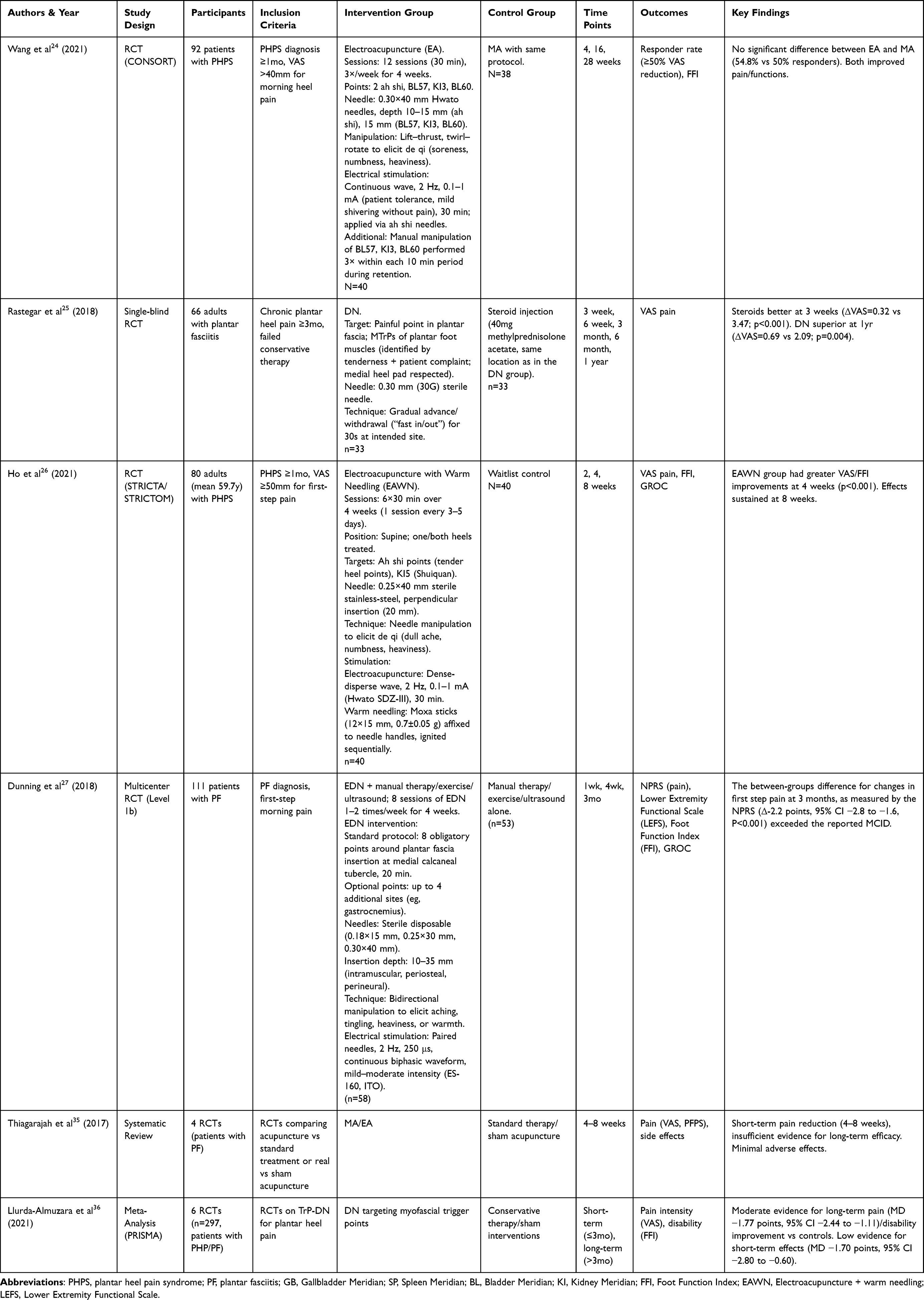 |
Table 4 Evidence Table on Acupuncture Therapy for Plantar Heel Pain Syndrome (PHPS)/Plantar Fasciitis (PF) |
Acupuncture for Lateral Epicondylitis (LE)
Two randomized controlled trials evaluated acupuncture’s efficacy for LE. A randomized controlled trial demonstrated that Fu’s subcutaneous needling (FSN) was more effective than transcutaneous electrical nerve stimulation (TENS) for LE in the short term.18 Evidence from a multicenter randomized clinical trial revealed that integrating electrical dry needling and thrust manipulation into a multimodal physical therapy regimen exhibited greater reductions in pain intensity and functional limitations in patients with lateral elbow tendinopathy compared to multimodal therapy alone at 3-month follow-up.19 The results underscore the therapeutic value of adjunctive acupuncture therapy in optimizing multimodal management for LE.
Three systematic reviews assessed the effectiveness of acupuncture for LE. Navarro-Santana et al28 reported moderate short-term pain reduction for manual acupuncture (MA), but not for electroacupuncture (EA). Another meta-analysis (10 RCTs, n=796) concluded acupuncture was superior to medicine therapy and blocking therapy in clinical efficacy rates.29 In contrast, a 2021 systematic review noted very low-certainty evidence that corticosteroid injections outperformed dry needling for LE pain at short-term, while dry needling showed superior long-term (≥12 weeks) effects.30
Current evidence suggests that manual acupuncture may exert short-term therapeutic effects on lateral epicondylitis, whereas dry needling appears to demonstrate superior long-term efficacy. For patients with LE, a course of MA can be considered for short-term symptom control. For those seeking long-term recovery, treatment plans should prioritize interventions that incorporate DN. However, substantial heterogeneity exists across studies regarding pathological complexity and severity, acupuncture modalities, treatment duration, and choice of comparison groups. These methodological variations necessitate cautious interpretation of the pooled findings.
Acupuncture for Carpal Tunnel Syndrome (CTS)
From 2015 to 2024, one randomized trials and three systematic reviews have investigated acupuncture’s efficacy for carpal tunnel syndrome (CTS). While the adjunctive EA showed numerical reductions in pain scores when combined with nocturnal splinting, the between-group differences (−0.7 points on NRS; 95% CI: −1.34 to 0.06) did not reach the clinically important difference, suggesting limited clinical utility of the combined intervention.20 A systematic review reported that manual acupuncture provides superior symptom relief compared to medications, but no significant pain reduction was observed.31 The majority of included studies had a high risk of bias, which substantially limits the validity of the conclusions.31 However, Dong et al32 found that Acupuncture alone had no advantage over medicine in improving symptom severity, but as an adjunctive treatment, acupuncture might benefit CTS. Moreover, Choi et al33 found Acupuncture and laser acupuncture may have little or no effect in the short term on symptoms of CTS in comparison with placebo or sham acupuncture. The two studies demonstrated low or very low certainty of evidence according to GRADE criteria.
Current evidence is insufficient to support the efficacy of acupuncture therapy for CTS and high-quality RCTs using standardized protocols and objective outcomes are needed to confirm efficacy. Therefore, acupuncture is not recommended for routine care of CTS, and clinicians should prioritize treatments with established efficacy.
Acupuncture for Patellofemoral Pain Syndrome (PFPS)
Three randomized trials and one systematic review have investigated the efficacy of acupuncture in adults with PFPS Since 2015. A 2020 randomized trial21 reported that trigger point dry needling (TrP-DN) had comparable efficacy to ischemic compression in improving pain, function, and pressure pain thresholds for patients with PFPS at 3-month follow-up. Another trial22 found that TrP-DN combined with quadriceps stretching group had greater pain reduction and functional improvement compared to sham needling combined with stretching group at the 6-week treatment visit and the 3-month follow-up, alongside enhanced neuromuscular coordination. A systematic review34 (2020) reported moderate short-term pain relief (SMD −0.64, 95% CI: −1.17 to −0.11) with TrP-DN compared to comparative group. However, a randomized parallel-group trial23 found no additional benefit when TrP-DN was combined with a multimodal program (manual therapy + exercise).
Overall, recent evidence suggests that TrP-DN may have efficacy for PFPS at short-to-medium term, though conflicting findings exist regarding its synergistic value in multimodal therapies. More high-quality trials investigating long-term effects are clearly needed. For patients with PFPS, TrP-DN can be considered a therapeutic option for short-to-medium term pain relief. However, its routine addition to a comprehensive multimodal physical therapy program is not consistently supported by current evidence.
Acupuncture for Plantar Heel Pain Syndrome (PHPS)/Plantar Fasciitis (PF)
Two reviews and a clinical trail demonstrate the efficacy of acupuncture therapy for PHPS/PF. Thiagarajah et al35 concluded acupuncture therapy provided short-term (4–8 weeks) pain relief caused by PF. Llurda-Almuzara et al36 further supported DN’s efficacy for PHPS/PF, showing low-quality evidence that TrP-DN reduces pain intensity in the short term (MD −1.70 points, 95% CI −2.80 to −0.60) and moderate-quality evidence for long-term (>3months) pain reduction (MD −1.77 points, 95% CI −2.44 to −1.11) and functional improvement compared to controls. Moreover, A clinical trial25 suggested that DN was superior to steroid injection in patients with plantar fasciitis in the long term (1 year of follow-up).
A clinical study compared the efficacy of different acupuncture modalities for PHPS/PF, while two randomized trials investigated the combined effects of acupuncture therapy. Wang et al24 randomized 92 patients to receive either EA or MA over 4 weeks (12 sessions). The results demonstrated comparable therapeutic effects between EA and MA for PHPS. Both interventions significantly reduced heel pain and improved foot function at 4-, 6-, and 28-week follow-ups, with equivalent response rates (≥50% pain reduction). Ho et al26 demonstrated that a 4-week combined therapy of electroacupuncture with warm needling (EAWN) significantly alleviated first-step pain and improved Foot Function Index (FFI) scores in PHPS patients at the 4-week endpoint, with therapeutic effects sustained through the 8-week follow-up. Dunning et al27 demonstrated that electrical dry needling combined with manual therapy and exercise produced clinically superior outcomes (between-group NPRS Δ-2.2, CI: −2.8 to −1.6; SMD: 0.85) with sustained pain reduction and functional improvement at 3-month follow-up for patients with PF.
Current evidence supports the role of acupuncture therapy in managing plantar heel pain. We can consider it as a viable alternative or adjunctive treatment modality to conservative interventions for PHPS/PF. Acupuncture, with DN being particularly supported for long-term efficacy, is a well-evidenced therapeutic option for PHPS/PF that can reduce reliance on pharmaceutical interventions.
Implications for Practice
The evidence across conditions indicates that acupuncture can be considered a viable adjunct or alternative to conventional therapies for extremity musculoskeletal pain. While modality-specific findings vary—manual acupuncture shows modest short-term benefit, electroacupuncture remains inconsistent, and dry needling demonstrates more sustained improvements—acupuncture consistently emerges as a low-risk intervention with potential to enhance multimodal rehabilitation programs. For clinicians, tailoring treatment choice to patient characteristics, preferences, and available expertise remains crucial. Integrating acupuncture into broader rehabilitation strategies may maximize therapeutic benefit and support individualized, evidence-informed care.
Potential Mechanisms of Acupuncture
The therapeutic effects of acupuncture for extremity musculoskeletal pain, as observed across the conditions in this review, may be explained by several interconnected physiological mechanisms. Acupuncture elicits neuromodulatory effects by activating descending pain inhibitory pathways and stimulating the release of endogenous opioids (eg, endorphins) and neurotransmitters, which contribute to its analgesic effect.9,37 Its anti-inflammatory properties, mediated through the modulation of local and systemic inflammatory cytokines, may also alleviate the neurogenic inflammation present in tendinopathies such as lateral epicondylitis and plantar fasciitis.10
In addition, dry needling directly targets myofascial dysfunction by inactivating trigger points, improving local blood flow, and reducing muscle tension, which may underpin its sustained efficacy in conditions like PFPS and PHPS. Specifically, dry needling has been proposed to disrupt ongoing nociceptive input from trigger points and modulate central sensitization,38 and in tendinopathies, it may induce controlled microtrauma that stimulates inflammatory healing responses and promotes collagen remodeling, such as a shift from type III to type I collagen.11 While the predominant mechanism may vary by condition and technique, this multi-modal action provides a plausible theoretical foundation for the clinical outcomes summarized in this review.
Key Strengths of Acupuncture: Efficacy and Safety in Pain Management
Acupuncture therapy has been demonstrated to possess distinctive advantages as an alternative treatment for musculoskeletal pain, particularly in medication-intolerant patients or those seeking drug-free treatment options.39 Different from pharmacological agents, acupuncture does not rely on chemicals and avoids the common side effects of medications, such as digestive discomfort, drug dependence, and liver and kidney burden.40 This is especially important for patients who have been chronically reliant on NSAIDs or opioids, as acupuncture offers a safe and effective alternative for pain management.41
In addition to providing localized pain relief, acupuncture therapy has a holistic modulating effect that improves the overall health of the patient through multiple modulations of the neural-immune system.42 Acupuncture exerts a systemic conditioning effect by affecting the cerebral cortex, central nervous system, and immune system, prompting the release of endogenous analgesic substances (eg, endorphins) in the body.37 This makes acupuncture a suitable treatment for pain at a single site, as well as in the management of patients presenting with multiple symptoms.43 This makes it particularly suitable for patients with a history of complex chronic pain.
Challenges and Limitations: Evidence Quality and Practical Considerations
The efficacy of acupuncture is contingent upon individual differences, with the patient’s constitution, condition, and sensitivity to acupuncture influencing the therapeutic outcome.44 Acupuncture requires an advanced level of manipulation technique, and the treatment effect is predicated upon the therapist’s level of experience and skill because of the depth of acupuncture, selection of acupoints, and manipulation techniques all contribute to the efficacy of treatment.45,46
Despite the extensive documentation of acupuncture therapy in clinical practice, the number of high-quality randomized controlled trials remains limited. Moreover, several studies have demonstrated that the absence of scientifically standardized acupuncture treatment protocols, the heterogeneity of the intervention protocols included in the studies, and the low methodological quality have resulted in a low grade of evidence for the efficacy of acupuncture in the treatment of extremity musculoskeletal pain.28–33
Future research should prioritize rigorous, multicenter RCTs with adequate power and adherence to STRICTA reporting guidelines47 to ensure methodological transparency. Mechanistic investigations are also needed to clarify the neurophysiological pathways underlying acupuncture’s effects. Furthermore, broader inclusion of regional and non-English trials will be essential for developing a globally representative evidence base.
Conclusions
Emerging clinical evidence suggests that acupuncture is a safe and potentially effective treatment for extremity musculoskeletal pain. Stronger support exists for plantar heel pain syndrome (PHPS) and lateral epicondylitis (LE), while trigger point dry needling may offer short-to-medium term benefits in patellofemoral pain syndrome (PFPS). Evidence remains insufficient for recommending acupuncture in carpal tunnel syndrome (CTS).
For clinical practice, acupuncture should be discussed with patients as a low-risk option, particularly for those unresponsive to or unwilling to pursue first-line treatments. Manual acupuncture may be suitable for short-term relief, while dry needling could be prioritized for longer-term outcomes. Importantly, acupuncture is best integrated into comprehensive multimodal strategies rather than applied in isolation.
Nevertheless, these conclusions are constrained by methodological heterogeneity and the limited number of high-quality studies. Future research should therefore focus on conducting large-scale, standardized RCTs, performing head-to-head comparisons of acupuncture modalities, and expanding the evidence base with underrepresented regional trials. Through these efforts, acupuncture may be more firmly integrated into comprehensive, evidence-based management strategies for musculoskeletal pain.
Acknowledgments
This work was supported by the Beijing Sport University Sports Rehabilitation Science Laboratory (Project Number: 2024KFZX002). The authors gratefully acknowledge the financial support provided by the laboratory, which made this research possible.
Funding
The financial support provided by the Beijing Sport University Sports Rehabilitation Science Laboratory (Project Number: 2024KFZX002).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396(10258):1204–1222.
2. Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ. 2003;81(9):646–656.
3. Scott A, Backman LJ, Speed C. Tendinopathy: update on pathophysiology. J Orthop Sports Phys Ther. 2015;45(11):833–841. doi:10.2519/jospt.2015.5884
4. Bhala N, Emberson J, Merhi A, et al. Vascular and upper gastrointestinal effects of non-steroidal anti-inflammatory drugs: meta-analyses of individual participant data from randomised trials. Lancet. 2013;382(9894):769–779.
5. Dean BJF, Lostis E, Oakley T, Rombach I, Morrey ME, Carr AJ. The risks and benefits of glucocorticoid treatment for tendinopathy: a systematic review of the effects of local glucocorticoid on tendon. Semin Arthritis Rheum. 2014;43(4):570–576. doi:10.1016/j.semarthrit.2013.08.006
6. Dommerholt J, Mayoral Del Moral O, Gröbli C. Trigger point dry needling. J Man Manip Ther. 2006;14(4):70E–87E. doi:10.1179/jmt.2006.14.4.70E
7. Yin C, Buchheit TE, Park JJ. Acupuncture for chronic pain: an update and critical overview. Curr Opin Anaesthesiol. 2017;30(5):583–592. doi:10.1097/ACO.0000000000000501
8. Zhang R, Lao L, Ren K, Berman BM. Mechanisms of acupuncture-electroacupuncture on persistent pain. Anesthesiology. 2014;120(2):482–503. doi:10.1097/ALN.0000000000000101
9. Chen T, Zhang WW, Chu Y-X, Wang Y-Q. Acupuncture for pain management: molecular mechanisms of action. Am J Chin Med. 2020;48(4):793–811. doi:10.1142/S0192415X20500408
10. McDonald JL, Cripps AW, Smith PK. Mediators, receptors, and signalling pathways in the anti‐inflammatory and antihyperalgesic effects of acupuncture. Evid Based Complement Alternat Med. 2015;2015:975632. doi:10.1155/2015/975632
11. McAphee D, Bagwell M, Falsone S. Dry needling: a clinical commentary. Int J Sports Phys Ther. 2022;17(4):551–560. doi:10.26603/001c.35693
12. Cox J, Varatharajan S, Côté P, Collaboration O. Effectiveness of acupuncture therapies to manage musculoskeletal disorders of the extremities: a systematic review. J Orthop Sports Phys Ther. 2016;46(6):409–429. doi:10.2519/jospt.2016.6270
13. Zhang Y, Wang C. Acupuncture and chronic musculoskeletal pain. Curr Rheumatol Rep. 2020;22(11):80. doi:10.1007/s11926-020-00954-z
14. Chang WD, Lai PT, Tsou YA. Analgesic effect of manual acupuncture and laser acupuncture for lateral epicondylalgia: a systematic review and meta-analysis. Am J Chin Med. 2014;42(6):1301–1314. doi:10.1142/S0192415X14500815
15. Sim H, Shin BC, Lee MS, Jung A, Lee H, Ernst E. Acupuncture for carpal tunnel syndrome: a systematic review of randomized controlled trials. J Pain. 2011;12(3):307–314. doi:10.1016/j.jpain.2010.08.006
16. Barton CJ, Lack S, Hemmings S, Tufail S, Morrissey D. The ‘best practice guide to conservative management of patellofemoral pain’: incorporating level 1 evidence with expert clinical reasoning. Br J Sports Med. 2015;49(14):923–934. doi:10.1136/bjsports-2014-093637
17. Clark RJ, Tighe M. The effectiveness of acupuncture for plantar heel pain: a systematic review. Acupunct Med. 2012;30(4):298–306. doi:10.1136/acupmed-2012-010183
18. Huang CH, Lin CY, Sun MF, Fu Z, Chou LW. Efficacy of Fu’s subcutaneous needling on myofascial trigger points for lateral epicondylalgia: a randomized control trial. Evid Based Complement Alternat Med. 2022;2022:5951327. doi:10.1155/2022/5951327
19. Dunning J, Mourad F, Bliton P, et al. Percutaneous tendon dry needling and thrust manipulation as an adjunct to multimodal physical therapy in patients with lateral elbow tendinopathy: a multicenter randomized clinical trial. Clin Rehabil. 2024;38:2692155241249968.
20. Chung VCH, Rst H, Liu S, et al. Electroacupuncture and splinting versus splinting alone to treat carpal tunnel syndrome: a randomized controlled trial. Cmaj. 2016;188(12):867–875. doi:10.1503/cmaj.151003
21. Behrangrad S, Abbaszadeh-Amirdehi M, Kordi Yoosefinejad A, Esmaeilnejadganji SM. Comparison of dry needling and ischaemic compression techniques on pain and function in patients with patellofemoral pain syndrome: a randomised clinical trial. Acupunct Med. 2020;38(6):371–379. doi:10.1177/0964528420912253
22. Ma YT, Li LH, Han Q, et al. Effects of trigger point dry needling on neuromuscular performance and pain of individuals affected by patellofemoral pain: a randomized controlled trial. J Pain Res. 2020;13:1677–1686. doi:10.2147/JPR.S240376
23. Espí-López GV, Serra-Añó P, Vicent-Ferrando J, et al. Effectiveness of inclusion of dry needling in a multimodal therapy program for patellofemoral pain: a randomized parallel-group trial. J Orthop Sports Phys Ther. 2017;47(6):392–401. doi:10.2519/jospt.2017.7389
24. Wang W, Liu Y, Jiao R, Liu S, Zhao J, Liu Z. Comparison of electroacupuncture and manual acupuncture for patients with plantar heel pain syndrome: a randomized controlled trial. Acupunct Med. 2021;39(4):272–282. doi:10.1177/0964528420947739
25. Rastegar S, Baradaran Mahdavi S, Hoseinzadeh B, Badiei S. Comparison of dry needling and steroid injection in the treatment of plantar fasciitis: a single-blind randomized clinical trial. Int Orthop. 2018;42(1):109–116. doi:10.1007/s00264-017-3681-1
26. Ho LF, Guo Y, Ching JY, et al. Efficacy of electroacupuncture plus warm needling therapy for plantar heel pain: a randomised waitlist-controlled trial. Acupunct Med. 2021;39(4):283–291. doi:10.1177/0964528420946048
27. Dunning J, Butts R, Henry N, et al. Electrical dry needling as an adjunct to exercise, manual therapy and ultrasound for plantar fasciitis: a multi-center randomized clinical trial. PLoS One. 2018;13(10):e0205405. doi:10.1371/journal.pone.0205405
28. Navarro-Santana MJ, Sanchez-Infante J, Gómez-Chiguano GF, Cummings M, Fernández-de-las-peñas C, Plaza-Manzano G. Effects of manual acupuncture and electroacupuncture for lateral epicondylalgia of musculoskeletal origin: a systematic review and meta-analysis. Acupunct Med. 2021;39(5):405–422. doi:10.1177/0964528420967364
29. Guo Y, Zhou Y, Zhou R, Wu P, Liang F, Yang Z. Effectiveness of acupuncture for lateral epicondylitis: a systematic review and meta-analysis of randomized controlled trials. Pain Res Manag. 2020;2020:8506591. doi:10.1155/2020/8506591
30. Sousa Filho LF, Barbosa Santos MM, Dos Santos GHF, da Silva Júnior WM. Corticosteroid injection or dry needling for musculoskeletal pain and disability? A systematic review and GRADE evidence synthesis. Chiropr Man Therap. 2021;29(1):49. doi:10.1186/s12998-021-00408-y
31. Wu IX, Lam VC, Ho RS, et al. Acupuncture and related interventions for carpal tunnel syndrome: systematic review. Clin Rehabil. 2020;34(1):34–44. doi:10.1177/0269215519877511
32. Dong Q, Li X, Yuan P, et al. Acupuncture for carpal tunnel syndrome: a systematic review and meta-analysis of randomized controlled trials. Front Neurosci. 2023;17:1097455. doi:10.3389/fnins.2023.1097455
33. Choi GH, Wieland LS, Sim H, Lee H, Lee MS, Shin BC. Acupuncture and related interventions for the treatment of symptoms associated with carpal tunnel syndrome. Cochrane Database Syst Rev. 2018;12(12):Cd011215. doi:10.1002/14651858.CD011215.pub2
34. Rahou-El-Bachiri Y, Navarro-Santana MJ, Gómez-Chiguano GF, et al. Effects of trigger point dry needling for the management of knee pain syndromes: a systematic review and meta-analysis. J Clin Med. 2020;9(7). doi:10.3390/jcm9072044.
35. Thiagarajah AG. How effective is acupuncture for reducing pain due to plantar fasciitis? Singapore Med J. 2017;58(2):92–97. doi:10.11622/smedj.2016143
36. Llurda-Almuzara L, Labata-Lezaun N, Meca-Rivera T, et al. Is dry needling effective for the management of plantar heel pain or plantar fasciitis? An updated systematic review and meta-analysis. Pain Med. 2021;22(7):1630–1641. doi:10.1093/pm/pnab114
37. Zhang R, Lao L, Ren K, Berman BM. Mechanisms of acupuncture–electroacupuncture on persistent pain. Anesthesiology. 2014;120(2):482–503.
38. Dommerholt J. Dry needling—peripheral and central considerations. J Man Manip Ther. 2011;19(4):223–227. doi:10.1179/106698111X13129729552065
39. Penney LS, Ritenbaugh C, DeBar LL, Elder C, Deyo RA. Provider and patient perspectives on opioids and alternative treatments for managing chronic pain: a qualitative study. BMC Fam Pract. 2016;17:1–15. doi:10.1186/s12875-016-0566-0
40. Vickers AJ, Linde K. Acupuncture for chronic pain. JAMA. 2014;311(9):955–956. doi:10.1001/jama.2013.285478
41. Cherkin DC, Sherman KJ, Avins AL, et al. A randomized trial comparing acupuncture, simulated acupuncture, and usual care for chronic low back pain. Arch Intern Med. 2009;169(9):858–866. doi:10.1001/archinternmed.2009.65
42. Cui J, Song W, Jin Y, et al. Research progress on the mechanism of the acupuncture regulating neuro-endocrine-immune network system. Vet Sci. 2021;8(8):149. doi:10.3390/vetsci8080149
43. Yuan J, Purepong N, Kerr DP, Park J, Bradbury I, McDonough S. Effectiveness of acupuncture for low back pain: a systematic review. Spine. 2008;33(23):E887–E900. doi:10.1097/BRS.0b013e318186b276
44. Kim Y-K, Park J-Y, Kim S-N, et al. What intrinsic factors influence responsiveness to acupuncture in pain?: a review of pre-clinical studies that used responder analysis. BMC Complement Altern Med. 2017;17(1):281. doi:10.1186/s12906-017-1792-2
45. Yu Z, Luo L, Li Y, et al. Different manual manipulations and electrical parameters exert different therapeutic effects of acupuncture. J Tradit Chin Med. 2014;34(6):754–758. doi:10.1016/S0254-6272(15)30092-3
46. Choi Y-J, Lee J-E, Moon W-K, Cho S-H. Does the effect of acupuncture depend on needling sensation and manipulation? Complement Ther Med. 2013;21(3):207–214. doi:10.1016/j.ctim.2012.12.009
47. MacPherson H, Altman DG, Hammerschlag R, et al. Revised STandards for reporting interventions in clinical trials of acupuncture (STRICTA): extending the CONSORT statement. J Altern Complement Med. 2010;16(10):
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.