")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Acupuncture Therapies for Individuals with Overweight or Obesity: An Overview of Systematic Reviews
Authors Chen J , Shergis JL , Guo X, Zhang AL , Wang H, Lu C, Xue CC , Xie C
Received 2 January 2022
Accepted for publication 11 May 2022
Published 30 May 2022 Volume 2022:15 Pages 1651—1666
DOI https://doi.org/10.2147/DMSO.S356853
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Jiaxin Chen,1,2 Johannah L Shergis,3 Xinfeng Guo,1,2 Anthony Lin Zhang,3 Hanlin Wang,1,2 Chuanjian Lu,1,2 Charlie C Xue,3 Changcai Xie1,2
1Guangdong Provincial Hospital of Chinese Medicine, Guangdong Provincial Academy of Chinese Medical Sciences, and The Second Clinical College, Guangzhou University of Chinese Medicine, Guangzhou, People’s Republic of China; 2State Key Laboratory of Dampness Syndrome of Chinese Medicine, Guangdong-Hong Kong-Macau Joint Laboratory on Chinese Medicine, and Immune Disease Research Guangdong Provincial Key Laboratory of Clinical Research on Traditional Chinese Medicine Syndrome, Guangzhou, 510120, People’s Republic of China; 3The China-Australia International Research Centre for Chinese Medicine, School of Health and Biomedical Sciences, RMIT University, Bundoora, Melbourne, Australia
Correspondence: Changcai Xie, Guangdong Provincial Hospital of Chinese Medicine, Guangdong Provincial Academy of Chinese Medical Sciences, and The Second Clinical College, Guangzhou University of Chinese Medicine, 111 Dade Road, Yuexiu District, Guangzhou, 510120, People’s Republic of China, Tel +86 13650997551, Email [email protected]
Purpose: An increasing number of people are affected by overweight or obesity, and the personal and social health burden is growing rapidly. Acupuncture is gaining popularity as an alternative treatment to manage weight. This research aims to update and synthesize the evidence of acupuncture therapies from systematic reviews for treating overweight and obesity.
Methods: Nine databases were searched from their inception to March 2022. Overweight or obesity was classified using standard diagnostic criteria. Published systematic reviews that included randomized controlled trials and quasi-randomized studies were eligible. Quality was assessed via the AMSTAR-2 scale and risk of bias using the ROBIS tool.
Results: Thirty-eight systematic reviews were identified. Acupuncture therapies and auricular acupoint stimulation showed benefits in terms of reducing body weight and body mass index. Catgut embedding therapy and abdominal acupuncture are currently not in widespread use with insufficient evidence. Acupuncture therapies appear to be safe. Most of the reviews were assessed as having high risk of bias and low confidence in the findings.
Conclusion: There is a need for larger and more methodologically sound randomized controlled trials to evaluate the effectiveness of acupuncture therapies for individuals who are affected by overweight or obesity.
Keywords: acupuncture, overweight, obesity, systematic review
Introduction
The prevalence of overweight and obesity is increasing rapidly around the world.1 Changes in the food environment and food systems as well as reduced opportunities for physical activity often account for the high incidence of people who are affected by overweight and obesity.2 It is estimated that more than one hundred million (5%) children and over six hundred million (12%) adults are affected by obesity worldwide.3 In 2017, China and India had the largest population of children with obesity, and the United States and China had the highest number of adults with obesity.3 Overweight and obesity is a risk factor for numerous chronic diseases, including cardiovascular disease, diabetes, chronic kidney disease and cancer.4,5 A high body mass index (BMI) greater than 25 kg/m2 (defined cut-off of overweight) accounted for four million deaths globally, and more than two-thirds of deaths were due to cardiovascular disease.3
Reduced energy intake, increased physical activity and behavioral change are the fundamental approaches to weight loss and weight maintenance recommended in almost all international guidelines.6–8 In addition to lifestyle therapy, pharmacotherapy is a vital alternative or adjunct method for losing weight.8,9 Currently, among the five long-term drug therapies approved by the US Food and Drug Administration, only orlistat is available worldwide.10 One recent study found that all the approved drugs for anti-obesity were associated with higher odds of weight loss by more than 5%.11 However, even though anti-obesity drugs can help people to lose weight, few patients are reluctant to use these drugs because of concerns about safety.9 Actually, pharmacotherapy of obesity has a long history populated with multiple unsatisfaction, which is mainly from the concerns of side effect, such as headache, dizziness, insomnia, nausea, constipation, diarrhea, and concerns of potential risk about cardiovascular disease, stroke, hypertension, etc.9,10 Some future candidate drugs for anti-obesity appear to be promising but there are still considerable barriers and challenges.12,13
In recent years, acupuncture therapy has gained popularity as a treatment for weight loss. There is also a number of clinical trials and systematic reviews that evaluate acupuncture for overweight and obesity.14,15 However, interpreting evidence in relation to acupuncture treatment is challenging due to a limited number of high-quality trials with adequate treatment durations. The aim of this overview is to critically evaluate and synthesize published systematic reviews and provide guidance for future research.
Methods
Protocol and Registration
This systematic overview was conducted following a predetermined written protocol registered on the PROSPERO database with registration number CRD42020163840.
Data Sources and Search Strategy
PubMed, Embase, Cumulative Index of Nursing and Allied Health Literature (CINAHL), Cochrane Central Register of Controlled Trials (including the Cochrane Library and Allied and Complementary Medicine Database), China BioMedical Literature (CBM), China National Knowledge Infrastructure (CNKI), Chongqing VIP (CQVIP) and Wanfang databases were searched from their inceptions to March 2022. For all included studies, reference lists were searched for further reviews. MEDLINE search strategy is provided (Supplementary Material: Appendix 1). No restrictions were applied to the search.
Eligibility Criteria
To be eligible, systematic reviews were required to meet the following criteria:
- Type of reviews: Systematic reviews of randomized controlled trials (RCTs) or reviews that included both RCTs and quasi-randomized studies where RCTs were in the majority.
- Type of participants: Overweight or obesity was classified using standard diagnostic criteria (eg, the 2016 AACE/ACE Guidelines).8 No restrictions regarding age, gender or condition duration were applied. Studies that included overweight or obesity as a complication of metabolic disorders such as diabetes mellitus, hyperlipidaemia were also included basing on the 2016 AACE/ACE Guidelines.8
- Type of intervention: Acupuncture therapies, including manual acupuncture, electroacupuncture, auricular (ear) acupuncture, acupressure, warming needle acupuncture, moxibustion, laser acupuncture, catgut embedding; used alone or in combination.
- Type of comparator: Placebo, no treatment or waitlist control, psychotherapy, pharmacotherapy, lifestyle therapies including dietary measures, physical activity, and/or behavioral changes.
- Type of outcomes: Measures of body composition including body weight (BW), BMI, waist circumference (WC), waist hip ratio (WHR) and body fat mass (BFM), or effective rate according to a recognized standard, or adverse events.
The full criteria are listed in Supplementary Material: Appendix 2.
Study Selection and Data Management
Two independent reviewers (JXC, HLW) screened titles and abstracts against the eligibility criteria and obtained full reports for all titles that appeared to meet the inclusion criteria or where there was uncertainty. The same two independent reviewers managed data extraction in duplicate for each eligible study, using a standard data collection form in Microsoft Excel. A third reviewer (XFG) was consulted when disagreements arose. Extracted information included authors, date of publication, country, details of studies such as participant characteristics, intervention, comparator, number of participants, meta-analysis results, whether a sensitivity or subgroup analysis was conducted, risk of bias assessment and adverse events.
Risk of Bias Assessment
Three authors (JXC, JLS, HLW) independently assessed the methodological quality of each included study using the AMSTAR-2 scale and the Risk of Bias in Systematic Reviews (ROBIS) tool.16,17 A fourth reviewer resolved any discrepancies (ALZ).
Data Synthesis
Due to the expected overlap of RCTs included in the systematic reviews and heterogeneity (particularly with regard to intervention and comparator arms), we conducted a narrative synthesis of the findings rather than pooling meta-analyses from the included reviews.
Results
The search identified 616 potentially relevant systematic reviews and 581 titles/abstracts were screened after duplicate removal (Figure 1). 77 full-text articles were assessed for eligibility and 38 systematic reviews were included in this overview. Results of the included reviews are presented in Table 1 (details of the individual studies can be found in Supplementary Material: Appendix 3). The summarized AMSTAR-2 scores and ROBIS scores are presented in Tables 2 and 3 (further justification statements are presented in Supplementary Material: Appendix 4 and Appendix 5). All excluded reviews are listed in Supplementary Material: Appendix 6. The 38 included reviews14,15,18–53 were published between 2009 and 2020. The reviews were mostly conducted in China (33 reviews)14,15,18,19,21–25,27–29,31–33,36–53 and one each from Australia,26 Iran,30 Korea,35 Canada34 and Brazil.20 The reviews assessed the following acupuncture therapies, including auricular acupoint stimulation (7 reviews),20,23,31,33,37,43,52 catgut embedding (6),19,22,25,32,38,46 abdominal acupuncture (2),28,32 electroacupuncture (2),15,49 laser acupuncture (1).30 The other 20 reviews14,18,21,24,26,27,29,34–36,39,40,42,44,45,47,48,50,51,53 did not investigate a particular type but assessed any form of acupuncture. Anthropometry outcomes were common, such as BMI (34 reviews),14,15,18–23,26–40,42,43,45–53 BW (30),14,15,18–20,22,23,26,29–40,42,43,45,47–53 WC (21),14,18,22,23,27–32,36,38,42,43,46–49,52,53 BFM (12),14,18,23,27,29–31,37,40,42,43,52 hip circumference (13),22,23,27,29–31,38,42,43,47,49,52,53 and adverse events were investigated in 27 reviews.14,15,18,19,21–23,25–32,34,35,37,39–43,45,47,48,51 All of the reviews, except two,30,37 conducted meta-analysis. The Cochrane Collaboration's tool for assessing risk of bias was used in 26 reviews14,15,18–20,22,25–29,31–33,35–40,45,46,48–51 and the Jadad score in 12 reviews.21,23,24,30,34,41–44,47,52,53 A total of 324 clinical trials were included in the reviews and 109 (33.6%) were included in more than one review.
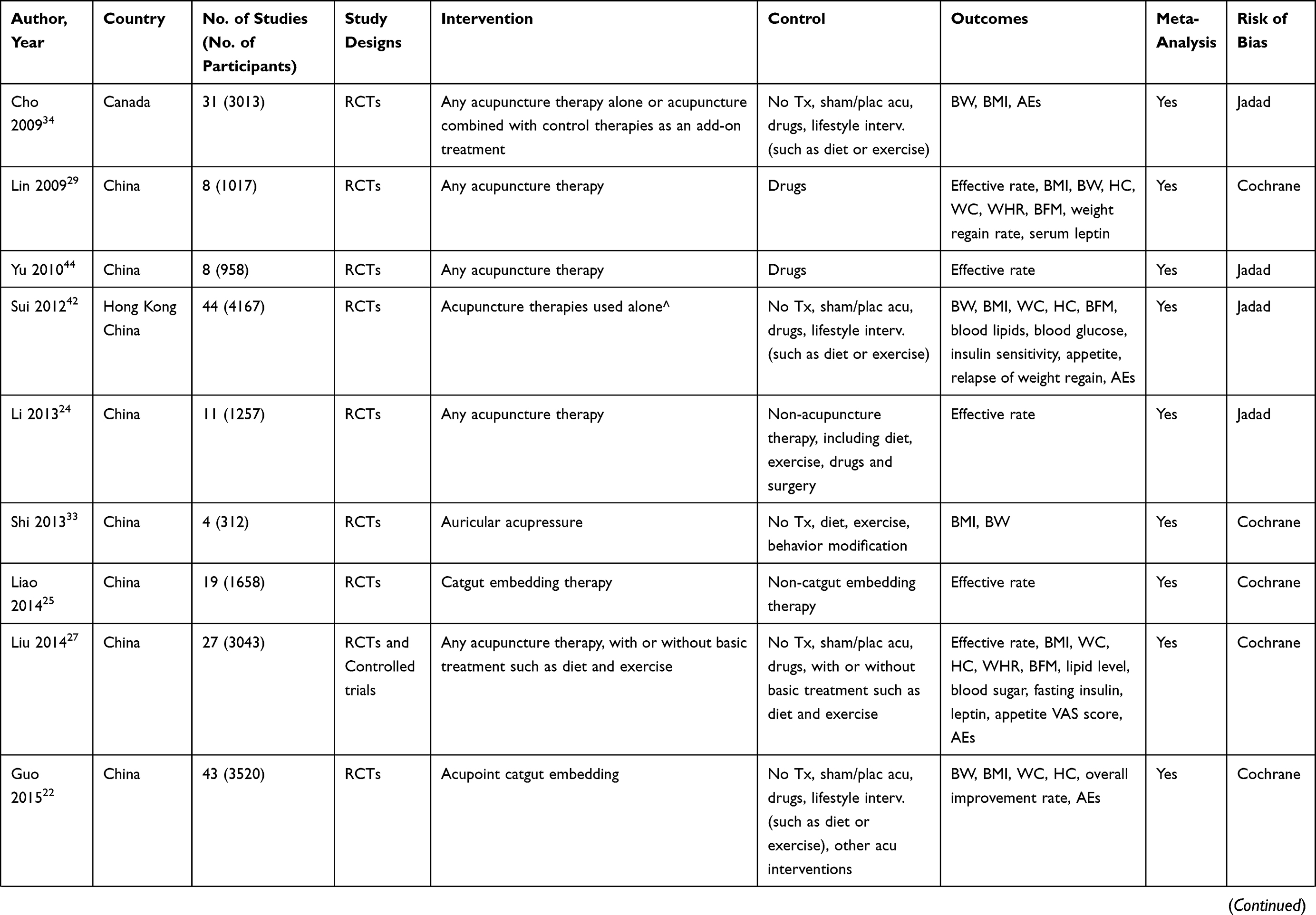 |  |  |  |
Table 1 Summary of the Included Systematic Reviews |
 |
Table 2 Result of AMSTAR-2 |
 |
Table 3 Results of ROBIS Tool |
 |
Figure 1 Flow diagram of study selection. |
Quality of the Included Reviews
AMSTAR-2
A summary of the AMSTAR-2 results can be found in Table 2. The confidence in the reviews were all rated as critically low except one22 that was rated as low. The major insufficiencies were the lack of registration or publication of protocols prior to commencement of the reviews and justification for excluding individual studies. Thirty14,15,18–23,25–27,29,30,32,34–37,39,40,42,43,45–52 of the 38 reviews (78.9%) employed the PICO (population, intervention, control group, and outcome) approach as an organizing framework for establishing study questions (AMSTAR-2 Item 1) but only five reviews14,20,22,32,48 registered or published their protocol before commencement of the review (Item 2). Three reviews justified the selection of study type, eg, RCTs (Item 3).19,23,43 Most reviews (84.2%)14,15,18,19,21,22,24–29,31–38,40–43,45–48,50–53 included a comprehensive literature search (Item 4), performed study selection in duplicate (78.9%)14,15,18–31,34–39,42,43,45–49,51 (Item 5) and also performed data extractions in duplicate (68.4%)14,15,18–23,26–30,36,37,40,42,45–53 (Item 6). However, none of the reviews provided a complete list of potentially relevant studies with justification for the exclusion of each (Item 7). All but one33 provided characteristic information of their included studies (Item 8) and 2614,15,18,19,22,25–28,31–33,35–37,39–41,45–51,53 used a satisfactory technique for assessing the risk of bias in individual studies, such as the Cochrane Risk of Bias Tool (Item 9). Only one review reported funding sources of the included studies (Item 10).20 Statistical methods for meta-analysis were appropriate in most reviews (81.6%)14,15,18–25,27–29,32,34,35,37,40–53 (Item 11) but only five reviews24,25,43,45,52 reported the potential impact of risk of bias on the results (Item 12). Although, when reviewers interpreted their results most discussed the impact of risk of bias (71.1%) (Item 13).18,21–31,33–37,39–42,44–47,50,52 Exploration of heterogeneity and its impact on the result and clinical recommendations was discussed in 18 reviews (Item 14).15,18,25,28–31,34–36,39,43–49 Publication bias was discussed in 24 reviews15,18–25,27,28,34,35,38,41–45,47–49,52,53 (Item 15) and potential sources of conflict of interest and review funding was noted in 28 reviews14,18–23,26,30–32,34–36,38,40,42–53 (Item 16).
ROBIS
The ROBIS tool is divided into four domains. Domain 1, which assesses concerns regarding specification of study eligibility criteria, was only at low risk of bias in two review.14,48 Domain 2 assesses any concerns regarding methods used to identify/select studies. Three14,28,45 achieved a low risk of bias rating overall, one34 was rated as unclear and the remaining 3414,15,18–27,29–33,35–44,46–53 were judged to be at a high risk of bias because some eligible studies were likely missing from the review. Domain 3 assesses concerns regarding methods used to collect data and appraise studies. 1414,22,26–28,37,40,45,47–51,53 of the 38 reviews achieved a low risk of bias, 1115,18,19,25,31,32,35,36,39,41,46 were at unclear risk and 1320,21,23,24,29,30,33,34,38,42–44,52 were at high risk of bias because some bias may have been introduced through the data collection or risk of bias assessment (Table 3). With regards to domain 4, which assesses concerns regarding the synthesis of results, the majority were rated at high risk of bias because potential bias were ignored or heterogeneity was not accounted.14,15,19–24,26,27,29,31–40,42,43,45–47,49–53 Two30,48 was rated as low risk of bias and five18,25,28,41,44 were at unclear risk. The final section of the tool provides a rating of the overall risk of bias of reviews. All the reviews were judged to be at a high risk of bias because one or more of the concerns raised in the other domains was not addressed in the review conclusions and/or reviews did not consider the relevance of the included studies in light of the review question.
Effects of Interventions
Seventeen reviews assessed various acupuncture therapies compared to sham acupuncture or no treatment.14,18,21,26,27,34,35,39,40,42,45,47,48,50–53
Five reviews reported significant reduction both in BW and BMI in acupuncture groups.18,34,42,45,47 In terms of BMI, four of the reviews had a high heterogeneity, which may have been due to various acupuncture treatments.18,42,45,47 In one recent review, Pan 2020,47 meta-analysis showed that acupuncture was superior to sham acupuncture in terms of BMI reduction (mean difference [MD] −0.61 kg/m2, 95% confidence interval [CI] −0.86, −0.36, I2 = 64.9%, n = 15) and BW reduction (MD −1.44 kg, 95% CI −2.26, −0.63, I2 = 66.8%, n = 14). Subgroup analysis based on different types of acupuncture therapies including auricular acupuncture and catgut embedding showed similar results to the overall pool of studies. The results were basically consistent with a previous study of Kepei et al in 2018.45
Six reviews showed inconsistent results with reductions in either BW or BMI but not both.39,40,50–53 The remaining three reviews failed to show a statistically significant reduction in BW or BMI when acupuncture was compared to sham.26,27,35 However, the number of included RCTs was very small with two reviews26,35 only including one eligible RCT each and the other review27 only including three RCTs.
One study compared acupuncture alone or in combination with lifestyle modification to sham acupuncture or no treatment.21 There was a significant reduction in BMI in the intervention group compared to control. The other three studies showed similar results, with reported reductions in BW and BMI.14,18,48
Auricular Acupoint Stimulation
Five reviews investigated auricular acupoint stimulation compared to sham auricular acupoint stimulation.20,23,33,37,43 Stimulation referred to auricular acupuncture, acupressure, or acupoint taping with seeds. All reviews reported statistically significant meta-analysis results in favour of the auricular acupoint therapies in terms of BW and BMI.
Dongqun et al examined the comparison of auricular points taping and no treatment.37 Only one RCT was included and it showed a favorable effect of auricular acupoint taping in reducing BW and BMI. In another study, results showed no difference in BMI when auricular acupoint stimulation was compared to sham or no treatment.31
Catgut Embedding
Three systematic reviews compared catgut embedding therapy to placebo embedding with variable results.19,22,32 Taipin et al pooled two studies in meta-analysis and reported a favourable effect of intervention on BW reduction (MD −3.10 kg, 95% CI −0.02, −6.0, I2=0).22 In 2018, William et al reported that catgut embedding reduced BW and BMI, however, results had errors as the data was incorrectly pooled.19 Jili et al failed to show a significant effect of catgut embedding on BW or BMI in participants with abdominal obesity.32
Abdominal Acupuncture
One review including one RCT, reported a significant reduction of BMI when abdominal acupuncture was compared to sham abdominal acupuncture in women with obesity (MD −2.01 kg, 95% CI −0.75, −3.27).28
Adverse Events
A total of 27 systematic reviews reported adverse events.14,15,18,19,21–23,25–32,34,35,37,39–43,45,47,48,51 Three reviews stated that no events occurred or were reported in the included studies.15,30,41 Adverse events relating to acupuncture treatments were reported in 24 systematic reviews and events appeared to be mild, tolerable and self-resolving.14,18,19,21–23,25–29,31,32,34,35,37,39,40,42,43,45,47,48,51 Local reaction to the acupuncture treatments were most common such as redness, pain or discomfort, soreness or swelling, bleeding or bruising.
Discussion
This overview represents a comprehensive review of systematic reviews and meta-analyses on the quality, efficacy and safety of acupuncture clinical trials for people with overweight and obesity. Thirty-eight systematic reviews including over three hundreds clinical trials are identified in this review. Evaluation of the reviews indicated that acupuncture therapies may be effective and safe for weight reduction. However, assessment using AMSTAR-2 and ROBIS indicated that the systematic reviews had methodological shortfalls, and it was difficult to draw a firm conclusion.
The number of people who are affected by overweight and obesity is increasing worldwide, often referred to as a global epidemic.54 The pathogenesis of overweight and obesity is multifaceted and includes a spectrum of environmental, genetic, and epigenetic factors, which all contribute to the disease. Among the environmental factors, an excessive energy intake, a sedentary lifestyle, and circadian rhythm sleep alterations are probably the most important determinants.55 Therefore, reducing daily calorie intake, regulating lifestyle and adapting activity and exercise habits appear to be the basic methods to lose weight. However, the long-term effectiveness of obesity treatments is poor and there are substantial barriers that undermine treatment results. Reasons like lack of recognition of obesity as a chronic condition, time restriction, low socioeconomic status, and a wide range of comorbidities including mental health, sleep, cardiovascular, respiratory, endocrine and digestive disorders should be taken into consideration. The absence of specific obesity training of health professionals, patient attitudes and self-determination as well as availability of obesity treatments are all important barriers.56 Unhealthy weight loss attitudes and short-term weight loss such as vomiting, fasting, using laxatives or diet drugs, has become a concern.57–59 Research suggests that non-medical use of prescription drugs for weight loss is relatively common and that this behavior is related to other harmful behaviors with no evidence of effective long-term weight loss.60 Stimulants are the most widely investigated drug with regard to unhealthy weight management practices, because of their potential (and reputation) for expedited weight loss and suppression of appetite.59–61
As acupuncture therapies have gained wider recognition throughout the world, acupuncture treatment for weight loss has increased in popularity. In addition to filiform needle acupuncture and electroacupuncture, various types of acupuncture therapies are also applied for losing weight clinically, such as auricular acupuncture, moxibustion, cupping, catgut embedding. According to individual symptom and TCM syndrome, as well as the characteristic of each method, different types of acupuncture therapies would be applied for different patients with obesity. The popularity of acupuncture for weight loss is not without reason. On one hand, acupuncture therapies can not only help to lose weight but also to improve obesity-related problems, such as feeling of heavy body, constipation, menstrual disorder, etc. On the other hand, it is a relatively safe therapy. Adverse events are mainly related to local reaction of the treatment, such as soreness and bruising, which are usually mild and could be self-relief. What’s more, when patients undergo acupuncture treatment, they would be inculcated with healthy knowledge about diet, exercise, lifestyle from their doctor or health manager, which makes them more easier to correct bad life habits and stick to their weight loss program.
The first research about acupuncture therapies for obesity treatment was published in the 1970s.62 It reported that 21 people with obesity achieved weight loss after employing auricular acupuncture treatment lasting from two to six weeks. Following this initial research, many more research studies begun to investigate this emerging area of acupuncture treatment. The potential mechanism of body weight reduction influenced by acupuncture is complex, and it may have several actions on biochemical markers of obesity such as obesity-related peptides (eg, leptin, ghrelin), glucose and lipid metabolism, insulin resistance, and inflammatory markers.63 Therefore, the benefits of acupuncture may be greater than weight loss alone and may include improved metabolism in terms of glucose and lipid levels.64 This prospect is of great significance since obesity is one of the main causes of metabolic disorders such as diabetes, hyperlipidemia, and hypertension.8
There are still some barriers and challenges when it comes to the development and promotion of acupuncture treatment for overweight and obesity. First of all, the lack of standard and precise therapeutic schemes, including acupoint selection, type of acupuncture therapy such as electroacupuncture, manual acupuncture, auricular acupuncture and so on, treatment frequency and duration, all make it difficult to recommend its application more widely. Secondly, effects of acupuncture for losing weight may be affected by factors like age, race, obesity complication, TCM constitution and so on. Therefore, it may be of great significance to discover the advantages group of acupuncture for weight loss. Weight regain is another concern. People with obesity and overweight always go through the cycle of “lose weight – weight regain”. Eventually, they have to compromise and give up their weight loss plan due to various reasons. Although this question was not specifically investigated in this overview or any of the included systematic reviews, it is worth exploring the long-term benefits of acupuncture in future studies. Furthermore, acupuncture is not available in all regions and comes at a cost. Unlike lifestyle interventions such as dieting or exercise, which can be undertaken anytime and anywhere, patients have to attend to a hospital or clinic to receive acupuncture treatments twice to three times a week for some time, which may be a significant barrier to its use.
Strengths and Limitations
The database search of this overview was thorough and up to date. The overview was not limited to the participants age and gender and type of acupuncture therapies. It excluded studies, which referred to obesity drugs such as sibutramine as it is no longer in use; therefore, this review provides relevant evidence for the current clinical environment.
However, there are also some methodological shortfalls that might limit the confidence of this overview. Firstly, the evidence might not be comprehensive since we only included systematic reviews that assessed RCTs and quasi-RCTs. The review only focused on the two main anthropometry outcomes namely BW and BMI and acupuncture effects on metabolic outcomes such as serum glucose and blood lipid levels were not assessed.
Conclusions
There are many systematic reviews that assess the efficacy and safety of acupuncture therapies for people with overweight or obesity. Results from the included systematic reviews showed promising benefits in terms of weight loss and BMI reduction. However, included systematic reviews had methodological shortfalls that significantly limited confidence in their results. Subsequently, more rigorous research is needed in the future.
Data Sharing Statement
All data generated or analyzed during this study are included in this article and its supplementary material files. Further enquiries can be directed to the corresponding author.
Funding
This work was supported by the China–Australia International Research Centre for Chinese Medicine (CAIRCCM)—a joint initiative of RMIT University, Australia, and the Guangdong Provincial Academy of Chinese Medical Sciences, China. We also received additional funding from the National Key R&D Program of China [Grant No. 2019YFC1709802], Guangdong Provincial Hospital of Chinese Medicine [2019 General Program, Grant No. YN2019ML01 and 2019 Treating Potential Disease Program, YN2019ZWB01] and Traditional Chinese Medicine Bureau of Guangdong Province [2020 General Program, Grant No. 20202068].
Disclosure
The authors declare that there is no conflict of interest regarding the publication of this article.
References
1. Roberto CA, Swinburn B, Hawkes C, et al. Patchy progress on obesity prevention: emerging examples, entrenched barriers, and new thinking. Lancet. 2015;385(9985):2400–2409. doi:10.1016/S0140-6736(14)61744-X
2. Swinburn BA, Sacks G, Hall KD, et al. The global obesity pandemic: shaped by global drivers and local environments. Lancet. 2011;378:804–814. doi:10.1016/S0140-6736(11)60813-1
3. Ashkan A, Mohammad HF, Marissa BR, et al. Health effects of overweight and obesity in 195 countries over 25 years. N Engl J Med. 2017;377(1):13–27.
4. David W, Stephen K, Emanuele DA, et al. Separate and combined associations of body-mass index and abdominal adiposity with cardiovascular disease: collaborative analysis of 58 prospective studies. Lancet. 2011;377(9771):1085–1095. doi:10.1016/S0140-6736(11)60105-0
5. Lauby-Secretan B, Scoccianti C, Loomis D, Grosse Y, Bianchini F, Straif K. Body fatness and cancer–viewpoint of the IARC working group. N Engl J Med. 2016;375(8):794–798. doi:10.1056/NEJMsr1606602
6. Yumuk V, Tsigos C, Fried M, et al. European guidelines for obesity management in adults. Obes Facts. 2015;8(6):402–424. doi:10.1159/000442721
7. National Clinical Guideline Centre. Obesity: identification, assessment and management of overweight and obesity in children, young people and adults: partial update of CG43; 2014.
8. Timothy GW, Jeffrey IM, Elise MB, et al. American Association of Clinical Endocrinologists and American College of Endocrinology Comprehensive Clinical Practice Guidelines for medical care of patients with obesity. Endocr Pract. 2016;22(Suppl):3.
9. Daniel HB, LucF VG. Progress and challenges in anti-obesity pharmacotherapy. Lancet Diabetes Endocrinol. 2018;6:237–248.
10. Kishore MG, John WA, Hans-Rudolf B. Pharmacotherapy for patients with obesity. Clin Chem. 2018;64(1):118–129. doi:10.1373/clinchem.2017.272815
11. Qingyang S, Yang W, Qiukui H, et al. Pharmacotherapy for adults with overweight and obesity: a systematic review and network meta-analysis of randomised controlled trials; 2021.
12. Fujioka K, Harris SR. Barriers and solutions for prescribing obesity pharmacotherapy. Endocrinol Metab Clin North Am. 2020;49(2):303–314. doi:10.1016/j.ecl.2020.02.007
13. Timo DM, Matthias B, Tschp MH, Dimarchi RD. Anti-obesity drug discovery: advances and challenges. Nat Rev Drug Discov. 2021;21(3):201–223. doi:10.1038/s41573-021-00337-8
14. Yumei Z, Xiaochao L, Chenyang C, Deli L, Haiyan Z. Acupuncture versus sham acupuncture for simple obesity: a systematic review and meta-analysis. Postgrad Med J. 2020;96(1134):221–227.
15. Zhongliang S, Aiqun S, Shuangyan Q, Yan W, Xiaohui T. The clinical effect of electroacupuncture on simple obesity: a meta analysis. Diet Health. 2019;6(008):95–96.
16. Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. doi:10.1136/bmj.j4008
17. Whiting P, Savović J, Higgins JPT, et al. ROBIS: a new tool to assess risk of bias in systematic reviews was developed. J Clin Epidemiol. 2016;69:225–234. doi:10.1016/j.jclinepi.2015.06.005
18. Xia C, Wei H, Jie D, Xiaoling C, Lu C, Zhongyu Z. Effect of acupuncture therapy on simple obesity in adults: a meta-analysis. J Clin Acupunct Moxibustion. 2016;32(09):64–69.
19. William CC, Ching L, Haiyong C. Clinical efficacy of acupoint embedment in weight control: a systematic review and meta-analysis. Medicine. 2018;97(36):e12267. doi:10.1097/MD.0000000000012267
20. Mendona CRD, Dos Santos LSC, Noll M, Silveira EA, Arruda JT. Effects of auriculotherapy on weight and body mass index reduction in patients with overweight or obesity: systematic review and meta-analysis. Complement Ther Clin Pract. 2019;38:101069. doi:10.1016/j.ctcp.2019.101069
21. Sijia F, Miao W, Yiyuan Z, Shigao Z, Guang J. Acupuncture and lifestyle modification treatment for obesity: a meta-analysis. Am J Chin Med. 2017;45(02):239–254. doi:10.1142/S0192415X1750015X
22. Taipin G, Yulan R, Jun K, Shi J, Tianxiao S, Fanrong L. Acupoint catgut embedding for obesity: systematic review and meta-analysis. J Evid Based Complementary Altern Med. 2015;401914. doi: 10.1155/2015/401914
23. ChingFeng H, Suer G, Fanhao C. Auricular acupressure for overweight and obese individuals: a systematic review and meta-analysis. Medicine. 2019;98(26):e16144. doi:10.1097/MD.0000000000016144
24. Deping L. Meta-Analysis of Curative Effect on Acupuncture for Simple Obesity [Postgraduate]. Hubei University of Chinese Medicine; 2013.
25. Jianqiong L, Xiang S, Ying C, Lichang L, Shengxu W. Clinical randomized controlled trials of acupoint catgut-embedding for simple obesity: aMeta-analysis. Zhongguo Zhen Jiu. 2014;34(6):621–626.
26. Kangxiao L, Angela Weihong Y, Charlie X, George Binh L. Traditional Chinese manual acupuncture for management of obesity: a systematic review. World J Metaanal. 2015;3(5):206.
27. Qing L. Acupuncture for Simple Obesity a Systematic Review. Chengdu University of Chinese Medicine; 2014.
28. Xiaohan L. To Evaluate the Abdominal Acupuncture Treatment for Simple Obesity by Systematic Review. Chengdu University of Chinese Medicine; 2015.
29. Xiaomiao L, Bo L, Yuanhao D, Jun X, Pan S. Systematic evaluation of therapeutic effect of acupuncture for treatment of simple obesity. Zhongguo Zhen Jiu. 2009;29(10):856–860.
30. Namazi N, Khodamoradi K, Larijani B, Ayati MH. Is laser acupuncture an effective complementary therapy for obesity management? A systematic review of clinical trials. Acupunct Med. 2017;35:452–459. doi:10.1136/acupmed-2017-011401
31. Zhizhong R, Yi X, Jing L, Xue Z, Zhilan H, Can D. Auricular acupuncture for obesity: a systematic review and meta-analysis. Int J Clin Exp Med. 2016;9(2):1772–1779.
32. Jili S, Xiaoqing J, Jianfang Z, YidanC XL. The effectiveness of acupoint catgut embedding therapy for abdominal obesity: a systematic review and meta-analysis. Evid Based Complement Alternat Med. 2019;2019(8):1–12.
33. Sujie S. Meta-analysis on curative effectiveness of auricular application pressure treatment for childhood simple obesity. Gansu Med J. 2013;32(06):401–403.
34. Cho SH, Lee JS, Thabane L, Lee J. Acupuncture for obesity: a systematic review and meta-analysis. Int J Obes. 2009;33(2):183–196. doi:10.1038/ijo.2008.269
35. Kim SY, Shin IS, Park YJ. Effect of acupuncture and intervention types on weight loss: a systematic review and meta-analysis. Obes Rev. 2018;19(11):1585–1596. doi:10.1111/obr.12747
36. Lihua W, Wei H, Yanji Z, Guoping R, Kuang S, Zhongyu Z. Systematic review and meta-analysis on acupuncture for obesity complicated with type 2 diabetes mellitus. Chin Arch Trad Chin Med. 2018;36(8):1882–1888.
37. Dongqun X, Chunxiang S, Dongqin K, ShuJin Y. Effect of auricular pressure therapy for simple obesity in adult: a meta-analysis. Chin J Evid-Based Med. 2015;15(10):1182–1189.
38. Lili X, Yuan G, Qiuyu T, Weidong S. Effects of therapy of acupoint catgut embedding in the treatment of simple obesity: a meta-analysis. SH J TCM. 2017;51(S1):34–38.
39. Yanyan X. Acupuncture for Obesity: A Systematic Review [Postgraduate]. Chengdu University of Chinese Medicine; 2015.
40. Junpeng Y, Zhiqiong H, Ying C, Mingmin X, Ying L. Acupuncture and weight loss in Asians: a PRISMA-compliant systematic review and meta-analysis. Medicine. 2019;98(33):e16815. doi:10.1097/MD.0000000000016815
41. Lifan Y, Longjian H, Yan L, Jinghui Z. A clinical meta-analysis of treating simple obesity by acupuncture. Clin J Chin Med. 2015;7(31):1–4.
42. Sui Y, Zhao HL, Wong VCW, et al. A systematic review on use of Chinese medicine and acupuncture for treatment of obesity. Obes Rev. 2012;13(5):409–430. doi:10.1111/j.1467-789X.2011.00979.x
43. Tzulin Y, Hsinhao C, Tsungping P, et al. The effect of auricular acupoint stimulation in overweight and obese adults: a systematic review and meta-analysis of randomized controlled trials. Evid Based Complement Alternat Med. 2017;2017:1–16.
44. Zhi Y, Chuanghui J, Bin X, Jiadong W, Luoyan J. Systematic review of clinical randomized controlled trial of acupuncture for simple obesity. Shizhen Guo Yi Guo Yao. 2010;21(002):434–436.
45. Kepei Z, Shigao Z, Chunyan W, Hanchen X, Zhang L. Acupuncture on obesity: clinical evidence and possible neuroendocrine mechanisms. Evid Based Complement Alternat Med. 2018;2018:1–15.
46. Hong N, Mingjing Z, Yuwei J, Kaiyu X. Acupoint catgut embedding for the treatment of obese women with perimenopausal syndrome: a meta-analysis. Chin Med J. 2020;17(24):
47. Junjun P, Su F, Zhenyu Z. Effects of acupuncture therapy for simple obesity: a meta analysis. J Clin Acupunct Moxibustion. 2020;36(08):54–61.
48. Jianrong C, Dongping C, Qing R, et al. Acupuncture and related techniques for obesity and cardiovascular risk factors: a systematic review and meta-regression analysis. Acupunct Med. 2020;38(4):227–234. doi:10.1136/acupmed-2018-011646
49. Yanling G, Yi W, Jing Z, Zhihai H, Yin S. Effectiveness of electroacupuncture for simple obesity: a systematic review and meta-analysis of randomized controlled trials. Evid Based Complement Alternat Med. 2020;2020(1):1–14.
50. Lin Z, Shihua T, Yu Z, et al. Systematic review of body mass reduction by single acupuncture therapy. Hunan J Tradit Chin Med. 2015;13(12):6.
51. Yanji Z, Jia L, Guoyan M, et al. Acupuncture and related therapies for obesity: a network meta-analysis. Evid Based Complement Alternat Med. 2018;2018:1–20.
52. Rongqiang Z, Jiao T, Fengying L, Yonghong M, Lixin H, Xiaoli Y. Acupuncture for the treatment of obesity in adults: a systematic review and meta-analysis. Postgrad Med J. 2017;13:409–430.
53. Rongqiang Z, Lixin H, Jiao T, et al. Meta-analysis of randomized clinical trials about acupuncture treatment for female simple obesity. Zhi ye yu jian kang. 2017;18(7):813–818.
54. Lavrenova EA, Drapkina OM. Insulin resistance in obesity: pathogenesis and effects. Obe Metab. 2020;17(1):48–55. doi:10.14341/omet9759
55. Vettor R, Conci S. Obesity pathogenesis. In: Sbraccia P, Finer N, editors. Obesity. Endocrinology. Springer Cham; 2019. doi:10.1007/978-3-319-47685-8_14-12017
56. Mauro M, Taylor V, Wharton S, Sharma Arya M. Barriers to obesity treatment. Eur J Intern Med. 2008;19(3):173–180. doi:10.1016/j.ejim.2007.09.011
57. Neumark-Sztainer D, Hannan PJ. Weight-related behaviors among adolescent girls and boys: results from a national survey. Arch Pediatr Adolesc Med. 2000;154(6):569. doi:10.1001/archpedi.154.6.569
58. Pisetsky EM, Chao YM, Dierker LC, May AM, Striegel‐Moore RH. Disordered eating and substance use in high‐school students: results from the youth risk behavior surveillance system. Int J Eat Disord. 2010;41:464–470.
59. Clayton HB, Demissie Z, Lowry R, Lundeen EA, Sharma AJ, Bohm MK. Unhealthy weight management practices and non-medical use of prescription drugs. Am J Prev Med. 2016;52:215–219.
60. Jeffers AJ, Benotsch EG. Non-medical use of prescription stimulants for weight loss, disordered eating, and body image. Eat Behav. 2014;15(3):414–418. doi:10.1016/j.eatbeh.2014.04.019
61. Jeffers A, Benotsch EG, Koester S. Misuse of prescription stimulants for weight loss, psychosocial variables, and eating disordered behaviors. Appetite. 2013;65:8–13. doi:10.1016/j.appet.2013.01.008
62. Soong YS. The treatment of exogenous obesity employing auricular acupuncture. Am J Chin Med. 1975;3(03):285–287. doi:10.1142/S0192415X75000311
63. Belivani M, Dimitroula C, Katsiki N, Apostolopoulou M, Cummings M, Hatzitolios AI. Acupuncture in the treatment of obesity: a narrative review of the literature. Acupunct Med. 2013;31(1):88. doi:10.1136/acupmed-2012-010247
64. Liang F, Koya D. Acupuncture: is it effective for treatment of insulin resistance? Diabetes Obes Metab. 2010;12(7):555–569. doi:10.1111/j.1463-1326.2009.01192.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.