Back to Journals » Journal of Pain Research » Volume 19
Acupuncture for Postherpetic Neuralgia: An Evidence Mapping
Authors Li X, Xie J, Wu Y, Hou Y, Wang W ![]() , Li J
, Li J ![]() , Li J
, Li J ![]()
Received 25 February 2026
Accepted for publication 13 May 2026
Published 4 June 2026 Volume 2026:19 605247
DOI https://doi.org/10.2147/JPR.S605247
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Xinrong Li,1,* Jing Xie,1,* Yongshuang Wu,1,* Yuchao Hou,1 Wenjia Wang,1 Junxiong Li,2 Jing Li1
1Yueyang Hospital of Integrated Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China; 2Huadong Hospital, Fudan University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jing Li, Yueyang Hospital of Integrated Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China, Email [email protected]
Objective: This study is to systematically evaluate the efficacy of acupuncture for PHN and provide a visual overview of treatment landscape.
Methods: A systematic search was conducted in PubMed, Embase, Web of Science, China National Knowledge Infrastructure (CNKI), Chinese Scientific Journals Database (VIP), and Wanfang Database for systematic reviews (SRs) on acupuncture for PHN up to Apr 18, 2025. Studies were included if they were SRs of randomized controlled trials (RCTs) assessing traditional Chinese acupuncture interventions for PHN, and excluded if they involved non-traditional acupuncture, herpes zoster, or PHN prevention research. Two independent reviewers utilized Excel, EndNote 20, and R software for data analysis and assessed the quality of included studies using the AMSTAR2 tool.
Results: Of 351 identified records, 40 SRs met inclusion criteria, encompassing 926 RCTs, 63,493 patients, 13 types of acupuncture interventions and 29 outcomes. Acupuncture interventions, particularly fire needling, CPBLC, Fu’s subcutaneous needling, plum-blossom needle, multi-acupuncture and multi-acupuncture + pharmacotherapy, showed the most robust benefits in improving effective rate, reducing visual analog scale (VAS) scores, and decreasing adverse reactions in PHN treatment. Despite most SRs reporting positive outcomes, the quality was generally low by AMSTAR2.
Conclusion: Acupuncture could be a valuable adjunct to standard PHN treatment, offering benefits in overall efficacy, pain management and treatment safety. However, high-quality clinical trials and systematic reviews are needed to confirm these preliminary results and guide clinical practice.
Keywords: acupuncture, evidence mapping, postherpetic neuralgia
Introduction
Postherpetic neuralgia (PHN) is the most frequent chronic complication of herpes zoster, which is conventionally defined as dermatomal pain persisting at least 90 days after the appearance of the acute herpes zoster rash.1 The risk of developing PHN from herpes zoster ranges from 5% to 32% and increases with patients’ age.2 PHN seriously affects patients in many ways. The pain is often intolerable and its duration varies widely, and in severe cases, it can last for years.3 In addition, more than half of PHN patients have psychological and physical problems, including anxiety, depression and poor sleep.4–7 Since the pathogenesis of PHN is still unclear, symptomatic treatments are mostly used to relieve pain, and drug efficacy can be limited by adverse effects and tolerated doses.8
As a treasure of traditional Chinese medicine (TCM), the analgesic effect of acupuncture has been confirmed by a variety of studies, and its efficacy on neuropathic pain is particularly significant.9,10 Previously, due to the lack of sufficient clinical research data, the analgesic benefit of acupuncture for PHN was once questioned.11 As acupuncture for PHN has garnered increasing attention, a substantial number of randomized clinical trials (RCTs), systematic reviews (SRs), and meta-analyses have been published to highlight its benefits. In the treatment of PHN, acupuncture has been demonstrated to be effective in analgesia and in relieving negative emotions with almost no adverse effects. It is worth noting that acupuncture consists of a broad range of interventions, including fire needle, electroacupuncture, bloodletting with cupping, moxibustion, etc.12–15 However, the existing SRs, though abundant, are always focused on specific interventions and lack cohesion in demonstrating the comprehensive advantages of acupuncture in treating PHN.
To fill this gap, we developed an evidence map in this study. As a relatively new methodology, evidence mapping offers an overview of the quantity, characteristics, and outcomes of related research broadly, unlike systematic reviews that typically concentrate on more confined research areas.16 We collected studies of specific types of acupuncture interventions, outlined their general information, assessed the effectiveness, evaluated the quality of supporting evidence, conducted in-depth analysis of the top three outcomes, and finally provided a user-friendly visual presentation. This evidence mapping would assist policymakers in interpreting current evidence and facilitating decision-making processes.
Method
Search Strategy
Two reviewers (XRL and JX) have systematically searched the following electronic databases: PubMed, Embase, Web of Science, China National Knowledge Infrastructure (CNKI), Chinese Scientific Journals Database (VIP), and Wanfang Databases, with date range from their inceptions to Apr 18, 2025, and without language restrictions. The two reviewers identified data on different sources before combining the results. A prior investigation about the current traditional acupuncture intervention in PHN was conducted, and specific treatments were added into the general idea of acupuncture.17,18 The search strategy was developed with the assistance of experts and included three search terms: “postherpetic neuralgia”, “acupuncture” and “meta-analysis” (detailed search strategies are reported in Supplementary Material 1).
Inclusion and Exclusion Criteria
Studies meeting the following criteria were included: (a) the study was a SR and meta-analysis of RCTs; (b) participants had been diagnosed with PHN defined by the American Academy of Family Physicians as dermatomal pain persisting for 30 days or pain persisting for 90 days after rash onset.19 No specific restrictions were imposed regarding age, gender, stages, complications, or previous treatments; (c) the experimental group of patients had to be given traditional Chinese acupuncture interventions, including but not limited to fire needle, electroacupuncture, bloodletting with cupping and moxibustion. The control group in the included RCTs could be conventional treatment, or placebo, or no treatment. There were no limitations on outcomes.
Studies meeting the following criteria were excluded: (a) the experimental group of patients were given non-traditional acupuncture interventions such as pharmaco-acupuncture, acupotomy, dry needling and acupoint injections; (b) studies including human immunodeficiency virus-associated herpes zoster; (c) studies whose aims were to reduce the risk of PHN; (d) studies from which data could not be extracted; (e) duplicate studies.
Study Selection and Data Extraction
Duplicate records were removed by literature management software (EndNote 20) or manually. Two independent reviewers (XRL and YSW) then selected studies according to the inclusion and exclusion criteria. The titles and abstracts of the extracted articles were skimmed for preliminary inclusion consideration. After excluding the irrelevant articles, a subsequent full-text screen was performed to remove other irrelevant studies. Disagreements between reviewers were firstly resolved by discussion, and an additional reviewer (JL) was consulted when necessary.
A data extraction form, including authors, patients, country, number of RCTs, study design, quality tools, intervention(s), controls or comparator(s) and outcomes, was built to keep a record of the main characteristics of included SRs. For studies conducting multiple meta-analyses, data extraction was performed by the unit of different interventions. Two authors (XRL and YSW) independently extracted and verified all data. The management and citation of references were facilitated by EndNote 20 software. The conclusions were divided into four categories: “harmful”, “no effect”, “potentially beneficial”, and “beneficial”. “Harmful”, “no effect”, and “beneficial” were directly extracted from the conclusions, while “potentially beneficial” was listed when the conclusions did not assert firm benefits, despite the positive effects reported in the results.
Methodological Quality Assessment
For the included literature, we used the Assessing the Methodological Quality of Systematic Reviews 2 (AMSTAR2) tool for comprehensively and critically appraising the included SRs. Based on the validated 16-item checklist, we assessed the SRs by using ratings of “affirmative”, “partially affirmative”, or “negative”. The overall confidence in the outcome of the review was rated as follows: “high” for no or one non-critical weakness, “moderate” for more than one non-critical weakness, “low” for one critical flaw with or without non-critical weaknesses, and “critically low” for more than one critical flaw with or without non-critical weaknesses. Similarly, the rating was performed independently by two reviewers (XRL and JX), while a third reviewer (JL) monitored the entire process.20
Data Synthesis and Evidence Map Presentation
For the purpose of quantitative description and graphical illustration, line graphs and bubble plots were employed using Microsoft Excel 2019 and the R package ggplot2. The line graphs represented trends in the year of publication of papers related to acupuncture for PHN. Specifically, the Y-axis showed the number of publications, the X-axis showed the year, and the colors represented different languages used in the papers. Two distinct types of bubble plots were developed to provide a thorough overview of the diverse acupuncture interventions and their effects on the most pertinent outcomes.
The first type of bubble plot aimed to observe the distribution of evidence and to summarize the interventions, outcomes, quantity and effectiveness of studies using acupuncture for the treatment of PHN. The categorization was based on meta-analysis topics. Bubbles, in this plot, represented the associations between various interventions and outcome types. The bubble size represented the number of included SRs, and the bubble color represented the effectiveness of studies indicating the validity of TCM. The interventions were organized in columns and correlated with different outcomes arranged in rows. Studies with more than one intervention and one outcome could be mapped across multiple cells within the evidence map.
The second type of bubble plot offered separate information on chosen outcomes. The effective rate and VAS score were set as primary outcomes, representing the effectiveness of acupuncture. Adverse reactions, refers specifically to pharmacotherapy-related side effects (eg, gastrointestinal discomfort, neurological symptoms) that are reduced when acupuncture is used, were set as secondary outcomes representing the safety of acupuncture in treating PHN. In these plots, bubbles indicated the sum of studies on a particular intervention, or if there are multiple studies on the same topic, of the same quality, and with the same effect, the bubbles reflected the sum of the characteristics of those studies. The position of each bubble was determined by two dimensions: the AMSTAR2 quality along the rows, and the effect along the columns. Additionally, the labels on these bubbles abbreviated the topics of each SRs, using initials derived from acupuncture names, while their size corresponded to the number of RCTs included.
Sensitivity Analysis
To assess whether the inclusion of “critically-low” quality SRs biased our overall conclusions, we conducted a methodological sensitivity analysis. Specifically, we compared the findings from the full set of included SRs (n = 40) with restricted results that excluded “critically-low” quality SRs according to the AMSTAR2 criteria. The comparison focused on three core outcomes: effective rate, VAS score, and adverse reactions. The consistency of direction and magnitude of reported benefits was qualitatively assessed between the two sets.
Result
Study Sample and Design Characteristics
The data encompasses a total of 40 SRs,21–60 which together include 926 RCTs and involve 63,493 participants. The PRISMA flow diagram in Figure 1 provides a summary of how these studies were selected. During the screening process, all studies that did not meet the inclusion criteria were excluded (the specific reasons for exclusion are detailed in Supplementary Table 1). Due to multiple meta-analyses conducted by some studies,44,48,49 we managed to extract 43 meta-analyses from the 40 SRs, covering 13 distinct acupuncture intervention types. Among these, four meta-analyses focused on fire needling, three on collateral-pricking and bloodletting cupping, two on Fu’s subcutaneous needling, and two on moxibustion. And if we also consider studies where multi-acupuncture was used either alone or in combination with moxibustion or pharmacotherapy, we found that a total of 26 articles employed multi-acupuncture. With one exception, which did not place restrictions on the control group,24 all studies compared acupuncture therapy to pharmacotherapy, either alone or in combination with other treatments. The outcomes of SRs were categorized into three main types, with the first being survival-related outcomes, including cure rate, effective rate, recovery rate, recurrence rate, response rate and adverse reactions; the second being symptoms-related outcomes, including clinical symptom score, DLQI score, QoL score, SF-36 score, PSQI score, QoS score, SQS score, ADPS score, global impression, Mc Gill score, NRS score, pain relief time, SF-MPQ score, VAS score, VPS score, pain areas, anxiety score, HAMA score, SAS score, HAMD score, SDS score and drug score; the third being lab tests, including the level of substance P.
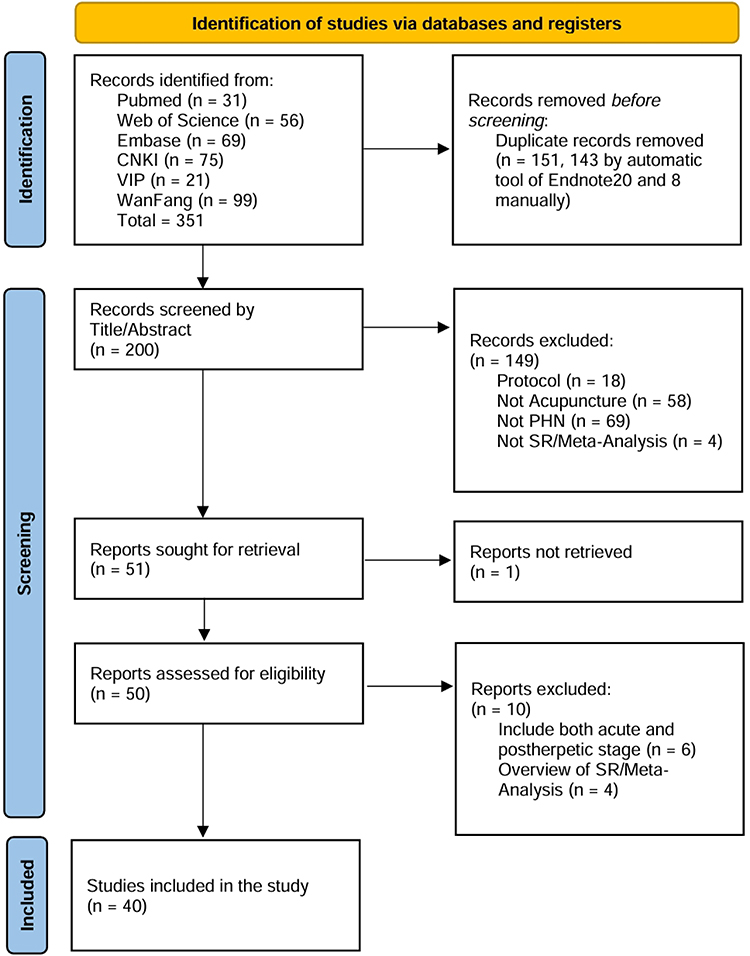 |
Figure 1 Flow diagram of the study selection process. A total of 351 records were identified from six databases. After removing 151 duplicates, 200 records were screened by title and abstract, and 51 related articles were assessed for eligibility. Finally, 40 systematic reviews and meta-analyses were included in the evidence mapping. |
Trends in the Year of Publication
Between December 2008 and April 2025, a total of 40 SRs on acupuncture for PHN were documented, showing a continued interest in both domestic and international academia. Notably, Chinese literature significantly outnumbered English literature, which reflected the regionalized feature of acupuncture research and the limitations of its international dissemination. The years 2022 and 2023 witnessed a peak in the publication of studies in Chinese and English. Approximately two-thirds of the included SRs were published within the past five years, indicating a growing clinical research focus on acupuncture for PHN. Therefore, the current period presents an opportunity for conducting a systematic synthesis of the existing evidence to consolidate findings and guide future clinical directions. The annual number of publications is clearly depicted in Figure 2.
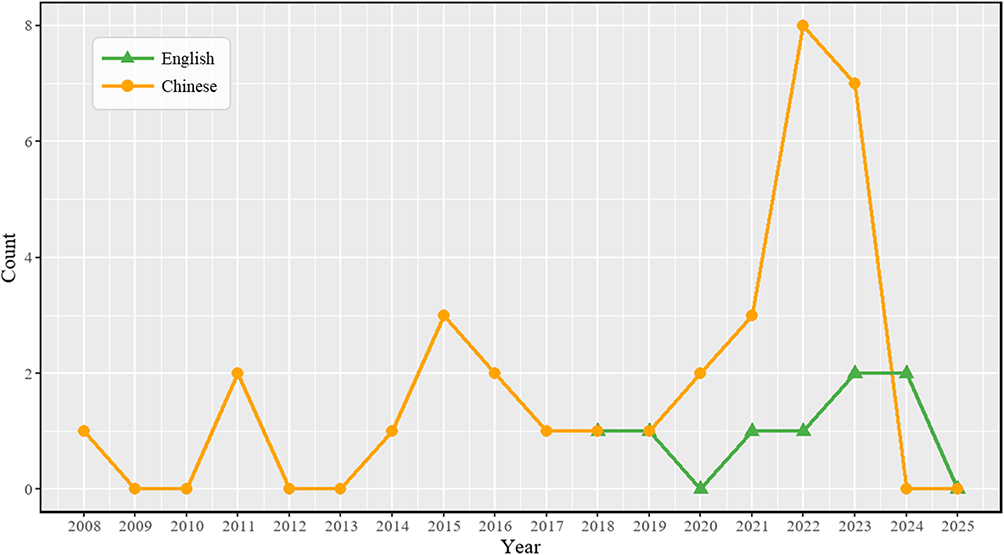 |
Figure 2 Trends in the year of publication. Publication volumes are shown separately for English and Chinese literature by year. |
Quality of Systematic Reviews
Upon reviewing the quality assessments, we observed significant shortcomings in two critical domains: protocol registered before commencement of the review (item two) and justification for excluding individual studies (item 7) (detailed ratings for included studies are reported in Supplementary Table 2). Over 85% of the included SRs failed to address these two items adequately. This highlighted systemic gaps in acupuncture research methods, driven by insufficient standardization and mandatory pre-publication checks in Chinese journals. To address this, researchers should pre-register protocols and detail exclusion criteria under PRISMA guidelines; editors should enforce checklist and registration requirements. These measures will improve reproducibility and strengthen global clinical relevance of PHN acupuncture studies.
These omissions rendered most SRs “critically low” quality in terms of meeting the AMSTAR2 criteria, 6 SRs were rated “low” and 34 SRs were deemed “critically low”, overshadowing other methodological strengths and diminishing the discriminative power of the assessment framework. We retained the original AMSTAR2 algorithm and supplemented it with a sensitivity analysis to ensure the reliability of the conclusions.
Across all items, adequacy of the literature search (40/40), detailed description of included studies (37/40), risk of bias assessment from individual studies (40/40), appropriateness of meta-analytical methods (38/40), consideration of the risk of bias when interpreting the results of the review (35/40) were mostly reported. In contrast, the items of protocol registered before commencement of the review (6/40), explanation of the study designs for inclusion (0/40), justification for excluding individual studies (1/40) and potential sources of conflict of interest (8/40) have yet to be improved. Figure 3 presents the AMSTAR2 standardized domain scores for each SR, along with their overall assessments.
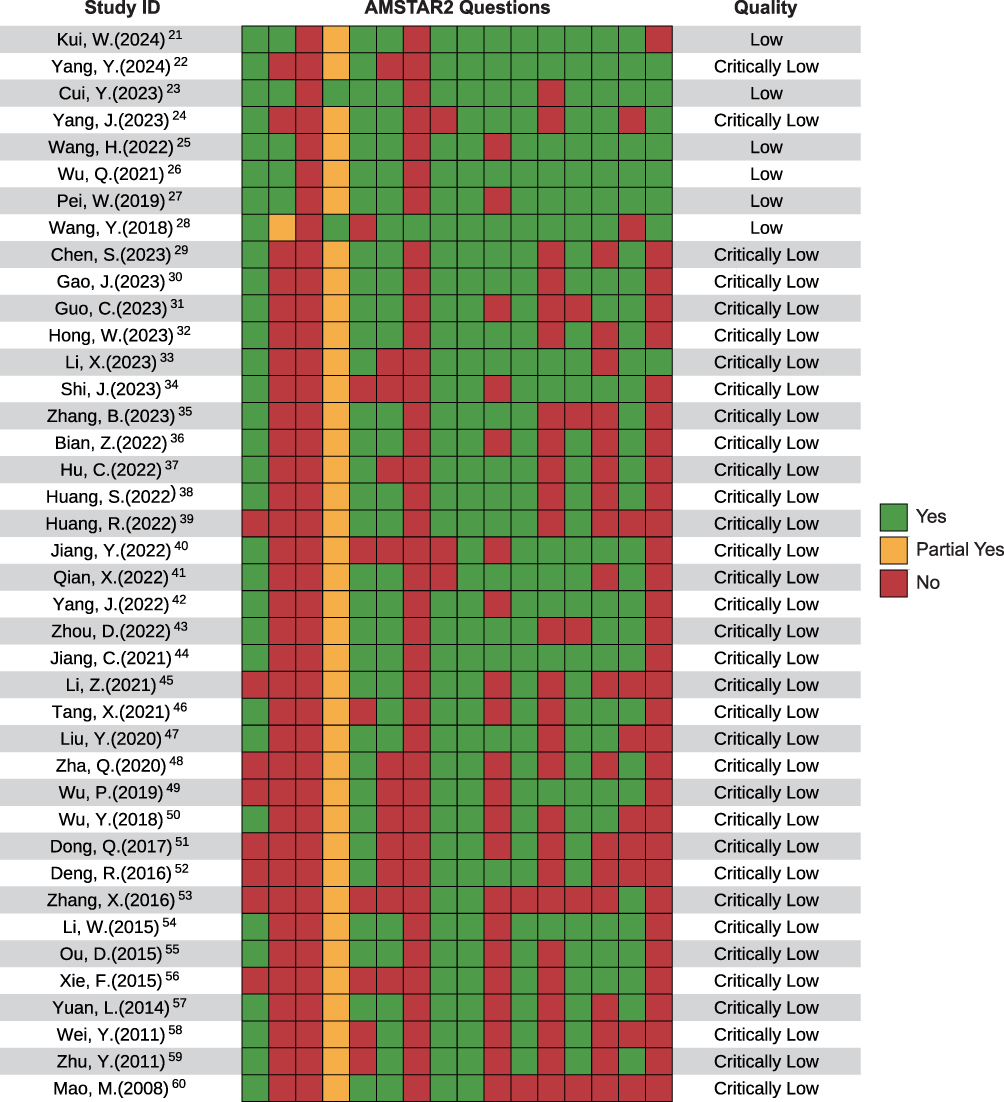 |
Figure 3 Quality of systematic reviews. AMSTAR2 was used to appraise the reporting quality of each included SR critically. Each question was answered with “Y”: Yes; “PY”: partial yes; or “N”: no. Questions: 1. PICO component? 2. Methods pre-set? Deviations justified? 3. Study designs explained? 4. Comprehensive search conducted? 5. Performed study selection duplicated? 6. Performed data extraction duplicated? 7. Exclusions listed and justified? 8. Studies described in detail? 9. The risk of bias (RoB) assessed satisfactorily? 10. Funding sources reported? 11. Meta-analysis methods appropriate? 12. RoB impact on meta-analysis assessed? 13. RoB considered in results? 14. Heterogeneity explained and discussed? 15. Publication bias investigated? 16. Conflicts of interest reported, including funding? The overall confidence of each SR was graded as “high”, “moderate”, “low” or “critically low”. |
Intervention Components Described in Included Systematic Reviews
Based on our comprehensive search, we identified a total of 8 different acupuncture interventions utilized in the treatment of PHN, including electroacupuncture (EA), collateral-pricking and bloodletting cupping (CPBLC), plum-blossom needle, fire needle, floating implantation, Fu’s subcutaneous needling, moxibustion and Jiaji points with surrounding needling. When considering studies that used multiple interventions, we compiled a total of 13 treatment strategies. Specifically, EA, CPBLC, fire needling, moxibustion, multi-acupuncture, and multi-acupuncture with pharmacotherapy were highlighted in more than three systematic reviews.
Evidence Map
The evidence map presented in Figure 4 provides a comprehensive overview of acupuncture’s application in PHN treatment studies, highlighting the potential effectiveness of each intervention for specific outcomes. For instance, multi-acupuncture strategies were evaluated in 19 SRs, of which 14 reported outcomes related to the effective rate. Among these 14 SRs, 12 demonstrated beneficial effects and 2 suggested potential beneficial effects. This corresponds to an 92.86% effective rate for multi-acupuncture in PHN management. Detailed information on these reviews is available in Table 1.
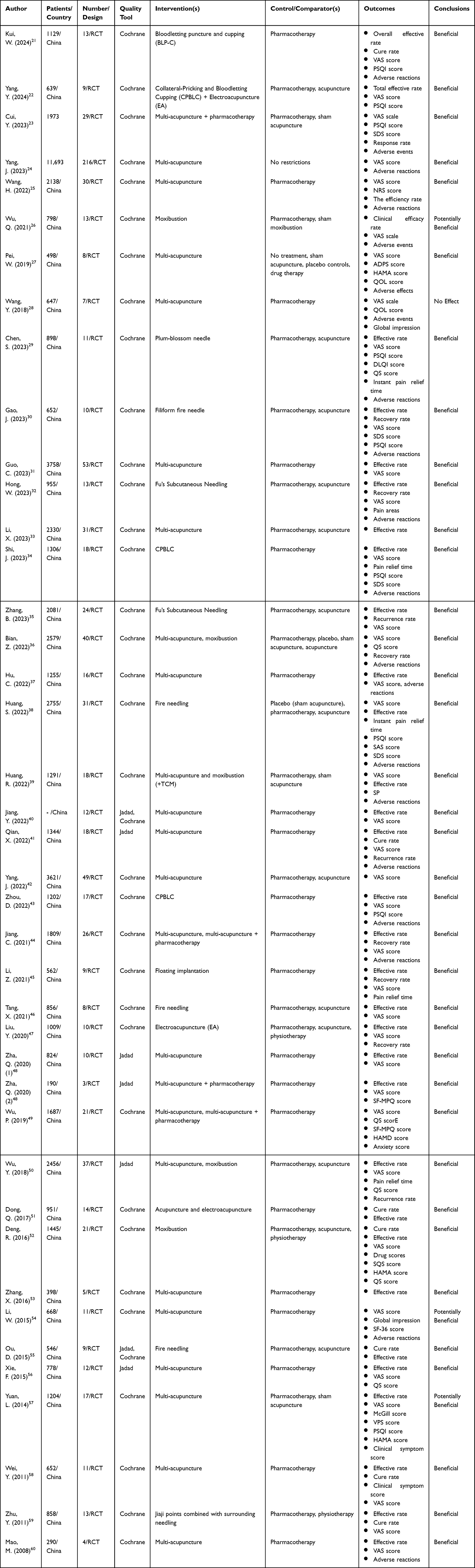 |
Table 1 Summary of Systematic Reviews or Meta-Analysis on Acupuncture for Postherpetic Neuralgia |
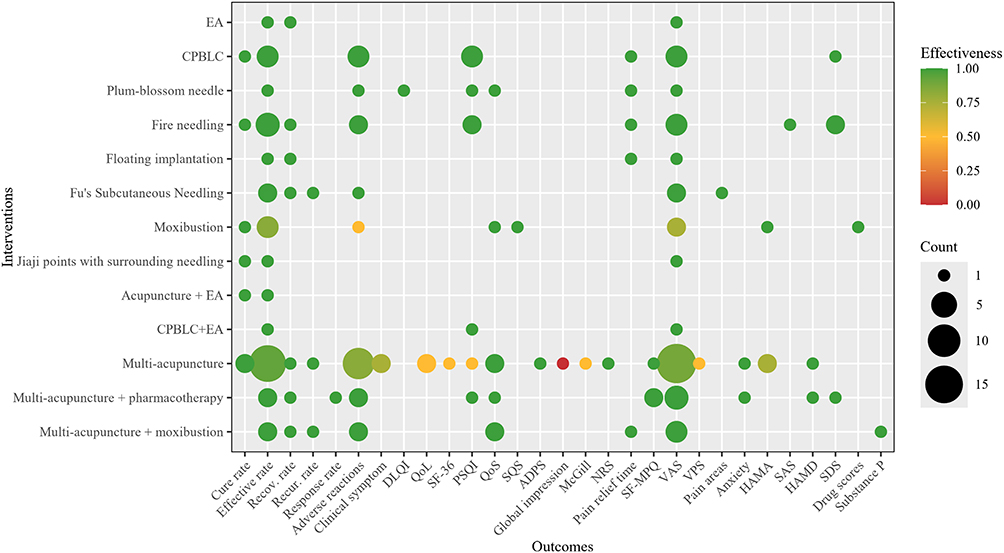 |
Figure 4 Evidence map of the identified acupuncture interventions to the outcomes of PHN. X-axis: outcomes divided into three sections (cure rate to adverse reactions: survival; clinical symptom score to drug scores: symptoms; substance P: lab tests). Y-axis: acupuncture interventions. (singular treatment: EA to Jiaji points with surrounding needling; composite treatment: acupuncture + EA to multi-acupuncture + moxibustion). Color: a gradient color scale is used, when green bubbles indicate that the systematic reviews identified on the topic demonstrated a beneficial or probably beneficial effect on the corresponding outcomes, while red bubbles indicate the opposite. Bubble size: the number of SRs and meta-analysis conducted on the topic. |
Out of all outcomes, 18 reported consistently positive results (100% beneficial), including cure rate, recovery rate, recurrence rate, response rate, DLQI score, QoS score, SQS score, ADPS score, NRS score, pain relief time, SF-MPQ score, pain areas, anxiety score, SAS score, HAMD score, SDS score, drug scores and substance P. Five outcomes reported mostly positive results (more than 80%), including effective rate, adverse reactions, PSQI score, VAS score and HAMA score. Five outcomes, clinical symptom, QoL score, SF-36 score, McGill score and VPS score, reported positive results in more than half of their cases. Meanwhile, one outcome showed contractive results, with more than half of ineffective results were reported in global impression.
The evidence map also reveals that effective rate, VAS score, and adverse reactions are mostly concerned, each involving more than 50% types of interventions. Effective rate is designated as the primary outcome, representing overall effectiveness; and VAS score and adverse reactions are considered secondary outcomes, representing acupuncture’s analgesic efficacy and safety, respectively. Based on these selected outcomes, further research led to the generation of three additional bubble plots.
Effective Rate
The evidence map of the latest SRs involving effective rate in Figure 5 focused on 13 distinct interventions. Out of the 40 SRs we reviewed, 36 supplied data related to effective rate. A significant majority, comprising 33 SRs (91.7%), indicated that the acupuncture interventions were beneficial in enhancing effective rate. However, a smaller subset of three SRs (8.3%) suggested that the impact might not be as substantial. Of these 36 SRs, four was assessed as low quality, and 32 as critically low quality. The “2.5 Data synthesis and evidence map presentation” section describes how each bubble in the evidence map was plotted, considering the number of RCTs included (which determines bubble size), the effectiveness (placed along the X-axis), and the overall confidence level (represented on the Y-axis).
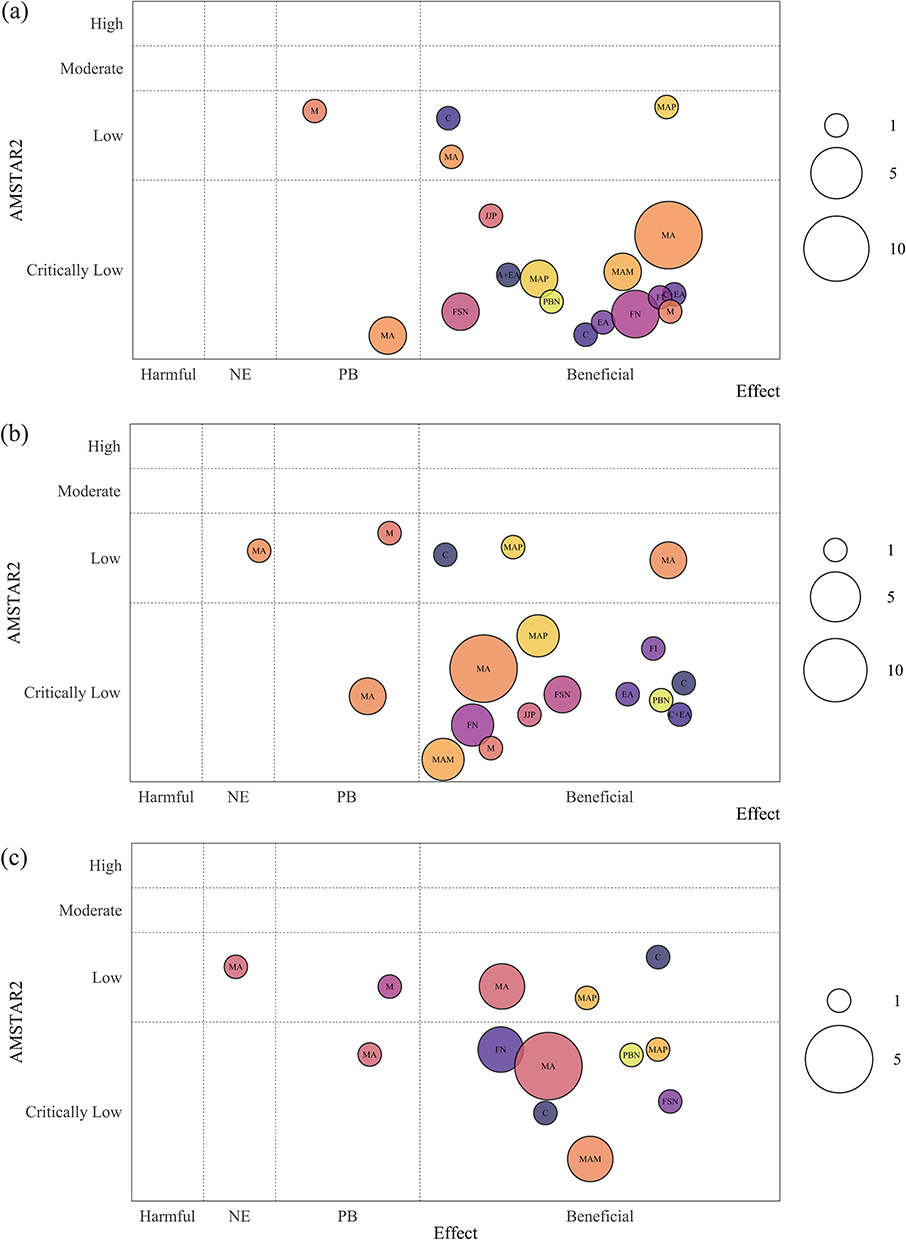 |
Figure 5 Evidence Map of the latest SRs involving (a) effective rate, (b) VAS score, (c) adverse reactions. X-axis: effectiveness of each acupuncture intervention; Y-axis: Overall confidence assessed by AMSTAR2. Bubble size: the number of studies included for each specific intervention (small circle = 1 study, medium circle = 5 studies, large circle = 10 studies). Each distinct circle color denotes a unique intervention. Abbreviations: A, acupuncture; C, CPBLC; EA, electroacupuncture; FI, floating implantation; FN, fire needling; FSN, Fu’s subcutaneous needling; JJP, Jiaji points with surrounding needling; M, moxibustion; MA, multi-acupuncture; MAM, multi-acupuncture + moxibustion; MAP, multi-acupuncture + pharmacotherapy; PBN, plum-blossom needle. |
Combining the number of RCTs, effectiveness, and the overall confidence, multi-acupuncture, fire needling, multi-acupuncture + pharmacotherapy, CPBLC, Fu’s subcutaneous needling, Jiaji points with surrounding needling, plum-blossom needle, and CPBLC + EA achieve more reliable effective rate in the treatment of PHN.
VAS Score
The evidence map of the latest SRs involving VAS score in Figure 5 focused on 12 distinct interventions. Out of the 40 SRs we reviewed, 39 supplied data related to VAS score. A vast majority of 35 SRs (89.7%) demonstrated that the relevant acupuncture interventions were beneficial in reducing the VAS score, while three SRs (7.7%) suggested that the effect of the interventions might not be as significant, and one SR (2.6%) indicated that acupuncture had no effect in improving VAS score. Of these 39 SRs, six was assessed as low quality, and 33 as critically low quality.
Combining the number of RCTs, effectiveness, and the overall confidence, multi-acupuncture, multi-acupuncture + pharmacotherapy, fire needling, CPBLC, Fu’s subcutaneous needling, Jiaji points with surrounding needling, multi-acupuncture +moxibustion, plum-blossom needle and CPBLC + EA could be more beneficial in improving VAS score compared to other interventions.
Adverse Reactions
The evidence map of the latest SRs involving adverse reactions in Figure 5 focused on 8 distinct interventions. Out of the 40 SRs we reviewed, 21 supplied data related to adverse reactions. Notably, 18 SRs (85.7%) demonstrated that the relevant acupuncture interventions were beneficial in reducing adverse reactions, and two SRs (9.5%) suggested that relevant acupuncture interventions may not be as significant in reducing adverse reactions. Conversely, only one SRs (4.8%) suggested that the effect might not be as dramatic. Of these 21 SRs, six was assessed as low quality, and 15 as critically low quality.
Combining the number of RCTs, effectiveness, and the overall confidence, multi-acupuncture, multi-acupuncture + pharmacotherapy, fire needling, CPBLC, Fu’s subcutaneous needling, multi-acupuncture +moxibustion, and plum-blossom needle could be more beneficial in alleviating adverse reactions compared to other interventions.
Sensitivity Analysis Results
Among all included SRs, the AMSTAR2 identified six SRs as “low” quality and 34 as “critically-low” quality. After excluding the 34 “critically low” quality SRs, the restricted subset comprised six SRs. When comparing the restricted subset with the full set, the overall conclusions remained unchanged.
Out of the six SRs we reviewed, four supplied data related to effective rate. Three SRs (75%) indicated that the acupuncture interventions were beneficial in enhancing effective rate, while one SR (25%) suggested that the impact might not be as substantial. All six SRs supplied data related to VAS score. A vast majority of four SRs (66.7%) demonstrated that the relevant acupuncture interventions were beneficial in reducing the VAS score, while one SR (16.7%) suggested that the effect of the interventions might not be as significant, and one SR (16.7%) indicated that acupuncture had no effect in improving VAS score. All six SRs supplied data related to adverse reactions. Similarly, four SRs (66.7%) demonstrated that the relevant acupuncture interventions were beneficial in reducing adverse reactions, one SR (16.7%) suggested that relevant acupuncture interventions may not be as significant in reducing adverse reactions, and one SR (16.7%) suggested that the effect might not be as dramatic.
Acupuncture interventions consistently demonstrated beneficial effects on improving effective rate, reducing VAS score, and decreasing adverse reactions in PHN treatment. No instance occurred where a beneficial effect reported in the full analysis became “harmful” in the restricted analysis. The result suggested that the inclusion of “critically low” quality SRs did not materially alter the direction of the evidence map.
Discussion
Summary of Findings
PHN is a common and refractory neuropathic pain following herpes zoster. Conventional pharmacotherapy often demonstrates side effects in managing PHN, leaving many patients enduring adverse events despite adherence to standardized medication regimens, which compromises patients’ quality of life.61,62 With the rapid growth of clinical studies on acupuncture and related therapies for PHN, the number of SRs and meta-analyses in this field has also surged. However, these studies focused on different aspects, involving different acupuncture methods, different outcomes and heterogeneous conclusions, which led to ambiguity in clinical decision-making regarding treatment options. As a result, the evidence map developed in this study systematically synthesized the distribution patterns and contentious issues of research in this domain, providing clinicians with a visual reference framework and enhancing the efficiency and precision of evidence retrieval and application.
This evidence map of acupuncture treating PHN was based on 40 published SRs and meta-analyses conducted between 2008 and 2025. This study identified 13 types of acupuncture interventions, including but not limited to fire needle, electroacupuncture, and other various traditional Chinese medicine acupuncture methods as well as combinations of single methods. The evidence underscored that acupuncture therapies, either as monotherapy or in combination with conventional interventions, demonstrate significant efficacy in PHN treatment, effectively alleviating pain and reducing adverse reactions of pharmacotherapy. Among various acupuncture interventions, fire needling, CPBLC, Fu’s subcutaneous needling, plum-blossom needle, multi-acupuncture and multi-acupuncture + pharmacotherapy showed the most robust evidence bases, supported by large sample sizes and consistent clinical outcomes, thus warranting prioritization as preferred complementary and alternative treatment options for PHN. As for global impression, the only indicator of poor efficacy found by the evidence mapping, is most likely the result of the small sample size involved (only one article was involved). This may be due to the fact that the current evidence comes from a limited number of existing studies, and future research should focus on conducting new trials with larger sample sizes to obtain more reliable results.
Early Acupuncture for PHN Prevention
Notably, literature excluded due to methodological limitations consistently revealed that interventions during acute herpes zoster may significantly reduce the incidence of PHN.63–68 This observation aligns with the classical Huangdi Neijing principle of “preventive treatment” (zhi wei bing), suggesting that early intervention may surpass post-PHN therapies in clinical efficacy. Early acupuncture is worth considering as an adjunctive strategy during the active herpes zoster phase. Mechanistic insights indicate that acupuncture can activate autonomic nerve pathways to regulate systemic inflammation, thereby impeding the acute-to-chronic pain transition.69 While acupuncture has demonstrated efficacy in managing PHN, reorienting the focus to its preventive application during active infection could optimize clinical outcomes and reduce long-term patient suffering.
However, rigorous scientific validation of this preventive effect would require a different research framework. Specifically, future research should include prospective cohort studies or well-designed RCTs that compare acute herpes zoster patients receiving early acupuncture versus standard care alone with long-term follow-up. We acknowledge this as an important future direction and welcome further discussions and collaborative efforts.
Advancement Beyond Previous Studies
Although previous network meta-analyses have evaluated multiple acupuncture interventions for PHN,17,18,70,71 we undertook evidence mapping instead of network meta-analysis for two fundamental advancements. First, network meta-analyses often focused on specific interventions, potentially omitting important acupuncture techniques. Second, they may lack a comprehensive literature search, missing studies that could provide crucial insights.
Unlike traditional systematic reviews or network meta-analyses that typically focus on specific interventions or require homogeneous effect sizes for quantitative synthesis, evidence mapping provides a broad, visual overview of the existing literature without synthesizing effect sizes. This approach is particularly suitable for traditional Chinese medicine, where interventions vary substantially in technique, frequency, and duration. Evidence mapping allows us to identify evidence clusters, gaps, and patterns across diverse interventions and outcomes, offering a valuable methodological alternative for fields with high clinical heterogeneity.
Despite these differences, both evidence mapping and network meta-analysis share a common focus on multiple interventions for the same disease and rely on a systematic review of existing studies. And evidence mapping offers a broader perspective, providing a more comprehensive overview of the evidence base and highlighting gaps in knowledge.
To date, despite the utilization of evidence mapping in various branches of traditional Chinese medicine, a comprehensive exploration of acupuncture’s role in treating PHN remains absent. Our approach offers three distinct strengths: (1) Categorization of outcomes into interpretable domains; (2) Mitigation of RCT overlap through prioritization of recent systematic reviews; (3) Multidimensional quality assessment using AMSTAR-2 to highlight methodological limitations. Our evidence map synthesizes key recommendations while visually presenting concordance and discordance across studies, directly informing clinical decision-making and future research prioritization.
Limitations
First, AMSTAR-2 assessment revealed that most included SRs demonstrated critically low methodological quality, primarily due to unregistered protocols and inadequate reporting of study exclusions. However, these reviews performed well in other critical domains: comprehensive literature searching, detailed study characteristics reporting, rigorous risk of bias assessment, appropriate meta-analytic methods, and consideration of bias in interpretation. Given the need for data comprehensiveness and the scarcity of high-quality studies, we included all of the literature that met the inclusion criteria, which may introduce bias. To mitigate potential bias, we explicitly annotated methodological deficiencies in Figure 3 and conducted a methodological sensitivity analysis, which confirmed that the direction of the main conclusions remained unchanged. However, the overall evidence base still requires methodological improvement.
Second, as an evidence map, we provided a broad overview of acupuncture interventions for PHN but did not quantitatively compare treatment efficacy, which might not align with the needs of stakeholders seeking specific, better therapies for PHN patients.
Third, there was substantial heterogeneity in both acupuncture methods (eg, retention time, stimulation intensity, session frequency) and inclusion criteria (30 days vs. 90 days definition of persistent pain). This inconsistency in diagnostic criteria might lead to variations in baseline pain duration and pain severity, which could in turn affect the estimated treatment effects. These factors prevented the standardization of treatment protocols. We could only cluster similar interventions into broad categories without specifying operational parameters, posing challenges for clinical replication. Moreover, we grouped 26 studies under the broad term “multi-acupuncture” due to the use of multiple techniques in a single study. This approach might mask the differential effectiveness of specific technique combinations. Future network meta-analyses could address this limitation by using well-defined and distinct intervention nodes.
Fourth, reliance on secondary data (SRs/MAs) inherits publication and outcome reporting biases from the source literature. Future research should address these limitations by conducting high-quality primary RCTs with standardized protocols and reporting.
Furthermore, due to linguistic constraints and an insufficient search strategy, the retrieval of identified research might not be completed. Finally, reliance on secondary data (SRs/MAs) rather than primary trials inherits publication and outcome reporting biases from the source literature, constraining the robustness of our conclusions.
Conclusion
The therapeutic landscape for PHN remains challenging due to the limited efficacy of conventional pharmacotherapy in pain management, quality of life improvement, and adverse reactions prevention. This evidence map synthesizes two decades of research evidence, providing an intuitive summary of the key findings from acupuncture interventions for PHN, and confirms the clinical value of acupuncture: as an independent or adjunctive therapy, it significantly reduces pain intensity, alleviates neuropathic sequelae such as anxiety, depression, and sleep disorders, and reduces adverse reactions compared to conventional pharmacological treatments.
Crucially, interventions like fire needling, CPBLC, Fu’s subcutaneous needling, plum-blossom needle, multi-acupuncture and multi-acupuncture with pharmacotherapy demonstrate the most consistent efficacy, validated through large-scale trials. While methodological limitations preclude definitive quantitative synthesis, this visual knowledge framework empowers policymakers to rapidly identify evidence-based interventions, optimize clinical pathways, and prioritize future research—particularly high-quality RCTs standardizing acupuncture parameters via STRICTA guidelines. Ultimately, integrating these evidence-informed approaches may transform PHN management paradigms where pharmacological options fall short.
Data Sharing Statement
Additional supporting information can be found online in the Supporting Information section.
Acknowledgments
We would like to thank Jing Li for advice on experimental design. We are very grateful to the support of the Department of Acupuncture and Moxibustion at Yueyang Hospital of Integrated Chinese and Western Medicine, Shanghai University of Traditional Chinese Medicine on this article, as well as Huadong Hospital, Fudan University. Funding from Shanghai Municipal Health Commission, Shanghai Municipal Administrator of Traditional Chinese Medicine and National Administration of Traditional Chinese Medicine is gratefully acknowledged.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by: 1. Shanghai Municipal Science and Technology Commission - Clinical Efficacy Evaluation and Inflammatory Factor Markers Exploration of Electroacupuncture for Preventing and Treating Perioperative Neurocognitive Disorders (23Y11922000); 2. Shanghai Municipal Science and Technology Commission - A Multicenter, Bidirectional Cohort Study on Transcutaneous Electrical Acupoint Stimulation for Moderate to Severe Cancer Pain in Liver Cancer (202440158); 3.Special Project for the Inheritance and Development of Acupuncture Schools (HKGYQYXM-2026-54).
Disclosure
All authors report no conflicts of interest in this work.
References
1. Johnson RW, Rice AS. Clinical practice. Postherpetic neuralgia. N Engl J Med. 2014;371(16):1526–18. doi:10.1056/NEJMcp1403062
2. Le P, Rothberg M. Herpes zoster infection. BMJ. 2019;364:k5095. doi:10.1136/bmj.k5095
3. Mortimer KJ, Cruz AA, Sepúlveda-Pachón IT, Jorga A, Vroling H, Williams C. Global herpes zoster burden in adults with asthma: a systematic review and meta-analysis. Eur Respir J. 2024;64(2):2400462. doi:10.1183/13993003.00462-2024
4. Zhu X, Hu P, Fan Z, et al. Effects of mindfulness-based stress reduction on depression, anxiety, and pain in patients with postherpetic neuralgia. J Nerv Ment Dis. 2019;207(6):482–486. doi:10.1097/NMD.0000000000000998
5. Lerman SF, Rudich Z, Brill S, Shalev H, Shahar G. Longitudinal associations between depression, anxiety, pain, and pain-related disability in chronic pain patients. Psychosom Med. 2015;77(3):333–341. doi:10.1097/PSY.0000000000000158
6. Drolet M, Brisson M, Schmader KE, et al. The impact of herpes zoster and postherpetic neuralgia on health-related quality of life: a prospective study. Cmaj. 2010;182(16):1731–1736. doi:10.1503/cmaj.091711
7. Du J, Sun G, Ma H, et al. Prevalence and risk factors of anxiety and depression in patients with postherpetic neuralgia: a retrospective study. Dermatology. 2021;237(6):891–895. doi:10.1159/000512190
8. Tang J, Zhang Y, Liu C, Zeng A, Song L. Therapeutic strategies for postherpetic neuralgia: mechanisms, treatments, and perspectives. Curr Pain Headache Rep. 2023;27(9):307–319. doi:10.1007/s11916-023-01146-x
9. Vickers AJ, Linde K. Acupuncture for chronic pain. JAMA. 2014;311(9):955–956. doi:10.1001/jama.2013.285478
10. Zhang R, Lao L, Ren K, Berman BM. Mechanisms of acupuncture-electroacupuncture on persistent pain. Anesthesiology. 2014;120(2):482–503. doi:10.1097/ALN.0000000000000101
11. Hempenstall K, Nurmikko TJ, Johnson RW, A’Hern RP, Rice AS. Analgesic therapy in postherpetic neuralgia: a quantitative systematic review. PLoS Med. 2005;2(7):e164. doi:10.1371/journal.pmed.0020164
12. Liu ZS, Peng WN, Liu BY, et al. Clinical practice guideline of acupuncture for herpes zoster. Chin J Integr Med. 2013;19(1):58–67. doi:10.1007/s11655-013-1191-y
13. Wang L, Zhou QC, Tian HF, Zhao JP. Analysis on the laws of acupoint selection and therapeutic operations with acupuncture based on the characteristics of postherpetic neuralgia. Chin Acupuncture Moxibustion. 2017;37(04):429–431.
14. Li JJ. Exploring the scientific basis of acupuncture therapy for the treatment of herpes zoster and postherpetic neuralgia. Trad Chin Med Res. 2019;32(03):77–80.
15. Liu Q, Wu X, Guo J, et al. Analgesic effect of electroacupuncture on postherpetic neuralgia: a trial protocol for a multicenter randomized controlled trial. Pain Ther. 2021;10(2):1755–1771. doi:10.1007/s40122-021-00283-8
16. Bragge P, Clavisi O, Turner T, Tavender E, Collie A, Gruen RL. The global evidence mapping initiative: scoping research in broad topic areas. BMC Med Res Methodol. 2011;11(1):92. doi:10.1186/1471-2288-11-92
17. Yang T, Xiao L, Li YK. Acupuncture and moxibustion for postherpetic neuralgia: an overview of systematic review. World Latest Med Inform. 2021;21(43):44–7,50.
18. Xia YF, Sun RH, Li SM, Wang YY, Li RR, Fang JQ. Different acupuncture therapies for postherpetic neuralgia: an overview of systematic reviews and meta-analysis. Chin J Integr Med. 2025;31(1):55–67. doi:10.1007/s11655-023-3613-4
19. Andrei G, Snoeck R. Advances and perspectives in the management of varicella-zoster virus infections. Molecules. 2021;26(4):1132. doi:10.3390/molecules26041132
20. Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. doi:10.1136/bmj.j4008
21. Kui W, Xie L, Li Y, et al. Efficacy and safety of bloodletting puncture and cupping in postherpetic neuralgia: a systematic review and meta-analysis. Biomed Rep. 2024;20(2). doi:10.3892/br.2023.1718
22. Yang Y, Xu W, Li M, Zhou Y, Qian Y. Collateral-pricking and bloodletting cupping combined with electroacupuncture for postherpetic neuralgia: a meta-analysis. Altern Ther Health Med. 2024;30(11):290–296.
23. Cui Y, Zhou X, Li Q, et al. Efficacy of different acupuncture therapies on postherpetic neuralgia: a Bayesian network meta-analysis. Front Neurosci. 2022;16:1056102. doi:10.3389/fnins.2022.1056102
24. Yang JW, Hu XY, Xiu WC, Tian ZY, Gang WJ, Jing XH. Acupuncture for the pain of postherpetic neuralgia: a scoping review. World J Acupuncture. 2023;33(4):358–366. doi:10.1016/j.wjam.2022.04.001
25. Wang H, Wan R, Chen S, et al. Comparison of efficacy of acupuncture-related therapy in the treatment of postherpetic neuralgia: a network meta-analysis of randomized controlled trials. Evid Based Complement Alternat Med. 2022;2022:3975389. doi:10.1155/2022/3975389
26. Wu Q, Hu H, Han D, Gao H. Efficacy and safety of moxibustion for postherpetic neuralgia: a systematic review and meta-analysis. Front Neurol. 2021;12. doi:10.3389/fneur.2021.676525
27. Pei W, Zeng J, Lu L, Lin G, Ruan J. Is acupuncture an effective postherpetic neuralgia treatment? A systematic review and meta-analysis. J Pain Res. 2019;12:2155–2165. doi:10.2147/JPR.S199950
28. Wang Y, Li W, Peng W, Zhou J, Liu Z. Acupuncture for postherpetic neuralgia: systematic review and meta-analysis. Medicine. 2018;97(34):e11986. doi:10.1097/MD.0000000000011986
29. Chen SY, Li XJ, Liu YW, Liu ZY. A Meta-analysis of efficacy and safety of treating post herpetic neuralgia by percussopunctator. Clin J Chinese Med. 2023;15(35):73–78.
30. Gao JY, Lu CJ, Yuan JJ, et al. The efficacy and safety of fire needling in the treatment of postherpetic neuralgia: a meta-analysis. J Guangzhou Univers Trad Chin Med. 2023;40(09):2403–2410.
31. Guo CQ. Clinical study and network Meta-analysis of acupuncture treatment for postherpetic neuralgia. Tianjin University of Traditional Chinese Medicine; 2023.
32. Hong WY, Jiang GH, Liu BQ. Meta-analysis and trial sequential analysis of randomized controlled trials of fu’s subcutaneous needling for postherpetic neuralgia. J Guangzhou Univers Trad Chin Med. 2023;40(01):261–270.
33. Li XJ, Wang Z, Han QY, Chen SZ, Wan HM. Different acupuncture methods for the treatment of postherpetic neuralgia: a network meta-analysis. World Chin Med. 2023;18(19):2752–2757.
34. Shi J. A meta-analysis on the treatment of postherpetic neuralgia by pricking and bleeding therapy. World Latest Med Inform. 2023;23(59):76–86.
35. Zhang B, Yin LW, Zhu HH, et al. Meta-analysis of Fu’s subcutaneous needling in the treatment of postherpetic neuralgia. J Guangzhou Univers Trad Chin Med. 2023;40(08):2108–2117.
36. Bian ZY. Acupuncture therapy for postherpetic neuralgia: a network Meta-analysis [Master]: Zhejiang Chinese Medical University; 2022.
37. Hu CX, Lin BC, Li ZX, Chen XZ, Xu NG. Systematic review and meta-analysis of single acupuncture therapy for postherpetic neuralgia. J Guangzhou Univers Trad Chin Med. 2022;39(11):2709–2717.
38. Huang SQ, Xiong J, Xiang J, Hua FH, Xiao Y, Yan LK. Efficacy and safety of fire needle for post-herpetic neuralgia: a systematic review. Chin J Evidence-Based Med. 2022;22(02):168–175.
39. Huang R, Dong ZW, Yan CC. Systematic assessment and meta-analysis on acupuncture for postherpetic neuralgia. China Med Pharm. 2022;12(24):32–36.
40. Jiang YH, Li YF, Fan BF. Traditional Chinese medicine external treatments for postherpetic neuralgia: a network meta-analysis. J China-Japan Friendship Hospital. 2022;36(02):109–111.
41. Qian X, Liu TF, Yuan AH. Meta-analysis on acupuncture and moxibustion in the treatment of postherpetic neuralgia. Guangming J Chin Med. 2022;37(07):1241–1245.
42. Yang JW. Study of influency factors of clinical efficacy of acupuncture and moxibustion in the treatment of postherpetic neuralgia. China Academy of Chinese Medical Sciences; 2022.
43. Zhou DN, Qi FJ, Wang ZJ, Wang YC. Meta-analysis of mainly treated with pricking blood and cupping in the treatment of postherpetic neuralgia. J Liaoning Univ Traditional Chin Med. 2022;24(08):166–171.
44. Jiang CXJ, Sun ZR, Yin HN. Meta-analysis of the efficacy and safety of acupuncture in the treatment of postherpetic neuralgia. J Emergency Traditional Chin Med. 2021;30(12):2083–2089.
45. Li Z. The effect of absorbable suture floating implantation on postherpetic neuralgia and and its influence on treg and Th17. Guangzhou University of Chinese Medicine; 2021.
46. Tang X, Chen XL, Xu DT, Tong HC. Meta analysis of the efficacy of fire needle therapy in the treatment of postherpetic neuralgia. World Latest Med Inform. 2021;21(12):268–9,71.
47. Liu YJ, Zhang QA, Wu YY, Shi Y, Fang JQ, Han DX. Meta-analysis for efficacy and safety of electroacupuncture in treating postherpetic neuralgia. J Guangzhou Univers Trad Chin Med. 2020;37(12):2472–2480.
48. Zha QP, Du YH, Li J, Zhang JJ, Chen LL. A meta-analysis of acupuncture and drugs in the treatment of postherpetic neuralgia. World Latest Med Inform. 2020;20(78):11–15.
49. Wu PP. Literature analysis and regularity of acupuncture in the treatment of postherpetic neuralgia. Liaoning University of Traditional Chinese Medicine; 2019.
50. Wu YJ. Meta analysis of the curative effect of warm acupuncture moxibustion in the treatment of post-herpetic neuralgia (PHN). Guangzhou University of Chinese Medicine; 2018.
51. Dong Q. Meta analysis of the efficacy of acupuncture and drug therapy for postherpetic neuralgia. J Liaoning Univ Traditional Chin Med. 2017;19(11):179–182.
52. Deng RY, Chen RX, Xiong J, Zhao W. System evaluation and meta-analysis of moxibustion on post-herpetic neuralgina. China J Tradition Chinese Med Pharm. 2016;31(12):5329–5332.
53. Zhang X, Li JX. Literature of clinical randomised controlled trials of acupuncture for postherpetic neuralgia: a meta-analysis. In:
54. Li W. Systematic evaluation and meta-analysis of acupuncture for postherpetic neuralgia. Beijing University of Chinese Medicine; 2015.
55. Ou DF, Zhou CE. System evaluation of RCT systematic about the treatment of postherpetic neuralgia by using fire needle. Clin J Trad Chin Med. 2015;27(01):115–119.
56. Xie FS. System evaluation of acupuncture and moxibustion treatment about postherpetic neuralgia. Guangzhou University of Chinese Medicine; 2015.
57. Yuan L. Acupuncture for postherpetic neuralgia: a systematic review and meta-analysis. Chengdu University of Traditional Chinese Medicine; 2014.
58. Wei YF, Gao SH. A systematic evaluation comparing the efficacy of acupuncture and western medicine in the treatment of postherpetic neuralgia. Henan Trad Chinese Med. 2011;31(11):1324–1327.
59. Zhu Y, Zhu LT, Li N, Li Y, Jin HZ. Jiaji points combined with surrounding needling for the treatment of postherpetic neuralgia: A meta-analysis. Chin J Tissue Eng Res. 2011;15(11):2064–2068.
60. Mao M. Clinical study on the treatment of postherpetic neuralgia by filiform-fire needle. Beijing University of Chinese Medicine; 2008.
61. Boyd A, Bleakley C, Hurley DA, et al. Herbal medicinal products or preparations for neuropathic pain. Cochrane Database Syst Rev. 2019;4(4):Cd010528. doi:10.1002/14651858.CD010528.pub4
62. Huerta M, Garcia MM, García-Parra B, Serrano-Afonso A, Paniagua N. Investigational drugs for the treatment of postherpetic neuralgia: systematic review of randomized controlled trials. Int J Mol Sci. 2023;24(16):12987. doi:10.3390/ijms241612987
63. Wang J, Wang X, Xia H, et al. An update of fire needle acupuncture for acute herpes zoster and prevention of postherpetic neuralgia in adults: a protocol for systematic review and meta-analysis. Medicine. 2021;100(1):e24180. doi:10.1097/MD.0000000000024180
64. Lu Y, Liu K, Liang Y, et al. Should we prescribe anticonvulsants for acute herpes zoster neuralgia and to prevent postherpetic neuralgia?: a protocol for meta-analysis and benefit-risk assessment. Medicine. 2021;100(7):e24343. doi:10.1097/MD.0000000000024343
65. Gawecka E, Viken O. Postherpetic neuralgia: new hopes in prevention with adult vaccination and in treatment with a concentrated capsaicin patch. Scand J Pain. 2012;3(4):220–228. doi:10.1016/j.sjpain.2012.05.070
66. Tang T, Bu HE, Jia M, et al. Efficacy and safety of injection in jiaji acupoints with corticosteroids for preventing post herpetic neuralgia in adults aged more than 50 years: a meta-analysis. Chin J Dermatovenereol Integr Trad Western Med. 2016;15(06):358–361.
67. Wang FC. Meta-analysis of early adjuvant treatment to prevent postherpetic neuralgia. Hebei Medical University; 2021.
68. Huang Y, Wu J, Cheng H, Liu Y. Moxibustion for herpes zoster and postherpetic neuralgia: a meta-analysis. Complexity. 2021;2021(1). doi:10.1155/2021/5551196
69. Liu S, Wang ZF, Su YS, et al. Somatotopic organization and intensity dependence in driving distinct NPY-expressing sympathetic pathways by electroacupuncture. Neuron. 2020;108(3):436–50.e7. doi:10.1016/j.neuron.2020.07.015
70. Yin ZH, Xu GX, Yang H, et al. A reappraisal of the systematic evaluation of acupuncture in the treatment of herpes zoster and its sequelae. Modernization Trad Chin Med Materia Medica. 2020;22(08):2772–2779.
71. Liu K, Zeng J, Pei W, et al. Assessing the reporting quality in randomized controlled trials of acupuncture for postherpetic neuralgia using the CONSORT statement and STRICTA guidelines. J Pain Res. 2019;12:2359–2370. doi:10.2147/JPR.S210471
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Integrated Western and Traditional Chinese Medicine Approaches for Herpes Zoster and Post-Herpetic Neuralgia: A Narrative Review
Li L, Xu J, Al-Danakh A, Xing Q
Drug Design, Development and Therapy 2026, 20:570847
Published Date: 13 January 2026