")
Back to Journals » International Journal of General Medicine » Volume 15
Acupuncture for Post-Stroke Cognitive Impairment: An Overview of Systematic Reviews
Authors Li L, Yang L, Luo B, Deng L, Zhong Y, Gan D, Wu X, Feng P , Zhu F
Received 30 May 2022
Accepted for publication 19 August 2022
Published 13 September 2022 Volume 2022:15 Pages 7249—7264
DOI https://doi.org/10.2147/IJGM.S376759
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Liuying Li,1 Lanying Yang,2 Biao Luo,2 Lvyu Deng,2 Yue Zhong,2 Daohui Gan,2 Xiaohan Wu,2 Peimin Feng,1 Fengya Zhu2
1Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China; 2Traditional Chinese Medicine Department, Zigong First People’s Hospital, Zigong, People’s Republic of China
Correspondence: Peimin Feng; Fengya Zhu, Email [email protected]; [email protected]
Background: Post-stroke cognitive impairment (PSCI) is one of the most common complications after stroke. In recent years, as a complementary alternative therapy, many systematic reviews (SRs) and meta-analysis (MAs) have reported the efficacy and safety of acupuncture in improving cognitive function in patients with PSCI, but the quality of evidence is unknown and therefore needs to be evaluated comprehensively.
Aim: We aimed to evaluate the SRs of acupuncture for patients with PSCI, to summarize the evidence quality of SRs to provide scientific evidence.
Methods: We searched for relevant SRs and MAs in seven databases up to March 22, 2022. Two reviewers independently completed literature retrieval, screening, and data extraction. We used A Measurement Tool to Assess Systematic Reviews 2 (AMSTAR 2) to evaluate the methodological quality; the Grading of Recommendations Assessment, Development and Evaluation (GRADE) tool to determine the strength of evidence; and the ROBIS tool to assess RoB.
Results: We identified 14 SRs. The methodological quality of all SRs was low (2/14) or very low (12/14). GRADE results showed 13 were moderate quality (26%), 5 were low quality (10%), and 32 were very-low quality (64%). RoB showed that one SR had a low risk and 13 had a high risk. Moderate quality results showed that combined acupuncture therapy was superior to western medicine or cognitive rehabilitation training in improving cognitive function, the total response rate, and the daily living ability of patients with PSCI.
Conclusion: Based on the evidence, acupuncture appears to be effective and safe in improving cognitive function for patients with PSCI, but the overall quality of SRs is not high. High-quality randomized controlled trials are needed to confirm the effectiveness and safety of acupuncture on the cognitive function of patients with PSCI.
Systematic Review Registration: PROSPERO CRD42022315441.
Keywords: acupuncture, PSCI, overview, AMSTAR-2, GRADE
Introduction
Stroke is a leading cause of mortality and disability worldwide.1 Post-stroke cognitive impairment (PSCI) is one of the most common complications after stroke, mainly manifested as impairments in memory, attention, orientation, and visuospatial function. PSCI refers to a series of syndromes that meet the diagnostic criteria for cognitive impairment after the occurrence of stroke.2 Two thirds of patients in the acute stage of stroke may have PSCI,3,4 and more than one third of patients with PSCI develop dementia after stroke recurrence4 and are easily overlooked.5 PSCI seriously affects rehabilitation compliance, delays the process of functional recovery, and reduces the quality of life.6 Therefore, early identification and timely intervention are of great significance to prevent the occurrence of PSCI and to control disease progression.
At present, the main therapeutic objectives for PSCI are to delay the progression of the disease and to prevent risk factors and complications, usually by combining drugs and non-drugs. Western medicine mainly uses calcium channel antagonists, cholinesterase inhibitors, and neurological agents7 alongside cognitive rehabilitation training. However, these interventions do not improve clinical efficacy, and the high cost and various adverse drug reactions also affect patient compliance. Therefore, it is necessary to explore other adjuvant treatment modalities.
In recent years, randomized controlled trials (RCTs) have shown the positive effect of acupuncture on improving the cognitive function and daily living ability of patients with PSCI,8,9 but the quality of evidence in favor of acupuncture for patients with PSCI presented in the relevant systematic reviews (SRs) and meta-analyses (MAs) is unclear. We aimed to collect, analyze, and present descriptive characteristics as well as the quantitative outcome data in SRs on acupuncture in patients with PSCI, and to assess their methodological quality.10 Our comprehensive evaluation also attempted to clarify the quality of the evidence for acupuncture treatment of patients with PSCI to provide better clinical support.
Methods
Search Strategy
We searched the Embase, Cochrane Library, PubMed, CNKI, SinoMed, VIP, and Wanfang databases for SRs published from the beginning to March 22, 2022 without language restriction. We used a combination of subject words and free words, including “stroke”, “post-stroke”, “apoplexy”, “cognitive dysfunction”, “cognition impairment”, “cognitive disorder”, “acupuncture”, “electro acupuncture”, “auricular acupuncture”, “scalp acupuncture”, “systematic review”, “systematic evaluation”, “meta-analysis.” In addition, we manually searched the list of references in the included SRs. The detailed retrieval strategy is shown in Supplementary document.
Inclusion Criteria
We included SRs and MAs based on RCTs of acupuncture for patients with PSCI. PSCI was diagnosed without restriction for gender, age, and course of disease. The treatment group included traditional acupuncture, electroacupuncture, ear acupuncture, head acupuncture, or acupuncture combined with other treatment. The control group was treated with any other methods except acupuncture, such as sham acupuncture, placebo, conventional therapy, western medicine, and cognitive function training. At least one of these results had to be reported in SRs: total effective rate, Mini-mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), activities of daily living (ADL), P300 peak latency, P300 amplitude, Barthel Index (BI), Loewenstein Occupational Therapy Cognitive Assessment (LOTCA), and Neurobehavioral Cognitive Status Examination (NCSE).
Exclusion Criteria
We excluded an SR if it met any of the following criteria: (a) the diagnostic criteria were unclear; (b) the intervention was mainly non-acupuncture or the control group received the same acupuncture therapy as the experimental group; (c) repeat publications; (d) unable to obtain the full text or incomplete data presented; (e) other types of research, such as animal experiments, protocols, conference papers, and case reports.
Study Selection and Data Extraction
According to the comprehensive retrieval strategy, two reviewers independently conducted literature retrieval and screening. The opinion of a third reviewer was sought when there was a disagreement. After identifying eligible studies, two researchers independently extracted relevant data according to standardized extraction tables, such as author, publication year, sample size, diagnostic criteria, interventions, outcomes, adverse reactions, conclusions, etc. Two reviewers cross-checked the extracted content, and a third reviewer was consulted to resolve any discrepancies.
Assessment of SRs
AMSTAR 2
Two reviewers used A Measurement Tool to Assess Systematic Reviews 2 (AMSTAR 2)11 to evaluate the methodological quality of SRs. This tool includes 16 items in total, with items 2, 4, 7, 9, 11, 13, and 15 considered key items. Items 2, 4, 7, 8, and 9 are rated as yes, no, or partially yes. The rest are rated as yes or no. Finally, the assessment level is divided into high, moderate, low, and very low.
ROBIS
We used the ROBIS tool12 to assess the risk of bias (RoB) for SRs. The evaluation process is divided into three stages: (a) evaluating correlation (selected according to the situation); (b) determine the degree of RoB in the SR process; (c) judge the RoB. We systematically evaluated four key areas for the second phase: (a) study eligibility criteria, (b) identification and selection of studies, (c) data collection and study appraisal, and (d) synthesis and findings. Each field consists of 5 or 6 key questions. The third stage judges the overall RoB according to the results of the second stage, and finally divides the risk level into “low risk”, “high risk”, and “unclear risk.” One person assessed RoB, another person checked this assessment, and then both reviewers discussed the results. In the case of a disagreement, a third party was consulted.
GRADE
Two researchers independently used the Grading of Recommendations Assessment, Development and Evaluation (GRADE) tool13 to evaluate the quality of the evidence. It includes five aspects: RoB, inconsistency, indirectness, imprecision, and publication bias. The two reviewers cross-checked the results, and disputes were decided by a third reviewer. We graded the quality of evidence as “high”, “moderate”, “low”, and “very low.”
Results
Search Results
We retrieved 505 related studies from the 7 databases. Of these, we deleted 204 duplicates and then screened 24 studies, followed by full-text evaluation. Finally, we included 14 SRs. The detailed flow chart is shown in Figure 1. The list of exclusions and reasons are shown in Excluded list in the Supplementary document.
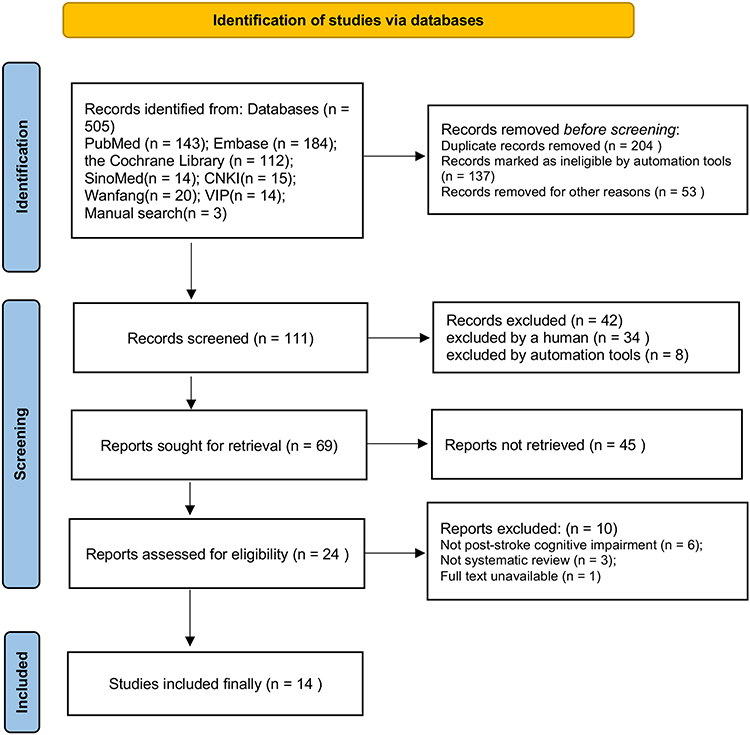 |
Figure 1 The detailed flow chart. |
Characteristics of the Included SRs
The 14 SRs14–27 were published from 2015 to 2021; two SRs19,27 were published in English and the others in Chinese. The SRs comprised a total of 263 RCTs and 19,224 subjects. Each SR included 8–42 RCTs, with a sample size of 506–3069 participants.
Six SRs defined the diagnostic criteria, and three SRs14,20,21 adopted the Main Points of Diagnosis of Various Cerebrovascular Diseases criteria. Three SRs18,20,24 adopted the Diagnostic and Statistical Manual of Mental Disorders (4th ed.) criteria. One SR16 used the Expert Consensus on the Management of Post-stroke Cognitive Impairment criteria. Zhang et al14 combined the Diagnostic and Therapeutic Criteria of TCM Diseases and Syndromes (ZY/T001.1-94). The remaining SRs did not mention specific diagnostic criteria. The control group usually received conventional treatment, cognitive rehabilitation training, or western medicine, and the treatment group combined traditional acupuncture, electroacupuncture, or ear acupuncture with the treatment received by the control group. The duration was usually 4–12 weeks. Adverse events were reported in six SRs,16,18,19,23–25 no adverse events were observed in one SR,22 and adverse events were not mentioned in the remaining SRs. Regarding the methodological quality assessment, four SRs14,20–22 used the Jadad scale, one SR15 did not report this information, and the remaining nine SRs used the Cochrane Collaboration’s RoB assessment tool. The basic characteristics of the literature are shown in Table 1.
 |
Table 1 The Basic Characteristics of the Literature |
Methodological Assessment
We used AMSTAR 2 to assess the methodological quality of the SRs. All SRs were low or very-low quality due to one or more serious deficiencies in critical items 2, 4, 7, 9, 11, 13, and 15, and multiple deficiencies in non-critical items.
Among the key items, only one SR reported the research protocol (item 219) and only one SR reported the exclusion list (item 716). The authors conducted a comprehensive database search to identify all relevant literature, but they did not search potential literature that might exist in detail (item 4). In 11 SRs, the authors synthesized data (item 11, except16,18,25). In 13 SRs, the authors considered RoB (Item 13, except15); 50% of SRs fully investigated and discussed the possible influence of publication bias on research results (item 15).
Among the non-critical items, the included SRs provided reasonable information on the inclusion criteria (item 1), literature screening and data extraction (items 5 and 6, except15), and basic characteristics (item 8), and they provided a heterogeneity discussion (item 14, except14,15). No SRs reported reasons for inclusion of RCTs (item 3). One SR reported funding source (item 1016); 50% of SRs considered the potential impact of RoB on the quality of evidence (item 12). Two SRs claims that there is no conflict of interest.19,27 The detailed results are shown in Table 2.
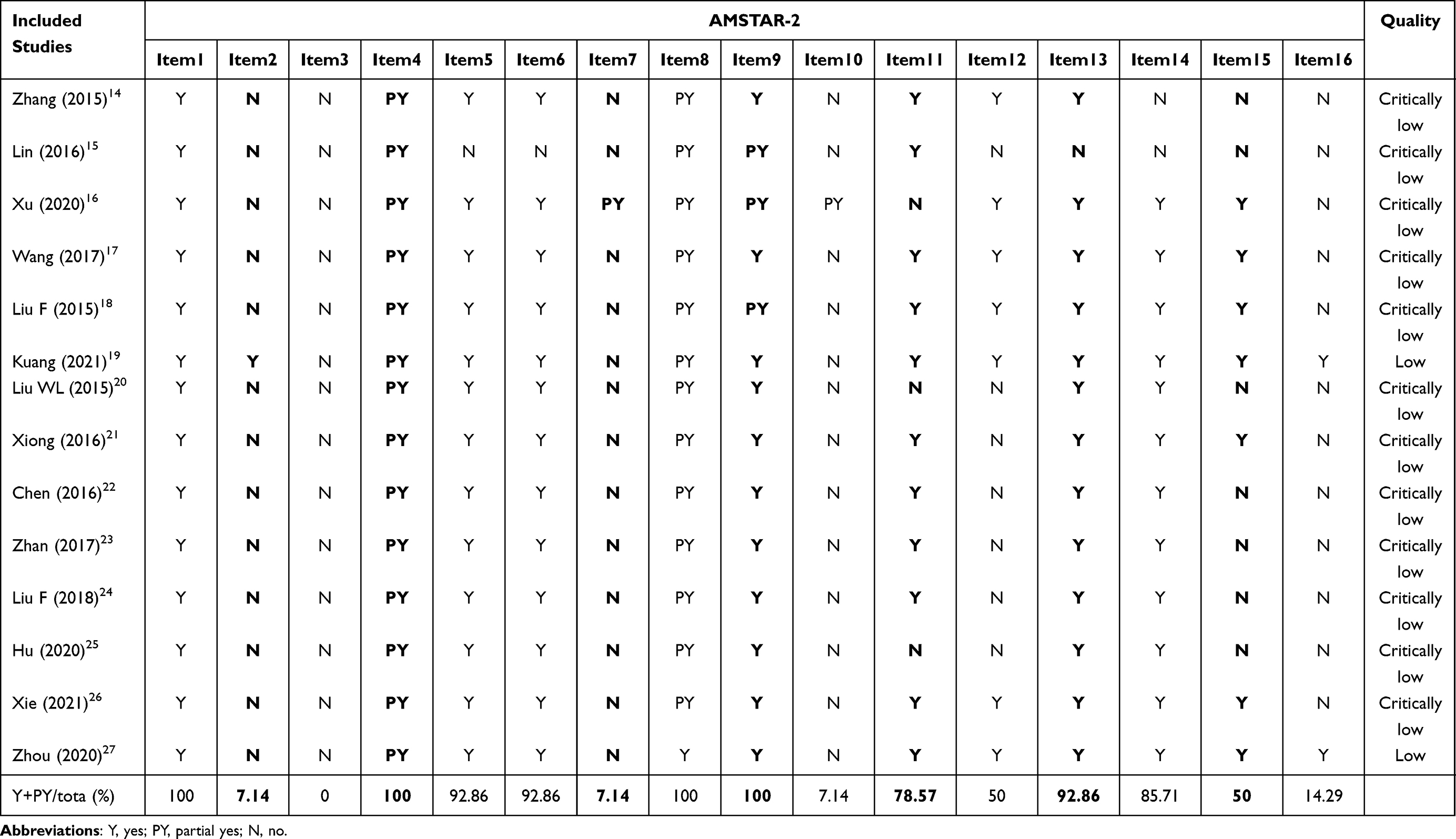 |
Table 2 The Detailed Results of AMSTAR-2 |
RoB
Only one SR19 (7.1%) had a low RoB; the remaining 13 SRs (92.9%) had a high RoB. The problems were related to research retrieval and screening, data extraction and quality evaluation, data synthesis, and presentation of the results. Failure to properly interpret and handle RoB may result in a high RoB for SRs, reducing the credibility of results and conclusions. The detailed results are shown in Figure 2 and Table 3.
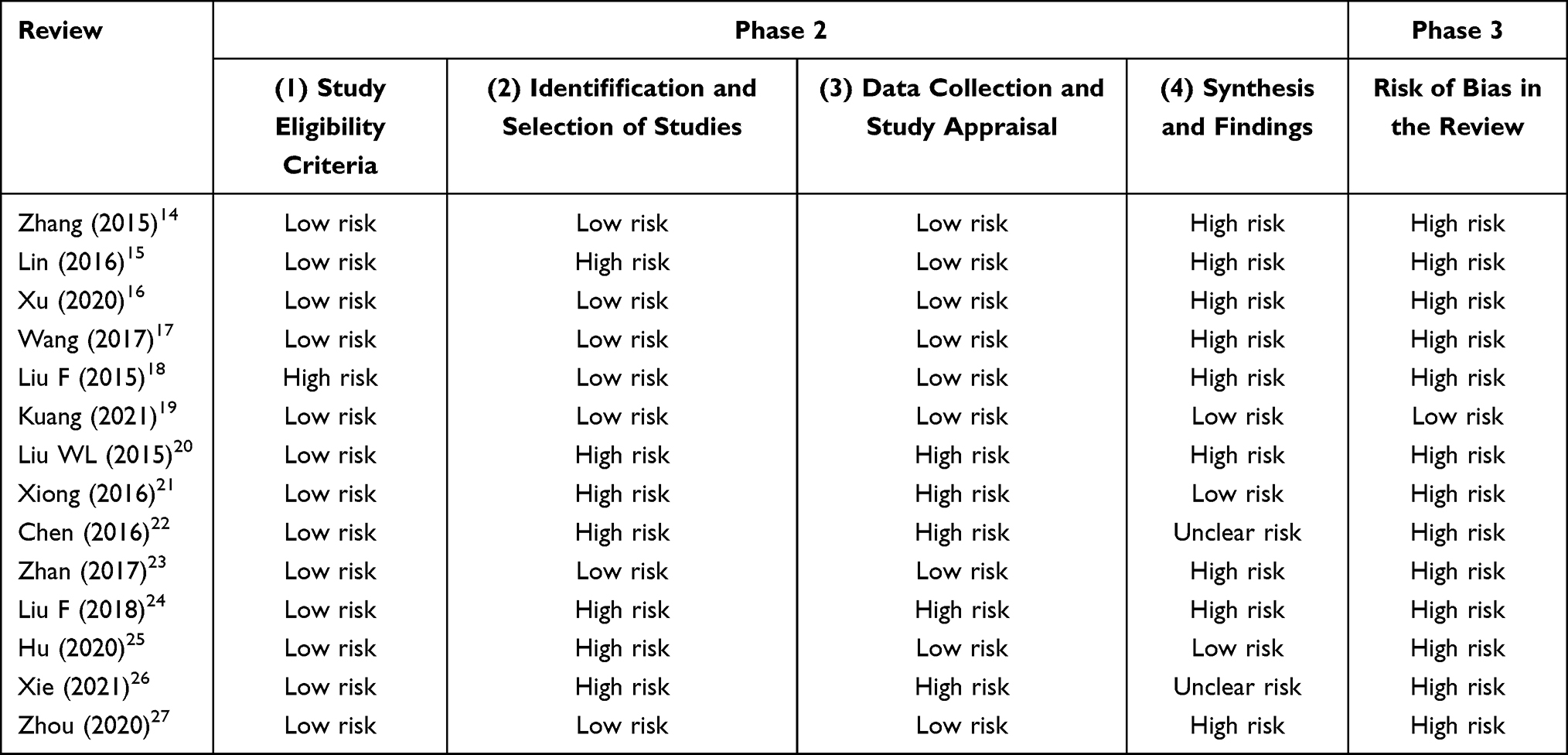 |
Table 3 The Detailed Results of RoB |
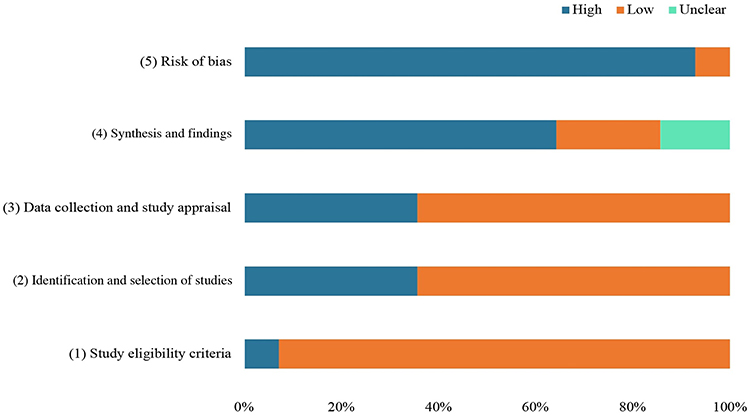 |
Figure 2 The detailed results of RoB. |
Quality of Evidence
We used the GRADE tool to evaluate the evidence quality of 50 outcomes. There were 13 outcomes of moderate quality (26%), 5 of low quality (10%), and 32 of very-low quality (64%); none was high quality. The main influencing factors of demotion were RoB, publication bias, inconsistency, and inaccuracy. The detailed results are shown in Table 4.
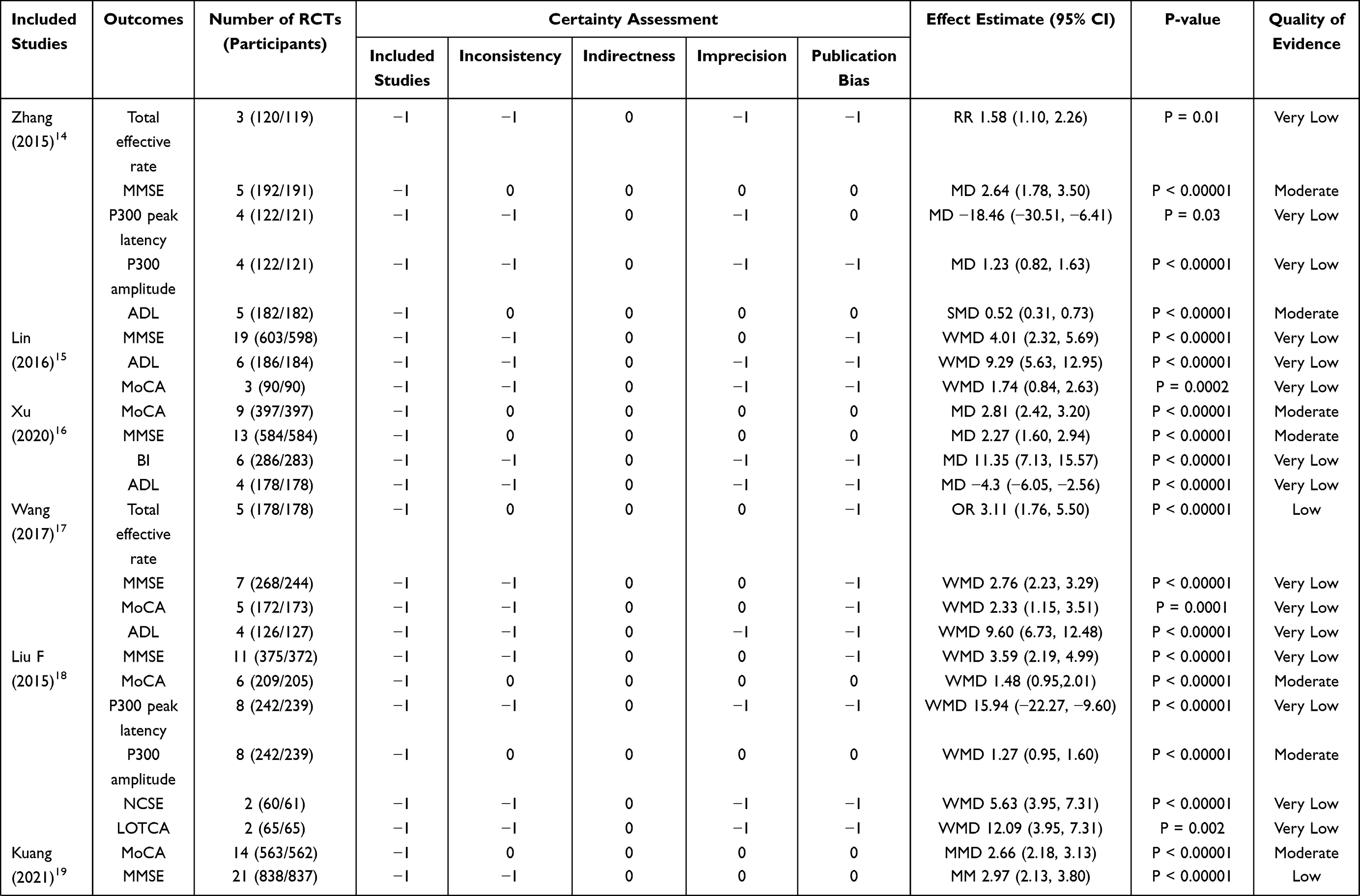 | 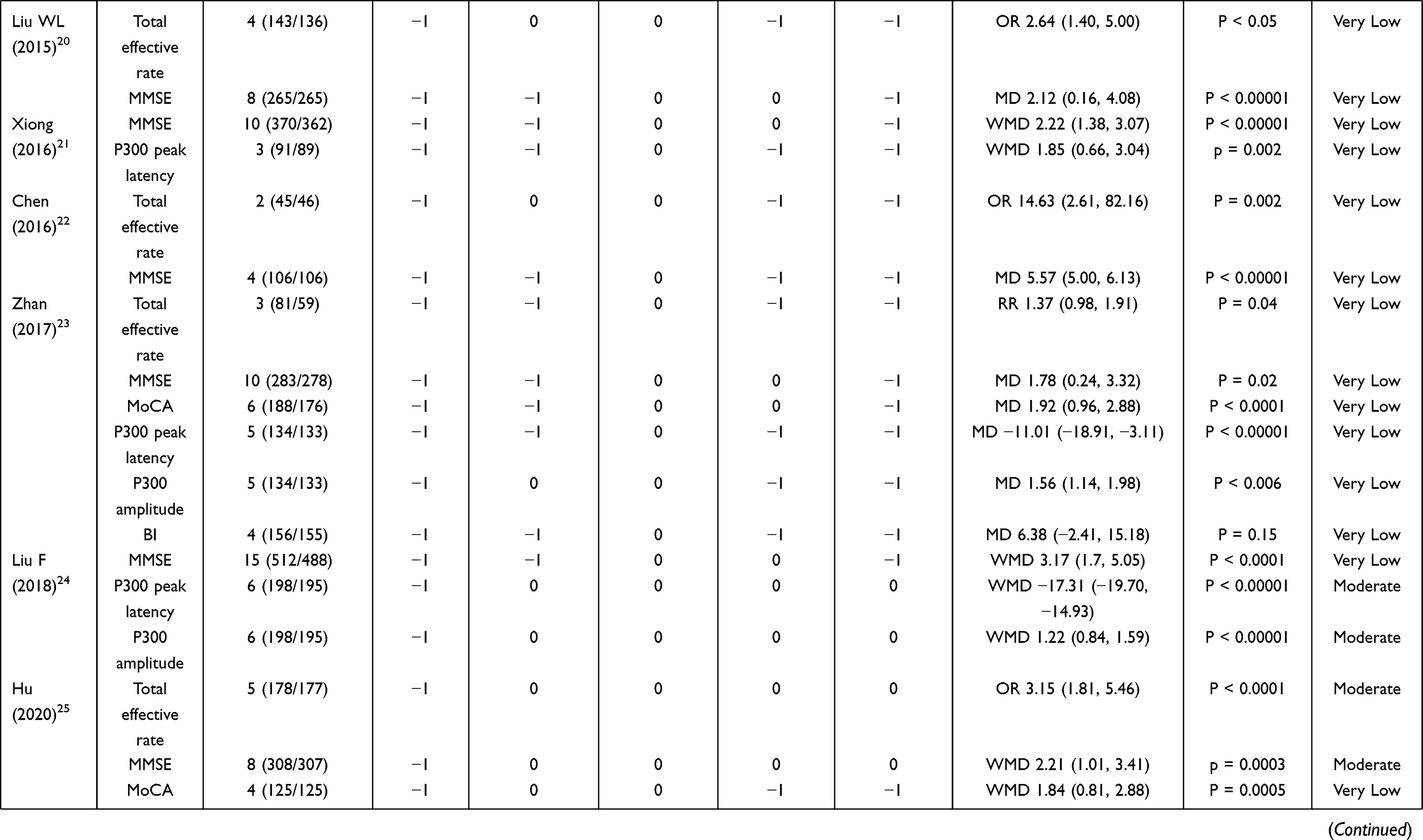 | 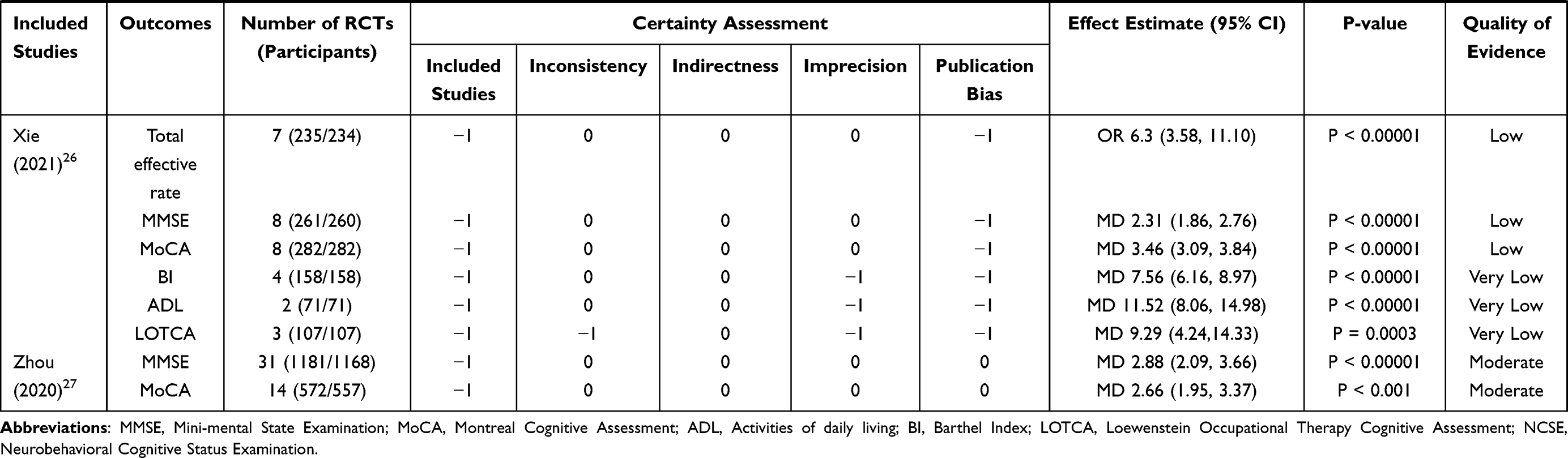 |
Table 4 The Detailed Results of GRADE |
Efficacy of Acupuncture for Patients with PSCI
This overview included three different acupuncture methods: traditional acupuncture (9 SRs), electroacupuncture (3 SRs), and scalp acupuncture (3 SRs). The results showed that these methods could significantly improve the MMSE score of PSCI patients. In addition, traditional acupuncture had a positive effect on improving the quality of life. We analyzed the outcomes, and the results suggested that acupuncture showed certain advantages in improving MMSE (14 SRs), total effective rate (7 SRs), MoCA (9 SRs), ADL (5 SRs), P300 peak Latency (6 SRs), P300 amplitude (4 SRs), BI (6 SRs), LOTCA (2 SRs) and NCSE (1 SRs). However, the overall quality of evidence was low. Based on the results of the moderate-quality evidence, four SRs suggested that acupuncture combined with routine therapy is more effective in improving MMSE14,16,25,27 and MoCA16,18,19,27 scores. In addition, some studies showed that P300 amplitude18,24,28 and P300 peak latency24 in the acupuncture group were better than in the control group. These results indicate that the cognitive function rehabilitation effect of acupuncture is better than western medicine or cognitive rehabilitation training alone. Acupuncture also seems to be effective in improving the total effective rate25 and daily living ability14 of patients with PSCI.
Adverse Events
Seven SRs reported no adverse events, six SRs reported adverse events, and one SR had no mention of adverse events. The main manifestations of the intervention group were subcutaneous hematoma or hemorrhage.16,18,24 In the control group, the main symptoms were dizziness and headache, nausea and vomiting,16,18,19,23 occasional itching,23 and blood pressure fluctuation.25 No serious adverse events occurred.
Discussion
Summary of the Main Results
We conducted a comprehensive and descriptive analysis of 14 SRs of acupuncture for patients with PSCI, involving 263 RCTs and 19,224 participants. Existing evidence suggests that acupuncture combined with cognitive rehabilitation training or western medicine is more effective than cognitive rehabilitation training or western medicine alone in improving the cognitive function of patients with PSCI, and does not cause serious adverse events. However, all SRs had low or very-low methodological quality, and 92.9% (13/14) of SRs were rated as high RoB. The GRADE results suggest that the quality of evidence for the efficacy of acupuncture needs to be improved.
Results-Based Discussion
A single SR seems to suggest the benefit of acupuncture in improving cognitive function in patients with PSCI, and the ROBIS assessment results indicate that the RoB for SRs are high. There is currently insufficient evidence to claim the efficacy and safety of acupuncture for improving cognitive function in patients with PSCI.
The methodological quality of SRs was low or very low according to AMSTAR 2. Of note, 92.9% (12/14) of SRs did not provide the previous protocol, meaning that we could not guarantee whether the research plan was followed strictly in the production process of SR, thus increasing the RoB. Moreover, 92.9% (12/14) of SRs did not list exclusions and reasons, which may have increased selection bias. Half of the SRs did not fully consider the impact of RoB on the results of the included studies, and the possibility of publication bias was not fully investigated when quantitative synthesis was carried out, which may affect the reliability of the results. In addition, 85.7% (12/14) of SRs did not declare potential conflicts of interest; hence, we could not determine whether the research conclusions were affected by potential interests.
According to the results of the evidence quality grading conducted by GRADE, only 26% of the results (13/50) were moderate. There are many factors contributing to the deterioration of evidence quality. First, the high RoB in all RCTs is the primary reason for the degradation of evidence quality. Factors such as study design, diagnostic criteria, course of disease, interventions, and acupuncture details may contribute to the high heterogeneity of RCTs, thereby increasing RoB in the original study, and thus reducing the reliability of the results of acupuncture for patients with PSCI. Publication bias (35/50), inconsistency (27/50) and inaccuracy (23/50) of SR also reduced the quality of evidence. The small number of RCTs with positive results, or the asymmetry of the funnel plot may lead to a large publication bias in outcomes. Inconsistency is mainly manifested in poor overlap of confidence intervals between different studies and high heterogeneity of the combined results (I2 > 50%), or the researchers did not provide reasonable explanation for results that had high heterogeneity. The small sample size and the small number of RCTs resulted in a wide 95% confidence interval, and 46% of the results were degraded due to inaccuracy.
Based on the results of all the evaluations, we propose several important recommendations to address the existing problems: (a) In order to further clarify the conclusions of the efficacy and safety of acupuncture in improving cognitive function in patients with PSCI, it is necessary for researchers to improve the quality of RCTs and to follow relevant clinical trial norms. According to the Consolidated Standards of Reporting Trials (CONSORT) and the STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA2010), clinical trials should be strictly designed, implemented, and reported to reduce the possibility of false positive results or RoB. (b) Authors should conduct comprehensive quality control of SR using AMSTAR 2, ROBIS, and GRADE tools to improve the stability and reliability of the evidence. (c) In particular, researchers should consider the persistent effects of acupuncture and pay attention to the long-term follow-up results. In addition, the effect of acupuncture has been controversial, and researchers need to clarify the specific efficacy of acupuncture on improving cognitive function in patients with PSCI, to ensure that positive outcomes are not due to the placebo effect.
Mechanism of Acupuncture to Improve Cognitive Function
For nearly 20 years, acupuncture has been widely studied for the treatment of pain, arthritis, neoplasms/cancer, pregnancy or labor, mood disorders, stroke, nausea, sleep, and paralysis/palsy,29 and as a means to regulate overall human health.30 Psychiatric manifestations of patients with dementia have been well documented in neuroimaging and neuropathological studies.31 Acupuncture had a synergistic effect on the recovery of upper limb dysfunction after stroke.32 Although the underlying mechanism of acupuncture treatment for cognitive dysfunction has not been fully elucidated, studies have shown that acupuncture can affect cognitive function by inhibiting the accumulation of toxic proteins in nervous system diseases, regulating glucose generation, reducing neuronal apoptosis, and providing neuroprotection.33 Animal experiments have shown that acupuncture could improve the cognitive ability of vascular dementia rats by increasing the content of 5-hydroxytryptamine (5-HT) in the hippocampus to regulate nerve conduction function.34 Moxibustion could reduce the expression of presenilin-1 (PS-1) mRNA and beta-site APP cleaving enzyme 1 (BACE-1) mRNA in the brain, subsequently block the production of amyloidβ-protein (Aβ) and reduce the level of serum IL-6, thereby inhibiting the chronic neuroinflammatory cascade.35 In addition, electroacupuncture can increase the expression of Beclin-1 in the brain tissue of ischemia-reperfusion model rats, and regulate the damage of autophagy network system to nerve cells.36 Functional magnetic resonance imaging (fMRI) results suggest that acupuncture tended to be associated with greater activation in the basal ganglia, brainstem, cerebellum, and insula, and more deactivation was seem in the so-called “default mode network” and limbic brain regions such as the amygdala and hippocampus. This suggests that the activity of specific brain regions induced by acupuncture is associated with the therapeutic effect of acupuncture on cognitive function.37
Discussion Based on Cognitive Function Assessment Scales
The MMSE, MoCA, NCSE, and LOTCA are commonly used and distinct tools to evaluate cognitive function. The MMSE was developed by Marshal and Susan Folstein of New York Hospital-Cornell Medical Center in NY, USA, in 1975.38 In 1988, Katzman et al39 adapted it to Chinese, and it is currently one of the most widely used scales by researchers to evaluate overall cognitive function. The scale contains seven domains: time orientation, place orientation, immediate memory, delayed memory, attention and computation, language, and visual space. It is simple and rapid and has good test-retest reliability. However, there are some limitations, such as lack of content to assess executive ability or poor sensitivity to mild cognitive impairment (MCI).38,40 Therefore, Nasreddine et al41 (Charles LeMoyne Hospital, Canada) developed the MoCA, which added an executive function score to the entry details of the MMSE to screen patients with MCI or MMSE usually within the normal range. This method can also quickly and reliably distinguish patients with MCI from patients with intact cognitive function, and has a high sensitivity and specificity for MCI, which can fill the deficiency of the MMSE. However, it is difficult to evaluate PSCI comprehensively and accurately using the MMSE or MoCA alone, so it is often recommended to combine multiple scales or scales in different cognitive function fields for comprehensive evaluation.42
The NCSE was compiled in 1983 and is divided into three general factors (level of consciousness, attention and orientation) and five major areas of cognitive function (language ability, structural ability, memory, computational ability, and reasoning ability). The NCSE adopts a functional profile to reflect different cognitive impairments and can also reflect the dynamic characteristics of cognitive function, with high sensitivity and reliability.43,44 However, the sensitivity is average for assessing reasoning, judgment, and structural abilities.45
The LOTCA was developed primarily for patients with acquired brain injury (ABI). One of its key advantages is the ability to assess a range of intact and impaired cognitive abilities,46 thus enhancing the design and planning of therapeutic interventions. At present, the scale is widely used in schizophrenia,47 stroke,48 and cognitive rehabilitation assessment of healthy children, adults, and the elderly.49 The main domains include containing orientation, visual perception, spatial perception, motor praxis, visuomotor organization, thinking operations, attention, and concentration; it has good internal consistency and inter-rater reliability.50
In this study, all SRs used the MMSE, and nine SRs used the MoCA. Four results for each scale were rated as moderate quality. Two SRs used the LOTCA and one SR used the NCSE; the evidence was very low quality. Therefore, the existing evidence cannot confirm that acupuncture improves the cognitive function of patients with PSCI, and the good effect obtained from clinical experience or small-scale application is not sufficient for application to evidence-based medicine. We need more large-sample and high-quality RCTs to prove the efficacy of acupuncture in patients with PSCI.
Selection of Acupoints
Only 3 SRs listed the characteristics of acupoint selection in detail. Based on the existing results and statistics, the top five acupoints used frequently are baihui (GV20), sishencong (EX-HN1), shenting (GV24), fengchi (GB20), and fengfu (GV16), which mainly involve the governor meridian and the Gallbladder meridian of foot-Shaoyang. The lesion site of PSCI is in the brain, so the main acupoints selected are concentrated in the brain. GV20, GV24 and GV16 belong to the governor meridian, which are closely connected with the brain and are important acupoints for regulating brain function. GB20 belongs to the Gallbladder meridian of foot-Shaoyang. It is good at treating mental diseases such as stroke, insomnia and epilepsy, and cooperated with EX-HN1 to treat mental disorders. These acupoints jointly regulate PSCI.
Strengths and Limitations
SRs based on high-quality RCTs are critical for clinical decision-making in evidence-based medicine. However, the marked increase in the number of SRs has questioned their quality. In recent years, many SRs showing that acupuncture improves cognitive function in patients with PSCI have been published. To our knowledge, this is the first comprehensive assessment of different SRs through inclusive retrieval and use of internationally recognized assessment tools. We have systematically assessed the methodological quality, RoB, and quality of evidence of relevant SRs by using the AMSTAR 2, ROBIS, and GRADE tools, respectively. We can intuitively understand the overall quality of SRs and the reliability of the results.
The limitation of our overview is that we could only synthesize and describe all the data quantitatively. Differences in RCT study designs and the details of acupuncture interventions may result in high RoB for SRs, which reduces the quality of the evidence and the methodology. Finally, we must point out that due to subjective factors, there could have been some deviations in our understanding of the assessment tools, but we have tried to minimize the errors in the assessment results.
Conclusion
Based on the collected evidence, acupuncture appears to be effective and safe in improving cognitive function in patients with PSCI, although the quality of the evidence from the original study and the methodological quality of the SRs reduced the reliability of the conclusions and the overall quality is not high. However, based on existing results, we still support the value of acupuncture as an adjunctive intervention for improving cognitive function in PSCI. In future research, it is necessary to confirm the efficacy and safety of acupuncture in patients with PSCI and to provide more reliable and scientific data that contributes to evidence-based medicine.
Disclosure
None of the authors stated any conflicts of interest in this study, and there were no potential commercial or financial relationships.
References
1. Vos T, Lim SS, Abbafati C, et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2020;396(10258):1204–1222. doi:10.1016/S0140-6736(20)30925-9
2. Skrobot OA, Black SE, Chen C, et al. Progress toward standardized diagnosis of vascular cognitive impairment: guidelines from the vascular impairment of cognition classification consensus study. Alzheimers Dement. 2018;14(3):280–292. doi:10.1016/j.jalz.2017.09.007
3. Mijajlović MD, Pavlović A, Brainin M, et al. Post-stroke dementia - a comprehensive review. BMC Med. 2017;15(1):11. doi:10.1186/s12916-017-0779-7
4. Yu KH, Cho SJ, Oh MS, et al. Cognitive impairment evaluated with vascular cognitive impairment harmonization standards in a multicenter prospective stroke cohort in Korea. Stroke. 2013;44(3):786–788. doi:10.1161/STROKEAHA.112.668343
5. Pollock A, St George B, Fenton M, et al. Top ten research priorities relating to life after stroke. Lancet Neurol. 2012;11(3):209. doi:10.1016/S1474-4422(12)70029-7
6. Fride Y, Adamit T, Maeir A, et al. What are the correlates of cognition and participation to return to work after first ever mild stroke? Top Stroke Rehabil. 2015;22(5):317–325. doi:10.1179/1074935714Z.0000000013
7. Sun MK. Potential therapeutics for vascular cognitive impairment and dementia. Curr Neuropharmacol. 2018;16(7):1036–1044. doi:10.2174/1570159X15666171016164734
8. Li T, Wu H, Soto-Aguliar F, et al. Efficacy of electrical acupuncture on vascular cognitive impairment with no dementia: study protocol for a randomized controlled trial. Trials. 2018;19(1):52. doi:10.1186/s13063-018-2458-1
9. Yang JW, Shi GX, Zhang S, et al. Effectiveness of acupuncture for vascular cognitive impairment no dementia: a randomized controlled trial. Clin Rehabil. 2019;33(4):642–652. doi:10.1177/0269215518819050
10. Pollock M, Fernandes RM, Becker LA, et al. What guidance is available for researchers conducting overviews of reviews of healthcare interventions? A scoping review and qualitative metasummary. Syst Rev. 2016;5(1):190. doi:10.1186/s13643-016-0367-5
11. Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both [J]. BMJ. 2017;358:j4008. doi:10.1136/bmj.j4008
12. Whiting P, Savović J, Higgins JP, et al. ROBIS: a new tool to assess risk of bias in systematic reviews was developed [J]. J Clin Epidemiol. 2016;69:225–234. doi:10.1016/j.jclinepi.2015.06.005
13. Schünemann HJ, Oxman AD, Brozek J, et al. Grading quality of evidence and strength of recommendations for diagnostic tests and strategies. BMJ. 2008;336(7653):1106–1110. doi:10.1136/bmj.39500.677199.AE
14. Zhang Y, Tang W, Song XG, et al. Systematic evaluation and meta-analysis of acupuncture combined with cognitive rehabilitation training in the treatment of cognitive impairment after stroke. Shanghai J Acupunct Moxibustion. 2015;34(10):1013–1020.
15. Xiaolan L, Weilin L, Erzheng L. Systematic evaluation of acupuncture in the treatment of overall cognitive dysfunction after stroke. Fujian J Tradit Chin Med. 2016;47(03):35–36.
16. Xu ZM, Liao X, Jia M, et al. Systematic evaluation of efficacy and safety of acupuncture in the treatment of cognitive impairment after stroke. BeijingJ Tradit Chin Med. 2020;39(11):1117–1122.
17. Jing W. Literature evaluation and clinical study of acupuncture in the treatment of cognitive impairment after stroke [PhD]. Guangzhou University of Chinese Medicine; 2017.
18. Fang L. Systematic evaluation and molecular mechanism of acupuncture in the treatment of cognitive dysfunction after stroke [PhD]: Fujian University of Traditional Chinese Medicine; 2015.
19. Kuang X, Fan W, Hu J, et al. Acupuncture for post-stroke cognitive impairment: a systematic review and meta-analysis. Acupunct Med. 2021;39(6):577–588. doi:10.1177/09645284211009542
20. Weilin L, Jia H, Jing TAO. Effects of electroacupuncture on cognitive dysfunction after ischemic stroke. Med Inform. 2015;2015(13):64.
21. Xiong J, Liao WJ, Liu Q, et al. Systematic evaluation of scalp acupuncture in the treatment of cognitive dysfunction after stroke. Chinese J Rehabilitation Med. 2016;31(03):333–339.
22. Chen LZ, Li W, Wang JQ, et al. Meta-analysis of scalp acupuncture in the treatment of cognitive impairment after stroke. Chin Med Rev. 2016;22(22):84–87.
23. Zhan J, Wang XW, Cheng F, et al. Electroacupuncture in the treatment of cognitive impairment after stroke: a systematic evaluation. Zhongguo Zhen Jiu. 2017;37(10):1119–1125. doi:10.13703/j.0255-2930.2017.10.025
24. Fang L, Liqun Y, Jinhui C. Effects of acupuncture at Baihui and Shenting points on cognitive dysfunction after stroke. Shanghai Journal of Acupuncture. 2018;37(01):104–111.
25. Shuting H, Min PI. Treatment of cognitive impairment after stroke by acupuncture at Baihui and Shuishou points: a systematic evaluation and meta-analysis. J Guangzhou Univ Tradit Chin Med;. 2020;37(10):2035–2042.
26. Xie DL, Yang K, Xie HH, et al. Clinical effect of scalp acupuncture on cognitive impairment after stroke: a meta-analysis. J Tradit Chin Med. 2021;27(12):130–136.
27. Zhou L, Wang Y, Qiao J, et al. Acupuncture for improving cognitive impairment after stroke: a meta-analysis of randomized controlled trials. Front Psychol. 2020;11:549265. doi:10.3389/fpsyg.2020.549265
28. Mao C, Fu XH, Yuan JQ, et al. Tong-xin-luo capsule for patients with coronary heart disease after percutaneous coronary intervention. Cochrane Database Syst Rev. 2015;2015;5:Cd010237.
29. Ma Y, Dong M, Zhou K, et al. Publication trends in acupuncture research: a 20-year bibliometric analysis based on PubMed. PLoS One. 2016;11(12):e0168123. doi:10.1371/journal.pone.0168123
30. Birch S. Treating the patient not the symptoms: acupuncture to improve overall health - Evidence, acceptance and strategies. Integr Med Res. 2019;8(1):33–41. doi:10.1016/j.imr.2018.07.005
31. Casanova MF, Starkstein SE, Jellinger KA. Clinicopathological correlates of behavioral and psychological symptoms of dementia. Acta Neuropathol. 2011;122(2):117–135. doi:10.1007/s00401-011-0821-3
32. Syros A, Kotlia P, Fotakopoulos G. Preliminary findings from an acupuncture and experiential/traditional music therapy during the standard care of rehabilitation exercise program for recovery on post-stroke upper limb dysfunction. Int J Neurosci. 2022;1–8. doi:10.1080/00207454.2020.1860972
33. Guo X, Ma T. Effects of acupuncture on neurological disease in clinical- and animal-based research. Front Integr Neurosci. 2019;13:47. doi:10.3389/fnint.2019.00047
34. Dong J, Zhang J, Li XH, et al. Effects of transportation Rendu acupuncture on cognitive ability and hippocampal 5-HT content in vascular dementia rats. Chin J Tradit Chin Med. 2017;24(02):129–131.
35. Zhu CF, Sun JJ, Han W, et al. Effect of Tongdu Tiaoshen moxibustion on hippocampal β-amyloid overexpression in rats with mild cognitive impairment. Acupunct Res. 2016;41(02):131–137.
36. Feng XD, Gao LL, Li RQ, et al. Effect of electroacupuncture on the expression of Beclin-1 protein and gene in brain tissue of rats with cerebral ischemia-reperfusion. Chin j Rehabilitation Med. 2016;31(12):
37. Huang W, Pach D, Napadow V, et al. Characterizing acupuncture stimuli using brain imaging with FMRI–a systematic review and meta-analysis of the literature. PLoS One. 2012;7(4):e32960. doi:10.1371/journal.pone.0032960
38. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi:10.1016/0022-3956(75)90026-6
39. Katzman R, Zhang MY, Ouang YQ, et al. A Chinese version of the mini-mental state examination; impact of illiteracy in a Shanghai dementia survey. J Clin Epidemiol. 1988;41(10):971–978. doi:10.1016/0895-4356(88)90034-0
40. Lonie JA, Tierney KM, Ebmeier KP. Screening for mild cognitive impairment: a systematic review. Int J Geriatr Psychiatry. 2009;24(9):902–915. doi:10.1002/gps.2208
41. Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. doi:10.1111/j.1532-5415.2005.53221.x
42. Geubbels HJ, Nusselein BA, van Heugten CM, et al. Can the Montreal Cognitive Assessment predict discharge destination in a stroke population in the hospital?. J Stroke Cerebrovasc Dis. 2015;24(5):1094–1099. doi:10.1016/j.jstrokecerebrovasdis.2015.01.034
43. Schwamm LH, Van Dyke C, Kiernan RJ, et al. The neurobehavioral cognitive status examination: comparison with the cognitive capacity screening examination and the mini-mental state examination in a neurosurgical population. Ann Intern Med. 1987;107(4):486–491. doi:10.7326/0003-4819-107-4-486
44. Schmitt FA, Ranseen JD, DeKosky ST. Cognitive mental status examinations. Clin Geriatr Med. 1989;5(3):545–564. doi:10.1016/S0749-0690(18)30670-0
45. Logue PE, Tupler LA, D’Amico C, et al. The neurobehavioral cognitive status examination: psychometric properties in use with psychiatric inpatients. J Clin Psychol. 1993;49(1):80–89. doi:10.1002/1097-4679(199301)49:1<80::AID-JCLP2270490111>3.0.CO;2-Z
46. Almomani F, Avi-Itzhak T, Demeter N, et al. Construct validity and internal consistency reliability of the Loewenstein occupational therapy cognitive assessment (LOTCA). BMC Psychiatry. 2018;18(1):184. doi:10.1186/s12888-018-1776-x
47. Su CY, Chen WL, Tsai PC, et al. Psychometric properties of the Loewenstein Occupational Therapy Cognitive Assessment-Second edition in Taiwanese persons with schizophrenia. Am J Occup Ther. 2007;61(1):108–118. doi:10.5014/ajot.61.1.108
48. Wang SY, Gong ZK, Sen J, et al. The usefulness of the Loewenstein Occupational Therapy Cognition Assessment in evaluating cognitive function in patients with stroke. Eur Rev Med Pharmacol Sci. 2014;18(23):3665–3672.
49. Josman N, Abdallah TM, Engel-Yeger B. Using the LOTCA to measure cultural and sociodemographic effects on cognitive cultural and sociodemographic effects on cognitive skills in two groups of children. Am J Occup Ther. 2011;65(3):e29–37. doi:10.5014/ajot.2011.09037
50. Katz N, Itzkovich M, Averbuch S, et al. Loewenstein Occupational Therapy Cognitive Assessment (LOTCA) battery for brain-injured patients: reliability and validity. Am J Occup Ther. 1989;43(3):184–192. doi:10.5014/ajot.43.3.184
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.