Back to Journals » Journal of Pain Research » Volume 19
Acupuncture for Comorbid Chronic Nonspecific Neck Pain and Chronic Insomnia: Protocol for a Multicenter, Randomized, Sham-Controlled Trial
Authors Liu S ![]() , Chen H
, Chen H ![]() , Shen X
, Shen X ![]() , Lun H, Fan J, Wang W
, Lun H, Fan J, Wang W ![]() , Shi G, Liu Z
, Shi G, Liu Z ![]()
Received 24 January 2026
Accepted for publication 2 April 2026
Published 17 April 2026 Volume 2026:19 598575
DOI https://doi.org/10.2147/JPR.S598575
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Houman Danesh
Sixing Liu,1,* He Chen,2,* Xinyu Shen,2,3 Hanwei Lun,2,3 Jiarong Fan,2,3 Weiming Wang,2 Guangxia Shi,1 Zhishun Liu2
1School of Acupuncture-Moxibustion and Tuina, Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 2Department of Acupuncture, Guang’anmen Hospital, China Academy of Chinese Medical Sciences, Beijing, People’s Republic of China; 3Graduate College, Beijing University of Chinese Medicine, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhishun Liu, Email [email protected] Guangxia Shi, Email [email protected]
Background: Chronic nonspecific neck pain (CNSNP) and chronic insomnia frequently coexist and may reinforce one another, yet high-quality evidence for nonpharmacological interventions targeting both conditions remains limited. This protocol describes a multicenter randomized trial evaluating the efficacy and safety of acupuncture for this clinically important comorbidity.
Methods: This multicenter, parallel-group, participant-, assessor-, and statistician-blinded, sham-controlled superiority trial will be conducted at six centers in China. A total of 128 eligible adults aged 18– 75 years with comorbid CNSNP and chronic insomnia will be randomly assigned in a 1:1 ratio to receive acupuncture or sham acupuncture. Participants will receive 12 treatment sessions over 4 weeks, followed by 12 weeks of post-treatment follow-up. The co-primary outcomes are the changes from baseline in average neck pain intensity measured by the Numerical Rating Scale (AP-NRS) and in insomnia severity measured by the Insomnia Severity Index (ISI) at week 4. Secondary outcomes include AP-NRS and ISI at other time points, and clinically important pain and sleep response rates, Neck Disability Index, maximum neck pain during neck movement, Pittsburgh Sleep Quality Index, Hospital Anxiety and Depression Scale, Patient Global Impression of Change, and medication use. Adverse events will also be assessed. Analyses will follow the intention-to-treat principle using mixed-effects models, and the co-primary outcomes will be tested with a fixed-sequence strategy to control the family-wise type I error rate.
Discussion: This trial addresses an important evidence gap in the management of comorbid CNSNP and chronic insomnia. Its multicenter design, standardized acupuncture procedures, sham comparator, formal blinding assessment, and validated patient-reported outcomes may improve internal validity, clinical interpretability, and generalizability.
Ethics and Dissemination: The protocol has been approved by the Ethics Committee of Guang’anmen Hospital, China Academy of Chinese Medical Sciences (Approval No. 2025-090-KY). Written informed consent will be obtained from all participants before enrollment. Findings will be disseminated through peer-reviewed publications and academic presentations.
Trial Registration: ClinicalTrials.gov NCT06996210; registered on May 30, 2025.
Keywords: chronic nonspecific neck pain, chronic insomnia, acupuncture, sham acupuncture, randomized controlled trial, study protocol
Introduction
Chronic nonspecific neck pain (CNSNP) and chronic insomnia are prevalent, persistent, and clinically burdensome conditions. According to the Global Burden of Disease Study 2023 (GBD 2023), 209.9 million people were living with neck pain worldwide in 2023, and there were 48.8 million prevalent cases of neck pain, corresponding to an age-standardized prevalence rate of 2.5% in China.1 A recent systematic review estimated that 16.2% of adults worldwide experience insomnia, and the pooled prevalence of insomnia in the general population in China has been reported as 15.0%.2,3 Both conditions are associated with impaired quality of life, reduced daytime functioning, and increased health-care use.1,4–7 CNSNP generally refers to neck pain lasting at least 3 months in the absence of a specific pathoanatomical process such as fracture, infection, inflammatory disease, malignancy, or cervical myelopathy.8,9 Chronic insomnia is characterized by persistent difficulty initiating sleep, maintaining sleep, or waking too early despite adequate opportunity for sleep, together with daytime impairment, and is diagnosed in this trial according to the International Classification of Sleep Disorders, Third Edition (ICSD-3).5,6,10
Epidemiological and mechanistic evidence supports a bidirectional relationship between neck pain and sleep disturbance.11–17 In patients with chronic neck pain, clinically important insomnia is common. In a retrospective cohort study, 22.9% of patients met criteria for clinically significant insomnia, and more than half reported at least mild sleep disturbance after the onset of neck pain.13 Poor sleep may heighten pain sensitivity through central sensitization, impaired endogenous pain inhibition, dysregulation of the hypothalamic-pituitary-adrenal axis, and inflammatory activation; conversely, persistent pain can fragment sleep, increase hyperarousal, and perpetuate psychological distress.12,15,17 The coexistence of CNSNP and chronic insomnia therefore reflects more than simple comorbidity; rather, it represents a mutually reinforcing symptom cluster associated with greater disability and more complex treatment needs.
Current management strategies for CNSNP commonly include exercise-based rehabilitation, manual therapy, education, and selected nonpharmacological interventions such as acupuncture, whereas chronic insomnia is primarily managed with cognitive behavioral therapy for insomnia (CBT-I) and, in selected patients, hypnotic medication.9,18,19 However, access to rehabilitation or CBT-I remains limited in many settings, and pharmacotherapy for insomnia or pain may be constrained by adverse events, tolerance, dependence, polypharmacy, and incomplete response.20–22 Accordingly, there is a clear need for accessible, effective, and well-tolerated nonpharmacological options for patients with comorbid CNSNP and chronic insomnia. Acupuncture has shown benefit in chronic neck pain23–25 and insomnia26–28 when each condition is studied separately, but evidence for the combined presentation remains sparse. Clinical studies relevant to comorbid neck pain and insomnia remain limited and have largely been published in Chinese, with common methodological constraints such as small sample size, short follow-up, and incomplete reporting.29–31 The present study was therefore designed as a superiority trial to investigate whether acupuncture is superior to sham acupuncture in improving both neck pain intensity and insomnia severity in adults with comorbid CNSNP and chronic insomnia. We hypothesize that acupuncture will produce greater improvement than sham acupuncture in both co-primary outcomes at week 4, with benefits extending into follow-up.
Study Design
This study is a multicenter, parallel-group, randomized, sham-controlled superiority trial with a 1:1 allocation ratio. Participants, outcome assessors, data managers, and statisticians will remain blinded to group assignment. Each participant will undergo a 17-week study period comprising a 1-week baseline phase, a 4-week treatment phase, and a 12-week post-treatment follow-up phase. The protocol is reported in accordance with the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) 2025 statement, together with the Revised Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA) and the Sham Acupuncture Reporting (SHARE) guideline.32–35 The study flow is shown in Figure 1, and the participant timeline is summarized in Figure 2 and Table 1.
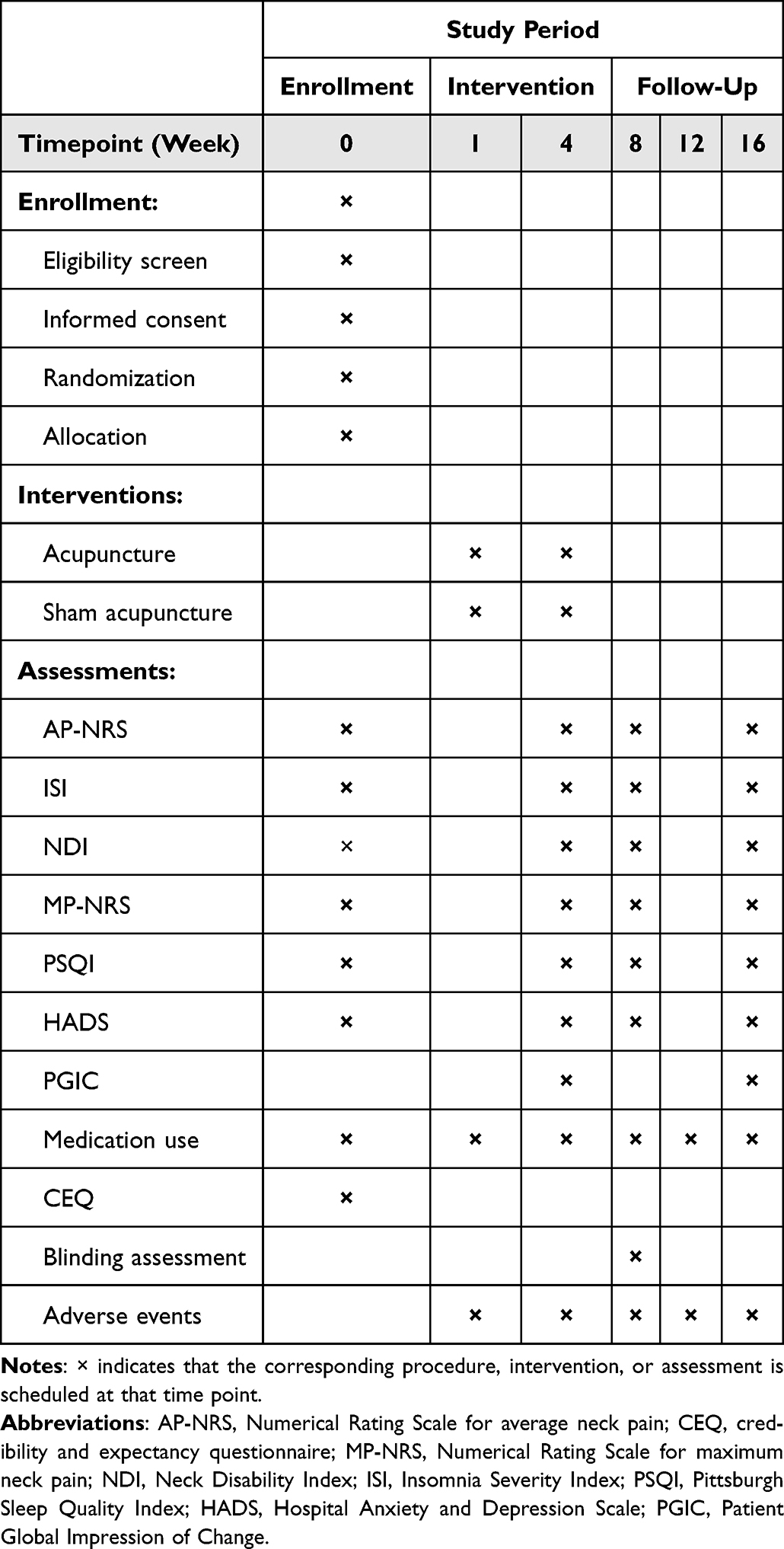 |
Table 1 Schedule of Enrollment, Interventions, and Assessments |
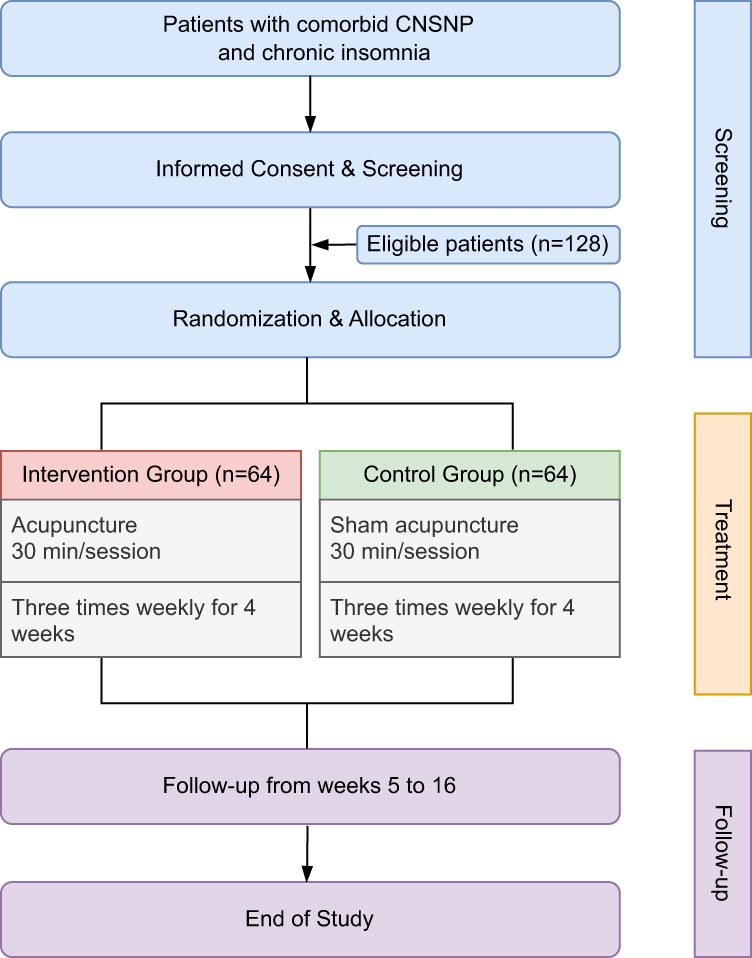 |
Figure 1 Study flow diagram of the trial. |
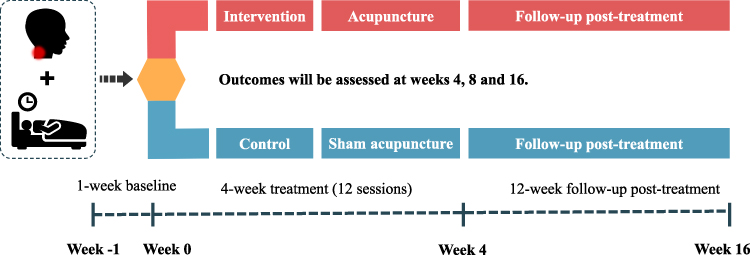 |
Figure 2 Overview of the participant timeline. |
Study Setting and Recruitment
The trial will be conducted at six centers in China: Guang’anmen Hospital, China Academy of Chinese Medical Sciences (Beijing); Beijing Friendship Hospital, Capital Medical University (Beijing); Beijing Hospital of Integrated Traditional Chinese and Western Medicine (Beijing); Beixiaguan Community Health Service Center, Haidian District (Beijing); Sports Medicine Institute of the General Administration of Sport of China (Beijing); and Shaanxi Provincial Hospital of Traditional Chinese Medicine (Xi’an, Shaanxi Province). Recruitment is planned from March 2026 to December 2027 through outpatient clinics, posters, hospital websites, and social-media-based advertisements.
Informed Consent
Before any trial-specific procedure is undertaken, trained investigators will provide potential participants with written and verbal information about the study objectives, procedures, potential benefits, and possible risks. Participant-facing information and consent documents will be provided in Chinese, the native language of the study population, and will be explained verbally by trained investigators. Adequate time will be allowed for questions and voluntary decision-making. Written informed consent will then be obtained. Participants may withdraw from the study at any time without penalty.
Randomization, Allocation Concealment, and Blinding
The allocation sequence will be generated by an independent statistician from INTELING Tech Co., Ltd. (Beijing, China) using center-stratified permuted blocks. The sequence will be embedded within a password-protected web-based randomization system. After eligibility has been confirmed and baseline assessment completed, a research assistant who is not involved in treatment delivery or outcome assessment will obtain the randomization result and notify the treating acupuncturist. Acupuncturists will not have access to upcoming allocations.
Participants, outcome assessors, data managers, and statisticians will remain blinded until the database has been locked unless emergency unblinding is required for clinical management of a serious adverse event. Treating acupuncturists cannot be blinded because of the nature of the intervention, but they will not perform outcome assessments, data cleaning, or statistical analyses. To support participant blinding, both groups will be treated in the same clinical environment, for the same session duration and visit schedule, using identical adhesive pads and visually similar needles.
Participants
Eligibility will be evaluated by licensed physicians at each site who have completed trial-specific training and have clinical experience in musculoskeletal and sleep-related disorders. Comorbidity is defined as fulfillment of both the CNSNP criteria and the chronic insomnia criteria at screening.
CNSNP will be defined as neck pain persisting for at least 3 months, located primarily in the cervical region, aggravated by movement or posture, and not attributable to a specific structural or systemic disorder. Conceptually, CNSNP overlaps with ICD-11 chronic primary cervical pain within the broader category of chronic primary musculoskeletal pain.8,9 The diagnosis will be based on history taking and physical examination, with additional imaging or specialist consultation obtained when clinically indicated to exclude specific causes. Chronic insomnia will be diagnosed according to ICSD-3 criteria: difficulty initiating sleep, maintaining sleep, or waking too early despite adequate opportunity for sleep, occurring at least 3 nights per week for at least 3 months and accompanied by daytime impairment.10
Inclusion criteria are as follows: (1) age 18−75 years; (2) diagnosis of comorbid CNSNP and chronic insomnia; (3) Numerical Rating Scale for average neck pain (AP-NRS) score ≥3 at baseline; (4) Insomnia Severity Index (ISI) score ≥10 at baseline; and (5) written informed consent.
Exclusion criteria are as follows: (1) neck pain attributable to trauma, fracture, malignancy, inflammatory disease, infection, myelopathy, or other specific pathology; (2) objective neurologic deficit, progressive radicular syndrome, or positive red-flag findings requiring urgent evaluation; (3) previous cervical spine surgery or major cervical trauma; (4) spinal ankylosis or other severe cervical structural abnormality; (5) use of systemic analgesics, muscle relaxants, or corticosteroids on ≥3 days per week for more than 2 consecutive weeks during the month before screening; (6) initiation of hypnotic, antidepressant, or other sleep-related medication, or a dose change in such medication, within 2 weeks before baseline; (7) substance- or medication-induced insomnia; (8) other primary sleep disorders, including suspected sleep apnea syndrome, restless legs syndrome, circadian rhythm disorder, or shift-work-related sleep disorder; (9) severe cardiac, hepatic, renal, hematologic, autoimmune, infectious, or malignant disease; (10) severe psychiatric disease, cognitive impairment, or communication disorder that would interfere with participation; (11) acupuncture for neck pain or insomnia within 30 days before screening; (12) substance abuse; or (13) pregnancy, lactation, or intention to become pregnant during the trial.
To improve external validity while maintaining protocol consistency, participants who are already using hypnotic medication at a stable dose for at least 2 weeks before baseline may be enrolled, provided that no dose escalation is planned during the 4-week treatment phase. All concomitant medications and non-study interventions will be recorded in detail.
Interventions
The acupuncture regimen was developed on the basis of prior clinical evidence, consensus among senior investigators, and routine clinical practice for coexisting neck pain and insomnia.23–25,28,36 All interventions will be delivered by licensed acupuncturists with at least 2 years of independent practice experience after centralized training in point location, needling procedures, sham procedures, and adverse-event documentation. Treatment will be administered in private rooms to reduce communication between participants and to standardize the treatment environment across sites.
The selected points are GV20 (Baihui), superior GV29 (superior Yintang), Jingbailao (EX-HN15), Wangu (GB12), Shenmen (HT7), Taixi (KI3), and one individualized ashi point identified by local tenderness. Point localization will follow China national standard for nomenclature and location of meridian points (GB/T 12346–2021).37 The locations are listed in Table 2 and illustrated in Figure 3. Foam adhesive pads will be applied before needling at all points except GV20, where pad fixation is impractical because of the hair-bearing scalp anatomy.
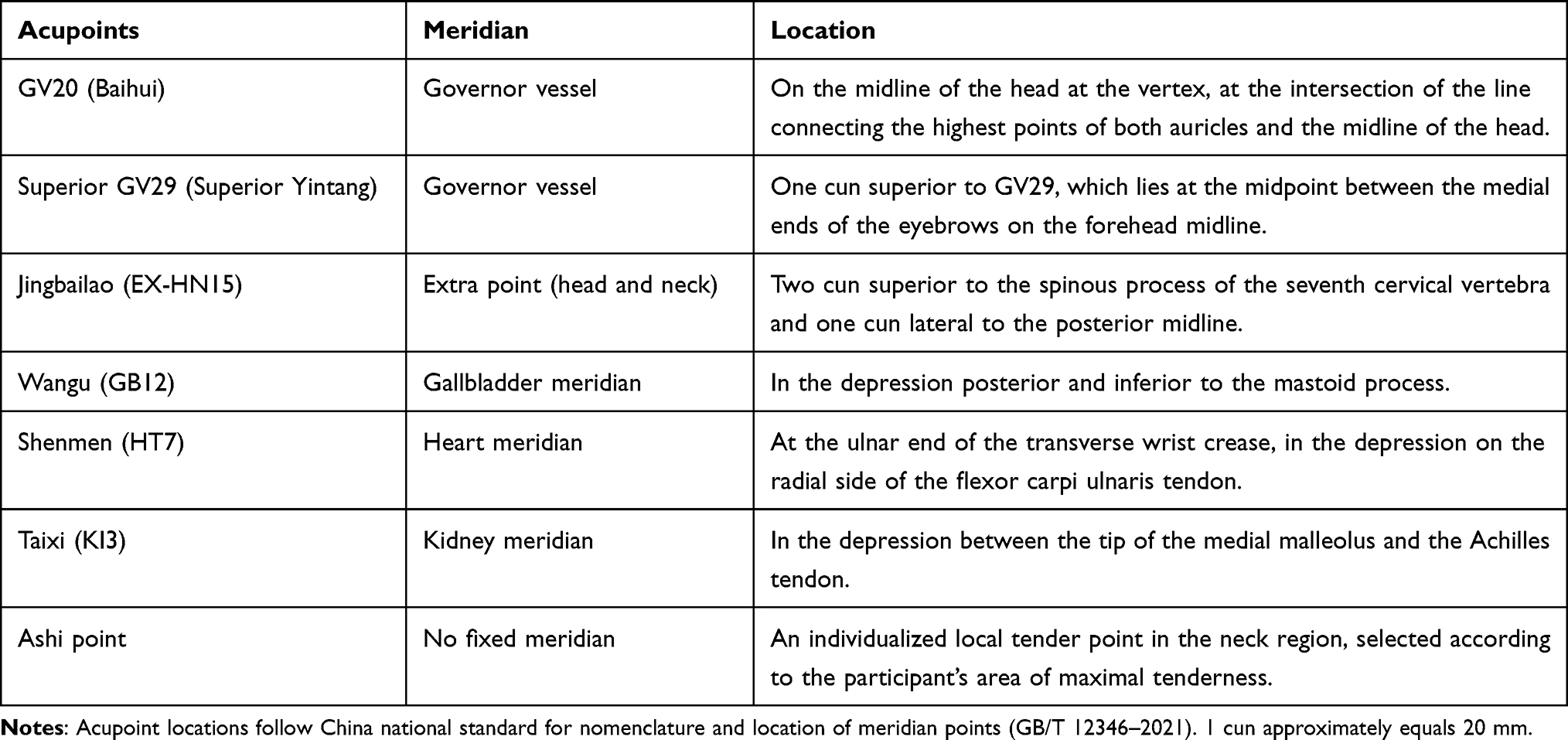 |
Table 2 Locations of Selected Acupoints |
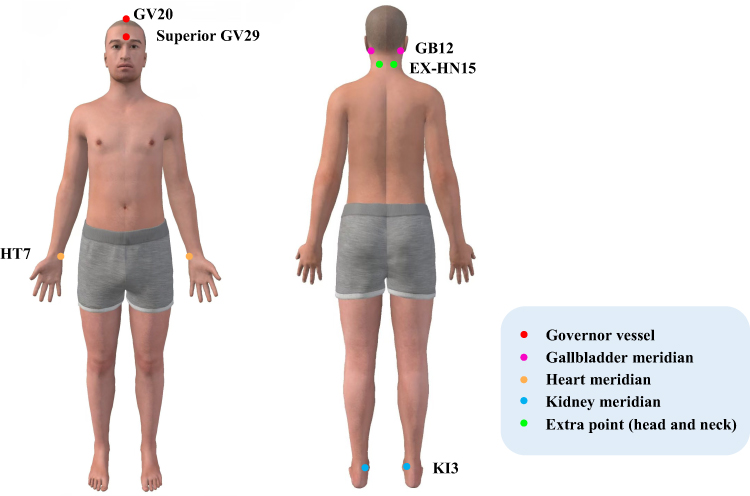 |
Figure 3 Locations of the selected acupuncture points. Colors indicate different meridians; the individualized ashi point is not displayed because its location varies by participant. |
Acupuncture Group
Sterile disposable stainless-steel needles (Hwato brand; Suzhou Medical Appliance Factory, Suzhou, China; diameter 0.30 mm; length 25 mm or 40 mm) will be used. After skin disinfection, needles will be inserted through the adhesive pads to an intended depth of approximately 10–30 mm according to point location and participant body habitus. Manual stimulation (lifting, thrusting, and rotating) will be applied to elicit deqi, characterized by sensations such as soreness, numbness, distension, or heaviness.38 Needles will be retained for 30 minutes, with additional manual stimulation every 10 minutes. Treatment will be administered 3 times per week, preferably on alternate days, for 4 consecutive weeks (12 sessions in total).
Sham Acupuncture Group
The sham procedure is designed to maximize treatment credibility and participant masking while minimizing specific acupuncture stimulation.34,39 Blunt-tipped placebo needles (Hwato brand; diameter 0.30 mm; length 25 mm) will be applied through visually identical adhesive pads at the same points used in the acupuncture group (Figure 4). At all acupoints except GV20, the placebo needles will touch the skin but will not penetrate it, and no attempt will be made to elicit deqi. At GV20, where adhesive-pad fixation is impractical, a sterile needle will be inserted superficially (approximately 2 mm) without manipulation to maintain visual comparability while minimizing specific stimulation. Session duration, participant positioning, therapist-participant interaction, and treatment frequency will be identical to those in the acupuncture group. This comparator was selected as a credible, low-intensity control that preserves participant blinding while helping to isolate the specific effect of acupuncture.34,39
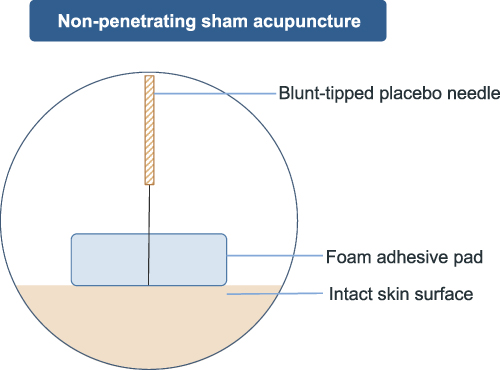 |
Figure 4 Illustration of the non-penetrating sham acupuncture procedure. |
Outcome Measurements
Outcome assessments will be performed at baseline and at weeks 4, 8, and 16. Each assessment is expected to take approximately 30 minutes to complete. Treatment credibility and expectancy will be assessed at baseline. Blinding success will be evaluated after completion of treatment. Medication use and adverse events will be recorded throughout the study.
The co-primary outcomes are the changes from baseline in AP-NRS and ISI at week 4. Average neck pain intensity will be measured with AP-NRS, an 11-point Numerical Rating Scale ranging from 0 (no pain) to 10 (worst imaginable pain). Participants will record their average neck pain intensity on 3 separate days during each assessment week, and the weekly mean will be used for analysis. For chronic pain trials, a reduction of approximately 2 points or 30% is generally regarded as clinically important.40 Insomnia severity will be measured with the ISI, a validated 7-item instrument with a score range of 0–28.41 A reduction of 6 points will be considered clinically important.42,43
Secondary outcomes are as follows: (1) changes from baseline in AP-NRS at weeks 8 and 16; (2) changes from baseline in ISI at weeks 8 and 16; (3) the proportion of participants achieving a ≥30% reduction in AP-NRS at weeks 4, 8, and 16; (4) the proportion of participants achieving a ≥6-point reduction in ISI at weeks 4, 8, and 16; (5) the proportion of participants achieving both a ≥30% reduction in AP-NRS and a ≥6-point reduction in ISI at weeks 4, 8, and 16; (6) changes from baseline in the Neck Disability Index (NDI) at weeks 4, 8, and 16; (7) the proportion achieving a ≥3.5-point reduction in NDI at weeks 4, 8, and 16; (8) changes in Numerical Rating Scale for maximum neck pain (MP-NRS) during neck movement at weeks 4, 8, and 16; (9) changes in Pittsburgh Sleep Quality Index (PSQI) scores at weeks 4, 8, and 16; (10) changes in Hospital Anxiety and Depression Scale (HADS) scores at weeks 4, 8, and 16; (11) Patient Global Impression of Change (PGIC) at weeks 4 and 16; and (12) use of analgesic or hypnotic medication during the study.
Neck-related disability will be measured with the NDI, a widely used and validated 10-item questionnaire; a change of approximately 3.5 points has been reported as clinically important in neck-pain populations.44–46 MP-NRS will be assessed during flexion, extension, lateral bending, and rotation, with an 11-point Numerical Rating Scale ranging from 0 (no pain) to 10 (worst imaginable pain). Subjective sleep quality will be measured with the PSQI, a widely used and validated instrument for subjective sleep assessment.47 Anxiety and depression symptoms will be evaluated using the HADS, a validated questionnaire developed for detecting anxiety and depression symptoms in medical settings.48 PGIC will be rated on a 7-point scale ranging from “very much improved” to “very much worse”.
Blinding assessment will be performed at week 4 by asking participants whether they believe they received acupuncture, sham acupuncture, or are uncertain. Responses will be summarized descriptively and analyzed using Bang’s Blinding Index.49 Safety will be assessed through active surveillance at each visit. Adverse events will be categorized by type, severity (mild, moderate, or severe), seriousness, and relatedness to treatment (unrelated, possibly related, probably related, or definitely related). Serious adverse events will be reported to the coordinating center and the ethics committee within 24 hours.
Patient Compliance and Concomitant Interventions
Attendance at treatment sessions and completion of follow-up visits will be recorded to assess adherence. Reasons for withdrawal, protocol deviation, and loss to follow-up will be documented in detail.
During the 4-week treatment phase, initiation of other non-study interventions specifically targeting neck pain or insomnia will be discouraged and recorded if it occurs. Stable pre-existing hypnotic medication is allowed as described above. If symptoms become intolerable, participants may receive rescue care according to routine practice at the participating center; all rescue medication and additional treatment will be recorded and considered in sensitivity analyses.
Sample Size
The sample size was determined on the basis of the co-primary outcomes. Using data from a previous sham-controlled trial of acupuncture for chronic neck pain,23 36 participants per group would provide 80% power at a two-sided α of 0.05 to detect a statistically significant between-group difference in change from baseline in AP-NRS. Using data from a sham-controlled trial of acupuncture for insomnia,50 54 participants per group would be required to detect a statistically significant between-group difference in ISI change. The larger estimate was adopted to ensure adequate power for both symptom domains. Assuming a 15% attrition rate, the final target sample size is 64 participants per group (128 participants in total).
Statistical Analysis
All efficacy analyses will follow the intention-to-treat principle and will include all randomized participants according to their assigned groups. Baseline characteristics will be summarized descriptively but will not be subjected to significance testing for group balance.
To control the family-wise type I error rate for the co-primary outcomes, a fixed-sequence testing strategy will be used. The between-group difference in change from baseline in AP-NRS at week 4 will be tested first. If significant at the two-sided 0.05 level, the between-group difference in change from baseline in ISI at week 4 will then be tested at the same α level. Continuous longitudinal outcomes, including AP-NRS, ISI, NDI, MP-NRS, PSQI, and HADS, will be analyzed using linear mixed-effects models with fixed effects for treatment group, time, treatment-by-time interaction, study center, and baseline value, together with a participant-level random effect. Binary responder outcomes will be analyzed using generalized linear mixed-effects models.
Medication use, protocol deviations, and adverse events will be summarized descriptively. Missing data for repeated continuous outcomes will be handled within the mixed-model framework under a missing-at-random assumption. For the co-primary outcomes, multiple imputation and per-protocol analyses will be conducted as sensitivity analyses. All secondary analyses will be considered exploratory, and no adjustment for multiplicity will be made. Statistical analyses will be performed using R software.
Data Management and Quality Control
All trial data will be entered into centralized electronic case report forms hosted on a password-protected electronic data capture platform managed by INTELING Tech Co., Ltd. The platform will maintain user-specific permissions, range checks, data-validation rules, and an audit trail for all entries and modifications. Source documents, informed consent forms, treatment logs, and adverse-event records will be stored securely at each site with restricted access.
Guang’anmen Hospital, China Academy of Chinese Medical Sciences, will serve as the coordinating center. Before trial initiation, all investigators and study staff will complete standardized training in participant screening, informed consent, intervention delivery, data entry, and safety reporting. An independent clinical monitor will periodically review recruitment, consent documentation, protocol adherence, and data quality. Because the trial involves a short intervention period and a low-risk nonpharmacological intervention, a separate data monitoring committee has not been established; however, serious adverse events and major protocol deviations will be reviewed promptly by the principal investigator and reported to the ethics committee in accordance with institutional requirements. No interim efficacy analysis is planned.
Ethics and Dissemination
The study has been approved by the Ethics Committee of Guang’anmen Hospital, China Academy of Chinese Medical Sciences (Approval No. 2025-090-KY) and registered at ClinicalTrials.gov (NCT06996210). The trial will be conducted in accordance with the Declaration of Helsinki and Good Clinical Practice principles.
Participants will be assigned unique identification codes, and directly identifying information will not be disclosed in publications. Appropriate medical evaluation and treatment will be provided for study-related adverse events, and associated reporting and compensation procedures will follow ethics-committee requirements and local regulations. After study completion, participants will return to or continue routine clinical care at the participating centers as clinically indicated; no trial-specific post-study treatment is mandated by the protocol. The results of the study will be disseminated through peer-reviewed journals and academic conferences.
Patient and Public Involvement
No patients or members of the public were involved in the design of the protocol, selection of outcome measures, or development of the dissemination plan.
Discussion
Comorbid CNSNP and chronic insomnia represent a clinically important but understudied therapeutic target. Because pain and sleep disturbance aggravate one another, a treatment strategy focused on only one domain may leave clinically meaningful symptoms unresolved.12,15,17 In routine practice, patients with neck pain and insomnia often present with overlapping pain, fatigue, impaired daytime functioning, anxiety, and low mood. These interacting manifestations may sustain symptom chronicity and complicate management, particularly when access to comprehensive nonpharmacological care is limited. The present protocol was therefore developed to test an acupuncture strategy targeting two coexisting symptom domains in a population that reflects common outpatient clinical practice while preserving rigorous methodological control.
The trial addresses an important evidence gap in the management of comorbid chronic neck pain and insomnia. More importantly, it was designed to address several methodological limitations of the existing literature by using a multicenter design, a sham-controlled comparator, formal blinding assessment, and prespecified co-primary outcomes for both pain and insomnia. Rather than focusing on a single symptom domain, the study evaluates the two core manifestations of the comorbidity simultaneously, which may improve the clinical interpretability of the findings. In addition, the protocol incorporates validated patient-reported outcomes and responder definitions anchored to clinically important thresholds, while detailed recording of analgesic and hypnotic medication use will allow a more nuanced interpretation of treatment effects in a setting that resembles real-world clinical practice. In this respect, the study is expected not only to provide efficacy data but also to offer a more rigorous methodological framework for future confirmatory and pragmatic trials in pain-sleep comorbidity.
The sham comparator was selected to balance methodological rigor against practical feasibility. Non-penetrating sham acupuncture can improve participant masking and reduce expectation-related bias, but it may still exert contextual or sensory effects and therefore should not be viewed as a completely inert placebo. For this reason, any between-group difference observed in the present trial is likely to reflect the incremental benefit of acupuncture beyond the effects of attention, ritual, and low-intensity tactile stimulation. This makes the comparison clinically meaningful while maintaining methodological credibility.
The biologic rationale for acupuncture in this comorbidity is plausible but remains incompletely understood. Experimental and clinical studies suggest that acupuncture may modulate peripheral nociceptive input, descending pain inhibition, inflammatory signaling, autonomic regulation, and central neural networks implicated in pain processing.51–54 For insomnia, proposed mechanisms include modulation of hyperarousal, limbic regulation, neurotransmitter systems, inflammatory pathways, and sleep-related brain networks.36,55–57 These mechanisms may be especially relevant when pain and insomnia coexist, because both conditions involve altered arousal, affective distress, and central pain processing. Nevertheless, mechanistic inferences should remain cautious. The current trial is designed to establish clinical efficacy and safety rather than to determine causal neurobiological pathways.
The trial also has limitations. Acupuncturists cannot be blinded, which creates the possibility of performance bias despite protocol standardization and centralized training. The sham acupuncture, although credible and low intensity, is unlikely to be fully inert, especially because minimal superficial stimulation is used at GV20 for technical reasons. In addition, the protocol emphasizes patient-reported outcomes rather than physiologic sleep measures such as polysomnography or actigraphy. This choice improves feasibility across six centers and aligns with the symptomatic focus of the trial, but it limits physiologic interpretation. The 12-week post-treatment follow-up will provide useful medium-term information, yet it will not fully address long-term durability. Finally, allowing stable pre-existing hypnotic treatment increases external validity but may introduce some heterogeneity, which is why medication exposure will be documented carefully and explored in sensitivity analyses.
Despite these limitations, the study is expected to provide clinically relevant evidence. If acupuncture proves superior to sham acupuncture, it could represent a useful nonpharmacological option for patients with comorbid CNSNP and chronic insomnia, particularly for those with incomplete response to, contraindications to, or poor access to standard treatments such as CBT-I or medication. If the findings are neutral, the trial will still help refine future research by informing decisions about outcome selection, sham control, treatment dose, and the incorporation of objective sleep measures. In either case, the study will advance the evidence base for the management of comorbid chronic neck pain and insomnia and may support the design of future pragmatic, mechanistic, and cost-effectiveness studies.
Data Sharing Statement
The data generated in this study will be available from the corresponding author, Zhishun Liu, upon reasonable request and in accordance with institutional and ethical requirements.
Ethics Approval and Consent to Participate
This study has received ethical approval from the Ethics Committee of Guang’anmen Hospital, China Academy of Chinese Medical Sciences (Approval No. 2025-090-KY). Written informed consent will be obtained from all participants before enrollment.
Acknowledgments
Sixing Liu and He Chen are co-first authors for this study. Zhishun Liu and Guangxia Shi are co-corresponding authors for this study. The authors thank 3Dbody (Shanghai) Digital Technology Co., Ltd. for permission to use their anatomy images to illustrate the locations of the selected acupuncture points.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work is supported by the High-Level Chinese Medical Hospital Promotion Project (HLCMHPP2023089). The funder has no role in study design, intervention delivery, data collection, data analysis, interpretation, or publication decisions.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Global Burden of Disease Collaborative Network. Global Burden of Disease Study 2023 (GBD 2023). Seattle, United States: Institute for Health Metrics and Evaluation (IHME); 2025. Available from: https://vizhub.healthdata.org/gbd-results/.
2. Benjafield AV, Sert Kuniyoshi FH, Malhotra A, et al. Estimation of the global prevalence and burden of insomnia: a systematic literature review-based analysis. Sleep Med Rev. 2025;82:102121. doi:10.1016/j.smrv.2025.102121
3. Cao XL, Wang SB, Zhong BL, et al. The prevalence of insomnia in the general population in China: a meta-analysis. PLoS One. 2017;12(2):e0170772. doi:10.1371/journal.pone.0170772
4. Morin CM, Drake CL, Harvey AG, et al. Insomnia disorder. Nat Rev Dis Primers. 2015;1:15026. doi:10.1038/nrdp.2015.26
5. Riemann D, Nissen C, Palagini L, Otte A, Perlis ML, Spiegelhalder K. The neurobiology, investigation, and treatment of chronic insomnia. Lancet Neurol. 2015;14(5):547–13. doi:10.1016/s1474-4422(15)00021-6
6. Sutton EL. Insomnia. Ann Intern Med. 2021;174(3):ITC33–ITC48. doi:10.7326/aitc202103160
7. Léger D, Bayon V. Societal costs of insomnia. Sleep Med Rev. 2010;14(6):379–389. doi:10.1016/j.smrv.2010.01.003
8. Treede RD, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the International Classification of Diseases (ICD-11). Pain. 2019;160(1):19–27. doi:10.1097/j.pain.0000000000001384
9. Castellini G, Pillastrini P, Vanti C, et al. Some conservative interventions are more effective than others for people with chronic non-specific neck pain: a systematic review and network meta-analysis. J Physiother. 2022;68(4):244–254. doi:10.1016/j.jphys.2022.09.007
10. American Academy of Sleep Medicine. International Classification of Sleep Disorders (3rd Ed.). Darien, IL: American Academy of Sleep Medicine; 2014.
11. Artner J, Cakir B, Spiekermann JA, et al. Prevalence of sleep deprivation in patients with chronic neck and back pain: a retrospective evaluation of 1016 patients. J Pain Res. 2013;6:1–6. doi:10.2147/jpr.S36386
12. Finan PH, Goodin BR, Smith MT. The association of sleep and pain: an update and a path forward. J Pain. 2013;14(12):1539–1552. doi:10.1016/j.jpain.2013.08.007
13. Kim SH, Lee DH, Yoon KB, An JR, Yoon DM. Factors associated with increased risk for clinical insomnia in patients with chronic neck pain. Pain Physician. 2015;18(6):593–598.
14. Jank R, Gallee A, Boeckle M, Fiegl S, Pieh C. Chronic pain and sleep disorders in primary care. Pain Res Treat. 2017;2017:9081802. doi:10.1155/2017/9081802
15. Haack M, Simpson N, Sethna N, Kaur S, Mullington J. Sleep deficiency and chronic pain: potential underlying mechanisms and clinical implications. Neuropsychopharmacology. 2020;45(1):205–216. doi:10.1038/s41386-019-0439-z
16. Yabe Y, Hagiwara Y, Sekiguchi T, et al. Sleep disturbance is associated with neck pain: a 3-year longitudinal study after the Great East Japan Earthquake. BMC Musculoskelet Disord. 2022;23(1):459. doi:10.1186/s12891-022-05410-w
17. Zhu M, Huang H. The underlying mechanisms of sleep deprivation exacerbating neuropathic pain. Nat Sci Sleep. 2023;15:579–591. doi:10.2147/nss.S414174
18. Edinger JD, Arnedt JT, Bertisch SM, et al. Behavioral and psychological treatments for chronic insomnia disorder in adults: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2021;17(2):255–262. doi:10.5664/jcsm.8986
19. Barkopoulos P, Cho JH. Hypnotic medications as an adjunct treatment to cognitive behavioral therapy for insomnia. Sleep Med Clin. 2023;18(1):95–111. doi:10.1016/j.jsmc.2022.10.004
20. Sateia MJ, Buysse DJ, Krystal AD, Neubauer DN, Heald JL. Clinical practice guideline for the pharmacologic treatment of chronic insomnia in adults: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2017;13(2):307–349. doi:10.5664/jcsm.6470
21. Hintze JP, Edinger JD. Hypnotic discontinuation in chronic insomnia. Sleep Med Clin. 2020;15(2):147–154. doi:10.1016/j.jsmc.2020.02.003
22. Morin CM, Edinger JD, Beaulieu-Bonneau S, et al. Effectiveness of sequential psychological and medication therapies for insomnia disorder: a randomized clinical trial. JAMA Psychiatry. 2020;77(11):1107–1115. doi:10.1001/jamapsychiatry.2020.1767
23. White P, Lewith G, Prescott P, Conway J. Acupuncture versus placebo for the treatment of chronic mechanical neck pain: a randomized, controlled trial. Ann Intern Med. 2004;141(12):911–919. doi:10.7326/0003-4819-141-12-200412210-00007
24. Fang J, Shi H, Wang W, et al. Durable effect of acupuncture for chronic neck pain: a systematic review and meta-analysis. Curr Pain Headache Rep. 2024;28(9):957–969. doi:10.1007/s11916-024-01267-x
25. Zhao L, Sun M, Yin Z, et al. Long-Term effects of individualized acupuncture for chronic neck pain: a randomized controlled trial. Ann Intern Med. 2024;177(10):1330–1338. doi:10.7326/m23-2425
26. Yin X, Gou M, Xu J, et al. Efficacy and safety of acupuncture treatment on primary insomnia: a randomized controlled trial. Sleep Med. 2017;37:193–200. doi:10.1016/j.sleep.2017.02.012
27. Yin X, Li W, Wu H, et al. Efficacy of electroacupuncture on treating depression-related insomnia: a randomized controlled trial. Nat Sci Sleep. 2020;12:497–508. doi:10.2147/nss.S253320
28. Yin X, Li W, Liang T, et al. Effect of electroacupuncture on insomnia in patients with depression: a randomized clinical trial. JAMA Network Open. 2022;5(7):e2220563. doi:10.1001/jamanetworkopen.2022.20563
29. Chen H, Chen W, Qin M, Yang Y, Su L. Clinical observation of scalp acupuncture of Lingnan flying needle therapy in the treatment of cervicogenic insomnia. J Guangzhou Univer Tradit Chin Med. 2022;39(6):1319–1322. doi:10.13359/j.cnki.gzxbtcm.2022.06.017
30. Zhang L, Guo L, Yin T, Chen A. Clinical effect of floating needle therapy on cervical insomnia. Systems Med. 2024;9(11):172–175. doi:10.19368/j.cnki.2096-1782.2024.11.172
31. Li M, Zhang H. Effect of auricular point intervention combined with mindfulness meditation on pain and sleep quality in patients with cervical spondylosis and insomnia. World J Sleep Med. 2025;12(9):2004–2006.
32. Chan AW, Boutron I, Hopewell S, et al. SPIRIT 2025 statement: updated guideline for protocols of randomized trials. Nat Med. 2025;31(6):1784–1792. doi:10.1038/s41591-025-03668-w
33. MacPherson H, Altman DG, Hammerschlag R, et al. Revised Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): extending the CONSORT statement. PLoS Med. 2010;7(6):e1000261. doi:10.1371/journal.pmed.1000261
34. Ma P, Liu X, Liu Z, et al. The SHARE: SHam Acupuncture REporting guidelines and a checklist in clinical trials. J Evid Based Med. 2023;16(4):428–431. doi:10.1111/jebm.12560
35. Hróbjartsson A, Boutron I, Hopewell S, et al. SPIRIT 2025 explanation and elaboration: updated guideline for protocols of randomised trials. BMJ. 2025:389: e081660. doi:10.1136/bmj-2024-081660
36. Zhao FY, Spencer SJ, Kennedy GA, et al. Acupuncture for primary insomnia: effectiveness, safety, mechanisms and recommendations for clinical practice. Sleep Med Rev. 2024;74:101892. doi:10.1016/j.smrv.2023.101892
37. Standardization Administration of the People’s Republic of China. GB/T 12346-2021, nomenclature and location of acupuncture points. 2021.
38. Zhong Z, Yao L, Liu YZ, et al. Objectivization study of acupuncture Deqi and brain modulation mechanisms: a review. Front Neurosci. 2024;18:1386108. doi:10.3389/fnins.2024.1386108
39. Park J, White A, Stevinson C, Ernst E, James M. Validating a new non-penetrating sham acupuncture device: two randomised controlled trials. Acupunct Med. 2002;20(4):168–174. doi:10.1136/aim.20.4.168
40. Farrar JT, Young JP Jr, LaMoreaux L, Werth JL, Poole MR. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94(2):149–158. doi:10.1016/s0304-3959(01)00349-9
41. Bastien CH, Vallières A, Morin CM. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Med. 2001;2(4):297–307. doi:10.1016/s1389-9457(00)00065-4
42. Yang M, Morin CM, Schaefer K, Wallenstein GV. Interpreting score differences in the Insomnia Severity Index: using health-related outcomes to define the minimally important difference. Curr Med Res Opin. 2009;25(10):2487–2494. doi:10.1185/03007990903167415
43. Qin Z, Zhu Y, Shi DD, Chen R, Li S, Wu J. The gap between statistical and clinical significance: time to pay attention to clinical relevance in patient-reported outcome measures of insomnia. BMC Med Res Methodol. 2024;24(1):177. doi:10.1186/s12874-024-02297-0
44. Vernon H, Mior S. The Neck Disability Index: a study of reliability and validity. J Manipulative Physiol Ther. 1991;14(7):409–415.
45. Pool JJ, Ostelo RW, Hoving JL, Bouter LM, De Vet HC. Minimal clinically important change of the neck disability index and the numerical rating scale for patients with neck pain. Spine. 2007;32(26):3047–3051. doi:10.1097/BRS.0b013e31815cf75b
46. Jorritsma W, Dijkstra PU, de Vries GE, Geertzen JH, Reneman MF. Detecting relevant changes and responsiveness of neck pain and disability scale and neck disability index. Eur Spine J. 2012;21(12):2550–2557. doi:10.1007/s00586-012-2407-8
47. Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
48. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x.
49. Bang H, Ni L, Davis CE. Assessment of blinding in clinical trials. Control Clin Trials. 2004;25(2):143–156. doi:10.1016/j.cct.2003.10.016
50. Zhang J, Qin Z, So TH, et al. Acupuncture for chemotherapy-associated insomnia in breast cancer patients: an assessor-participant blinded, randomized, sham-controlled trial. Breast Cancer Res. 2023;25(1):49. doi:10.1186/s13058-023-01645-0
51. Zhao ZQ. Neural mechanism underlying acupuncture analgesia. Prog Neurobiol. 2008;85(4):355–375. doi:10.1016/j.pneurobio.2008.05.004
52. Zhang R, Lao L, Ren K, Berman BM. Mechanisms of acupuncture-electroacupuncture on persistent pain. Anesthesiology. 2014;120(2):482–503. doi:10.1097/aln.0000000000000101
53. Fan Z, Dou B, Wang J, et al. Effects and mechanisms of acupuncture analgesia mediated by afferent nerves in acupoint microenvironments. Front Neurosci. 2023;17:1239839. doi:10.3389/fnins.2023.1239839
54. He L, Zhou R, Hou S, et al. Exploration of key brain regions involved in acupuncture and moxibustion analgesia: an imaging-based study. J Pain Res. 2025;18:2051–2067. doi:10.2147/jpr.S505312
55. Wang YK, Li T, Ha LJ, et al. Effectiveness and cerebral responses of multi-points acupuncture for primary insomnia: a preliminary randomized clinical trial and fMRI study. BMC Complement Med Ther. 2020;20(1):254. doi:10.1186/s12906-020-02969-6
56. Shi XH, Wang YK, Li T, et al. Gender-related difference in altered fractional amplitude of low-frequency fluctuations after electroacupuncture on primary insomnia patients: a resting-state fMRI study. Brain Behav. 2021;11(1):e01927. doi:10.1002/brb3.1927
57. Zang S, Chen Y, Chen H, Shi H, Zhou L. Effects of acupuncture on the brain in primary insomnia: a coordinate-based meta-analysis of fMRI studies. Front Neurol. 2023;14:1180393. doi:10.3389/fneur.2023.1180393
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.