Back to Journals » Journal of Pain Research » Volume 18
Acupuncture at Myofascial Trigger Points Versus Conventional Acupuncture for Knee Osteoarthritis: A Protocol for a Randomized Controlled Trial
Authors Zhang C ![]() , Xue H, Xu J, Liu A
, Xue H, Xu J, Liu A ![]() , Gao K, Zhang L
, Gao K, Zhang L ![]()
Received 10 June 2025
Accepted for publication 3 September 2025
Published 11 September 2025 Volume 2025:18 Pages 4743—4753
DOI https://doi.org/10.2147/JPR.S545853
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Chao Zhang,1,2,* Hongfei Xue,1,2,* Jiankang Xu,1,2,* Aifeng Liu,1,2 Kuiliang Gao,1,2 Longyao Zhang1,2
1Orthopedics Department, The First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, Tianjin, People’s Republic of China; 2National Clinical Research Center for Chinese Medicine Acupuncture and Moxibustion, Tianjin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Longyao Zhang, Orthopedics Department, The First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, Tianjin, People’s Republic of China, Email [email protected] Kuiliang Gao, Orthopedics Department, The First Teaching Hospital of Tianjin University of Traditional Chinese Medicine, Tianjin, People’s Republic of China, Email [email protected]
Background: Knee osteoarthritis (KOA) is a prevalent degenerative joint disease that significantly impacts pain and mobility. Acupuncture targeting Myofascial Trigger Points (MTrPs), guided by the “pain as acupoint” strategy, has been proposed as a more precise intervention approach.
Objective: This study aims to compare the efficacy of MTrP acupuncture versus conventional acupuncture in patients with early- to mid-stage KOA.
Methods: In this assessor-blinded randomized controlled trial, 106 KOA patients (Kellgren–Lawrence grade II/III) will be randomly assigned (1:1) to receive either conventional meridian-based acupuncture (Group A) or acupuncture targeting both meridian points and MTrPs (Group B). Both groups will receive treatment five times weekly for two weeks. The primary outcome is the response rate, defined as a ≥ 2-point reduction in VAS and ≥ 6-point improvement in WOMAC function score. Secondary outcomes include pressure pain threshold (PPT), three-dimensional gait analysis, and patient acceptability.
Results: This study is expected to demonstrate whether MTrP acupuncture provides superior pain relief and functional improvement compared to conventional acupuncture.
Conclusion: Findings will contribute novel clinical evidence for optimizing individualized acupuncture strategies in the management of KOA.
Trial Registration: ChiCTR, ChiCTR2300073707, Registered on July 19, 2023.
Keywords: knee osteoarthritis, acupuncture, myofascial trigger points, individualized treatment, clinical trial
Background
Knee Osteoarthritis (KOA) is a chronic degenerative disease caused by multiple factors, such as mechanical and chemical influences. Its primary pathological characteristics include changes in intra- and extra-articular tissues, such as degenerative alterations in cartilage, subchondral bone sclerosis or cystic changes, joint space narrowing, synovial inflammation, meniscus damage, and surrounding ligament contracture. Clinically, KOA manifests as recurrent knee pain, swelling, stiffness, and functional impairment.1,2 With the improvement of living standards, an aging population, and rising obesity rates, the prevalence of KOA continues to increase. Studies have shown that approximately 15% of the Chinese population suffers from KOA, with prevalence closely related to age. The incidence is relatively low in younger populations, while among individuals over 40 years old, the prevalence ranges from 10% to 17%. In people over 60 years old, the prevalence can reach up to 50%, and in those over 75, it can be as high as 80%. KOA has become one of the leading causes of pain and disability in elderly individuals.3 In advanced stages, KOA often leads to severe functional limitations, resulting in reduced physical activity and disability, placing a significant burden on both society and families. It accounts for approximately 85% of the global osteoarthritis burden. Therefore, research on KOA is of great significance, particularly in pain relief and functional improvement, where an integrated approach combining traditional Chinese and Western medicine plays a crucial role. Recent authoritative studies have demonstrated that acupuncture has significant efficacy in the treatment of chronic pain conditions. Clinical research consistently reports that acupuncture can effectively reduce pain intensity, enhance functional mobility, and improve overall quality of life, leading to its widespread application in clinical settings.4,5 Meta-analyses of numerous acupuncture clinical studies involving KOA patients have consistently indicated the potential effectiveness of acupuncture as a therapeutic intervention.6,7
Furthermore, studies have found a high correlation between myofascial trigger points (MTrPs) and KOA, particularly in the gastrocnemius and vastus medialis muscles, where the prevalence of MTrPs can reach 50%–100%.8 MTrPs are highly sensitive points located in taut bands of muscle fibers that present with spontaneous or pressure-induced pain, often accompanied by referred pain, muscle stiffness, and restricted movement.9 MTrPs have been confirmed to be associated with various chronic musculoskeletal pain conditions, such as neck and shoulder pain, lower back pain, and chronic pelvic pain.10–12 In KOA patients, MTrPs are highly prevalent. Studies have shown that in patients with mild to moderate KOA, the prevalence of MTrPs in muscles such as the vastus medialis and gastrocnemius ranges from 11% to 50%.8 In patients awaiting total knee arthroplasty, the prevalence of MTrPs is nearly 100%.13 These findings suggest that MTrPs may play a crucial role in the onset and persistence of KOA-related pain.
In traditional Chinese medicine (TCM) theory, the treatment principles for KOA pain emphasize “treating with fire needling and bleeding techniques, selecting points based on tenderness and pain localization”, meaning that acupuncture point selection is primarily based on the patient’s reported pain sites, known as “Ashi points”.14 The distribution characteristics of MTrPs closely align with the principles of Ashi point selection. Given their similarities in clinical point selection and treatment methods, some researchers consider MTrPs to be a microscopic and refined representation of Ashi points.15 Based on this perspective, acupuncture at MTrPs can be regarded as a modern interpretation of the “selecting points based on pain localization” principle in acupuncture treatment.
Previous studies have confirmed that acupuncture targeting MTrPs can effectively alleviate KOA-related pain and improve joint function.16 However, there is still a lack of high-quality randomized controlled trials comparing MTrP acupuncture with conventional acupuncture protocols. Moreover, the synergistic effects of combining traditional meridian acupuncture with MTrP acupuncture in KOA remain insufficiently studied, particularly with regard to objective outcome measures and underlying biomechanical mechanisms. The progression of KOA is not only closely associated with chemical factors such as inflammatory cytokines and neurotransmitters but also with biomechanical factors including abnormal joint stress distribution and lower limb muscle dysfunction.17 Studies have shown that gait parameters, periarticular muscle conditions, and plantar pressure distribution in KOA patients are correlated with disease severity. Therefore, exploring the mechanisms of acupuncture intervention for KOA from a biomechanical perspective holds significant clinical value.18
This study is based on the acupuncture principle of “treating where the pain is” and focuses on early-to-mid KOA patients. It employs traditional acupuncture combined with MTrP needling to systematically evaluate clinical efficacy and biomechanical effects. Pain and functional scales (VAS, WOMAC) and PPT values assess clinical outcomes, while three-dimensional gait analysis (3DGA) explores the biomechanical mechanisms of acupuncture for KOA. This study aims to reveal the clinical and biomechanical effects of acupuncture through a multimodal evaluation, providing objective evidence for precision acupuncture treatment and advancing TCM-WM integration in KOA management. We hypothesize that compared to acupuncture at acupoints alone, combined acupuncture targeting both acupoints and MTrPs will not only provide more significant symptom improvement but also achieve better correction of biomechanical function.
Methods
Study Design
This is a parallel, two-group randomized controlled exploratory study with an 8-week follow-up period. The protocol has been registered in the Chinese Clinical Trial Registry (Registration No. ChiCTR2300073707) and will be conducted in accordance with the Declaration of Helsinki. The study will be reported following the Consolidated Standards of Reporting Trials (CONSORT) statement and its relevant extensions for randomized trials. The protocol is reported in accordance with the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT)19 (Supplementary Material 1). An overview of the patient flow in the study is shown in Figure 1 and Table 1.
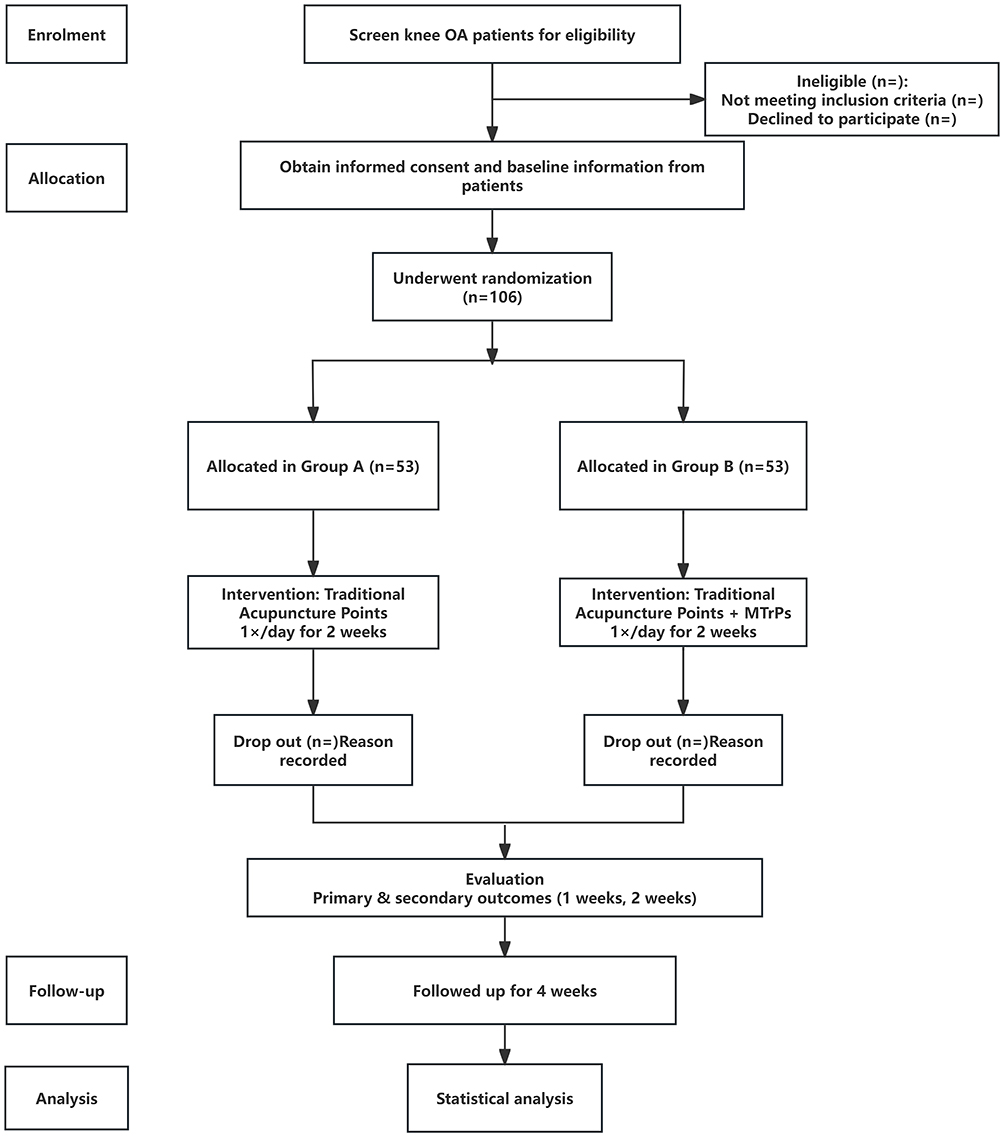 |
Figure 1 Trial flow chart: Consolidated Standards of Reporting Trials (CONSORT) diagram. OA: Osteoarthritis. Notes: CONSORT figure adapted from Schulz KF, Altman DG, Moher D. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. PLoS Med. 2010;7(3): e1000251. Copyright: © 2010 Schulz et al. Creative Commons Attribution License.20 |
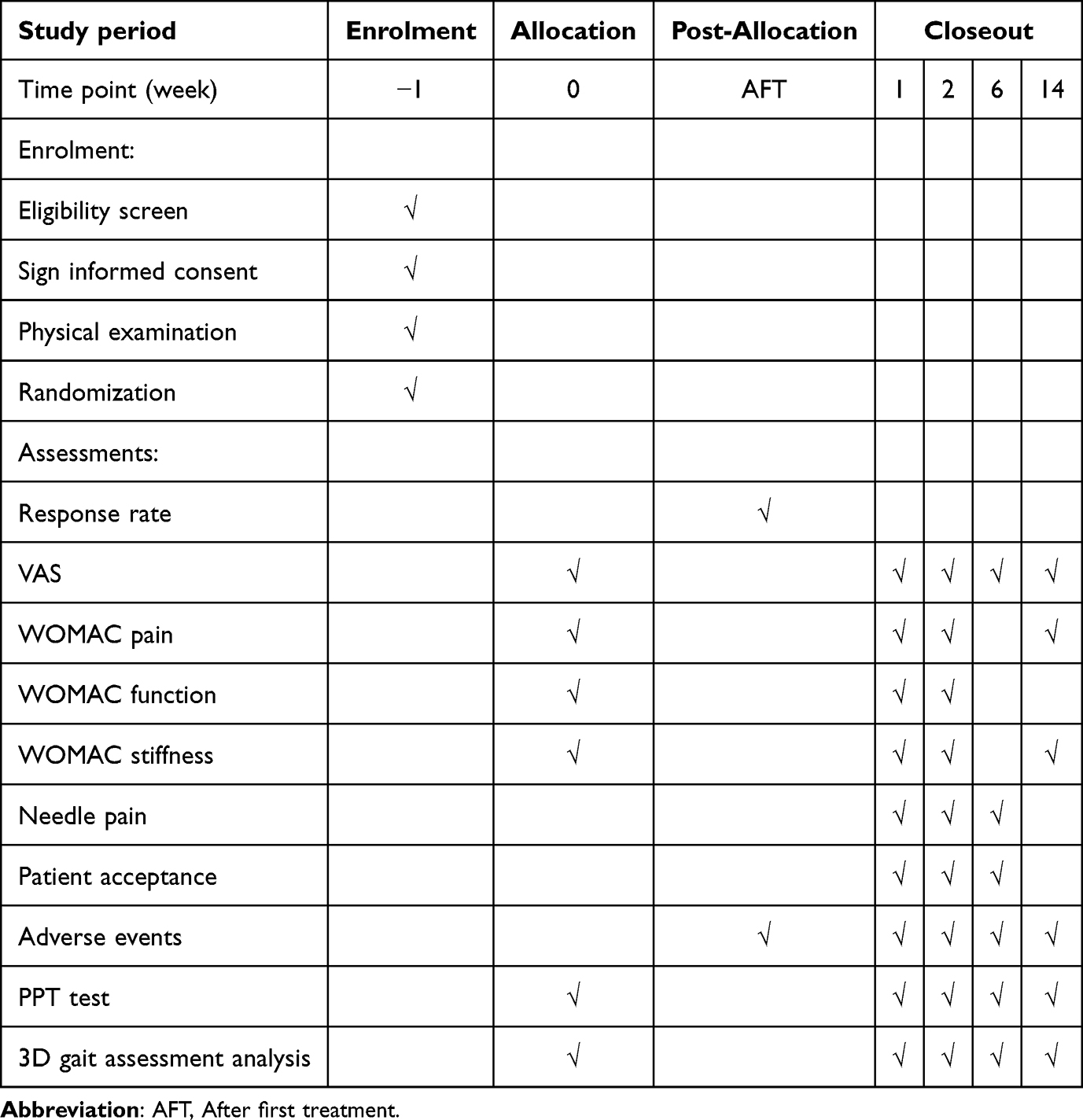 |
Table 1 Schedule of Enrolment, Interventions, and Assessments |
Study Setting, Recruitment, and Ethics
Recruitment will take place at the First Teaching Hospital of Tianjin University of Traditional Chinese Medicine. The study aims to enroll 106 KOA patients using acupuncture students. Ethical approval has been granted by the Medical Ethics Committee of the First Teaching Hospital of Tianjin University of Traditional Chinese Medicine (Approval No. TYLL2023[K]011).
Patients will be recruited through WeChat (a social networking platform), outpatient clinics, and printed advertisements. Individuals interested in participating will be invited to contact the clinical research coordinator via phone. The CRC will conduct an initial screening based on the inclusion and exclusion criteria and, if appropriate, schedule a face-to-face baseline visit with a senior physiotherapy specialist. Patients will also be offered a free radiographic assessment.
All eligible patients will provide written informed consent. The CRC will discuss the study in detail with potential participants (including study objectives, procedures, time commitments, and potential risks and benefits) before obtaining written consent. Patient record confidentiality will be protected. Upon enrollment, each patient will be assigned a unique random number, which will serve as the only direct identifier in all case report forms.
Inclusion Criteria
- Age between 18 and 70 years, male or female.
- Diagnosed with knee osteoarthritis according to the American College of Rheumatology criteria.
- Symptoms persisting for more than six months.
- Radiographically confirmed KOA (Kellgren–Lawrence grade II or III).
- Average knee pain severity ≥ 4 (on an 11-point numerical rating scale) over the past week.
- Agreement to avoid any analgesic medications during the trial (patients will be provided with long-acting antipyretic analgesic tablets if pain intensity reaches ≥ 8 on the 11-point scale).
- Signed informed consent.
Exclusion Criteria
- History of knee surgery or awaiting surgery (eg, knee replacement or arthroscopic surgery).
- Knee pain caused by other conditions (eg, loose bodies, severe joint effusion, infection, malignancy, autoimmune disease, or trauma).
- Underwent arthroscopic surgery in the past year or intra-articular injection within the past four months.
- Received acupuncture treatment in the past three months.
- Severe acute/chronic organic or psychiatric disorders.
- Pregnant or breastfeeding women.
- Coagulation disorders (eg, hemophilia).
- Participation in other clinical studies in the past three months.
- History of pacemaker implantation, metal allergy, or needle phobia.
Randomization and Blinding
This study employs a randomized controlled design with parallel groups. A total of 106 patients were randomly assigned to either the control group or the experimental group in a 1:1 ratio using SPSS 26. Randomization was performed with a predefined seed (2888) to ensure reproducibility. Patients were allocated based on a computer-generated random sequence, with numbers 1–53 assigned to the control group (conventional acupuncture) and 54–106 to the experimental group (acupoint combined with MTrP needling).
Due to the nature of the intervention, blinding of acupuncturists and patients was not feasible. However, outcome assessors and data analysts were blinded to group allocation to minimize bias. Due to the nature of the intervention, blinding of the acupuncturists and patients was not feasible.
Intervention
Patients were randomly assigned to Group A and Group B using a random number table Acupuncture treatment strategies are generally considered a practical compromise, requiring both a certain degree of standardization and personalization. This treatment is based on an excellent Chinese textbook and traditional Chinese medicine meridian theory to treat “Bi syndrome”. Additionally, the therapy has been discussed and refined by experts in the field of acupuncture and has shown significant efficacy in alleviating symptoms of early-to-mid KOA.
Group A
The conventional acupuncture control group used acupoints from clinical and medical textbooks for KOA treatment: Dubi, Neixiyan, Zusanli, Yanglingquan, Xuehai, Liangqiu, and Heding. Patients were in a supine position, with standard disinfection. A 0.25 mm × 40 mm needle was inserted 10–30 mm deep (based on acupoint). Manual stimulation for 10 seconds was applied to achieve “Deqi”. After “Deqi”, needles were retained for 30 minutes, once per day, 5 times a week, for 2 weeks.
Group B
The “treating where the pain is” MTrPs acupuncture group: The practitioner uses their left thumb to gently stabilize the site, while the right thumb applies pressure, pushing, circling, or lifting to identify tender points. Pain is categorized into 4 levels: mild tenderness (level 1), moderate tenderness (level 2), frowning/verbal pain (level 3), and pain that resists pressure (level 4). Points with level 3 or 4 tenderness are selected for treatment. In addition to conventional acupuncture, selected MTrPs are treated, with the same needle retention time, technique, and frequency as the control group. If both knees are affected, both may be treated, but MTrPs will only be applied to the more painful knee.
Acupuncturists must hold a licensed Traditional Chinese Medicine practitioner certificate and have at least 10 years of experience. If any adverse events occur, acupuncture treatment will be discontinued, and the acupuncturist may decide to terminate the trial. In cases of intolerable knee pain, patients will be instructed to use Tylenol as a rescue medication. The use of Tylenol will be recorded by the outcome assessors. Other treatments, such as any type of injection, moxibustion, auricular acupuncture, or cupping, are not permitted.
Outcome
Primary outcome Measurement
If only one knee is affected, the evaluation results will be related to that knee. If both knees are affected but only one meets the ACR criteria and is classified as Kellgren–Lawrence grade II or III, only that knee will be evaluated. If both knees meet the inclusion criteria (ACR and Kellgren–Lawrence grade II or III), the more painful knee will be randomly selected for evaluation.
Primary Outcome Measures: The pain VAS is a self-assessment tool where patients select a number from 0 to 10 to indicate the intensity of pain experienced over the past week, with 0 representing no pain and 10 representing the most severe pain. The WOMAC scale assesses participants’ ability to move and perform daily activities. It consists of 17 questions (each rated from 0 to 4) reflecting the difficulty in activities caused by KOA. A higher score indicates worse physical function. The WOMAC scale will be assessed at weeks 0, 1, 2, 6, and 14. The WOMAC functional subscale will be assessed at weeks 4, 8, and 16. The response rate refers to the proportion of patients who, compared to baseline, show an improvement of at least 2 units in average pain (VAS) and at least 6 units improvement in the WOMAC functional subscale at week 2. Adverse events and serious adverse events will be recorded from baseline to week 14.
Secondary Outcome Measures
Tender Point PPT Measurement
This study selects acupuncture intervention points as target points and MTrPs to assess changes in their pressure pain threshold (PPT). The procedure is as follows: The patient assumes a seated position, with the knee flexed at 90° and both feet flat on the floor to fully expose the detection area. The practitioner locates the points based on the “Acupuncture Point Anatomical Atlas”, gently sliding the thumb pad along the anatomical landmarks to palpate, confirming the surface projection of the acupoint. Then, vertical pressure (4 kg/cm²) is applied to mark sensitive points with a pain level of ≥3. A digital pressure pain threshold meter (FPX25, Wagner Instruments, USA) is used to measure PPT. The probe is placed vertically on the marked point’s skin, applying pressure at a constant rate (50 N/s). The pressure is stopped immediately when the patient first reports pain, and the instrument’s pressure value is recorded as PPT. Each acupoint is measured three times with 3-minute intervals, and the average value is taken as the final PPT. Paired t-tests of pre- and post-treatment data are performed using SPSS 26.0 software (significance level α = 0.05) to assess the effect of acupuncture on improving the pain threshold at the acupoint.
Three-Dimensional Gait Assessment Analysis
This study uses the Right Gait Posture Medical 3.0 dynamic gait analysis system (Shenzhen Xingzheng Technology Co., Ltd.) to collect gait data through a mobile terminal and dynamically detect foot movement. Before the test, participants are informed of the instructions and are provided with suitable insoles based on shoe size. The data collection module is attached to the bottom of the insole. After connecting to the terminal, the patient is instructed to walk normally for 2 minutes.
The system includes gait tracking, swing phase analysis, support phase analysis, step phase analysis, and micro-motion analysis. This study selects 8 indicators to assess walking ability, including walking speed, step frequency, support phase, swing phase, sagittal plane landing angle, sagittal plane push-off angle, coronal plane landing inversion angle, and coronal plane ground clearance. Walking speed and step frequency are important indicators of functional status in KOA patients. Due to pain, stiffness, or muscle weakness, patients often exhibit slowed walking speed and reduced step frequency. Changes in the ratio of support phase (60% of the gait cycle) and swing phase (40%) reflect compensatory gait in KOA patients. A decrease in sagittal plane landing and push-off angles suggests that pain and dorsal flexor weakness affect gait propulsion. An increased coronal plane landing inversion angle exacerbates knee joint load and accelerates disease progression, while decreased coronal plane ground clearance may be related to lower limb muscle strength decline (Figure 2).
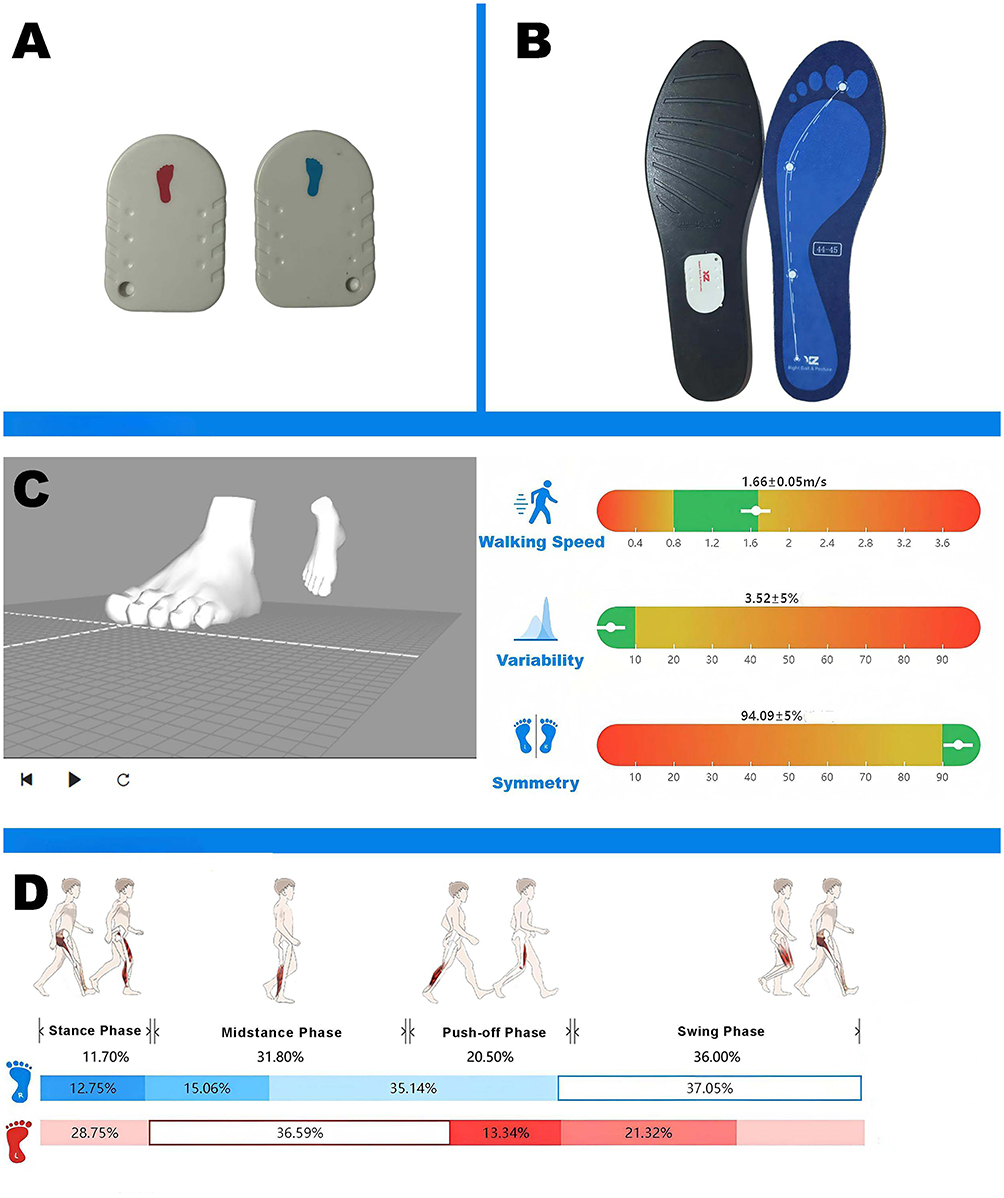 |
Figure 2 Schematic diagram of 3D gait analysis. (A) Left and right foot pressure sensors. (B) Smart insoles for gait monitoring. (C) 3D posture model and gait metrics (walking speed, variability, symmetry). (D) Step - phase breakdown (stance, midstance, push - off, swing) with percentage distribution for right and left feet. Blue bar: Corresponds to the right foot. Segmented sections and percentage values of this bar represent the time proportions of the right foot in the Stance Phase, Midstance Phase, Push-off Phase, and Swing Phase. Red bar: Corresponds to the left foot. Segmented sections and percentage values of this bar represent the time proportions of the left foot in the Push-off Phase, Swing Phase, Stance Phase, and Midstance Phase. |
Acupuncture Pain and Patient Acceptance
To assess the pain experienced by patients during treatment and their willingness to undergo further treatment, this study used the VAS to evaluate pain intensity immediately during and after the treatment. A score of 0 indicated no pain during the treatment, while a score of 10 indicated severe pain. Additionally, patients were asked if they would be willing to undergo the same treatment again after completion, with the question: “Considering the potential discomfort during the treatment, would you be willing to receive this treatment again in the future if needed?” Patients could respond with “Accept” or “Decline”.
Sample Size
The sample size was estimated using the formula: n=π0 (1-π0) [(μa+μb)/d]2, where π0 is the known population rate, π1 is the expected population rate for the trial outcome, and d=π1-π0. Based on preliminary pilot trials and literature reports, the effectiveness rate of acupuncture combined therapy for KOA is approximately 91.7%, and the effectiveness rate of acupuncture for KOA is about 73.0%. Setting α=0.05, β=0.1, π0=0.730, π1=0.917, d=0.917–0.730=0.187, with one-sided μ0.05=1.645 and μ0.1=1.282, the formula indicates that 48 participants per group are required. Considering a dropout rate of less than 10%, the sample size was increased to 53 per group, resulting in a total of 106 participants.
Data Collection, Management, and Monitoring
To promote patient retention and completion of follow-up, all interventions are provided to the patients free of charge.
Case Report Forms (CRFs) will be completed on paper and then entered into an Excel spreadsheet by independent researchers as the first level of data accuracy control. The second level of data integrity control will involve regular monitoring and validation of the data. The original CRF forms and all other documents (including informed consent forms) will be securely archived at the First Affiliated Hospital of Tianjin University of Traditional Chinese Medicine. The research ethics committee of the First Affiliated Hospital will conduct independent audits of the trial every five months, and the results of the audits will determine whether the study should be terminated early.
Statistical Analysis
All analyses will follow an intention-to-treat (ITT) approach, with all patients analyzed according to their assigned treatment group and receiving at least one treatment. The significance level will be set at 0.05 (two-sided). Baseline characteristics of patients will be summarized by treatment group. For continuous variables, data will be presented as means (standard deviation) or medians (interquartile range), depending on the normality of distribution. Count data will be presented as percentages. For the primary outcome, response rates at 8 weeks will be compared between groups M and L using chi-square tests. For secondary outcomes, continuous variables, including WOMAC pain, function, and stiffness scores, NRS, SF-12, acupuncture treatment expectations and credibility, and overall treatment effects, will be compared between groups at all follow-up time points using unpaired Student’s t-tests or Wilcoxon rank-sum tests. For the analysis of dropouts, missing data will be handled using the “last observation carried forward” method. Statistical analysis will be performed using SPSS version 21.0 (IBM SPSS Statistics, New York, USA).
Ethics and Dissemination
This study has been approved by the Ethics Committee of the First Affiliated Hospital of Tianjin University of Traditional Chinese Medicine (Ethical Approval No.: TYLL2023[K]Z011). The trial has also been registered on ClinicalTrials.gov (Registration No.: ChiCTR2300073707) and will be reported following the CONSORT statement and the STRICTA guidelines for acupuncture clinical trials. Patients will be enrolled in the study after receiving information about the research and signing the informed consent form. The results of the pilot study will be published in a peer-reviewed journal.
Discussion
This study aims to evaluate the efficacy of acupuncture on MTrPs in early to mid-stage KOA and compare it with conventional acupuncture protocols. KOA’s pathology involves cartilage degeneration, synovial inflammation, and myofascial dysfunction. Acupuncture, a key TCM therapy, has been widely used in treating KOA, but conventional protocols may not consider individual factors, affecting outcomes. We anticipate that the combined intervention will demonstrate superior effects compared to acupuncture at acupoints alone in terms of pain relief, improvement of joint function, and optimization of gait parameters, thereby addressing the current gap in individualized acupuncture treatment for KOA.
Mechanistically, the “pain as acupoint” strategy may exert analgesic effects via multiple pathways. Peripherally, acupuncture activates Aδ and C fibers, increases adenosine release (up to 24 times normal levels), inhibits pro-inflammatory cytokines (TNF-α, IL-1β), and promotes anti-inflammatory mediators (IL-10), while improving circulation.21,22 Acupuncture also adjusts joint stress balance and releases myofascial trigger points to correct soft tissue tension.23 Centrally, acupuncture increases serotonin (5-HT) and norepinephrine (NE) levels by 40%-60%, enhances descending inhibitory pathways, and reduces glutamate release and NMDA receptor phosphorylation, reversing peripheral and central sensitization;24 fMRI studies show that acupuncture can regulate brain regions involved in pain processing, such as the anterior cingulate cortex (ACC).25《The “pain as acupoint” theory in Ling Shu aligns with modern acupuncture mechanisms, regulating both peripheral and central pain modulators.26
If the study results support our hypothesis, the individualized treatment approach combining MTrP and acupoint needling will become a new paradigm for pain management in KOA. This approach not only helps improve patients’ quality of life and physical function, reducing the limitations caused by chronic pain on daily activities, but also promotes the integration of traditional Chinese and Western medicine in clinical practice, advancing the modernization and wider application of acupuncture therapy.
The innovations of this study are as follows: (1) The adoption of an individualized “pain as acupoint” strategy for selecting MTrPs, which, based on traditional meridian acupuncture, integrates pain point screening to make the acupuncture sites better align with the pain distribution characteristics of the patient, potentially enhancing the analgesic effect; (2) A comprehensive clinical efficacy evaluation through multidimensional outcome measures (VAS, WOMAC, PPT, gait analysis, etc)., combined with patient acceptability assessments, to increase the clinical guidance value of the study; (3) The use of a strict randomized controlled design and intention-to-treat (ITT) analysis to ensure the scientific rigor and reliability of the data.
Despite the advantages of the study design, there are still limitations: (1) The follow-up period is 14 weeks, which does not allow for the observation of long-term efficacy. Future studies could extend the follow-up period to further explore the long-term effects; (2) The outcome measures mainly rely on clinical subjective assessments, lacking objective evaluations from imaging or biomarkers; (3) The participants are only from a single center, so the generalizability of the findings needs further verification. (4) Due to the nature of acupuncture, it is challenging to blind both practitioners and patients, which may introduce observer or expectancy bias. Although we have minimized this through assessor blinding and standardized protocols, it remains an unavoidable limitation.
Future research can further explore the molecular and biomechanical mechanisms of MTrP acupuncture under the “pain as acupoint” theory, utilizing multimodal assessment methods to deepen the understanding of acupuncture’s effects, and expand the application of this treatment strategy to other chronic musculoskeletal disorders.
Conclusion
This study is expected to provide new clinical evidence for individualized treatment of knee osteoarthritis combining myofascial trigger point and acupoint acupuncture. Despite limitations such as a short follow-up period, lack of objective measures, single-center design, and challenges with blinding, the results will still offer valuable insights for clinical practice and lay the foundation for future mechanistic research and treatment optimization.
Trial Status
This trial is currently recruiting patients. The protocol version is 20230600, dated June 10, 2023. Recruitment began on September 30, 2023, and is expected to be completed by December 31, 2025.
Ethics Approval and Informed Consent
This study has been approved by the Medical Ethics Committee of the First Affiliated Hospital of Tianjin University of Traditional Chinese Medicine. Informed consent will be obtained from all patients before the trial begins.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (No. 81873316), the Tianjin Municipal Education Commission Project (No. 2021ZD013) and the Innovation Team Training Program of the First Teaching Hospital of Tianjin University of Traditional Chinese Medicine (No. 4042502041).
Disclosure
No potential conflict of interest was reported by the authors.
References
1. Lv Z, Yang YX, Li J, et al. Molecular classification of knee osteoarthritis. Front Cell Dev Biol. 2021;9:725568. doi:10.3389/fcell.2021.725568
2. Zhang L, Zhang C, Zhang J, Liu A, Wang P, Xu J. A bidirectional mendelian randomization study of sarcopenia-related traits and knee osteoarthritis. Clin Interv Aging. 2023;18:1577–1586. doi:10.2147/CIA.S424633
3. Wang M, Liu L, Zhang CS, et al. Mechanism of traditional Chinese medicine in treating knee osteoarthritis. J Pain Res. 2020;13:1421–1429. doi:10.2147/JPR.S247827
4. Cook CE, Degenhardt B, Aspinall S, Nim C, Malik S, Keter D. Myofascial pain syndromes: controversies and suggestions for improving diagnosis and treatment. J Orthop Sports Phys Ther. 2025;55:1–4. doi:10.2519/jospt.2025.13072
5. Wang Y, Aaron R, Attal N, Colloca L. An update on non-pharmacological interventions for pain relief. Cell Rep Med. 2025;6:101940. doi:10.1016/j.xcrm.2025.101940
6. Liu C-Y, Duan Y-S, Zhou H, et al. Clinical effect and contributing factors of acupuncture for knee osteoarthritis: a systematic review and pairwise and exploratory network meta-analysis. BMJ Evid-Based Med. 2024;29:374–384. doi:10.1136/bmjebm-2023-112626
7. Luo H, Jing C, Liu H. Curative effect of electroacupuncture and manual acupuncture for knee osteoarthritis: a meta-analysis. Iran J Public Health. 2024;53:1951–1963. doi:10.18502/ijph.v53i9.16450
8. Duarte FCK, Chien R, Ghazinour G, Murnaghan K, West DWD, Kumbhare DA. Myofascial pain as an unseen comorbidity in osteoarthritis: a scoping review. Clin J Pain. 2023;39:188–201. doi:10.1097/AJP.0000000000001102
9. Money S. Pathophysiology of trigger points in Myofascial pain syndrome. J Pain Palliat Care Pharmacother. 2017;31:158–159. doi:10.1080/15360288.2017.1298688
10. Lew J, Kim J, Nair P. Comparison of dry needling and trigger point manual therapy in patients with neck and upper back myofascial pain syndrome: a systematic review and meta-analysis. J Man Manip Ther. 2021;29(3):136–146. doi:10.1080/10669817.2020.1822618
11. Shah JP, Thaker N, Heimur J, Aredo JV, Sikdar S, Gerber L. Myofascial Trigger Points Then and Now: a Historical and Scientific Perspective. PM R. 2015;7:746–761. doi:10.1016/j.pmrj.2015.01.024
12. Stieven FF, Ferreira GE, de Araújo FX, Angellos RF, Silva MF, da Rosa LHT. Immediate effects of dry needling and myofascial release on local and widespread pressure pain threshold in individuals with active upper trapezius trigger points: a randomized clinical trial. J Manipulative Physiol Ther. 2021;44:95–102. doi:10.1016/j.jmpt.2020.07.003
13. Núñez-Cortés R, Cruz-Montecinos C, Vásquez-Rosel Á, Paredes-Molina O, Cuesta-Vargas A. Dry needling combined with physical therapy in patients with chronic postsurgical pain following total knee arthroplasty: a case series. J Orthop Sports Phys Ther. 2017;47:209–216. doi:10.2519/jospt.2017.7089
14. Wang R-H, Xue P-J, Xing H-J, Jia C-S, Shi J. Complex network analysis on regularities of acupoint combinations and application characteristics of acupuncture and moxibustion in the treatment of knee osteoarthritis. Zhen Ci Yan Jiu. 2022;47:65–70. doi:10.13702/j.1000-0607.20210080
15. Liu L, Skinner MA, McDonough SM, Baxter GD. Traditional Chinese Medicine acupuncture and myofascial trigger needling: the same stimulation points? Complement Ther Med. 2016;26:28–32. doi:10.1016/j.ctim.2016.02.013
16. Ughreja RA, Prem V. Effectiveness of dry needling techniques in patients with knee osteoarthritis: a systematic review and meta-analysis. J Bodyw Mov Ther. 2021;27:328–338. doi:10.1016/j.jbmt.2021.02.015
17. Du X, Liu Z-Y, Tao -X-X, et al. Research progress on the pathogenesis of knee osteoarthritis. Orthop Surg. 2023;15:2213–2224. doi:10.1111/os.13809
18. Pan J, Huang W, Huang Z, Luan J, Zhang X, Liao B. Biomechanical analysis of lower limbs during stand-to-sit tasks in patients with early-stage knee osteoarthritis. Front Bioeng Biotechnol. 2023;11:1330082. doi:10.3389/fbioe.2023.1330082
19. Chan A-W, Tetzlaff JM, Gøtzsche PC, et al. SPIRIT 2013 Explanation and Elaboration: guidance for protocols of clinical trials. BMJ. 2013;346:e7586.
20. Schulz KF, Altman DG, Moher D. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. PLoS Med. 2010;7(3):e1000251. doi:10.1371/journal.pmed.1000251
21. Goldman N, Chen M, Fujita T, et al. Adenosine A1 receptors mediate local anti-nociceptive effects of acupuncture. Nat Neurosci. 2010;13:883–888. doi:10.1038/nn.2562
22. Xu Y, Hong S, Zhao X, et al. Acupuncture alleviates rheumatoid arthritis by immune-network modulation. Am J Chin Med. 2018;46:997–1019. doi:10.1142/S0192415X18500520
23. Amani M, Shafizadegan Z, Taheri N. Effects of dry needling on pain in patients with knee osteoarthritis: a preliminary study. Adv Biomed Res. 2022;11:47. doi:10.4103/abr.abr_102_21
24. Lin J-G, Kotha P, Chen Y-H. Understandings of acupuncture application and mechanisms. Am J Transl Res. 2022;14:1469–1481.
25. Xie K, Pan X, Huang F, et al. Needle knife therapy plus sodium hyaluronate injection for knee osteoarthritis: a protocol for a systematic review and meta-analysis. Medicine. 2020;99:e23242.
26. Shi G-X, Tu J-F, Wang T-Q, et al. Effect of Electro-Acupuncture (EA) and Manual Acupuncture (MA) on markers of inflammation in knee osteoarthritis. J Pain Res. 2020;13:2171–2179. doi:10.2147/JPR.S256950
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.