Back to Journals » Journal of Pain Research » Volume 19
Acupressure Needle Therapy Combined with Lumbar Plexus Block in Patients Undergoing Hip Arthroplasty
Authors Huang C ![]() , Zhou J
, Zhou J ![]() , Liu H, Ju N, Yang P, Zhu S, Li J, Zhang X
, Liu H, Ju N, Yang P, Zhu S, Li J, Zhang X
Received 20 January 2026
Accepted for publication 7 May 2026
Published 26 May 2026 Volume 2026:19 597510
DOI https://doi.org/10.2147/JPR.S597510
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Chaoqun Huang,1,2,* Jiansong Zhou,1,2,* Hao Liu,1,2 Nanbin Ju,1,2 Peiyi Yang,1 Siling Zhu,3 Jun Li,1,2 Xutong Zhang1,2
1Department of Anesthesiology and Perioperative Medicine, The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, Wenzhou, People’s Republic of China; 2Key Laboratory of Anesthesiology of Zhejiang Province, Wenzhou Medical University, Wenzhou, People’s Republic of China; 3Department of Acupuncture and Physical Therapy, The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, Wenzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xutong Zhang, Department of Anesthesiology and Perioperative Medicine, The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, Wenzhou, People’s Republic of China, Tel/Fax +86 139 5776 5100, Email [email protected]
Objective: To investigate the analgesic effects of acupressure needle therapy combined with lumbar plexus block for anesthesia in elderly patients undergoing unilateral hip arthroplasty.
Methods: A total of 147 older patients set to have elective hip surgery from February 2025 to September 2025 were randomly divided into three groups: the acupressure needle group (Group A), the lumbar plexus group (Group L), and the combined acupressure needle and lumbar plexus block group (Group AL), with 49 patients in each group. All patients underwent hip arthroplasty under general anesthesia with endotracheal intubation. We compared the intraoperative consumption of remifentanil and propofol among the three groups. Additionally, the incidence of cognitive dysfunction (assessed by the 3D-CAM) on postoperative within 48 hours, numerical rating scale (NRS) scores for pain at rest and during movement (hip lift at 45°) at 6, 12, 24, and 48 hours postoperatively, quality of recovery scores (QoR-40 and ADL scores), patient satisfaction, preoperative and postoperative levels of IL-1β/IL-6 and serum CRP, PACU NRS scores, total consumption of postoperative analgesic pumps, effective and total presses of the PCA button (at 12, 24, 36, and 48 hours after surgery), rescue analgesic use in the ward, and opioid-related adverse reactions (nausea and vomiting) were evaluated.
Results: Using acupressure needle therapy along with a lumbar plexus block during general anesthesia led to less need for remifentanil and propofol during surgery, reduced the amount of pain relief needed afterward, decreased side effects from opioids like nausea and vomiting, lowered pain scores after surgery, and made patients more satisfied.
Conclusion: This combined strategy provides an effective optimized multimodal analgesic option for elderly patients undergoing hip replacement and is particularly valuable in comprehensive management regimens aimed at reducing opioid exposure.
Keywords: hip arthroplasty, acupressure needle, 3D-CAM score, lumbar plexus, NRS score
Introduction
The most popular hip reconstruction procedure among the elderly is total hip replacement, which can somewhat restore hip mobility function and enhance the elderly’s quality of life.1 However, older patients are more likely to face problems during and after surgery because they often have weaker heart and lung systems, different body functions, existing health issues, frailty, and less physical strength.2 Particularly during surgery, opioids worsen postoperative respiratory depression, impair cognitive function and stress, and exacerbate postoperative weakness, and dementia in older patients.3 Therefore, for the perioperative analgesia management of elderly patients, the focus should be on achieving excellent analgesic effects while reducing the dosage of opioid drugs.
Recent research has demonstrated that nerve block technology has a much better analgesic effect than traditional opioid analgesia in the perioperative management of anesthesia in older patients. It also speeds up postoperative rehabilitation and has no effect on the cognitive function of older patients after surgery.4,5 Although regional anesthetic techniques such as lumbar plexus and femoral nerve blocks are effective for postoperative analgesia, there is a risk of postoperative muscle weakness.6 Furthermore, nerve block does not always offer sufficient pain relief after hip surgery, and sustained intravenous analgesia maintenance with a specific dose of opioids is still needed for follow-up analgesia.7 Reduced perioperative opioid use is currently necessary for enhanced recovery after surgery rapid epithelial recovery (ERAS).8 To investigate whether traditional Chinese medicine (TCM) acupuncture-assisted anesthesia can accomplish the intended analgesic effect, further reduce the use of opioids, improve the quality of life for the elderly following surgery, and achieve rapid recovery, this study combined non-drug press-acupuncture therapy with nerve block technology.
Within traditional Chinese acupuncture, acupuncture is one of the therapy modalities. Weak and persistent stimulation of the patient’s skin can be achieved by inserting, fixing, and burying the intradermal needles under the skin or in the skin beneath the patient’s acupoint. By acting on key nodes of the HPA axis9 and regulating the upstream and downstream neuro-endocrine-immune network,10 it provides a safe and effective non-pharmacological intervention strategy for stress-related disorders. Currently, postoperative nausea and vomiting is the primary use of TCM acupuncture and moxibustion in anesthesia. The impact of associated analgesia and inflammation on the best way to combine nerve block in anesthesia and analgesia is rarely discussed, and the quality of research papers is often low. This study employed a randomized, double-blind design in which neither the participants nor the researchers knew who was receiving treatment, aiming to determine whether combining acupuncture with a lumbar plexus block and general anesthesia could improve patient recovery by reducing postoperative pain and related side effects.
Methods
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki. It has completed prospective clinical trial registration at the Chinese Clinical Trial Registry (ChiCTR). The registration date is December 19, 2024, and the registration number is ChiCTR2500096649. Detailed information can be accessed via the registration website:https://www.chictr.org.cn/bin/project/edit?pid=204978. Ethical approval was obtained from the Human Research Ethics Committee of the Second Affiliated Hospital of Wenzhou Medical University on December 19, 2024 (approval number: 2024-K-372-02). Written informed consent was obtained from all subjects participating in the trial, and all methods were performed in accordance with the relevant guidelines and regulations. This manuscript adheres to the applicable CONSORT (Consolidated Standards of Reporting Trials) guidelines.
Study Design
This study is a prospective, randomized, double-blind trial undertaken by a Grade A tertiary hospital in China from February 2025 to September 2025 (The first case was enrolled on February 5, 2025.). A total of 166 cases (A total of 19 cases in withdrew from the study due to changes in postoperative treatment methods or dropping out midway, 49 cases in each group were included in the trial), aged 65 to 80 years, irrespective of gender, with a BMI ranging from 18.5 to 25.2kg/m2, were selected for unilateral hip replacement and classified by the American Society of Anesthesiologists (ASA) as class I–III. Criteria for exclusion: Impaired cardiac function (EF<50%), chronic obstructive pulmonary disease, significant hepatic or renal dysfunction, diabetes mellitus, psychiatric disorders affecting cooperation or adherence to psychotropic medications, difficulties in verbal communication, prolonged administration of analgesics or non-steroidal anti-inflammatory drugs within the past 2 weeks, history of drug or metal hypersensitivity, abnormal coagulation profile, concomitant autoimmune disease, infectious pathology Patients with disease, infection at the nerve block site, a history of lower extremity nerve injury, and localized face erythema and edema, as well as dermatological conditions.
Participants in the study were allocated to three groups: the acupuncture press treatment group (group A), the lumbar plexus group (group L), and the acupuncture combined with lumbar plexus block treatment group (group AL) in a 1:1:1 ratio. They were randomly assigned to the same experienced TCM acupuncturist by the nurse anesthetist utilizing a numerical table generated by SPSS statistical software (all participants in the three groups received either the actual acupuncture press or the acupuncture body removed). An expert anesthesiologist, not participating in the treatment, conducted the lumbar plexus block. Following the execution of pertinent technical procedures, tracheal intubation was conducted by a different anesthesiologist utilizing intravenous anesthetic and intraoperative anesthesia management. The anesthesiologist completed intraoperative data collection for patients, while researchers gathered postoperative follow-up data.(Figure 1)
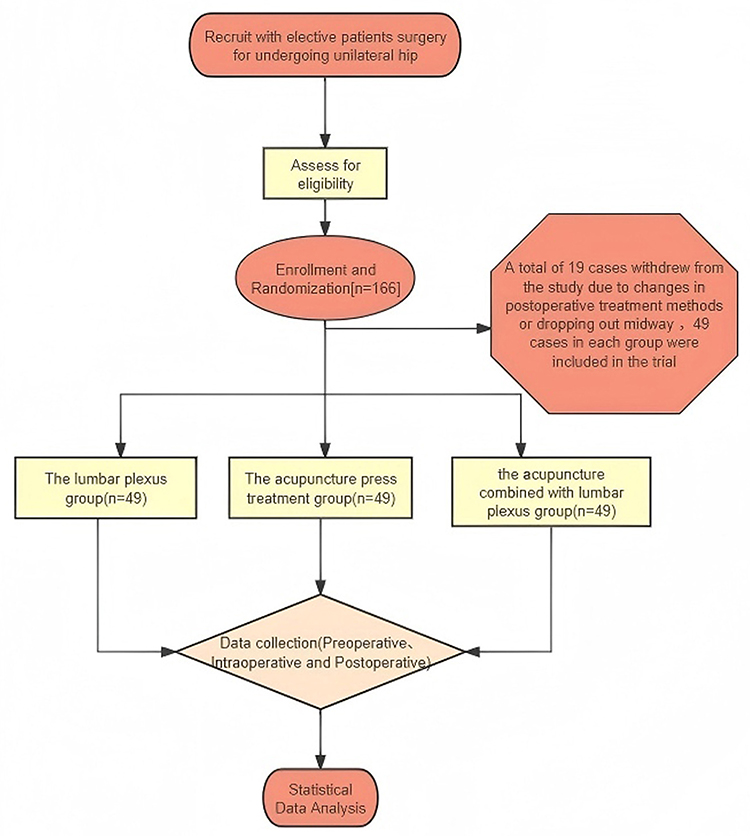 |
Figure 1 Anesthesia flow. |
Anaesthesia Induction and Maintenance
The trial patients underwent a preoperative assessment the evening prior to surgery, during which a comprehensive evaluation was conducted and their ASA classification was determined. Informed consent was obtained from patients after they were apprised of the trial technique, the anesthetic protocol, and any related risks. Furthermore, the NRS score and the utilization of a postoperative intravenous self-controlled analgesia pump were elucidated to the patients. All patients received acupuncture or lumbar plexus blocks 30 minutes before to general anesthesia. Upon the patients’ admittance to the anesthetic induction room, routine mask oxygen inhalation, electrocardiogram (ECG), pulse oxygen saturation (SpO2), and noninvasive blood pressure (NIBP) monitoring were conducted. Each patient received a standardized protocol for general anesthetic induction and maintenance upon entering the operating room, which included sequential administration of 0.2 µg/kg sufentanil, 2.0 mg/kg propofol, and 0.2 mg/kg cis-atracurium. Following the establishment of muscle relaxation and successful tracheal intubation, mechanical ventilation was initiated by connecting to the anesthesia machine with a tidal volume of 6–8 mL/kg, a FIO2 of 50%, and an I:E ratio of 1:2. The initial ventilation rate was set at 12 breaths per minute, with end-expiratory CO2 maintained at 35–45 mmHg by adjusting the respiratory rate. Propofol at a dosage of 0.05 to 0.2 mg·kg-1·min-1, remifentanil 0.1–0.5 µg·kg−1·min−1 was administered to sustain the anesthetic monitoring index (BIS) within the range of 40 to 60. Cis-atracurium was administered at a dosage of 0.05 mg/kg every 30 minutes throughout the procedure, and the acupuncture sites were stimulated 10 times. Simultaneously, liquid management and thermal insulation strategies were implemented throughout the operation. SBP and HR were sustained within ±20% of the baseline value by modulating the pump speed of propofol and remifentanil. 20µg of deoxyadrenaline was administered for blood pressure reductions above 20% of baseline, 10mg of urapidil was provided for blood pressure elevations above 20% of baseline, and 0.3mg of atropine was given for heart rates below 45 beats per minute. Intraoperative fluid management and thermal insulation protocols must be implemented. The PCIA (patient-controlled intravenous analgesia) electronic analgesic pump was activated 10 minutes before to the conclusion of the procedure, administering sufentanil at a rate of 0.04 µg/kg•h, with a continuous background infusion of 1 mL/h, a bolus dosage of 2 mL/h, and a lockout interval of 15 minutes. Propofol and remifentanil were discontinued upon suturing the skin, and the tracheal catheter was extracted following the administration of neostigmine at a BIS value of 70. Following the stabilization of the patient’s vital signs, he was transferred to the Post-Anesthesia Care Unit for additional monitoring.
Experimental Intervention
This was a prospective, randomized, double‑blind, placebo‑controlled clinical trial. A simple randomization method was adopted. An anesthesia nurse who was not involved in this study generated a random number sequence using SPSS software and prepared random number cards. The cards were sealed in opaque envelopes, which were numbered in accordance with the order of the random sequence. The sealed envelopes were uniformly stored and kept by a pharmacist in a locked special cabinet. Trained clinical researchers were responsible for participant enrollment. They obtained the corresponding numbered envelopes from the anesthesia nurse sequentially according to the enrollment order, opened the envelopes on the spot after the participants signed the informed consent form, and assigned the participants to the corresponding groups based on the random numbers shown on the cards. Throughout the study, investigators responsible for efficacy assessment did not participate in random sequence generation, envelope storage, or group assignment. Participants in this study were randomly assigned to three groups: the acupuncture treatment group (group A), the lumbar plexus group (group L), and the acupuncture coupled with lumbar plexus block treatment group (group AL), with 49 instances in each group. All patients received acupuncture and/or a lumbar plexus block 30 minutes before to general anesthesia. In groups A and AL, points were selected based on “Chin Acupuncture Therapy”:11 the hip point (approximately one transverse finger above the anterior mandibular angle, where the masseter muscle elevates during mastication, and the depression, referred to as the chin che point, was enhanced according to the acupoint), the sacral point (0.5 inches anterior to the angle of the lower jaw), and the Neiguan point (2 inches above the transverse stripe of the distal palm of the wrist), totaling three points and three needles. For standard disinfection, a 0.20 × 1.5mm press-tack needle was chosen. The adhesive tape on the needle body was removed using aseptic technique, and the needle was inserted into the designated acupoint on the cheek, followed by gentle pressure to enhance fixation. The needle was kept for 48 hours post-operation (During this period, the needle follows the movement of the facial muscles to achieve acupoint stimulation). The L group was secured at the aforementioned sites using the press-needle, with the needle body detached. A lumbar plexus block was performed by injecting 30 mL of a solution containing 0.375% L-bupivacaine and 1% lidocaine into the psoas major muscle area (Group A was given 30 mL of normal saline). All acupuncture procedures were conducted by the same skilled TCM acupuncturist, while the nerve block was administered by the same proficient anesthesiologist.(Figure 2)
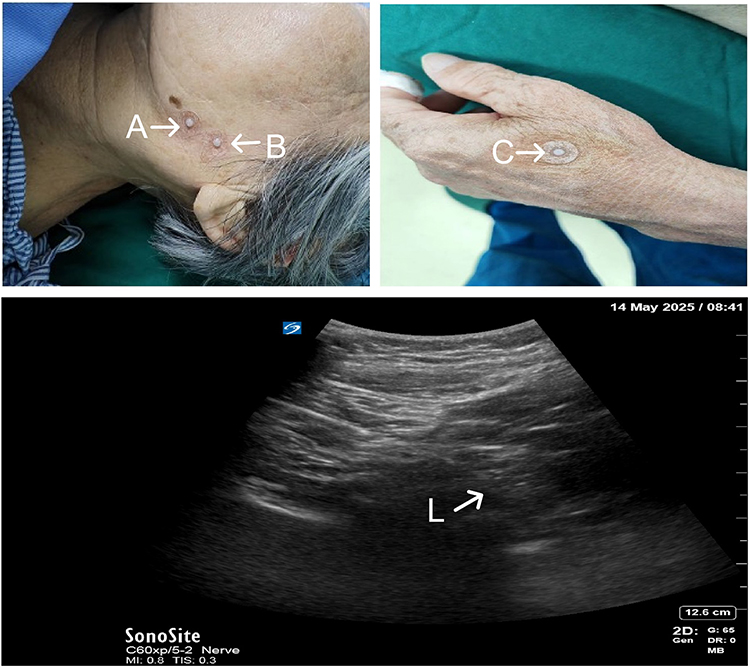 |
Figure 2 (A) the sacral point (B) the Hip point (C) the Neiguan point L:Lumbar Plexus. |
Outcome Assessment
This study’s primary indices were NRS resting and exercise pain scores recorded at each time interval (6h, 12h, 24h, and 48h) post-surgery. The secondary indexes comprised the total dosage of propofol and remifentanil, the levels of IL-1β/IL-6, and serum CRP before and after the surgery. Total analgesic pump consumption (mL), incidence of delirium within 48 hours based on cognitive function score (3D-CAM), effective and total number of compressions with PCIA key (12h, 24h, 36h, and 48h), number of ward analgesia interventions during PCIA pump usage (5 mg intramuscular relief with dezocine if resting NRS score > 4). If the NRS score remained > 4 after 1 hour, a 5 µg intravenous injection of sufentanil was administered for remediation, and the medication was documented. Activity of Daily Living score (ADL) at each time point within 48 hours post-surgery and postoperative rehabilitation score (QoR-40), postoperative hospital duration, patient satisfaction (subjects evaluated analgesic satisfaction using a digital scoring scale (NRS) 48 hours post-surgery/assessed patients’ satisfaction with anesthesia using a 0–10 digital scoring method), and analgesic drug-related adverse reactions (nausea and vomiting) were recorded.
Statistical Methods
Sample Size Calculation
The sample size was determined by the endpoint of the primary outcome measure. The primary outcome of this study was the postoperative pain NRS score (a continuous variable). According to a preliminary experiment with 10 patients in each group, thePostoperative 24-hour movement pain NRS score were 2.2 ± 1.4 in group AL, 2.9 ± 1.1 in group L, and 3.3 ± 1.5 in group A. A two‑tailed test was adopted with a significance level of α = 0.05 and a test power (1−β) of 0.90. The sample size was calculated using PASS 21.0 software by One‑Way Analysis of Variance Assuming Equal Variances (F‑Tests), which showed that at least 141 subjects were required. Considering an approximately 15% dropout rate, the total sample size was increased to 166 cases. In accordance with a 1:1:1 allocation ratio, a total of 166 participants were planned to be enrolled in this study. The statistical analysis was conducted using SPSS 25.0 program. The measurement data adhering to a normal distribution were represented as mean ± standard deviation ( ), the measurement data exhibiting skewed distribution were represented as M (P25, P75), and the categorical data were represented as frequency (n) and percentage (%). ANOVA test for repeated measures was used for normally distributed and chi-square, and Welch’s test was used for normally distributed but not chi-square; Generalized Estimating Equations (GEEs) were employed for comparison across several time points. The Kruskal–Wallis H-test was employed to analyze the skewed distribution measurement data, while the chi-square test or Fisher’s exact probability approach was utilized for categorical data. A P-value of less than 0.05 was deemed statistically significant.
), the measurement data exhibiting skewed distribution were represented as M (P25, P75), and the categorical data were represented as frequency (n) and percentage (%). ANOVA test for repeated measures was used for normally distributed and chi-square, and Welch’s test was used for normally distributed but not chi-square; Generalized Estimating Equations (GEEs) were employed for comparison across several time points. The Kruskal–Wallis H-test was employed to analyze the skewed distribution measurement data, while the chi-square test or Fisher’s exact probability approach was utilized for categorical data. A P-value of less than 0.05 was deemed statistically significant.
Results
General Data Comparison
A total of 147 cases (49 cases in each group) were included. No significant differences were observed in general characteristics, operation time, blood pressure, heart rate, preoperative pain NRS scores, or intraoperative blood loss among the three groups (all P>0.05). (Tables 1 and 2)
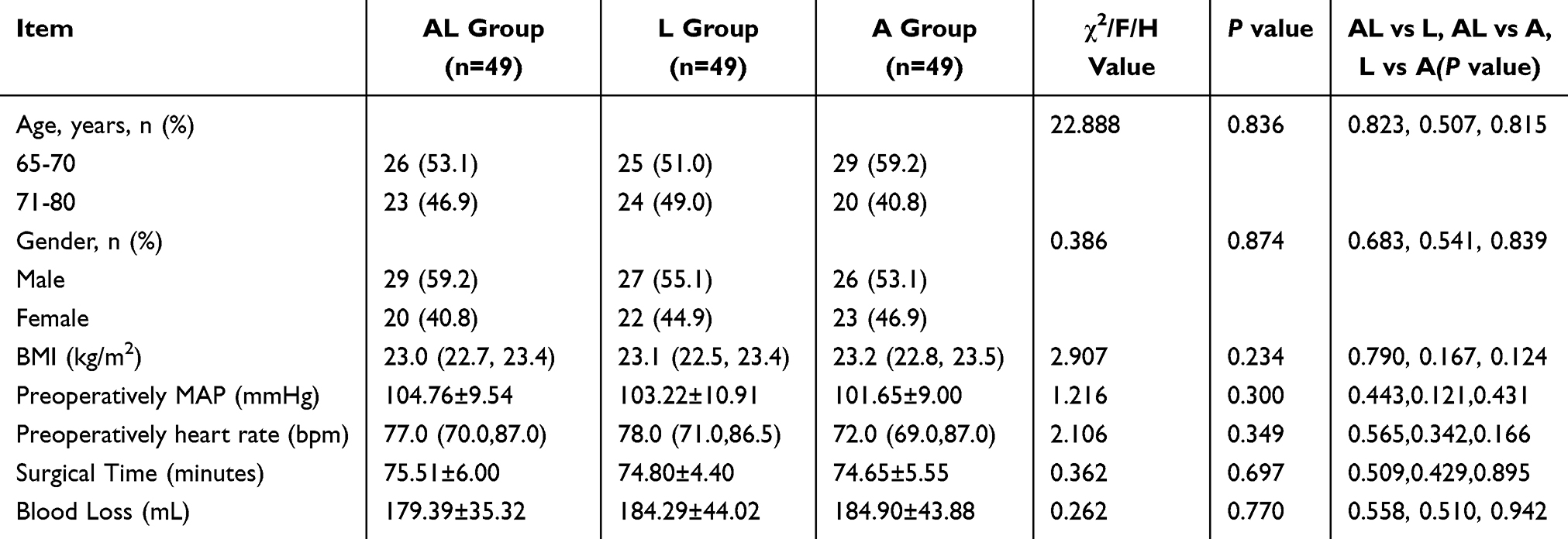 |
Table 1 Comparison of General Characteristics of Patients in Each Group |
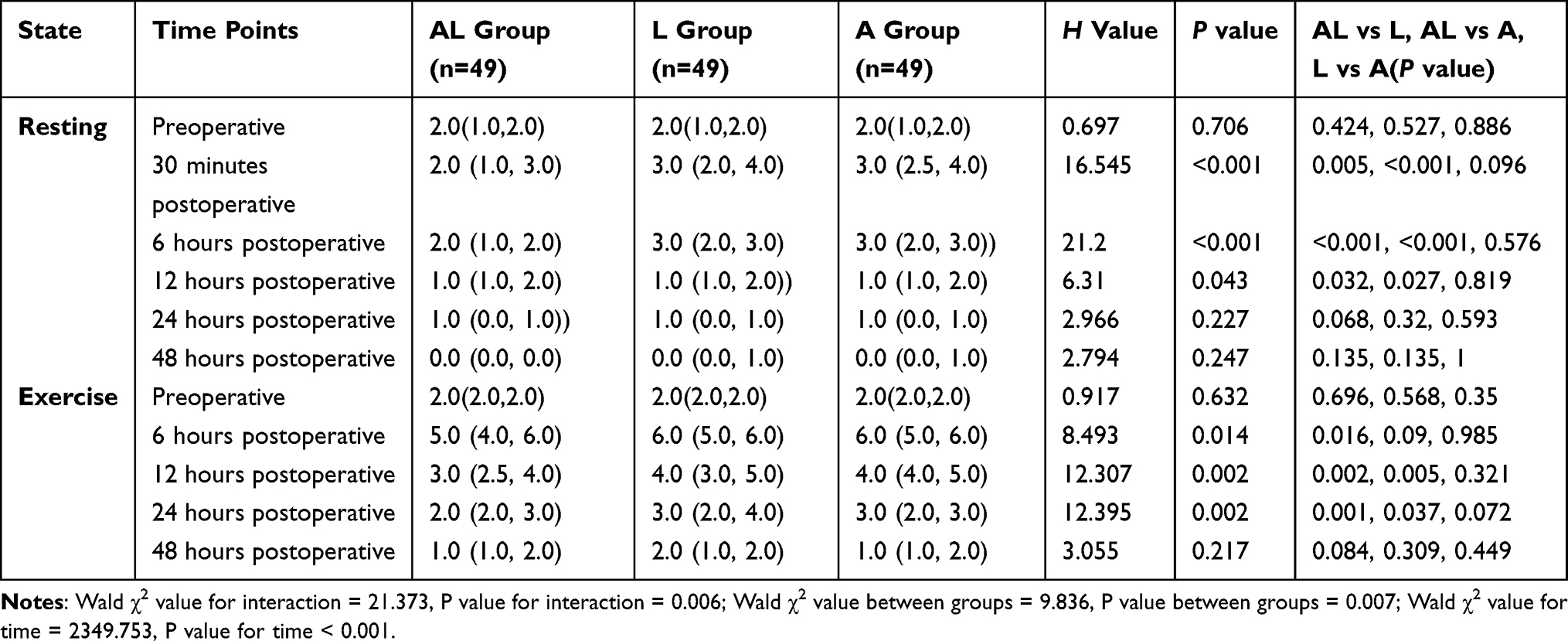 |
Table 2 Comparison of Resting and Exercise NRS Scores at Different Time Points Postoperatively |
Primary Outcome
NRS resting and exercise scores were documented at 30 minutes, 6 hours, 12 hours, 24 hours, and 48 hours, respectively. The NRS resting and exercise scores of the three groups were evaluated using a generalized estimation equation. It was determined that regardless of resting or exercising, an interaction between the group and time was present (Resting: Waldχ2 interaction = 34.155, P < 0.001; Motion: Waldχ2 interaction = 21.373, P = 0.006), necessitating a separate impact analysis. The individual effect analysis indicated that the NRS score after 30 minutes, 6 hours, and 12 hours post-operation in the AL group was considerably lower than that in the L and A groups (P < 0.05). The exercise NRS score after 24 hours post-operation was considerably lower than that in groups L and A (P < 0.05). A significant difference in exercise NRS scores was seen 6 hours post-operation between group AL and group L (P < 0.05), whereas no significant difference was found between group A and group L (P > 0.05). No statistical significance was observed between group L and group A (P >0.05). The independent effect analysis of time indicated that the NRS scores for all groups progressively diminished with time, with the scores for rest and exercise at 6h, 12h, 24h, 36h, and 48h post-surgery being significantly lower than preoperative levels (all P < 0.05). (Table 2, Figure 3a and b)
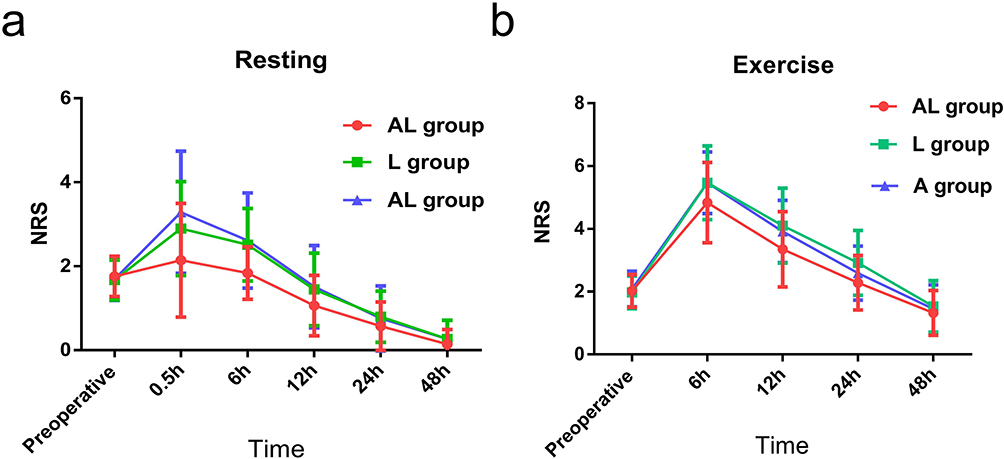 |
Figure 3 (a) shows that the postoperative Resting NRS scores decreased over time, and the pain score of the AL group was significantly lower than those of the L group and the A group. (b) shows that the postoperative Exercise NRS scores decreased over time, and the pain score of the AL group was significantly lower than those of the L group and the A group. |
Secondary Outcomes
Intraoperative Anesthetics and Postoperative Analgesics
The intraoperative dosages of propofol and remifentanil in the AL and L groups were significantly lower than those in group A, with statistical significance (P < 0.05); however, no significant difference was observed between the AL and L groups (P> 0.05). The quantity of supplementary remedial medications utilized in the AL group was significantly less than that in the L and A groups (P< 0.05). The total consumption of the postoperative analgesic pump exhibited significant variation among the three groups (P< 0.05). (Table 3)
 |
Table 3 Comparison of General Characteristics of Patients in Each Group |
Comparison of Inflammatory Indicators
There was no statistical significance in preoperative and postoperativeIL-1β, IL-6 and CRP among the three groups (P>0.05). (Table 4)
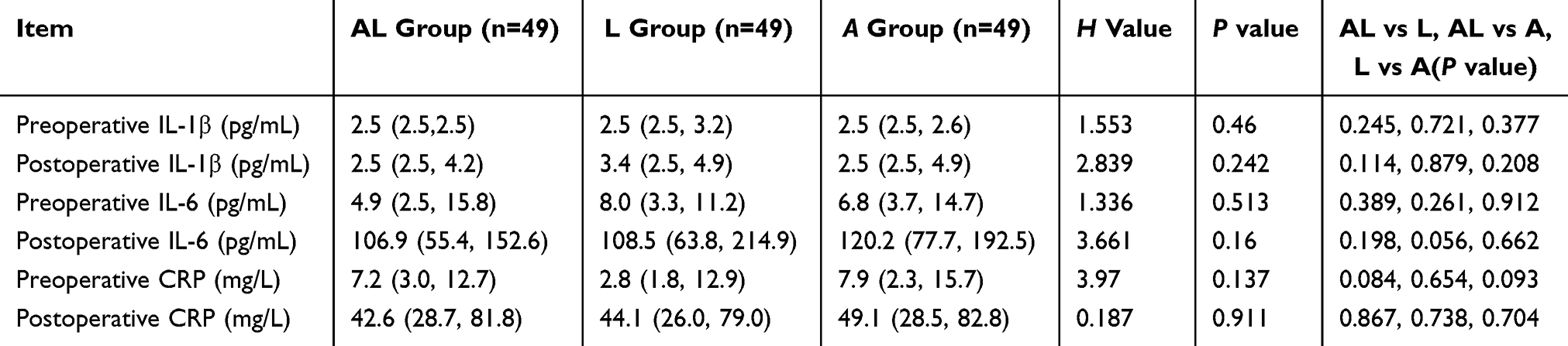 |
Table 4 Comparison of Preoperative and Postoperative IL-1β, IL-6, and CRP Levels in Each Group |
The Score of Each Scale
The satisfaction results, QoR-40 score, ADL score, and 3D-CAM score for the three groups at each postoperative time point indicated that the satisfaction of the AL group significantly surpassed that of the L group and A group 24 hours post-surgery, with a statistically significant difference (P < 0.05). At 48 hours postoperatively the satisfaction of the AL group remained higher than that of the L group (P < 0.05). No substantial difference was seen between group L and group A (P>0.05). At 48 hours postoperatively, the incidence of 3D-CAM-positive cases in Group AL and Group A was significantly lower than that in Group L, with a statistically significant difference (P < 0.05). No substantial difference was observed in the scores at subsequent time points (P>0.05). (Table 5)
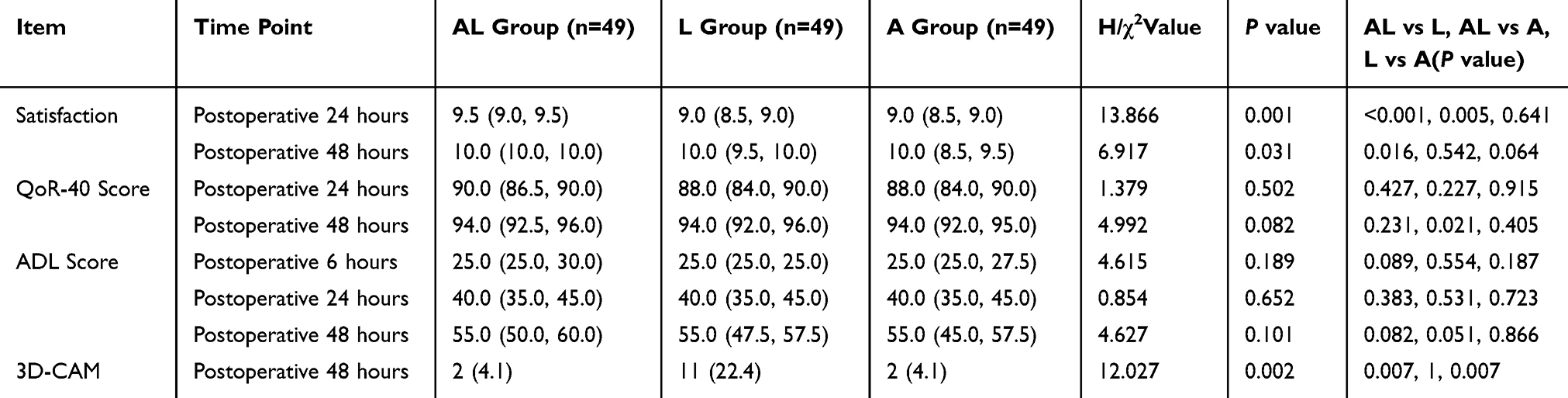 |
Table 5 Comparison of Postoperative Satisfaction, QoR-40 Scores, ADL Scores, and 3D-CAM Scores in Each Group |
Analgesic Pump Compression and Postoperative Remedial Medication
The effective and total compressions at each time point for the three groups were examined using a generalized estimation equation. It was determined that regardless of effective compressions or total compressions, there existed an interaction between the groups and time (effective compressions: Waldχ2 value interaction = 37.074, P value interaction < 0.001; total press number: Waldχ2 value interaction = 36.448, P value interaction < 0.001), necessitating a separate effect analysis. The comparative study of single effects between groups revealed that the quantity of effective analgesic pump compressions at 12, 24, and 36 hours post-operation in the AL group was significantly lower than in the L and A groups, with a statistically significant difference (P< 0.05). The total count of analgesic pumps at 12 and 24 hours post-operation in the AL group was much lower than in the L and A groups, with a statistically significant difference (P< 0.05). The total number of analgesic pump compressions at 36 hours post-operation exhibited a significant difference between the AL group and the A group (P < 0.05). No significant difference was seen in the effective number and total number of analgesic pump compressions between group L and group A at any time point (P>0.05). The analysis of individual time effects revealed that as time progressed, both the effective and total counts of analgesic pump compressions in each group diminished progressively. The total effective compressions and total compressions within 48 hours post-operation showed that AL group was much lower than in the L and A groups (P < 0.05). There was no statistically significant difference in the total cumulative effective compressions or total cumulative compressions between Group L and Group A (both P > 0.05). (Table 6, Figure 4a and b)
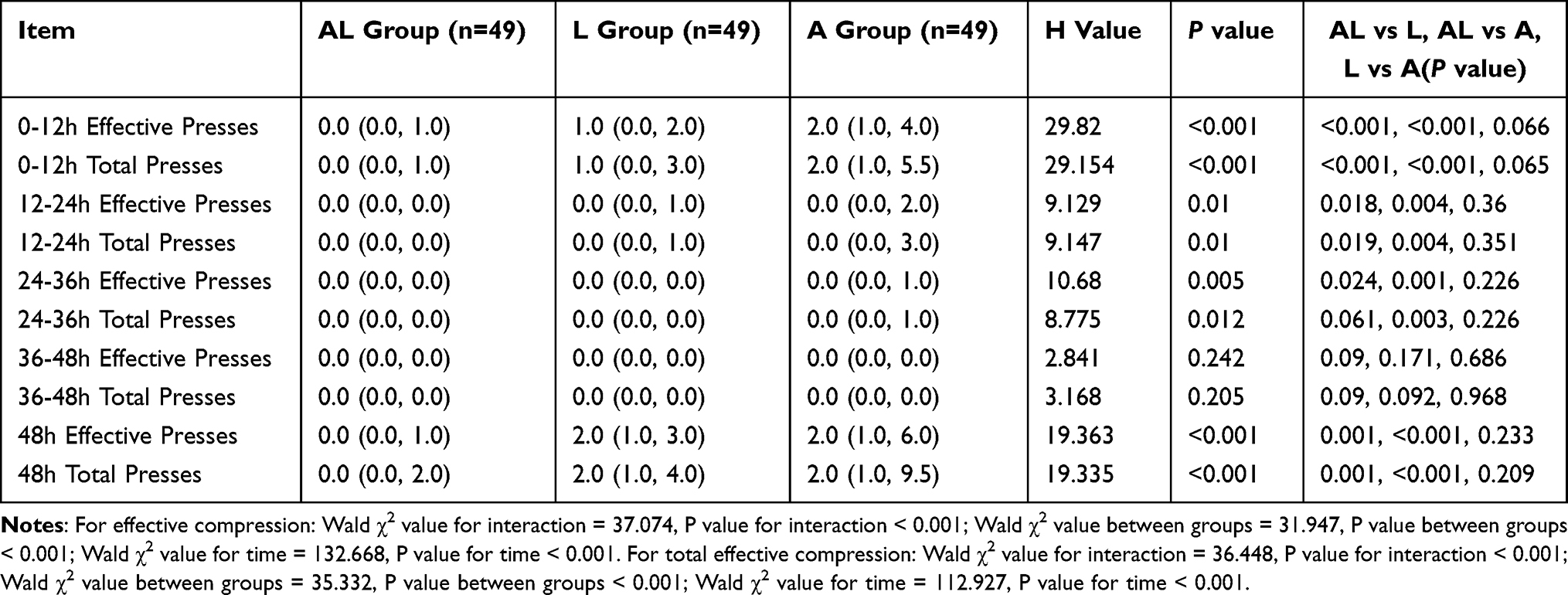 |
Table 6 Comparison of Effective and Total PCIA Button Presses at Different Postoperative Time Points |
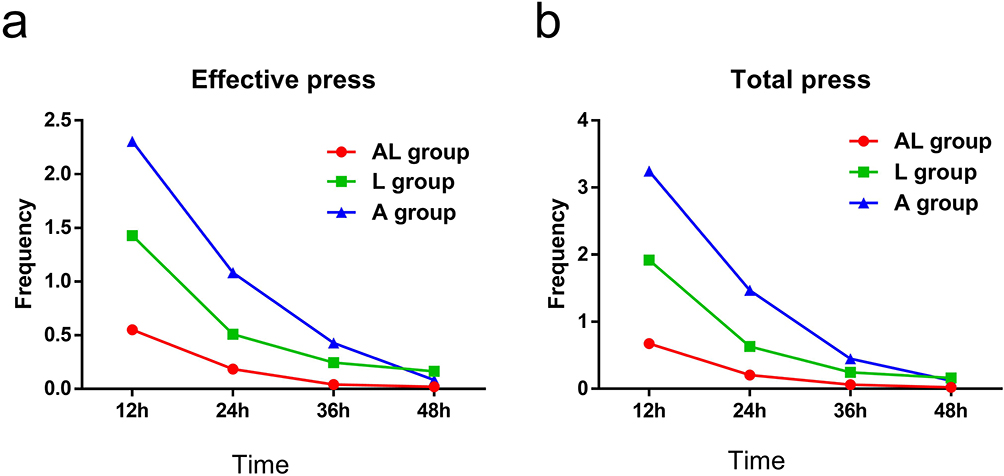 |
Figure 4 (a) shows that the effective pressing of the three groups of analgesic pumps decreased over time. The analgesic effect of the AL group was significantly better than that of the L group and the A group. (b) shows that the total pressing of the analgesic pumps in the three groups decreased over time. The analgesic effect of the AL group was significantly better than that of the L group and the A group. |
Postoperative Nausea and Vomiting Side Effects
The cases of postoperative nausea and vomiting (PONV) in the three groups at each time point were analyzed by generalized estimation equation. In terms of the frequency of nausea and vomiting, no interaction between groups and time was found. (Waldχ2 value interaction = 12.084, P value interaction = 0.06; Wald χ2 = 5.795 among groups, P = 0.055 among groups). However, the incidence of nausea and vomiting in AL group was significantly lower than that in L group within 24 hours after surgery, with statistical significance (P < 0.05). The incidence of nausea and vomiting in patients treated with acupuncture combined with lumbar plexus block was 0.630 times higher than that in patients with lumbar plexus block alone within 48hours. (Table 7 and Figure 5)
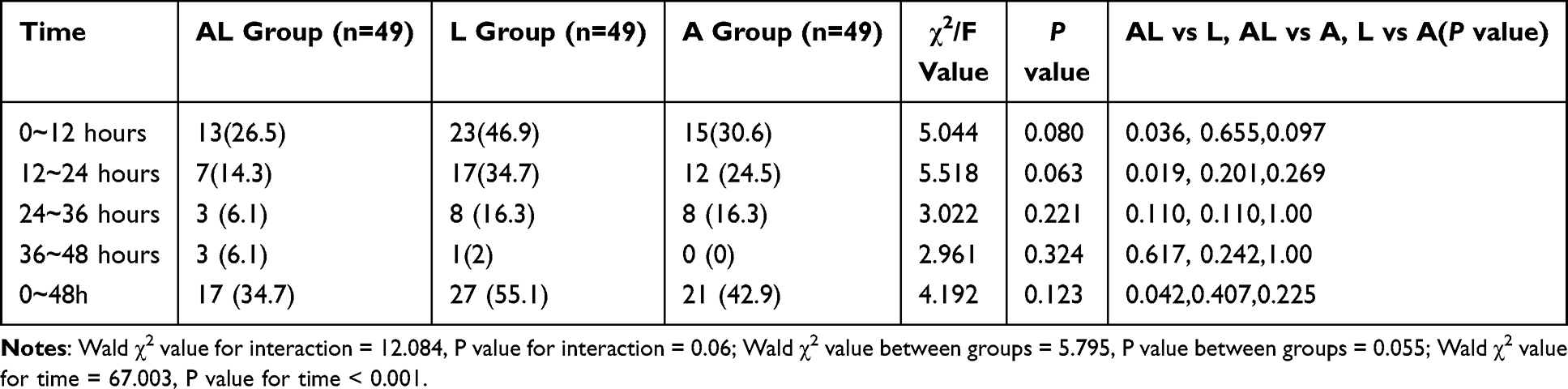 |
Table 7 Comparison of Postoperative Nausea and Vomiting Incidence at Different Time Points |
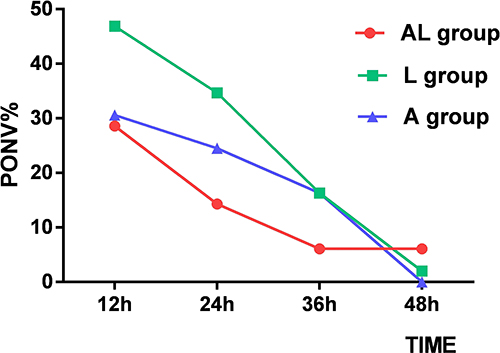 |
Figure 5 Shows that Postoperative nausea and vomiting decrease over time, especially within 36 hours after surgery. |
Analysis of the composition of PONV scores in the three groups showed that in terms of PONV score of 3 within 0–12 hours after surgery, the L group had a higher than the AL group and A group (P < 0.05), while there was no statistical significance in other comparisons (P > 0.05). (Table 8)
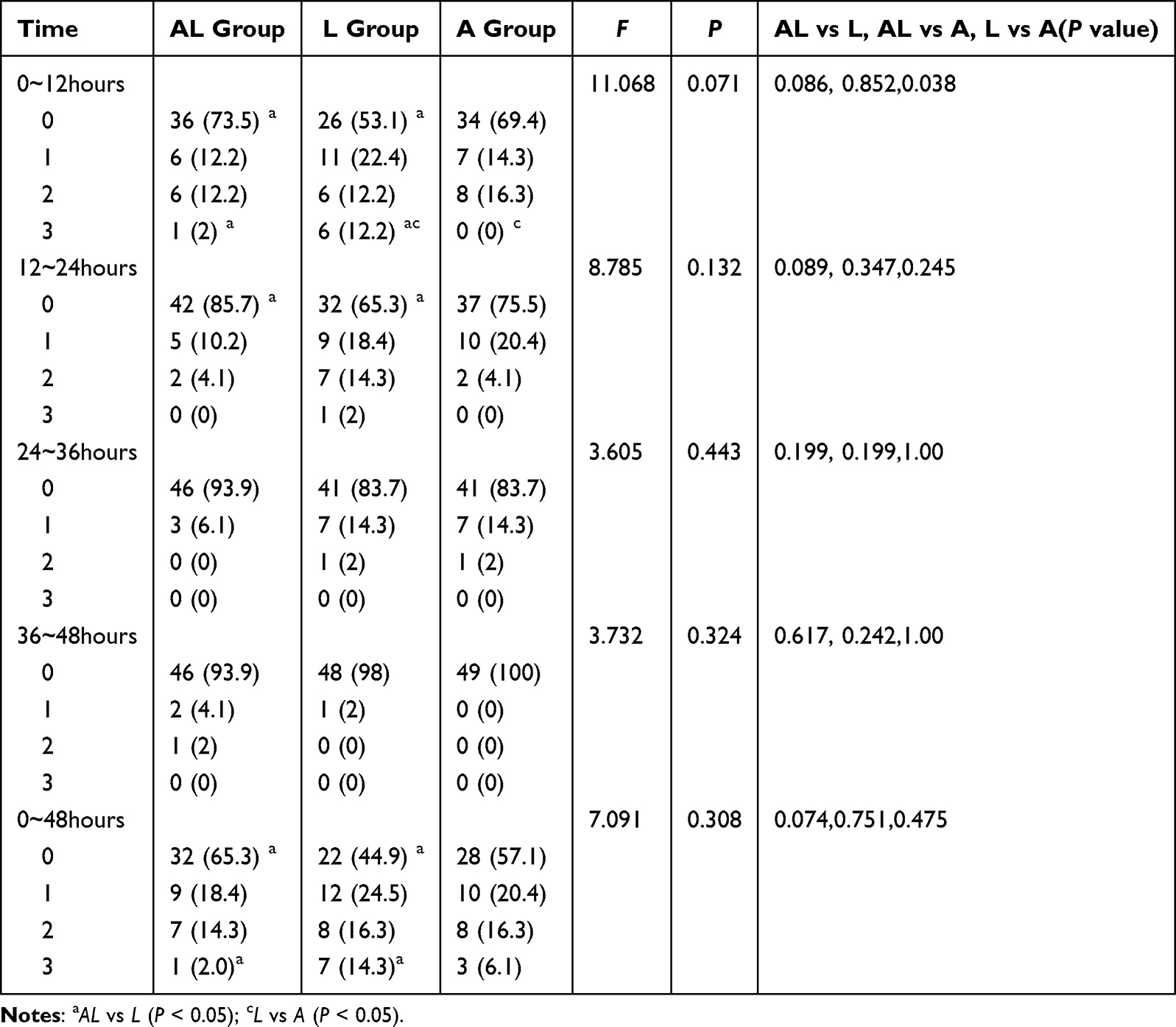 |
Table 8 Comparison of Postoperative Nausea and Vomiting Score at Different Time Points [n=49, n (%)] |
Discussion
This study indicated that acupuncture, in conjunction with lumbar plexus block, can yield a significant analgesic impact in senior patients following total hip replacement surgery, offering an alternative analgesic strategy to diminish postoperative opioid use. Acupuncture in conjunction with lumbar plexus block demonstrated a markedly enhanced postoperative analgesic efficacy compared to isolated lumbar plexus block and standalone acupuncture analgesia. This mode incorporated traditional Chinese acupuncture treatment, resulting in a considerably lower postoperative analgesia score compared to the non-combined analgesia group at many time intervals, and it also had a superior therapeutic effect on postoperative nausea and vomiting. These results contribute positively to the stable internal environment of elderly orthopedic patients post-surgery and may facilitate speedy rehabilitation and enhancement of their quality of life following the procedure.
Multiple studies12,13 have reported that the incidence of postoperative delirium (POD) in patients after hip fractures surgery ranges from 16% to 50%, among which a large-scale prospective study (n=107,028) showed an incidence of 19.7% to 20.5%. Pain, inflammation, sleep difficulties, and other illnesses are the triggering elements that expedite the formation of POD. Specifically, pain is intricately linked to postoperative psychosis. It results in significant postoperative consequences, such as protracted recovery, deterioration in physical and cognitive abilities, loss of autonomy, and elevated mortality rates.14 Consequently, the selection of anesthesia technique is crucial, as it must account for both the efficacy of the anesthesia and its safety. The application of nerve block anesthetic technologies in geriatric orthopedics is presently the predominant approach in perioperative anesthesia. Ultrasound-guided lumbar plexus nerve block can mitigate the stress response in senior patients undergoing total hip replacement, decrease the occurrence of postoperative cognitive impairment, enhance hemodynamic stability, and improve the efficacy and safety of postoperative rehabilitation. The quantity of postoperative opioid analgesics should concurrently be decreased.15
Currently, there is a consensus among anesthesiologists to minimize or completely abolish the use of perioperative opioids. The metabolism and excretion of opioids in the elderly are diminished, resulting in prolonged retention in the body,16 which can precipitate a range of adverse effects, including respiratory depression, gastrointestinal dysfunction, and cognitive impairment, potentially elevating postoperative mortality in older patients.17,18
Therefore, this study adopted the combination of acupuncture and lumbar plexus block anesthesia technology. Acupuncture is one of the traditional treatment methods of traditional Chinese acupuncture, and acupuncture embedding can enhance the analgesic effect of acupuncture at all levels of the central nervous system.19 fMRI evidence indicates that acupuncture analgesia achieves multi-faceted regulation of pain perception, emotional response, and central sensitization through the integration of a distributed network consisting of the limbic lobe, paralimbic lobe, and neocortex.20 The sustained and inadequate stimulation of particular acupoints alters the microscopic structure of adjacent tissues, enhances metabolism (increasing alkaline substances), and regulates the functions of the meridians and organs.21 It may diminish postoperative reliance on analgesic medications.22 This study’s results indicate that adjuvant acupuncture treatment is superior than lumbar plexus block anesthetic alone for analgesia. Within 48 hours post-surgery, the analgesic score for the group receiving a combination of acupuncture and lumbar plexus block was significantly superior to that of the non-combination groups. This indicates that acupuncture possesses notable analgesic properties, effectively complements lumbar plexus block and analgesia, and diminishes the necessity for narcotic drugs and opioids during and after the procedure. This aligns with current reports on needle insertion therapy: Research suggests that needle insertion may generate an endogenous peptide with morphine-like effects due to localized skin hypersensitivity to pain, resulting in an endogenous opioid effect.23 This process aims to facilitate a generally painless treatment by stimulating local alkaline substances and alleviating local soft tissue spasms.24
It is important to acknowledge that while press-acupuncture possesses anesthetic and analgesic properties, the analgesic impact is quite mild. This study indicates that, when comparing the acupuncture group alone, the intraoperative anesthetic dosage in the lumbar plexus block group the combined acupressure needle and lumbar plexus block group are lower than those in the acupuncture group. Consequently, acupuncture alone is insufficient for perioperative analgesia in patients undergoing total hip replacement. This study found that the inhibitory effect of acupuncture adjuvant therapy on postoperative inflammatory factors did not improve, and acupuncture treatment failed to replicate the previously reported efficacy in significantly reducing the anti-inflammatory effects of IL-6, TNF-α, and other inflammatory factors.25 The disparity in selected acupoints, coupled with the limitation of acupuncture to stimulating just the subcutaneous tissue, the absence of electroacupuncture, and insufficient acupuncture depth, may be contributing factors. Acupuncture in conjunction with lumbar plexus block anesthesia markedly outperforms the non-combined group on the suppression of postoperative nausea and vomiting, patient satisfaction, quality of life metrics, and delirium scale scores. Recent research indicate that acupuncture can suppress the protein kinase Mzeta-glutamate receptor (PKM zeta GluRl ACC signaling pathway) and mitigate anxiety. Down-regulating CB1R in GABAergic neurons enables the ventral hippocampus (vHPC) to exert an anti-anxiety effect and alleviate pain-induced anxiety.26 Consequently, adjuvant acupuncture therapy may enhance cognitive function preservation and expedite recovery in senior orthopedic patients post-surgery.
Although the between-group differences in NRS scores reported in this study are statistically significant, it is crucial to carefully evaluate their clinical relevance. In the field of pain research, a reduction of ≥1.0–1.5 points in postoperative movement pain NRS scores is generally regarded as the minimal clinically important difference from the patient’s perspective.27 In this study, the combination group (AL) exhibited a 1.2–1.5-point reduction in movement pain NRS scores compared with the lumbar plexus block group (L) during key postoperative periods (eg, 6 and 12 hours), indicating that the enhanced analgesic effect reached or approached the threshold of clinical significance.
However, the core value of this combined intervention may lie more in the multidimensional and synergistic improvements it provides. For elderly patients, the goal of postoperative management is not only to reduce absolute pain scores but also to minimize treatment-related burden, especially opioid-related adverse effects. Our results showed that, along with improved analgesia, the combination regimen significantly reduced total perioperative opioid exposure, postoperative analgesic requirements, and the incidence of nausea and vomiting, while enhancing patient satisfaction and quality of early recovery. This combination of “moderate analgesic enhancement” and “reduced multiorgan adverse events” constitutes an optimized strategy with clear net clinical benefits.
Particularly in elderly populations, reducing opioid use directly lowers the risk of respiratory depression, delirium, and gastrointestinal dysfunction, which may promote a smoother and faster recovery process. Therefore, the clinical significance of the combined regimen is reflected in the optimization of the overall benefit-risk profile, rather than a dramatic difference in a single pain score.
The limitation of this study is that the press acupuncture set is too short. Although it can reduce the discomfort of patients to a great extent, compared with conventional acupuncture, it may not stimulate the meridians enough. Secondly, due to the limited sample size and the difference of selected acupuncture points, no effect on inflammation inhibition can be found after surgery. In the future, the sample size will be increased, the acupuncture method with a longer needle body will be adopted, and more effective acupuncture points combined with nerve blocks will be explored to provide a safer and more effective clinical choice for anesthesia technology.
Data Sharing Statement
The data supporting the conclusions of this study are publicly available in the Supplementary Dataset of the Chinese Clinical Trial Registry (ChiCTR) at [https://www.chictr.org.cn/bin/project/edit?pid=204978]. For additional unpublished raw data of this study (eg, individual patient pain score records and intraoperative medication administration logs), reasonable requests can be submitted to the corresponding author (Xutong Zhang, email: [[email protected]]) for non-commercial research purposes. All data requests must comply with the ethical approval guidelines of the Second Affiliated Hospital of Wenzhou Medical University and the requirements of relevant data protection regulations.
Consent for Publication
Written informed consent for publication has been obtained from all participants. The consent givers have been shown and reviewed the complete content of the manuscript intended for publication, confirming their agreement to its dissemination. The corresponding author will provide copies of the signed consent forms to the journal editorial office if requested.
Acknowledgments
We thank XTZ for technical assistance in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that this study was partially supported by the Department of Science and Technology of Zhejiang Province (LGD21H310004).
Disclosure
Mr Xutong Zhang reports a patent “visual lumbar puncture needle” issued. The authors declare that the research was conducted in the absence of any other commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Learmonth ID, Young C, Rorabeck C. The operation of the century: total hip replacement. Lancet. 2007;370:1508–14. doi:10.1016/S0140-6736(07)60457-7
2. Liu J, Li X, Xie W, et al. Risk factors and short-term outcomes of postoperative pulmonary complications in elderly patients after cardiopulmonary bypass. Clin Interv Aging. 2024;19:31–39. doi:10.2147/CIA.S439601
3. Auckley ED, Bentov N, Zelber-Sagi S, Jeong L, Reed MJ, Bentov I. Frailty status as a potential factor in increased postoperative opioid use in older adults. BMC Geriatr. 2021;21(1):189. doi:10.1186/s12877-021-02101-4
4. De Simone B, Chouillard E, Podda M. The 2023 WSES guidelines on the management of trauma in elderly and frail patients. World J Emerg Surg. 2024;19:18. doi:10.1186/s13017-024-00537-8
5. Kukreja P, Uppal V, Kofskey AM. Quality of recovery after pericapsular nerve group (PENG) block for primary total hip arthroplasty under spinal anaesthesia: a randomised controlled observer-blinded trial. Br J Anaesth. 2023;130(6):773–779. doi:10.1016/j.bja.2023.02.017
6. Lee KH, Wang JC, Chang CY, et al. Regional anaesthesia modalities for primary total Hip arthroplasty: a systematic review and component network meta-analysis. Br J Anaesth. 2025;135(2):469–482. doi:10.1016/j.bja.2025.04.019
7. Safa B, Trinh H, Lansdown A, et al. Ultrasound-guided suprainguinal fascia iliaca compartment block and early postoperative analgesia after total hip arthroplasty: a randomised controlled trial. Br J Anaesth. 2024;133(1):146–151. doi:10.1016/j.bja.2024.04.019
8. Huang X, Deng S, Lei X, Lu S, Dai L, She C. Effect of enhanced recovery after surgery on older patients undergoing transvaginal pelvic floor reconstruction surgery: a randomised controlled trial. BMC Med. 2025;23(1):43. doi:10.1186/s12916-025-03880-y
9. Wang Y, Du X, Duan C, et al. Regulating the plasticity of hippocampal neurons via electroacupuncture in depression model mice. Cell Prolif. 2025;58(10). doi:10.1111/cpr.70057
10. Zhou X, Sun Z, Cui Y, Yin H. Novel insights of acupuncture in ischemic stroke: orchestrating neuro-endocrine-immune network. Front Immunol. 2026;17:1772371. doi:10.3389/fimmu.2026.1772371
11. Chen X, Tong S, Zhu Y, Xu T, Guo X, Zhong W. Immediate modulations of cheek acupuncture on brain oscillations and connectivity in individuals with chronic pain. IEEE Trans Neural Syst Rehabil Eng. 2025;33:4229–4240. doi:10.1109/TNSRE.2025.3621122
12. O’Brien K, Feng R, Sieber F, et al. Outcomes with spinal versus general anesthesia for patients with and without preoperative cognitive impairment: secondary analysis of a randomized clinical trial. Alzheimers Dement. 2023;19(9):4008–4019. doi:10.1002/alz.13132
13. Neuman MD, Feng R, Carson JL, et al. Spinal anesthesia or general anesthesia for hip surgery in older adults. N Engl J Med. 2021;385(22):2025–2035. doi:10.1056/NEJMoa2113514
14. Lee S, Xue Y, Petricca J, et al. The impact of pre-operative depression on pain outcomes after major surgery: a systematic review and meta-analysis. Anaesthesia. 2024;79(4):423–434. doi:10.1111/anae.16188
15. Greig P, Sotiriou A, Kailainathan P, et al. Evaluation of neuraxial analgesia on outcomes for patients undergoing robot assisted abdominal surgery. J Clin Anesth. 2024;95:111468. doi:10.1016/j.jclinane.2024.111468
16. Hatton GE, Kregel HR, Pedroza C, et al. Age-related opioid exposure in trauma: a secondary analysis of the multimodal analgesia strategies for trauma (MAST) randomized trial. Ann Surg. 2021;274(4):565–571. doi:10.1097/SLA.0000000000005065
17. Herzig SJ, Anderson TS, Jung Y, Ngo L, Kim DH, McCarthy EP. Relative risks of adverse events among older adults receiving opioids versus NSAIDs after hospital discharge: a nationwide cohort study. PLoS Med. 2021;18(9):e1003804. doi:10.1371/journal.pmed.1003804
18. Santosa KB, Priest CR, Oliver JD, et al. Long-term health outcomes of new persistent opioid use after surgery among medicare beneficiaries. Ann Surg. 2023;278(3):e491–e495. doi:10.1097/SLA.0000000000005752
19. Usichenko TI, Henkel BJ, Klausenitz C, et al. Effectiveness of acupuncture for pain control after cesarean delivery: a randomized clinical trial. JAMA Network Open. 2022;5(2):e220517. doi:10.1001/jamanetworkopen.2022.0517
20. Tan LL, Kuner R. Neocortical circuits in pain and pain relief. Nat Rev Neurosci. 2021;22(8):458–471. doi:10.1038/s41583-021-00468-2
21. Bae SJ, Ji JY, Oh JY, et al. The role of skin mast cells in acupuncture induced analgesia in animals: a preclinical systematic review and meta-analysis. J Pain. 2021;22(12):1560–1577. doi:10.1016/j.jpain.2021.06.006
22. Müller M, Schmucker C, Naumann J, Schlueter N, Huber R, Lederer AK. Acupuncture in management of acute dental pain - A systematic review and meta-analysis. Jpn Dent Sci Rev. 2023;59:114–128. doi:10.1016/j.jdsr.2023.02.005
23. Shi JT, Cao WY, Zhang XN, et al. Local analgesia of electroacupuncture is mediated by the recruitment of neutrophils and released β-endorphins. Pain. 2023;164(9):1965–1975. doi:10.1097/j.pain.0000000000002892
24. Chen Z, Yao K, Wang X, et al. Acupuncture promotes muscle cells ATP metabolism in ST36 acupoint local exerting effect by activating TRPV1/CaMKII/AMPK/PGC1α signaling pathway. Chin Med. 2025;20(1):112. doi:10.1186/s13020-025-01169-z
25. Wang J-H, Wang -N-N, Yuan B. Anti-inflammation mechanism of electro-scalp acupuncture in treatment of ischemic stroke based on IL-12 mediated JAK/STAT signaling pathway. Zhongguo Zhen Jiu. 2022;42(10):1137–1144. doi:10.13703/j.0255-2930.20210821-0006
26. Liu SB, Wang ZF, Su YS, et al. A neuroanatomical basis for electroacupuncture to drive the vagal-adrenal axis[J]. Nature. 2021;598(7882):641–645. doi:10.1038/s41586-021-04001-4
27. Kim BT, Baek CH, Kim JG, Elhassan BT. Arthroscopic lower trapezius tendon transfer effectively relieves pain and improves shoulder function in patients with irreparable infraspinatus tears: minimum 5-year follow-up. Arthroscopy. 2025;41(8):2774–2781. doi:10.1016/j.arthro.2025.01.044
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.