Back to Journals » Journal of Pain Research » Volume 18
Acupotomy for Military Training-Induced Lumbar Radiculopathy with Sciatica: Protocol of a Randomized Controlled Trial
Authors Hong K, Gao J, Hu L, Long X, Wu X, Wen B
Received 3 May 2025
Accepted for publication 5 August 2025
Published 16 August 2025 Volume 2025:18 Pages 4123—4138
DOI https://doi.org/10.2147/JPR.S535852
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Kun Hong,1,2,* Juan Gao,3,* Lijuan Hu,3 Xiaomei Long,4 Xi Wu,2 Boping Wen3
1Department of Acupuncture and Moxibustion No.3 Affiliated Hospital of Chengdu University of Traditional Chinese Medicine (West District), Chengdu, Sichuan, People’s Republic of China; 2College of Acupuncture, Moxibustion and Tuina, Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, People’s Republic of China; 3Department of Rehabilitation Medicine, General Hospital of the Western Theater of the Chinese People’s Liberation Army, Chengdu, Sichuan, People’s Republic of China; 4Department of Pharmacy, Chongqing Yongchuan District People’s Hospital, Chongqing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Boping Wen, General Hospital of the Western Theater of the Chinese People’s Liberation Army, Chengdu, Sichuan, People’s Republic of China, Tel +86 13658002028, Email [email protected] Xi Wu, Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, People’s Republic of China, Tel +86 18008020710, Email [email protected]
Background: Military personnel face elevated risks of chronic sciatica due to repetitive mechanical loading during combat training. Conventional therapies, such as nonsteroidal anti-inflammatory drugs (NSAIDs) and physical therapy, often fall short in addressing the urgent need for rapid functional recovery. Acupotomy, a minimally invasive technique that integrates acupuncture with microsurgical dissection, has the potential to alleviate both central and peripheral nerve compression; however, its efficacy within military populations remains inadequately studied.
Methods: This single-center, parallel-group randomized controlled trial will enroll 80 active-duty military personnel (aged 18– 45 years) with MRI-confirmed L4–S1 lumbar disc herniation and sciatica for at least three months. Participants will be randomly assigned in a 1:1 ratio to receive either ultrasound-guided acupotomy (administered once a week for a total of four sessions) or sham acupotomy. The primary outcomes will include leg pain intensity, measured using the Visual Analogue Scale (VAS), and functional disability, assessed via the Oswestry Disability Index (ODI). Secondary outcomes include lumbar function (as measured by the Japanese Orthopaedic Association scale), blinding efficacy, and adverse events.
Conclusion: This study aims to provide high-quality evidence for the treatment of military training-related sciatica with acupotomy via a rigorous RCT design. If the results confirm its efficacy and safety, it could address multiple levels of nerve compression in ≤ 4 weeks, thereby redefining nonsurgical therapies in direct support of combat readiness. Future studies should expand the scope of the study and deepen the mechanism exploration to promote its application in a wider range of clinical scenarios.
Trial Registration: This protocol has been registered at ITMCTR (No. 2025000628. Registered on: 1 April 2025).
Keywords: acupotomy, lumbar radiculopathy, military training, randomized controlled trial, sciatica
Introduction
Background and Rationale
Sciatica is a neuropathic pain syndrome characterized by pain radiating along the sciatic nerve distribution, resulting from mechanical compression or inflammatory stimulation of the L4-S1 nerve roots commonly caused by lumbar disc herniation (LDH), spinal stenosis, or degenerative spondylolisthesis.1,2 Active-duty military personnel exhibit a 40% higher incidence of lumbar spondylolisthesis with sciatica compared to civilians, with 15% progressing to chronic low back pain.3 Harsh training regimens involving repetitive weight lifting, prolonged load-bearing, and high-impact maneuvers elevate lumbar intravertebral disc pressures by 300–400%,4,5 generating a biomechanical environment that predisposes to annular fissures, nucleus pulposus herniation, and subsequent nerve root compression and irritation.6
In general, the herniated disc material predominantly causes mechanical compression and neuroinflammation, which would lead to perineural fibrosis, ectopic neuronal discharge, and central sensitization.7,8 Compounding this, mandatory load carriage induces a “double-crush” phenomenon: nerve roots are compressed both centrally (by disc herniation or spinal stenosis) and peripherally (by myofascial adhesions from sustained postural stress during load-bearing).9 Such cumulative microtrauma, combined with inadequate recovery between training cycles, accelerates the transition to chronic, treatment-resistant sciatica.10
Conventional first-line therapies exhibit limited effectiveness in active-duty service members. NSAIDs have a high risk of gastrointestinal bleeding and nephrotoxicity for military personnel.11,12 Epidural steroids do not address structural compression and require repeat injections in 30–40% of cases.13 Physical therapy is difficult to adhere to because of time constraints and disruption to tactical training.14 Surgical interventions such as microdiscectomy, while often providing substantial symptomatic relief, necessitate prolonged recovery periods that impair combat readiness. Furthermore, postoperative fibrosis may compromise proper tactical gear fitment and predispose to secondary musculoskeletal injuries.15,16 These collective therapeutic shortcomings highlight the critical need for interventions capable of delivering rapid functional restoration without compromising military operational capacity.
Acupotomy, a minimally invasive technique integrating traditional acupuncture principles with microsurgical dissection, addresses both central and peripheral nerve compression by releasing myofascial adhesions and osseoligamentous stenosis.17–19 Preclinical studies show that acupotomy could downregulate pro-inflammatory cytokines (IL-6, TNF-α) in compressed nerve roots, facilitate axonal repair.20 Clinically, in a recent cohort also showed that acupotomy could produce significant pain reduction and functional improvement.21 The mechanisms of acupotomy for treating intervertebral foramen stenosis are to address ligamentous decompression and peripheral nerve entrapment via lumbar perineural release, with particular therapeutic relevance for military patients.22
Objectives
The effects of acupotomy for LDH have not yet been fully confirmed because high credibility evidence is scant, and no published protocol of a randomized controlled trial can be found that is about the effectiveness and safety of the acupotomy intervention in the patient with LDH. Therefore, we designed the protocol of a randomized controlled trial to review and estimate the effects of acupotomy for treating LDH and its related symptoms, aiming to provide references for clinical treatment of LDH.
Methods
Trial Design
This is a single-center, parallel-group, randomized, sham-controlled trial consisting of 4 weeks of treatment and 4 weeks of follow-up. The procedure of the trial is shown in Figure 1. This protocol is reported following the Standard Protocol Items: Recommendations for Interventional Trials.
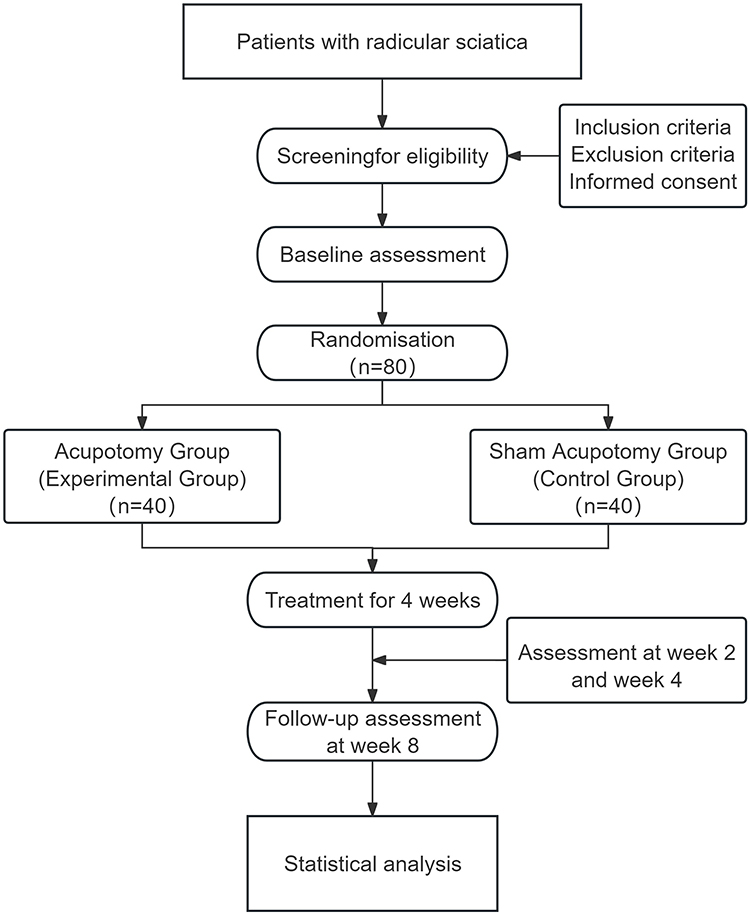 |
Figure 1 Flow diagram of the trial procedure. |
Study Participants
The trial will be conducted at the General Hospital of the Western Theatre of the Chinese People’s Liberation Army according to the 2019 sciatica diagnosis and treatment criteria for participants diagnosed with radicular sciatica.23 Enrolled participants will be assessed for eligibility by a specialised physician and will sign an informed consent form to participate following voluntary agreement.
Eligibility Criteria
Inclusion Criteria
Patients will be considered for enrolment if they meet the following criteria: (1) Aged 18 to 45 years, (2) with MRI-confirmed L4–S1 lumbar disc herniation and corresponding radicular symptoms, manifesting as unilateral lower limb radiation below the knee persisting >3 months, alongside either a positive straight leg raise test or objective neurological deficits (sensory disturbances, motor weakness, or reflex abnormalities).
Exclusion Criteria
Exclusion criteria include: (1) sciatica induced by other diseases than lumbar disc herniation (eg, spinal tumors, infections, or fractures), (2) having severe spinal disease or severe progressive neurological symptoms, (3) having cardiovascular, liver, kidney or haematopoietic system diseases, mental health disorders or other severe coexisting diseases, (4) pregnant or lactating women or those planning to conceive during the trial, (5) taking drugs that have a therapeutic effect on sciatica, (6) having had lumbar disc surgery within the past 1 year, (7) planning to receive surgery or interventional treatment during the treatment period.
Criteria for Discontinuing or Modifying Allocated Interventions
- patients who failed to complete the treatment schedule in accordance with the design of the study protocol after enrollment;
- patients with poor compliance, who change or receive other related treatments during the course of the study;
- patients with serious complications or other serious illnesses during the course of the study;
- patients who request to discontinue the trial or withdraw from the study during the course of the trial;
Interventions
Acupotomy or sham acupotomy will be performed by a professionally trained needleblade practitioner. All practitioners completed a 40-hour standardized course endorsed by the Chinese Association of Acupuncture and Moxibustion (CAAM). Four treatments will be given over a 4-week period, once a week. Treatment offered in this trial is developed by experts and refers to our pilot study.
Acupotomy Group (Experimental Group)
The acupotomy intervention will be performed in strict accordance with the standardized protocol established by the International Society of Pain Medicine (ISPM) and CAAM. The procedure will be guided by real-time ultrasound imaging (Philips EPIQ 7, C5-2B MHz Convex Array Probe) to ensure precise needle placement. The specific operation is as follows:
Step 1: Preoperative Preparation
The patient will be placed in the prone position. Routine disinfection of the local skin will be conducted, and the operator will perform hand disinfection followed by wearing sterile gloves.
Step 2: Lateral Recess Release
Under ultrasound visualization corresponding to Figure 2, 1% lidocaine will be injected for local infiltration anesthesia at the surface landmark designated by the red arrow in Figure 3. A No. 3 acupotomy (0.8 mm × 80 mm, Figure 4) will be inserted percutaneously through the designated point. Under continuous ultrasound guidance, the acupotomy will be advanced cautiously, avoiding vascular and neural structures, towards the target site indicated by the arrow in Figure 2. Release will be performed by piercing the ligamentum flavum without penetrating the dorsal dural sac. Precise cutting maneuvers (2–3 controlled motions) will be executed along the medial border of the facet joint using a “lifting-advancing” technique. The procedure will be terminated immediately upon tactile feedback indicating fascial release, followed by careful needle withdrawal.
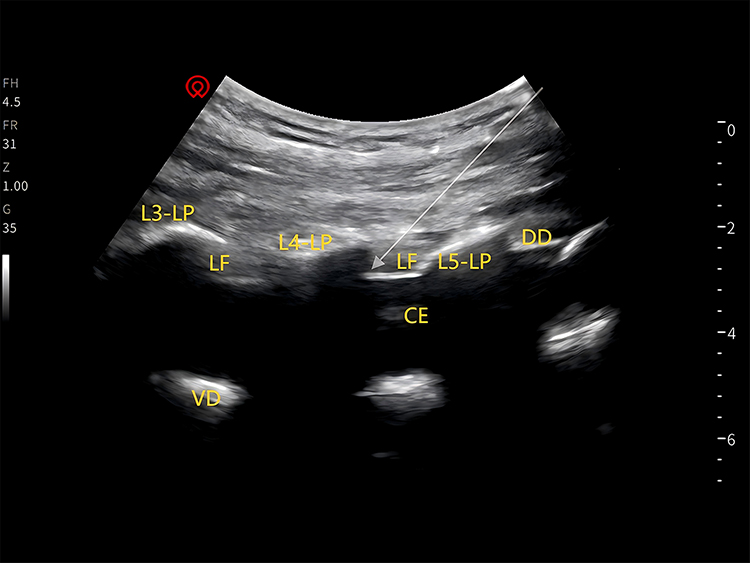 |
Figure 2 Ultrasound Image of the Lateral Recess Location for Acupotomy Release. Note: The arrows show the fourth lumbar disc herniation as the site of acupotomy release. |
 |
Figure 3 Acupotomy Entry Landmark for Lateral Recess Release. Notes: The arrows indicate the sites of the fourth lumbar disc herniation as a column of the acupotomy loosening injection site and the local infiltration anesthesia injection site. |
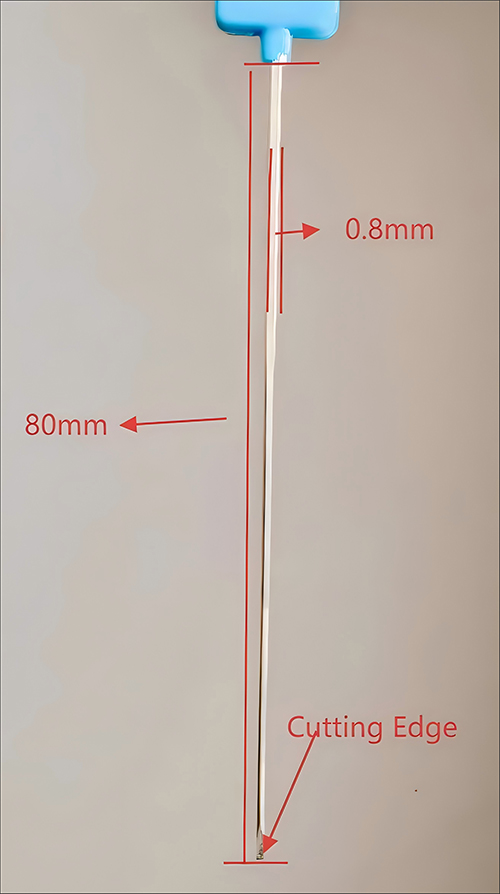 |
Figure 4 No. 3 acupotomy (0.8 mm diameter × 80 mm length). |
Step 3: Intervertebral Foramen (IVF) Outer Orifice Release
Upon achieving ultrasound visualization corresponding to Figure 5, 1% lidocaine will be injected for local infiltration anesthesia at the surface landmark designated by the red arrow in Figure 6. A No. 3 acupotomy will be inserted percutaneously through this point. Under continuous ultrasound monitoring to avoid neurovascular structures, the acupotomy will be advanced cautiously to the target site indicated by the arrow in Figure 5. Precise cutting maneuvers (2–3 controlled motions) will be performed. The procedure will cease immediately upon tactile confirmation of reduced tissue resistance. The acupotomy will be withdrawn under continuous ultrasound visualization to ensure avoidance of adjacent structures.
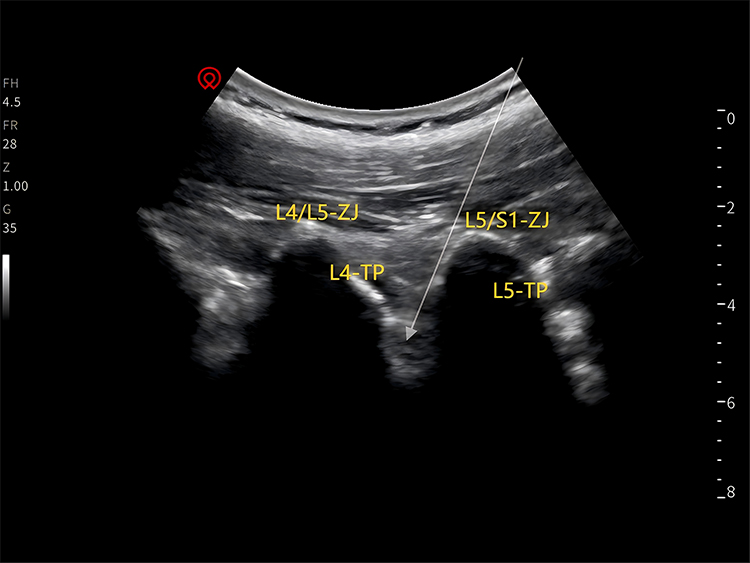 |
Figure 5 Ultrasound Image of the IVF Outer Orifice Location for Acupotomy Release. Note: The arrows show the fourth lumbar disc herniation as the site of acupotomy release. |
 |
Figure 6 Acupotomy Entry Landmark for IVF Outer Orifice Release. Abbreviations: LP, Lamina; L3, The third lumbar vertebra; L4, the fourth lumbar vertebra; L5, the fifth lumbar vertebra; S1, the first sacral vertebra; TP, Transverse Process; DD, Dorsal Dural Sac; VD, Ventral Dural Sac; LF, Ligamentum Flavum; CE, Cauda Equina; ZJ, Zygapophyseal Joint; IVF, Intervertebral Foramen. Notes: The arrows indicate the sites of the fourth lumbar disc herniation as a column of the acupotomy loosening injection site and the local infiltration anesthesia injection site. |
Step 4: Lumbar Nerve Entrapment Site Release
Under real-time ultrasound guidance, the entrapped segment of the lumbar nerve will be localized based on precise anatomical landmarks. Release will be performed using a No. 3 acupotomy, adhering to a standardized four-step insertion protocol:
Insertion: Rapid percutaneous insertion at the ultrasound-identified entrapment site.
Advancement: Layered advancement with continuous ultrasound confirmation of neurovascular structure avoidance.
Verification: Needle tip position will be verified by characteristic fascial resistance patterns.
Release: Targeted fascial release will be performed at the pathological interface identified by hypoechoic tissue characteristics. Instrument withdrawal will commence immediately upon tactile feedback indicating reduced fascial tension, maintaining continuous ultrasound visualization throughout retraction.
Sham Acupotomy Group (Control Group)
The sham procedure will maintain identical parameters to the active intervention group regarding instrumentation (No. 3 acupotomy), patient positioning, anatomical landmarking, sterilization protocols, and treatment schedule, with key procedural modifications the following key procedural modifications:
Step 1: Lateral Recess simulation: the acupotomy will be inserted rapidly longitudinally through the skin with 5–10 mm muscle layer penetration followed by horizontal handle oscillation (amplitude ≤5 mm) for 3 seconds without osseous contact.
Step 2: extraspinal foramen simulation: superficial fascia penetration will be limited to ≤3 mm depth without ligamentous or bony contact, accompanied by combined horizontal-vertical handle shaking (frequency 1 Hz) for 5 seconds.
Step 3: nerve pathway simulation: a controlled 2.0±0.5 mm epidermal puncture will be performed followed by 5-second needle retention without tissue manipulation, with immediate withdrawal upon completion of the timed interval. Withdrawal of all needles will be accompanied by standardized 1-minute digital compression to prevent hematoma formation.
Relevant Concomitant Care Permitted or Prohibited During the Trial
During the trial period, no other Chinese or Western drugs for sciatica and no other treatment methods will be permitted, except for the regulated intervention methods. Celebrex (Pfizer Pharmaceutical) may be prescribed for participants experiencing unbearable pain as rescue medicine, based on their needs.
Outcomes
The efficacy of the intervention will be evaluated by two independent research assistants blinded to group assignment, based on pre-specified primary and secondary outcomes. Assessments will be performed at the following time points: baseline, end of the first treatment course (week 2), end of the second treatment course (week 4), and one-month follow-up (week 8) as detailed in Table 1.
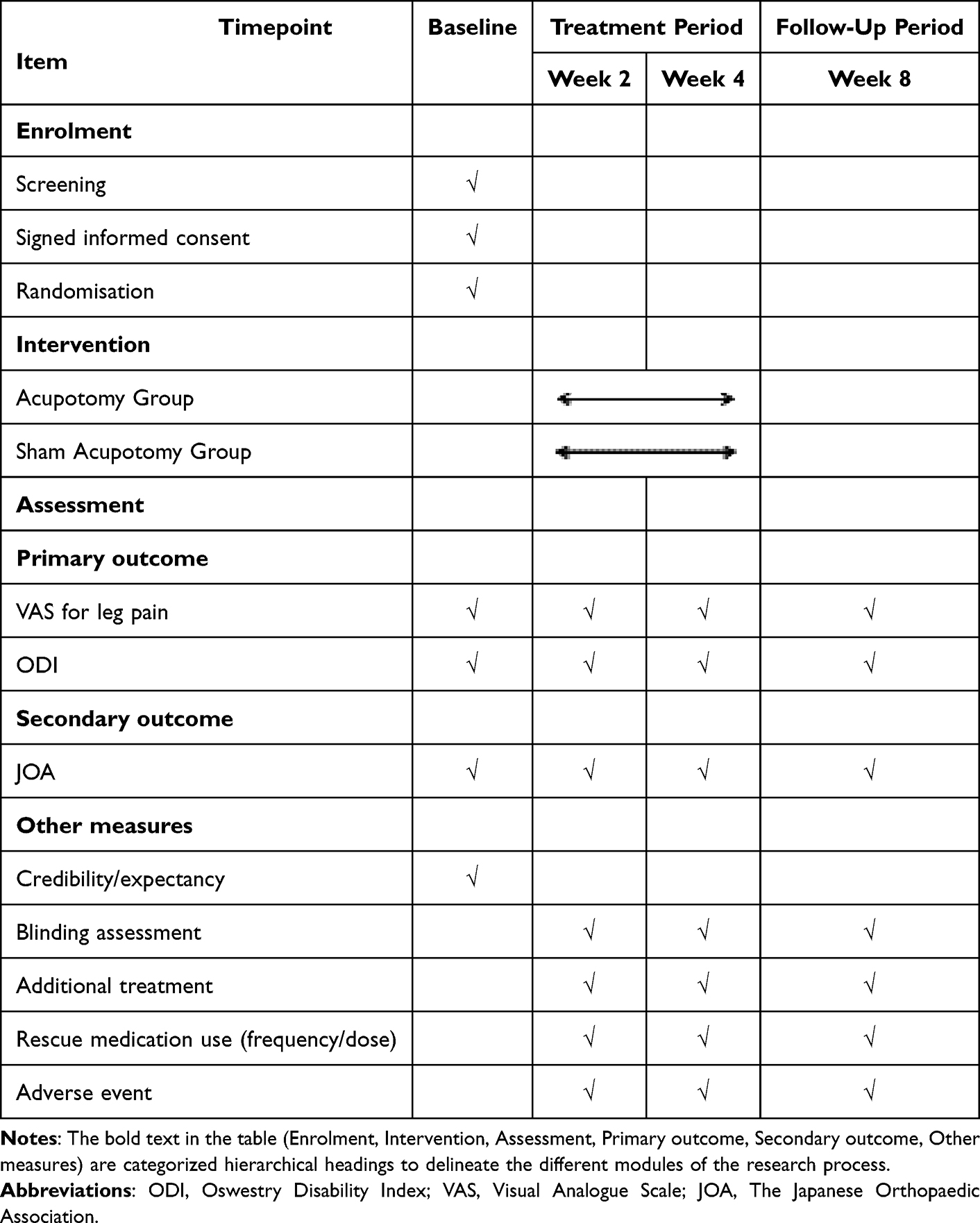 |
Table 1 Schedule of Recruitment, Interventions and Assessments |
Baseline
The eligible participants’ general condition, including demographic and clinical characteristics, age, weight, and treatment history of the disease, will be recorded in CRF. The research assistants will complete the primary and secondary outcomes assessment before the first treatment.
Primary Outcomes
Visual Analogue Scale (VAS) for Leg Pain: The primary outcomes are changes in leg pain intensity and disability from baseline to treatment completion. Leg pain intensity will be quantified using a 100-mm Visual Analogue Scale (VAS), where patients will mark their average pain level over the preceding 24 hours. The scale is anchored by the descriptors “no pain at all” (0 mm) and “my pain is as bad as it could possibly be” (100 mm). Scores will be calculated as the linear distance (in millimeters) from the zero point to the patient’s mark, with higher values reflecting greater pain severity. A reduction of ≥15 mm (on a 100-mm VAS) will be considered clinically significant, consistent with established benchmarks for neuropathic pain interventions.24
Oswestry Disability Index (ODI): Functional disability will be assessed via the 10-item ODI, which evaluates perceived limitations in daily activities, including pain intensity, lifting, self-care, walking, sitting, sexual function, standing, social life, sleep quality, and travel capacity. Each item presents six scenario-based statements ranked from 0 (no disability) to 5 (maximum disability). An improvement of ≥10 points (absolute change) or ≥30% reduction from baseline will be considered a clinically meaningful functional recovery.25
Secondary Outcomes
Japanese Orthopaedic Association (JOA) Low Back Pain Rating Scale: JOA Low Back Pain Rating Scale (score range 0–29) will assess lumbar spine functional status through clinical symptom severity, physical signs, and mobility limitations. Scoring criteria: poor: <10 points, moderate: 10–15 points, good: 16–24 points, excellent: 25–29 points. Lower scores reflect greater functional impairment. Assessments will be conducted at baseline, weeks 2, 4 (end of treatment), and week 8 (follow-up). An increase of ≥5 points from baseline will represent minimal clinically important improvement in lumbar function.26
Blinding
Blinding effectiveness will be evaluated at weeks 2, 4, and 8 using Bang’s Blinding Index (BI). Participants will be asked to guess their group allocation (“verum”, “sham”, or “unsure”), Successful blinding will be defined as a BI not significantly different from 0 (95% CI including 0, P > 0.05); and no systematic guessing patterns detected via chi-square tests.
Adverse Events (AEs)
All AEs will be systematically documented, including time of onset, duration, severity (graded per CTCAE v5.0), actions taken, and causal relationship to treatment (classified as “definite”, “probable”, “possible”, “unlikely”, or “unrelated”).
Rescue Medication Handling
Rescue medication (Celebrex) use will be recorded as follows:
- recorded quantitatively at each assessment (dose, frequency, timing).
- incorporated as a covariate in linear mixed models to control for confounding effects.
- analyzed in sensitivity analyses excluding participants with high-frequency use (>3 doses/week).
Sample Size
Sample size estimation will be performed using G*Power 3.1.9.7 (Heinrich-Heine-Universität Düsseldorf, Germany)27 to detect a clinically relevant difference in leg pain intensity (VAS scores) between groups. Based on preliminary data, we assumed a between-group difference of 15 mm (SD = 18 mm), yielding a Cohen’s d of 0.833 (large effect). A two-tailed independent t-test with α = 0.05 and 90% power required 32 participants per group. Accounting for a 20% attrition rate, the final sample size will be increased to 40 per group (80 total), ensuring sufficient power for intention-to-treat analysis. Normality and homogeneity of variances will be verified post hoc via Shapiro–Wilk and Levene’s tests in R Statistical Software (v4.4.2).
Recruitment
In this trial, patients with radicular sciatica will be recruited via posters in the military. Study doctors will make the diagnoses on the basis of symptoms, physical examinations and imaging findings. To promote recruitment, relevant clinical tests and treatments will be offered free for candidates.
Risk-Benefit Assessment
The benefits that subjects and society will likely receive from this study include the potential for patients’ conditions to be improved; patients will receive free medical care and evaluation of their condition during the trial.
Risks to subjects participating in this trial include: the risk of administering and withdrawing treatment; and the risk of the disease itself. During the trial, the investigator has the right to discontinue the clinical trial in the case at the investigator’s discretion, and to protect the health and interests of the subject in accordance with the rules for combination therapy and medication, and the criteria for discontinuing and withdrawing from the study.
Assignment of Interventions: Allocation
Sequence Generation
Participants will be randomized 1:1 to receive either acupotomy or sham acupotomy. Block randomization with a block size of 4 will be implemented using the blockrand package in R Statistical Software (v4.4.2) to generate the allocation sequence. The randomization scheme will be designed to ensure each block contained exactly 2 participants per group, maintaining balance across recruitment periods.
Concealment Mechanism
The allocation sequence will be concealed using sequentially numbered, opaque, sealed envelopes managed by an independent statistician until interventions will be assigned.
Implementation
The allocation sequence, generated via block randomization (block size = 4) using R Statistical Software (v4.4.2), assigns participants 1:1 to either the acupotomy group or the sham acupotomy group. The Clinical Evaluation Center, acting as an independent entity, will communicate each participant’s randomization number and allocated treatment group to the designated manipulation therapists via encrypted text messages or secure WeChat notifications. This ensures therapists receive clear, unambiguous assignment information while maintaining the integrity of the randomization process.
Assignment of Interventions: Blinding
Who Will Be Blinded
Participants, outcome assessors, and statisticians will be blinded to group allocation. Both verum and sham acupotomy devices will be identical in appearance, and during treatment, the investigator provided subjects with uniformly standardized verbal guidelines to ensure that subjects could not guess whether they belonged to the experimental or control group by verbal cues from healthcare professionals, thus protecting the validity of blinding Practitioners performing the interventions will be unavoidably unblinded due to the technical differences between verum and sham procedures. To minimize performance bias: Practitioners will follow a strict standardized protocol, (1) will be prohibited from communicating with participants regarding treatment details, and (2) will have no role in outcome assessment.
Procedure for Unblinding if Needed
Unblinding, limited to predefined scenarios, will be conducted by authorized personnel with details recorded in the CRF: (1) Post-study completion, after the final follow-up, database locking, and preliminary analysis, an independent statistician or coordinator will retrieve the blinded allocation sequence from sealed envelopes, cross-reference group assignments with anonymized participant IDs, and document the process in the CRF. (2) For participants who actively withdraw or passively withdraw, the treating investigator may request unblinding from the Clinical Evaluation Center for clinical management, with verification of allocation, reason for withdrawal, and involved personnel recorded in the CRF to ensure safety and data integrity.
Data Collection and Management
Data Collection and Tools
A structured electronic data capture (EDC) system will be developed to ensure standardized and accurate collection of study variables. CRFs will be pre-validated and aligned with the trial’s primary and secondary outcomes, including demographic characteristics (age, gender, weight), clinical metrics (VAS, ODI, JOA scores), AEs, and protocol adherence records. Data fields will be designed to capture longitudinal assessments at baseline, weeks 2, 4 (end of treatment), and week 8 (follow-up), with built-in range checks and logical validations to minimize entry errors.
Data Entry and Validation
Trained personnel will perform dual-entry verification using R Statistical Software (v4.4.2) with the tidyverse package for data cleaning and validation. Automated logic checks will be implemented through custom scripts to flag outliers and inconsistencies. A three-phase reconciliation process will be executed: (1) script-driven outlier detection (range checks, cross-variable consistency); (2) manual line-by-line CRF-database comparison; (3) final arbitration by senior data managers for unresolved discrepancies.
Data Storage and Security
All data will be stored on password-protected servers with restricted access permissions. Patient identifiers will be anonymized, and anonymized datasets will be archived for at least 5 years post-publication. Access to raw data will require approval from the principal investigator and ethics committee.
Data Locking
The database will undergo a blinded audit by an independent review panel (principal investigator, biostatistician) prior to locking. Key milestones will include: (1) 100% resolution of data queries via audit trail review. (2) finalization of analysis population definitions. (3) ratification of the statistical analysis plan (SAP) alignment with protocol v2.0. (4) a signed data lock certificate will be formalized database closure, with read-only permissions implemented thereafter.
Quality Control
The trial protocol has been reviewed and revised by experts in the fields of needlepoint, orthopedics, statistics and methodology. Prior to the start of the trial, all investigators will be trained in patient screening, Acupotomy manipulation, and EDC-based data entry. Regular monitoring will be performed by investigators at General Hospital of the Western Theater of the Chinese People’s Liberation Army. The EDC platform enabled granular tracking of data modifications, including user-specific timestamps and revision histories, to ensure protocol adherence and data integrity.
Confidentiality and Ethics Compliance
Patient confidentiality will be maintained through anonymization of all records. Data sharing will adhere to ethical guidelines, with de-identified datasets available upon reasonable request post-publication.
Plans for Collection, Laboratory Evaluation and Storage of Biological Specimens for Genetic or Molecular Analysis in This Trial/Future Use
No biological specimens will be collected in this study.
Statistical Methods
Analysis Principles
All analyses will adhere to the intention-to-treat (ITT) principle, including all randomly assigned participants regardless of protocol adherence or dropout. A per-protocol (PP) analysis will serve as a sensitivity analysis, restricted to participants who complete at least 2 treatment sessions without major protocol violations to evaluate result robustness. Statisticians blinded to group allocation will conduct analyses using R Statistical Software (v4.4.2) with two-sided p < 0.05 denoting statistical significance.
Baseline Data Analysis
Demographic and clinical characteristics (eg, age, gender, baseline VAS, ODI scores) will be summarized using descriptive statistics: continuous variables as mean ± standard deviation (SD) for normal distributions or median (interquartile range, IQR) for skewed data, and categorical variables as counts and percentages. Between-group baseline comparability will be tested using independent t-tests or Wilcoxon rank-sum tests for continuous outcomes and χ²-tests or Fisher’s exact tests for categorical data.
Efficacy Analyses
Primary Outcomes
Leg Pain Intensity (VAS) and Functional Disability (ODI):
Repeated-measures linear mixed models (LMM) will assess mean changes from baseline to follow-up time points (weeks 2, 4, 8). Fixed effects will include group (acupotomy vs sham), time (baseline, week 2, week 4, week 8), and their interaction, with baseline scores as a covariate. Random effects will account for participant-specific variability (intercept and slope). Model assumptions (normality, homogeneity of variance) will be verified using residual plots, and sphericity of the variance-covariance matrix will be tested using Mauchly’s test. If sphericity is violated (P < 0.05), Greenhouse-Geisser corrections will adjust degrees of freedom to maintain Type I error control.
Secondary Outcomes
For lumbar spine function evaluated by the JOA score, longitudinal changes will be analyzed using a linear mixed model identical to that for primary outcomes, treating JOA as a continuous variable. Blinding efficacy will be rigorously assessed at weeks 2, 4, and 8 using Bang’s BI. AE frequencies (graded as mild/moderate/severe per CTCAE v5.0) and treatment-related AEs will be compared between groups using chi-square tests or Fisher’s exact tests for low-frequency events.
Missing Data Handling
Primary outcomes (VAS, ODI) will handle missing data using multiple imputation (MI) under the assumption of Missing at Random (MAR). To assess the robustness of results under potential MNAR mechanisms, sensitivity analyses will be conducted via pattern-mixture models. These models stratify participants based on missing data patterns and estimate outcome trajectories under different MNAR scenarios. Secondary outcomes: Missing data will be addressed via complete-case analysis for exploratory endpoints, with sensitivity analyses assessing the impact of missingness.
Safety Analyses
Serious adverse events (SAEs) will be tabulated descriptively, and their association with treatment groups will be explored using Fisher’s exact tests. Safety summaries will include event severity, causality (definite/possible/unlikely/unrelated), and management protocols.
Credibility/Expectancy Analysis
Baseline credibility/expectancy scores will be analyzed using linear mixed models to assess their association with treatment outcomes. Audio recordings of practitioner–patient interactions will be reviewed to ensure compliance with standardized communication protocols.
Statistical Reporting
Continuous outcomes will be reported as least squares means (±SE) from LMMs, with 95% confidence intervals (CIs) for between-group differences at each time point. Binary outcomes will be presented as proportions (95% CIs), with effect sizes reported as risk ratios (RR) or odds ratios (OR) where appropriate. All analyses will use ITT populations as the primary analysis set, with PP results presented in supplementary tables to demonstrate consistency.
Software and Reproducibility
Statistical code will be archived for reproducibility, with all analyses following a pre-specified Statistical Analysis Plan (SAP) finalized before database locking. Data management and validation will be performed using R Statistical Software (v4.4.2) and its ecosystem (eg, tidyverse, lme4, mice) to ensure ≥99.5% data accuracy and methodological transparency. Statistical analyses will adhere to the ITT principle, including all 80 randomized participants in their originally assigned groups. Sensitivity analyses will be performed on a per-protocol set, defined as participants who completed at least two treatment sessions (4 weeks) without major protocol deviations.
Plans to Give Access to the Full Protocol, Participant Level-Data and Statistical Code
CRF data will be shared on ResMan (www.medresman.org.cn) within 3 months of publication, with access granted following ethical committee review and completion of a data use agreement. Military personnel identifiers (eg, unit number) will be removed during anonymization, and only aggregated data will be released. To protect military-specific privacy, participant unit affiliations and mission-related data will be excluded from the dataset, and anonymized IDs will be generated using a hashing algorithm unlinkable to personal information.
Oversight and Monitoring
The trial governance will be structured to ensure adherence to protocol objectives and ethical standards. A Trial Steering Committee (TSC) will serve as the central oversight body, comprising senior principal investigators, a clinical research center director, and an ethics committee representative. The principal investigators will oversee trial conduct, resolve protocol deviations, and approve major amendments. The clinical research center director will coordinate operational activities, including site management and resource allocation. The ethics committee representative ensured compliance with the Declaration of Helsinki, reviewed safety reports, and monitored informed consent processes. The TSC will convene quarterly to review trial progress, safety data, and Good Clinical Practice (GCP) compliance, with meeting minutes will be archived for audits.
A three-tiered Data Monitoring Committee (DMC) will be established to safeguard data integrity and participant safety. First-level monitors will include certified practitioners with extensive clinical experience, who will be responsible for real-time procedural oversight during interventions, verifying ultrasound-guided needle placement, and documenting participant retention efforts. Second-level monitors, comprising ethics and compliance specialists, will review informed consent documentation, track AEs per CTCAE v5.0 guidelines, and ensure timely reporting of serious AEs to the TSC. Third-level monitors, consisting of biostatisticians and data managers, will validate datasets using dual-entry verification and automated logic checks, resolving discrepancies and ensuring alignment with predefined statistical analysis plans.
Independent Adjudication of Treatment-Related AEs
To minimize bias in causality assessment, an independent adjudication committee comprising three experts (a neurologist, an orthopedic surgeon, and a statistician) blinded to group allocation reviewed all reported AEs. The committee evaluated the likelihood of causality (definite, probable, possible, unlikely, or unrelated) based on predefined criteria: (1) temporal relationship between intervention and AE onset. (2) biological plausibility of the AE mechanism. (3) exclusion of confounding factors (eg, pre-existing conditions). Discrepancies in adjudication will be resolved through majority voting, and final determinations will be documented in the CRFs.
Quality Control Mechanisms
Eligibility criteria will be strictly enforced by board-certified neurologists using standardized diagnostic assessments, including imaging-confirmed disc herniation and clinical evaluations. A random 10% of eligibility records will undergo monthly audits to mitigate selection bias. CRFs will be completed within 24 hours of participant assessments, with amendments requiring dual signatures and timestamped justifications. Statistical oversight will include blinded reviews of data cleaning protocols and missing data imputation strategies, such as multiple imputation for primary outcomes. Data management utilized validated software to ensure reproducibility, with all analytical syntax archived for audit purposes.
Reporting and Documentation
Monitoring reports will be generated at multiple tiers: First-level monitors will submit monthly updates on protocol adherence and participant compliance, while second-level monitors will compile quarterly summaries of safety profiles and ethics compliance. Prior to database lock, third-level monitors confirmed resolution of all data queries and validated population definitions. All reports will be stored in a secure repository accessible only to authorized personnel and regulatory authorities. This structured approach ensured rigorous oversight, transparency, and alignment with international clinical research standards.
Adverse Event Reporting and Harms
Adverse Event Recording and Reporting Methods
All AEs, regardless of severity, will be systematically documented according to the CTCAE v5.0. However, only AEs of Grade ≥2 (moderate to severe) will be included in the primary safety analysis to focus on clinically meaningful risks.
Treatment of Serious Adverse Events (SAE)
SAE refers to events that cause death, permanent or significant disability, permanent damage to organ function, or result in hospitalization or prolonged hospitalization. The researcher should immediately take necessary measures to ensure the safety of the subject in the event of an SAE and must report the SAE to the sponsor and the ethics committee within 24 hours. If the SAE requires emergency unblinding, the clinical trial center and the blind editor should jointly perform the unblinding. The researcher will then decide on further treatment measures based on the unblinded information.
Plans for Communicating Important Protocol Amendments to Relevant Parties (Eg Trial Participants, Ethical Committees)
Any modification of the protocol must be approved by the study organizer, the ethics committee, and the clinical research center. Additionally, all modifications must be updated in the clinical research registration center.
Dissemination Plans
The results of the trial will be published in peer-reviewed journals and disseminated to the media and the public.
Discussion
The rising global healthcare burden of lumbar disc herniation (LDH) has intensified research into effective therapies. While prior studies have evaluated acupuncture and massage for sciatica in civilian populations,28,29 combat-related low back pain frequently involves disc herniation with sciatica—present in 62% of cases.30 Traditional therapies are often suboptimal for military operational contexts, as prolonged recovery times and side-effect risks conflict with operational imperatives. A 2025 meta-analysis of interventional pain techniques31 demonstrated that ultrasound-guidance reduces adverse events by 37% compared to blind procedures, supporting its risk-reduction utility in resource-constrained settings. This study addresses an evidence gap by examining non-pharmacological interventions for occupational sciatica and proposing military healthcare improvements. If proven effective, acupotomy could emerge as a pivotal non-pharmacological military medicine treatment, reducing reliance on NSAIDs and epidural injections. Its short recovery enables weekly sessions, potentially decreasing medical discharges through accelerated return-to-duty rates—critical for sustaining combat readiness. Future cost-effectiveness analyses may establish its economic advantage over surgery or long-term pharmacotherapy, with findings extending to civilian cohorts like firefighters facing comparable physical demands.
The study has several limitations. Acupotomy’s efficacy is highly operator-dependent, relying significantly on practitioner skill and experience. Primary outcomes were assessed only at 4 weeks and 1 month post-treatment, leaving its long-term effectiveness (eg, at 6 months or 1 year) unknown. The participant cohort consisted solely of active-duty military personnel aged 18–45, limiting generalizability to other populations. Additionally, the nature of the intervention complicates blinding and introduces potential placebo effects, which could impact the assessment of allocation concealment. We must also account for neurophysiological effects from the sham procedure. A superficial puncture (5–10 mm depth) may stimulate cutaneous nociceptors, potentially inducing transient pain modulation through gate control mechanisms. Alternatively, it might trigger limited pro-inflammatory cytokine release (eg, IL-6),32 contributing to non-specific pain modulation. While we will statistically control for rescue medication (Celecoxib), its analgesic effects may obscure the treatment’s therapeutic benefits. This approach reflects real-world military clinical practice, where adjunct medication is often unavoidable in severe sciatica cases. Dynamic MRI for intervertebral foraminal volume assessment was considered but omitted due to cost and logistical constraints in military settings.
Future studies will elucidate acupotomy’s mechanisms by incorporating biomarker assessments and advanced imaging. Dynamic MRI will evaluate intervertebral foramen volume changes, while ultrasound elastography measures lumbar fascial tension. Neurophysiological monitoring via electromyography and nerve conduction velocity will assess nerve function recovery, clarifying the “mechanical decompression” and “nerve remodeling” mechanisms. Additionally, multicenter validation with larger samples from diverse military units will be conducted, alongside long-term follow-ups to examine chronic pain prevention and symptom recurrence rates. Studies will also explore combining acupotomy with physical therapy or core training,33 potentially optimizing military rehabilitation and accelerating service members’ return to duty.
Abbreviations
AE, Adverse Event; CAAM, Chinese Association of Acupuncture and Moxibustion; CRF, Case Report Form; CTCAE, Common Terminology Criteria for Adverse Events; DMC, Data Monitoring Committee; EDC, Electronic Data Capture; GCP, Good Clinical Practice; ISPM, International Society of Pain Medicine; ITT, Intention-To-Treat; JOA, Japanese Orthopaedic Association Low Back Pain Rating Scale; LDH, Lumbar Disc Herniation; MAR, Missing At Random; MI, Multiple Imputation; MNAR, Missing Not At Random; MRI, Magnetic Resonance Imaging; NSAIDs, Nonsteroidal Anti-Inflammatory Drugs; ODI, Oswestry Disability Index; PP, Per-Protocol; SAE, Serious Adverse Event; SAP, Statistical Analysis Plan; TSC, Trial Steering Committee; VAS, Visual Analogue Scale; SD, Standard Deviation; IQR, Interquartile Range; LMM, Linear Mixed Models; BI, Blinding Index; RR, Risk Ratios; OR, Odds Ratios; MICE, Multiple Imputation by Chained Equations.
Data Sharing Statement
All data will be preserved for at least 5 years after publication. The principal investigator will have access to the final trial dataset, and it is permitted for readers to access the trial data by contacting the corresponding author (Boping Wen). Information on patients will remain anonymous including name, age and telephone number.
Ethics Approval and Consent to Participate
The trial protocol (V.2.0, February, 2025) has followed the principles of the Declaration of Helsinki and has been approved by the Ethics Committee of the General Hospital of the Western Theater of the Chinese People’s Liberation Army (No. 2025EC3-ky005). The study has been registered on the International Traditional Medicine Clinical Trials Registry (ITMCTR, http://itmctr.ccebtcm.org.cn/) in April 2025. Written informed consent will be obtained from all participants prior to their enrolment in the study.
Acknowledgment
The authors thank the participants, investigators, and staff at General Hospital of the Western Theater of the Chinese People’s Liberation Army for their contributions.
Author Contributions
Kun Hong and Juan Gao equally contributed to this work and share first authorship. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Supported by General Hospital of the Western Theater of the Chinese People’s Liberation Army Youth Incubation Program (2021-XZYG-C40). The funders had no role in study design, data collection, or analysis.
Disclosure
None of the authors have any potential conflicts of interest to declare in relation to this study. All funding sources for this research will be exclusively allocated to research-related expenses, with no portion used for authors’ personal remuneration, labor fees, or salary costs.
References
1. National Guideline Centre (UK). Low Back Pain and Sciatica in Over 16s: Assessment and Management. London: National Institute for Health and Care Excellence (NICE);2016.
2. Ropper AH, Zafonte RD. Sciatica. N Engl J Med. 2015;372(13):1240–1248. doi:10.1056/NEJMra1410151
3. Knox J, Orchowski J, Scher DL, Owens BD, Burks R, Belmont PJ. The incidence of low back pain in active duty United States military service members. Spine. 2011;36(18):1492–1500. doi:10.1097/BRS.0b013e3181f40ddd
4. Attwells RL, Birrell SA, Hooper RH, Mansfield NJ. Influence o-f carrying heavy loads on soldiers’ posture, movements and gait. Er-Gonomics. 2006;49(14):1527–1537. doi:10.1080/00140130600757237
5. Cohen SP, Gallagher RM, Davis SA, Griffith SR, Carragee EJ. Spine-area pain in military personnel: a review of epidemiology, etiology, diagnosis, and treatment. Spine J. 2012;12(9):833–842. doi:10.1016/j.spinee.2011.10.010
6. Knapik JJ, Reynolds KL, Harman E. Soldier load carriage: historical, physiological, biomechanical, and medical aspects. Mil Med. 2004;169(1):45–56. doi:10.7205/milmed.169.1.45
7. Deyo RA, Mirza SK. CLINICAL PRACTICE. herniated lumbar intervertebral disk. N Engl J Med. 2016;374(18):1763–1772. doi:10.1056/NEJMcp1512658
8. Risbud MV, Shapiro IM. Role of cytokines in intervertebral disc degeneration: pain and disc content. Nat Rev Rheumatol. 2014;10(1):44–56. doi:10.1038/nrrheum.2013.160
9. Upton AR, McComas AJ. The double crush in nerve entrapment syndromes. Lancet. 1973;302(7825):359–362. doi:10.1016/S0140-6736(73)93196-6
10. Chevan J, Riddle DL. Factors associated with care seeking from physicians, physical therapists, or chiropractors by persons with spinal pain: a population-based study. J Orthop Sports Phys Ther. 2011;41(7):467–476. doi:10.2519/jospt.2011.3637
11. Qaseem A, Wilt TJ, McLean RM, Forciea MA. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American college of physicians. Ann Intern Med. 2017;166(7):514–530. doi:10.7326/M16-2367
12. Coxib and traditional NSAID Trialists’ (CNT) Collaboration; Bhala N, Emberson J, Merhi A, et al. Vascular and upper gastrointestinal effects of non-steroidal anti-inflammatory drugs: meta-analyses of individual participant data from randomised trials. Lancet. 2013;382(9894):769–779. doi:10.1016/S0140-6736(13)60900-9
13. Manchikanti L, Kaye AD, Soin A, et al. Comprehensive evidence-based guidelines for facet joint interventions in the management of chronic spinal pain. Pain Physician. 2020;23(3S):S1–S127.
14. Suri P, Rainville J, Kalichman L, Katz JN. Does this older adult with lower extremity pain have the clinical syndrome of lumbar spinal stenosis? JAMA. 2010;304(23):2628–2636. doi:10.1001/jama.2010.1833
15. Weinstein JN, Tosteson TD, Lurie JD, et al. Surgical vs nonoperative treatment for lumbar disk herniation: the spine patient outcomes research trial (SPORT): a randomized trial. JAMA. 2006;296(20):2441–2450. doi:10.1001/jama.296.20.2441
16. Ambrossi GL, McGirt MJ, Sciubba DM, et al. Recurrent lumbar disc herniation after single-level lumbar discectomy: incidence and health care cost analysis. Neurosurgery. 2009;65(3):574–578. doi:10.1227/01.NEU.0000350224.36213.F9
17. Asano H, Plonka D, Weeger J. Effectiveness of acupuncture for nonspecific chronic low back pain: a systematic review and meta-analysis. Med Acupunct. 2022;34(2):96–106. doi:10.1089/acu.2021.0057
18. Li X, Zhang H, Zhang S, et al. Musculoskeletal ultrasound-guided acupotomy therapy in the treatment of refractory nonspecific low back pain: a single-blind, randomized controlled trial. Medicine. 2024;103(52):e41066. doi:10.1097/MD.0000000000041066
19. Zhang Y, Lao L, Chen H, Ceballos R. Acupuncture use among American adults: what acupuncture practitioners can learn from national health interview survey 2007? Evid Based Complement Alternat Med. 2012;2012:1–8. doi:10.1155/2012/710750
20. Yu JN, Guo CQ, Hu B, et al. Effects of acupuncture knife on inflammatory factors and pain in third lumbar vertebrae transverse process syndrome model rats. Evid Based Complement Alternat Med. 2014;2014(1):892406. doi:10.1155/2014/892406
21. Lee JH, Lee HJ, Woo SH, et al. Effectiveness and safety of acupotomy on lumbar spinal stenosis: a pragmatic, pilot, randomized controlled trial. J Pain Res. 2023;16:659–668. doi:10.2147/JPR.S399132
22. Jensen RK, Kongsted A, Kjaer P, Koes B. Diagnosis and treatment of sciatica. BMJ. 2019;367:l6273. doi:10.1136/bmj.l6273
23. Ostelo RW, Deyo RA, Stratford P, et al. Interpreting change scores for pain and functional status in low back pain: towards international consensus regarding minimal important change. Spine. 2008;33(1):90–94. doi:10.1097/BRS.0b013e31815e3a10
24. Fritz JM, Irrgang JJ. A comparison of a modified oswestry low back pain disability questionnaire and the quebec back pain disability scale [published correction appears in Phys Ther. 2008 Jan;88(1):138-9]. Phys Ther. 2001;81(2):776–788. doi:10.1093/ptj/81.2.776
25. Kasai Y, Fukui M, Takahashi K, et al. Verification of the sensitivity of functional scores for treatment results - Substantial clinical benefit thresholds for the Japanese orthopaedic association back pain evaluation questionnaire (JOABPEQ). J Orthop Sci. 2017;22(4):665–669. doi:10.1016/j.jos.2017.02.012
26. Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/bf03193146
27. Yu FT, Liu CZ, Ni GX, et al. Acupuncture for chronic sciatica: protocol for a multicenter randomised controlled trial. BMJ Open. 2022;12(5):e054566. doi:10.1136/bmjopen-2021-054566
28. Da W, Liu S, Qian Q, et al. Five-step knee adjustment manipulation based on the ‘muscle and bone balance’ principle for treating knee osteoarthritis: study protocol for a randomized controlled trial. J Pain Res. 2025;18:1775–1791. doi:10.2147/JPR.S502187
29. Xing WY, Zhang YH, Yang QH, Wang XQ. Prevalence and risk factors of low back pain in military personnel: a systematic review. EFORT Open Rev. 2024;9(10):1002–1012. doi:10.1530/EOR-22-0113
30. Xiao Y, Zhang Y, Li S, et al. Ultrasound-guided drug injection combined with mini-acupotomy therapy for acute lumbar sprain: a prospective interventional study. Eur J Orthop Surg Traumatol. 2025;35(1):108. doi:10.1007/s00590-025-04234-3
31. Lee YS, Kim SY, Lee H, Chae Y, Lee MS. ACURATE: a guide for reporting sham controls in trials using acupuncture. J Evid Based Med. 2023;16(1):82–90. doi:10.1111/jebm.12524
32. Jeong JK, Kim E, Yoon KS, et al. Acupotomy versus manual acupuncture for the treatment of back and/or leg pain in patients with lumbar disc herniation: a multicenter, randomized, controlled, assessor-blinded clinical trial. J Pain Res. 2020;13:677–687. doi:10.2147/JPR.S234761
33. Liu T, Peng Y, Zhu S, et al. Effect of miniscalpel-needle on relieving the pain of myofascial pain syndrome: a systematic review. J Tradit Chin Med. 2015;35(6):613–619. doi:10.1016/s0254-6272(15)30148-5
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.