Back to Journals » Journal of Multidisciplinary Healthcare » Volume 12
Active Care In Practice: Long-Term Experiences From An Education Programme
Authors Ververda J ![]() , Hauge S
, Hauge S
Received 17 June 2019
Accepted for publication 20 September 2019
Published 29 October 2019 Volume 2019:12 Pages 871—879
DOI https://doi.org/10.2147/JMDH.S219775
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Video abstract presented by Janet Ververda.
Views: 77
Janet Ververda, Solveig Hauge
Faculty of Health and Social Sciences, Department of Nursing and Health Sciences, University of South-Eastern Norway, Porsgrunn, Norway
Correspondence: Janet Ververda
Faculty of Health and Social Sciences, Department of Nursing and Health Sciences, University of South-Eastern Norway, Postboks 235, Kongsberg, Porsgrunn 3603, Norway
Tel +47 35 57 54 24
Email [email protected]
Purpose: To explore whether the Active Care education programme has influenced the participants in practice over time and if so how.
Method and material: A hermeneutic explorative approach. Semi-structured focus group interviews and individual interviews with participants from the education programme from 2014 to 2015. Participants came from different areas in care and had different professional backgrounds. Systematic text condensation analysis based on Malterud.
Results: The Active Care programme has given the participants new knowledge that motivated, inspired and gave them power to change their practice. The new knowledge seems to give resonance in their basic values and strengthens their understanding of the importance of the users’ basic needs and right to be empowered.
Conclusion: Active teaching methods that appeal to participants help to understand and expand carers’ repertoire and increases professionalism across professions and positions. Structural factors need to be addressed to meet the goal of integrated person-centered services.
Keywords: healthy ageing, person centered care, empowerment, professionalism
Plain Language Summary
This study describes how the education programme Active Care has helped the participants from across professions and positions to change their practice. The aim of the programme was to teach how the participants could implement activities, based on users’ preferences, to promote health. The participants were interviewed three years after they had completed the programme. Active Care had given the participants tools to use their personal values to meet their users in a professional and empowering way. Active teaching methods that enable the participants to be authentic and are based on their own practice appear to have influence over time.
Introduction
Health can be seen as a summation of the circumstances and actions of an individual during their whole life span. This life-course approach presents opportunities, as people are able to influence how they age by adopting healthier lifestyles and by adapting to age-associated changes. This view demands a reorientation in health care to a preventative model and promotion of rehabilitation and independent living and is known as healthy ageing.1–3
In its global strategy and action plan on ageing and health 2016–2020, the WHO adopted the framework on integrated, people-centered health services or person-centered care (PCC). This framework entails ensuring a continuum of health promotion and responding to people’s preferences, among others.2 Recipients of care, in their context, need to be engaged and empowered, which again demands a better-trained workforce to have the attributes to deliver care along those principles.4
In order to become better trained towards integrated, people-centered health services, the Active Care (AC) education programme was developed and taught across Norway between 2013 and 2015.5,6 The AC programme has been evaluated, but no longer-term effects of an AC program have been explored.5 One of the challenges is that effects of education programmes in health care are difficult to evaluate.7
This study was designed to find out whether the education program had influenced the participants in practice over time and if so how.
The Active Care Education Programme
The aim of the AC education programme is to educate carers from different areas in care and with different professional backgrounds and positions how they can offer their users the opportunity to promote, restore and maintain health with focus on activities. Activities promote health and reduce costs when based on people’s preferences.8–11 Therefore, ideologically, the AC program is grounded in PCC. Even though the use of PCC is more and more common, some claim the terms to be vague, leading to an inconsistent operationalization and implementation of this care approach.4,12,13 This may explain why there still is a gap between the theoretical frameworks and the practical implementation of PCC.14 The active care education programme tried to fill this gap.
Implementation of care based on people’s preferences through various education programmes has been documented.15–18 These programmes are aimed at specific professions, at specific diagnoses, or specific contexts. The AC education programme was aimed at staff who work “close to users/patients in healthcare” as well as “leaders of units and divisions in healthcare”.5 As such, this program is of interest since it educates carers across settings and levels, which is a prerequisite for a mutual understanding and implementation of a PCC approach.4
One of the key ideas in the programme included, therefore, working with assessment methods - and preconditions to implement these methods – related to users, as well as user participation and empowerment. Network and voluntary work were themes to help students identify and mobilize resources in the users’ network and the community. During the whole course of the programme, the students worked on how active care concepts can be implemented systematically to achieve well-being for the person in a care setting. It appeared that implementing AC has flourishing as an outcome.5,6
The programme lasted eight days, spread over four meetings in a local classroom. During the meetings, the students attended lectures on active care-related themes and participated in discussions to relate these themes to their own practice. Students gained further understanding by visiting places in the vicinity where active care concepts were implemented. This allowed students to integrate theory and practice and to obtain better knowledge about local activities and enterprises with the intention of using these in their work. After every meeting, the students delivered an assignment, cumulating in a final exam.
The program used action learning as a method to enable students to learn from experience by understanding one’s role in these experiences and to be aware of other forces influencing the experience.19 The varied academic level of the participants was useful for learning as the different viewpoints contributed to increased reflective activity.20
The aim of this study is to explore whether the Active Care education programme has influenced the participants in practice over time and if so how.
Methods And Material
The Study
To understand how the participants experienced the implementation of the education programme over time, a hermeneutic explorative design was used.21 In this paper, it means that to understand the participants’ experiences, these experiences need to be interpreted in light of the participants’ places of work. Hermeneutics allows to find these meanings in relation to the phenomenon and to interpret these meanings. Hermeneutics also adds a person’s reflection of a situation or experience. This means that the researcher’s reflections about the questions, methods and position may have an impact on the data or knowledge.21
In order to obtain the participants’ understanding, they were invited to focus groups or individual interviews. Focus groups promote dialogue through collective engagement and can be used to achieve higher levels of understanding of issues important to the group. The role of the researcher becomes also de-centred.22,23 The latter was important because the first author was lecturer and facilitator on the program; therefore, socially desirable answers could be expected.
The themes of the interview guide consisted of the themes of the AC education programme (action learning, active ageing, strategies, contexts, network, voluntary work and working together5 and the prerequisites for PCC (attributes of staff, the environment, the process and the outcome of PCC)4 These themes were chosen to find out how knowledge of the AC program was used in integrated PCC.
The Sample
A considerable amount of time was spent on how to collect material and select a purposeful sample. The strength of the AC programme was that the participants came from different areas in care and had different professional backgrounds. This needed to be reflected in the material. In addition, there were participants in the programme in leading positions who might be able to shed light on organizational issues, which is often described as highly important.1,4,14 It was felt that also these elements had to be reflected in the material. The sample had, therefore, to be as varied as possible in order to reflect these different perspectives, but also showing possible similarities. Therefore, we selected two samples: one consisting of leaders and one of the participants who worked directly user related.
In order to get the biggest chance of obtaining respondents, the counties with the largest number of participants in the last years in the AC programme were chosen to meet the demands of sample size.5,22 These 91 participants were invited by email and followed up by phone calls. All but three were willing to be interviewed. However, because of long travel distances, many felt they had to spend too much spare time to get to the interview site. Other possibilities for meeting places and times were offered but did not solve the problem. Only one of the participants could get time off work. Because of these reasons, only two group interviews were held with three participants in one group and two in another. Five other participants were interviewed individually. In all ten participants divided over two counties were interviewed (Table 1).
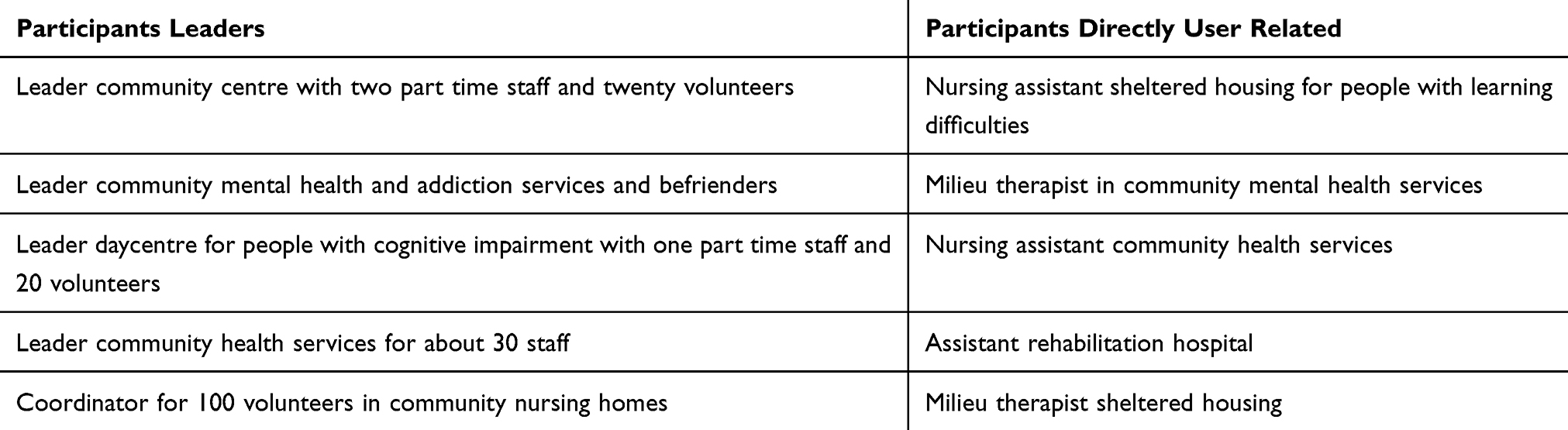 |
Table 1 Participants In The Interviews |
Data Collection
The Interviews
The interviews started by an introduction after which some time was spent stating the purpose of the study, the amount of time needed to complete the interview (max 2 hrs), the right to withdraw from the study (also stated on the form) and how the results were thought to be used. The position of the researcher was underlined and questions from the participants regarding these issues were answered. This was done to create a mutual understanding and an as relaxed and good as possible atmosphere.24 The interviews took place in the autumn of 2018, were taken up on a dictaphone and transcribed.
Material
The material consisted of the transcriptions of the interviews and represents all fields in community health care.
Analysis
The texts were analyzed in the steps according to Malterud’s systematic text condensation.25 In the first step, the texts were read and reread and notes were taken to get a first impression of what the participants had experienced after the education programme was finished and what it meant to them now. From these themes, it became clear how much the respondents stretched themselves to deliver good care, regardless of their place of work and/or position. The words “very complex and ill users” were mentioned by almost all respondents.
In the second step, meaningful units were identified with codes that represented different aspects of the respondents in the education programme. The codes of the leaders and staff were checked and cross-checked against each other on the coding sheet, the themes and the text. The codes seemed to be alike for both leaders and staff. After careful consideration, it was decided to collapse data from both groups of respondents into one. In the following step, the codes were categorized into subgroups. During this condensation process, it was confirmed that the codes from leaders and staff were alike.
Before abstracting these subgroups further in the fourth step, the categories were tested against the texts to make sure the meaning was retained. This extraction and interpretation constituted the hermeneutic circle.21 The content of each category was described and citations were found to represent the categories (Figure 1).
 |
Figure 1 One theme in the analysis process. |
Credibility
It was of importance for the first author to make her position clear, to remain decentered, to focus on listening to the participants and to learn from them. This way a safe environment where the participants could share ideas, beliefs and attitudes could be created, which would validate the experiences of the participants. With this in mind, it was hoped that the chosen design would enable the participants to be honest about their experiences in order to share valuable information on implementation of the AC education programme.26
In the group discussions, the participants’ experiences were recognized, shared and explored. In the individual interviews phrases like “can you tell me a bit more” or “do you have an example” were used to prompt elaboration of the experiences. The concrete experiences showed also validity in the sense that all respondents discussed most themes in a concrete manner. It gave good insight into the day-to-day experiences of the respondents at their place of work.25
Ethical Issues
Ethical approval for this study was obtained from the Norwegian Centre for Research Data. Approval to use the material was obtained from the Centre of Care Research and head of the faculty at University of South Eastern Norway. The participants were traced back with the help from the administrative staff so that they could give their written consent to participate in the study. Those willing to participate were further informed of the objectives of the study. Written consent to use the text of the interviews for this paper was obtained after all questions concerning this study and the intended use of participants’ responses were answered. Confidentiality of the data was maintained.
Results
The results are presented along with four themes (Table 2). Quotes from the material illustrate the findings.
 |
Table 2 Interpreted Themes And Subthemes |
Getting The Knack Of It
“You need the will, ideology, a supervisor and then you see the residents liking it and then it contaminates to colleagues you know”. All respondents mentioned how knowledge from the education programme contributed to increased competence in a demanding system. This phrase sums up how most respondents got the knack of active care, for which the education programme was the impetus.
Most respondents talked about how the education programme increased their motivation. One respondent describes it as follows:
It was so nice to be taken care of a bit for once: simple but good lunches and music in the breaks and to hear that you are doing a good job … it was very motivating and you only want to learn more.
Others underlined the importance of meeting others and being able to discuss their work and get ideas. This wanting to learn, but also doing more varied from taking further courses, to becoming coordinator, to doing a Master or to setting up courses for volunteers about active care.
All but one of the respondents said they still used this systematic knowledge from the course. It was underlined that the combination of theory and practical implementation strengthened their competence and made it stick. “It (the AC program) gave me the tools to think systematically” and “it gave me the words, the terminology, acceptance, gave possibilities, confidence”. As an example, some respondents conveyed they had used this knowledge and confidence to assess their users again, this time asking their users what was important for them. They thought they knew their users well after so many years, but “there were many surprises” and “it did something with us, the way we were thinking”. Another one mentioned that “I got more substance, more words, things I can refer to which helps me to communicate. Also, when I apply for funding I can have my head up high because I know what I do is professional”.
That their knowledge contaminated their colleagues and users was mentioned several times. One said “I use it to show my colleagues that it is possible” and “there are quite a few who need to know how to do that in practice” and “those who want to learn more are offered a course and they think it is really nice”.
Some respondents had found a way of dealing with colleagues who were still unsure: “the positive contamination (sic) gets larger and larger and then those just sit there, feeling embarrassed between the two of them”. One respondent tells “I have used it (the obtained tools) a lot for myself, my colleagues and yes, also for users”.
The Powers That Be
“You better lower your ambitions they said” shows how clear power issues can become when trying to implement different or new views – or wanting to work together on equal terms as a person-centered approach suggests.
Working in collaboration was mentioned by all the respondents. Leaders expressed “When we are confident and clear in our position as leader we can give room to others” and non-leaders confirmed that “you need a clear and safe leader who points out what direction we shall go” or “My leader is very strict. But when I go and see her she listens and then helps if she can”. Others mentioned “My leader is highly involved” or “you really need to work together with your leader”.
Collaboration also included volunteers who are “wise people with a lot of experience” because “we are after all a team and I get a lot of support from them”.
All respondents agreed that the education programme had given a better understanding of the importance of involving the whole team when implementing active care: “As long as you have the same values, it does not matter what position you are in or what your back ground is”.
All but one respondent mentioned lack of collaboration by “the system” meaning the senior management and levels above. One respondent said that “the system is of more importance than the users of it” and another one “there are strong forces, a lot of economics and then there is just us”. One said “I see how much bad management there is around in the public sector. They only look at figures and have really no clue of the resources at all”.
Half the respondents had contacted local politicians, some even in their spare time, to inform them about active care. “They all said they were impressed and that we are doing a good job. They all say they will support us. But when it comes to it, we have not seen a penny”. This was experienced as being let down again and explained as a competition with other issues due to “election time”. One leader had even heard that “White papers are written in the capital; here we are not in the capital” implying that local policy makers had the power to do things their own way.
The gap between specialist- and community care was also mentioned. Although trying to collaborate towards what is best for the user, different communication lines and cultures rather gave the feeling of competing about the user, leaving them being “caught by the system”. The importance of grounding active care top-down and bottom-up in order to make it work was underlined. Only one respondent could say that “there is agreement throughout the whole organization but you need a clearly visible leader”.
Good Things Come In Small Packages
“Suddenly you use a lot of time finding their glasses back”. This theme concerns seeing the user as a person with every day needs and wants in an as normal a context as possible.
All respondents talked about the importance of the small things like reading a paper together, listening to music, going for a walk or “sleeping in as long as they want” when this was important for the user’s well-being. These things were seen as part of everyday life. As one put it “We are more interested in what happens casually, that is what active care has taught me too”. Part of this is facilitating an environment to allow this to happen: “Now I can see a user drinking coffee and sipping a liquor and having a chat with my colleague before lunch” and “we will now open a pub and a café on the premises, they are grown-ups you know”.
One felt that this way of thinking was getting back to the basics. She described how a very quiet place “where you could hear a needle fall” was turned into a place where “nobody eats alone, there is chaos and mess and things get lost but people love it. They say they never want to go back”. Demands from the system were the backside of this person-centered approach. “How can I document these obvious daily events that make people thrive?” Another respondent told about someone with a lot of pain: “To see the happiness in their eyes when being allowed to have a bath to release that pain. It is impossible to describe, so small yet so important for them”.
Another element is a sense of empowerment: “When we find out about their wishes and thoughts we try to facilitate to make it happen”. Most respondents referred to the program where they had learned that “even though we are all different, we are all going for it” so that users, who had feared a situation “came back and smiled from ear to ear”. This could be an ordinary, but long longed for family trip or a holiday “like everybody else”. Experiences like these helped users and staff grow.
Columbus’ Egg
“I cannot understand that things need to be so difficult, it is so obvious”. Most of the respondents had a fair amount of experience in the area they worked in. All respondents mentioned a personal interest in activities that were reinforced by the education programme because it confirmed the righteousness of using activities in their work. Phrases like “that is just how I am” were used to describe their personalities. Characteristics like being generous, giving that little extra and being a prime driver were mentioned. Two respondents felt they had been in the game for such a long time that they had seen most of it. Still, the programme helped them to confirm and systematize their experiences, although one working in mental health felt she had always worked like that since it was inherent in the field.
Four respondents added “I just do it (reading for a user). It is in my own time but I just do it”. Another said “I rather ask forgiveness for having done something than not having been allowed to”, meaning that she would do what she felt was right and informing colleagues afterwards. Others confirmed to do so too when it was about obvious things.
Some respondents called this creativity, which both had positive and ironic connotations. On the positive side, the respondents had examples of how their “outside the box” thinking helped them to find solutions and felt that the education programme had encouraged them to think like that. “Sometimes we fail but then we can learn from that”. One advised her colleagues to stop complaining about rules that could not be bend but rather use energy to “Work around it”. Another used the motto “when you ask what is the worst that can happen, suddenly a lot is possible”.
On the ironic side, the expression “we cannot be octopuses either” sums up all the creative demands on health care workers these days. One nurse mentioned how they cleared an office in the middle of the night to move a patient. “You can always work smarter in theory. Practice can be very different”. Another one told that every now and then staff sighed “Oh, how are we going to solve this now again?” concerning more cuts and yet more documents that needed to be administrated. Several respondents mentioned the benefits of adding creative therapists like musicians and artists to their team, but exchanging these with professional health workers “I would not dare”. At some places, professional competence was needed “to even meet the most acute practical or medical needs”, however hard some “tried to stand up against it”.
Discussion
The AC programme is thus far the only known education program with emphasis on activities across professions to achieve person-centered care. Our overall interpretation of the findings is that the AC program has given the participants new knowledge, which has motivated and inspired themselves and their colleagues and gave power to change their practice. The new knowledge seems to give resonance in their basic values and strengthens their understanding of the importance of the users’ basic needs and right to be empowered. As such, we will argue that the AC programme has led to new knowledge and new practice in a long-term perspective. In the following, we will discuss possible reasons why the participants experienced these long-term effects.
Firstly, having their own work place as a starting point and getting the tools to structure their experiences and knowledge in order to develop their work place, might be an important reason for why the participants still, after four to five years, used the obtained knowledge. During the programme, the close connection between the new theory and their everyday practice was strengthened by sharing and discussing examples. Educational knowledge and everyday knowledge became formed in schemas. When knowledge is organized in memory, it can be preserved and effectively accessed.27 This may explain why the respondents remembered so many aspects of the programme so well.
In addition, it is known that when knowledge is obtained cumulatively and is maintained and further expanded on, retention of this knowledge lasts over many decades.28–30 This means that both the processes and outcomes of education are of importance in learning, as well as how the environment adapts to the changes.7 These factors not only underline the importance of keeping the clinical practice component firmly established in health education31 and to prepare students for dealing with the unpredictable.31,32 It may also explain why the respondents still use knowledge from the AC program on a daily basis.
Studies in other fields confirm that education programmes that meet the beneficial effect of learning in a social setting support a long-term use of new knowledge.33 The open climate in the classroom with discussions, the musical entertainment and informal meetings among the participants in breaks can, therefore, be seen as a contributing factor.34 In addition, was the program based on a so-called hybrid problem-based learning method (H-PBL) whereby PBL is combined with traditional teaching methods.35 Visits in the vicinity to see examples of active care, as well as cumulative assignments reinforcing the aforementioned methods, might have supported the learning process further.
Secondly, another aspect with our findings is the respondents’ descriptions of how well the theoretical basis in the AC program connected with their professional values. Professional values (altruism/caring, excellence, ethics, respect, communication, accountability) are shared by most of the caring professions, but integrity and justice are emphasized. The latter entails being fair, truthful and committed and addressing opportunities for participation in society.36 Some authors call this authenticity and is one of the attributes in PCC.14,37,38
Being authentic is meaningful to the caregiver as a person and has positive effects on personal accomplishment and job satisfaction.39 This human capital also affects quality of care, but tends to be neglected in the dominant business model of health.40 Our findings confirm the importance of humanization in care, which can serve as a means to decrease the workload.41,42 Job satisfaction decreases the intention to leave and ought to be a priority with the future challenges in health care in mind.43
In addition are competence and cooperation recognized as factors that decrease stress and increase job satisfaction, confirming the need for continuous education to achieve a manageable environment to work in.42–44 Continuous education and supervision can facilitate compassion, but demands organizational structures in which the carers’ and users’ values are respected and supported. Clear communication and leadership, as well as involvement of the health care providers, help to find the right balance between personal and professional boundaries to prevent caring fatigue and to ensure a person-centered culture.14,45–47
Innovation can be experienced as a provocation, even though it is grounded in white papers.48 It is unclear whether providers from across divisions and occupations are aware of the importance of having their distinctive roles and input into patient care along the patient pathways. When making these roles explicit, power can become a collaborative matter, rather than competitive or authoritative.49 Although clinical pathways have been implemented in Norway, our findings stress the importance of managers who are able to mediate between policies and practice.50
Implications
This study underlines the importance of developing education program using active teaching methods that appeal to the participants. The combination of theory with practical examples seems particularly valuable to secure long-term effects of education programmes in health care. To meet the challenges of evaluation of health care education programmes, structured measuring tools need to be applied to become clearer on the effects of educational interventions in care. The AC programme has given a step in that direction.
Limitations
The respondents represented all fields in care. Therefore, the sample suits the purpose well. Even so, the respondents in this study were the first to react to the invitation to participate in this study. This may indicate they were especially motivated to share their experiences. It can, therefore, be suggested that this motivation is due to a greater awareness of personal involvement and health care politics.
Conclusion
An education programme such as active care influences participants over time when well delivered. Using active teaching methods that appeal to the participants helps to understand and to expand the carers’ repertoire and increases professionalism. Collaboration is important for implementing active care as an integrated person-centered approach. Structural factors hamper the carers’ professionalism and ought to be addressed to meet the demands of future healthcare. Rather than devaluing active care, an increased focus on educating and supporting staff seems necessary to meet the goal of integrated person-centered services.
Acknowledgments
Many thanks to project leader Gro Lorentzen for our discussions and your patience. A great big thank you to the participants for sharing your experiences with us.
Author Contributions
Both authors contributed substantially to conception and design, data acquisition, data analysis and interpretation. JV designed the study, collected the data, analyzed the data and drafted and critically revised the manuscript for intellectual content and approved the final version. SH contributed to the analysis, supervised the whole writing process critically for scientific content and approved the final version. Both authors are accountable for all aspects of the work and ensure that questions related to the accuracy or integrity of the work are appropriately investigated and resolved. All authors gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. WHO. WHO global strategy on people-centred and integrated health services. Interim report/HIS/SDS/2015.6; 2015. Available from: http://apps.who.int/iris/bitstream/handle/10665/155002/WHO_HIS_SDS_2015.6_eng.pdf;jsessionid=9A678D36FE48474E1483C155C01580F6?sequence=1.
2. WHO. Progress reports. Seventy-first world health assembly; 2016. Available from: http://apps.who.int/gb/ebwha/pdf_files/WHA71/A71_41Rev2-en.pdf.
3. WHO. The global strategy and action plan on ageing and health. Available from: http://www.who.int/ageing/global-strategy/en/.
4. McCormack B, McCance T. Person-Centred Practice in Nursing and Health Care, Theory and Practice. Chichester, West Sussex: Joh. Wiley & Sons; 2017.
5. Lorentzen G. Suksesser og snubletråder. Oppsummering av opplæringsprogrammet Aktiv omsorg. Senter for omsorgsforskning, rapportserie nr. 1/2017 [Successes and pitfalls. Summary of the education programme Active Care. Center of Care research, report series nr. 1/2017]. Available from: http://hdl.handle.net/11250/2434573.
6. Ververda J, Hauge S. Implementing active care through (cultural) activities of daily living: a person centred approach to achieve flourishing. Nurs Open. 2019;6(2):583–590. doi:10.1002/nop2.242
7. Haji F, Morin MP, Parker K. Rethinking programme evaluation in health professions education: beyond ‘did it work? Med Educ. 2013;47:342–351. doi:10.1111/medu.12091
8. Jensen A, Stickley T, Torrissen W, Stigmar K, Arts on prescription in Scandinavia: a review of current practice and future possibilities. Perspect Public Health. 2017;137(5):268–274. doi:10.1177/1757913916676853
9. Conner TS, De Young CG, Silvia PJ. Everyday creative activity as a path to flourishing. J Posit Psychol. 2016;13(2):181–189. doi:10.1080/17439760.2016.1257049
10. Verhaeghe N, De Smedt D, De Maeseneer J, Maes L, Van Heeringen AL. Cost-effectiveness of health promotion targeting physical activity and healthy eating in mental health care. BMC Public Health. 2014;14. doi:10.1186/1471-2458-14-856
11. Disch PG, Lorentzen G. Aktiv omsorg – prioritering, kompetanse og kompetansebehov, Rapport 6/2012. Senter for omsorgsforskning, sør.[Active Care - priorities, competence and need for competence. Report 6/2012., Center for Care Research, south].
12. Soudani S, Fox M. Patient-centred care: clarification of it specific elements to facilitate interpersonal care. J Interprof Care. 2014;28(2):134–141. doi:10.3109/13561820.2013.862519
13. Sharma T, Bamford M, Dodman D. Person-centred care: an overview of reviews. Contemp Nurse. 2015;51(2–3):107–120. doi:10.1080/10376178.2016.1150192
14. Santana MJ, Manalili K, Jolley RJ, Zelinsky S, Quan H, Lu M. How to practice person-centred care: a conceptual framework. Health Expect. 2018;21:429–440. doi:10.1111/hex.12640
15. Carlström ED, Ekman I. Organisational culture and change: implementing person‐centred care. J Health Organ Manag. 2012;26(2):175–191. doi:10.1108/14777261211230763
16. Schwind JK, Lindsay GM, Coffey S, Morrison D, Mildon B. Opening the black box of person-centred care: an arts-informed narrative inquiry into mental health education and practice. Nurse Educ Today. 2014;34(8):1167–1171. doi:10.1016/j.nedt.2014.04.010
17. Scerri A, Innes A, Scerri C. Dementia training programmes for staff working in general hospital settings – a systematic review of the literature. Aging Ment Health. 2017;21(8):783–796. doi:10.1080/13607863.2016.1231170
18. Gee S, Scott M, Croucher M Walking in Another’s Shoes: encouraging person-centred care through an experiential education programme. Canterbury District Health: Good Practice Publication Grant e- Book; 2011. Available from: www.akoaotearoa.ac.nz/gppg-ebook. Accessed May 18, 2018.
19. Tiller T. Aksjonslæring – forskende partnerskap i skolen (2.utg) [Action learning - research partnership at schools (2. ed)]. Kristiansand: Høyskoleforlaget; 2006.
20. Ghaye T. In what ways can reflective practices enhance human flourishing? Reflective Pract. 2010;11(1):1–7. doi:10.1080/14623940903525132
21. Sloan A, Bowe B. Phenomenology and hermeneutic phenomenology: the philosophy, the methodologies, and using hermeneutic phenomenology to investigate lecturers’ experiences of curriculum design. Qual Quant. 2014;48:1291–1303. doi:10.1007/s11135-013-9835-3
22. Creswell JW. Qualitative Inquiry and Research Design. Choosing among Five Traditions.
23. Kamberelis G, Dimitriadis G, Focus groups. Contingent articulations of pedagogy, politics and inquiry. In: NK D, YS L, editors. Collecting and Interpreting Qualitative Material. London: Sage; 2013.
24. Halkier B. Fokusgrupper [Focus groups]. Oslo: Gyldendal; 2010.
25. Malterud K. Systematic text condensation: a strategy for qualitative analysis. Scand J Public Health. 2012;40:795–805. doi:10.1177/1403494812465030
26. Madriz E. Focus Groups in feminist research. In: Denzin NK, Lincoln YS, editors. Handbook of Qualitative Research.
27. Conway M, Cohen G, Stanhope N. Very long‐term memory for knowledge acquired at school and university. Appl Cogn Psychol. 1992;6(6):467–482. doi:10.1002/(ISSN)1099-0720
28. Myers CG. Coactive vicarious learning: towards a relational theory of vicarious learning in organisations. Acad Manage Rev. 2018;43(4):610–634. doi:10.5465/amr/2016.0202
29. Rashid P. Surgical education and adult learning: integrating theory into practice. F1000Res. 2017;6:143. doi:10.12688/f1000research.10870.1
30. Young RF, Astarita AC. Practice theory in language learning. (Report). Lang Learn. 2013;63:171. doi:10.1111/j.1467-9922.2012.00743.x
31. Gonczi A. Competency-based approaches: linking theory and practice in professional education with particular reference to health education. Educ Philos Theory. 2013;45(12):1290–1306. doi:10.1080/00131857.2013.763590
32. Torgersen GE red. Pedagogikk for det uforutsette [Pedagogy for the unexpected]. Bergen: Fagbokforlaget; 2015.
33. Becker C, Lauterbach G, Dettweiler U, Spengler S, Mess F. Effects of regular classes in outdoor education settings: a systematic review on students’ learning, social and health dimensions. Int J Environ Res Public Health. 2017;14(5):E485. doi:10.3390/ijerph14050485
34. Geboers E, Geijsel F, Admiraal W, Ten Dam G. Review of the effects of citizenship education. Educ Res Rev. 2013;9:158. doi:10.1016/j.edurev.2012.02.001
35. Carrió M, Agell L, Baños JE, et al. Benefits of using a hybrid problem-based learning curriculum to improve long-term learning acquisition in undergraduate biology education. FEMS Microbiol Lett. 2016;363(15). doi:10.1093/femsle/fnw159
36. Tsou P, Shih J, Ho MJ. A comparative study of professional and interprofessional values between health professional associations. J Interprof Care. 2015;29(6):628–633. doi:10.3109/13561820.2015.1046159.
37. Laird EA, McCance T, McCormack B, Gribbend B. Patients’ experiences of in-hospital care when nursing staff were engaged in a practice development programme to promote person-centeredness. A narrative analysis study. Int J Nurs Stud. 2015;52(9):1454–1462. doi:10.1016/j.ijnurstu.2015.05.002
38. Williams C, McCormack B. Learning to be an effective person-centred practicioner. In: McCormack B, van Dulmen S, Eide H, Skovdahl K, Eide T, editors. Person Centred Healthcare Research. Chichester: Wiley Blackwell; 2017.
39. van den Pol-Grevelink A, Jukema JS, Smits CH. Person-centred care and job satisfaction of caregivers in nursing homes: a systematic review of the impact of different forms of person-centred care on various dimensions of job satisfaction. Int J Geriatr Psychiatry. 2012;27(3):219–229. doi:10.1002/gps.2719
40. Araujo CA, Cas SA. The nursing professional and creation of values in health. Acta Paulista De Enfermagem. 2016;29(4):III–IV.
41. McCrae N. Person-centred care: rhetoric and reality in a public healthcare system. Br J Nurs. 2013;22(19):P1125–P1128. doi:10.12968/bjon.2013.22.19.1125
42. Fagerström L, Vainikainen P. Nurses’ experiences of nonpatient factors that affect nursing workload: a study of the PAONCIL instrument’s nonpatient factors. Nurs Res Pract. 2014;2014:1–9. doi:10.1155/2014/167674
43. Lindqvist R, Alenius LS, Runesdotter S, et al. Organization of nursing care in three Nordic countries: relationships between nurses´workload, level of involvement in direct patient care, job satisfaction, and intention to leave. BMC Nurs. 2014;13(27):13. doi:10.1186/1472-6955-13-27
44. Van Eerd D, Newman K, Deforge R, Urquhart R, Cornelissen E, Dainty K. Knowledge brokering for healthy aging: a scoping review of potential approaches. Implement Sci. 2016;11(1):140. doi:10.1186/s13012-016-0504-5
45. Peters E. Compassion fatigue in nursing: a concept analysis. Nurs Forum. 2018;53(4):466–480. doi:10.1111/nuf.12274
46. Duarte J, Pinto-Gouveia J. Empathy and feelings of guilt experienced by nurses: a cross-sectional study of their role in burnout and compassion fatigue symptoms. Appl Nurs Res. 2017;35:42–47. doi:10.1016/j.apnr.2017.02.006
47. Sinclair S, Raffin-Bouchal S, Venturato L, Mijovic-Kondejewski J, Smith-Macdonald L. Compassion fatigue: a meta-narrative review of the healthcare literature. Int J Nurs Stud. 2017;69:9. doi:10.1016/j.ijnurstu.2017.01.003
48. Dewar B, MacBride T. Developing caring conversations in care homes: an appreciative inquiry. Health Soc Care Community. 2017;25(4):1375–1386. doi:10.1111/hsc.12436
49. Nugus P, Greenfield D, Travaglia J, Westbrook J, Braithwaite J. How and where clinicians exercise power: interprofessional relations in health care. Soc Sci Med. 2010;71(5):898–909. doi:10.1016/j.socscimed.2010.05.029
50. Helsedirektoratet. Veileder om oppfølging av personer med store og sammensatte behov. Available from: https://helsedirektoratet.no/retningslinjer/oppfolging-av-personer-med-store-og-sammensatte-behov/seksjon?Tittel=helhetlige-pasientforlop-11286.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.