Back to Journals » OncoTargets and Therapy » Volume 14
Acquired ALK Resistance Mutations Identified from Liquid Biopsy in an ALK-Rearranged Squamous Cell Lung Cancer Patient Treated with Sequential ALK TKI Therapy: A Case Report
Authors Yao B, Han X, Pang L, Xu C, Liu S, Cheng X, Chen J
Received 14 April 2021
Accepted for publication 21 July 2021
Published 3 August 2021 Volume 2021:14 Pages 4329—4333
DOI https://doi.org/10.2147/OTT.S315832
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Prof. Dr. Takuya Aoki
Bin Yao,1 Xue Han,2 Linrong Pang,1 Caihong Xu,1 Sisi Liu,2 Xiaochun Cheng,1 Jun Chen1
1Department of Radiotherapy and Chemotherapy, The Affiliated People’s Hospital of Ningbo University, Ningbo, Zhejiang, People’s Republic of China; 2Department of Research and Development, Nanjing Geneseeq Technology Inc., Nanjing, Jiangsu, People’s Republic of China
Correspondence: Xiaochun Cheng; Jun Chen
Department of Radiotherapy and Chemotherapy, The Affiliated People’s Hospital of Ningbo University, Ningbo, Zhejiang, People’s Republic of China
Tel +86-13736005125
; +86-13777975439
Email [email protected] [email protected]
Abstract: Anaplastic lymphoma kinase (ALK) rearrangement is extremely rare in lung squamous cell carcinoma (LSCC), and it remains controversial as to whether LSCC patients with ALK rearrangement can benefit from ALK tyrosine kinase inhibitors (TKIs). Here, we report an LSCC patient with ALK rearrangement who was treated with sequential ALK TKI therapies and experienced a clinical benefit of 35 months. Although the use of ALK TKIs showed clinical benefits, targeted next-generation sequencing (NGS) for dynamic monitoring of circulating tumor DNA (ctDNA) from patient plasma revealed the accumulation of ALK resistance mutations, which could provide valuable information in designing the treatment strategy. Our study highlights the importance of dynamic monitoring of ctDNA using NGS to discover tumor evolution to guide treatment decision-making and provides meaningful insights into the potential treatment options for ALK-positive LSCC patients.
Keywords: ALK rearrangement, dynamic monitoring, resistance mutation, next-generation sequencing
Introduction
Non-small cell lung carcinoma (NSCLC) is the main type of lung cancer, among which the most common histological subtypes are lung adenocarcinoma (LADC) and lung squamous cell carcinoma (LSCC).1 With the development of targeted therapy and next-generation sequencing (NGS) technology, the therapeutic strategies for lung cancer have evolved into targeted precision medicine.
Tumor cells release circulating free DNA (cfDNA) into the blood. A liquid biopsy or blood sample can provide comprehensive genetic information of all cancerous lesions (primary and metastases), which overcomes spatial and temporal heterogeneity of a single tissue biopsy, as well as facilitates dynamic tracking of genomic evolution in a minimally invasive manner.
In LADC, anaplastic lymphoma kinase (ALK) rearrangement has been one of the most common targetable alterations, occurring in approximately 5% of LADC patients.2 In contrast to LADC, ALK-rearranged LSCC is rare with an estimated frequency at 0–1.36%.3 Crizotinib is a first-generation ALK tyrosine kinase inhibitor (TKI) approved for use in ALK-positive NSCLC patients. Despite a high initial efficacy, almost all treated patients eventually develop resistance to crizotinib, including secondary mutations in ALK, and experience disease progression. However, the second-generation ALK TKIs ceritinib, alectinib and brigatinib, are effective against the acquired resistance mutations of crizotinib.4–6 Additionally, third-generation ALK TKIs, including lorlatinib, entrectinib, and ensartinib, also overcome resistance to first- and second-generation ALK inhibitors and exhibit marked efficacy against brain metastasis.7,8 Although ALK-targeted therapy has demonstrated clear clinical utility for NSCLC patients with ALK gene fusions, it remains controversial as to whether ALK-rearranged LSCC patients could benefit from ALK TKIs.9 Herein, we report a LSCC patient with ALK rearrangement who was treated with sequential therapies of ALK TKIs. The patient exhibited a clinical benefit of 35 months and showed stable disease on immunotherapy plus chemotherapy after experiencing failure from multiline treatments.
Case Report
A 46-year-old male with no smoking history was diagnosed with stage IVB LSCC (cT2bN2M1c) with three brain metastases in May 2017 (Supplementary Figure 1). A computed tomography (CT) scan and magnetic resonance imaging (MRI) indicated a 4×5 cm dense mass in the right lung and metastatic lesions in the brain, respectively (Figure 1B, Baseline). Immunohistochemistry (IHC) staining of a tumor biopsy was positive for the LSCC markers P40, P63, and cytokeratin (CK) 5/6, but negative for the LADC markers thyroid transcription factor-1 (TTF-1), CK7, and Napsin-A. An EML4-ALK fusion was identified by amplification refractory mutation system-polymerase chain reaction (ARMS-PCR) using an AmoyDx EML4‐ALK Fusion Gene Detection Kit. The patient was initially treated with crizotinib (250 mg once daily) and whole-brain radiotherapy (30Gy/10F) to relieve the symptom of dizziness. After an initial partial response (PR) was achieved (Figure 1B, Crizotinib PR), the patient exhibited a progression-free survival (PFS) of 17 months (Figure 1A). In October 2018, the size of the brain lesions increased and a new lung lesion was observed (Figure 1B, Crizotinib PD), thus, indicating progressive disease (PD). Subsequently, cell-free DNA extracted from 4 mL of plasma was subjected to library construction, followed by capture-based targeted NGS using a panel of 139 cancer-related genes spanning 110 KB of the human genome. NGS revealed an EML4-ALK fusion (E6:A20) with a mutation allelic frequency (MAF) of 0.1% in the patient’s plasma ctDNA (Table 1). The patient was then switched from crizotinib to brigatinib at a dose of 90 mg in the first week and 180 mg thereafter. The patient achieved a complete response (CR) for the lung lesion and a PR for the brain lesions (Figure 1B, Brigatinib CR & PR). In September 2019, the disease progressed again with a PFS of 11 months (Figure 1A). NGS of the patient’s plasma using a panel of 139 cancer-related genes revealed a new ALK G1202R (MAF = 0.2%) mutation, in addition to the EML4-ALK fusion (MAF = 0.1%) (Table 1). A third-line treatment with loratinib was administered at a dose of 100 mg and achieved a PFS of 7 months (Figure 1A). Loratinib (100 mg QD) and crizotinib (250 mg QD) were then taken by the patient himself at the same time. However, within 2 months of initiating this therapy, additional symptoms developed, indicating PD (Figure 1A). Follow-up genomic testing with 139 cancer-related genes identified only the EML4-ALK fusion (MAF = 0.1%), while the ALK G1202R mutation was absent from plasma samples (Table 1). The patient was then administered a treatment of alectinib (600 mg twice daily) and chemotherapy consisting of albumin-bound paclitaxel (400 mg d1) and carboplatin (500 mg d1). Endostar, a modified recombinant human endostatin that suppresses angiogenesis, was also administered at a dose of 30 mg. After 2 months of treatment (Figure 1A), the disease progressed and in addition to the EML4-ALK (MAF = 0.1%) and ALK G1202R (MAF = 0.1%) mutations in the plasma, new mutations were again identified by NGS targeting 139 cancer-related genes, including ALK D1203N (MAF = 0.3%), SMARCA4 R1243W (MAF = 0.3%), and TP53 P152L (MAF = 0.3%) (Table 1).
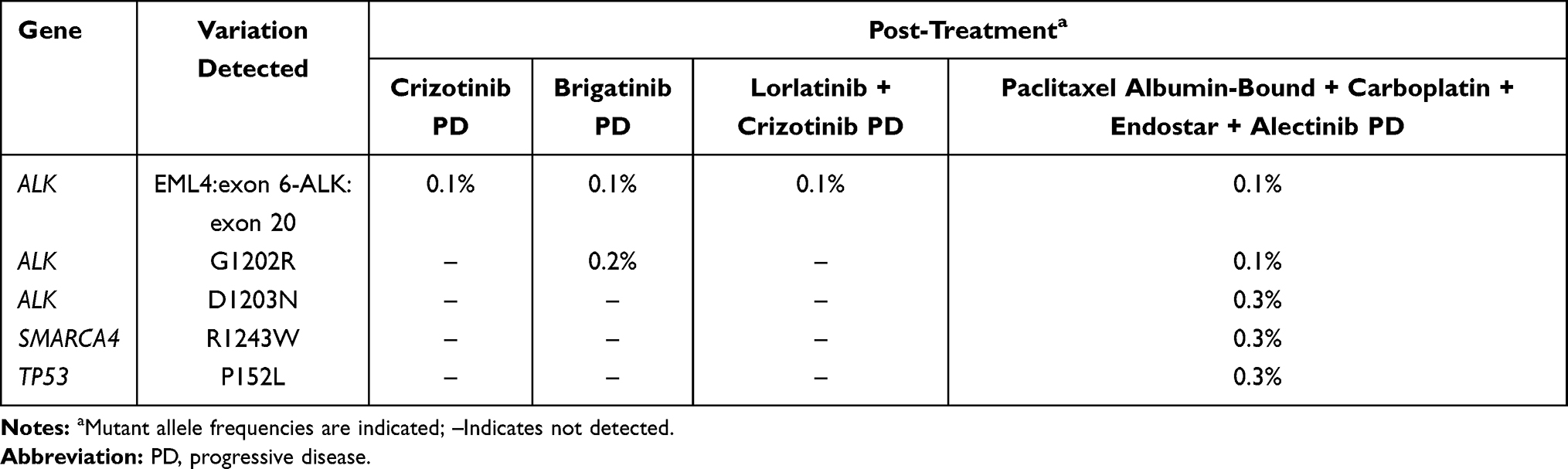 |
Table 1 Genetic Alterations Detected in ctDNA Samples During the Treatment Course |
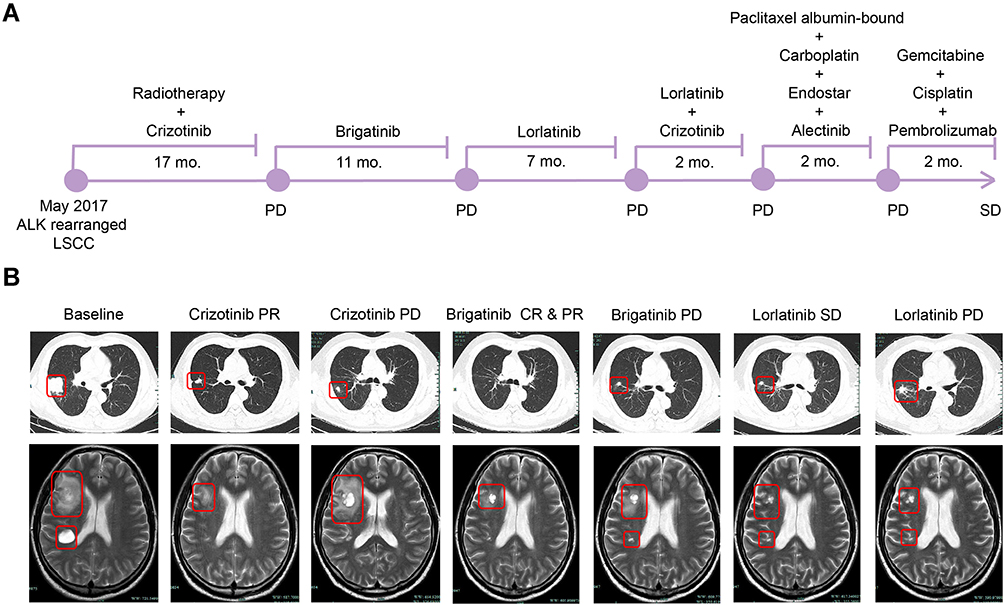 |
Figure 1 Medication strategy and disease conditions of the patient during treatment. (A) An illustrated summary of the treatment received by the patient. (B) Thoracic CT images of primary lung lesions and MRI images of brain metastatic lesions during sequential ALK-TKI treatment. Tumors are indicated by red frames. Abbreviations: LSCC, lung squamous cell carcinoma; mo., months; CR, complete response; PR, partial response; PD, progressive disease; SD, stable disease. |
In July 2020, although PD-L1 expression was negative, the therapy was switched to an immunochemotherapy regimen consisting of gemcitabine (1.8 g d1 and d8), cisplatin (40 mg d1–3), and pembrolizumab (100 mg). Following this treatment, the patient achieved SD with a sustained and ongoing response for 2 months (Figure 1A).
Discussion
ALK rearrangement occurs in ~5% of LADC patients, but in only ~1% of LSCC patients.10 Thus, it remains unknown whether LSCC patients with ALK rearrangements would benefit from ALK TKI therapy. In the present case, the patient was diagnosed with LSCC with an ALK fusion. Sequential administration of ALK TKIs (crizotinib, brigatinib, and lorlatinib) was performed and provided a clinical benefit of 35 months. However, such treatment may also have accelerated the accumulation of ALK-resistance mutations, which was also reported in a previous study.11 Among the ALK-resistance mutations in NSCLC reported by other studies, including G1269R, F1174L, E1210K, L1196M, G1202R, D1203N and F1171T,11–13 we identified the G1202R and D1203N mutations in this case using dynamic NGS monitoring. No resistance mutations were detected following crizotinib failure, which could be due to the MAF being below the detection limit of our assay (0.05% with sequencing depth at 30,000 x). Additionally, the patient’s tumor sample, which might have had other resistance mutations, was insufficient for genetic testing as the tissue biopsy was too small and was subjected to pathological and immunohistochemical analyses instead. Thus, further evaluations could be performed for this patient. Notably, ALK G1202R was previously reported as a potential brigatinib resistance mutation, which was also consistent with our findings.14 It was also reported that lorlatinib could inhibit the ALK G1202R mutant,7 and in the current case, the ALK G1202R mutation was not detected following lorlatinib and crizotinib treatment. However, two ALK-resistance mutations, ALK G1202R and D1203N, were detected following the failure of the combined treatment (chemotherapy, endostar and alectinib).
ALK G1202R was also reported as an alectinib resistance mutation,15 while D1203N has only been reported in a single patient who received ceritinib or brigatinib, but not alectinib.16 However, the ALK D1203N mutation was more common following relapse on lorlatinib, and was almost always observed with other ALK-mutants.17
As chemotherapy with endostar has proved to be effective for advanced NSCLC patients and could be a salvage strategy for patients experiencing failure with targeted therapies,18–20 the patient in this study received a combined treatment of chemotherapy, endostar, and alectinib.
Mutations in the TP53 gene have been reported in 50% of NSCLC patients with the frequency of such alterations being highest in LSCC patients.21 Moreover, non-disruptive TP53 mutations are associated with shorter survival times in patients with advanced NSCLC.22 In this case, the TP53 mutation P152L was detected following the conclusion of the combined treatment of chemotherapy, endostar, and alectinib, and the disease progressed within two months thereafter. Currently, no standard treatment exists for patients with the acquired mutations identified in this study following sequential TKI therapy. It has been reported that pembrolizumab combined with platinum-based chemotherapy could improve OS and PFS for metastatic LSCC, regardless of the level of PD-L1 expression.23 Hence, the patient was administered gemcitabine, cisplatin, and pembrolizumab as a sixth-line treatment and achieved SD.
Conclusions
In summary, our report presented a rare ALK-positive LSCC patient who was treated with sequential TKI therapies and developed different resistance mutations, which were detected by dynamic NGS monitoring. We highlight the importance of dynamic monitoring of ctDNA using NGS to identify genomic tumor evolution and guide treatment decision-making. Thus, this study provides meaningful insight into the potential treatment options for ALK-positive LSCC patients.
Data Sharing Statement
All datasets generated for this study are included in the manuscript.
Ethics Approval and Consent for Publication
This research was approved by the Ethics Committee of The Affiliated People’s Hospital of Ningbo University, and written informed consent for publication of the clinical details and images was obtained from the patient, and did not require institutional approval to publish the case details.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Xue Han and Sisi Liu are employees of Nanjing Geneseeq Technology Inc., China. The authors report no other conflicts of interest to declare.
References
1. Fernandez-Cuesta L, Foll M. Molecular studies of lung neuroendocrine neoplasms uncover new concepts and entities. Transl Lung Cancer Res. 2019;8(Suppl 4):S430–S434. doi:10.21037/tlcr.2019.11.08
2. Devarakonda S, Morgensztern D, Govindan R. Genomic alterations in lung adenocarcinoma. Lancet Oncol. 2015;16(7):e342–e351. doi:10.1016/S1470-2045(15)00077-7
3. Watanabe J, Togo S, Sumiyoshi I, et al. Clinical features of squamous cell lung cancer with anaplastic lymphoma kinase (ALK)-rearrangement: a retrospective analysis and review. Oncotarget. 2018;9(35):24000–24013. doi:10.18632/oncotarget.25257
4. Kim DW, Tiseo M, Ahn MJ, et al. Brigatinib in patients with crizotinib-refractory anaplastic lymphoma kinase-positive non-small-cell lung cancer: a randomized, multicenter phase II trial. J Clin Oncol. 2017;35(22):2490–2498. doi:10.1200/JCO.2016.71.5904
5. Facchinetti F, Bordi P, Bini P, Bidin L, Camisa R, Tiseo M. Enteral administration of TKIs: report of a response to ceritinib in an ALK-positive NSCLC patient and literature review. Curr Drug Targets. 2018;19(14):1649–1656. doi:10.2174/1389450119666180213102939
6. Fan J, Xia Z, Zhang X, et al. The efficacy and safety of alectinib in the treatment of ALK+ NSCLC: a systematic review and meta-analysis. Onco Targets Ther. 2018;11:1105–1115. doi:10.2147/OTT.S156170
7. Zou Helen Y, Friboulet L, Kodack David P, et al. PF-06463922, an ALK/ROS1 inhibitor, overcomes resistance to first and second generation ALK inhibitors in preclinical models. Cancer Cell. 2015;28(1):70–81. doi:10.1016/j.ccell.2015.05.010
8. Karachaliou N, Santarpia M, Gonzalez Cao M, et al. Anaplastic lymphoma kinase inhibitors in Phase I and phase II clinical trials for non-small cell lung cancer. Expert Opin Investig Drugs. 2017;26(6):713–722. doi:10.1080/13543784.2017.1324572
9. Wang H, Sun L, Sang Y, et al. A study of ALK-positive pulmonary squamous-cell carcinoma: from diagnostic methodologies to clinical efficacy. Lung Cancer. 2019;130:135–142. doi:10.1016/j.lungcan.2019.02.015
10. Yang X, Peng P, Zhang L. Multiline treatment of advanced squamous cell carcinoma of the lung: a case report and review of the literature. World J Clin Cases. 2019;7(14):1899–1907. doi:10.12998/wjcc.v7.i14.1899
11. Ding M, Deng L, Yu R, et al. Case report: temporal heterogeneity of ALK activating mutations in sequential ALK TKI-treated non-small-cell lung cancer revealed using NGS-based liquid biopsy. Clin Lung Cancer. 2019;20(3):e229–e232. doi:10.1016/j.cllc.2019.02.014
12. Nagasundaram N, Wilson Alphonse CR, Samuel Gnana PV, Rajaretinam RK. Molecular dynamics validation of crizotinib resistance to ALK mutations (L1196M and G1269A) and identification of specific inhibitors. J Cell Biochem. 2017;118(10):3462–3471. doi:10.1002/jcb.26004
13. Katayama R, Friboulet L, Koike S, et al. Two novel ALK mutations mediate acquired resistance to the next-generation ALK inhibitor alectinib. Clin Cancer Res. 2014;20(22):5686–5696. doi:10.1158/1078-0432.CCR-14-1511
14. Sabari JK, Santini FC, Schram AM, et al. The activity, safety, and evolving role of brigatinib in patients with ALK-rearranged non-small cell lung cancers. Onco Targets Ther. 2017;10:1983–1992. doi:10.2147/OTT.S109295
15. Ou SH, Azada M, Hsiang DJ, et al. Next-generation sequencing reveals a novel NSCLC ALK F1174V mutation and confirms ALK G1202R mutation confers high-level resistance to alectinib (CH5424802/RO5424802) in ALK-rearranged NSCLC patients who progressed on crizotinib. J Thorac Oncol. 2014;9(4):549–553. doi:10.1097/JTO.0000000000000094
16. Urbanska EM, Sørensen JB, Melchior LC, Costa JC, Santoni-Rugiu E. Changing ALK-TKI-resistance mechanisms in rebiopsies of ALK-rearranged NSCLC: ALK- and BRAF-mutations followed by epithelial-mesenchymal transition. Int J Mol Sci. 2020;21(8):2847. doi:10.3390/ijms21082847
17. Dagogo-Jack I, Rooney M, Lin JJ, et al. Treatment with next-generation ALK inhibitors fuels plasma ALK mutation diversity. Clin Cancer Res. 2019;25(22):6662–6670. doi:10.1158/1078-0432.CCR-19-1436
18. Qiu D, Zhang Y, Xue YB, et al. Chemotherapy combined with Endostar as salvage treatment for EGFR-tyrosine kinase inhibitor primary resistance in an advanced non-small cell lung cancer patient with EGFR L858R mutation and ROS1 fusion: a case report. Thorac Cancer. 2019;10(4):1023–1028. doi:10.1111/1759-7714.13003
19. Wang J, Sun Y, Qin S. Results of Phase IV clinical trial of combining endostar with chemotherapy for treatment of advanced non-small cell lung cancer (NSCLC).. J Clin Oncol. 2010;28(15_suppl):7598. doi:10.1200/jco.2010.28.15_suppl.7598
20. Han B, Xiu Q, Wang H, et al. A multicenter, randomized, double-blind, placebo-controlled study to evaluate the efficacy of paclitaxel-carboplatin alone or with endostar for advanced non-small cell lung cancer. J Thorac Oncol. 2011;6(6):1104–1109. doi:10.1097/JTO.0b013e3182166b6b
21. Mogi A, Kuwano H. TP53 mutations in nonsmall cell lung cancer. J Biomed Biotechnol. 2011;2011:583929. doi:10.1155/2011/583929
22. Molina-Vila MA, Bertran-Alamillo J, Gascó A, et al. Nondisruptive p53 mutations are associated with shorter survival in patients with advanced non-small cell lung cancer. Clin Cancer Res. 2014;20(17):4647–4659. doi:10.1158/1078-0432.CCR-13-2391
23. Paz-Ares L, Luft A, Vicente D, et al. Pembrolizumab plus chemotherapy for squamous non–small-cell lung cancer. N Engl J Med. 2018;379(21):2040–2051. doi:10.1056/NEJMoa1810865
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.