")
Back to Journals » Clinical Ophthalmology » Volume 17
Accuracy of the Lacrimal Syringing Test in Relation to Dacryocystography and Dacryoendoscopy
Authors Nakamura J , Kamao T , Mitani A, Mizuki N, Shiraishi A
Received 26 February 2023
Accepted for publication 28 April 2023
Published 3 May 2023 Volume 2023:17 Pages 1277—1285
DOI https://doi.org/10.2147/OPTH.S409662
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jutaro Nakamura,1,2 Tomoyuki Kamao,1 Arisa Mitani,1 Nobuhisa Mizuki,2 Atsushi Shiraishi1
1Department of Ophthalmology, Ehime University Graduate School of Medicine, Toon, Ehime, 791-0295, Japan; 2Department of Ophthalmology and Visual Science, Yokohama City University Graduate School of Medicine, Yokohama, Kanagawa, 236-0004, Japan
Correspondence: Jutaro Nakamura, Department of Ophthalmology, Ehime University Graduate School of Medicine, Toon, Ehime, 791-0295, Japan, Tel +8189-960-5361, Fax +8189-960-5364, Email [email protected]
Purpose: This study aimed to evaluate the accuracy of the lacrimal syringing test (syringing) in relation to dacryocystography (DCG) and dacryoendoscopy (DE) in lacrimal pathway (LP) obstruction.
Methods: We retrospectively reviewed 101 patients (188 LPs) who underwent syringing, cone-beam computed tomography (CBCT)-DCG, and DE to diagnose the degree and site of LP obstruction. The degree of obstruction was classified into patent, partial obstruction, and complete obstruction. The degree of LP obstruction was determined by combining the findings of DE and CBCT-DCG and was designated as DCG+DE. When differentiating complete or partial obstruction on DE was uncertain, complete or partial obstruction was assigned if the DCG showed evidence of contrast media obstruction or passage, respectively. The consistency between syringing and DCG+DE was evaluated by calculating the weighted kappa coefficient.
Results: The sensitivity and specificity of syringing were 94% and 89%, respectively. The weighted Cohen’s kappa value of agreement between syringing and DCG+DE was κ = 0.73 (SE = 0.04, 95% confidence interval [CI]: 0.66– 0.80, p < 0.01). When divided into presaccal and postsaccal obstruction categories, the kappa values were κ = 0.40 (SE = 0.11, 95% CI: 0.19– 0.62, p < 0.01) and 0.55 (SE = 0.09, 95% CI: 0.37– 0.73, p < 0.01), respectively. Furthermore, when limited to common canaliculus obstruction (stenoses), which accounted for 78% (46 LPs) of the total presaccal obstructions, the kappa value was κ = 0.29 (SE = 0.12, 95% CI: 0.05– 0.54, p = 0.021), which demonstrated the lowest consistency between syringing and DCG+DE.
Conclusion: Syringing was “substantially” in agreement with DCG+DE in detecting the degree of LP obstruction. Moreover, syringing was a sufficiently sensitive and specific test when performed by an experienced clinician. However, distinguishing between complete and partial obstructions by syringing was sometimes difficult, particularly in the common canaliculus obstruction (stenosis).
Keywords: epiphora, nasolacrimal duct, lacrimal passage obstruction, stenosis, lacrimal drainage system, lacrimal sac, lacrimal syringing, irrigation, dacryocystography, dacryoendoscopy, weighted kappa coefficient
Introduction
The lacrimal syringing test (syringing) is the most frequently performed test to investigate epiphora in clinical practice.1–3 Syringing is a practical test, providing valuable information on the presence, localization, and nature of the lacrimal pathway (LP) obstruction. Syringing helps in evaluating whether the canaliculus, lacrimal sac, and nasolacrimal duct (NLD) are qualitatively patent, partially obstructed, or completely obstructed. Meanwhile, functional epiphora is a dysfunctional drainage system without an identifiable anatomical obstruction, and syringing has limited reliability in differentiating partial NLD obstruction from functional epiphora.4,5 Dacryocystography (DCG) is a classic and valuable test to visualize LP obstruction.6,7 The basic idea of DCG is to find the site with initial occlusion of the contrast media and diagnose it as the obstructed level. A normal LP has multiple indentations or narrowings and irregularities; therefore, differentiating these normal findings from true pathological stenosis is often complicated. Furthermore, DCG is not helpful in finding the cause of functional epiphora cases because the findings are normal.4,8,9 Dacryoendoscopy (DE) is the investigation method of directly visualizing the lumen of the LP.10 The use of dacryoendoscope, not only for diagnostic inspections, but also for treatments of LP obstructions, has remarkably increased over the past two decades, especially in East Asia, including Japan, Korea, and the Philippines.11–14 East Asians have relatively flat facial features, with a less elevated superior orbital rim than other ethnic groups, which could allow relatively easy usage of a dacryoendoscope.15,16 Moreover, the development of bent-tip and curved probes facilitate observation until the end of the LP in cases that could not be observed by conventional straight-type probes (Supplementary Figure 1).17,18 With advances in fiberoptic systems, dacryoendoscopes offer image quality of 10,000–15,000 pixels; therefore, mucosal inflammation, granulation, foreign bodies, and dacryoliths can be visualized.
 |
Figure 1 Complementary findings of DE and DCG. (A) DE showed a micro-hole in the center of the obstructed site in NLD. Complete or partial obstruction was not clearly visible in the endoscopic images. (B) Sagittal DCG image showed contrast passage, and the site was confirmed as a partial obstruction (arrowhead). The original DCG images were converted to monochrome to facilitate the observation of the contrast media. Abbreviations: DCG, dacryocystography; DE, dacryoendoscopy; NLD, nasolacrimal duct. |
Syringing is the most commonly used procedure to examine epiphora and is one of the most fundamental and essential examinations in dacryology. This study aimed to evaluate the accuracy of syringing in relation to DCG and DE. The degree and site of LP obstruction were comprehensively identified by combining the findings of DE and DCG, designated as DCG+DE, and the accuracy of syringing was then evaluated.
Methods
Patient Selection
This study retrospectively investigated 101 patients (188 LPs) who underwent syringing, DCG, and DE as preoperative evaluation of LP obstruction at Ehime University Hospital between January 2021 and March 2022. Syringing was conducted during the first clinical visit, and DCG and DE were subsequently performed on a different day in that order. These examinations were conducted or supervised by three trained ophthalmologists, namely, TK, AM, and AS, with 11, 5, and 15 years of experience in dacryoendoscopic surgeries, respectively. Each clinician was responsible for the series of tests mentioned above on each patient. Notably, TK and AM performed 106 and 82 LP examinations, respectively. Patients with a history of systemic chemotherapy with 5-fluorouracil, docetaxel, or idoxuridine and those with a history of radiation therapy given to the cranial region, posttraumatic bone deformity, or eyelid malposition were excluded from this study. Eligible patients were evaluated not only on the symptomatic side but also on the asymptomatic side with the above three tests. The operated side was excluded from the statistical analysis if there was a history of lacrimal recanalization surgery on one side of the LP. The side without a history of surgery was included in the analysis. Moreover, if the diagnostic DE was challenging to perform on the other side because of a pain, only one side was evaluated. The degree and site of LP obstruction were examined, and the degree of obstruction was classified into patent, partial obstruction, and complete obstruction. The duration of obstruction was defined as the period of chronic epiphora described in the patient’s questionnaire. The duration of obstruction was expressed in months and set to zero if asymptomatic.
Syringing
All the patients received topical ocular surface anesthesia before the examination. If the punctum was small, a Nettleship punctum dilator was used. A blunt-tipped 23-G lacrimal cannula on a 2.5-mL syringe with saline solution was inserted through the upper and lower punctum, and syringing was performed under minimal pressure. The absence of any reflux was considered patent (true negative). If the saline refluxed totally and did not irrigate into the nose, complete obstruction was considered; meanwhile, partial obstruction was characterized by partial irrigation into the nose with some extent of reflux. When serous reflux material was observed, canalicular, common canalicular, or upper lacrimal sac obstruction was considered. When viscous reflux material was observed, obstruction at the distal sites, such as the lacrimal sac or NLD was considered. The communication between the upper and lower canaliculi was also determined. The reflux from the punctum opposite to the injecting side was considered an obstruction in the common canaliculus or more distal structures. Direct reflux of saline from the injecting punctum with failure to advance the cannula into the lacrimal fossa was diagnosed as complete obstruction of the canaliculus. Subsequently, a Bowman’s probe was inserted from the punctum to measure the length of occlusion to the soft stop.19,20
DCG
Patients who presented acute dacryocystitis and allergy to contrast media or iodine were excluded from the examination. After topical anesthesia with 4% lidocaine instillation, the LP was washed with saline. The contrast media was a non-ionic, water-soluble agent (1–2 mL; Omnipaque 300 [iohexol]; GE Healthcare, Tokyo, Japan). It was manually injected slowly through the upper and lower puncta until the patient reported that the solution reached the nose or until the contrast agent backflow from the punctum. DCG was performed bilaterally to examine both sides of the LP. In capturing the images, cone-beam computed tomography (CBCT) was initiated shortly after contrast medium injection. Three-dimensional CBCT-DCG images were acquired using Accuitomo F17 (Morita, Kyoto, Japan). Imaging conditions were a scan time of 17.5 s and X-ray output of 90 kV and 8.0 mA. Image manipulation was performed using dedicated computer software (i-Dixel 2.0; Morita, Kyoto, Japan). Partial obstruction was considered if both of the following criteria were met: (1) Apparent thinner contrast in the LP continuity, and (2) LP dilatation proximal to the thin contrasted area. DCG images were evaluated by an ophthalmologist and a radiologist; the latter was totally blinded to all other patient information.
DE
Patients with acute dacryocystitis were excluded. Patients were placed in a supine position on the procedural bed, and topical ocular surface and mucosal surface anesthesia of the LP were administered with 4% lidocaine. If necessary, subcutaneous infiltration anesthesia around the punctum and inner canthus was added with 2% lidocaine and epinephrine. The punctum was dilated with a dilator, and a bent-type rigid dacryoendoscope (MT-3 or CK-10, Fibertech, Tokyo) was inserted through the upper and lower puncta. During the examination, the tip of the probe passed through the canaliculus and common canaliculus, reaching the lacrimal sac from the internal common punctum. Then, the probe was rotated 90° inferiorly to view the lacrimal sac and NLD, until the NLD opening on the inferior meatus. DE was bilaterally performed to examine both sides of the LP. When partial or complete LP obstruction was detected, the site, degree, and characteristics of the obstructed area were recorded. Complete obstruction was defined as complete obstruction on the endoscopic view. Patent was defined as the absence of pathological changes in the LP lumen, such as inflammatory or fibrotic stenosis, granulation, foreign bodies, or dacryoliths. Other cases were classified as partial obstruction.
DCG+DE
The site and degree of obstruction were classified according to the DE findings as the “gold standard”. Meanwhile, in the following cases, DCG and DE were complementarily integrated to determine the obstruction status. (1) In cases where DE diagnosed complete obstruction, but DCG showed the passage of contrast media, partial obstruction was considered based on DCG (Figure 1). (2) In cases such as common canalicular stenosis (CCS) + complete NLD obstruction, CCS prevents the DE probe from passing through; hence, DE cannot be used to visualize sites beyond the stenotic site. However, DCG could reveal complete obstruction of the NLD, and the DCG findings were used. (3) When stenosis was present at multiple sites along the LP, it prevented diagnostic DE from being visualized beyond the stenotic site. Conversely, DCG could identify the site of complete obstruction regardless of stenosis; hence, it was used.
Sensitivity and Specificity Analysis
The sensitivity of syringing test corresponded to the rate of LPs with partial or complete obstruction on DCG+DE and positive in the syringing test (true positives). The specificity of syringing corresponded to the rate of patent LPs on DCG+DE that were negative (patent) on syringing (true negatives).
Statistical Analysis
Inter-rater reliability analysis was performed between dependent samples of syringing and DCG+DE. Accordingly, the weighted Cohen’s kappa, a measure of the agreement between two dependent categorical samples, was calculated. To interpret the calculated kappa values, Landis and Koch’s classification table was used as a guide (Supplementary Table 1).21 All statistical analyses were performed using the online statistics calculator DATAtab (Graz, Austria; URL https://datatab.net).
Results
The study included 22 male patients (43 LPs) and 79 female patients (145 LPs). The mean age of the patients was 71.4 (standard deviation [SD] = 13.8) years. The present study included 124 and 64 cases of symptomatic and asymptomatic LPs, respectively, and the mean duration of LP obstruction was 20.4 (SD = 56.0) months. Among 64 cases of asymptomatic LPs, 33, 23, and 7 were identified as patent, partial, and complete obstructions in DCG+DE, respectively.
Table 1 presents the results of consistency between syringing and DCG+DE in all cases (top), presaccal obstruction (middle), and postsaccal obstruction (bottom). DCG+DE demonstrated 38 patents, 71 partial obstructions, and 79 complete obstructions in a total of 188 LPs (Table 1, top). The consistency of patent, partial obstruction, and complete obstruction between syringing and DCG+DE was observed in 34, 33, and 78 LPs, respectively. The matching rate of syringing and DCG+DE was 77%. The sensitivity and specificity of syringing were 94% and 89%, respectively. The weighted Cohen’s kappa value of agreement between syringing and DCG+DE was κ = 0.73 (standard error [SE] = 0.04, 95% CI: 0.66–0.80, p < 0.01), indicating a “substantial” agreement according to Landis and Koch’s classification (Supplementary Table 1). Of the 86 LPs with complete obstruction on DE, seven showed contrast passage on DCG, leading to a diagnosis of partial obstruction in DCG+DE. Meanwhile, 29 of 107 LPs (27%) diagnosed with complete obstruction by syringing revealed partial obstruction by DCG+DE. The breakdown of this discrepancy included 16 LPs with CCS, 7 LPs with postsaccal stenosis, and 3 LPs with postsaccal dacryolithiasis.
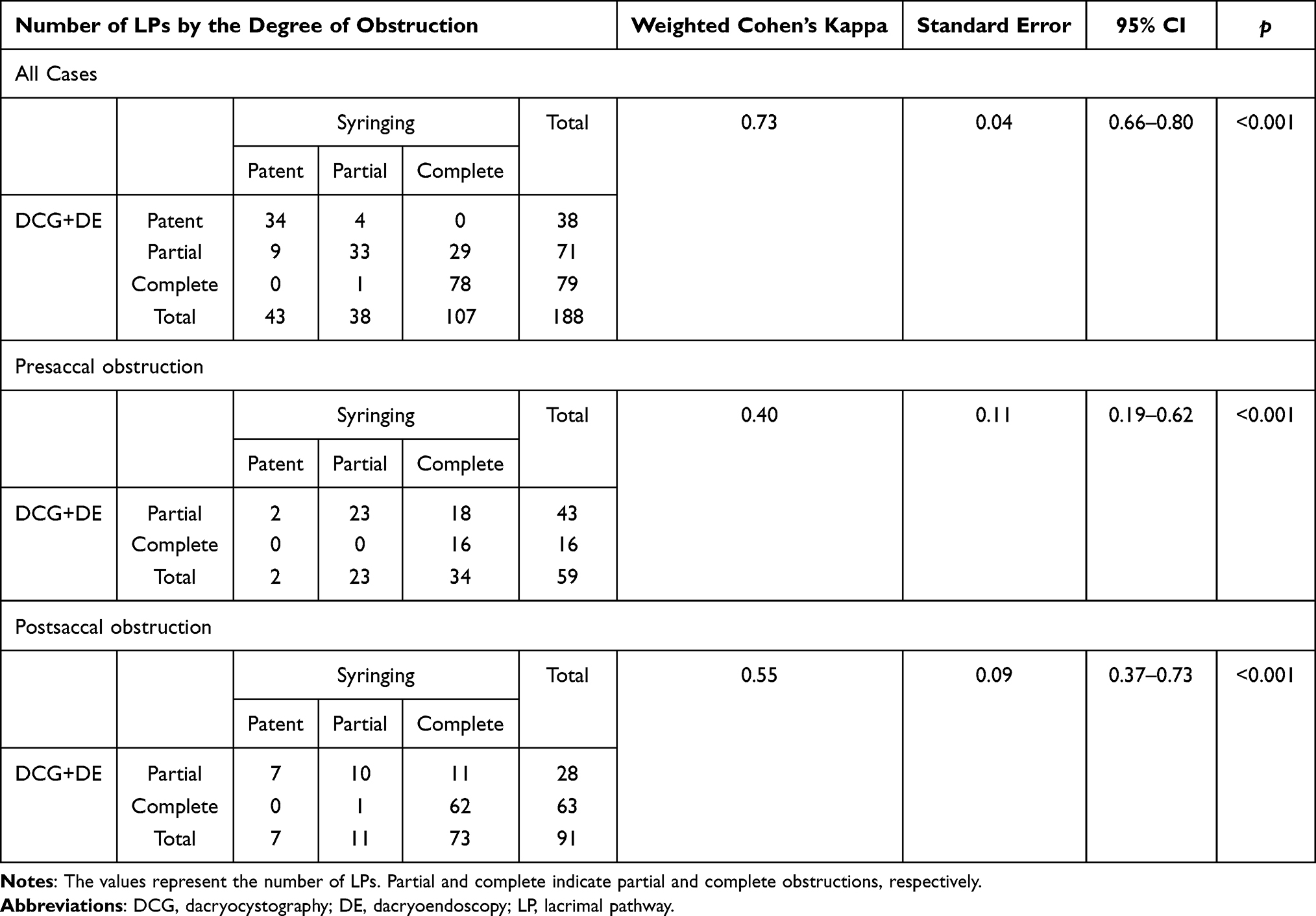 |
Table 1 Consistency Analysis Between Syringing and DCG+DE in All Cases (Top), Presaccal Obstruction (Middle), and Postsaccal Obstruction (Bottom) |
Similarly, the middle and bottom of Table 1 show the subgroup analysis results, which were divided into presaccal and postsaccal obstruction. Regarding presaccal obstruction, DCG+DE demonstrated 43 partial obstructions and 16 complete obstructions in a total of 59 LPs. The consistency of partial and complete obstructions between syringing and DCG+DE was observed in 23 and 16 LPs, respectively. The matching rate of syringing and DCG+DE was 66%. The kappa value was κ = 0.40 (SE = 0.11, 95% CI: 0.19–0.62, p < 0.01), indicating a “fair” agreement. Likewise, regarding the postsaccal obstruction, DCG+DE demonstrated 28 partial obstructions and 63 complete obstructions in a total of 91 LPs. The consistency of partial and complete obstructions between syringing and DCG+DE was observed in 10 and 62 LPs, respectively. The matching rate was 79%, and the kappa value was κ = 0.55 (SE = 0.09, 95% CI: 0.37–0.73, p < 0.01), indicating a “moderate” agreement.
Furthermore, we examined the reason behind the consistency reduction in the presaccal obstruction category. Our results showed that partial or complete obstruction of the common canaliculus, synonymous with CCS and common canaliculus obstruction (CCO), respectively, accounted for 78% (46 LPs) of the total presaccal obstructions. Therefore, we aimed to evaluate the consistency in the common canaliculus (Table 2). DCG+DE demonstrated 37 partial obstructions (CCS) and 9 complete obstructions (CCO) in a total of 46 common canaliculi. The results also showed that the matching rate was 59%, and only about half of the partial obstructions could be identified by syringing (18 out of 37). The kappa value was κ = 0.29 (SE = 0.12, 95% CI: 0.05–0.54, p = 0.021).
 |
Table 2 Consistency Analysis Between Syringing and DCG+DE in the Common Canaliculus |
Discussion
Syringing is the most frequently performed test in clinical practice and the most fundamental and essential examination in diagnosing lacrimal drainage system obstruction.1–3 Various studies have attempted to evaluate the accuracy of syringing in contrast to other examination methods.1,3,4,22,23 The present study compared syringing results to the combined (and complementary) findings of DCG and DE (DCG+DE). To the best of our knowledge, this is the first study to address the accuracy of syringing in relation to a combination of DCG and DE. Our results showed that syringing had a sensitivity and specificity of 94% and 89.5%, respectively, with reference to DCG+DE. The kappa value was κ = 0.73 (95% CI: 0.66–0.80), indicating “substantial” agreement with DCG+DE. When all the cases were divided into presaccal and postsaccal sub-categories, the kappa values were κ = 0.4 (95% CI: 0.19–0.62) and 0.55 (95% CI: 0.37–0.73), respectively. To investigate the reason behind relatively low consistencies of presaccal obstructions, we focused on the common canaliculus, which accounted for the most significant proportion of presaccal cases (78%). Accordingly, we found a kappa value of κ = 0.29 (95% CI: 0.05–0.54). The low consistency was due to the low accuracy of syringing in diagnosing CCS/CCO. Thus, it was potentially difficult to distinguish partial or complete obstruction in the common canaliculus by syringing.
Regarding DCG, Nixon et al reported that the sensitivity and specificity of syringing were 86% and 53%, respectively.23 Further, recently, Shapira et al used the combination of DCG and dacryoscintigraphy to examine postsaccal obstruction, and they reported that the sensitivity and specificity of syringing were 91% and 65%, respectively.4 According to Bae et al, the sensitivity and positive predictive value of syringing were 86.7% and 92.9%, respectively; nonetheless, the weighted kappa coefficient of syringing and DE was κ = 0.55 (95% CI: 0.37–0.73). Moreover, this group reported the consistency of DE and digital subtraction DCG, with a kappa value of κ = 0.60 (95% CI: 0.40–0.81).22 Meanwhile, the consistency between CBCT-DCG and DE in our study was κ = 0.58 (95% CI: 0.49–0.66) (Supplementary Table 2). The relatively lower consistency in our study between DCG and DE was presumably due to the lower sensitivity of CBCT-DCG in detecting partial obstructions compared with real-time digital subtraction DCG.
Generally, DCG is less sensitive in detecting stenotic lesions; moreover, the normal LP comprises multiple indentations or apparent narrowings and irregularities. Therefore, differentiating these normal findings from true pathological stenosis is often complicated (Figure 2).9,22,24 Specifically, CCS is considered challenging to delineate by DCG.23 In the present study, partial obstruction on DCG was barely delineated in the canaliculi or common canaliculus according to our criteria. On the contrary, direct visualization of the LP lumen by DE allows differentiation between physiological narrowing and true pathological stenosis. Although some patients were diagnosed with complete obstruction by DE, on DCG scan, the contrast media reached the nasal cavity, confirming that the lesion was a partial obstruction (Figure 1). The present study found that among the 86 cases of LPs with complete obstruction on DE, 7 showed passage of contrast media on DCG scan, leading to the diagnosis of partial obstruction on DCG+DE. This discrepancy indicates that even though DE reveals visually complete obstruction, the contrast media occasionally passes through the site and can be visualized as anatomically unobstructed, suggesting that the diagnosis of partial or complete obstruction is contradictory between DCG and DE and that the combined diagnosis of DCG and DE is complementary.
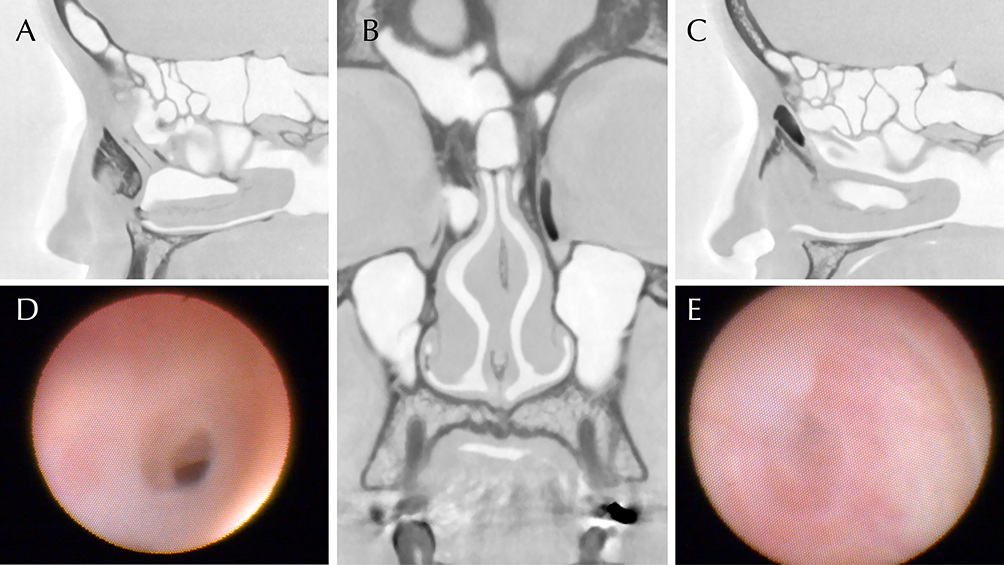 |
Figure 2 Consistency and discrepancy of findings between syringing and DCG+DE. DCG and diagnostic DE images of a 42-year-old female patient with a chief complaint of epiphora and discharge on her left eye lasting for 1 year. Syringing showed complete obstruction on the left and patency on the right. (A) Sagittal DCG image of the right LD. The contrast agent passed through the NLD and reached the nose. (B) Coronal DCG image showed complete obstruction at the middle of the left LD. The right LP allowed the passage of the contrast media. (C) Sagittal DCG image of the left LD. The left lacrimal sac was dilated, and the contrast media pooled at the middle of the NLD. (D) DE view of the partially obstructed site (right LP) of the same patient. NLD stenosis was observed due to inflammatory fibrous tissues. DCG+DE detected NLD partial obstruction, whereas syringing diagnosed this as a patent LP; hence, DCG+DE diverged from syringing on the right side. (E) DE view of the obstructed site (left LP). Membranous inflammatory complete obstruction was observed in the middle part of the NLD. Thus, DCG+DE was consistent with syringing on the left side. The original DCG images were converted to monochrome to facilitate the observation of the contrast media. Abbreviations: DCG, dacryocystography; DE, dacryoendoscopy; LP, lacrimal pathway; NLD, nasolacrimal duct. |
Shapira et al reported that the efficiency of epiphora improvement after endoscopic dacryocystorhinostomy (DCR) in NLD stenosis was less favorable than that in complete NLD obstruction.25 Meanwhile, Ilgit et al reported that the functional success and anatomical patency rate of partial obstruction after transluminal balloon dilation were higher than those of complete obstruction.26 Moreover, Javate et al reported that compared with complete obstruction, postsaccal partial obstruction had a better outcome of functional patency after endoluminal lacrimal duct recanalization (ELDR) with silicone intubation.11 Recently, Kamao et al analyzed the patency rate 6 months after ELDR. The patency rates of partial and complete postsaccal obstructions were 100% (8/8) and 83.1% (54/65), respectively. Furthermore, the outcome of ELDR for postsaccal obstruction was dependent on the preoperative obstruction period and degree of obstruction, proposing that ELDR was a favorable indication for a relatively early stage of LP obstruction, namely, stenosis or partial obstruction, before mucosal inflammation and subsequent fibrotic organic obstruction progressed, leading into sclerotic lesions.12,27
Moreover, this study evaluated both symptomatic and asymptomatic sides simultaneously. According to the responses of the patients to questionnaire, out of the 188 LPs investigated, 64 sides were asymptomatic. Further, among these 64 asymptomatic LPs, 33, 23, and 7 were identified as patent, partial, and complete obstructions by DCG+DE, respectively. These findings may help the clinician to counsel patients regarding an asymptomatic side that can develop epiphora in the future.
This study has several limitations. First, this was a single-center retrospective cohort study. Second, the interpretation of syringing and DCG has some degree of subjectivity. In particular, syringing is susceptible to the influence of the clinician’s experience and skill. Therefore, to minimize inter-tester bias in this study, syringing was performed only by three well-trained ophthalmologists with at least 5 years of experience in dacryoendoscopic surgery. Moreover, DCG readings were proceeded separately by an ophthalmologist and a radiologist, who was totally blinded to all other patient information.
In conclusion, syringing was a sufficiently sensitive and specific test when performed by an experienced clinician. However, distinguishing between complete and partial obstruction by syringing was sometimes difficult, particularly in the common canaliculus. Accumulating evidence has shown that compared with complete obstruction, those with partial NLD obstruction have better results after ELDR; hence, a comprehensive evaluation with DCG and DE could become an indicator to determine whether ELDR or DCR is suitable.
Abbreviations
CBCT, cone-beam computed tomography; CCS, common canalicular stenosis; CCO, common canalicular obstruction; DCG, dacryocystography; DCR, dacryocystorhinostomy; DE, dacryoendoscopy; ELDR, endoluminal lacrimal duct recanalization; LP, lacrimal pathway; NLD, nasolacrimal duct; SD, standard deviation; SE, standard error.
Data Sharing Statement
The datasets analyzed in this study are available from the corresponding author (JN) on reasonable requests.
Ethics Approval and Consent to Participate
The protocol and consent forms for the study were approved by the institutional review board of Ehime University (ethical approval no. 1601003). The study was registered in the University Hospital Medical Information Network Clinical Trials Registry (UMIN 000025180). Each patient provided written informed consent before registration. All procedures used in this study were performed under the tenets of the Declaration of Helsinki.
Acknowledgments
The authors would like to express their sincere gratitude to Dr. Toru Suzuki for his continuous scientific mentoring and instructions.
Funding
The study was supported by the Japan Society for the Promotion of Science Postdoctoral Fellowship for Research Abroad (Kaitoku-NIH, #24112 to JN). The funding source had no role in the study design, data collection, analysis, publication decisions, or manuscript preparation.
Disclosure
The authors declare that they do not have any competing interests and are solely responsible for the content and writing of the paper.
References
1. Conway ST. Evaluation and management of ‘functional’ nasolacrimal blockage: results of a survey of the American society of ophthalmic plastic and reconstructive surgery. Ophthal Plast Reconstr Surg. 1994;10(3):
2. Cuthbertson FM, Webber S. Assessment of functional nasolacrimal duct obstruction—a survey of ophthalmologists in the southwest. Eye. 2004;18(1):20–23. doi:10.1038/sj.eye.6700522
3. Saleh GM, Gauba V, Tsangaris P, et al. Digital subtraction dacryocystography and syringing in the management of epiphora. Orbit. 2007;26(4):249–253. doi:10.1080/01676830600987375
4. Shapira Y, Juniat V, Macri C, et al. Syringing has limited reliability in differentiating nasolacrimal duct stenosis from functional delay. Graefes Arch Clin Exp Ophthalmol. 2022;260(9):3037–3042. doi:10.1007/s00417-022-05654-1
5. Sahlin S, Chen E. Evaluation of the lacrimal drainage function by the drop test. Am J Ophthalmol. 1996;122(5):701–708. doi:10.1016/S0002-9394(14)70490-8
6. Montecalvo RM, Zegel HG, Barnett FJ, et al. Evaluation of the lacrimal apparatus with digital subtraction macrodacryocystography. RadioGraphics. 1990;10(3):483–490. doi:10.1148/radiographics.10.3.2188309
7. Singh S, Ali MJ, Paulsen F. Dacryocystography: from theory to current practice. Ann Anat. 2019;224:33–40. doi:10.1016/j.aanat.2019.03.009
8. Shapira Y, Macri C, Usmani E, et al. Outcomes of intubation and endoscopic DCR in functional nasolacrimal duct obstruction. Rhinology. 2022;60(4):308–312. doi:10.4193/Rhin22.047
9. Guzek JP, Ching AS, Hoang T-A, et al. Clinical and radiologic lacrimal testing in patients with epiphora. Ophthalmology. 1997;104(11):1875–1881. doi:10.1016/S0161-6420(97)30013-X
10. Hoshi S, Tasaki K, Maruo K, et al. Improvement in dacryoendoscopic visibility after image processing using comb-removal and image-sharpening algorithms. J Clin Med. 2022;11(8):2073.
11. Javate RM, Pamintuan FG, Cruz RT Jr. Efficacy of endoscopic lacrimal duct recanalization using microendoscope. Ophthal Plast Reconstr Surg. 2010;26(5):330–333. doi:10.1097/IOP.0b013e3181c7577a
12. Kamao T, Zheng X, Shiraishi A. Outcomes of bicanalicular nasal stent inserted by sheath-guided dacryoendoscope in patients with lacrimal passage obstruction: a retrospective observational study. BMC Ophthalmol. 2021;21(1):103. doi:10.1186/s12886-020-01678-5
13. Kim SE, Beak JU, Paik J-S, et al. Long-term efficacy of dacryoendoscopy-guided recanalization and silicone tube intubation. Korean J Ophthalmol. 2022;36(3):185–193. doi:10.3341/kjo.2021.0117
14. Lee SM, Lew H. Transcanalicular endoscopic dacryoplasty in patients with primary acquired nasolacrimal duct obstruction. Graefes Arch Clin Exp Ophthalmol. 2021;259(1):173–180. doi:10.1007/s00417-020-04833-2
15. Whitnall SE. Anatomy of the Human Orbit and Accessory Organs of Vision. Huntington, NY: Krieger Publishing; 1979.
16. Nakamura J, Kamao T, Mitani A, et al. Analysis of lacrimal duct morphology from cone-beam computed tomography dacryocystography in a Japanese population. Clin Ophthalmol. 2022;16:2057–2067. doi:10.2147/OPTH.S370800
17. Emmerich KH, Meyer-Rüsenberg HW, Simko P. Endoscopy of the lacrimal drainage system. Ophthalmologe. 1997;94(10):732–735. doi:10.1007/s003470050195
18. Suzuki T. Transcanalicular lacrimal surgery with a miniature caliber endoscope. Jpn J Ophthalmic Surg. 2003;16(4):485–491.
19. Kominek P, Della Rocca R, Rosenbaum S. Diagnostics. In: Atlas of Lacrimal Surgery. Springer; 2007:29–51.
20. Patrinely JR, Anderson RL. A review of lacrimal drainage surgery. Ophthal Plast Reconstr Surg. 1986;2(2):97–102. doi:10.1097/00002341-198601050-00008
21. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159–174. doi:10.2307/2529310
22. Bae SH, Park J, Lee JK. Comparison of digital subtraction dacryocystography and dacryoendoscopy in patients with epiphora. Eye. 2021;35(3):877–882. doi:10.1038/s41433-020-0990-1
23. Nixon J, Birchall IWJ, Virjee J. The role of dacryocystography in the management of patients with epiphora. Br J Radiol. 1990;63(749):337–339. doi:10.1259/0007-1285-63-749-337
24. Beigi B, Uddin JM, McMullan TFW, et al. Inaccuracy of diagnosis in a cohort of patients on the waiting list for dacryocystorhinostomy when the diagnosis was made by only syringing the lacrimal system. Eur J Ophthalmol. 2007;17(4):485–489. doi:10.1177/112067210701700401
25. Shapira Y, Macri C, Usmani E, et al. DCR for nasolacrimal duct stenosis may be less effective than for complete obstruction. Eye. 2023;37(4):760–763. doi:10.1038/s41433-022-02048-9
26. Ilgit ET, Yüksel D, Unal M, et al. Transluminal balloon dilatation of the lacrimal drainage system for the treatment of epiphora. Am J Roentgenol. 1995;165(6):1517–1524. doi:10.2214/ajr.165.6.7484599
27. Paulsen FP, Thale AB, Maune S, et al. New insights into the pathophysiology of primary acquired dacryostenosis. Ophthalmology. 2001;108(12):2329–2336. doi:10.1016/S0161-6420(01)00946-0
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.