Back to Journals » Infection and Drug Resistance » Volume 15
Access to Essential Personal Safety, Availability of Personal Protective Equipment and Perception of Healthcare Workers During the COVID-19 in Public Hospital in West Shoa
Authors Chaka EE ![]() , Mekuria M
, Mekuria M ![]() , Melesie G
, Melesie G
Received 1 December 2021
Accepted for publication 13 April 2022
Published 29 April 2022 Volume 2022:15 Pages 2315—2323
DOI https://doi.org/10.2147/IDR.S344763
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Eshetu E Chaka,1 Mulugeta Mekuria,1 Getu Melesie2
1Department of Public Health, College of Medicine and Health Science, Ambo University, Ambo, Ethiopia; 2Department of Pharmacy, College of Medicine and Health Science, Ambo University, Ambo, Ethiopia
Correspondence: Eshetu E Chaka, Email [email protected]
Introduction: The pandemic of coronavirus disease-2019 has fundamentally changed the physician–patient relationship due to health care workers’ being at high risk of getting COVID-19 infection from their patients. Therefore, healthcare workers are a priority to be protected and prevent transmission within a healthcare setting.
Objective: To assess the actual and perceived personal safety of healthcare workers practicing in public hospitals.
Methods and Materials: A descriptive cross-sectional study design was done among 361 health professionals in West Shoa. A simple random sampling technique was used to select representative respondents. Data was collected by a pretested, self-administered questionnaire. The collected data was entered into EPI-Info and exported to STATA for analysis. Descriptive statistics were used to present the data.
Results: A total of 361 healthcare workers responded to the question with a 97% response rate. The median age of the study participants was 29. Of the total participants, access to personal protective equipment was: hand sanitizer 322 (89.2%), disposable gloves 285 (78.9%), face mask 280 (77.6%), KN95 face mask 163 (45.2%) and facial protective shields 112 (31%). One hundred sixty-nine (46.8%) of the study participants reported that their hospital has personal safety policies and procedures. One hundred sixty-one (44%) reported that they perceived no support, while only 35 (9.7%) participants reported that they perceived full support from their hospital. Furthermore, the participants perceived that their local concerned bodies took fewer necessary measurements to defend physical integrity in the workplace (mean 2.86 SD = 3.34).
Conclusion: There are many healthcare workers who have limited access to the majority of essential PPE. The majority of study participants perceived limited support from their health facilities, hospitals and local concerned bodies. Therefore, hospitals and local public health authorities should increase access to PPE to protect healthcare workers.
Keywords: personal protective equipment, access, perception, reality
Introduction
Coronavirus Disease 2019 (COVID-19) is a disease caused by the SARS-CoV-2 virus. Infected people can spread SARS-CoV-2 to other people through respiratory droplets produced when an infected person coughs or sneezes. A person may also get COVID-19 by touching a surface that has SARS-CoV-2 on it, followed by touching their own nose, mouth, and eyes.1,2
Personal protective equipment (PPE) is an essential component to safeguarding against COVID-19 cross-infection. Therefore, PPE is a current hot topic, probably the most talked about and sensitive subject during the current COVID-19 for healthcare workers working with COVID-19 infected patients. The shortage of PPE and inappropriate use of the equipment are the main problems related to PPE in the healthcare setting.3
At the beginning, COVID-19 infected many healthcare workers, posing a big challenge for epidemic control. For instance, as of early March, there were over 2600 infected, with 13 dying in Italy as of March 20, 2020, and the infected number increased to 3300, and at least 22 died in China.4,5 Among the 19 staff members positively diagnosed with COVID, 88.3% developed psychological stress or emotional changes during their isolation period in Wuhan.6
Although worldwide, millions of people stay at home to minimize the transmission of severe COVID-19, healthcare workers go to clinics and hospitals, putting themselves at high risk of COVID-2019.4
As the COVID-19 pandemic accelerates worldwide, access to PPE for healthcare workers is a key concern. Medical staff are prioritized in many countries, but PPE shortages have been described in the most affected facilities. Some medical staff are waiting for equipment while already seeing patients who may be infected with COVID-19 or are supplied with equipment that might not meet requirements. In addition, they are anxious about spreading the infection to their family, which puts their personal safety at risk.4
One of the precautions to be applied by healthcare workers during caring for patients with COVID-19 is the use of appropriate PPE. The WHO recommends implementing safety protocols for healthcare workers. However, basic PPEs are not always available in many health facilities dealing with COVID-19 patients. Many health facilities around the globe do not have access to an appropriate number of human resources and diagnostic and/or therapeutic protocols to care for patients suffering from COVID-19.7
Healthcare workers are dedicated to working in close contact with infected people with inadequate PPE during an outbreak of COVID-19. The majority of reported COVID-19 cases among healthcare workers might be due to poor safety procedures, inadequate access to PPE, diagnostic protocols, and inappropriate use of PPE. Therefore, this study was aimed at evaluating reality and perception about access to personal safety among healthcare workers during the COVID-19 pandemic in a public hospital in West Shoa. As far as researchers’ knowledge is concerned, there are limited studies on the access of personal safety during the COVID-19 pandemic in the study area. Hence, the study findings might help to highlight whether there is a need for essential PPE to care for suspected and/or confirmed cases of COVID-19 in the study area to protect healthcare workers in the workplace.
Materials and Methods
The study was conducted in three hospitals (Ambo Referral Hospital, Ambo General Hospital, and Guder Hospital), which were selected purposefully from eight hospitals in the West Shoa Zone public hospitals from June 5 to August 30, 2020. A descriptive cross-sectional study design was done on 100 randomly selected participants using the lottery method, using the study participant identification card as a sampling frame. All healthcare workers who were working and available during the data collection period were included in the study. The sample size was determined by the single population proportion formula and using the following assumption: The proportion (P) of previous study participants who had access to disposable gowns was 67.3% (Latin); the maximum acceptable error/margin of error (d) was 5%; and the level of significance was 0.05 = 1.96. Then the minimum sample size after adding a 10% non-response rate is 372. Then, proportional allocation was used to select the number of healthcare workers from each hospital.
Data Collection Tool and Techniques
Structured, paper-based, self-administered questionnaires were created to collect data. The questionnaire contained three parts. The first part was used to gather socio-demographic information of the study participants and included age, sex, occupation, and monthly income; the second section was developed to evaluate access to PPE, personal safety policies and procedures, COVID-19 diagnostic and management processes, and institutional support with human resources in case healthcare workers get sick. The third part has two items used to evaluate respondents’ perceptions about their institutions’ taking all the required measurements to protect physical integrity in the workplace (10-point Likert scale; 0 = no support, 10 = full support) and participants’ perceptions regarding their local public health authorities’ taking all the necessary measurements to protect physical integrity in the workplace (10-point Likert scale; 0 = no support, 10 = full support).
The pilot study of the questionnaire was done on 5% of the sample size in Bako hospital, and training was given for data collection facilitators. Daily supervision was done to check the completeness of the questionnaire. Before data analysis, the data were cleaned, edited, and checked.
Data Processing and Analysis
The data were checked, coded, and entered into Epi-Info version 7.2.2.6 and export to the STATA version 14 software for analysis. Descriptive statistics, frequency, and a percentage were used to present the data.
Ethical Consideration
The Institutional Review Ethics Committee of the College of Health Sciences, College of Medicine and Health Science, Ambo University approved this research as oral consent was enough to conduct this research and ethical clearance was obtained. All the information was kept confidential and the study was done as per the ethical guidelines of the Declaration of Helsinki Only oral informed consent was taken from each participant because the research did not contain any risk to the study participants, and since the study participants are health professionals, they are expected to be aware that the research did not harm them but rather benefit them by increasing the accessibility of PPE. Oral consent was taken from all study participants after explaining the objectives of the study to them. All information obtained from the respondents was kept confidential using code. The data was not provided to a third party. The study respondents were informed that they have the full right to refuse to take part in this research and that they also have the full right to withdraw at any time they wish.
Results
A total of 361 health professionals responded to the question, with a 97% response rate. The median age of the study participants is 29, with an inter-quartile range of 6. Of the total respondents, male health workers account for 218 (60.4%) and 207 (57.3%) of them (Table 1).
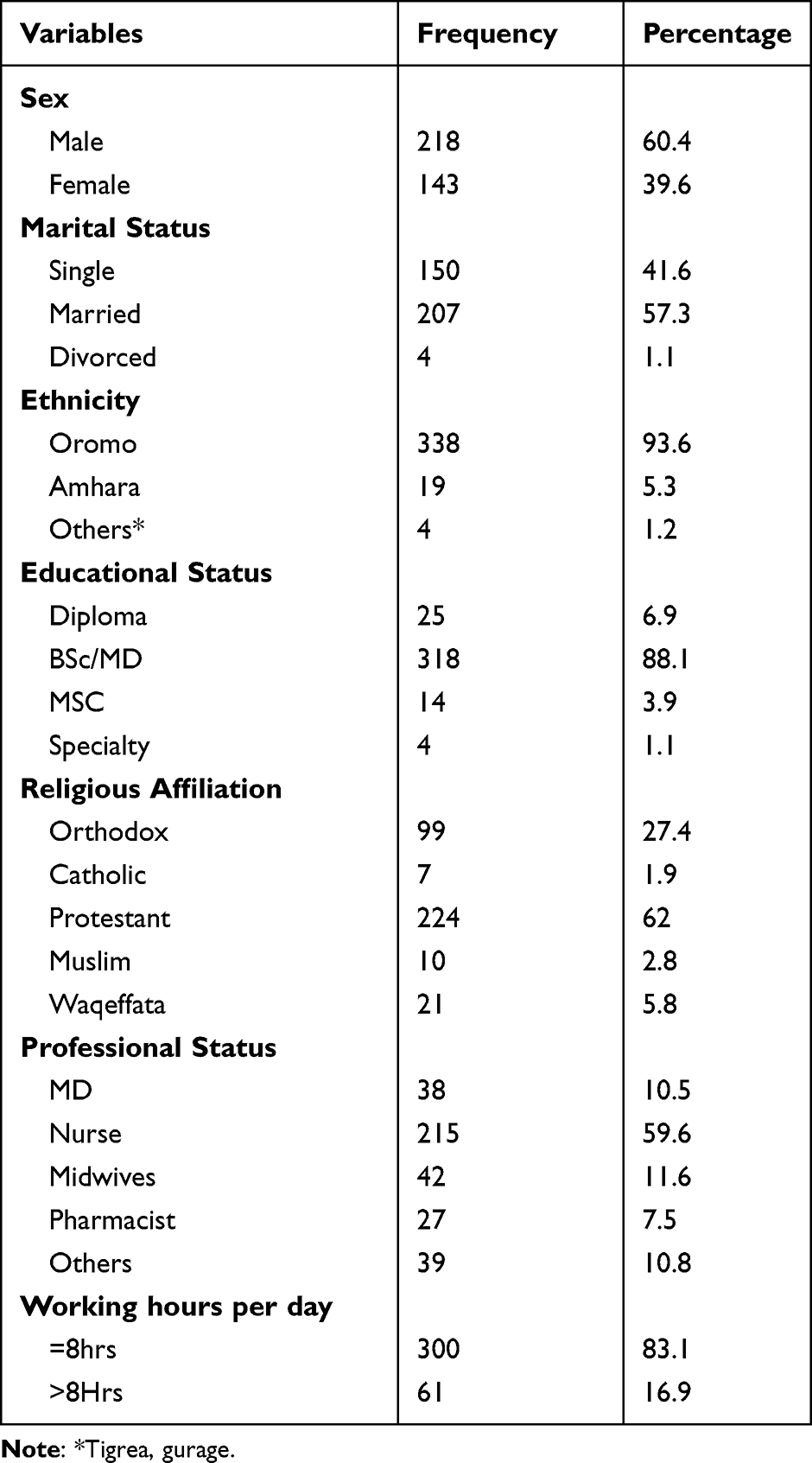 |
Table 1 Socio-Demographic Characteristics of Study Participants June 5 to August 30, 2020 |
Training on Personall Protective Equipment (PPE) and Ability to Use Correctly
Although it is expected that all healthcare workers get training on PPE, only 236 (65.4%) of study participants reported that they got training on how to put on and remove PPE. The respondents were asked whether they believed they could correctly don and doff based on the information received during training, and more than 80% of them reported knowing how to do it for disposable gloves, face masks, and NK95 face masks (Table 2).
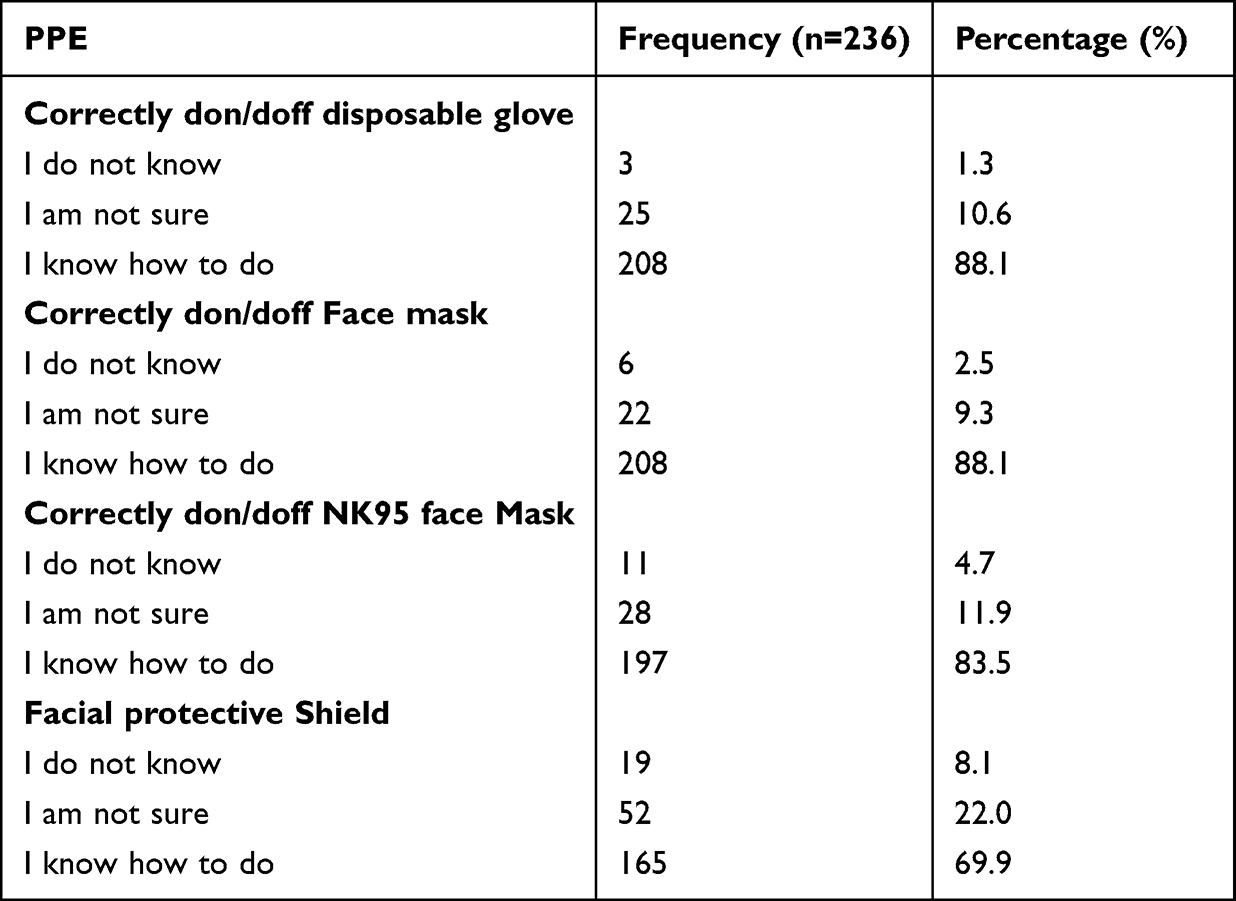 |
Table 2 Believe About Correctly Don and Doff PPE After Getting Training of Respondent June 5 to August 30, 2020 |
Access to Essential PPE
Study participants responded that they had access to hand sanitizer 322 (89.2%), disposable gloves 285 (78.9%), face masks 280 (77.6%), KN95 face masks 163 (45.2%) and facial protective shields 112 (31%) (Figure 1). One hundred sixty-nine (46.8%) of the study participants reported that their hospital has personal safety policies and procedures. Furthermore, the vast majority of them (310, 85.8%) reported having access to personal safety policies and procedures in their workplace. More than two-thirds (247, 68.4%) of the study participants reported that they do not have access to COVID-19 diagnostic and management systems.
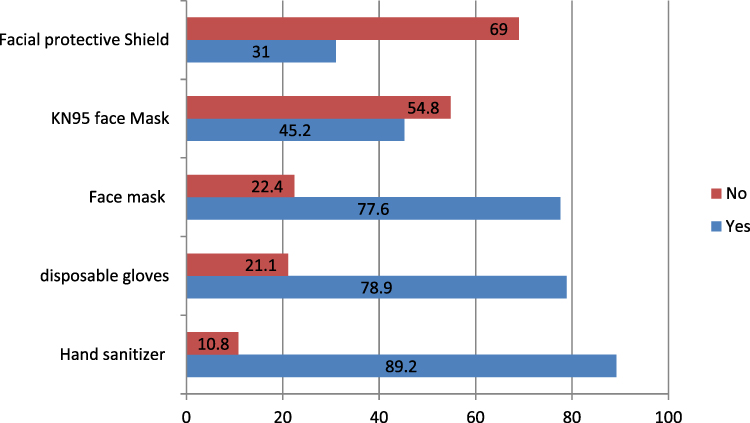 |
Figure 1 Type of personal protective equipment available to health professionals’ access to personal safety policies and procedures in the workplace. |
Perception About Access to PPE
Regarding perception about access to adequate PPE necessary for daily professional activity, 55 (15.2%), 183 (50.7%), and 123 (34%) respondents reported it as rarely/never, sometimes, and always, respectively (Figure 2). The analysis of perceptions among gender, education, marital status, and professional status toward access to adequate PPE for their daily activities was done and the results are shown in (Table 3).
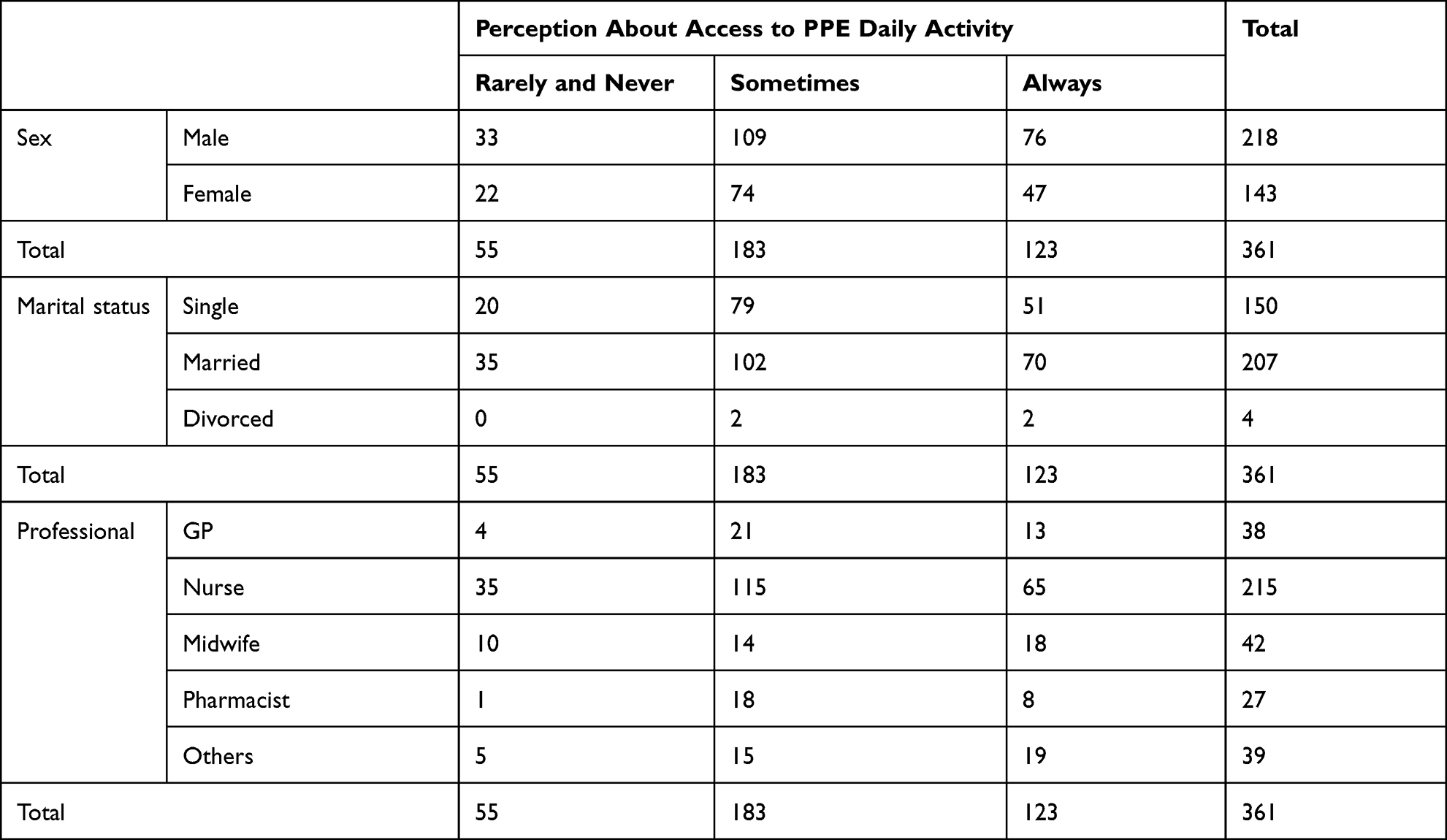 |
Table 3 Believe to Have Adequate Access to PPE for Daily Activity Cross Tabulation of Respondent June 5 to August 30, 2020 |
 |
Figure 2 Perception about access to adequate PPE among health professionals. |
Regarding perception about access to adequate information to use PPE to protect healthcare workers from contracting COVID-19 have received, only 126 (35%) participants reported as they always received adequate information (Figure 3).
 |
Figure 3 Perception about access to adequate information to use PPE among health professionals. |
Perception About Support from Their Own Hospital and Local Public Health Authorities
Participants in the study were asked about their perceptions of the hospital where they work, including whether they provide extra human resources to health professionals in the event they become ill, and reported mean = 2.68 Sd = 3.35. One hundred sixty-one (44%) reported that they perceived no support, while only 35 (9.7%) participants reported that they perceived themselves as fully supported.
Moreover, study participants’ perceptions about their own hospital and whether they were taking all the needed measurements to protect physical integrity in the workplace was mean 2.96 SD = 3.40. Of them, about 149 (41.3%) reported that they perceived no support, and about 37 (10.2%) were perceived as full support.
Furthermore, the participant was asked their perceptions about their nearby governmental health authorities taking all the needed measurements to protect physical integrity in the workplace and reported a mean of 2.86 SD = 3.34. Of them, about 151 (41.8%) reported that they perceived no support and about 33 (9.1%) perceived full support.
Finally, participants were asked about their perception of the risk of contracting COVID-19 within the next 30 days, and they reported that the mean risk of contracting COVID-19 is 62.2, with a standard deviation of 34.6.
Discussion
Ensuring a constant supply of PPE is important to protect healthcare workers from COVID-19. Our study aimed to assess the reality and perception of personal safety among health professionals in West Shoa, Ethiopia during the current COVID-19 pandemic. Many studies show that adequate training, proper use, and uninterrupted accessibilities of adequate PPE reduce the risk of infection when treating cases of COVID-19.8,9 Our results show that about 236 (65.4%) workers received training on COVID-19 infection prevention and controls. This finding is in line with the studies conducted in Ethiopia.10 This may be due to the fact that both the studies were conducted in the same country that is using similar guidelines and policies to train human power.
Inadequate PPE may put HCPs at risk of contracting the virus and infecting other healthcare workers and their families. This problem did not only exist in Ethiopia; it was also reported in China11 and other countries. This study’s findings showed that the majority of the healthcare workers had access to hand sanitizer, surgical face mask, and disposable gloves. However, there are healthcare workers that do not have access to KN95 face masks and facial protective shields as per WHO recommendation during the COVID-19 pandemic. This finding is similar to a study done in Latin America that reported access to PPE such as hand sanitizer (95%), disposable gloves (91.1%), disposable gowns (67.3%), disposable surgical masks (83.9%), N95 masks (56.1%), and facial protective shields (32.6%). In line with a study conducted in Latin America, our study findings showed that the majority of study participants had access to personal safety procedures and policies and had access to COVID-19 diagnostic and management processes.7
When asked whether they had received adequate information regarding the use of PPE to protect themselves from contracting COVID-19, only 34.9% of the healthcare workers reported that they had always received adequate information. The remaining respondents never, rarely, or sometimes received such information. This funding is similar to a study conducted in April,9,12 suggesting the main reasons for this difference are frequent changes due to in national and international guidelines about the use of PPE during the course of a pandemic and a lack of clarity in information. Moreover, this study finding showed that the majority of respondents perceived there to be inadequate help from their hospital and nearby governmental health authorities regarding their wellbeing. The finding is similar to a study done in Latin America that reported healthcare workers in that country had inadequate help from healthcare authorities during the COVID-19 pandemic.7
Finally, this study had some limitations. First, the study focused on more general populations of healthcare workers rather than those who might have direct contact with COVID-19 patients. Secondly, the results of this study are based on a self-reported questionnaire using a cross-sectional design that might not represent the true situation. Lastly, the study was not designed for hypothesis testing since it is difficult to generate outcome variables but mainly to generate descriptive information.
Conclusion and Recommendation
Many healthcare workers had limited access to essential PPE such as the NK95 face mask and facial protective shield, although access to other essential PPE seems good and there is a need to increase access to the particular PPE mentioned above. The need for implementing personal safety policies and allocating human resources in the work place. Training on PPE should be given to all healthcare workers to increase their personal safety and the integrity of the workplace.
The majority of study participants perceived inadequate support from their hospital and nearby governmental health authorities. Therefore, hospitals and local, nearby governmental health authorities should take all required protocols to protect physical integrity in the workplace through providing full support to healthcare workers.
Acknowledgment
We would like to acknowledge Ambo University for giving us an opportunity to address current hot public health concerns and would extend our gratitude to all study participants.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Safety, O. and H. Administration. Guidance on Preparing Workplaces for COVID-19. US: Department of Labor; 2020.
2. World Health Organization. Rational use of personal protective equipment for coronavirus disease (COVID-19): interim guidance; 2020.
3. Cook T. Personal protective equipment during the coronavirus disease (COVID) 2019 pandemic–a narrative review. Anaesthesia. 2020;75(7):920–927. doi:10.1111/anae.15071
4. Lancet T. COVID-19: protecting health-care workers. Lancet. 2020;395(10228):922. doi:10.1016/S0140-6736(20)30644-9
5. Mason DJ, Friese CR. Protecting health care workers against COVID-19—and being prepared for future pandemics. JAMA Health Forum. American Medical Association; 2020.
6. Jin Y-H, Huang Q, Wang YY, et al. Perceived infection transmission routes, infection control practices, psychosocial changes, and management of COVID-19 infected healthcare workers in a tertiary acute care hospital in Wuhan: a cross-sectional survey. Mil Med Res. 2020;7(1):1–13. doi:10.1186/s40779-020-00254-8
7. Delgado D, Wyss Quintana F, Perez G, et al. Personal safety during the COVID-19 pandemic: realities and perspectives of healthcare workers in Latin America. Int J Environ Res Public Health. 2020;17(8):2798. doi:10.3390/ijerph17082798
8. Birhanu A, Balis B, Yadeta TA, Bayu M. Personal protective equipment utilization practice and psychological preparedness of health care workers against COVID-19 pandemic in Eastern Ethiopia. SAGE Open Med. 2021;9:1–10. doi:10.1177/20503121211051925
9. Wang W, Min YZ, Yang CM, et al. Association of personal protective equipment use with successful protection against covid-19 infection among health care workers. medRxiv. 2020. doi:10.1101/2020.04.24.20070169
10. Suleiman A, Bsisu I, Guzu H, et al. Preparedness of frontline doctors in Jordan healthcare facilities to COVID-19 outbreak. Int J Environ Res Public Health. 2020;17(9):3181. doi:10.3390/ijerph17093181
11. Chapman S. Personal protective equipment (PPE) for healthcare workers: new cochrane evidence. Evidently cochrane; April 28, 2020. Available from: https://www.evidentlycochrane.net/personal-protective-equipment/.
12. Hakim M, Khattak FA, Muhammad S, et al. Access and use experience of personal protective equipment among frontline healthcare workers in Pakistan during the COVID-19 emergency: a cross-sectional study. Health Secur. 2021;19(2):140–149. doi:10.1089/hs.2020.0142
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.