")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Access and Disparities in the Use of Telemedicine Among Patients with Chronic Conditions in Saudi Arabia: A Cross-Sectional Study
Authors Almalki ZS , Imam MT, Abou Chahin NF, ALSammak NS, Entabli SM, Alhammad SK, Alanazi GF, Kharsa RA, Alonazi LA, Mandil RA, Albassam AA , Alshehri AM , Alahmari AK, Alem GM , Alalwan AA , Alamer A
Received 10 October 2023
Accepted for publication 28 November 2023
Published 4 December 2023 Volume 2023:16 Pages 3789—3798
DOI https://doi.org/10.2147/JMDH.S433653
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ziyad S Almalki,1 Mohammad T Imam,1 Nada F Abou Chahin,2 Naheda S ALSammak,2 Shahad M Entabli,2 Shatha K Alhammad,2 Ghuyudh F Alanazi,2 Rama A Kharsa,2 Layla A Alonazi,2 Rasha A Mandil,2 Ahmed A Albassam,1 Ahmed M Alshehri,1 Abdullah K Alahmari,1 Ghada M Alem,1 Abdullah A Alalwan,1 Ahmad Alamer1
1Department of Clinical Pharmacy, College of Pharmacy, Prince Sattam Bin Abdulaziz University, Al-Kharj, Saudi Arabia; 2Collage of Pharmacy, Almaarefa University, Riyadh, Saudi Arabia
Correspondence: Ziyad S Almalki, Department of Clinical Pharmacy, College of Pharmacy, Prince Sattam Bin Abdulaziz University, Al-Kharj, Saudi Arabia, Tel +966 11 588 7315, Email [email protected]
Purpose: This study investigated the access to and disparities in telemedicine use among patients with chronic conditions in Riyadh, Saudi Arabia.
Patients and Methods: A cross-sectional study of randomly selected primary healthcare centers was conducted to ensure that each of the 17 municipalities in Riyadh were represented. Three hundred and forty-two participants who completed the questionnaire were interviewed using a standardized questionnaire. The relationship between demographic and socioeconomic factors and telemedicine utilization was evaluated using the chi-square test and multivariable mixed-effects logistic regression model.
Results: Among the 342 participants, the study revealed that 25.73% of the patients utilized telemedicine. Older participants had lower odds of telemedicine use than did those aged ≤ 30 years [adjusted odds ratio (AOR) = 0.112, 95% confidence interval (CI) = 0.045– 0.279 for 50– 59 years; AOR = 0.19, 95% CI = 0.076– 0.474 for 60– 69 years; AOR = 0.223, 95% CI = 0.092– 0.542 for ≥ 70 years]. Female sex (AOR = 2.519, 95% CI = 1.44– 4.408), having a higher education level (AOR = 3.434, 95% CI = 1.037– 7.041 for secondary education and AOR = 5.87, 95% CI = 2.761– 8.235 for higher education), and living in urban areas (AOR = 2.721, 95% CI = 1.184– 6.256) were associated with higher odds of telemedicine use. Among socioeconomic factors, employed participants had higher odds of telemedicine use (AOR = 4.336, 95% CI = 2.3– 8.174). Furthermore, compared to those with the highest socioeconomic status (SES) index, those with the lowest SES were less likely to use telemedicine than those with the highest SES index (AOR = 0.193, 95% CI = 0.055– 0.683 for the lower bottom (poorest).
Conclusion: This study highlights a significant disparity in the utilization of telemedicine services across different populations, primarily due to demographic and socioeconomic factors.
Keywords: healthcare system, socioeconomic, digital health, inequities
Introduction
The burden of chronic diseases in Saudi Arabia has increased owing to various challenges, including limited access to healthcare services, escalating medical costs,1 an aging population,2 and a shortage of healthcare providers.3 To address these concerns, the Ministry of Health (MOH) has taken significant steps to ensure accessible healthcare services for all Saudi Arabian citizens by launching digital platforms such as the “Sehhaty” platform, MOH Formulary App, and “Anat”. Additionally, the Ministry established the 937 Call Center, which operates 24/7 to cater to the health needs of the callers.4
Telemedicine has become crucial for the remote delivery of healthcare services.5 This is considered a major breakthrough in healthcare service delivery that can potentially enhance the quality of medical care. Telemedicine can address issues such as lengthy waitlists, limited accessibility in rural areas, limited service hours, and patient no-shows,6,7 which are particularly beneficial for patients with chronic illnesses who require regular care. Patient satisfaction with virtual services and treatments is increasing, indicating the potential benefits of this approach.8 Therefore, incorporating telemedicine services is a promising strategy for effectively managing chronic diseases and improving patient quality of life.
Telemedicine has the potential to meet the health care needs of underserved populations. This can exacerbate existing disparities in access to healthcare for patients from demographic and socioeconomic backgrounds who already face inequities.9 It is crucial for the MOH to take action and make telemedicine services available to all patients, regardless of their socioeconomic background, to ensure equal healthcare opportunities for both citizens and expatriates in the public sector.
Despite the growing popularity of telemedicine in Saudi Arabia, there are still concerns regarding equity issues that have not been fully investigated or reported. Therefore, this study aimed to examine access to telemedicine and disparities in telemedicine consumption among patients with chronic conditions in Riyadh. By identifying the factors that influence patient utilization of telemedicine, the Saudi MOH can develop tailored strategies to encourage its adoption across different populations.
Materials and Methods
Study Design and Study Population
Primary healthcare settings are deemed the best option for recruiting patients with chronic conditions, because of their crucial role in providing comprehensive and ongoing care. As such, a cross-sectional study was conducted in randomly selected primary healthcare centers across all 17 municipalities in Riyadh between November 1, 2022, and March 3, 2023. The criteria for participation included individuals who were 18 years of age or older and currently live in Saudi Arabia. Additionally, the participants were required to have a minimum of one of the following chronic conditions: hypertension, dyslipidemia, diabetes mellitus, congestive heart failure, kidney disease, thyroid disease, mental disorders, or anemia. Non-Saudi individuals were recruited to enhance the diversity and representativeness of the participant population for research conducted in primary health care centers. Individuals under the age of 18 and those with insufficient abilities to engage in the survey or offer permission were excluded.
Convenience sampling was used in this study as all eligible participants were included. According to Government Statistics, the prevalence rate of chronic conditions in Saudi Arabia is 15.9%.10 The minimum required sample size for this study was determined to be 206 individuals using the Raosoft calculator. The computation was conducted with a confidence level of 95% and margin of error of 5%, with an assumed response rate of 50%. Nevertheless, 342 participants were ultimately enrolled to ensure sufficient sample size.
This study adhered to the ethical guidelines of the Declaration of Helsinki and was approved by the Institutional Review Board of the MOH (IRB Log Number 22-490). The informed consent form addressed anonymity and confidentiality concerns, and was signed by all participants prior to their involvement in the study. The participants were informed of the voluntary nature of their participation and that they could withdraw at any time without facing negative consequences.
Data Collection and Questionnaires
During their visit to the primary healthcare facility, respondents were interviewed face-to-face using a standardized questionnaire. The questionnaire was divided into three parts and covered sociodemographic and clinical profile factors and healthcare service consumption over the previous three months. Field specialists carefully evaluated and confirmed the structure of the questionnaire to ensure validity. A pilot study was conducted by administering the questionnaire twice to 10 people, with a two-week interval between administrations, to ensure its reliability. The internal validity of each questionnaire was assessed. We selected teams of highly qualified interviewers, who were briefed on delivering the questionnaire to ensure dependability and consistency throughout the interviews.
Independent Variables
When analyzing healthcare service consumption, it is crucial to consider the factors that affect people’s decisions and actions. These factors can vary greatly and are influenced by complex determinants.11 Therefore, we included the following questions to identify these factors in the questionnaire. The questions were categorized into various categories, including sociodemographic characteristics such as age (continuous data), gender (male or female), marital status (married or not married), nationality (Saudi or non-Saudi), education level (illiterate/read/write, primary education, intermediate education, secondary education, or higher education), employment status (employed or unemployed), residential area (rural or urban), health insurance status (having health insurance or not having health insurance), and whether they had a regular doctor (having a regular doctor or not having a regular doctor).
Socioeconomic status (SES) is a crucial factor in social research, and is often measured using indicators such as education, income, and occupation. However, a composite measure is required in countries where the variables may be inaccurate or insufficient. Many researchers have suggested that a country-specific SES index is a better economic indicator than income.12,13 Our study used principal component analysis to create a valid country-specific SES index from different asset holdings. This enabled us to measure SES more concisely and meaningfully.14 An SES index was constructed for each interview by considering many indicators, including education level, employment status of the household head, housing type, housing tenure, car ownership, and ownership of household assets. The housing types were categorized as follows: traditional homes, villas, villa floors, apartments, and other housing options. Additionally, the classification of housing tenure encompassed four groups: privately owned housing, rented housing, provided housing, and alternative forms of tenure. Information related to car ownership was categorized into three distinct groups: individuals without a car, individuals with a single car, and individuals with two or more cars. In this study, we investigated asset ownership by utilizing eight dichotomous variables: phone availability, television availability, desktop or laptop availability, connectivity to the Internet, library availability, satellite availability, video availability, and video game availability. Each participant’s SES was categorized into one of five categories, with the first category being the lowest SES (poorest) and the fifth category representing the highest SES (wealthiest).
During the interview, the participants were asked about their medical history and whether they had been diagnosed with any chronic disease. Clinical indicators consisted of various categories of chronic diseases, including dyslipidemia, diabetes mellitus, hypertension, asthma, thyroid disease, kidney disease, congestive heart failure, psychiatric disorders, and anemia. Additionally, participants were asked to report their self-assessed health status, which was categorized as excellent, very good, good, fair, or poor.
Dependent Variable
To assess the use of telemedicine within the study group, we inquired if participants engaged with healthcare professionals through two-way synchronous communication methods such as video conferencing, phone calls, or mobile apps. Based on their responses, we divided the study population into two categories: those who used telemedicine within the last three months and those who only received in-person care. We excluded individuals who lacked reliable Internet access or had significant cognitive impairments to ensure that everyone had access to and could effectively participate in telemedicine.
Statistical Analysis
Participants were described using descriptive statistics. To identify associations, we performed a chi-squared test for categorical variables. To investigate the correlation between telemedicine use and demographic and socioeconomic factors, we used a multivariate mixed-effects logistic regression model that was adjusted for sex, age, and marital status. Telemedicine was the dependent variable. Age, gender, marital status, nationality, education level, employment status, residential area, health insurance status, and whether they had a regular doctor, SES, Dyslipidemia, Diabetes mellitus, Hypertension, Asthma, Thyroid disease, Kidney Disease, Congestive Heart Failure, Psychiatric disease, anemia, and self-rating of health were used as independent variables. Univariate logistic regression analysis was performed. Predictors with P<0.20 were included in the final multivariate logistic regression model. Statistical significance was determined by setting the significance level for all analyses at ≤ 5%. All analyses were performed using the statistical software SAS (version 9.4; SAS Institute, Inc., Cary, NC, USA).
Results
This study included 342 participants from diverse backgrounds. The majority of participants (28.95%) were aged between 50 and 59 years, male (57.89%), married (79.82%), Saudi nationals (94.15%), and had completed secondary education (32.8%). Additionally, a significant number of the participants (82.46%) lived in urban areas. Of all participants, 88 (25.73%) used telemedicine and completed the questionnaire. Table 1 presents the characteristics of the participants.
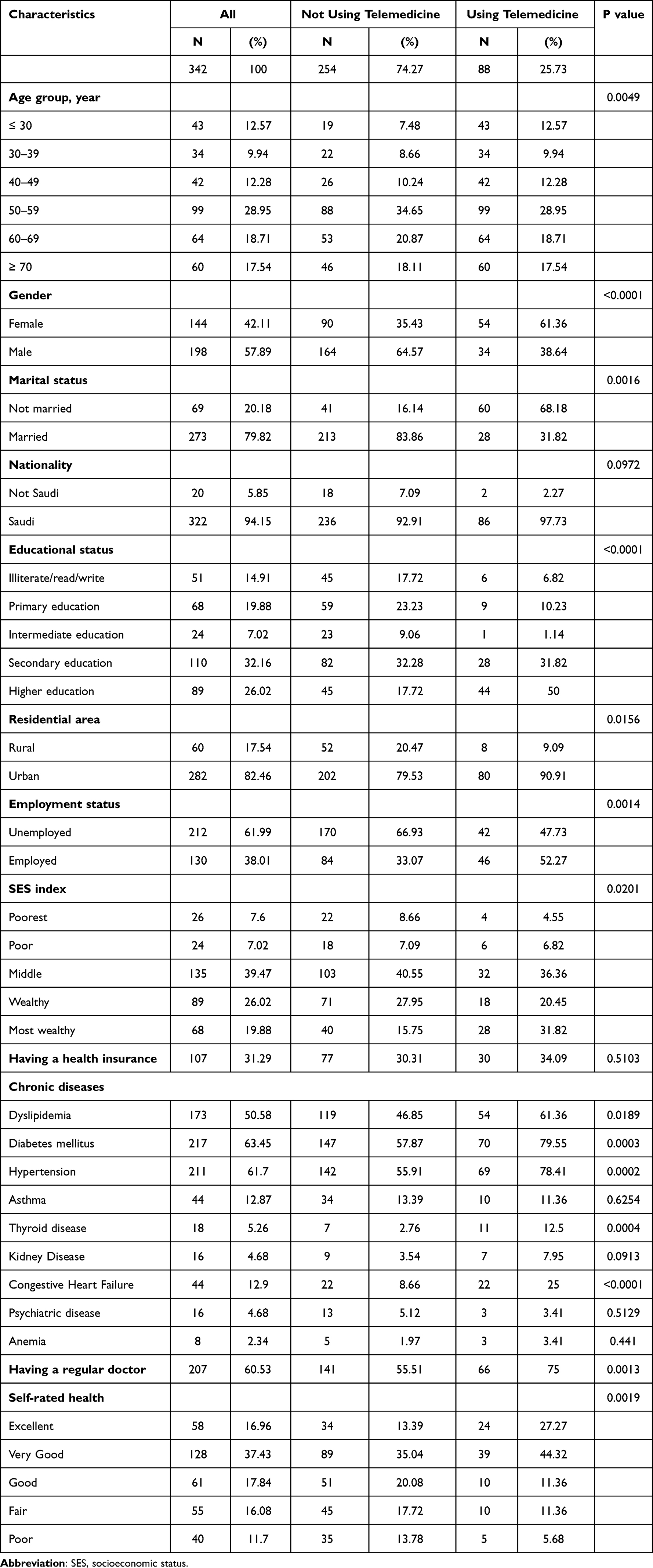 |
Table 1 Characteristics of Study Participants |
Multivariate logistic regression analysis (Table 2) revealed various demographic and health-related factors that significantly predicted telemedicine utilization. We found that individuals aged 50 years and above had lower odds of using telemedicine than those aged 30 years and below [adjusted odds ratio (AOR) = 0.112, 95% confidence interval (CI)= 0.045–0.279 for 50–59 years; AOR = 0.19, 95% CI = 0.076–0.474 for 60–69 years; AOR = 0.223, 95% CI = 0.092–0.542 for ≥ 70 years]. Women were more likely to use telemedicine (AOR = 2.519, 95% CI = 1.44–4.408), and those with higher education levels (AOR = 3.434, 95% CI = 1.037–7.041 for secondary education and AOR = 5.87, 95% CI = 2.761–8.235 for higher education). Living in urban areas was also associated with a higher odds of telemedicine use (AOR = 2.721, 95% CI = 1.184–6.256).
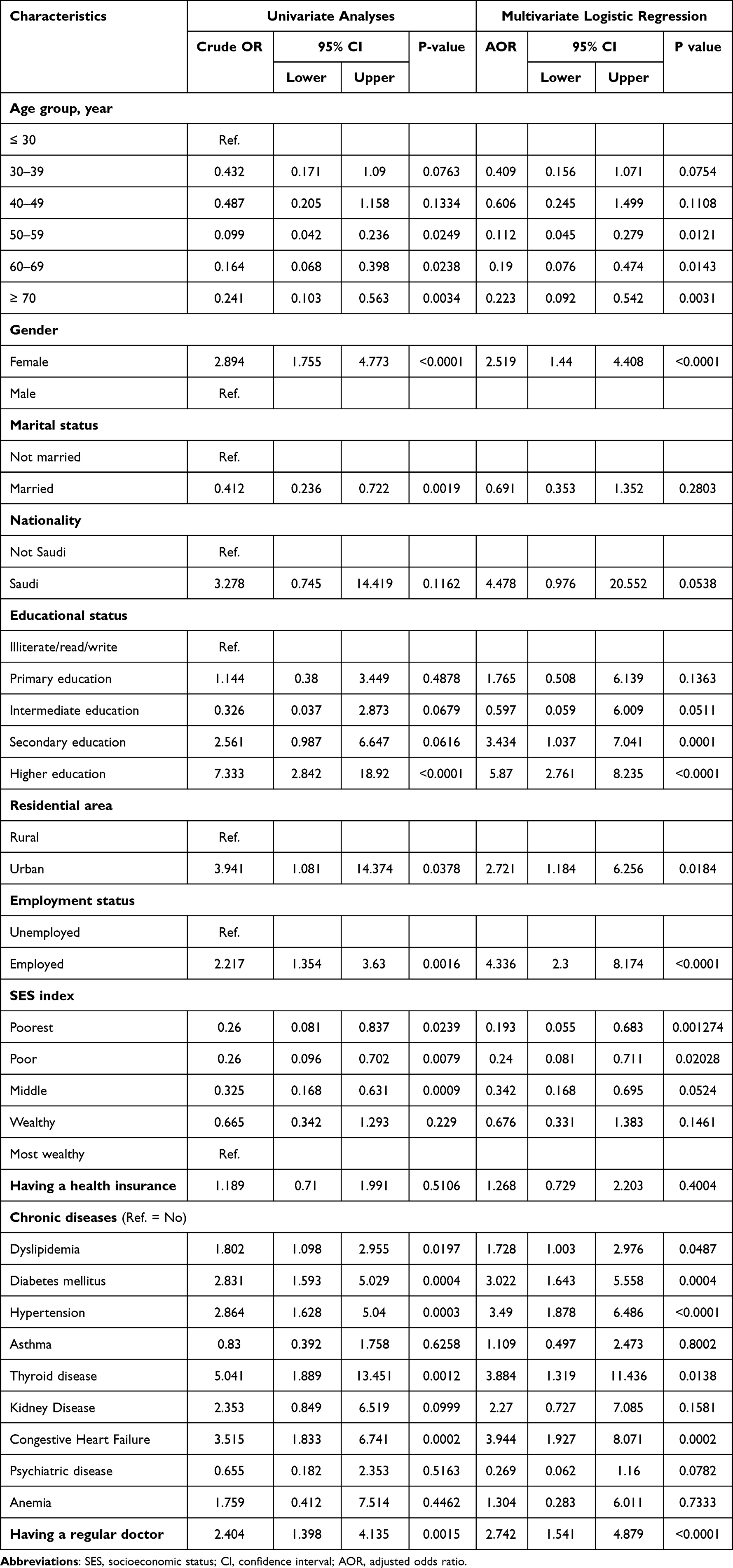 |
Table 2 Factors Associated with Telemedicine Use |
Among socioeconomic factors, employed participants had higher odds of telemedicine use(AOR = 4.336, 95% CI = 2.3–8.174). Furthermore, we found that individuals with lower SES were less likely to use telemedicine(AOR = 0.193, 95% CI = 0.055–0.683 for the lower bottom(poorest), and AOR = 0.24, 95% CI = 0.0881–0.711 for the upper bottom(poor]). In addition, patients with chronic conditions, such as hypertension(AOR = 3.49; 95% CI, 1.878–6.486), diabetes mellitus(AOR = 3.022, 95% CI = 1.643–5.558), dyslipidemia(AOR = 1.728, 95% CI = 1.003–2.976), thyroid disease(AOR = 3.884, 95% CI = 1.319–11.436), and congestive heart failure(AOR = 3.944, 95% CI = 1.927–8.071), were more likely to use telemedicine. Finally, patients with ongoing and established relationships with a regular doctor were more likely to engage in telemedicine(AOR = 2.742, 95% CI = 1.541–4.879).
Telemedicine was associated with higher self-reported health (AOR = 2.519, 95% CI = 1.44–4.408) (Figure 1). This has allowed individuals with better health to take advantage of telemedicine, as they have the physical and cognitive ability to navigate technology and utilize virtual platforms for their healthcare needs.
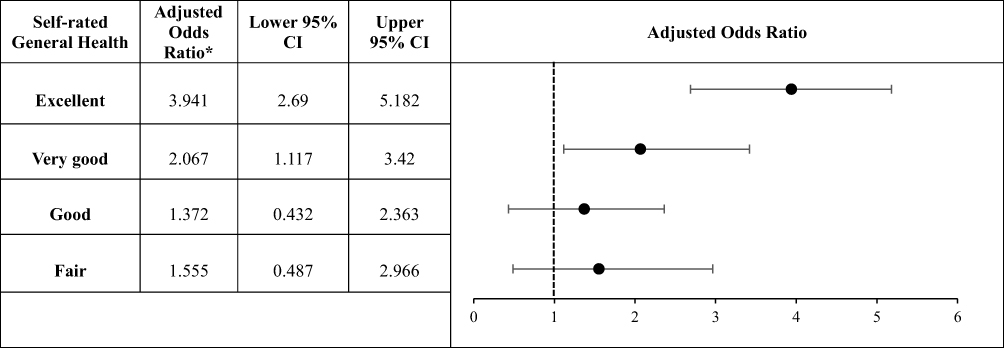 |
Figure 1 The association between telemedicine use and self-rated general health. *“Poor” was used as a reference for this analysis. |
Discussion
There is a noticeable trend in exploring the significant gaps in healthcare access for marginalized communities regarding advanced healthcare delivery techniques, such as telemedicine. This research endeavored to analyze the use of telemedicine for individuals with chronic illnesses in Riyadh, Saudi Arabia, and to detect inequities in this domain.
Based on the results of this study, telemedicine may not be frequently utilized in Saudi Arabia despite its advantages, or may not be commonly used in certain groups of patients. According to this study, there was a notable difference in the use of telemedicine services among the various groups, largely influenced by demographic and socioeconomic factors. This aligns with previous research indicating that elderly patients often face difficulties accessing digital health products, resulting in slower adoption rates.15–17 These challenges include difficulties with technology literacy, limited access to the Internet or devices, and concerns regarding privacy and security.18,19 Addressing these barriers is crucial for promoting greater utilization of telemedicine services among older adults.
Research has shown gender disparities in healthcare utilization, with women seeking medical attention and utilizing healthcare services more often than men.20 This trend can be attributed to several factors, such as women taking greater responsibility for their health and being more concerned about their well-being.21 Our study supports previous findings that indicate that females are more inclined to utilize telemedicine services than males.
Studies have shown that patients with higher education levels are more likely to use telemedicine.22,23 The results of this study confirm this observation. It is worth noting that the impact of educational level on telemedicine use may differ based on various factors such as the availability of technology and digital skills. Additionally, the results of this study raise awareness of potential fairness issues concerning the use of telemedicine.
Our findings showed that telemedicine is more commonly used by patients residing in urban areas, indicating the importance of implementing policies and interventions to address this disparity. Ensuring that underserved populations in rural areas have equal access to health care services, including telemedicine, is crucial. Previous studies have also supported these findings, demonstrating a higher utilization of telemedicine among patients in urban areas.24,25
Furthermore, our research revealed that individuals with higher employment or socioeconomic status tended to use telemedicine services more frequently. This is primarily due to the financial stability and ability to invest in the equipment and internet connectivity required for telemedicine.26 However, this discrepancy in access to telemedicine is worrisome, as it may further widen existing healthcare disparities.
Based on our findings, patients who regularly visited doctors tended to use telemedicine more frequently. This aligns with previous research that reported similar findings.27 The high consumption of telemedicine among patients with a consistent healthcare provider indicates that building a strong patient-provider rapport is critical for accepting and embracing telemedicine as a reliable healthcare delivery option.28
Telemedicine has become more common in the management and treatment of chronic conditions, such as hypertension, diabetes mellitus, dyslipidemia, thyroid disease, and congestive heart failure. This trend towards telemedicine can be attributed to its convenience and accessibility, as it provides patients with chronic conditions a platform to receive medical care, monitor their symptoms, and engage in self-care.29 Patients no longer need to travel to physical clinics for routine checkups or follow-up appointments as they can consult healthcare providers from their homes. Overall, this was a positive sign. Access to ongoing quality medical care is crucial for individuals with chronic conditions to manage their health and well-being properly.
Our research indicates that individuals in good health tend to prefer telemedicine. This aligns with similar studies on telemedicine, which suggest that patients with better overall health are more responsive to these services.30–32 In the context of this study, it appears that patients with fewer and less severe chronic conditions tend to use telemedicine services more often than those with multiple chronic illnesses or more severe diseases. This highlights the advantages of remote management for patients requiring consistent monitoring and medical attention but not necessarily immediate in-person care.
This study provides important insights into differences in the use of telemedicine services among various populations. However, this study had several limitations. First, its cross-sectional design captures data only at a specific time and cannot establish cause-and-effect relationships. Second, by excluding patients without internet access, the study may have overlooked a significant portion of the population that could benefit from telemedicine. Third, using face-to-face interviews as a data collection method may introduce limitations and biases such as recall bias, social desirability bias, and interviewer bias. Finally, the sample size was small and only represented one region, which limits the generalizability of the findings to a larger population.
Conclusion
This study highlights the disparity in the utilization of telemedicine services among patients with chronic diseases, which can be attributed to demographic and socioeconomic factors. Furthermore, there was a correlation between an individual’s overall well-being and the likelihood of using telemedicine services. It is essential to address and rectify these disparities to provide equitable access to telemedicine services. It is crucial to prioritize vulnerable groups in the allocation of interventions to ensure equitable access to these valuable services. By directly acknowledging and addressing these disparities, health care systems can promote health equity and enable various groups to utilize telemedicine services.
Acknowledgments
This study is supported via funding from Prince Sattam bin Abdulaziz University project number (PSAU/2023/R/1444).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rahman R, Salam MA. Policy discourses: shifting the burden of healthcare from the state to the market in the Kingdom of Saudi Arabia. INQUIRY. 2021;58:00469580211017655. doi:10.1177/00469580211017655/ASSET/IMAGES/LARGE/10.1177_00469580211017655-FIG1.JPEG
2. Salam AA. Ageing in Saudi Arabia: new dimensions and intervention strategies. Sci Rep. 2023;13(1):1–11. doi:10.1038/s41598-022-25639-8
3. Gurajala S. Healthcare system in the Kingdom of Saudi Arabia: an expat doctor’s perspective. Cureus. 2023;15(5). doi:10.7759/CUREUS.38806
4. Health sector transformation program - vision 2030. Available from: https://www.vision2030.gov.sa/v2030/vrps/hstp/.
5. Haleem A, Javaid M, Singh RP, Suman R. Telemedicine for healthcare: capabilities, features, barriers, and applications. Sensors Int. 2021;2:100117. doi:10.1016/J.SINTL.2021.100117
6. Ameis SH, Lai MC, Mulsant BH, Szatmari P. Coping, fostering resilience, and driving care innovation for autistic people and their families during the COVID-19 pandemic and beyond. Mol Autism. 2020;11(1):1–9. doi:10.1186/S13229-020-00365-Y/TABLES/1
7. Gajarawala SN, Pelkowski JN. Telehealth benefits and barriers. J Nurse Pract. 2021;17(2):218. doi:10.1016/J.NURPRA.2020.09.013
8. Alharbi KG, Aldosari MN, Alhassan AM, Alshallal KA, Altamimi AM, Altulaihi BA. Patient satisfaction with virtual clinic during Coronavirus disease (COVID-19) pandemic in primary healthcare, Riyadh, Saudi Arabia. J Family Community Med. 2021;28(1):48. doi:10.4103/JFCM.JFCM_353_20
9. Leone E, Eddison N, Healy A, Royse C, Chockalingam N. Do UK Allied Health Professionals (AHPs) have sufficient guidelines and training to provide telehealth patient consultations? Hum Resour Health. 2022;20(1). doi:10.1186/S12960-022-00778-1
10. The general authority for statistics in Saudi Arabia. Statistical Yearbook of 2018. Available from: https://www.stats.gov.sa/ar/258.
11. Bastani P, Mohammadpour M, Samadbeik M, Bastani M, Rossi-Fedele G, Balasubramanian M. Factors influencing access and utilization of health services among older people during the COVID − 19 pandemic: a scoping review. Arch Public Health. 2021;79(1):1–11. doi:10.1186/S13690-021-00719-9/FIGURES/5
12. Howe LD, Hargreaves JR, Gabrysch S, Huttly SRA. Is the wealth index a proxy for consumption expenditure? A systematic review. J Epidemiol Community Health. 2009;63(11):871–877. doi:10.1136/JECH.2009.088021
13. Victora CG. Socio-economic differences in health, nutrition, and population within developing countries: an overview. JAMA. 2007;298(16):1943–1949. doi:10.1001/jama.298.16.1943
14. Friesen CE, Seliske P, Papadopoulos A. Using principal component analysis to identify priority neighbourhoods for health services delivery by ranking socioeconomic status. Online J Public Health Inform. 2016;8(2):192. doi:10.5210/OJPHI.V8I2.6733
15. Levine DM, Lipsitz SR, Linder JA. Trends in seniors’ use of digital health technology in the United States, 2011–2014. JAMA. 2016;316(5):538–540. doi:10.1001/JAMA.2016.9124
16. Price JC, Simpson DC. Telemedicine and health disparities. Clin Liver Dis. 2022;19(4):144. doi:10.1002/CLD.1171
17. Latulipe C, Gatto A, Nguyen HT, et al. Design considerations for patient portal adoption by low-income, older adults. Proc SIGCHI Conf Hum Factors Comput Syst. 2015;2015:3859. doi:10.1145/2702123.2702392
18. Wilson J, Heinsch M, Betts D, Booth D, Kay-Lambkin F. Barriers and facilitators to the use of e-health by older adults: a scoping review. BMC Public Health. 2021;21(1):1–12. doi:10.1186/S12889-021-11623-W/TABLES/2
19. Mao A, Tam L, Xu A, et al. Barriers to telemedicine video visits for older adults in independent living facilities: mixed methods cross-sectional needs assessment. JMIR Aging. 2022;5(2):e34326. doi:10.2196/34326
20. Mustard CA, Kaufert P, Kozyrskyj A, Mayer T. Sex differences in the use of health care services. N Engl J Med. 1998;338(23):1678–1683. doi:10.1056/NEJM199806043382307
21. Chang HT, Lai HY, Hwang IH, Ho MM, Hwang SJ. Home healthcare services in Taiwan: a nationwide study among the older population. BMC Health Serv Res. 2010;10(1):1–6. doi:10.1186/1472-6963-10-274/TABLES/3
22. Stamenova V, Agarwal P, Kelley L, et al. Uptake and patient and provider communication modality preferences of virtual visits in primary care: a retrospective cohort study in Canada. BMJ Open. 2020;10(7):e037064. doi:10.1136/BMJOPEN-2020-037064
23. Hardcastle L, Ogbogu U. Virtual care: enhancing access or harming care? Healthc Manage Forum. 2020;33(6):288–292. doi:10.1177/0840470420938818
24. Hall JN, Ackery AD, Dainty KN, et al. Designs, facilitators, barriers, and lessons learned during the implementation of emergency department led virtual urgent care programs in Ontario, Canada. Front Digit Health. 2022:4. doi:10.3389/FDGTH.2022.946734
25. Bhatia RS, Chu C, Pang A, Tadrous M, Stamenova V, Cram P. Virtual care use before and during the COVID-19 pandemic: a repeated cross-sectional study. C Open. 2021;9(1):E107. doi:10.9778/CMAJO.20200311
26. Mistry SK, Shaw M, Raffan F, et al. Inequity in access and delivery of virtual care interventions: a scoping review. Int J Environ Res Public Health. 2022;19(15):9411. doi:10.3390/IJERPH19159411/S1
27. Gray C, Wray C, Tisdale R, Chaudary C, Slightam C, Zulman D. Factors influencing how providers assess the appropriateness of video visits: interview study with primary and specialty health care providers. J Med Internet Res. 2022;24(8):e38826. doi:10.2196/38826
28. Toh N, Pawlovich J, Grzybowski S. Telehealth and patient-doctor relationships in rural and remote communities. Can Fam Physician. 2016;62(12):961.
29. Burton L, Rush KL, Smith MA, et al. Empowering patients through virtual care delivery: qualitative study with micropractice clinic patients and health care providers. JMIR Form Res. 2022;6(4):e32528. doi:10.2196/32528
30. Lilly CM, Cody S, Zhao H, et al. Hospital mortality, length of stay, and preventable complications among critically ill patients before and after tele-ICU reengineering of critical care processes. JAMA. 2011;305(21):2175–2183. doi:10.1001/JAMA.2011.697
31. Arora P, Mehta D, Ha J. Impact of telehealth on health care resource utilization during the COVID-19 pandemic. J Comp Eff Res. 2022;11(5):301–309. doi:10.2217/CER-2021-0242/ASSET/BD13C512-4247-4E96-AEDD-BD12423C68CB/ASSETS/IMAGES/LARGE/FIGURE4.JPG
32. Berlin A, Lovas M, Truong T, et al. Implementation and outcomes of virtual care across a tertiary cancer center during COVID-19. JAMA Oncol. 2021;7(4):597–602. doi:10.1001/JAMAONCOL.2020.6982
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.