Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Acceptability, Appropriateness and Feasibility of a Nurse-Led Integrated Care Intervention for Patients with Severe Exacerbation of COPD from the Healthcare Professional’s Perspective – A Mixed Method Study
Authors Hübsch C ![]() , Clarenbach C
, Clarenbach C ![]() , Chadwick P
, Chadwick P ![]() , Peterer M, Beckmann S
, Peterer M, Beckmann S ![]() , Naef R
, Naef R ![]() , Schmid-Mohler G
, Schmid-Mohler G ![]()
Received 7 February 2023
Accepted for publication 30 May 2023
Published 19 July 2023 Volume 2023:18 Pages 1487—1497
DOI https://doi.org/10.2147/COPD.S404712
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Christine Hübsch,1,2 Christian Clarenbach,2,3 Paul Chadwick,4 Matthias Peterer,5 Sonja Beckmann,1 Rahel Naef,1,6 Gabriela Schmid-Mohler1,2
1Centre of Clinical Nursing Science, University Hospital Zurich, Zurich, Switzerland; 2Division of Pulmonology, University Hospital Zurich, Zurich, Switzerland; 3Faculty of Medicine, University of Zurich, Zurich, Switzerland; 4Centre for Behaviour Change, University College London, London, UK; 5Physiotherapy Occupational Therapy, University Hospital Zurich, Zurich, Switzerland; 6Institute for Implementation Science in Health Care, Faculty of Medicine, University of Zurich, Zurich, Switzerland
Correspondence: Gabriela Schmid-Mohler, Centre of Clinical Nursing Science, University Hospital Zurich, Rämistrasse 100, Zurich, CH-8091, Switzerland, Tel +41 44 255 20 03, Email [email protected]
Purpose: To improve inpatient care and self-management in patients with severe acute exacerbations of COPD, we implemented a nurse-led behavioral intervention. This study aimed to assess implementation outcomes from the perspective of the healthcare professionals (HCP) who delivered it.
Methods: Using an explanatory sequential mixed method approach, we conducted an online questionnaire and two small group interviews. We applied descriptive statistics for quantitative data, a framework analysis for qualitative data, and a mixed methods matrix to integrate the results.
Results: A total of 19 of 27 invited participants answered the online questionnaire; 9 of 19 participated in the group interviews. The intervention’s overall acceptability, appropriateness, and feasibility was rated high to very high (median 5/5; 4/5 and 4/5). Enablers to implementation included general recognition of the need for specialized care, sufficient knowledge of the intervention by HCP, and strong interprofessional collaboration. Main barriers included the lack of resident physician’s resources and difficulties in adaptability.
Conclusion: While the acceptance of the intervention was very high, the perceived appropriateness and feasibility were affected by its complexity. The availability of a knowledgeable interprofessional core team is a strategy that supports the implementation of complex interventions.
Keywords: COPD, self-management, complex intervention, implementation outcomes, program evaluation, behaviour change wheel
Introduction
Integrated, structured, and personalized self-management interventions are key components in the treatment and long-term management of chronic obstructive pulmonary disease (COPD).1–4 Such interventions’ overall aim is to motivate, engage and support patients with COPD to adapt their health-related behaviors according to best available evidence and develop skills to manage their disease.3 For those with stable COPD, behaviors such as early recognition and treatment of exacerbations, smoking cessation, physical activity, maintenance of a healthy diet, medication adherence, and management of dyspnea and burdensome emotions are associated with improvements in health-related quality of life and reductions in respiratory-related hospitalizations, as well as improvements in dyspnea and exercise capacity.4–6
In Switzerland, quality of acute inpatient care for patients with severe acute exacerbations of COPD (AECOPD) is high, but researchers have identified a lack of coordinated self-management support across various sectors.7,8 To address this gap in service delivery, Schmid-Mohler et al9 developed the nurse-led integrated care COPD (NICCO) intervention. The development was guided by the Behaviour Change Wheel (BCW) framework.10 NICCO is an evidence-based, standardized, and complex hospital-ward-initiated behavioral intervention to improve self-management in patients with AECOPD.
Outcome evaluation of complex interventions is vital to implementation success and for achieving desired changes in clinical and service outcomes.11 Implementation outcomes are defined as “effects of deliberate and purposive actions to implement new […] services”.1 Based on the work of Proctor et al11 acceptability, appropriateness, and feasibility were chosen as implementation outcomes because they are described as leading for implementation success at the time of study conception.12 Our intention was to assess implementation outcomes six months after the intervention was introduced to adapt the content and delivery accordingly.
Aim
The aim of this study was to assess the newly implemented AECOPD intervention’s acceptability, appropriateness, and feasibility from the perspectives of the involved healthcare professionals (HCP) and to understand its barriers and enablers. The results will be used to adapt and further implement the intervention.
Methods
Study Design
An explanatory sequential mixed method (quant –QUAL) design was applied. This design requires the collection and analysis first of quantitative then of qualitative data. The quantitative and qualitative results are then integrated during the interpretation phase. This design uses qualitative data to help explain and elaborate quantitative results in greater depth.13 For the current study, the quantitative data were gathered via an online questionnaire using web-based SurveyMonkey®; qualitative data were collected first via open-ended questions in the same questionnaire, then in small group interviews (Figure 1).
 |
Figure 1 Explanatory Sequential Mixed Method Design. |
The NICCO Intervention
The overall aim of the NICCO intervention is to positively influence the patients’ quality of life while avoiding rehospitalizations. Using the BCW as a methodological approach,10 interventions concerning three key behaviors that influence COPD progression were developed: exacerbation management, physical activity, and ongoing smoking.9 The final intervention includes six complementary behaviors: adherence to vaccination recommendations; adherence to inhalation; adherence to long-term oxygen; adherence to nutrition to prevent or manage underweight; management of dyspnea and related emotional distress; and writing an advance care plan for end-of-life-care. While the intervention is delivered by a range of different professionals (nurses, physicians, physiotherapists and, if needed, social workers, nutritionists, and psychiatrists) the overall lead has an advanced practice nurse (APN) team.7 The APN team consists of four nurses with experience in the field of pneumology, of whom the team leader has a doctorate, one nurse has a master’s degree, one has a bachelor’s degree, and one is an experienced nurse. The highly standardized intervention is based on a comprehensive assessment and starts face-to-face during patients’ hospital stay for AECOPD. Post-discharge telephone support by the APN team continues one to two weekly for at least twelve weeks.
Setting, Recruitment and Participants
The current study took place at the pneumological clinic of the University Hospital Zurich. In November 2020, we invited internal and external HCP who have been involved in direct patient care since the NICCO intervention has been introduced (ie, June 2020) to complete an online questionnaire. The APN team members identified 27 eligible persons, whom the primary author contacted via email.
Data Collection
Online Questionnaire
In November 2020, we conducted the online questionnaire. It had three parts: (1) Sociodemographic data on professional designation and place of work; and (2) German translations of the Acceptability of Intervention Measure (AIM), the Intervention Appropriateness Measure (IAM), and the Feasibility of Intervention Measure (FIM) scales.12 Each of the three scales contains four items; all are rated on a 5-point response scale (1 = completely disagree, 5 = completely agree), we added a sixth option—“no response” (0 points). For the questionnaire’s translation and adaption, we conducted a best practice process including forward and backward translation.14 For the final part (3), we used two open-ended questions: “I have the following suggestions for improvement for the NICCO intervention” and “This is what else I would like to feed back on the NICCO intervention”.
Small Group Interviews
In December 2020, we conducted two 45-minute small group interviews. Due to restrictions on in-person meetings during the COVID-19 pandemic, the Zoom video communication platform was used. A PhD-trained clinical nurse scientist who is not involved in the NICCO intervention conducted both interviews. We used a structured interview guide, which was based on the results of the online questionnaires (median/ interquartile range per scale). We presented these results to the participants and asked open-ended questions regarding each scale (acceptability, appropriateness, feasibility). We focused on reasons for the results as well as suggestions for improvement; for example, “Is there anything that would increase its appropriateness from your perspective?”. The interview was digitally recorded and transcribed by a professional transcription service.
Data Analysis
Quantitative Analysis
Descriptive statistics, ie, percentages, median and interquartile range (difference between the 75th and 25th percentiles of the data), were calculated for each scale. Due to the non-normal data distribution, we did not calculate the mean. Missing data and the response option “no response” were excluded from the median and interquartile range calculations. Statistical analyses used SPSS Statistics, version 26.15
Qualitative Analysis
The first and last author analyzed the qualitative data (open-ended questions of the questionnaire and small group interviews) thematically. We chose an approach based on framework analysis,16 which allows a mixture of inductive and deductive approaches.17 In a first step, the three level 1 categories were deductively derived from the questionnaire: “Acceptability”, “Appropriateness” and “Feasibility”. Definitions of these can be found in Table 1. For the German definitions, we used the translation by Gutt et al.18
 |
Table 1 Definition of Acceptability, Appropriateness and Feasibility By Proctor et al11 |
In a second step, we analyzed the text passages assigned to level 1 inductively and formed ten subcategories (level 2). Then, we constructed a matrix, using cases for the rows and (sub)categories for the columns. Our four cases were: group interviews 1 and 2 and the hospital-internal and hospital-external participants of the online questionnaire. We wrote a summary in flow text for each subcategory and case. The contents of the cases per subcategory were compared and differences and similarities identified; then each subcategory and finally each main category was summarized as a whole and illustrated with quotations. We used the Nvivo qualitative data analysis software.19
Integration of Quantitative and Qualitative Data
As the final step, we used a mixed methods matrix to contrast the qualitative and quantitative results and to use the qualitative data to explain the quantitative. We constructed a matrix, using the three main categories “Acceptability”, “Appropriateness” and “Feasibility” for the rows and the corresponding qualitative and quantitative data for the columns. For the qualitative data, the overall summaries of the main categories in flow text were used, for the quantitative data, the results of the AIM, IAM and FIM questionnaire were used. The integration of qualitative and quantitative data was entered in another column in flow text and discussed within the research team.20
Ethics
This study followed the principles of good clinical practice and was approved by the governmental ethics committee (BASEC Nr. 2019–00797).21 All participants were informed in written and oral form about voluntary participation, anonymized analyses, data confidentiality, and publication of anonymized data. For participation in the interview and video recording we obtained oral consent for feasibility reasons during the pandemic. Participation in the online questionnaire was anonymous. The video recordings of the interviews were stored on a password-protected computer within the University Hospital Zurich and deleted after transcription. In the interview-transcripts, all person- and setting-related information was anonymized via pseudonyms.
Results
Participants
A total of nineteen HCP completed the online questionnaire (response rate: 70%). Of these, fifteen were hospital-internal HCP; the remaining four were external. For the group interviews, nine hospital-internal and no hospital-external HCP participated. Characteristics of the participating HCP for each case are listed in Table 2.
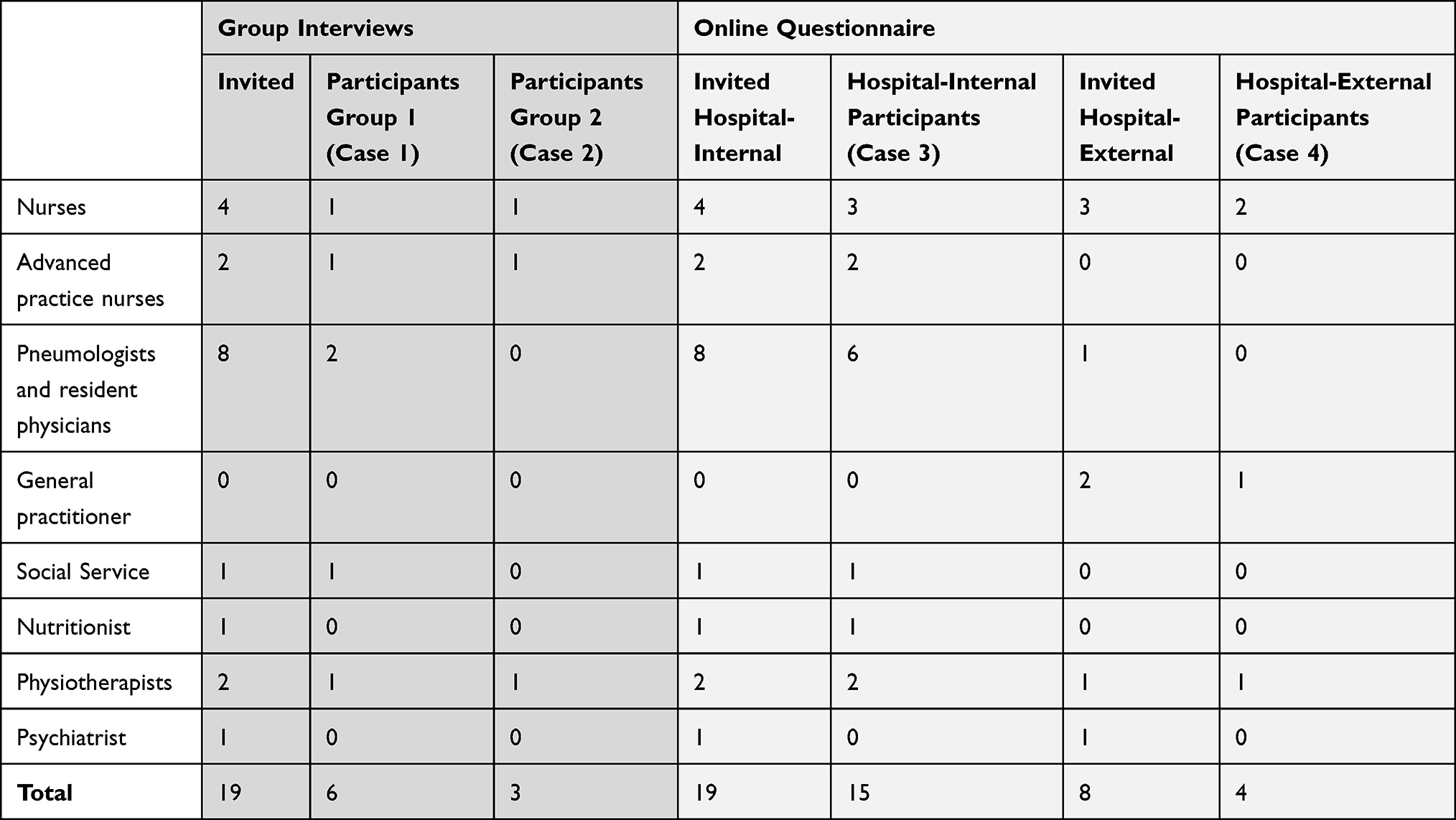 |
Table 2 Invited and Participating Healthcare Professionals of the Group interviews and the Online Questionnaire |
Quantitative Results
Of the nineteen participants, thirteen (68.4%) answered all 12 items (total missing values: 17 of 228 (7.5%)). The medians of the three scales ranged between “agree” (4; IAM and FIM) and “completely agree” (5; AIM). The interquartile ranges were between 0 (FIM) and 1 (AIM and IAM). Figure 2 shows the distribution of the three scales’ percentage of answers.
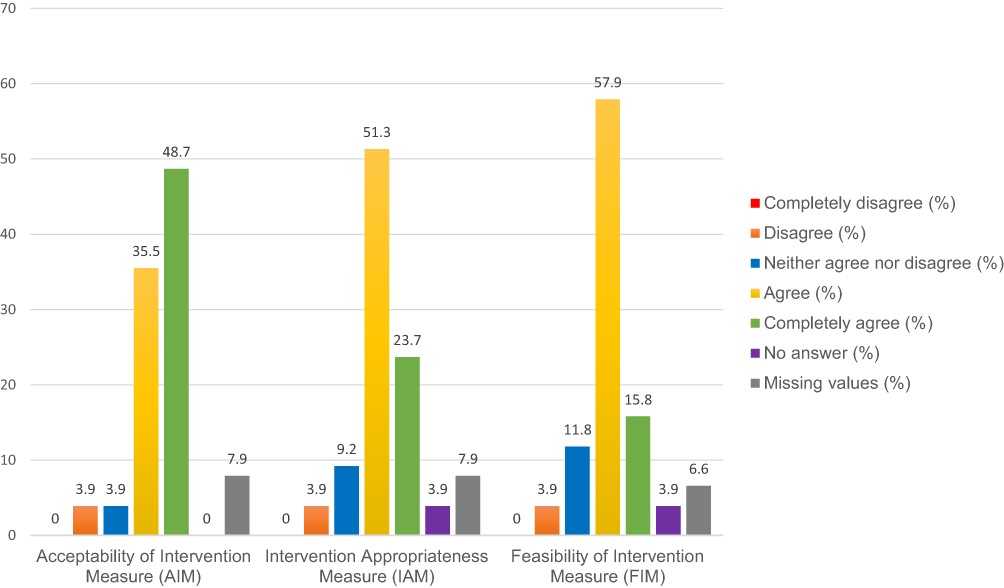 |
Figure 2 Results of the Aim, IAM and FIM (% of Answers per Scale). |
Qualitative Results
Across the three implementation outcomes (Level 1) our inductive analysis identified ten subcategories (Level 2). The resulting index is shown in Table 3. The contents of each subcategory are described in the following section.
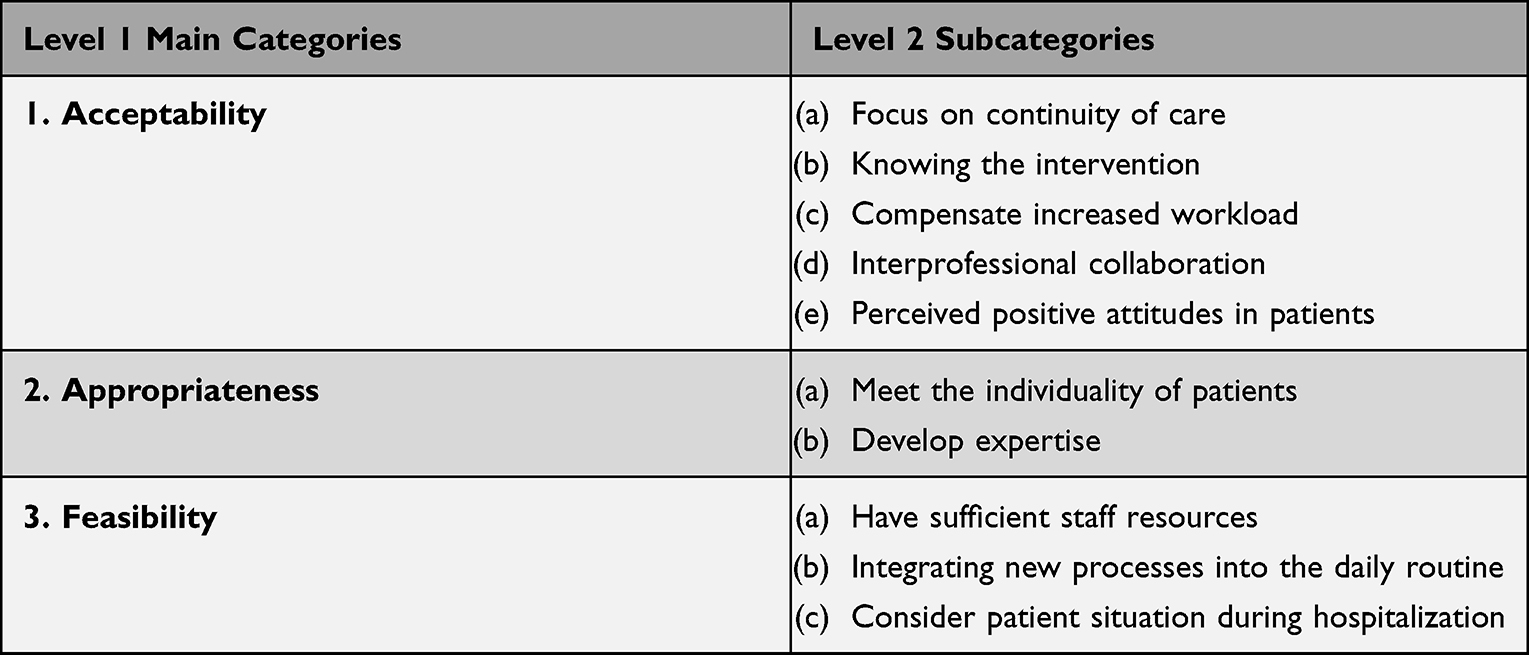 |
Table 3 Qualitative Index |
Acceptability
Focus on Continuity of Care
Acceptability of the NICCO intervention was enhanced by the unanimous agreement of the interprofessional team that it was beneficial regarding the care needs of patients with COPD by focusing on continuity of care.
That is the explanation for me why the acceptance is so high: Because the need is there and the intervention makes sense in relation to the clinical picture. (Physiotherapist)
However, the participants felt that the focus on the hospitalized patients—and therefore not on continuity of care beyond hospitalization—reduced the acceptance of resident physicians. Prejudicial attitudes, eg, towards the action plan or patient self-management, as well as a lack of trust in the APN team, were thought to be additional challenging factors.
Knowing the Intervention
Acceptability increased as the participants became familiar with the intervention, its benefits, and the associated tasks. Alongside an introduction about the background, structures and processes of the intervention, a knowledgeable permanent core team and clear, readily-available information on the intranet were supportive factors.
You’ve got enough information about it [the NICCO intervention]. And I can imagine that’s one reason why the acceptance is so high. (Ward Nurse)
Compensate Increased Workload
Acceptability was influenced by participants’ perceptions of the degree to which the additional workload required by the intervention was compensated for by additional staff resources—the APN team.
(…) The instruction of the inhalation technique that we do, we have already done before. The rest of the [additional nursing] work is actually done by the APN team. (Ward nurse)
Additional workload—primarily the administrative tasks—that was not compensated by the APN team, was seen as a burden, thereby affecting acceptance. Documentation templates were described as helpful to minimize time expenditure.
Interprofessional Collaboration
Acceptability of the intervention was related to how successful the interprofessional collaboration was, both within the clinic and among the outpatient services. Interprofessional communication and mutual trust were considered to be easier if people already worked together and the competences and contact persons were clearly defined. Divergent attitudes within the interprofessional team, eg, regarding self-administration of steroids and antibiotics by patients, were described as barriers to fruitful collaboration.
I find it very difficult to work with external pulmonologists. Because they may not have the same interest or commitment. (APN)
Perceived Positive Attitudes in Patients
Acceptability was increased when the HCP perceived that the patients had positive attitudes towards the intervention. The initial consultation with the APN-team was considered to be central for establishing trust between patient and the APN, which in turn supported sustainable behavioral change in everyday life. A possible negative influence on patients’ attitudes was seen in the fact that they were mostly hospitalized only for a short time, so they may feel overwhelmed by the volume of information they receive.
When it [the NICCO intervention] is offered, some [patients] are overwhelmed because it is a lot. (APN)
Appropriateness
Meet the Individuality of Patients
Appropriateness was influenced by the perceived adaptability of the intervention for the individual patient. The intervention was described as very complex, highly standardized with a tremendous amount of content that needs to be conveyed in a short time. As the intervention was new, flexibility regarding tailoring to patient situation was experienced as limited. Customizations were described as easier where a basis of trust existed between patient and APN team.
Difficult balancing act between adhering to the standardization and responding personally to the patient. (…) For me it often feels like a dilemma, because I want to satisfy both equally. (APN)
Develop Routine
Appropriateness was affected by the complexity of the training required to develop a routine in order to feel competent in the delivery of the intervention. Alongside continuity within the health care team, accumulated and previous experiences were described as advantageous. Staff absences and a lack of continuity among resident physicians were seen as complicating factors. During the COVID-19 pandemic, fewer patients were hospitalized with AECOPD, which in turn led to a lack of relevant experience.
Due to Corona there are also much fewer people with a COPD exacerbation. Because of that it is also more difficult to get a routine. (APN)
Feasibility
Have Sufficient Staff Resources
Feasibility of the intervention was positively related to existing staff resources— in particular, the additional APN team. In contrast, no additional resources were available in the medical service and the existing ones were already scarce.
If we don’t create more resources, and that also applies to the physicians, not just to the nursing staff, the project will simply fail from the medical side. (Pneumologist)
The COVID-19 pandemic depleted both personnel and time resources.Integrating New Processes into the Daily Routine
Feasibility was increased both by integrating new processes into the affected professional groups’ daily routines and by not significantly disrupting them. Integration was facilitated by staff continuity, as well as tools; eg, pocket-size cards containing outlines of important processes.
We have tried to solve this [lacking routine] with pocket cards that you have with you. You can work through them according to point. (Physiotherapist)
Consider Patient Situation During Hospitalization
Feasibility was related to the patient situation during hospitalization. It was described as helpful if newly hospitalized patients were referred early to the APN team, physiotherapy, and social services, as this gave time to carry out patient contacts at the hospital at convenient times and for an adequate duration. Delays occurred because physicians alone have the competence to prescribe these services. However, the patient’s condition did not always allow for a comprehensive intervention during hospitalization.
The question also arises: what condition do the patients come in? (…) One must not forget that the patient is very likely to first think about this: ‘How do I get more air’? (Physiotherapist)
Integration of Quantitative and Qualitative Results
Integrating the qualitative and quantitative results in a mixed method matrix led to broader insights regarding the three main categories, ie, acceptability, appropriateness, and feasibility.
Acceptability
Acceptability was particularly impaired by the additional workload and the lack of information about the NICCO intervention, according to the qualitative statements. This could explain the negative outliers in the quantitative data (“disagree”): these answers possibly came from person(s) who saw the additional effort as a burden or did not know sufficiently the intervention. In the interviews, the quantitative data’s largely positive assessment of acceptance reflected the participants’ recognition of two factors: the broad support the intervention received from both staff and patients, and strong interprofessional collaboration.
Appropriateness
The qualitative data indicated that the intervention’s lower rating of appropriateness could have resulted from the lack of routine, partly due to fewer hospitalized patients during the COVID-19 pandemic, which led to a lack of flexibility in adapting the intervention to individual patients. However, as the intervention considers every patient’s individuality, the overall appropriateness was assessed as high. One likely reason that some respondents could not quantitatively gauge appropriateness (“no answer”) is that those persons did not know the details of the intervention well enough to assess it.
Feasibility
Our qualitative data show that feasibility issues arose because, coupled with the intervention’s complexity, processes, interfaces, and competences were not always clear. As a result, necessary services were sometimes involved late, causing intervention delays during an already short hospital stay. Additionally, several factors may have led participants to consider the intervention difficult to apply. Most notably, at a time when personnel resources were scant, it required an introduction, time and mental work. In contrast, the APN team, whose resources were adequate and the processes generally familiar, assessed the feasibility as good. Also, several participants gave no rating for feasibility (“no answer”). This was likely due to their lack of active involvement in the process.
Discussion
In this study, we assessed the acceptability, appropriateness, and feasibility of a newly implemented, highly-standardized AECOPD hospital-ward-initiated intervention from the perspectives of the involved HCP. These considered the overall acceptability, appropriateness, and feasibility as high to very high. The explanatory sequential mixed method approach was particularly useful as it helped us to understand barriers and enablers affecting the new intervention’s implementation—information highly relevant to its adaptation and further implementation.
The overall acceptability of the NICCO intervention is very high: the need for the specialized care it provided patients with AECOP was undisputed among the participants. Our findings regarding how HCP attitudes and knowledge, resources, and professional collaboration affected acceptability are supported by the literature.22–27 The focus on continuity of care, which required a “mindset shift”, is also acknowledged.22,27–29 Negative attitudes toward the action plan or self-management by physicians—identified as barriers here—may stem from a lack of confidence in writing action plans or a fear of harming the patient. Such apprehensions may be based on study findings suggesting a link between comprehensive care management programs and increased mortality.29,30 It is also widely understood that an implementation’s success depends heavily on HCP knowing the intervention’s content and feeling confident in its implementation.22,24 However, the evaluation shows that the practical application is difficult, especially where the HCP lack continuity, which also necessitates repeated training. Regarding interprofessional collaboration, continuity of health personnel is also a key factor not only for reducing difficulty, but for building mutual trust and a professional relationship. In practice, however, successful collaboration is not always easily achievable, especially where resident physicians and hospital-external HCP change frequently. This finding is supported by the literature.22,24–26 A recently study from Switzerland evaluated the “Living well with COPD” program’s nationwide implementation by the Swiss Lung Association, concluding that the program was successfully implemented with high acceptability.23 In contrast to our study, that implementation took place in the outpatient setting. Further, recruitment was based on patient motivation and was not limited to patients with AECOPD. Our program’s inclusion of patients with high symptom burden, regardless of their levels of motivation or initiative, very likely also contributed to our addition of the outcome subcategory “Perceived positive attitudes in patients”. Patients’ attitudes thus had an influence on the acceptance of the HCP.
The NICCO intervention’s appropriateness is described as high, with room for improvement regarding its adaptability and the development of expertise. Wide variation in the needs of people with COPD makes it difficult to establish and evaluate a standardized intervention. Balancing standardization and individualization is demanding but highly relevant to a trustful and respectful patient-health-professional-relationship.7 Evidence strength and quality, adaptability and complexity are also typical intervention characteristics described in the Consolidated Framework for Implementation Research.31 The developers of the NICCO intervention aimed for high strength of evidence and transparency, therefore, the BCW guided the intervention development. Consequently, it was perceived as complex and challenging to adapt. We noted that both the HCP experience and expertise influenced the extent to which the intervention was individualized. The COVID-19 pandemic led to a reduction in patients hospitalized due to AECOPD in our clinic, thereby delaying the build-up of experience. Similar effects have been described in other countries.32,33
The feasibility of the NICCO intervention was also impacted by the pandemic, as it affected resources. Especially for the medical service, the already scarce personnel resources were further strained. This was a key barrier that required measures beyond the implementation of an APN team. Moreover, the patient’s condition, which is pivotal to the start of behavioral change, must also be considered. It is common for co-morbidities such as psychiatric illnesses to complicate the standardized implementation of a self-management intervention that relies on stable physical and psychological capacities.9,27
The literature on outcomes in implementation research continues to develop and recent publications describe acceptability, appropriateness, and feasibility as possible predictors or determinants of implementation, classified as “antecedent assessments” rather than as direct implementation outcomes.34,35 Our work is based on a different conceptualization, but can contribute to transparency in order to compare research results and to demonstrate the practical usefulness of existing instruments.36
Strengths and Limitations
To increase the quality of the data, indexing of the qualitative data was carried out independently by two persons and the results compared. Results of the analysis were validated with the cooperation of one to two selected members of each of the two interview groups. The interviews were conducted and the analysis reviewed by independent experts.
As a limitation, it must be mentioned that the translated instrument could not be validated psychometrically, as the quantitative dataset was too small. However, another German-speaking research group simultaneously translated the instrument used. They psychometrically tested it with teachers with good results in terms of reliability and validity.36 The comparison of the two German instruments resulted in seven items being identical and five items differing in terms of wording. Furthermore, the group interviews included neither resident physicians nor hospital-external HCP, as none could be recruited. This may have influenced the results, as their assumed position could only be obtained through third parties (eg, senior physicians). Considering the transferability of the intervention, it should be taken into account that this implementation outcomes evaluation is context-specific and would need to be repeated if expanded to another setting.31
Implications for Practice
Our results had several direct implications for the NICCO interventions design and delivery. Based on this evaluation, we will review the adaptability of our intervention and, especially, strengthen the focus on individualized patient’ goals. Furthermore, measures to reduce resident physicians’ workload in delivering the intervention – in particular administrative tasks – are planned. eg tailored introductions, templates for documentation, standardization of prescriptions, and delegation of defined interventions to the APN team. An interprofessional core team has been established to support continuity, practice routine, knowledge transfer and collaboration. Regarding intervention fidelity, semiannual interprofessional advisory board meetings – involving a patient - to discuss evaluation outcomes and possible adaptions to the intervention will be established. A lack of knowledge remained regarding the perspectives of resident physicians and hospital-external HCP. We address this need proactively, beginning with continuous assessment, utilize the online questionnaire used in this study.
Conclusion
This mixed method study, which addresses the acceptability, appropriateness, and feasibility of a newly implemented complex AECOPD intervention from the perspectives of the involved HCP, demonstrates the importance of an early stage implementation outcome evaluation. While the acceptance of the intervention was very high, the perceived appropriateness and feasibility were affected mainly due to high complexity, difficulties of adaptability and a lack of continuity of the HCP. Planned measures are an increased focus on patient goals and forming an interprofessional core team. With regard to implementation fidelity, regular repetition of the outcome evaluation and interprofessional discussions regarding possible measures are recommended.
Acknowledgments
We thank the hospital-internal and -external participants who completed the online questionnaire and group interviews for their valuable contributions. We also thank their respective superiors for enabling their participation.
We are also grateful our involved colleagues from the APN and Physiotherapy teams, Mieke Koletsos-Lamers, Adina Wehrle, Nicola Greco and Céline Aregger, for their support with recruitment and data collection.
From UH Zurich we owe many thanks to Annina Baltes-Wieser, Head of Nursing Division C, to Heidi Petry (PhD, RN), Head of the Centre of Clinical Nursing Science, to Malcolm Kohler (MD), Medical Co-Director of Primary Area 1 and Director of the Department of Pulmonology, to Gabi Brenner, Director of Nursing, to Christine Meier, Head of Physiotherapy/Occupational Therapy, and to Monika Anderegg, Head of the Pulmonology Ward, for their consistent, ongoing and energetic support of this project.
We thank Barbara Schwaninger for her transcription of the interviews and Chris Shultis for editing support.
Funding
This work was supported by a research grant from LUNGE ZUERICH, Switzerland.
Disclosure
Christian Clarenbach: received advisory fees from Roche, Novartis, Boehringer, GSK, Astra Zeneca, Sanofi, Vifor, OM Pharma, Grifols, Daiichi Sankyo and Mundipharma. Paul Chadwick: received speakers honoraria for talks delivered to Roche. The authors report no other conflicts of interest in this work.
References
1. Lenferink A, Brusse-Keizer M, van der Valk PD, et al. Self-management interventions including action plans for exacerbations versus usual care in patients with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2017;8:Cd011682.
2. Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease 2021 Report. Global Initiative for Chronic Obstructive Lung Disease; 2020.
3. Effing TW, Vercoulen JH, Bourbeau J, et al. Definition of a COPD self-management intervention: international expert group consensus. Eur Respir J. 2016;48(1):46–54. doi:10.1183/13993003.00025-2016
4. Poot CC, Meijer E, Kruis AL, Smidt N, Chavannes NH, Honkoop PJ. Integrated disease management interventions for patients with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2021;9. doi:10.1002/14651858.CD009437.pub3
5. Zwerink M, Brusse-Keizer M, van der Valk PD, et al. Self management for patients with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2014. doi:10.1002/14651858.CD002990.pub3
6. Long H, Howells K, Peters S, Blakemore A. Does health coaching improve health-related quality of life and reduce hospital admissions in people with chronic obstructive pulmonary disease? A systematic review and meta-analysis. Br J Health Psychol. 2019;24(3):515–546. doi:10.1111/bjhp.12366
7. Schmid-Mohler G, Clarenbach C, Brenner G, et al. Advanced nursing practice in COPD exacerbations: the solution for a gap in Switzerland? Eur Respir J. 2020;6(2). doi:10.1183/23120541.00354-2019
8. Markun S, Franzen DP, Dalla Lana K, et al. Acute exacerbated COPD: room for improvement in key elements of care. Int J Chron Obstruct Pulmon Dis. 2017;12:2969–2975. doi:10.2147/COPD.S145496
9. Schmid-Mohler G, Hübsch C, Greco N, et al. Supporting behavior change after AECOPD – development of a hospital-initiated intervention using the behavior change wheel. Int J Chron Obstruct Pulmon Dis. 2022;17:1651–1669. doi:10.2147/COPD.S358426
10. Michie S, Atkins L, West R. Behaviour Change Wheel - a Guide to Designing Interventions. Silverback Publishing; 2014.
11. Proctor E, Silmere H, Raghavan R, et al. Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Adm Policy Ment Health Ment. 2011;38(2):65–76. doi:10.1007/s10488-010-0319-7
12. Weiner BJ, Lewis CC, Stanick C, et al. Psychometric assessment of three newly developed implementation outcome measures. Implement Sci. 2017;12(108). doi:10.1186/s13012-017-0635-3
13. Creswell JW. A Concise Introduction to Mixed Methods Research. SAGE Publications; 2014.
14. Wild D, Grove A, Martin M, et al. Principles of good practice for the translation and cultural adaptation process for patient‐reported outcomes (PRO) measures: report of the ISPOR task force for translation and cultural adaptation. Value Health. 2005;8(2):94–104. doi:10.1111/j.1524-4733.2005.04054.x
15. IBM Corp. IBM SPSS Statistics for Windows, Version 25.0. IBM Corp; 2017.
16. Ritchie J, Spencer L, O’ Connor W. Carrying Out Qualitative Analysis. In: Ritchie J, Lewis J, editors. Qualitative Research Practice: A Guide for Social Science Students and Researchers. SAGE; 2003:219–262.
17. Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. 2013;13(117). doi:10.1186/1471-2288-13-117
18. Gutt A-K, Hoben M, Roes M, Willmeroth T, Wesselborg B, Kuske S. Systematische Übersetzung und Cross-Validierung definierter Implementierungsoutcomes der Gesundheitsversorgung. Z Evid Fortbild Qual Gesundhwes. 2018;135–136:72–80. doi:10.1016/j.zefq.2018.06.005
19. QSR International Pty Ltd. NVivo Pro Qualitative Data Analysis Software, Version 12. QSR International Pty Ltd; 2018.
20. O’Cathain A, Murphy E, Nicholl J. Three techniques for integrating data in mixed methods studies. Br Med J. 2010;341(7783):1147–1150.
21. International Council for Harmonisation (ICH). Guideline for good clinical practice E6 (R2); 2016. Available from: https://www.ema.europa.eu/en/ich-e6-r2-good-clinical-practice.
22. Davy C, Bleasel J, Liu H, Tchan M, Ponniah S, Brown A. Factors influencing the implementation of chronic care models: a systematic literature review. BMC Fam Pract. 2015;16(102). doi:10.1186/s12875-015-0319-5
23. Strassmann A, Guler M, Steurer-Stey C, et al. Nationwide implementation of the self-management program “Living well with COPD”: process and effectiveness evaluation using a mixed-methods approach. Patient Educ Couns. 2021;105(3):670–678. doi:10.1016/j.pec.2021.06.018
24. Carron T, Bridevaux P-O, Lörvall K, et al. Feasibility, acceptability and effectiveness of integrated care for COPD patients: a mixed methods evaluation of a pilot community-based programme. Swiss Med Wkly. 2017;147:w14567. doi:10.4414/smw.2017.14567
25. Cochrane B, Foster J, Boyd R, Atlantis E. Implementation challenges in delivering team-based care (‘TEAMcare’) for patients with chronic obstructive pulmonary disease in a public hospital setting: a mixed methods approach. BMC Health Serv Res. 2016;16(347). doi:10.1186/s12913-016-1592-2
26. Dennis S, Reddel HK, Middleton S, et al. Barriers and outcomes of an evidence-based approach to diagnosis and management of chronic obstructive pulmonary disease (COPD) in Australia: a qualitative study. Fam Pract. 2017;34(4):485–490. doi:10.1093/fampra/cmw103
27. Brook J, McGraw C. Multidisciplinary perspectives: application of the consolidated framework for implementation research to evaluate a health coaching initiative. Health Soc Care Community. 2018;26(3):e386–e395. doi:10.1111/hsc.12536
28. Newman P, Varnam R, McDowell A. Health coaching with long-term conditions. Pract Nurs. 2013;24(7):344–346. doi:10.12968/pnur.2013.24.7.344
29. Roberts NJ, Younis I, Kidd L, Partridge MR. Barriers to the implementation of self management support in long term lung conditions. Lond J Prim Care. 2013;5(1):35–47. doi:10.1080/17571472.2013.11493370
30. Fan VS, Gaziano JM, Lew R, et al. A comprehensive care management program to prevent chronic obstructive pulmonary disease hospitalizations: a randomized, controlled trial. Ann Intern Med. 2012;156(10):673–683. doi:10.7326/0003-4819-156-10-201205150-00003
31. Damschroder LJ, David CA, Rosalind EK, Susan RK, Jeffery AA, Julie CL. Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implement Sci. 2009;50:4.
32. Lawless M, Burgess M, Bourke S. Impact of COVID-19 on hospital admissions for COPD exacerbation: lessons for future care. Medicina. 2022;58(66):66. doi:10.3390/medicina58010066
33. Farrugia Y, Spiteri MBP, Grech N, et al. The impact of COVID-19 on hospitalised COPD exacerbations in Malta. Pulm Med. 2021;2021:1–7. doi:10.1155/2021/5533123
34. Damschroder LJ, Reardon CM, Opra Widerquist MA, Lowery J. Conceptualizing outcomes for use with the consolidated framework for implementation research (CFIR): the CFIR outcomes addendum. Implement Sci. 2022;17(1). doi:10.1186/s13012-021-01181-5
35. Reilly KL, Kennedy S, Porter G, Estabrooks P. Comparing, contrasting, and integrating dissemination and implementation outcomes included in the RE-AIM and implementation outcomes frameworks. Front Public Health. 2020;8:430.
36. Kien C, Griebler U, Schultes MT, Thaler KJ, Stamm T. Psychometric testing of the German versions of three implementation outcome measures. Glob Implement Res Appl. 2021;1(1):183–194. doi:10.1007/s43477-021-00019-y
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevention of Re-Hospitalization for Acute Exacerbations: Perspectives of People with Chronic Obstructive Pulmonary Disease: A Qualitative Study
Hobman A, Levack WMM, Jones B, Ingham TR, Fingleton J, Weatherall M, McNaughton AA, McNaughton HK
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:207-218
Published Date: 2 March 2023
Taking Charge After Acute Exacerbation of Chronic Obstructive Pulmonary Disease: A Randomized Controlled Feasibility Trial of a Psychologically Informed Self-Management Intervention
Levack WMM, Weatherall M, McNaughton HK, McNaughton AA, Hobman A, Jones B, Ingham TR, Fingleton J
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:317-325
Published Date: 15 March 2023
Long-Term Usage and Improved Clinical Outcomes with Adoption of a COPD Digital Support Service: Key Findings from the RECEIVER Trial
Taylor A, Cushing A, Dow M, Anderson J, McDowell G, Lua S, Manthe M, Padmanabhan S, Burns S, McGinness P, Lowe DJ, Carlin C
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1301-1318
Published Date: 22 June 2023
Effects of Adherence to an mHealth Tool for Self-Management of COPD Exacerbations
Bischoff EW, Ariens N, Boer L, Vercoulen J, Akkermans RP, van den Bemt L, Schermer TR
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2381-2389
Published Date: 1 November 2023
Shifting Responsibilities: Developing a Pan-European Service Model for an eHealth Technology Supporting Self-Management of People with Chronic Obstructive Pulmonary Disease and Comorbidities
te Braake E, Grünloh C, Tabak M
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:175-192
Published Date: 17 January 2024