Back to Journals » International Journal of General Medicine » Volume 17
ABO Blood Type and Pretreatment Systemic Inflammatory Response Index Associated with Lymph Node Metastasis in Patients with Breast Cancer
Received 13 July 2024
Accepted for publication 16 October 2024
Published 23 October 2024 Volume 2024:17 Pages 4823—4833
DOI https://doi.org/10.2147/IJGM.S486873
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Kenneth Adler
Nating Xiong,1 Wendao Han,1 Zhikang Yu2,3
1Department of Blood Transfusion, Meizhou People’s Hospital, Meizhou Academy of Medical Sciences, Meizhou, People’s Republic of China; 2Institute of Basic Medical Sciences, Meizhou People’s Hospital, Meizhou Academy of Medical Sciences, Meizhou, People’s Republic of China; 3Guangdong Engineering Technological Research Center of Clinical Molecular Diagnosis and Antibody Drugs, Meizhou People’s Hospital, Meizhou Academy of Medical Sciences, Meizhou, People’s Republic of China
Correspondence: Zhikang Yu, Institute of Basic Medical Sciences, Meizhou People’s Hospital, Meizhou Academy of Medical Sciences, Meizhou, People’s Republic of China, Email [email protected]
Background: Lymph node metastasis (LNM) is an important prognostic factor for breast cancer. Inflammatory stimulation can change tumor microenvironment and lead to LNM, but the relationship between LNM and peripheral immunoinflammatory indices has not been clarified in breast cancer.
Methods: The clinical information of 1918 patients with breast cancer admitted to Meizhou People’s Hospital from October 2017 to December 2023 were retrospectively analyzed. The relationship of clinicopathological features (age, body mass index (BMI), ABO blood types, family history of cancer, tumor site, disease stage, LNM, distant metastasis, and molecular subtypes) and peripheral immunoinflammatory indices (pan-immune inflammation value (PIV), systemic immune inflammation index (SII), and system inflammation response index (SIRI)) were analyzed.
Results: There were 935 (48.7%) patients had no LNM and 983 (51.3%) had LNM. There were statistically significant differences in the distributions of ABO blood groups (p=0.022) and molecular subtypes (p< 0.001) between the two groups. PIV, SII, and SIRI levels in patients with LNM were significantly higher than those without LNM (all p< 0.05). The proportions of LNM in patients with high PIV, SII, and SIRI levels were higher than those with low PIV, SII, and SIRI levels, respectively. Logistic regression analysis showed that non-O blood type (non-O blood type vs O blood type, odds ratio (OR): 1.327, 95% confidence interval (CI): 1.056– 1.667, p=0.015), luminal B subtype (luminal B vs luminal A, OR: 2.939, 95% CI: 2.147– 4.022, p< 0.001), HER2+ subtype (HER2+ vs luminal A, OR: 2.044, 95% CI: 1.388– 3.009, p< 0.001), and high SIRI level (≥ 0.875 vs < 0.875, OR: 1.572, 95% CI: 1.092– 2.265, p=0.015) were independently associated with LNM.
Conclusion: Non-O blood type, luminal B and HER2+ subtypes, and high SIRI level (≥ 0.875) have potential role in predicting the status of LNM in breast cancer patients.
Keywords: breast cancer, lymph node metastasis, system inflammation response index, ABO blood group
Introduction
Breast cancer is a kind of malignant tumor which occurs in the epithelial tissue of the breast and has a high incidence in women.1 According to statistics released in 2020, the global incidence of breast cancer is 11.7%, and it has become the highest incidence of malignant tumors in the world.2 Breast cancer is classified into four molecular subgroups: luminal A, luminal B, human epidermal growth factor receptor 2 (HER2) enriched (HER2+), and triple negative breast cancer (TNBC), based on the expression of hormone receptors (HR) (including estrogen receptor (ER) and progesterone receptor (PR)), HER2, and Ki67 (a proliferation index marker) in the patient’s cancer tissue.3 Different molecular subtypes of breast cancer have relatively unique clinicopathological features and different prognoses.4,5
Patients with metastatic breast cancer have a poorer prognosis, and the most common site of breast cancer spread is the local lymph nodes.6,7 Lymph node metastasis (LNM) is an important prognostic factor for breast cancer patients.8 Cancer metastasis refers to the process by which primary tumor cells spread to other parts of the body.9 Cancer metastasis involves a continuous physiological process, including the invasion of cancer cells through the extracellular matrix (ECM), entry into the circulation (endosis), survival in the blood circulation or lymphatic system, dissemination to distant tissues, and finally colonization and growth into secondary tumors.10 Breast cancer is a highly heterogeneous disease where even similar clinical and pathological features can lead to different outcomes. Risk assessment of LNM in breast cancer requires comprehensive consideration.
Cancer related inflammation (CRI) changes the tumor microenvironment, which is closely related to the occurrence and development of tumors.11,12 Inflammatory cells in the body include neutrophils, lymphocytes, monocytes, and platelets. Activated neutrophils can release reactive oxygen species (ROS) and induce tissue oxidative damage, and change tumor microenvironment, and further promote cell differentiation and tumor cell growth and reproduction.13,14 Lymphocytes can activate the adaptive immune response and play a role in inhibiting the tumor growth process.15 Tumor-associated macrophages (TAMs) stimulate angiogenesis, tumor cell invasion and extravasation by secreting cytokines.16,17 The imbalance of the proportion of inflammatory cells in these local tumor microenvironments ultimately leads to the disharmony between the tumor-promoting and tumor-inhibiting effects, leading to the occurrence and progression of tumors.
Pan-immune inflammation value (PIV), systemic immune inflammation index (SII), and system inflammation response index (SIRI) are several comprehensive immunoinflammatory biomarkers based on complete blood counts.18–21 PIV, SII, and SIRI represent the balance between various immune cells, reflecting the restrictive relationship between pro-tumor inflammation and anti-tumor immune response, and can judge the relationship between the immune system and tumor development. Several researches showed that high SII22–24 and high PIV24 were associated with an increased risk for LNM in breast cancer patients. In addition, breast cancer patients with low SIRI or PIV levels had significantly better overall survival than those with high SIRI or PIV levels.25 Another study showed that SIRI was also associated with the efficacy of neoadjuvant therapy in breast cancer patients.26 However, the relationship between PIV, SII, and SIRI levels and LNM in patients with breast cancer CRC has not been clarified completely. The purpose of this study was to evaluate this relationship. It should provide additional valuable reference data for diagnosis and treatment options for breast cancer patients.
Materials and Methods
Participants
It was a cross-sectional analytical study with a total of 1918 breast cancer patients who were hospitalized in Meizhou People’s Hospital, between October 2017 and December 2023. The inclusion criteria of the study as follows: (1) patients with histopathologically confirmed breast cancer; (2) no radiotherapy or chemotherapy was given before surgery; (3) clinicopathological data and preoperative blood routine data were complete. The exclusion criteria as follows: (1) breast cancer patients with other tumors; (2) breast cancer patients with severe organ dysfunction, severe infectious disease, and autoimmune disease; (3) clinical records were incomplete. This study was supported by the Ethics Committee of the Meizhou People’s Hospital.
Data Collection
Clinicopathological features of the patients were collected from the medical records system of our hospital, including age, body mass index (BMI), ABO blood types, family history of cancer, tumor site (left breast, right breast, bilateral), disease stage, LNM, distant metastasis, molecular subtypes, and pretreatment peripheral inflammatory indices levels. Blood routine test data were collected before treatment. The patient’s venous blood was collected, blood cell analysis was tested by Sysmex XE-2100 hematology analyzer (Sysmex Corporation, Japan) according to standard operating procedures (SOP). In this study, patients were divided into two groups according to age: ≥55 years old and <55 years old. BMI was divided into three subgroups based on the Chinese criteria:27,28 <18.5 kg/m2, 18.5–23.9 kg/m2, and ≥24.0 kg/m2.
Data Processing and Statistical Analysis
The inflammation index PIV, SII, and SIRI were calculated according to the following formula:
PIV=monocyte×neutrophil×platelet/lymphocyte;
SII=platelet×neutrophil/lymphocyte;
SIRI=monocyte×neutrophil/lymphocyte.
SPSS statistical software version 26.0 (IBM Inc., USA) was used for data analysis. The patients’ clinicopathological features were summarized with descriptive statistics. Categorical variables were compared using χ2 test and Fisher’s exact test. Receiver operating characteristic (ROC) curve analysis was used to determine the optimal cutoff values of PIV, SII, and SIRI to distinguish LNM. Association between LNM and the clinicopathological features, PIV, SII, and SIRI levels was evaluated by Fisher’s exact test. Age, BMI, ABO blood types, family history of cancer, laterality of breast cancer, molecular subtypes, and levels of PIV, SII, and SIRI were selected as covariates in the multivariate logistic regression analysis for LNM, based on estimating the odds ratios (OR) and their 95% confidence intervals (CIs). p<0.05 was considered statistically significant.
Results
Clinicopathological Features of the Breast Cancer Patients
Among 1918 breast cancer patients included in this study, 1153 (60.1%) patients were younger than 55 years old and 765 (39.9%) cases with aged ≥55 years old. There were 121 (6.3%), 827 (43.1%), and 970 (50.6%) cases with BMI < 18.5 kg/m2, 18.5–23.9 kg/m2, and ≥24.0 kg/m2, respectively. There were 584 (30.4%), 440 (22.9%), 120 (6.3%), and 774 (40.4%) cases with A, B, AB, and O blood type, respectively. The proportion of patients with family history of cancer, III-IV stage, LNM, and distant metastasis was 8.6% (165/1918), 29.6% (568/1918), 51.3% (983/1918), and 8.1% (155/1918), respectively. The number of luminal A, luminal B, HER2+, and TNBC patients was 236 (12.3%), 642 (33.5%), 206 (10.7%), and 238 (12.4%), respectively. The level of PIV, SII, and SIRI in these patients was 206.25 (131.94, 330.38), 530.70 (384.39, 783.03), and 0.82 (0.57, 1.24), respectively (Table 1).
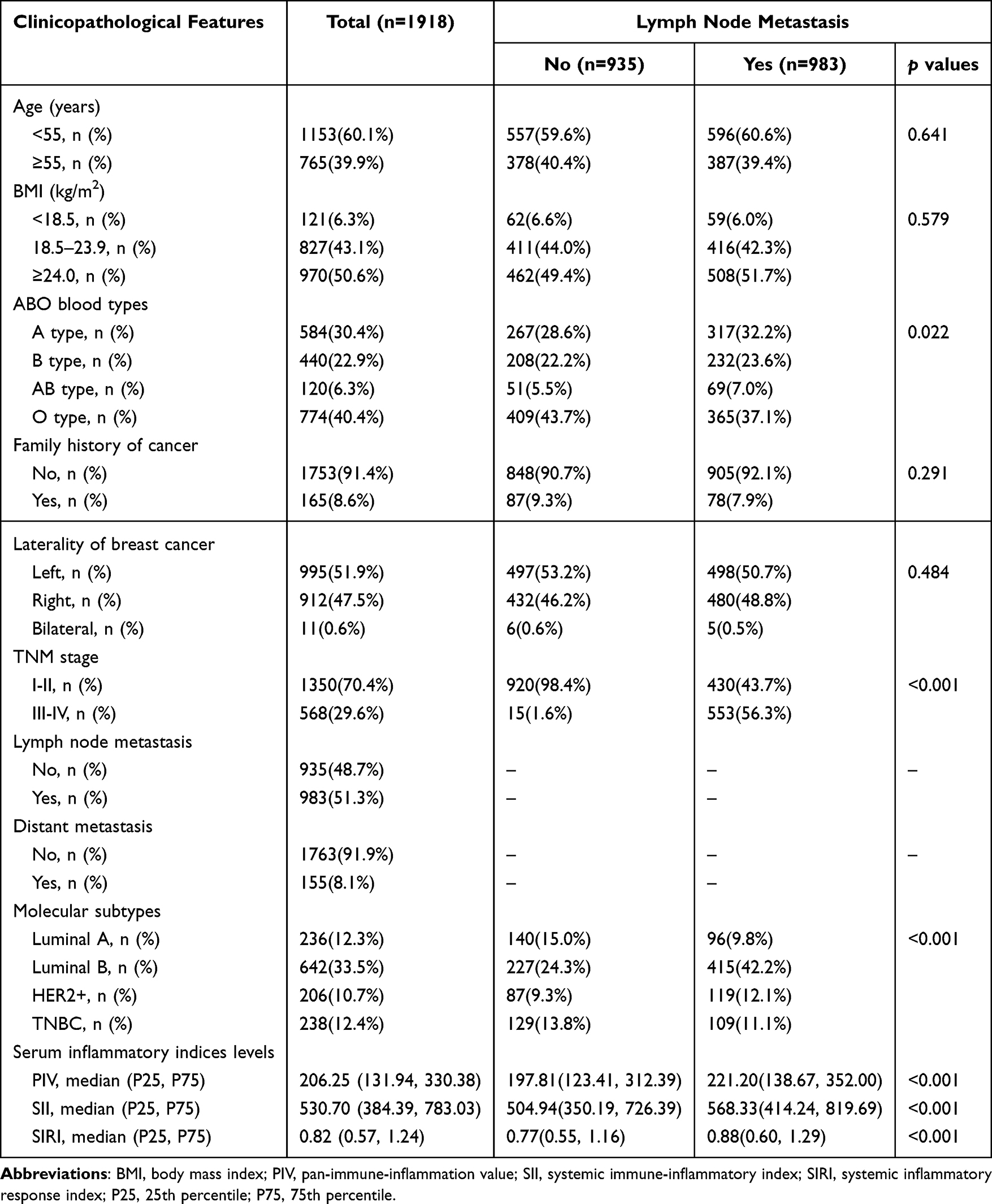 |
Table 1 The Clinicopathological Features of All Patients and Comparison of Clinicopathological Features Among Breast Cancer Patients with or Without Lymph Node Metastasis |
Comparison of Clinicopathological Features Among Breast Cancer Patients with or Without LNM
In this study, 935 (48.7%) patients had no LNM and 983 (51.3%) patients with LNM. The proportion of O blood type in patients with LNM was lower than those without LNM (37.1% vs 43.7%, p=0.022). The proportions of luminal B subtype (42.2% vs 24.3%) and HER2+ subtype (12.1% vs 9.3%) in patients with LNM were higher than those without LNM (p<0.001). The levels of PIV (221.20 (138.67, 352.00) vs 197.81 (123.41, 312.39)), SII (568.33 (414.24, 819.69) vs 504.94 (350.19, 726.39)), and SIRI (0.88 (0.60, 1.29) vs 0.77 (0.55, 1.16)) in patients with LNM were significantly higher than those in patients without LNM (all p<0.05). There was no statistically significant difference in distributions of age (p=0.641), BMI (p=0.579), and laterality of breast cancer (p=0.484), and proportion of family history of cancer (p=0.291) those with and without LNM (Table 1).
Clinicopathological Characteristics Were Compared According to the Different Levels of PIV, SII, and SIRI
ROC curve analysis was used to determine the optimal cutoff values of PIV, SII, and SIRI to distinguish LNM. When LNM was considered as the endpoint of PIV, SII, and SIRI, the cut-off value of PIV was 221.19 (sensitivity 50.1%, specificity 58.2%, area under the ROC curve (AUC)=0.548), the cut-off value of SII was 542.74 (sensitivity 53.2%, specificity 57.0%, AUC = 0.566), and the cut-off value of SIRI was 0.875 (sensitivity 50.6%, specificity 59.5%, AUC = 0.548) (Figure 1).
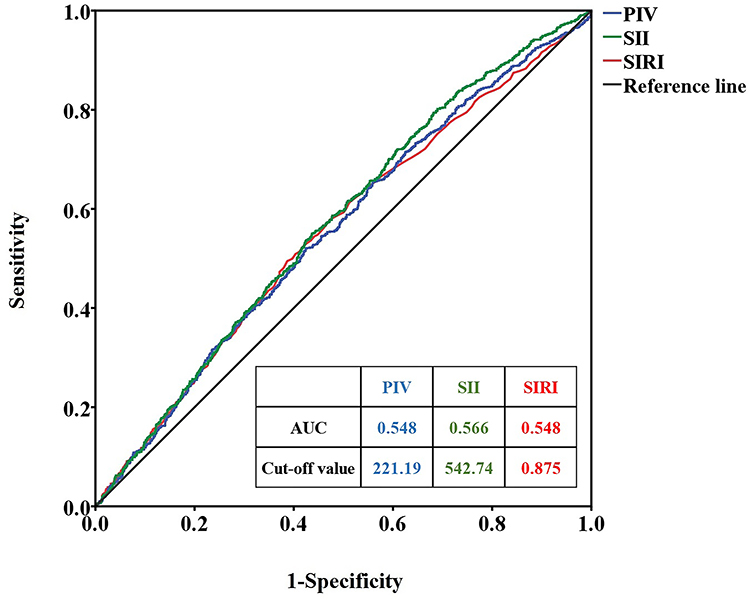 |
Figure 1 The ROC curve of PIV, SII, and SIRI based on LNM. Abbreviations: PIV, pan-immune-inflammation value; SII, systemic immune-inflammatory index; SIRI, systemic inflammatory response index; LNM, lymph node metastasis. |
The proportion of aged <55 years old, and distant metastasis in patients with PIV ≥ 221.19, SII ≥ 542.74, and SIRI ≥ 0.875 was higher than those in patients with PIV < 221.19, SII < 542.74, and SIRI < 0.875, respectively (all p<0.05). The proportion of O blood type in patients with PIV ≥ 221.19 was higher than those with PIV < 221.19 (43.5% vs 37.7%, p=0.010), and in patients with SIRI ≥ 0.875 was higher than those with SIRI < 0.875 (43.3% vs 37.9%, p=0.019). The proportion of LNM in patients with PIV ≥ 221.19 was higher than those with PIV < 221.19 (55.7% vs 47.4%, p<0.001), in patients with SII ≥ 542.74 was higher than those with SII < 542.74 (56.5% vs 46.3%, p<0.001), and in patients with SIRI ≥ 0.875 was higher than those with SIRI < 0.875 (56.7% vs 46.6%, p<0.001). There were statistically significant differences in the distributions of molecular subtypes of breast cancer among different levels of PIV (p=0.003), and SIRI (p=0.010). There was no significant difference in the distributions of BMI and laterality of breast cancer, and the proportion of family history of cancer among different levels of PIV, SII, and SIRI (all p>0.05) (Table 2).
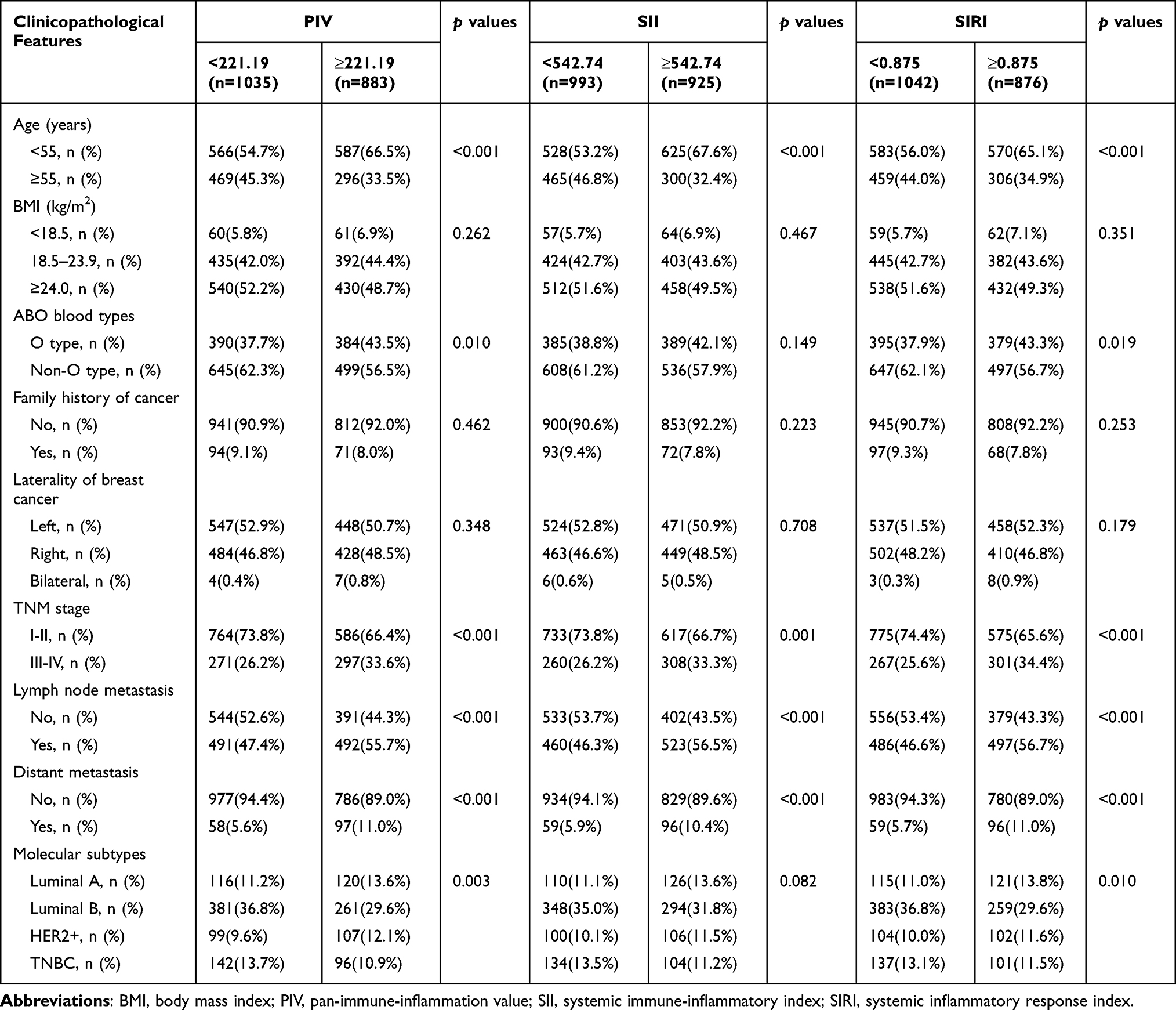 |
Table 2 Clinicopathological Characteristics Were Compared According to the Different Levels of PIV, SII, and SIRI in Breast Cancer Patients |
Logistic Regression Analysis of the Relationship Between LNM and Clinicopathological Characteristics
The results of univariate analysis showed that non-O blood type (non-O blood type vs O blood type, odds ratio (OR): 1.317, 95% confidence interval (CI): 1.097–1.581, p=0.003), luminal B subtype (luminal B vs luminal A, OR: 2.666, 95% CI: 1.963–3.621, p<0.001), HER2+ subtype (HER2+ vs luminal A, OR: 1.995, 95% CI: 1.365–2.915, p<0.001), high PIV level (≥221.19 vs <221.19, OR: 1.394, 95% CI: 1.164–1.670, p<0.001), high SII level (≥542.74 vs <542.74, OR: 1.507, 95% CI: 1.259–1.805, p<0.001), and high SIRI level (≥0.875 vs <0.875, OR: 1.500, 95% CI: 1.252–1.797, p<0.001) were significantly associated with LNM in breast cancer patients. Multivariate regression logistic analysis showed that non-O blood type (non-O blood type vs O blood type, OR: 1.327, 95% CI: 1.056–1.667, p=0.015), luminal B subtype (luminal B vs luminal A, OR: 2.939, 95% CI: 2.147–4.022, p<0.001), HER2+ subtype (HER2+ vs luminal A, OR: 2.044, 95% CI: 1.388–3.009, p<0.001), and high SIRI level (≥0.875 vs <0.875, OR: 1.572, 95% CI: 1.092–2.265, p=0.015) were independently associated with LNM in breast cancer patients. In other words, breast cancer patients with SIRI ≥ 0.875 were more than 1.5 times more likely to develop LNM than those SIRI < 0.875 (Table 3).
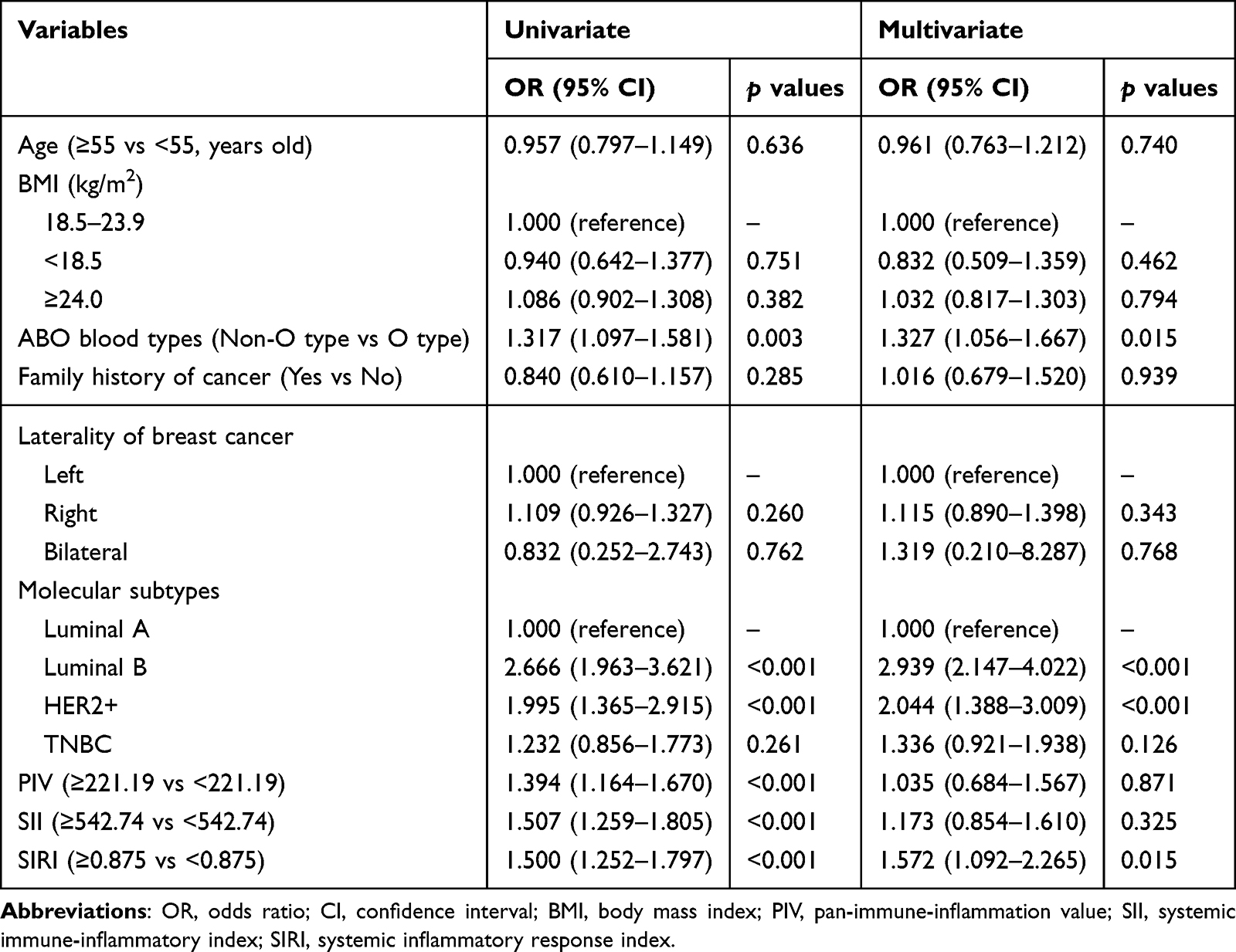 |
Table 3 Logistic Regression Analysis of the Relationship Between Lymph Node Metastasis and Clinicopathological Characteristics in Breast Cancer Patients |
Discussion
LNM of breast cancer predicts poor prognosis, and its clinical significance is even more important than the size of the primary tumor.29 Lymph reflux in breast cancer mainly flows to axillary lymph nodes, and axillary lymph node dissection (ALND) is the main treatment for axillary lymph nodes, but ALND can bring long-term complications, such as lymphedema, upper limb paresthesia, and shoulder joint movement disorders.30 In patients with negative axillary lymph nodes, ALND does not provide a corresponding benefit.31 Sentinel lymph node biopsy (SLNB) has become the surgical method for axillary lymph node management instead of ALND.32 For patients with positive sentinel lymph node (SLN) confirmed by pathology, it is considered necessary to perform ALND.33 In this study, high SIRI level (≥0.875), non-O blood type, luminal B and HER2+ subtypes were independently associated with LNM in breast cancer.
In this study, high SIRI level (≥0.875) was an independent risk factor for LNM in breast cancer patients. Several studies had found that breast cancer patients with high SIRI level had relatively shorter disease-free survival (DFS)34–36 and overall survival (OS)34–37 than patients with low SIRI level. Breast cancer patients with high pretreatment SIRI level had significantly lower pathological complete response (pCR) rate after neoadjuvant chemotherapy (NAC) than patients with low SIRI levels.38 In this study, SIRI was confirmed to be a predictor of LNM in breast cancer. In addition, several researches showed that high SII index was associated with an increased risk for LNM in patients breast cancer.22–24 Tong et al found that high levels of PIV, and SII were the risk factors of LNM in breast cancer.24 However, the results of this study did not confirm a significant relationship between PIV, SII and LNM in breast cancer.
Moreover, patients with luminal B and HER2+ subtypes of breast cancer were more likely to have LNM in present study. Some studies showed that LNM is more common in patients with luminal B subtype breast cancer,39,40 and HER2+ subtype breast cancer.41 Min SK et al found that patients with luminal type breast cancer had a higher rate of LNM than non-luminal type patients.42 In addition, a study has found that TNBC patients have the least possibility of LNM.43 It may be related to the differences in the expression levels of ER, PR, HER2, and Ki67 on tumor cells. However, TNBC patients have a poor prognosis and a higher local recurrence rate than other types of breast cancer.44,45 The differences between these features in different molecular subtypes may be due to differences in immune cells, tumor-associated macrophages, and cancer-associated fibroblasts in the breast cancer tumor microenvironment of different molecular subtypes.46 Some studies have shown that there is no significant difference in LNM among different molecular types.47
In addition, non-O blood type was independently associated with LNM in breast cancer patients in this study. There were relatively few studies on the relationship of ABO blood types and LNM in breast cancer. Serkan Akin et al found that there was no significant difference in LNM among breast cancer patients with different ABO blood types.48 A study from Morocco found that A and AB blood types were associated with a higher incidence of LNM in breast cancer.49 Moreover, several studies had found that A blood type is associated with a high risk of breast cancer.50–53 In addition, some studies have linked ABO blood type to the prognosis of breast cancer.54,55 But there were other studies that have found no association between ABO blood group and the risk,56,57 and the prognosis58 of breast cancer. ABO blood group is considered to be the most important blood group in the human blood group system.59 In addition to the expression of ABO group antigen A and B antigens on red blood cells, these antigens are also highly expressed on the surface of other human cells and tissues, including epithelial cells and vascular endothelial cells.60,61 The expression of A and B antigens is associated with increased cell motility, and A antigen is associated with resistance to apoptosis, promotion of tumorigenesis and metastasis and spread in the rat model.62,63 They may also be involved in intercellular adhesion and cell membrane signaling processes as well as immune responses to the host.64,65
This study provides evidence of non-O blood type, luminal B and HER2+ subtypes, and high SIRI level (≥0.875) were independently associated with LNM in breast cancer patients. It provides valuable reference information for LNM risk prediction of breast cancer. However, the study has some limitations that are worth noting. First, as a retrospective study, our hypothesis needs to be verified with prospective longitudinal studies. Second, this study did not follow-up breast cancer patients, and did not analyze the relationship between the levels of pretreatment immunoinflammatory indices and clinical prognosis. Third, this study is a single-center study and lacks external data for verification. Therefore, if a multi-center, prospective study can be conducted and follow-up is conducted, the results obtained will be more clinically valuable.
Conclusions
Summary, non-O blood type, luminal B and HER2+ subtypes, and high SIRI level (≥0.875) have potential role in predicting the status of LNM in breast cancer patients. The prediction of LNM risk based on the above factors can provide valuable reference information for clinical diagnosis and prognosis assessment.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval
All participants were informed on the study procedures and goals and the informed consent from all the participants was obtained. The study was performed under the guidance of the Declaration of Helsinki and approved by the Ethics Committee of Medicine, Meizhou People’s Hospital.
Acknowledgments
The authors thank their colleagues, who were not listed in the authorship of the Department of Blood Transfusion, Department of Breast Surgery, and Department of Medical Oncology, Meizhou People’s Hospital, for their helpful comments on the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Cultivation Project of Scientific Research in Meizhou People’s Hospital (Grant No.: PY-C2020031, and PY-C2020033), and the Guangdong Basic and Applied Basic Research Foundation (2021A1515220106).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Liang Y, Zhang H, Song X, Yang Q. Metastatic heterogeneity of breast cancer: molecular mechanism and potential therapeutic targets. Semin Cancer Biol. 2020;60:14–27. doi:10.1016/j.semcancer.2019.08.012
2. Sung H, Ferlay J, Siegel RL. Global cancer statistics 2020: globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
3. Liu QQ, Sun HF, Yang XL, et al. Survival following radiotherapy in young women with localized early-stage breast cancer according to molecular subtypes. Cancer Med. 2019;8(6):2840–2857. doi:10.1002/cam4.2186
4. Islam D, Islam MS, Dorin SI. Prevalence of breast cancer subtypes among different ethnicities and bangladeshi women: demographic, clinicopathological, and integrated cancer informatics analysis. Cancer Inform. 2023;22:11769351221148584. doi:10.1177/11769351221148584
5. Fang W, Huang Y, Han X, Peng J, Zheng M. Characteristics of metastasis and survival between male and female breast cancer with different molecular subtypes: a population-based observational study. Cancer Med. 2022;11(3):764–777. doi:10.1002/cam4.4469
6. Liu YM, Ge JY, Chen YF, et al. Combined single-cell and spatial transcriptomics reveal the metabolic evolvement of breast cancer during early dissemination. Adv Sci. 2023;10(6):e2205395. doi:10.1002/advs.202205395
7. Wang W, Qiu P, Li J. Internal mammary lymph node metastasis in breast cancer patients based on anatomical imaging and functional imaging. Breast Cancer. 2022;29(6):933–944. doi:10.1007/s12282-022-01377-7
8. To B, Isaac D, Andrechek ER. studying lymphatic metastasis in breast cancer: current models, strategies, and clinical perspectives. J Mammary Gland Biol Neoplasia. 2020;25(3):191–203. doi:10.1007/s10911-020-09460-5
9. Alizadeh AM, Shiri S, Farsinejad S. Metastasis review: from bench to bedside. Tumour Biol. 2014;35(9):8483–8523. doi:10.1007/s13277-014-2421-z
10. Brabletz T, Lyden D, Steeg PS, Werb Z. Roadblocks to translational advances on metastasis research. Nat Med. 2013;19(9):1104–1109. doi:10.1038/nm.3327
11. Candido J, Hagemann T. Cancer-related inflammation. J Clin Immunol. 2013;33(1):S79–84. doi:10.1007/s10875-012-9847-0
12. Habanjar O, Bingula R. Crosstalk of inflammatory cytokines within the breast tumor microenvironment. Int J Mol Sci. 2023;24(4):4002. doi:10.3390/ijms24044002
13. Kidane D, Chae WJ, Czochor J, et al. Interplay between DNA repair and inflammation, and the link to cancer. Crit Rev Biochem Mol Biol. 2014;49(2):116–139. doi:10.3109/10409238.2013.875514
14. Bodogai M, Moritoh K, Lee-Chang C, et al. Immunosuppressive and prometastatic functions of myeloid-derived suppressive cells rely upon education from tumor-associated B Cells. Cancer Res. 2015;75(17):3456–3465. doi:10.1158/0008-5472.CAN-14-3077
15. Blum KS, Pabst R. Lymphocyte numbers and subsets in the human blood. Do they mirror the situation in all organs? Immunol Lett. 2007;108(1):45–51. doi:10.1016/j.imlet.2006.10.009
16. Varol C, Mildner A, Jung S. Macrophages: development and tissue specialization. Annu Rev Immunol. 2015;33:643–675. doi:10.1146/annurev-immunol-032414-112220
17. Nielsen SR, Schmid MC. Macrophages as key drivers of cancer progression and metastasis. Mediators Inflamm. 2017;2017:9624760. doi:10.1155/2017/9624760
18. Yang XC, Liu H, Liu DC, Tong C, Liang XW, Chen RH. Prognostic value of pan-immune-inflammation value in colorectal cancer patients: a systematic review and meta-analysis. Front Oncol. 2022;12:1036890. doi:10.3389/fonc.2022.1036890
19. Xia Y, Xia C, Wu L. Systemic immune inflammation index (SII), system inflammation response index (SIRI) and risk of all-cause mortality and cardiovascular mortality: a 20-year follow-up cohort study of 42,875 US adults. J Clin Med. 2023;12(3):1128. doi:10.3390/jcm12031128
20. Ye C, Yuan L, Wu K, Shen B, Zhu C. Association between systemic immune-inflammation index and chronic obstructive pulmonary disease: a population-based study. BMC Pulm Med. 2023;23(1):295. doi:10.1186/s12890-023-02583-5
21. Çakır N, Koc AN. Gamma-glutamyl transpeptidase-platelet ratio, systemic immune inflammation index, and system inflammation response index in invasive Aspergillosis. Rev Assoc Med Bras. 2021;67(7):1021–1025. doi:10.1590/1806-9282.20210475
22. Ji Y, Wang H. Prognostic prediction of systemic immune-inflammation index for patients with gynecological and breast cancers: a meta-analysis. World J Surg Oncol. 2020;18(1):197. doi:10.1186/s12957-020-01974-w
23. Zhang Y, Sun Y. Prognostic value of the systemic immune-inflammation index in patients with breast cancer: a meta-analysis. Cancer Cell Int. 2020;20:224. doi:10.1186/s12935-020-01308-6
24. Tong L, Wang S, Zhang R, Wu Y, Xu D, Chen L. High levels of SII and PIV are the risk factors of axillary lymph node metastases in breast cancer: a retrospective study. Int J Gen Med. 2023;16:2211–2218. doi:10.2147/IJGM.S411592
25. Yamanouchi K, Maeda S. The efficacy of inflammatory and immune markers for predicting the prognosis of patients with stage IV breast cancer. Acta Med Okayama. 2023;77(1):37–43. doi:10.18926/AMO/64360
26. Zhang Y, Wu J, Chen W, Liang X. Pretreatment system inflammation response index (SIRI) is a valuable marker for evaluating the efficacy of neoadjuvant therapy in breast cancer patients. Int J Gen Med. 2024;17:4359–4368. doi:10.2147/IJGM.S478000
27. He W, Li Q, Yang M, et al. Lower BMI cutoffs to define overweight and obesity in China. Obesity (Silver Spring. Md). 2015;23(3):684–691. doi:10.1002/oby.20995
28. Tang J, Zhu X, Chen Y, et al. Association of maternal pre-pregnancy low or increased body mass index with adverse pregnancy outcomes. Sci Rep. 2021;11(1):3831. doi:10.1038/s41598-021-82064-z
29. Yoshihara E, Smeets A, Laenen A, et al. Predictors of axillary lymph node metastases in early breast cancer and their applicability in clinical practice. Breast. 2013;22(3):357–361. doi:10.1016/j.breast.2012.09.003
30. Lucci A, McCall LM, Beitsch PD, et al. Surgical complications associated with sentinel lymph node dissection (SLND) plus axillary lymph node dissection compared with SLND alone in the American college of surgeons oncology group trial Z0011. J Clin Oncol. 2007;25(24):3657–3663. doi:10.1200/JCO.2006.07.4062
31. McLaughlin SA, Wright MJ, Morris KT, et al. Prevalence of lymphedema in women with breast cancer 5 years after sentinel lymph node biopsy or axillary dissection: objective measurements. J Clin Oncol. 2008;26(32):5213–5219. doi:10.1200/JCO.2008.16.3725
32. Krag DN, Anderson SJ, Julian TB, et al. Technical outcomes of sentinel-lymph-node resection and conventional axillary-lymph-node dissection in patients with clinically node-negative breast cancer: results from the NSABP B-32 randomised Phase III trial. Lancet Oncol. 2007;8(10):881–888. doi:10.1016/S1470-2045(07)70278-4
33. Manca G, Rubello D, Tardelli E, et al. Sentinel lymph node biopsy in breast cancer: indications, contraindications, and controversies. Clin Nucl Med. 2016;41(2):126–133. doi:10.1097/RLU.0000000000000985
34. Chen L, Kong X, Wang Z, Wang X, Fang Y, Wang J. Pretreatment systemic inflammation response index in patients with breast cancer treated with neoadjuvant chemotherapy as a useful prognostic indicator. Cancer Manag Res. 2020;12:1543–1567. doi:10.2147/CMAR.S235519
35. Wu HY, Lin CY, Tzeng YD, et al. Preoperative systemic inflammation response index: clinicopathologic predictor of pathological complete response in HER2-positive breast cancer patients receiving neoadjuvant systemic therapy. J Chin Med Assoc. 2024;87(2):226–235. doi:10.1097/JCMA.0000000000001034
36. Zhu M, Chen L, Kong X, et al. The systemic inflammation response index as an independent predictor of survival in breast cancer patients: a retrospective study. Front Mol Biosci. 2022;9:856064. doi:10.3389/fmolb.2022.856064
37. Jiang C, Zhang S, Qiao K, Xiu Y, Yu X, Huang Y. The pretreatment systemic inflammation response index as a useful prognostic factor is better than lymphocyte to monocyte ratio in breast cancer patients receiving neoadjuvant chemotherapy. Clin Breast Cancer. 2022;22(5):424–438. doi:10.1016/j.clbc.2022.03.003
38. Dong J, Sun Q, Pan Y, Lu N, Han X, Zhou Q. Pretreatment systemic inflammation response index is predictive of pathological complete response in patients with breast cancer receiving neoadjuvant chemotherapy. BMC Cancer. 2021;21(1):700. doi:10.1186/s12885-021-08458-4
39. Pereira A, Siegrist J. Clustering molecular subtypes in breast cancer, immunohistochemical parameters and risk of axillary nodal involvement. J Pers Med. 2022;12(9):1404. doi:10.3390/jpm12091404
40. Catteau X, Koopmansch C, Maris C, Colart P, Noël JC. Predictive factors of lymph node metastasis and effectiveness of intraoperative examination of sentinel lymph node in breast carcinoma: a retrospective Belgian study. Ann Diagn Pathol. 2020;49:151607. doi:10.1016/j.anndiagpath.2020.151607
41. Isheden G, Grassmann F, Czene K, Humphreys K. Lymph node metastases in breast cancer: investigating associations with tumor characteristics, molecular subtypes and polygenic risk score using a continuous growth model. Int, J, Cancer. 2021;149(6):1348–1357. doi:10.1002/ijc.33704
42. Min SK, Lee SK. Relation between tumor size and lymph node metastasis according to subtypes of breast cancer. J Breast Cancer. 2021;24(1):75–84. doi:10.4048/jbc.2021.24.e4
43. Si C, Jin Y, Wang H, Zou Q. Association between molecular subtypes and lymph node status in invasive breast cancer. Int J Clin Exp Pathol. 2014;7(10):6800–6806. PMID: 25400761.
44. Karim AM, Eun Kwon J, Ali T, et al. Triple-negative breast cancer: epidemiology, molecular mechanisms, and modern vaccine-based treatment strategies. Biochem Pharmacol. 2023;212:115545. doi:10.1016/j.bcp.2023.115545
45. Dass SA, Tan KL, Selva Rajan R, Mokhtar NF. Triple negative breast cancer: a review of present and future diagnostic modalities. Medicina. 2021;57(1):62. doi:10.3390/medicina57010062
46. Kashyap D, Bal A, Irinike S, et al. Heterogeneity of the tumor microenvironment across molecular subtypes of breast cancer. Appl Immunohistochem Mol Morphol. 2023;31(8):533–543. doi:10.1097/PAI.0000000000001139
47. Setyawati Y, Rahmawati Y, Widodo I, Ghozali A, Purnomosari D. The association between molecular subtypes of breast cancer with histological grade and lymph node metastases in Indonesian woman. Asian Pac J Cancer Prev. 2018;19(5):1263–1268. doi:10.22034/APJCP.2018.19.5.1263
48. Akin S, Altundag K. Clinical associations with ABO blood group and rhesus blood group status in patients with breast cancer: a nationwide retrospective study of 3944 breast cancer patients in Turkey. Med Sci Monit. 2018;24:4698–4703. doi:10.12659/MSM.909499
49. Zouine S, Marnissi F, Otmani N, et al. ABO blood groups in relation to breast carcinoma incidence and associated prognostic factors in Moroccan women. Med Oncol. 2016;33(7):67. doi:10.1007/s12032-016-0784-2
50. Meo SA, Suraya F, Jamil B, et al. Association of ABO and Rh blood groups with breast cancer. Saudi J Biol Sci. 2017;24(7):1609–1613. doi:10.1016/j.sjbs.2017.01.058
51. Bothou A, Tsikouras P, Zervoudis S, et al. Blood groups type linked to breast cancer in a Greek cohort of women - a case control study. J BUON. 2019;24(5):1884–1888. PMID: 31786851.
52. Saxena S, Chawla VK, Gupta KK, Gaur KL. Association of ABO blood group and breast cancer in Jodhpur. Indian J Physiol Pharmacol. 2015;59(1):63–68. PMID: 26571986.
53. Miao SY, Zhou W, Chen L, Wang S, Liu XA. Influence of ABO blood group and Rhesus factor on breast cancer risk: a meta-analysis of 9665 breast cancer patients and 244,768 controls. Asia Pac J Clin Oncol. 2014;10(2):101–108. doi:10.1111/ajco.12083
54. Park S, Kim KS, Kim JS, et al. Prognostic value of ABO blood types in young patients with breast cancer; a nationwide study in Korean Breast Cancer Society. Med Oncol. 2017;34(6):118. doi:10.1007/s12032-017-0974-6
55. Cihan YB. Significance of ABO-Rh blood groups in response and prognosis in breast cancer patients treated with radiotherapy and chemotherapy. Asian Pac J Cancer Prev. 2014;15(9):4055–4060. doi:10.7314/apjcp.2014.15.9.4055
56. Gates MA, Xu M, Chen WY, Kraft P, Hankinson SE, Wolpin BM. ABO blood group and breast cancer incidence and survival. Int, J, Cancer. 2012;130(9):2129–2137. doi:10.1002/ijc.26220
57. Yu J, Gao F, Klimberg VS, Margenthaler JA. ABO blood type/Rh factor and the incidence and outcomes for patients with triple-negative breast cancer. Ann Surg Oncol. 2012;19(10):3159–3164. doi:10.1245/s10434-012-2533-x
58. Dogan I, Ayhan M, Gurbuz M, et al. The frequency and prognostic significance of ABO/Rh blood groups in male breast cancer patients: a multicenter study. Medicine. 2022;101(35):e30147. doi:10.1097/MD.0000000000030147
59. Bertsch T, Lüdecke J, Antl W, Nausch LWM. Karl Landsteiner: the discovery of the ABO blood group system and its value for teaching medical students. Clin Lab. 2019;65(6). doi:10.7754/Clin.Lab.2018.181218
60. Cao X, Wen ZS, Sun YJ, Li Y, Zhang L, Han YJ. Prognostic value of ABO blood group in patients with surgically resected colon cancer. Br J Cancer. 2014;111(1):174–180. doi:10.1038/bjc.2014.302
61. Eastlund T. The histo-blood group ABO system and tissue transplantation. Transfusion. 1998;38(10):975–988. doi:10.1046/j.1537-2995.1998.381098440863.x
62. Le Pendu J, Marionneau S, Cailleau-Thomas A, Rocher J, Le Moullac-Vaidye B, Clément M. ABH and Lewis histo-blood group antigens in cancer. APMIS. 2001;109(1):9–31. doi:10.1111/j.1600-0463.2001.tb00011.x
63. Marionneau S, Le Moullac-Vaidye B, Le Pendu J. Expression of histo-blood group A antigen increases resistance to apoptosis and facilitates escape from immune control of rat colon carcinoma cells. Glycobiology. 2002;12(12):851–856. doi:10.1093/glycob/cwf103
64. Hakomori S. Antigen structure and genetic basis of histo-blood groups A, B and O: their changes associated with human cancer. Biochim Biophys Acta. 1999;1473(1):247–266. doi:10.1016/s0304-4165(99)00183-x
65. Hakomori S. Tumor-associated carbohydrate antigens defining tumor malignancy: basis for development of anti-cancer vaccines. Adv Exp Med Biol. 2001;491:369–402. doi:10.1007/978-1-4615-1267-7_24
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Multicenter Retrospective Analysis on Lymph Node Metastasis in Clinically Node-Negative (cN0) Patients with Small-Sized Breast Cancer
Yan X, Fei Y, Dong T, Zhu Z, Zhu Z, Gao W, Wang D, Zhang J
Cancer Management and Research 2025, 17:2601-2608
Published Date: 31 October 2025