Back to Journals » Journal of Pain Research » Volume 19
Abnormal Regional Brain Functional Activity and Brain Network Connectivity in Primary Trigeminal Neuralgia Patients: An Activation Likelihood Estimation Meta-Analysis Based on Resting-State fMRI
Authors Yang H ![]() , Zhang C, Sun B, Li M, Xu X, Yang H
, Zhang C, Sun B, Li M, Xu X, Yang H ![]()
Received 10 October 2025
Accepted for publication 24 January 2026
Published 4 February 2026 Volume 2026:19 573011
DOI https://doi.org/10.2147/JPR.S573011
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Hongan Yang,1,* Chuan Zhang,1– 3,* Baijintao Sun,1,* Mingtao Li,1 Xiaoxue Xu,1 Hanfeng Yang1,3
1Department of Radiology, Affiliated Hospital of North Sichuan Medical College, Nanchong, People’s Republic of China; 2Innovation Center for Science and Technology, Affiliated Hospital of North Sichuan Medical College, Nanchong, People’s Republic of China; 3Biotechnology Innovation Drug Application and Transformation Key Laboratory of Sichuan Province, North Sichuan Medical College, Nanchong, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hanfeng Yang, Department of Radiology, Affiliated Hospital of North Sichuan Medical College, No. 1 Maoyuan South Road, Nanchong, Sichuan, 637000, People’s Republic of China, Tel +86 15182927120, Email [email protected]
Objective: This study integrates resting-state functional magnetic resonance imaging (rs-fMRI) studies to systematically identify core regions of altered regional brain activity and abnormal functional connectivity within cerebral networks in patients with primary trigeminal neuralgia (PTN).
Methods: We systematically searched PubMed, Web of Science, and EMBASE for rs-fMRI studies (between January 2010 and June 2025) comparing PTN patients with healthy controls (HCs). Through a standardized data extraction protocol, coordinates of divergent brain functional metrics and network connectivity parameters were collected. Ultimately, we included 16 studies, of which 14 were related to functional specific indices (375 patients) and 5 to functional connectivity (204 patients). Separate modality-specific Activation Likelihood Estimation (ALE) meta-analyses were conducted for studies employing Amplitude of Low-Frequency Fluctuation (ALFF/fALFF), Regional Homogeneity (ReHo), and Degree Centrality (DC), to reflect their unique neurophysiological meanings.
Results: ALE analysis revealed index-specific alteration patterns with limited spatial overlap. The ALFF/fALFF analysis identified consistent hypoactivity in the left medial prefrontal cortex. In contrast, ReHo and DC analyses converged to show hyperactivity in the posterior cerebellar lobe and temporal pole. Notably, Seed-based functional connectivity analyses yielded no convergent findings, and limbic system activation was highly heterogeneous.
Conclusion: Our meta-analysis demonstrates that PTN involves complex, multidimensional brain remodeling, not a dysfunction of a single “pain center.” The distinct spatial patterns identified by different rs-fMRI metrics underscore their complementary value in uncovering PTN pathophysiology. These findings advance the understanding of PTN’s central mechanisms, support the development of targeted interventions, and highlight the need to differentiate neurophysiological metrics and clinical subtypes in future research.
Keywords: primary trigeminal neuralgia, resting-state functional magnetic resonance imaging, meta-analysis, regional brain activity, functional connectivity
Introduction
Primary trigeminal neuralgia (PTN) is a chronic neuropathic facial pain disorder characterized by paroxysmal, electric shock-like or stabbing pain attacks in the distribution of one or more branches of the trigeminal nerve.1–3 Approximately one-third of patients with chronic TN experience moderate to severe depression, and about half of these patients also exhibit anxiety symptoms directly related to TN.4–6
In clinical practice, PTN patients often encounter challenges such as diminished drug efficacy, severe side effects, or pain recurrence and inadequate pain relief after surgical intervention, posing significant hurdles to pain management and patients’ quality of life. This heterogeneity in treatment response implies potential interindividual variations in the underlying central mechanisms. Although PTN has traditionally been considered to be primarily associated with peripheral lesions of the trigeminal nerve root, the experience of chronic pain extends far beyond peripheral signal afference. Long-term chronic pain stimulation drives secondary adaptive remodeling in the brain, and these central adaptive changes may represent the key to the transition of pain from acute to chronic, the emergence of emotional comorbidities (such as anxiety and depression), and heterogeneity in treatment response. Multiple rs-fMRI studies have reported abnormal changes in regional brain functional activity, functional network connectivity, and related clinical behavioral aspects in TN patients from different perspectives.7 For example, some studies used low-frequency amplitude (ALFF), fractional low-frequency amplitude (fALFF), regional homogeneity (ReHo), and other methods to analyze spontaneous brain activity in TN patients, identifying abnormal ALFF or ReHo values in specific brain regions.8,9 Ge et al conducted a more comprehensive study on ALFF, ReHo, and dynamic frequency. Other studies focusing on brain network connectivity changes have found disorders in resting-state network modular organization,10 dynamic characteristics of functional networks,11 and structural and functional connectivity of the salience network12 in TN patients. These findings indicate that the central nervous system of trigeminal neuralgia patients has undergone changes at multiple levels, which may play a key role in the process of pain perception, transmission, and regulation.
However, discrepancies exist across studies in terms of methodology, sample characteristics, and analytical metrics, leading to inconsistent findings regarding specific regional brain abnormalities and altered connectivity patterns. Notably, some results even demonstrate contradictory conclusions. Therefore, a systematic meta-analytical integration of available brain functional imaging data is essential to identify stable central functional remodeling patterns in patient populations, localize consistent abnormal brain regions and network connectivity alterations, and provide evidence for defining core neural circuits of pain chronicity and target interventions. The activation likelihood estimation (ALE) is a well-established coordinate-based meta-analysis method that assesses statistical convergence of reported brain coordinates across studies, serving as an ideal method to synthesize heterogeneous study findings and identify consistently affected brain regions.13 Based on this, this study uses the ALE meta-analysis method to systematically integrate the brain functional imaging data of patients with PTN. This study aims to use ALE meta-analysis to independently analyze studies using different indices (eg, ALFF/fALFF, ReHo, DC), with the objective of uncovering multidimensional features of brain functional abnormalities in PTN patients and exploring the specificity of each index in revealing pathological changes. Specifically, we hypothesized that these different fMRI indices, which capture distinct aspects of neural function, would reveal complementary and largely non-overlapping patterns of brain alterations, thereby reflecting the multifaceted pathophysiology of PTN.
Materials and Methods
This study has been prospectively registered in PROSPERO (https://www.crd.york.ac.uk/PROSPERO/home) with registration number: CRD42025641261.
Literature Inclusion and Exclusion Criteria
The literature inclusion criteria were as follows: (1) Studies were required to be peer-reviewed investigations utilizing rs-fMRI to compare cerebral functional alterations between PTN patients and HCs; (2) Participants must have been formally diagnosed with PTN according to internationally recognized criteria (ICHD-3);14 (3) Studies must utilize analytical approaches including amplitude of ALFF, fALFF, ReHo, degree centrality (DC), or seed-based functional connectivity; additionally, reported brain regions showing significant differences must be presented with Montreal Neurological Institute (MNI)15 or Talairach stereotactic coordinates.
The literature exclusion criteria were as follows: (1) Studies published in languages other than English were excluded; (2) Studies were excluded if they represented duplicate publications or contained overlapping data with previously included studies; (3) Studies were excluded if they failed to report stereotactic coordinates (MNI/Talairach); (4) Studies were excluded if they were reviews, meta-analyses, or case reports; (5) Studies with low methodological quality, as determined by predefined criteria, were excluded due to insufficient evidence for inclusion in subsequent analyses.
Literature Search Strategy
A systematic search was conducted for rs-fMRI studies published between January 2010 and June 2025 in PubMed, Web of Science, and EMBASE databases. Search terms included: “trigeminal neuralgia”, “primary trigeminal neuralgia”, “classic trigeminal neuralgia”, “idiopathic trigeminal neuralgia”, “fMRI”, “functional connectivity”, “FC”, “functional MRI”, “Resting-State Functional MRI”, “rs-fMRI”, “ALFF”, “fALFF”, “amplitude of low-frequency fluctuation”, “fractional amplitude of low-frequency fluctuation”, “ReHo”, “regional homogeneity”. To avoid omissions, we also manually searched reference lists of relevant reviews. All retrieved records were imported into EndNote (a reference management tool) for screening.
Literature Screening and Data Extraction
Literature screening and data extraction were independently performed by two reviewers, followed by cross-verification. Discrepancies were resolved through discussion. The data extraction included: (1) Study information: first author, publication year, sample size, age, VAS score, disease duration, analysis method, correction method, peak center coordinate presentation format, and peak center coordinates of differential brain regions; (2) Further analysis of extracted MNI coordinates using MRIcroGL, adhering to ALE analysis criteria.
Quality Assessment
Study quality was assessed using the Newcastle-Ottawa Scale (NOS), which evaluates three domains: (1) Selection of Study Participants, including representativeness of the case group, appropriateness of control group selection, reliability of exposure determination methods, and response rate; (2) Comparability of Groups, assessing control of confounding factors during design (eg, age, gender) and statistical adjustments during analysis (eg, multivariate regression); and (3) Exposure/Outcome Assessment, evaluating objectivity of outcome measurement (eg, blinding or laboratory testing), adequacy of follow-up duration (covering disease latency), and completeness of outcome data. Studies scoring>6 points (maximum 9) were included for subsequent analysis.
Meta-Analysis Strategy
Considering that different resting-state fMRI indices reflect distinct physiological dimensions of neural activity, pooled analysis without discrimination may obscure significant changes specific to individual indices, leading to ambiguous results. Therefore, we adopted a modality-specific meta-analysis strategy, conducting independent ALE meta-analyses for studies using three types of indices: (1) Amplitude metrics (ALFF/fALFF): Reflecting the energy consumption level of spontaneous neuronal activity at rest;16 (2) ReHo index: Reflecting the temporal consistency of neuronal activity within local brain regions;17 (3) DC index: Reflecting the importance of brain region nodes in the whole-brain functional network. Studies have suggested that regions with reduced ReHo often coincide with those showing decreased nodal efficiency, implying an inherent association between local synchrony and global connectivity.11,12,17 Given that both ReHo and DC measure the local information integration capacity of brain regions to some extent,17,18 we conducted an exploratory joint analysis to test whether these two indices showed synergistic alterations and to enhance the robustness of the results. Each analysis was performed independently, and their outcomes were regarded as reflections of different aspects of TN pathophysiology.
Data Processing
This study integrated neuroimaging data in standard MNI space using GingerALE 3.0.2 (https://www.brainmap.org/ale/) to quantify PTN-related activation consistency and identify differential patterns vs controls.
MNI coordinates and participant numbers were compiled into focus files per GingerALE best practices. ALE analysis involved iterative Gaussian smoothing to generate MA maps, followed by voxel-wise weighted overlay; higher ALE values indicated stronger cross-study consistency.19 Monte Carlo simulations (1000 iterations) with cluster-level FWE correction controlled error rates, using uncorrected p < 0.001 for cluster formation and FWE-corrected p < 0.05 for significance.20,21
For seed-based functional connectivity studies, we employed an adapted Meta-Analytic Connectivity Modeling (MACM) approach to integrate findings across different seed regions.22,23 Specifically, we used Sleuth 3.0.4 software to perform a “dual screening” of the seed-based studies: first, we identified all brain regions that were reported as showing altered connectivity in PTN patients (regardless of seed), and then we treated these regions as if they were activation foci in a conventional ALE. In this way, we could use GingerALE to conduct a convergence analysis on the reported connectivity foci, analogous to how ALE is applied to activation peaks[nature.com]. This allowed us to detect brain regions that were consistently reported as part of abnormal connectivity networks in PTN across multiple seed-based studies.
Finally, MRIcroGL (https://www.nitrc.org/mricrogl) overlaid ALE maps onto standard templates, generating 3D volume renderings of activated regions.
Result
Results of Systematic Literature Search and Data Extraction
A total of 251 relevant articles were initially retrieved. After stepwise screening, 16 eligible studies were finally included.8–10,16,17,24–34 The literature screening process is detailed in Figure 1. Specifically, 9 studies adopted ALFF/fALFF analysis,8,16,24,26,28,30,31,34 6 used ReHo analysis,9,17,24,26,27,31 3 applied DC analysis,24,29,32 and 5 focused on seed-based functional connectivity.10,28,30,33,34 Detailed literature data are presented in Tables 1 and 2.
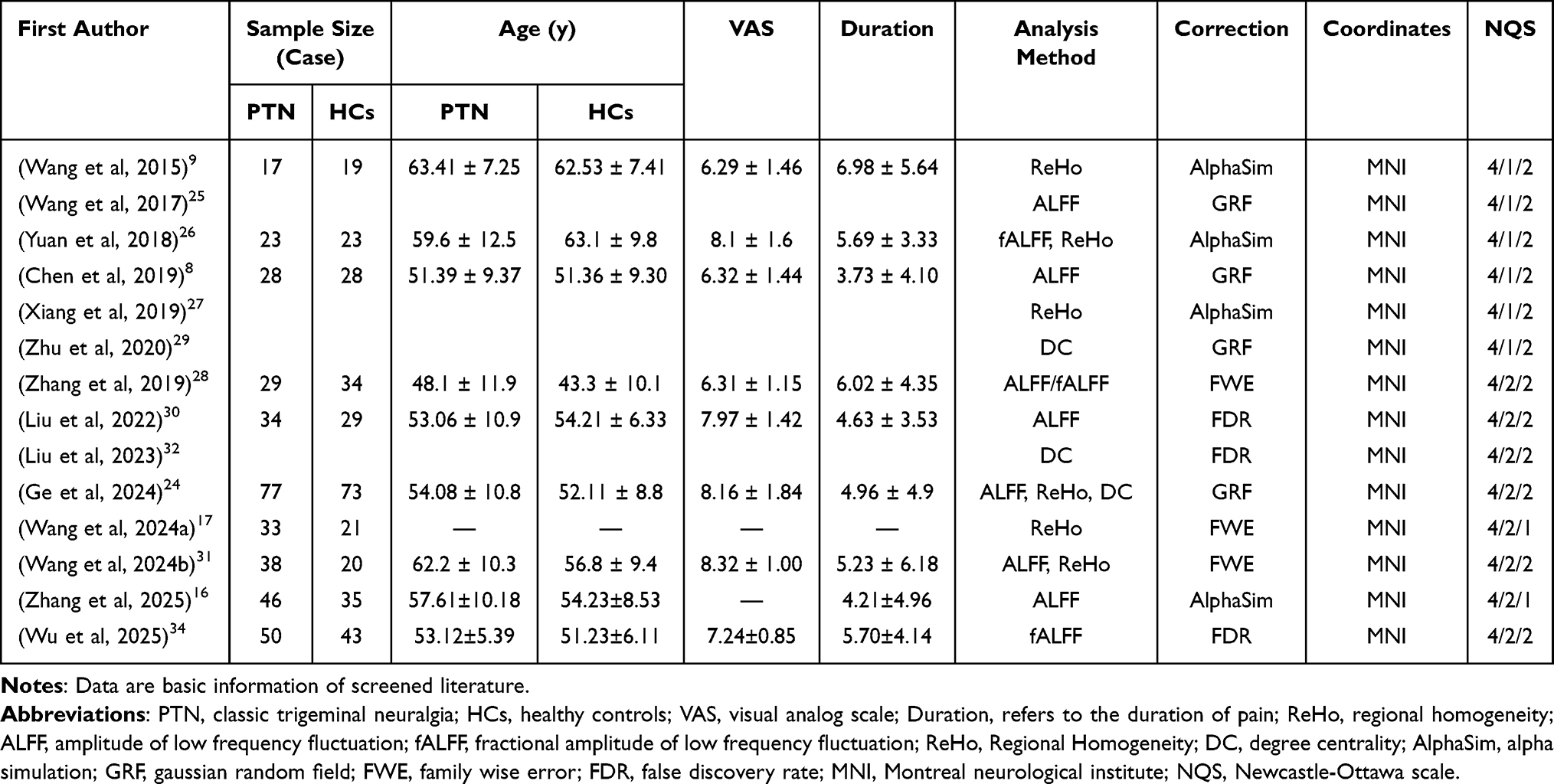 |
Table 1 The Literature Data Included in the ALE Analysis |
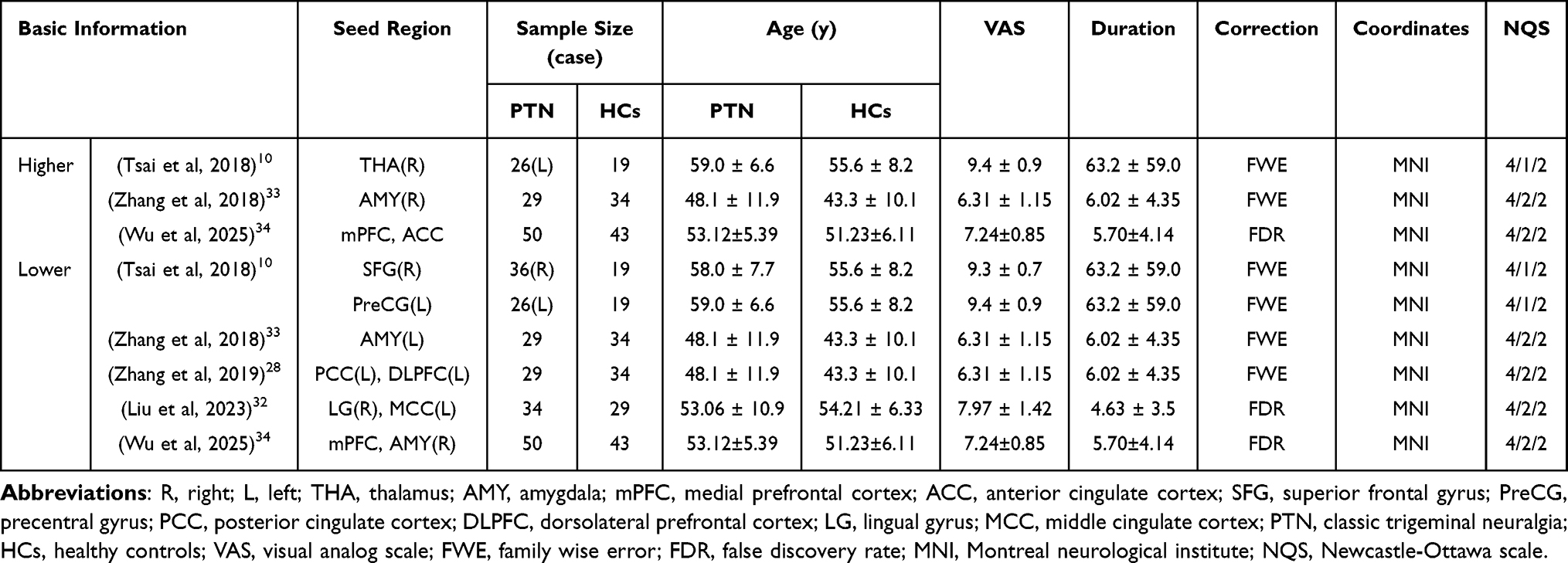 |
Table 2 The Literature Data Related to Seed-Based Functional Connectivity |
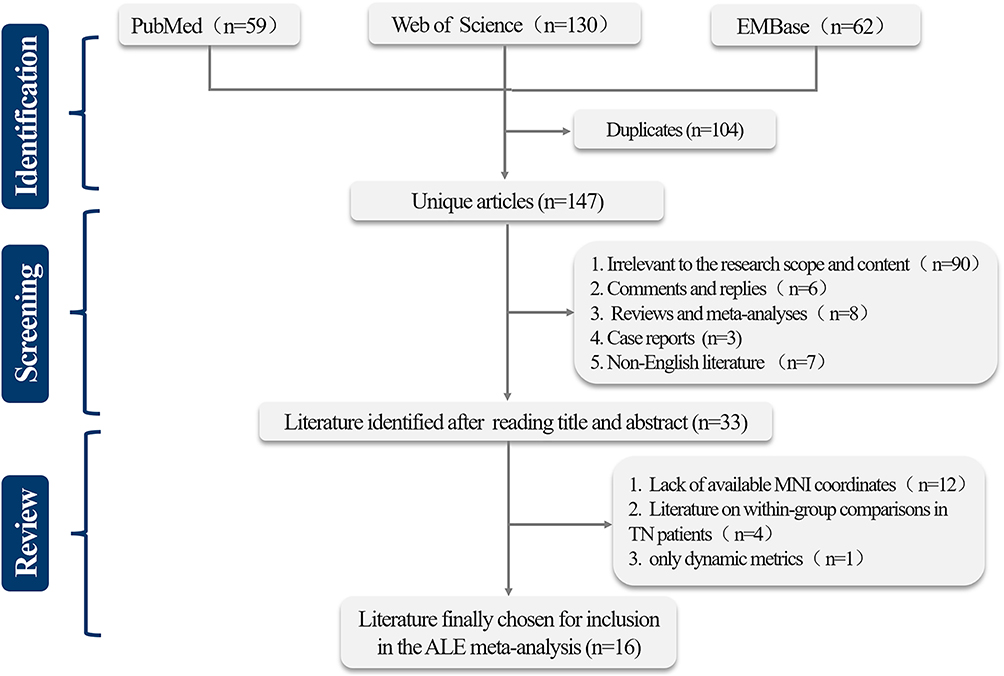 |
Figure 1 Flowchart of literature selection for TN ALE meta-analysis. |
Results of Data Analysis
In the independent analysis of ALFF/fALFF, patients with PTN exhibited reduced co-activation in the left medial frontal gyrus (Figure 2 and Table 3). The independent ReHo analysis revealed increased co-activation in the left temporal pole and right posterior cerebellar lobe in PTN patients (Figure 3 and Table 4). In the DC-based independent analysis, PTN patients showed reduced co-activation in the right lingual gyrus–cuneus region (Figure 4 and Table 5). Combined ReHo and DC analyses demonstrated synergistic enhancement of co-activation in the left temporal pole and bilateral posterior cerebellar lobes, alongside synergistic reduction in the right cuneus (Figure 5 and Table 6).
 |
Table 3 Convergent Regions of Reduced Activation in PTN Patients in Exclusive ALFF/fALFF Analysis |
 |
Table 4 Convergent Regions of Increased Activation in PTN Patients in Exclusive ReHo Analysis |
 |
Table 5 Convergent Regions of Reduced Activation in PTN Patients in Exclusive DC Analysis |
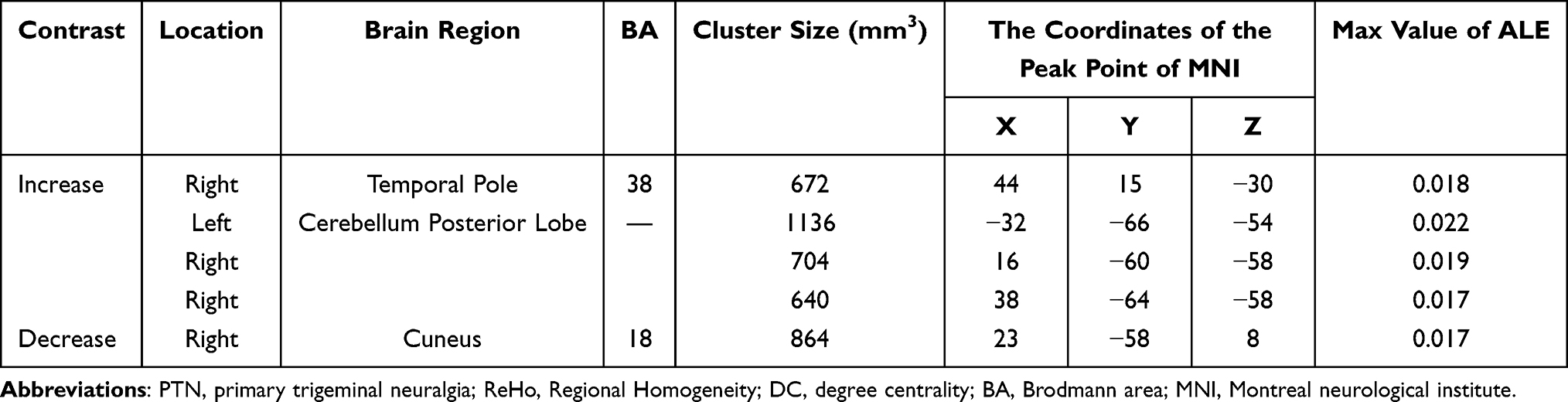 |
Table 6 Convergent Regions of Reduced Activation in PTN Patients in Combined ReHo&DC Analysis |
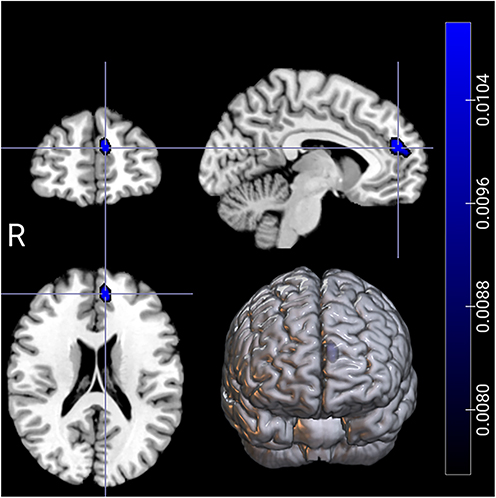 |
Figure 2 Convergent regions of reduced activation in PTN patients in the exclusive ALFF/fALFF analysis. The analysis identified a significant cluster in the left medial frontal gyrus. Results are displayed on a standard MNI template. The color bar indicates the ALE value. Statistical significance was determined using a cluster-forming threshold of p < 0.001 with a cluster-level FWE correction at p < 0.05. |
 |
Figure 3 Convergent regions of increased activation in PTN patients in the exclusive ReHo analysis. The analysis identified significant clusters in (A) the right temporal pole and (B) the left cerebellum posterior lobe. Results are displayed on a standard MNI template. The color bar indicates the ALE value. Statistical significance was determined using a cluster-forming threshold of p < 0.001 with a cluster-level FWE correction at p < 0.05. |
 |
Figure 4 Convergent regions of reduced activation in PTN patients in the exclusive DC analysis. The analysis identified a significant cluster spanning (A) the right cuneus and (B) the right lingual gyrus. Results are displayed on a standard MNI template. The color bar indicates the ALE value. Statistical significance was determined using a cluster-forming threshold of p < 0.001 with a cluster-level FWE correction at p < 0.05. |
 |
Figure 5 Convergent regions of synergistic alteration in PTN patients in the combined ReHo & DC analysis. The analysis revealed regions of increased activation in (A) the right temporal pole, (B) the left cerebellum posterior lobe, and (C and D) the right cerebellum posterior lobe. A region of decreased activation was identified in (E) the right cuneus. Results are displayed on a standard MNI template. The color bars indicate the ALE values. Statistical significance was determined using a cluster-forming threshold of p < 0.001 with a cluster-level FWE correction at p < 0.05. |
Regarding seed-based functional connectivity, no significant co-activation clusters were identified in the cross-seed core regions through ALE analysis.
Discussion
Modality-specific meta-analyses based on different fMRI indices depicted a multidimensional profile of brain functional remodeling in PTN patients. Results showed minimal spatial overlap among abnormal brain regions identified by independent analyses. We argue that this finding does not diminish the biological significance of the results, but rather profoundly reveals the complexity and multidimensionality of central mechanisms in PTN. Additionally, although studies by Nardoni et al35 and Zhu et al36 both identified consistent structural and functional changes in TN patients, neither strictly distinguished between different functional indices or imaging modalities in their respective meta-analyses, but instead combined multiple results for analysis. This approach may mask significant changes under specific indices, and due to the lack of index differentiation, there is a certain ambiguity in interpreting the meta-analytic results. Below, we contextualize major findings to explore their potential neurobiological implications and associations with PTN pathophysiology. Thus, the following section will interpret the key findings in conjunction with relevant specific indices and conduct an in-depth discussion on the causes of PTN heterogeneity, aiming to provide certain references for future research.
Prefrontal Cortex
The medial prefrontal cortex (mPFC), a key subregion of the PFC, serves as a critical node for emotional and cognitive processing in chronic pain. It integrates nociceptive information with emotional responses and forms a “pain-emotion-cognition” interactive network through extensive neural circuits connecting to the hippocampus, amygdala, thalamus, and other regions.37–39 Furthermore, the mPFC plays a key role in the endogenous pain modulation network by projecting to the periaqueductal gray (PAG) and rostral ventromedial medulla (RVM), thereby activating descending pain inhibitory systems to effectively suppress spinal nociceptive transmission.
The meta-analysis based on ALFF/fALFF indicates that, when compared to HCs, PTN patients have areas of reduced co-activation in the left mPFC. We tentatively hypothesize that under the long-term chronic pain stimulation, the decreased intensity of spontaneous activity in the mPFC of PTN patients may suggest a certain functional deficiency in this area. This functional deficiency can lead to impairments in the related descending pain inhibitory pathways, which in turn worsen pain sensitization. Moreover, it may be linked to the impaired regulation of negative emotions such as anxiety, depression, and catastrophic thinking in TN patients.
In related functional studies, latest study observed decreased ALFF in the left superior/medial frontal gyrus of TN patients, which inversely correlated with pain severity and negative emotional indices.40 Sliding window functional connectivity analysis revealed that PFC-PAG connectivity negatively correlated with perceived pain intensity during spontaneous TN fluctuations.41 In seed-based functional connectivity analyses, studies found that amygdala-DLPFC and amygdala-mPFC circuits correlate with clinical pain duration and emotional state ratings, respectively; Zhang et al reported that posterior cingulate-mPFC functional connectivity strength inversely correlates with pain intensity.28 A recent study by Lv et al identified the ventral hippocampus-mPFC circuit and CRH-CRHR1 signaling as mediators of chronic TN-related anxiety and depression, with pathway/signal inhibition effectively alleviating anxiety- and depression-like behaviors. These findings align closely with our results, suggesting that prefrontal dysfunction may drive the chronification of pain through weakened descending pain inhibition and limbic system regulation, forming a “pain-emotion-cognition” vicious cycle.
Occipital Lobe
The medial occipital lobe (lingual gyrus-cuneus complex) integrates visual processing and pain perception.42 Our rs-fMRI analysis revealed consistent hypoactivation in the right cuneus-lingual gyrus via ReHo/ReHo-DC metrics, suggesting adaptive chronic pain responses involving visual-nociceptive integration dysfunction and pain-modulatory circuit suppression.
Previous studies suggest that increased temporal lobe activity in TN patients may induce dysfunction in brain regions, potentially heightening sensitivity to action recognition related to TN pain attacks,43,44 while structural MRI reports reduced cuneus cortical thickness correlated with carbamazepine dosage, indirectly supporting functional suppression in this region.45
Cerebellum
While traditionally linked to motor coordination, the cerebellum modulates pain via interactions with sensory-motor, executive, and limbic systems.46–49 A meta-analysis conducted by Moulton et al demonstrated consistent activation of vermal lobules IV/V and hemispheric lobules V/VI during pain processing in chronic pain patients.47 Subsequent meta-analyses by Lanz et al.,50 Jensen et al51 and Xu et al52 further linked chronic pain to altered activation intensity in lobules V/VI and Crus I.
In this study, consistent co-activation synergistic enhancement in the posterior cerebellar lobe of PTN patients was identified in both independent ReHo analysis and combined ReHo-DC analysis. We hypothesize that this reflects functional network remodeling of the cerebellum under chronic pain conditions, suggesting that this region not only exhibits increased local neuronal synchronization but also serves as a critical “hub” within the pain network, mediating functional connectivity with pain-related regions across the whole brain.
Studies have demonstrated altered persistent activity patterns in the cerebellum of chronic pain patients. For instance, patients with chronic orofacial neuropathic pain exhibit increased oscillation intensity in the low-frequency range within lobule VI and Crus I of the cerebellum.53 Furthermore, functional connectivity (FC) between the cerebellum and other cortical/subcortical regions is aberrant in chronic pain populations. For example, enhanced FC between the left Crus I and bilateral insular regions has been observed in patients with persistent headache.54 Mehnert et al further reported that noxious trigeminal input induces activation in multiple cerebellar regions (lobule VI, VIIIa, Crus I), which show enhanced connectivity with classical “pain matrix” regions and bilateral precentral gyrus facial areas.55
Temporal Lobe
The temporal lobe plays a role in numerous intricate functions, such as language processing, auditory perception, memory handling, and emotional control.56–58 In recent years, it has been regarded as one of the brain regions for central pain integration.59
Our ALE analysis revealed enhanced left temporal pole co-activation in PTN via ReHo/ReHo-DC metrics, linking temporal lobe dysfunction to chronic pain modulation and disease severity. Structural MRI studies demonstrate negative correlations between superior temporal gyrus (STG) gray matter volume and pain duration/anxiety scores,60 while aberrant STG-posterior cingulate gyrus(PCG)/default mode network(DMN) connectivity exacerbates pain persistence.61 Temporal lobe volume loss further correlates with TN progression,62 highlighting its role in pain chronification and potential as a neuromodulatory target.
Others
The limbic system (including the amygdala, hippocampus, cingulate gyrus, etc.) serves as the central hub for emotional and memory processing, playing a pivotal role in the development and maintenance of chronic pain.63 The chronification of pain is often accompanied by spatiotemporal reorganization of brain activity, shifting from sensory to emotional and limbic regions.64
Although numerous studies have reported abnormalities in the extensive limbic system and its related structures (such as the thalamus) in TN patients,10–12,17,28,31,33,65–67 this meta-analysis failed to identify cross-study consistent activation clusters in these regions. We argue that this is not a methodological failure but an important signal reflecting clinical reality. Specifically, the heterogeneity of the limbic system may be associated with the following factors: (1) Pain subtypes and severity: differences in pain frequency, intensity, and the presence of persistent pain among patients may lead to varying limbic system responses. For example, Wang et al found significantly increased ALFF values in the right anterior cingulate gyrus of TN patients with high neurovascular compression (NVC) scores,31 while Zhang et al reported decreased ALFF values in the bilateral anterior cingulate gyrus;28 (2) Clinical subtypes and lateralization effects in PTN:recent studies have revealed that there are potential differences in functional connectivity and spontaneous brain activity between classical trigeminal neuralgia (CTN), idiopathic trigeminal neuralgia (ITN), and trigeminal neuralgia on different sides;34,68 (3) Emotional comorbidities: Limbic system activity and connectivity may differ between TN patients with emotional disorders and those without. For instance, some studies have found abnormally increased functional connectivity of the amygdala in TN patients,33 whereas others have reported reduced functional connectivity and nodal efficiency in the hippocampus;17 (3) Disease duration and stage: Neuroplasticity during TN progression exhibits dynamic changes, and functional reorganization of the limbic system may have time-dependent characteristics and complex topological properties. For example, using dynamic functional network connectivity analysis, Zhang et al found reduced nodal efficiency in the anterior cingulate cortex (within the salience network) and thalamus/caudate nucleus (within the subcortical network), with changes in topological properties negatively correlated with TN duration and attack frequency.11 This suggests that the involvement of the limbic system may differ across different disease stages.
Additionally, in seed-based functional connectivity analyses, our study observed no significant cluster formation. Potential contributing factors include: 1) spatial dispersion of coordinate data due to varying anatomical seed point selections across PTN-related connectivity studies, which may reduce the ALE algorithm’s ability to detect consistent activation; 2) disparities in experimental paradigms, insufficient study inclusion, and small sample sizes across studies, leading to increased spatial fuzziness in MA maps and reduced ALE value convergence. Therefore, larger sample sizes, refined seed-based analysis protocols, stricter data filtering, stratified analysis, and multi-method cross-validation may improve detection of PTN-specific dysfunctional couplings.
Clinical Value and Futural Prospection
In our study, the final results highlight the central role of prefrontal dysfunction in descending pain inhibition failure, the potential compensatory value of cerebellar and temporal networks in chronic pain adaptation, and the marked heterogeneity of activation patterns in traditional limbic structures and thalamus. These findings provide important neuroimaging clues for the future development of more targeted individualized treatment strategies.
Current studies indicate that while pharmacological therapies and invasive surgical interventions can alleviate pain symptoms in TN patients to varying degrees, a subset of individuals still experience inadequate pain control or pain recurrence.2,69–75 Based on the preceding discussion, we hypothesize that there may be subgroup differences in central neuroimaging signatures among PTN patients with varying treatment responses. Danyluk et al found that limbic system functional changes correlate with surgical treatment resistance in TN, enabling partial differentiation between responders and non-responders.76 Prof. Karen D. Davis’ team identified structural differences in brain regions between treatment-effective and treatment-ineffective TN patient groups, proposing that neuroimaging-based brain signatures could identify patients likely to benefit from therapy, thereby highlighting the potential of neuroimaging analysis for treatment efficacy evaluation and patient stratification in TN.77–79 Liu et al analyzed rs-fMRI data from migraine patients and demonstrated that functional connectivity strength within the limbic system, prefrontal cortex, and other brain regions effectively distinguished patient subgroups with varying headache frequencies.80 However, current research predominantly focuses on cross-sectional resting-state fMRI studies, with notable gaps in neuroimaging-based PTN subgroup classification, longitudinal dynamic mechanism investigations, and explorations of whole-brain dynamic functional connectivity patterns. Limited sample sizes further restrict the comprehensive capture of dynamic functional alterations during TN progression. Future studies should prioritize large-scale longitudinal cohorts, multimodal technical integration, and individualized modeling to elucidate dynamic brain network characteristics in PTN patients, thereby providing scientific foundations for personalized treatment strategies and prognostic prediction.
Furthermore, long-term pharmacotherapy or repeated surgical interventions may lead to more severe side effects and complications in patients with refractory or recurrent TN.81–83 Consequently, there is an urgent clinical and patient-driven demand for non-invasive, safe, and effective therapeutic alternatives to conventional drugs and surgeries. Brain stimulation, a non-invasive technology capable of guiding neuroplasticity, aims to alleviate chronic pain by directly altering brain activity through induced electrical stimulation.84 Retrospective studies in chronic pain have demonstrated promising analgesic effects of non-invasive brain stimulation techniques, particularly repetitive transcranial magnetic stimulation (rTMS) and transcranial direct current stimulation (tDCS).84,85 A recent review by Babakhani et al evaluated tDCS efficacy in refractory TN patients, finding significant pain reduction with differing polarities potentially acting through distinct neural pathways. Neuroimaging methods were shown to identify imaging biomarkers of tDCS treatment response in TN.86 rTMS studies further indicate that targeting the primary motor cortex (M1) effectively alleviates pain in refractory TN.87,88 Despite promising analgesic outcomes of transcranial electrical stimulation in chronic TN management, the underlying mechanisms of non-invasive neuromodulation remain unclear, stimulation protocols lack standardization, and interventions typically rely on fixed anatomical targets (eg, M1 or DLPFC). Future research is warranted to elucidate optimal individualized treatment strategies and target selection. Additionally, the complexity of chronic TN pain necessitates longitudinal investigations using multimodal fMRI techniques to characterize baseline and post-intervention features of the brain’s nociceptive-perceptive and inhibitory pathways, thereby comprehensively analyzing pain-related neural networks across sensory, cognitive, and emotional dimensions.
Limitations
First, a major limitation of this study is that due to most original studies failing to provide subgroup coordinate data for stratified meta-analysis, we did not separately analyze different subtypes of primary trigeminal neuralgia (ie, classic trigeminal neuralgia and idiopathic trigeminal neuralgia). Secondly, several of our ALE analyses, particularly the DC analysis, were based on a relatively small number of studies (n=3), which may limit the statistical power and the stability of the identified convergence patterns. Thirdly, the combined ReHo and DC analysis was exploratory in nature, designed to test for synergistic alterations. While the results are theoretically grounded, they should be interpreted with caution pending further validation in future studies. Additionally, we did not differentiate clinical heterogeneities such as persistent pain and pain laterality effects in patients. We speculate that clinical heterogeneity may be one of the key reasons leading to the highly discrete activation patterns of the limbic system and the failure to form consistent results. Future original studies should strive to report detailed data of different clinical subtypes to reveal neuroimaging markers of specific subgroups. Finally, the ALE method only models based on activation coordinates reported in the literature, which is essentially a spatial convergence analysis and cannot obtain activation intensity, range, and temporal dynamic information of neural activity in the original images.
Conclusion
This study systematically revealed the complex landscape of brain functional remodeling in PTN patients through modality-specific meta-analysis. Our core contribution lies in demonstrating that different fMRI indices uncover complementary rather than overlapping abnormal patterns. Collectively, these findings challenge the traditional approach of seeking a single “pain center” and emphasize the necessity of understanding PTN central mechanisms from a multi-dimensional and multi-metric perspective. However, due to study limitations, further research is required to validate and refine these findings, promoting clinical progress in PTN diagnosis and treatment.
Abbreviations
PTN, Primary Trigeminal Neuralgia; fMRI, functional Magnetic Resonance Imaging; ALE, Activation Likelihood Estimation; rs-fMRI, Resting-State Functional Magnetic Resonance Imaging; HC(s), Healthy Control (s); ALFF, Amplitude of Low-Frequency Fluctuation; fALFF, Fractional Amplitude of Low-Frequency Fluctuation; ReHo, Regional Homogeneity; DC, Degree Centrality; MNI, Montreal Neurological Institute; NOS, Newcastle-Ottawa Scale; FC, Functional Connectivity; VAS, Visual Analogue Scale; NVC, Neuro Vascular Compression; STG, Superior Temporal Gyrus; PCG, Posterior Cingulate Gyrus; DMN, Default Mode Network; PFC, Prefrontal Cortex; mPFC, medial Prefrontal Cortex; PAG, Periaqueductal Gray; RVM, Rostral Ventromedial Medulla; DLPFC, Dorsolateral Prefrontal Cortex; CRH, Corticotropin-Releasing Hormone; CRHR1, Corticotropin-Releasing Hormone Receptor 1; MACM, Meta-Analytic Connectivity Modeling; FWE, Family-Wise Error; BOLD, Blood Oxygen Level-Dependent; rTMS, repetitive Transcranial Magnetic Stimulation; tDCS, transcranial Direct Current Stimulation; ICHD-3, International Classification of Headache Disorders, 3rd edition; EEG, Electroencephalogram.
Data Sharing Statement
All supporting documentation related to this meta-analysis, comprising data collection templates, research datasets, coding frameworks, and methodological records, are available upon request to verified academic professionals. Researchers seeking to replicate or extend the work may initiate access procedures by emailing the study’s principal investigator, Dr. Hongan Yang, through his official university Email (Email: [email protected]).
Funding
This work was supported by the Sichuan Provincial Natural Science Foundation Youth Fund Project (24NSFSC1783), Research and Development Plan Project of Affiliated Hospital of North Sichuan Medical College (2023PTZK002, 2024GC012), Youth Science and Technology Talent Program of Nanchong Science and Technology Bureau (25KJCXRC0012), Special Project for the Central Government to Guide the Development of Local Science and Technology in Sichuan Province (2024ZYD0092).
Disclosure
Hongan Yang, Chuan Zhang and Baijintao Sun contributed equally to this work and share first authorship. All authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Bendtsen L, Zakrzewska JM, Heinskou TB, et al. Advances in diagnosis, classification, pathophysiology, and management of trigeminal neuralgia. Lancet Neurol. 2020;19:784–16. doi:10.1016/S1474-4422(20)30233-7
2. Cruccu G, Di Stefano G, Truini A. Trigeminal Neuralgia. N Engl J Med. 2020;383:754–762. doi:10.1056/NEJMra1914484
3. Ashina S, Robertson CE, Srikiatkhachorn A, et al. Trigeminal neuralgia. Nat Rev Dis Primers. 2024;10:39. doi:10.1038/s41572-024-00523-z
4. Garcia-Isidoro S, Castellanos-Sanchez VO, Iglesias-Lopez E, Perpiña-Martinez S. Invasive and non-invasive electrical neuromodulation in trigeminal nerve neuralgia: a systematic review and meta-analysis. Curr Neuropharmacol. 2021;19:320–333. doi:10.2174/1570159X18666200729091314
5. Zakrzewska JM, Wu J, Mon-Williams M, Phillips N, Pavitt SH. Evaluating the impact of trigeminal neuralgia. Pain. 2017;158:1166–1174. doi:10.1097/j.pain.0000000000000853
6. Lv -S-S, Lv X-J, Cai Y-Q, et al. Corticotropin-releasing hormone neurons control trigeminal neuralgia-induced anxiodepression via a hippocampus-to-prefrontal circuit. Sci Adv. 2024;10:eadj4196. doi:10.1126/sciadv.adj4196
7. Reddan MC, Wager TD. Modeling pain using fMRI: from regions to biomarkers. Neurosci Bull. 2018;34:208–215. doi:10.1007/s12264-017-0150-1
8. Chen Y, Xiang C-Q, Liu W-F, et al. Application of amplitude of low‑frequency fluctuation to altered spontaneous neuronal activity in classical trigeminal neuralgia patients: a resting‑state functional MRI study. Mol Med Rep. 2019;20:1707–1715. doi:10.3892/mmr.2019.10404
9. Wang Y, Zhang X, Guan Q, Wan L, Yi Y, Liu C-F. Altered regional homogeneity of spontaneous brain activity in idiopathic trigeminal neuralgia. Neuropsychiatr Dis Treat. 2015;11:2659–2666. doi:10.2147/NDT.S94877
10. Tsai Y-H, Yuan R, Patel D, et al. Altered structure and functional connection in patients with classical trigeminal neuralgia. Hum Brain Mapp. 2018;39:609–621. doi:10.1002/hbm.23696
11. Zhang P, Jiang Y, Liu G, et al. Altered brain functional network dynamics in classic trigeminal neuralgia: a resting-state functional magnetic resonance imaging study. J Headache Pain. 2021;22:147. doi:10.1186/s10194-021-01354-z
12. Xu H, Seminowicz DA, Krimmel SR, Zhang M, Gao L, Wang Y. Altered structural and functional connectivity of salience network in patients with classic trigeminal neuralgia. J Pain. 2022;23:1389–1399. doi:10.1016/j.jpain.2022.02.012
13. Turkeltaub PE, Eden GF, Jones KM, Zeffiro TA. Meta-analysis of the functional neuroanatomy of single-word reading: method and validation. Neuroimage. 2002;16:765–780. doi:10.1006/nimg.2002.1131
14. Olesen J. International classification of headache disorders. Lancet Neurol. 2018;17:396–397. doi:10.1016/S1474-4422(18)30085-1
15. Mazziotta JC, Toga AW, Evans A, Fox P, Lancaster J. A probabilistic atlas of the human brain: theory and rationale for its development. The international consortium for brain mapping (ICBM). Neuroimage. 1995;2:89–101. doi:10.1006/nimg.1995.1012
16. Zhang W, Sun B, Zhang C, et al. Altered amplitude of low-frequency fluctuation of the brain regions associated with pain symptoms and negative emotion in trigeminal neuralgia. World Neurosurg. 2025;197:123875. doi:10.1016/j.wneu.2025.123875
17. Wang Z, Li Z, Zhou G, et al. Graph theory-driven structural and functional connectivity analyses revealing regulatory mechanisms of brain network in patients with classic trigeminal neuralgia. Brain Imaging Behav. 2024. doi:10.1007/s11682-024-00915-5
18. Deng X, Liu L, Chen J, Liu Z, Feng H. Cognitive decline in patients with trigeminal neuralgia: a resting-state fMRI study. Brain Behav. 2025;15:e70434.
19. Turkeltaub PE, Eickhoff SB, Laird AR, Wiener M, Fox M, Fox P. Minimizing within-experiment and within-group effects in Activation Likelihood Estimation meta-analyses. Hum Brain Mapp. 2012;33:1–13. doi:10.1002/hbm.21186
20. Eickhoff SB, Laird AR, Grefkes C, Wang LE, Zilles K, Fox PT. Coordinate-based activation likelihood estimation meta-analysis of neuroimaging data: a random-effects approach based on empirical estimates of spatial uncertainty. Hum Brain Mapp. 2009;30:2907–2926. doi:10.1002/hbm.20718
21. Eickhoff SB, Bzdok D, Laird AR, Kurth F, Fox PT. Activation likelihood estimation meta-analysis revisited. Neuroimage. 2012;59:2349–2361. doi:10.1016/j.neuroimage.2011.09.017
22. Robinson JL, Laird AR, Glahn DC, Lovallo WR, Fox PT. Metaanalytic connectivity modeling: delineating the functional connectivity of the human amygdala. Hum Brain Mapp. 2010;31:173–184. doi:10.1002/hbm.20854
23. Robinson JL, Laird AR, Glahn DC, et al. The functional connectivity of the human caudate: an application of meta-analytic connectivity modeling with behavioral filtering. Neuroimage. 2012;60:117–129. doi:10.1016/j.neuroimage.2011.12.010
24. Ge X, Wang L, Yan J, et al. Altered brain function in classical trigeminal neuralgia patients: ALFF, ReHo, and DC static- and dynamic-frequency study. Cereb Cortex. 2024;34:bhad455.
25. Wang Y, Xu C, Zhai L, et al. Spatial-temporal signature of resting-state BOLD signals in classic trigeminal neuralgia. J Pain Res. 2017;10:2741–2750. doi:10.2147/JPR.S143734
26. Yuan J, Cao S, Huang Y, et al. Altered spontaneous brain activity in patients with idiopathic trigeminal neuralgia: a resting-state functional MRI study. Clin J Pain. 2018;34:600–609. doi:10.1097/AJP.0000000000000578
27. Xiang C-Q, Liu W-F, Xu Q-H, et al. Altered spontaneous brain activity in patients with classical trigeminal neuralgia using regional homogeneity: a resting-state functional MRI study. Pain Pract. 2019;19:397–406. doi:10.1111/papr.12753
28. Zhang Y, Mao Z, Pan L, et al. Frequency-specific alterations in cortical rhythms and functional connectivity in trigeminal neuralgia. Brain Imag Behav. 2019;13:1497–1509. doi:10.1007/s11682-019-00105-8
29. Zhu P-W, Chen Y, Gong Y-X, et al. Altered brain network centrality in patients with trigeminal neuralgia: a resting-state fMRI study. Acta Radiol. 2020;61:67–75. doi:10.1177/0284185119847678
30. Liu H, Hou H, Li F, et al. Structural and functional brain changes in patients with classic trigeminal neuralgia: a combination of voxel-based morphometry and resting-state functional MRI study. Front Neurosci. 2022;16:930765. doi:10.3389/fnins.2022.930765
31. Wang Z, Zhao Z, Song Z, et al. Functional alterations of the brain default mode network and somatosensory system in trigeminal neuralgia. Sci Rep. 2024;14:10205. doi:10.1038/s41598-024-60273-6
32. Liu H, Zheng R, Zhang Y, et al. Alterations of degree centrality and functional connectivity in classic trigeminal neuralgia. Front Neurosci. 2023;16:1090462. doi:10.3389/fnins.2022.1090462
33. Zhang Y, Mao Z, Pan L, et al. Dysregulation of pain- and emotion-related networks in trigeminal neuralgia. Front Hum Neurosci. 2018;12:107. doi:10.3389/fnhum.2018.00107
34. Wu M, Qiu J, Chen Y, Jiang X. Stratifying trigeminal neuralgia and characterizing an abnormal property of brain functional organization: a resting-state fMRI and machine learning study. J Neurosurg. 2025;143:74–82. doi:10.3171/2024.11.JNS241935
35. Nardoni L, Tullo MG, Stefano GD, Fiorelli M, Caramia F. Structural brain alterations and changes in resting-state functional connectivity in patients with trigeminal neuralgia: a meta-analysis. Neuroimage Clin. 2025;46:103759. doi:10.1016/j.nicl.2025.103759
36. Zhu T, Wang Z, Wu W, et al. Altered brain functional networks in schizophrenia with persistent negative symptoms: an activation likelihood estimation meta-analysis. Front Hum Neurosci. 2023;17:1204632. doi:10.3389/fnhum.2023.1204632
37. Thompson JM, Neugebauer V. Cortico-limbic pain mechanisms. Neurosci Lett. 2019;702:15–23. doi:10.1016/j.neulet.2018.11.037
38. Kang D, McAuley JH, Kassem MS, Gatt JM, Gustin SM. What does the grey matter decrease in the medial prefrontal cortex reflect in people with chronic pain? Eur J Pain. 2019;23:203–219. doi:10.1002/ejp.1304
39. Yang S, Chang MC. Chronic pain: structural and functional changes in brain structures and associated negative affective states. IJMS. 2019;20:3130. doi:10.3390/ijms20133130
40. Zhang W, Sun B, Zhang C, et al. Altered ALFF of the brain regions associated with pain symptoms and negative emotion in trigeminal neuralgia. World Neurosurg. 2025;197:123875.
41. Meylakh N, Crawford LS, Mills EP, et al. Altered corticobrainstem connectivity during spontaneous fluctuations in pain intensity in painful trigeminal neuropathy. eNeuro. 2024;11:ENEURO.0522–23.2024.
42. Tanglay O, Young IM, Dadario NB, et al. Anatomy and white-matter connections of the precuneus. Brain Imaging Behav. 2022;16:574–586. doi:10.1007/s11682-021-00529-1
43. Watanabe M, Shrivastava RK, Balchandani P. Advanced neuroimaging of the trigeminal nerve and the whole brain in trigeminal neuralgia: a systematic review. Pain. 2024.
44. de Lussanet MHE, Behrendt F, Puta C, et al. Impaired visual perception of hurtful actions in patients with chronic low back pain. Hum Mov Sci. 2013;32:938–953. doi:10.1016/j.humov.2013.05.002
45. Parise M, Kubo TTA, Doring TM, Tukamoto G, Vincent M, Gasparetto EL. Cuneus and fusiform cortices thickness is reduced in trigeminal neuralgia. J Headache Pain. 2014;15:17. doi:10.1186/1129-2377-15-17
46. Borsook D, Moulton EA, Tully S, Schmahmann JD, Becerra L. Human cerebellar responses to brush and heat stimuli in healthy and neuropathic pain subjects. Cerebellum. 2008;7:252–272. doi:10.1007/s12311-008-0011-6
47. Moulton EA, Schmahmann JD, Becerra L, Borsook D. The cerebellum and pain: passive integrator or active participator? Brain Res Rev. 2010;65:14–27. doi:10.1016/j.brainresrev.2010.05.005
48. Moulton EA, Elman I, Pendse G, Schmahmann J, Becerra L, Borsook D. Aversion-related circuitry in the cerebellum: responses to noxious heat and unpleasant images. J Neurosci. 2011;31:3795–3804. doi:10.1523/JNEUROSCI.6709-10.2011
49. Li CN, Keay KA, Henderson LA, Mychasiuk R. Re-examining the mysterious role of the cerebellum in pain. J Neurosci. 2024;44:e1538232024.
50. Lanz S, Seifert F, Maihöfner C. Brain activity associated with pain, hyperalgesia and allodynia: an ALE meta-analysis. J Neural Transm. 2011;118:1139–1154. doi:10.1007/s00702-011-0606-9
51. Jensen KB, Regenbogen C, Ohse MC, Frasnelli J, Freiherr J, Lundström JN. Brain activations during pain: a neuroimaging meta-analysis of patients with pain and healthy controls. Pain. 2016;157:1279–1286. doi:10.1097/j.pain.0000000000000517
52. Xu A, Larsen B, Henn A, et al. Brain responses to noxious stimuli in patients with chronic pain: a systematic review and meta-analysis. JAMA Network Open. 2021;4:e2032236.
53. Alshelh Z, Di Pietro F, Youssef AM, et al. Chronic neuropathic pain: it’s about the rhythm. J Neurosci. 2016;36:1008–1018. doi:10.1523/JNEUROSCI.2768-15.2016
54. Szabo E, Chang Y-HC, Shulman J, et al. Alterations in the structure and function of the brain in adolescents with new daily persistent headache: a pilot MRI study. Headache. 2022;62:858–869. doi:10.1111/head.14360
55. Mehnert J, Schulte L, Timmann D, May A. Activity and connectivity of the cerebellum in trigeminal nociception. Neuroimage. 2017;150:112–118. doi:10.1016/j.neuroimage.2017.02.023
56. Binding LP, Dasgupta D, Giampiccolo D, Duncan JS, Vos SB. Structure and function of language networks in temporal lobe epilepsy. Epilepsia. 2022;63:1025–1040. doi:10.1111/epi.17204
57. Trimmel K, Vos SB, Caciagli L, et al. Decoupling of functional and structural language networks in temporal lobe epilepsy. Epilepsia. 2021;62:2941–2954. doi:10.1111/epi.17098
58. Meletti S, Tassi L, Mai R, Fini N, Tassinari CA, Russo GL. Emotions induced by intracerebral electrical stimulation of the temporal lobe. Epilepsia. 2006;47 Suppl 5:47–51. doi:10.1111/j.1528-1167.2006.00877.x
59. Tanner JJ, Hanchate S, Price CC, et al. Relationships between chronic pain stage, cognition, temporal lobe cortex, and sociodemographic variables. J Alzheimers Dis. 2021;80:1539–1551. doi:10.3233/JAD-201345
60. Ge X, Wang L, Pan L, et al. Alteration of the cortical morphology in classical trigeminal neuralgia: voxel-, deformation-, and surface-based analysis. J Headache Pain. 2023;24:17. doi:10.1186/s10194-023-01544-x
61. Zeng X, Sun Y, Zhiying Z, Hua L, Yuan Z. Chronic pain-induced functional and structural alterations in the brain: a multi-modal meta-analysis. J Pain. 2025;28:104740. doi:10.1016/j.jpain.2024.104740
62. Obermann M, Rodriguez-Raecke R, Naegel S, et al. Gray matter volume reduction reflects chronic pain in trigeminal neuralgia. Neuroimage. 2013;74:352–358. doi:10.1016/j.neuroimage.2013.02.029
63. Vachon-Presseau E, Centeno MV, Ren W, et al. The emotional brain as a predictor and amplifier of chronic pain. J Dent Res. 2016;95:605–612. doi:10.1177/0022034516638027
64. McCarberg B, Peppin J. Pain pathways and nervous system plasticity: learning and memory in pain. Pain Med. 2019;20:2421–2437. doi:10.1093/pm/pnz017
65. Wang Y, Cao D, Remeniuk B, Krimmel S, Seminowicz DA, Zhang M. Altered brain structure and function associated with sensory and affective components of classic trigeminal neuralgia. Pain. 2017;158:1561–1570. doi:10.1097/j.pain.0000000000000951
66. Yu X, Lv W, Liu X, Kang X, Zhang L. Abnormal activation of brain regions in idiopathic trigeminal neuralgia patients by fMRI: an activation likelihood estimation meta-analysis. Clin Neurol Neurosurg. 2023;228:107710. doi:10.1016/j.clineuro.2023.107710
67. Zhang P, Wan X, Ai K, et al. Rich-club reorganization and related network disruptions are associated with the symptoms and severity in classic trigeminal neuralgia patients. Neuroimage Clin. 2022;36:103160. doi:10.1016/j.nicl.2022.103160
68. Li L, Du H, Li X-Y, et al. A study of brain function changes in patients with trigeminal neuralgia of different laterality based on rs-fMRI. J Oral Facial Pain Headache. 2025;39:148–156. doi:10.22514/jofph.2025.015
69. Günther T, Gerganov VM, Stieglitz L, Ludemann W, Samii A, Samii M. Microvascular decompression for trigeminal neuralgia in the elderly: long-term treatment outcome and comparison with younger patients. Neurosurgery. 2009;65:477–482. [discussion 482]. doi:10.1227/01.NEU.0000350859.27751.90
70. Spatz AL, Zakrzewska JM, Kay EJ. Decision analysis of medical and surgical treatments for trigeminal neuralgia: how patient evaluations of benefits and risks affect the utility of treatment decisions. Pain. 2007;131:302–310. doi:10.1016/j.pain.2007.02.009
71. Wang DD, Raygor KP, Cage TA, et al. Prospective comparison of long-term pain relief rates after first-time microvascular decompression and stereotactic radiosurgery for trigeminal neuralgia. J Neurosurg. 2018;128:68–77. doi:10.3171/2016.9.JNS16149
72. Greve T, Tonn J-C, Mehrkens J-H. Microvascular decompression for trigeminal neuralgia in the elderly: efficacy and safety. J Neurol. 2021;268:532–540. doi:10.1007/s00415-020-10187-w
73. Raygor KP, Lee AT, Nichols N, et al. Long-term pain outcomes in elderly patients with trigeminal neuralgia: comparison of first-time microvascular decompression and stereotactic radiosurgery. Neurosurg Focus. 2020;49:E23.
74. Andersen ASS, Heinskou TB, Rochat P, et al. Microvascular decompression in trigeminal neuralgia - a prospective study of 115 patients. J Headache Pain. 2022;23:145. doi:10.1186/s10194-022-01520-x
75. Lee A, McCartney S, Burbidge C, Raslan AM, Burchiel KJ. Trigeminal neuralgia occurs and recurs in the absence of neurovascular compression. J Neurosurg. 2014;120:1048–1054. doi:10.3171/2014.1.JNS131410
76. Danyluk H, Lang S, Monchi O, Sankar T. Pre-operative limbic system functional connectivity distinguishes responders from non-responders to surgical treatment for trigeminal neuralgia. Front Neurol. 2021;12:716500. doi:10.3389/fneur.2021.716500
77. Desouza DD, Moayedi M, Chen DQ, Davis KD, Hodaie M. Sensorimotor and pain modulation brain abnormalities in trigeminal neuralgia: a paroxysmal, sensory-triggered neuropathic pain. PLoS One. 2013;8:e66340.
78. DeSouza DD, Hodaie M, Davis KD. Diffusion imaging in trigeminal neuralgia reveals abnormal trigeminal nerve and brain white matter. Pain. 2014;155:1905–1906. doi:10.1016/j.pain.2014.05.026
79. Davis KD. Imaging vs quantitative sensory testing to predict chronic pain treatment outcomes. Pain. 2019;160(1):S59–65.
80. Mu J, Chen T, Quan S, Wang C, Zhao L, Liu J. Neuroimaging features of whole-brain functional connectivity predict attack frequency of migraine. Hum Brain Mapp. 2020;41:984–993. doi:10.1002/hbm.24854
81. Xi L, Liu X, Shi H, et al. Comparative safety and efficacy of percutaneous radiofrequency thermocoagulation and percutaneous balloon compression in CT-guided and local anesthesia for recurrent trigeminal neuralgia. Front Neurol. 2023;14:1336261. doi:10.3389/fneur.2023.1336261
82. Gupta M, Sagi V, Mittal A, et al. Results of three or more gamma knife radiosurgery procedures for recurrent trigeminal neuralgia. J Neurosurg. 2021;135:1789–1798. doi:10.3171/2020.10.JNS202323
83. Fan X, Xu F, Ren H, et al. The analysis of percutaneous balloon compression on efficacy and negative emotion in the treatment of recurrent trigeminal neuralgia after surgical procedures. Pain Physician. 2021;24:E1255–62.
84. Fregni F, Freedman S, Pascual-Leone A. Recent advances in the treatment of chronic pain with non-invasive brain stimulation techniques. Lancet Neurol. 2007;6:188–191. doi:10.1016/S1474-4422(07)70032-7
85. Knotkova H, Hamani C, Sivanesan E, et al. Neuromodulation for chronic pain. Lancet. 2021;397:2111–2124. doi:10.1016/S0140-6736(21)00794-7
86. Babakhani B, Tabatabaei NH, Elisevich K, et al. A preliminary study of the efficacy of transcranial direct current stimulation in trigeminal neuralgia. Front Hum Neurosci. 2022;16:848347. doi:10.3389/fnhum.2022.848347
87. Freigang S, Fresnoza S, Lehner C, et al. Twenty-three months repetitive transcranial magnetic stimulation of the primary motor cortex for refractory trigeminal neuralgia: a single-case study. Life. 2023;13:126. doi:10.3390/life13010126
88. Säisänen L, Huttunen J, Hyppönen J, et al. Efficacy and tolerability in patients with chronic facial pain of two consecutive treatment periods of rTMS applied over the facial motor cortex, using protocols differing in stimulation frequency, duration, and train pattern. Neurophysiol Clin. 2022;52:95–108. doi:10.1016/j.neucli.2022.03.001
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.