Back to Journals » Journal of Inflammation Research » Volume 14
A Web-Based Survey on Factors for Unvaccination and Adverse Reactions of SARS-CoV-2 Vaccines in Chinese Patients with Psoriasis
Authors Wang Q ![]() , Lv C, Han X, Shen M
, Lv C, Han X, Shen M ![]() , Kuang Y
, Kuang Y
Received 26 September 2021
Accepted for publication 15 November 2021
Published 27 November 2021 Volume 2021:14 Pages 6265—6273
DOI https://doi.org/10.2147/JIR.S341429
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Monika Sharma
Qiaolin Wang,1– 3 Chengzhi Lv,4 Xi Han,5 Minxue Shen,1– 3,6 Yehong Kuang1– 3
1Department of Dermatology, Xiangya Hospital, Central South University, Changsha, Hunan, People’s Republic of China; 2National Clinical Research Center for Geriatric Disorders (Xiangya Hospital), Changsha, Hunan, People’s Republic of China; 3Hunan Engineering Research Center of Skin Health and Disease; Hunan Key Laboratory of Skin Cancer and Psoriasis (Xiangya Hospital), Changsha, Hunan, People’s Republic of China; 4Department of Psoriasis, Dalian Dermatosis Hospital, Dalian, Liaoning, People’s Republic of China; 5ULink College Guangzhou, Guangzhou, Guangdong, People’s Republic of China; 6Department of Social Medicine and Health Management, Xiangya School of Public Health, Central South University, Changsha, Hunan, People’s Republic of China
Correspondence: Minxue Shen
Department of Social Medicine and Health Management, Xiangya School of Public Health, Central South University, 87 Xiangya Road, Changsha, Hunan, People’s Republic of China
Email [email protected]
Yehong Kuang
Department of Dermatology, Xiangya Hospital, Central South University, 87 Xiangya Road, Changsha, Hunan, People’s Republic of China
Email [email protected]
Purpose: Vaccination is one of the most important strategy to prevent infections and control epidemics, but it also raises concerns about safety in patients receiving treatments. This study aimed to investigate the rate and factors for unvaccination, as well as adverse reactions and deterioration of disease after SARS-CoV-2 vaccination in psoriatic patients.
Methods: A web-based questionnaire survey on SARS-CoV-2 vaccination, adverse reactions, and self-reported change of disease condition after vaccination in patients with psoriasis was conducted. Demographic, clinical, and psychological data were collected. Multivariable logistic regression was used in the estimation of associations.
Results: A total of 788 psoriatic patients were investigated, and 68.9% reported SARS-CoV-2 vaccination. Younger age, use of interleukin-17 inhibitors, and symptoms of anxiety were associated with unvaccination. The incidence of overall adverse reactions after vaccination was 30.8%, and no severe adverse reaction was reported. The most common local and systemic adverse reactions were pain at the injection site and fatigue, respectively. Most patients reported no change in psoriasis after vaccination, while 16.6% and 4.4% reported slight and significant deteriorations of the disease, respectively. Nonadherence to treatment, symptoms of anxiety and depression, and perceived stress were associated with self-reported deterioration of psoriasis after vaccination.
Conclusion: While a favorable safety profile of SARS-CoV-2 vaccines is observed, receiving biologic treatment is factor for unvaccination in patients with psoriasis. Deterioration of psoriasis reported by a small proportion of patients is partially attributable to mental and behavioral factors.
Keywords: COVID-19, SARS-CoV-2, vaccine, unvaccination, psoriasis, safety, adverse reaction
Introduction
Psoriasis is a chronic inflammatory skin disorder linked to genetic, immunologic, metabolic, and environmental factors,1,2 with an increased risk of infections because of the disease itself or the use of immunosuppressive drugs.3,4 Coronavirus disease 2019 (COVID-19), caused by the novel coronavirus SARS-CoV-2, has spread worldwide, and raised a number of concerns among patients with psoriasis. SARS-CoV-2 vaccination has became one of the most important strategy to prevent the infection and control the pandemic. At the time of data collection, more than 70% Chinese completed the vaccination for SARS-CoV-2, at least five different COVID-19 vaccines, mainly consisting of inactivated and protein subunit vaccine, have been approved for emergency use in China, and a strong willingness to vaccinate in general population was reported by several cross-sectional studies.5,6 Although psoriasis is not a contraindication for many vaccinations of infectious diseases, the vaccination rate in patients with psoriasis remains low owing to the concerns about the safety of vaccines and unawareness of the risk of infection.3,7 Although evidence is limited, some case series recently reported psoriasis flare-up linked to SARS-CoV-2 vaccination.8,9 However, studies systematically investigated adverse reactions after vaccination for SARS-CoV-2 in psoriatic patients are scarce. Real-world data is urgently needed to address public concerns on the side effects of the vaccines.
The purpose of the current study is to investigate the rate and factors for SARS-CoV-2 vaccination, as well as the adverse reactions and changes of psoriasis conditions after vaccination in a real-world setting.
Methods
Study Design and Population
A web-based cross-sectional study was conducted in a group of Chinese patients with psoriasis. We developed a self-administered online survey for the collection of questionnaires. The survey link was created through Wen-Juan-Xing platform (Changsha Ranxing Information Technology Co., Ltd., Hunan, China), the largest online survey platform in China. Our study population was psoriatic patients in social media platforms (WeChat groups and teledermatology platforms) no matter whether they completed SARS-CoV-2 vaccination. Patients with a confirmed diagnosis of psoriasis in dermatology clinics were introduced by their dermatologists to the platforms for the purposes of health management and follow-up.10,11 We posted the link on the platforms without any incentive measures when they anonymously completed the survey. All participants can submit the questionnaire only once based on their IP addresses. For the purpose of quality control, the questionnaire cannot be submitted unless all required questions have been answered. This survey was conducted between 22 Jul 2021 and 3 Aug 2021. Electronic informed consents were obtained from all patients before the investigation. This study adhered to the Declaration of Helsinki and was approved by the institutional research ethics boards of Xiangya Hospital, Central South University (Changsha, China).
Questionnaires
We developed the questionnaire based on our previous study that investigated the impact of COVID-19 pandemic on the outcomes of psoriatic patients,11 and made modifications according to the purpose of current study. We revised the questionnaire after a consultation with epidemiologists and dermatologists.
To investigate the rate of SARS-CoV-2 vaccination, a single question “have you completed the vaccination for SARS-CoV-2?” was asked first, followed by the type of vaccine. Reasons for unvaccination were then investigated, with the following responses: “a lack of vaccines supply”, “concern about psoriasis deterioration after vaccination”, “concern about adverse reactions of the vaccine”, “concern about interactions between the vaccine and treatment for psoriasis”, “having other disease that is a contraindication”, “not recommended for vaccination owing to severe psoriasis”, “not in the range of vaccination age”, “unnecessary to be vaccinated because of good control of pandemic”, and “other reasons”.
Factors for unvaccination included gender, age, educational level, marital status, metabolic comorbidities (hypertension, hyperlipidemia, diabetes, and gout), clinical type of psoriasis, body surface area (BSA) of psoriatic lesions (self-rated palm size, ≤3%, 3–10%, >10%), course of psoriasis (<1 year, 1–5 years, >5 years), current treatment including the use of interleukin-17 (IL-17) inhibitors, and psychological symptoms were collected. Symptoms of depression and anxiety were measured by the two-item Patient Health Questionnaire (PHQ-2) and the two-item Generalized Anxiety Disorder (GAD-2) respectively with 3 as the cut-off point for both scales.12,13 Perceived stress was measured by a visual analogue scale (VAS) with 0–10 as the range, significant perceived stress was defined as the cutoff ≥7 in this study.10,14,15
Adverse reactions after SARS-CoV-2 vaccination, included local and systemic reactions, were measured by a single question that allows multiple answers “Did you have any adverse reactions after the vaccination”, with several responses according to related clinical trials.
The deterioration of psoriasis after SARS-CoV-2 vaccination was measured by the Global Rating of Change (GRC). We used a single question “Is there any changes in your condition of psoriasis since the SARS-CoV-2 vaccination” with the 5-graded Likert responses: significant deterioration, slight deterioration, no change, slight alleviation, significant alleviation. Self-reported significant and slight deterioration was defined as the endpoint for analysis.
To investigate factors for the changes of psoriasis conditions, psychological factors (described above), current treatment for psoriasis, and adherence to the treatment were asked. Adherence to the treatment was assessed by a simple question “Have you been adhered to the medication or treatment for psoriasis prescribed by your dermatologist before and after the vaccination”. Nonadherence to treatment was defined as discontinuing therapies before or after the vaccination.
Sample Size Estimation
According to the empirical estimation, a sample size of 5–10 times the number of variables is required for multivariable regression. With 13 variables potentially associated with unvaccination in our study, 130 patients with unvaccination are required to avoid the violation of the principle of approximately ten outcome events per variable in the regression.16 Since more than 70% Chinese completed the vaccination for SARS-CoV-2 at the time of data collection, we expected to reach a minimum sample size of 130/(1–0.7) = 434.
Statistical Analysis
Categorical variables including demographic and clinical information, adverse reactions, and other patient-reported outcomes were displayed as counts (percentages) and compared using the chi-square test or Fisher’s exact test. Continuous variables with normal distribution were expressed as mean ± standard deviation (SD) and compared with analysis of variance (ANOVA). Multivariable logistic regression was used to identify factors for unvaccination (y/n), while disordered multinomial logistic regression was used to investigate factors for the deterioration psoriasis (three categories) after vaccination, and adjusted odds ratio (aOR) and 95% confidence interval (CI) were presented as the effect sizes. All data were analyzed with SPSS 23 (IBM, SPSS Statistics 23). P value < 0.05 was considered statistically significant.
Results
A total of 788 valid questionnaires were collected. The mean age of the participants was 40.2 ± 12.3 years, and 38.5% were female. Five hundred and forty-three (68.9%) completed SARS-CoV-2 vaccination, among whom 486 (89.5%) received inactivated vaccine, 45 (8.3%) received protein subunit vaccine, and 12 (2.2%) received adenovirus vector vaccine. Characteristics of the patients between unvaccinated and vaccinated for SARS-CoV-2 are shown in Table 1. Significant differences between the groups were identified for age, educational level, marital status, type of psoriasis, BSA of skin lesion, use of IL-17 inhibitors, symptoms of anxiety and depression, and perceived stress.
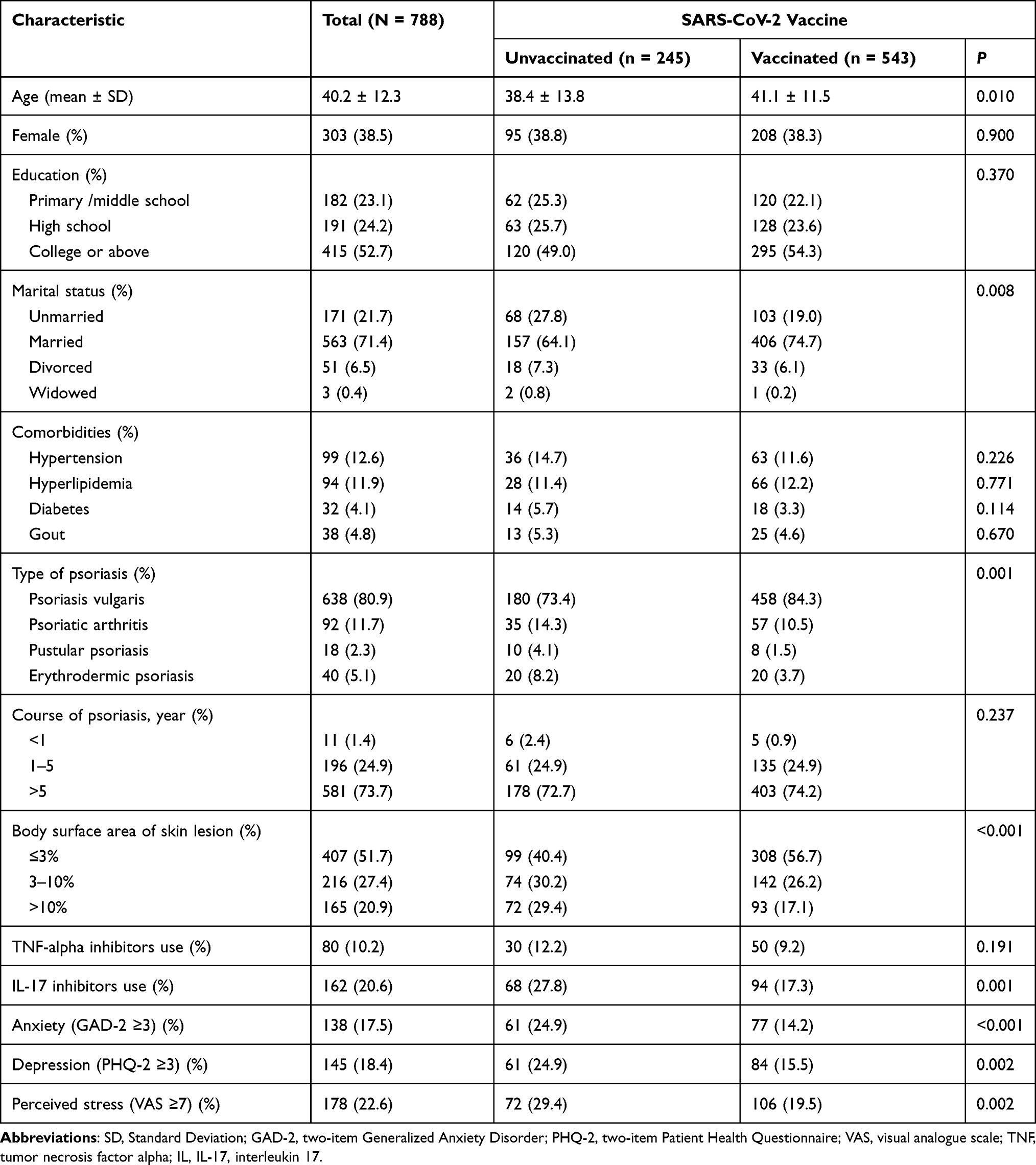 |
Table 1 Characteristics of Patients Vaccinated and Unvaccinated for SARS-CoV-2 |
In the 245 participants who were not vaccinated, the top three reasons for their decision included concerns about psoriasis deterioration after vaccination (53.9%), interactions between the vaccines with treatment for psoriasis (33.1%), and adverse reactions of the vaccines (26.1%). We then performed logistic regressions with adjustments, and identified age (aOR = 0.97; 95% CI: 0.96–0.99), type of psoriasis, severity of psoriasis (aOR = 1.84 for BSA > 3; aOR = 2.79 for BSA > 10), use of IL-17 inhibitors (aOR = 1.77; 95% CI: 1.21–2.58), and symptoms of anxiety (aOR = 1.65; 95% CI: 1.10–2.46) as significant factors for unvaccination (Table 2). Patients with psoriatic arthritis (aOR = 2.05), pustular psoriasis (aOR = 3.03), or erythrodermic psoriasis (aOR = 2.28) were less likely to be vaccinated compared with psoriasis vulgaris.
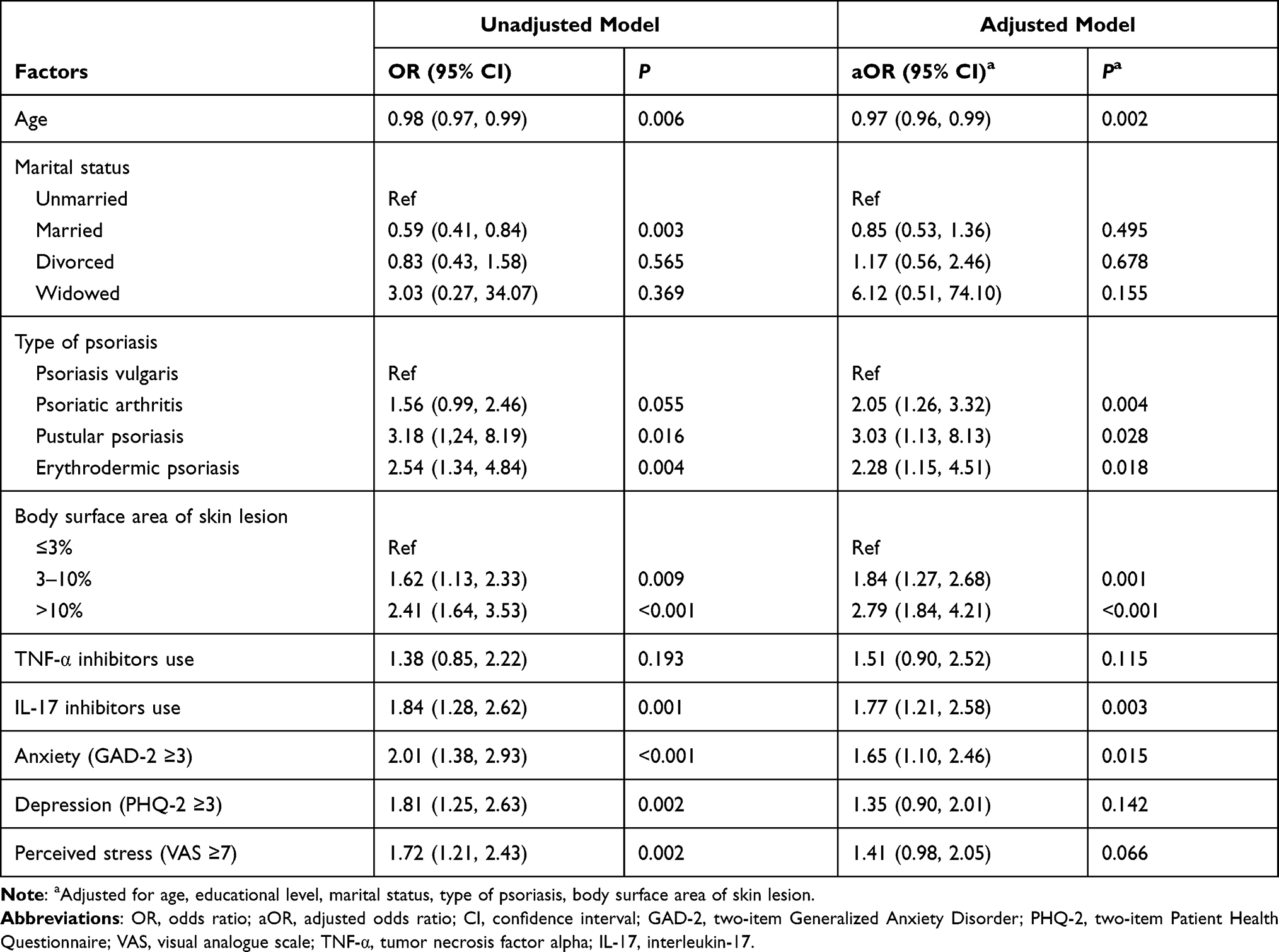 |
Table 2 Factors for Unvaccination in Patients with Psoriasis |
Table 3 shows adverse reactions post vaccination by types of vaccination and treatment for psoriasis. The overall incidence of adverse reactions was 30.8% (167/543), and 23.0% and 16.4% for local and systemic reactions, respectively. No severe adverse reaction was reported. The most common local adverse reaction was pain at the injection site (20.1%), accounting for 68.3% of overall adverse reactions, followed by induration and swelling (2.8%), and itch and redness (1.1%). The most frequent systemic adverse reaction was fatigue (8.5%), followed by rash and itch (4.4%), stuffy and runny nose (2.6%), and headache (2.0%). In addition, the inactivated vaccine and protein subunit vaccine showed similar profiles of adverse reactions. Use of biologics (27.2%) was not associated with an increased incidence of adverse reactions compared to those receiving traditional (25.6%) or topical therapies (37.9%), or no treatment (27.3%).
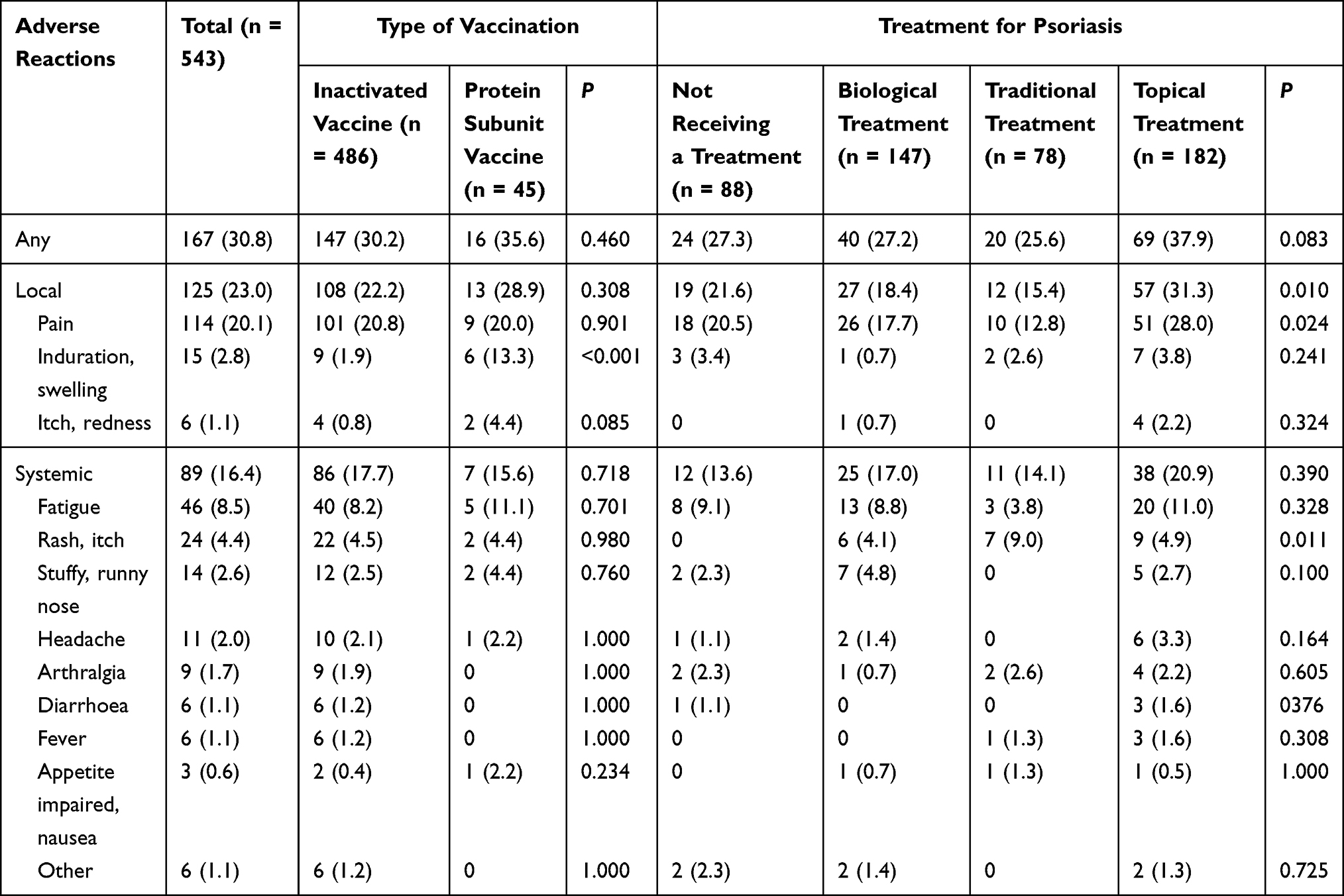 |
Table 3 Adverse Reactions After Vaccination by the Type of Vaccines and Treatment for Psoriasis |
Changes of psoriasis condition after vaccination stratified by the type of vaccines and therapies for psoriasis are shown in Figure 1. Most reported no change, while 16.6% and 4.4% reported slight and significant deteriorations, respectively, and 4.6% reported alleviation after the vaccination. Patients receiving biologics were less likely to report deteriorations after vaccination compared with those receiving traditional or topical treatments. Further analysis in Table 4 indicates nonadherence to the treatment (aOR for slight deterioration [aORsli] = 2.02 vs for significant deterioration [aORsig] = 2.42), symptoms of anxiety (aORsli= 2.67 vs aORsig= 5.06) and depression (aORsli= 2.33 vs aORsig= 3.90), and perceived stress (aORsli= 2.19 vs aORsig= 2.38) were dose-dependently associated with the deterioration of psoriasis. Use of IL-17 inhibitors showed a strong protective effect on the deterioration of psoriasis (aORsig= 0.17) after vaccination with a marginal significance (P = 0.085).
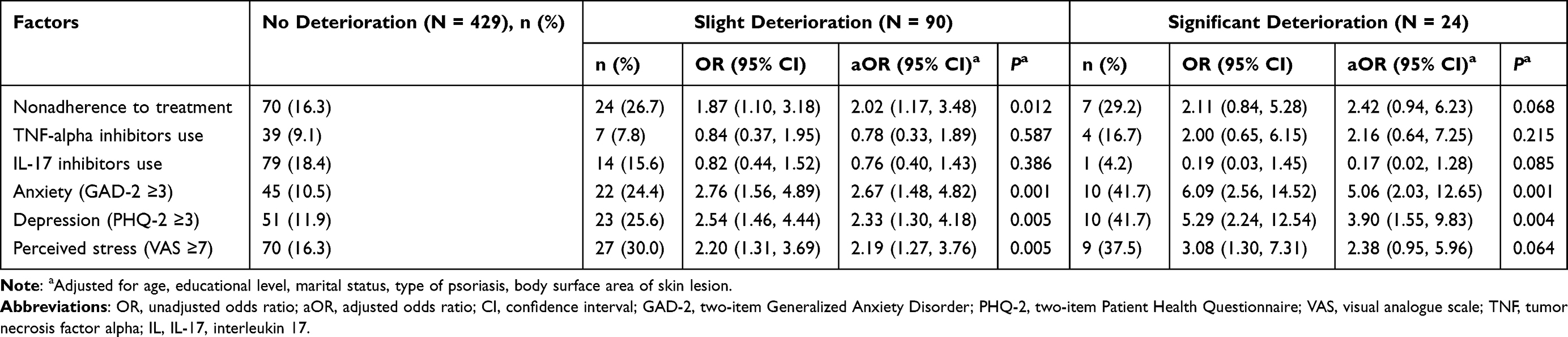 |
Table 4 Factors for Deterioration of Psoriasis After Vaccination |
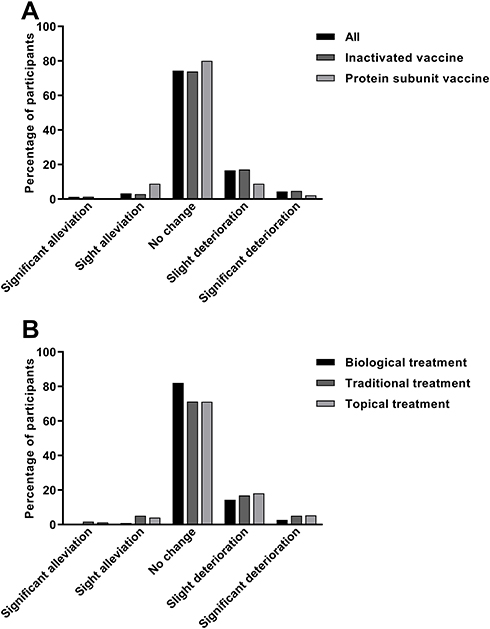 |
Figure 1 Changes of psoriasis condition after vaccination, stratified by (A) type of vaccines and (B) treatment for psoriasis. |
Discussion
We conducted a cross-sectional study through social media and reported a high vaccination rate of 68.9% for SARS-CoV-2 in a group of Chinese patients with psoriasis. We found that younger age, use of IL-17 inhibitors, type and severity of psoriasis, and symptoms of anxiety were significantly associated with unvaccination. The overall incidence of adverse reactions was 30.8% after the vaccination for SARS-CoV-2, and no severe adverse reaction was reported. The use of biologics in the treatment of psoriasis was not associated with increased risks of adverse reactions. Some patients reported a deterioration of psoriasis after the vaccination, which is partially attributable to psychological factors and nonadherence to the treatment.
Patients with immune-mediated inflammatory diseases might refuse the vaccination because of the concerns about side effects of the vaccines, resulting in a low vaccination rate.3 A recent study showed that younger age, biological treatment, and a history of chronic disease seemingly contributed to the vaccination for SARS-CoV-2, which might be driven by heightened health awareness and risk perception.17 In contrast, we found that patients of a younger age or receiving a treatment with IL-17 inhibitors were less likely to get vaccinated. Patients with comorbidities or receiving therapeutic immunosuppressants were usually excluded from clinical trials of the vaccines, and the lack of information about the safety and efficacy of the vaccines in certain groups of patients is likely to cause a low vaccination rate. We also recognized that patients with anxiety, moderate-to-severe psoriasis (BSA > 3), and certain types of psoriasis were more reluctant to be vaccinated. These findings consistently indicate that the willingness to accept the vaccination is compromised by a stronger disease severity, more tissues involved, and novel treatments received. Trials as well as health education are needed to address public concerns about the safety of the vaccines.
We reported an overall incidence of adverse reactions of 30.8% after the vaccination, which was slightly higher than the data from clinical trials. The rates of adverse reactions related to inactivated SARS-CoV-2 vaccine, BBIBP-CorV, was 29% in Phase 1 and 23% in Phase 2, respectively.18 Another trial of China-made inactivated SARS-CoV-2 vaccine, CoronaVac (Sinovac Life Sciences, Beijing, China), reported an incidence of adverse events of 33–35% in phase 2 and 18.9% in Phase 3.19,20 Phase 1/2 clinical trials of the protein subunit SARS-CoV-2 vaccine also confirmed good tolerance and immunogenicity.21 Skin-related adverse events caused by SARS-CoV-2 vaccines in the trials included local pain, induration, swelling, itch, redness, and systemic rash, etc. Previous study also reported delayed injection site reaction associated with SARS-CoV-2 vaccines made by other manufacturers.22,23 Interestingly, the risk of adverse reactions in patients receiving biologics was not significantly higher than those under traditional or topical therapies in our study. Consistent findings were reported by an observational study that evaluated the safety of SARS-CoV-2 vaccines in psoriatic patients treated with biologics.24 We advocate that psoriatic patients on biological and conventional treatments should get vaccinated for SARS-CoV-2 as soon as possible, because delayed vaccination may place the vulnerable group at an increased risk of infection.25
While most participants reported no change of psoriasis after the vaccination, some claimed deteriorations. Although vaccines are infrequent factors for the aggravation of psoriasis, several case series reported psoriasis flare-up following the vaccinations for SARS-CoV-2,8,9,26–28 H1N1 influenza,29 and pneumococcal pneumonia.30 The mechanisms linked to psoriasis deterioration after vaccination are yet to be understood. The potential mechanisms may include the dysregulation of immune system owing to vaccine adjuvants or viral components.29 Previous studies have postulated that Th1 and Th17 may play a critical role in triggering a deterioration of psoriasis after vaccination.31,32 However, our study revealed a comparable rate of and similar risk factors for the deterioration of psoriasis with a previous study that investigated the change of psoriasis at the early stage of COVID-19 pandemic when no vaccine was available,10 indicating that the deterioration might be attributable to factors beyond the disease per se, at population level. Mental health problems are common in psoriatic patients and to some extent, are associated with the aggravation of psoriasis.33 Patient education and intervention are needed to target the mental and behavioral problems.
This study has some limitations. A primary limitation is that the change of psoriasis was not inquired in patients who did not receive the vaccine, since there was a lack of definitive starting point of the change. This limited us to infer about the association of vaccination with the aggravation of psoriasis. Second, selection bias might exist in web-based survey, the vaccination rate in psoriasis patients might be overestimated owing to the lack of data from geriatric and pediatric patients who were less accessible to the social media and had a lower vaccination rate for the restriction of vaccination age. In addition, the incidence rate of adverse reactions might be overestimated or underestimated. Third, recall bias from patient-reported outcomes might increase the errors of measurement and cause biased estimates of the associations. The strength of the study included a large sample size and a systematic evaluation of demographic, clinical, behavioral, and psychological factors in the context of real-world clinical practice.
In conclusion, the rate of SARS-CoV-2 vaccination in the Chinese patients with psoriasis was relatively high. Younger age, biological treatment, symptoms of anxiety, and type and severity of psoriasis were factors for unvaccination. A slightly higher rate of vaccine-related adverse reactions was reported by the patients compared with the data from clinical trials. No severe adverse reaction was reported, and no significant difference in adverse reactions was observed between the common types of vaccines. A small proportion of patients reported aggravation of psoriasis after vaccination, which was partially attribute to mental and behavioral factors, indicating a necessity of patient education. Our study implied a favorable safety profile of SARS-CoV-2 vaccines, and the benefits of vaccination should not be underappreciated.
Data Sharing Statement
All available data can be obtained by contacting the corresponding author Yehong Kuang.
Acknowledgments
We would like to thank the Psoriatic Patient Blog (https://www.yxb365.com/portal.php) and all participants for their assistance in the online survey.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (81573049, 81430075, 81830096, 82073447), Key R & D Program of Hunan Province (2018SK2082), National key R & D program (2018YFC0117004), the Ministry of Science and Technology of the People’s Republic of China (2016YFC0900802). The funder did not participate in the study.
Disclosure
The authors have no conflict of interest to declare.
References
1. Tan L, Zhao S, Zhu W, et al. The Akkermansia muciniphila is a gut microbiota signature in psoriasis. Exp Dermatol. 2018;27(2):144–149. doi:10.1111/exd.13463
2. Zeng C, Wen B, Hou G, et al. Lipidomics profiling reveals the role of glycerophospholipid metabolism in psoriasis. Gigascience. 2017;6(10):1–11. doi:10.1093/gigascience/gix087
3. Rahier JF, Moutschen M, Van Gompel A, et al. Vaccinations in patients with immune-mediated inflammatory diseases. Rheumatology (Oxford). 2010;49(10):1815–1827. doi:10.1093/rheumatology/keq183
4. Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker J. Psoriasis. Lancet. 2021;397(10281):1301–1315. doi:10.1016/S0140-6736(20)32549-6
5. Wang J, Jing R, Lai X, et al. Acceptance of COVID-19 vaccination during the COVID-19 pandemic in China. Vaccines (Basel). 2020;8(3):482.
6. Zhang Y, Luo X, Ma ZF. Willingness of the general population to accept and pay for COVID-19 vaccination during the early stages of COVID-19 pandemic: a nationally representative survey in mainland China. Hum Vaccin Immunother. 2021;17(6):1622–1627. doi:10.1080/21645515.2020.1847585
7. Wack S, Patton T, Ferris LK. COVID-19 vaccine safety and efficacy in patients with immune-mediated inflammatory disease: review of available evidence. J Am Acad Dermatol. 2021;85(5):1274–1284. doi:10.1016/j.jaad.2021.07.054
8. Krajewski PK, Matusiak L, Szepietowski JC. Psoriasis flare-up associated with second dose of Pfizer-BioNTech BNT16B2b2 COVID-19 mRNA vaccine. J Eur Acad Dermatol Venereol. 2021. doi:10.1111/jdv.17449
9. Onsun N, Kaya G, Isik BG, Gunes B. A generalized pustular psoriasis flare after CoronaVac COVID-19 vaccination: case report. Health Promot Perspect. 2021;11(2):261–262. doi:10.34172/hpp.2021.32
10. Wang Q, Luo Y, Lv C, et al. Nonadherence to treatment and patient-reported outcomes of psoriasis during the COVID-19 epidemic: a web-based survey. Patient Prefer Adherence. 2020;14:1403–1409. doi:10.2147/PPA.S263843
11. Kuang Y, Shen M, Wang Q, et al. Association of outdoor activity restriction and income loss with patient-reported outcomes of psoriasis during the COVID-19 pandemic: a web-based survey. J Am Acad Dermatol. 2020;83(2):670–672. doi:10.1016/j.jaad.2020.05.018
12. Liu ZW, Yu Y, Hu M, Liu HM, Zhou L, Xiao SY. PHQ-9 and PHQ-2 for screening depression in Chinese rural elderly. PLoS One. 2016;11(3):e0151042. doi:10.1371/journal.pone.0151042
13. Plummer F, Manea L, Trepel D, McMillan D. Screening for anxiety disorders with the GAD-7 and GAD-2: a systematic review and diagnostic metaanalysis. Gen Hosp Psychiatry. 2016;39:24–31. doi:10.1016/j.genhosppsych.2015.11.005
14. Dutheil F, Pereira B, Moustafa F, Naughton G, Lesage FX, Lambert C. At-risk and intervention thresholds of occupational stress using a visual analogue scale. PLoS One. 2017;12(6):e0178948. doi:10.1371/journal.pone.0178948
15. Lesage FX, Berjot S. Validity of occupational stress assessment using a visual analogue scale. Occup Med (Lond). 2011;61(6):434–436. doi:10.1093/occmed/kqr037
16. Peduzzi P, Concato J, Kemper E, Holford TR, Feinstein AR. A simulation study of the number of events per variable in logistic regression analysis. J Clin Epidemiol. 1996;49(12):1373–1379. doi:10.1016/S0895-4356(96)00236-3
17. Sotiriou E, Bakirtzi K, Papadimitriou I, et al. COVID-19 vaccination intention among patients with psoriasis compared with immunosuppressed patients with other skin diseases and factors influencing their decision. Br J Dermatol. 2021;185(1):209–210. doi:10.1111/bjd.19882
18. Xia S, Zhang Y, Wang Y, et al. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBIBP-CorV: a randomised, double-blind, placebo-controlled, phase 1/2 trial. Lancet Infect Dis. 2021;21(1):39–51. doi:10.1016/S1473-3099(20)30831-8
19. Tanriover MD, Doganay HL, Akova M, et al. Efficacy and safety of an inactivated whole-virion SARS-CoV-2 vaccine (CoronaVac): interim results of a double-blind, randomised, placebo-controlled, phase 3 trial in Turkey. Lancet. 2021;398(10296):213–222. doi:10.1016/S0140-6736(21)01429-X
20. Zhang Y, Zeng G, Pan H, et al. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine in healthy adults aged 18–59 years: a randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. Lancet Infect Dis. 2021;21(2):181–192. doi:10.1016/S1473-3099(20)30843-4
21. Yang S, Li Y, Dai L, et al. Safety and immunogenicity of a recombinant tandem-repeat dimeric RBD-based protein subunit vaccine (ZF2001) against COVID-19 in adults: two randomised, double-blind, placebo-controlled, phase 1 and 2 trials. Lancet Infect Dis. 2021;21(8):1107–1119. doi:10.1016/S1473-3099(21)00127-4
22. Sprute R, Schumacher S, Pauls M, Pauls W, Cornely OA. Delayed cutaneous hypersensitivity reaction to vaxzevria (ChAdOx1-S) vaccine against SARS-CoV-2. Drugs R D. 2021. doi:10.1007/s40268-021-00358-z
23. Baden LR, El Sahly HM, Essink B, et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N Engl J Med. 2021;384(5):403–416. doi:10.1056/NEJMoa2035389
24. Skroza N, Bernardini N, Tolino E, et al. Safety and impact of anti-COVID-19 vaccines in psoriatic patients treated with biologics: a real life experience. J Clin Med. 2021;10(15):3355. doi:10.3390/jcm10153355
25. Diotallevi F, Campanati A, Radi G, et al. Vaccination against SARS-CoV-2 and psoriasis: the three things every dermatologist should know. J Eur Acad Dermatol Venereol. 2021;35(7):e428–e30. doi:10.1111/jdv.17256
26. Lehmann M, Schorno P, Hunger RE, Heidemeyer K, Feldmeyer L, Yawalkar N. New onset of mainly guttate psoriasis after COVID-19 vaccination: a case report. J Eur Acad Dermatol Venereol. 2021;35(11). doi:10.1111/jdv.17561
27. Nagrani P, Jindal R, Goyal D. Onset/flare of psoriasis following the ChAdOx1 nCoV-19 corona virus vaccine (Oxford-AstraZeneca/Covishield): report of two cases. Dermatol Ther. 2021;34(5):e15085. doi:10.1111/dth.15085
28. Sotiriou E, Tsentemeidou A, Bakirtzi K, Lallas A, Ioannides D, Vakirlis E. Psoriasis exacerbation after Covid-19 vaccination: report of 14 cases from a single center. J Eur Acad Dermatol Venereol. 2021;35(12). doi:10.1111/jdv.17582
29. Gunes AT, Fetil E, Akarsu S, Ozbagcivan O, Babayeva L. Possible triggering effect of influenza vaccination on psoriasis. J Immunol Res. 2015;2015:258430. doi:10.1155/2015/258430
30. Yoneyama S, Kamiya K, Kishimoto M, Komine M, Ohtsuki M. Generalized exacerbation of psoriasis vulgaris induced by pneumococcal polysaccharide vaccine. J Dermatol. 2019;46(11):e442–e43. doi:10.1111/1346-8138.15007
31. Kamiya K, Kishimoto M, Sugai J, Komine M, Ohtsuki M. Risk factors for the development of psoriasis. Int J Mol Sci. 2019;20(18):4347. doi:10.3390/ijms20184347
32. Shi CR, Nambudiri VE. Widespread psoriasis flare following influenza vaccination. Vaccine. 2017;35(36):4785–4786. doi:10.1016/j.vaccine.2017.06.067
33. Tian Z, Huang Y, Yue T, et al. A Chinese cross-sectional study on depression and anxiety symptoms in patients with psoriasis vulgaris. Psychol Health Med. 2019;24(3):269–280. doi:10.1080/13548506.2018.1529323
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.