")
Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 8
A systematic review to evaluate exercise for anterior cruciate ligament injuries: does this approach reduce the incidence of knee osteoarthritis?
Authors Duncan K, Chopp-Hurley J, Maly M
Received 22 July 2015
Accepted for publication 5 November 2015
Published 8 January 2016 Volume 2016:8 Pages 1—16
DOI https://doi.org/10.2147/OARRR.S81673
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chuan-Ju Liu
Koji J Duncan, Jaclyn N Chopp-Hurley, Monica R Maly
School of Rehabilitation Science, McMaster University, Hamilton, ON, Canada
Purpose: Among a variety of conservative and surgical options to treat anterior cruciate ligament (ACL) injuries, we do not understand which options could potentially prevent knee osteoarthritis (OA). The aim of this systematic review was to examine the evidence pertaining to exercise treatment of ACL injuries in the context of knee OA.
Methods: Medline, Embase, CINAHL, PubMed, and PEDro (Physiotherapy Evidence Database) databases were systematically searched using keywords encompassed within four primary key terms: knee, osteoarthritis, anterior cruciate ligament, and exercise. Clinical studies evaluating the effect of an exercise treatment for ACL injuries on the development of knee OA in adult humans were included. The PEDro scale was used to critically assess the studies included in the review.
Results: Eighteen studies were included in this review, with a median PEDro score of 6/11 (range, 2/11–9/11). Three studies provided statistical evidence that exercise following ACL injury lowered the risk for knee OA development. Nine studies demonstrated no benefit of exercise in preventing knee OA incidence relative to either operative treatment or the contralateral, unaffected knee. However, exercise resulted in higher knee instability. Nonetheless, there were no significant differences in subjective or objective knee outcomes for early versus late ACL reconstruction.
Limitations: This review was not registered through PROSPERO.
Conclusion: The relationship between a rehabilitative exercise for ACL injuries and long-term knee OA prevalence is inconclusive. However, research suggests initial conservative treatment with optional late ACL reconstruction because this treatment strategy may reduce the risk of knee OA. More research, ideally randomized controlled trials or comparable designs, is required prior to establishing clinical guidelines for ACL injury management.
Keywords: exercise therapy, knee, ligament, articular, osteoarthrosis, rehabilitation
Introduction
The most commonly injured ligament of the knee is the anterior cruciate ligament (ACL). Rupture, elongation, and/or fraying of the ACL often occur within activities that require pivoting movements such as soccer or basketball.1 Therefore, ACL injuries occur most frequently among young, competitive athletes.2 The primary function of the ACL is to stabilize the knee by resisting hyperextension, anterior tibial translation, and knee joint internal/external rotation.3 The ACL also helps to resist varus and valgus forces when the knee is in a flexed position.3 Injury of the ACL occurs when stresses applied directly or indirectly to the knee exceed the ACL tissue tolerance. Direct contact injuries generally occur through a forceful valgus stress and often result in concomitant injuries to the medial meniscus and the medial collateral ligament.3 ACL injuries are most commonly caused through noncontact mechanisms. This indirect contact accounts for 70%–80% of all ACL injuries and is frequently attributed to poor body mechanics during jumping or pivoting.3
In the long term, elevated risks of knee osteoarthritis (OA) and poor knee function exist in those with ACL injuries, predominantly due to knee joint instability.1,4,5 In fact, OA affects up to 50% of individuals that have had an ACL injury.2 OA can lead to chronic pain, limited function, as well as an overall reduction in the quality of life.6 To further contribute to knee OA risk, an ACL injury can occur concurrently with meniscal tears.1 The meniscus acts as a secondary stabilizer of the knee, and knee instability is associated with a high risk of OA development.5 A partial or total meniscectomy is often performed when the meniscus is injured, which is also recognized as a substantive risk factor in the development of knee OA.1
There are no specific guidelines whether ACL injuries should be treated conservatively with rehabilitation programs, or with surgical reconstruction.2 Posttraumatic ACL injuries can be managed through different treatment options, including conservative (typically exercise combined with bracing and activity modification) and nonconservative (surgical repair of the ACL) approaches. The restoration of neuromuscular knee function after injury through exercise may play a key role in preventing the development of OA.6 However, operative treatment for an ACL injury is common, primarily due to its associated improvements in knee stability and better restoration of activity level.2 While there is an abundance of research reviewing the effect of operative treatment on the development of knee OA, there has been minimal research examining the long-term effects of exercise for ACL deficiency.7 Since poor muscle function is implicated in the development of OA, exercise, and rehabilitation after an ACL tear may be advantageous for preventing the development of OA.6 Through the use of rigorous neuromuscular training, muscular function after an ACL injury can be effectively regained, including improvements in strength, dynamic stability, postural awareness, and muscular coordination.8 As well, a conservative approach to ACL injuries eliminates the risk of surgical complications.8 These complications include the risk of infection, arthrofibrosis, graft failure, donor site morbidity, and pain.8
The purpose of this review was to critically examine whether exercise after an ACL injury reduces the risk of knee OA development compared to an operational approach. Treatment effectiveness was evaluated using several outcome measures, including signs of knee degeneration on images acquired with a variety of modalities, as well as both subjective and objective measures of knee stability and function.
Methods
Search and evaluation strategy
Medline (1946–Present), Embase (1974–Present), CINAHL (1981–Present), PubMed, and Physiotherapy Evidence Database (PEDro) databases were systematically searched using keywords encompassed within four primary key terms: knee (5 keywords), osteoarthritis (11 keywords), anterior cruciate ligament (4 keywords), and exercise (48 keywords) (Table 1). After each search was performed, the publication titles and abstracts were evaluated based on specific inclusion/exclusion criteria. Inclusion criteria included the following: 1) full text journal article, 2) longitudinal design, 3) prescribed exercise intervention for ACL rupture, and 4) measurement of incidence of knee OA using an imaging modality (ie, radiographs, magnetic resonance imaging [MRI]). Study design (ie, randomized controlled trial [RCT], prospective/retrospective case series or cohort) was not restricted, however review papers (ie, narrative, systematic, meta-analyses) were not included. Studies were excluded if they did not use human participants who were over 18 years of age. This search was last conducted in September 2015. All articles were imported into Mendeley Desktop© (version 1.14) through which duplicates were removed and articles were screened for inclusion.
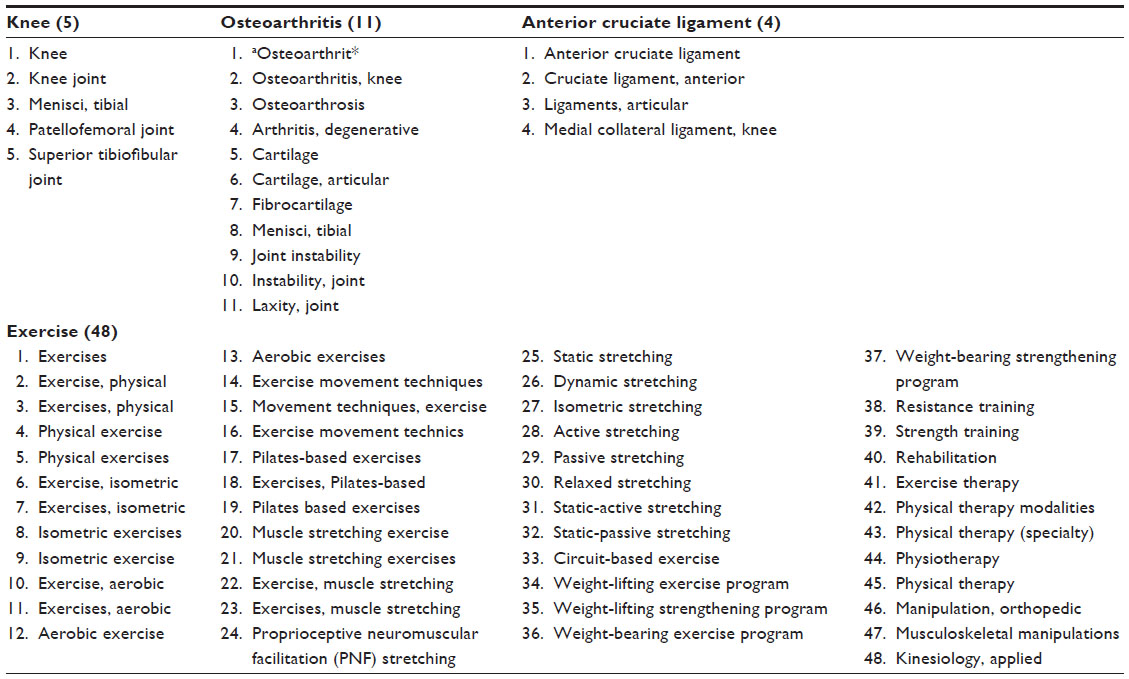 | Table 1 Search strategy; 68 key words within four key terms (knee, osteoarthritis, anterior cruciate ligament, exercise) |
Measurement of the incidence of knee OA
Several measurements of knee OA incidence were included in this review: 1) radiographs, 2) bone scans, 3) MRI, and 4) signs and symptoms associated with knee function. These outcome measures were required to provide evidence of joint degradation associated with knee OA. Signs of joint space narrowing and osteophyte formation were noted on radiographs. In one study, bone scans were used to complement radiographic findings, with the regional specific changes evaluated and scored.9 MRI has been recently used to specifically evaluate regional changes in knee cartilage.10,11 Finally, clinical measurements of signs associated with impaired knee function due to ACL deficiency and knee OA, such as knee laxity were included.
Apart from imaging evidence of joint degradation, subjective and objective assessments of knee stability and function were often reported. Subjective and objective measurements were recorded in this review. Knee instability, range of motion, and laxity measurements may be evaluated primarily using the Lachman test, pivot shift test, and side-to-side laxity (≥3 mm) using a KT-1000 arthrometer. Additional manual tests, such as the anterior drawer test, and flexion/extension range of motion may also be used to evaluate knee stability. Studies may quantify lower limb muscle strength differences between the injured and uninjured knees.12–14 Also, standardized subjective reports of knee function may be assessed using scores obtained from questionnaires, including the Knee Injury and Osteoarthritis Outcome Score, International Knee Documentation Committee (IKDC), Lysholm, and Short Form-36. Self-reported knee instability, pain, and swelling were also recorded. Finally, the activity level was evaluated predominantly using Tegner scores, however, subjective reports of sport or occupational modifications due to injury or treatment were reported.
Each of the included studies was reviewed to determine whether specific trends could be identified with respect to the relationship between conservative management of ACL injuries through exercise and the incidence of knee OA. This included considering related factors such as knee instability, length of follow-up period, and late surgical intervention.
Critical appraisal
Included studies were critically reviewed using the PEDro critical appraisal scale. The PEDro scale was developed to assist researchers in identifying clinical trials with adequate internal validity and interpretable outcomes based on sufficient statistical information.15 The PEDro scale appraises articles based on eleven criteria. These criteria involve the eligibility of study participants, allocation to groups, blinding procedures, and the use of outcome measures.15 A high score on the PEDro scale indicates that the study has high internal validity.
Results
A total of 18 studies were included in this review. The search strategy elicited 2,260 articles. After duplicates were removed (562), 1,698 were screened by title and abstract. Thirty-seven full journal articles were reviewed for eligibility, with 18 articles meeting all of the inclusion criteria. Studies were primarily excluded due to not specifically assessing OA using an imaging approach and/or describing the approach used to address cartilage changes, as well as not specifically describing an exercise treatment plan to conservatively treat the ACL injury. In addition, any review papers, those studies evaluating nonhuman participants or children (<18 years) were excluded. A summary of the included studies, specifically the PEDro score, sample, and intervention as well as the results, are shown in Table 2. Three of the studies reported a different set of outcome measures from the same sample and thus their results are integrated within the table.1,16,17
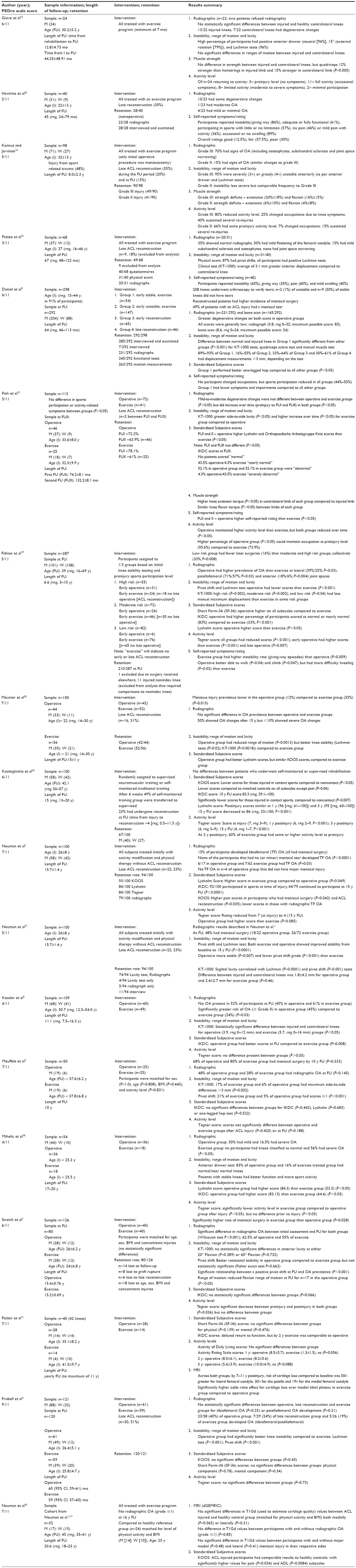 | Table 2 Summary of studies included in review |
The median PEDro score of the included studies was 6/11 and ranged from 2/11 to 9/11. A variety of intervention approaches was used to determine the effect of an exercise program on knee OA development. Eight of the included studies employed solely a rehabilitative exercise intervention, while ten compared this conservative treatment with an operative ACL reconstruction treatment. Exercise programs varied across the included studies, however, several adopted similar neuromuscular training themes, including the quadriceps and hamstrings muscle training, in addition to stability, mobility, and range of motion exercises (Table 3). In two studies, while researchers indicated that a rehabilitation program was provided, specific details of the program were not indicated. As well, in addition to the exercise program, some treatment strategies included activity modification, such as avoiding competitive sport, or activities involving contact or pivoting movements.5,16,18
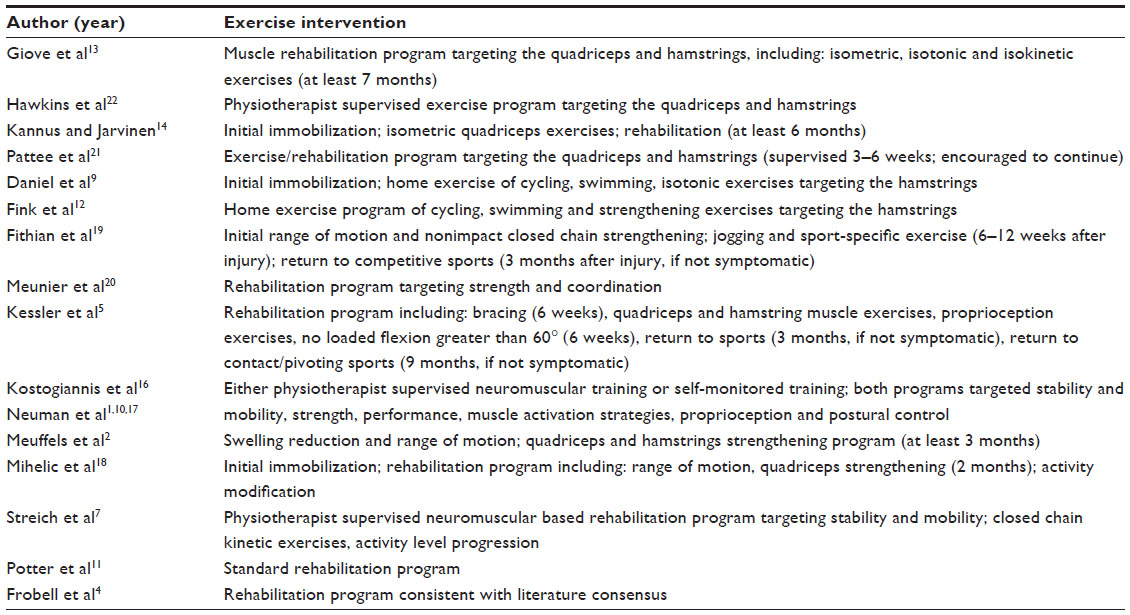 | Table 3 Exercise intervention description in the included studies |
While all included studies contained participant groups initially treated with an exercise intervention, several required late surgical intervention within the follow-up period. Specifically, in twelve of the included studies, a median of 23% (range, 5%–51%) of participants in the exercise group required late ACL reconstruction (Table 2). Despite this, it appears there is a minimal disadvantage to having delayed reconstruction.19 While a higher risk of meniscal surgery was evident in those who underwent ACL reconstruction later than 3 months post-ACL injury, the risk of radiographic degenerative changes was lower in this later reconstruction group. Across included studies, the mean and median follow-up period post-ACL injury, was 11 years with a range of 4–20 years.
Each study included a different combination of outcome measures (Table 2). Fourteen studies used radiographic imaging to evaluate OA prevalence, while two studies specifically assessed cartilage morphology or composition using MRI. Among the studies that captured radiographs, five different grading systems were adopted. The criteria for each of these scales used to address OA severity were comparable; predominantly evaluating joint space narrowing and osteophyte formation, while some also considered the presence of sclerosis, flattening of the femoral condyles, subchondral cysts, calcification of ligaments, or varus/valgus deformity.4,9,14 Grading systems included the following: the Kellgren and Lawrence classification,2,5 IKDC radiograph grading system,7,18,19 the Fairbanks scale,12,13,20,21 and recommendations posed by the Osteoarthritis Research Society International.1 The remaining studies did not use a standardized radiographic grading scale and/or used the alternate subjective and objective measures of knee stability, laxity, and function to evaluate the treatment success.
Three of the included studies provided statistical evidence that an exercised-based rehabilitation program for ACL injury treatment lowered the risk for knee OA development.1,5,19 Several studies demonstrated no statistically significant difference between surgical reconstruction and the conservative exercise treatment for ACL injury, despite some showing trends of higher OA prevalence in either operative2,4,7,9 or exercise5,18,20 treatment groups. However, research demonstrated trends that both knee instability2,17,19 and meniscal tear prevalence5,19 are associated with an elevated risk for OA incidence following exercise as compared to operative treatment, though this trend was inconsistent across studies. Additionally, while researchers in one study showed a reduction in subjective outcome scores and activity levels at the end of the follow-up period (15 years), reasonable scores were still reported (Lysholm score =86, IKDC score =83.3 at 15-year follow-up), with authors suggesting that this decline may be partially attributed to age-related changes.16 In fact, at the 3-year follow-up, 60% of participants who underwent rehabilitative exercise and activity modification, had comparable activity levels to their preinjury state. Thus, this strategy of combining exercise with activity modification appears effective.
Discussion
Exercise and knee OA prevalence
The current available evidence regarding the effectiveness of exercise in reducing the risk of OA development is not conclusive. While some researchers demonstrated a lower prevalence of knee OA following exercise,1,5,19 most of the included studies showed no statistical advantage of exercise in reducing the risk of knee OA.
It is possible that the study sample sizes prohibited finding significant differences. Over half of the included studies had initial sample sizes ≥100 participants; however, many of these studies subdivided participants into two treatment groups (operative and conservative). The sample size within each group was often unequal because, instead of random allocation, the treatment allocation was generally selected based on a combination of participant preference, physician recommendation, and activity level, with a competitive, athletic population generally recommended for surgery.5,7,19 As well, within the conservative group, up to 51% of participants had reconstructive surgery by the end of the follow-up period. Cross-over from exercise to operative treatment resulted from either clinical signs and symptoms, notably chronic instability and giving way,7,12,14,20 and/or physical activity level, with a higher incidence of late surgery in a high risk group of young athletes;19–21 this subsequently resulted in a lower exercise group sample size. Additionally, the sample size was reduced by retention rates at follow-up, as well as the inability to obtain all outcome measures from study participants that completed the follow-up evaluation.
The length of the follow-up period could have contributed to the difference in OA prevalence between treatment groups, as degenerative changes may not have yet become evident.13,22 While progressive degradation has been noted in participants with established knee OA over as little as 2 years, these studies used measures from MRI which are more sensitive to change than many radiographic measures.23,24 The necessary study follow-up period to detect cartilage degradation post-ACL injury is unclear. However, in the current review, the studies showing a lower prevalence of OA in the exercise treatment group, represented short (6 years), moderate (11 years), and long (15 years) follow-up durations.
Exercise and associated risk factors for knee OA
Apart from radiographic evidence, several other outcome measures can be used to predict the risk of knee OA development. In particular, knee instability and laxity are highly evident following an ACL injury, with research showing that 96% of participants had positive anterior drawer and Lachman stability tests.13 Knee instability, identified using a pivot shift test, was significantly related to OA prevalence (P<0.001).7 Further, despite similar radiographic outcomes, higher pivot shift, and Lachman test scores and maximal side-to-side displacements (KT-1000) indicative of knee instability, were identified in the exercise group.2,17,19 These findings may suggest that while exercise may pose higher risk for OA development, the progression may not occur for several years.
Among those with an ACL injury, meniscal tears have been consistently recognized as a risk factor for OA development. It was suggested that the loss of meniscal integrity, which acts to stabilize the knee in the absence of an intact ACL, may contribute to knee instability and subsequent risk of OA.5 However, while certain studies demonstrated a higher incidence of meniscal tears with exercise,5,19 others showed a similar prevalence of meniscal tear between treatment groups, despite the increased knee instability and laxity in the exercise group.4,12 Additionally, in one study, no differences in radiographic degeneration were shown in those participants requiring a meniscectomy.13
Similar to the divergence in objective outcome measures of stability and degeneration, subjective measures of knee pain and function following treatment were inconsistent across studies. Several researchers showed that, compared to operative treatment, exercise resulted in lower outcome scores at follow-up, as noted by IKDC scores,5,12,18,19 self-reported ratings,12,19 and Lysholm scores.12,20 Additionally, participants treated with exercise demonstrated lower relative activity, sports and occupation-related capabilities compared to both operative treatment and their baseline (preinjury) measurement.12,19 Alternatively, other researchers showed no difference in subjective knee function scores between treatment groups.1,2,4,7,11
Additional risk factors related to ACL injury and OA development exist, including sex, age, and body mass. Researchers have identified a higher incidence of ACL injuries sustained in women compared to men, with a ratio of 3:1.25 As 70%–80% of ACL injuries result from noncontact, often occurring during sport, younger females are at a high risk for injury.3 Alternatively, OA is a progressive degenerative disease that exists more prominently in women ≥55 years of age.26 Obesity has been identified as a risk factor for OA development. High body mass leads to cartilage degeneration by increasing the mechanical load incurred at the knee joint.27 Reducing body mass will concurrently reduce knee joint loading, with a ratio of 1:4.28 As well, both greater age (P=0.03) and body mass index (P=0.03) related to OA development in those with ACL ruptures.5 This suggests that ACL injuries sustained at a young age pose risk for OA development and that this risk may be exacerbated by higher body mass. Thus, while rehabilitative exercise strives to improve muscle strength and knee joint stability, a secondary target of the exercise should be reducing total body mass. For example, rehabilitation strategies that aim to initiate weight loss would in turn reduce knee joint loading and subsequently reduce the risk of OA.
Factors contributing to treatment outcome
With inconsistencies present across the literature regarding the effectiveness of exercise after ACL injuries, it is important to consider possible factors that may confound treatment outcomes. ACL tear severity and the duration between injury and operative treatment were two factors evaluated within the included research studies. Kannus and Jarvinen14 compared OA prevalence, instability, muscle strength, and activity level for those with grade II and grade III ACL injuries. Overall, tear severity was inversely related to all outcomes measures. This could partially explain the lack of statistical findings between treatment groups, as the participant sample may have included several grades of injury. Similarly, only one study included individuals who had sustained an isolated ACL injury with no concomitant ligament, meniscal, or chondral injuries. While the results favored exercise due to the lower prevalence of radiographic OA, the results of this study may not be generalizable to most ACL injuries, as isolated ACL-ruptures rarely occur.5 Research by Fithian et al19 included three treatment levels across the three study groups (high risk, moderate risk, low risk). Participants were initially prescribed exercise or early operative treatment, however, several undergoing exercise treatments opted for late operative treatment (>3 months postinjury). While those who solely underwent exercise had poorer stability and subjective function scores than operative groups, no statistically significant differences were present between early and late operative treatments with the exception of showing greater prevalence of meniscal tears in the late operative group. However, the exercise treatment group had significantly lower radiographic degeneration than operative groups. These findings, particularly the little added benefit of early ACL reconstruction, suggest that the best outcome after ACL injury results from late operative repair, after a period of exercise, following injury.
Limitations
The difficulty in evaluating the effectiveness of exercise after ACL injuries stems from the limited ability to conduct RCTs. Predominant limitations include a lack of randomization and concealed allocation, which subsequently results in low PEDro scores (median, 6/11) across the included studies. The use of randomization could create an ethical issue because clinical recommendations and patient preference may not match random allocation.1 Also, with regards to exercise or operative treatment of ACL injuries, it is not feasible to blind participants to treatment group. As well, it is not possible to blind the surgeons performing reconstruction, or the therapists leading the exercise. In practice, the treatment adopted stems primarily from patient preference and physician recommendation, which often considers the current activity level of the patient. For example, one study stratified participants by activity level, with all high risk individuals (defined as young and participating in competitive activity) recommended for operative treatment.19 Despite the physician recommendation, 44% of high risk participants declined and were treated with exercise. The only RCT included in this review (Frobell et al4) studied 121 active adults with an ACL injury. Participants were randomized to receive either early reconstruction or rehabilitation with the option of delayed ACL reconstruction. At a 5-year follow-up, the two groups did not differ in terms of the presence of radiographic knee OA. This RCT had the highest PEDro score of 9/11.
Despite the overall median PEDro score, several aspects of the included studies were conducted well, adding to the overall rigor of the evidence. Notably, many studies had longer follow-up times (up to 20 years). This time frame is highly advantageous for examining OA development, as OA is a disease that slowly progresses over variable time periods, but typically over several years. The studies also included reasonably large sample sizes (in some cases matching participants between treatment arms) and had rigorous inclusion/exclusion criteria. Additionally, independent assessors, who were unaware of the treatment received, often evaluated the radiographs; thereby limiting potential bias.
It is possible that variation in exercise programs also limited the ability to identify an effect of exercise after ACL injury on knee OA risk. Common goals included neuromuscular rehabilitation, reduction of swelling, increased joint mobility, and the modification of activities, which included a reduction in participation in sports and activities. However, because the description of the exact treatment plan was limited in most studies, comparing the effectiveness of different exercise programs was challenging. In fact, it is possible that research addressing the incidence of OA following conservative management of ACL injuries should be excluded from this review, due to not explicitly reporting their exercise management program. Future research should provide detailed reports of conservative treatment protocols and exercise programs, which would assist in offering more definitive conclusions regarding the effectiveness of exercise in reducing OA prevalence following an ACL injury.
Comparisons between exercise and operative management of ACL injuries was also limited by late operative procedures (notably ACL reconstruction). Many of the included studies initially prescribed exercise, but several participants underwent late reconstruction during the follow-up period. Finally, radiographic measurement of OA, which was included in 14 studies, is the current gold standard in diagnosing OA.10 However, radiography is insensitive to early degenerative changes and may not be the best available tool for determining the risk of OA development. Research examining the sensitivity of different imaging modalities to evaluate OA changes in the knee, namely radiographs, computed tomography and MRI, demonstrated that MRI was better able to detect changes while also being able to evaluate soft tissue abnormalities (meniscus, ligaments).29 Additionally, the diagnostic capability of ultrasound for OA has been recently studied.30 While images from ultrasound denoting cartilage degeneration were a strong predictor of arthroscopic findings, negative findings from the ultrasound exam were identified in cases where arthroscopic OA was present. Thus, MRI, which is more sensitive to early cartilage changes, may be more effective in determining the risk of OA development.10,11 Advances in imaging which enables assessment of cartilage composition with noninvasive techniques, such as transverse relaxation time (T2) mapping, may be useful in evaluating OA progression in future studies.
It should be noted that there is an important potential risk for assessor bias associated with this review due to not registering the protocol through PROSPERO. The lack of conclusive findings regarding the effectiveness of exercise treatment for ACL injuries reduces this risk. A PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) checklist, however, has been completed (Table 4) to demonstrate the scientific rigor in reporting this review.31
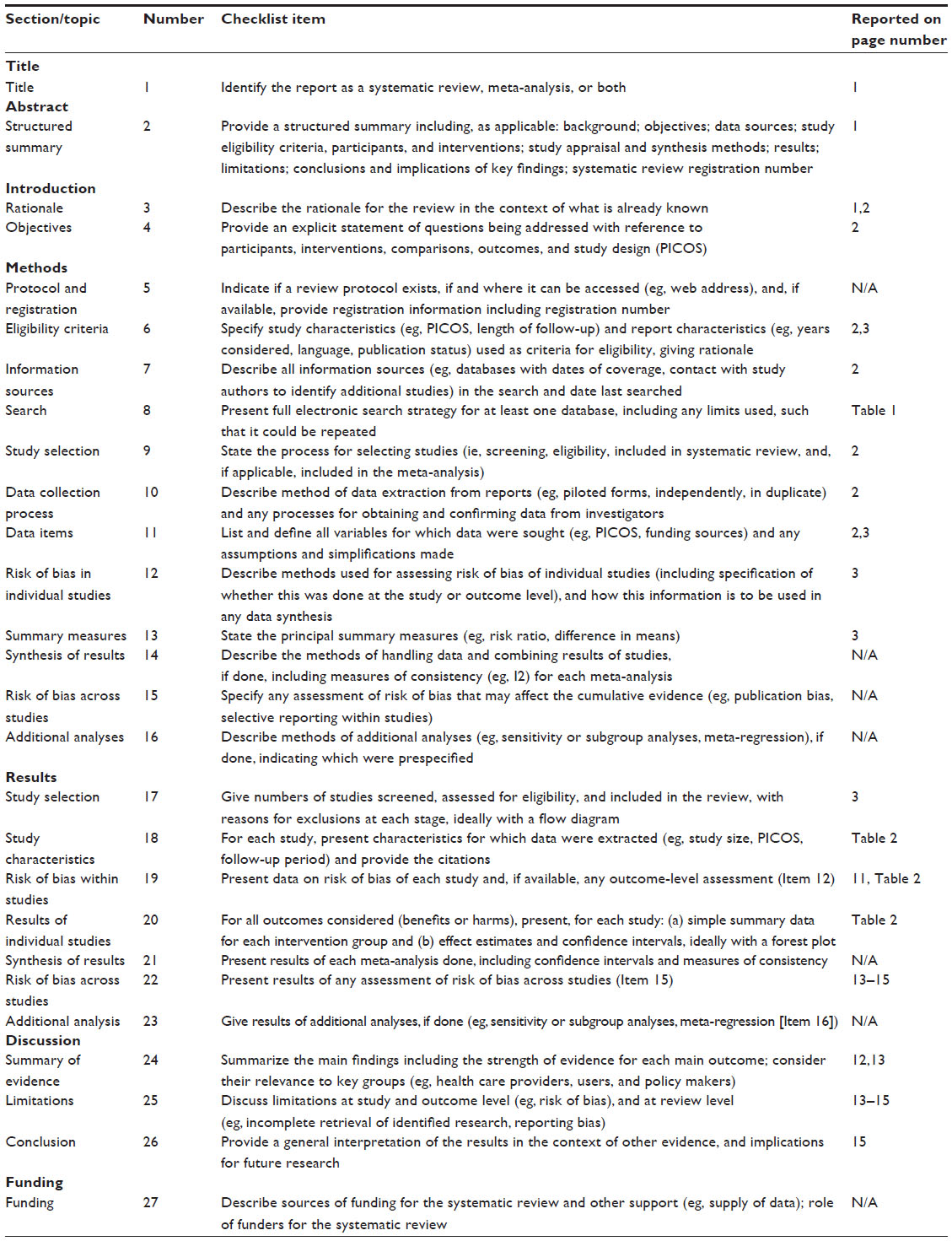 | Table 4 PRISMA 2009 checklist |
Conclusion
The collective results from this review demonstrated that the evidence regarding exercise after ACL injuries to reduce the risk of knee OA is inconclusive. However, compared to operative treatment, some evidence may suggest that exercise could increase the risk of knee instability and subsequent meniscal tears, which can further increase the risk of knee OA. However, this finding was not consistent. Additionally, research suggested that there was minimal benefit in undergoing early reconstructive treatment, with lower prevalence of OA shown in those who initially pursued exercise. Thus, initial exercise management, with the option of late ACL reconstruction, may be beneficial in reducing the risk of knee OA.
Future research specifically addressing the effect of knee stability and concomitant meniscus injuries on the development of OA and their relationship to exercise versus operative treatment of ACL injuries is required. Ideally, conducting randomized controlled or comparable trials would provide high quality evidence for ACL management and OA progression. Including activity modification treatment to prevent knee OA in ACL injured patients, rather than solely an exercise intervention may offer insight into conservative treatment strategies. Researchers suggest that modification of activity, including reduction of participation in physical activity and the avoidance of pivotal sports, may subsequently reduce the need for late ACL reconstruction.16
Understanding of the effects of exercise on the risk of developing knee OA is critical for the development of clinical treatment guidelines for ACL injuries. This may include differential treatment based on tear severity and activity level, in addition to combined treatments of exercise and activity modification.
Disclosure
The authors report no conflicts of interest in this work.
References
Neuman P, Englund M, Kostogiannis I, Friden T, Roos H, Dahlberg LE. Prevalence of tibiofemoral osteoarthritis 15 years after nonoperative treatment of anterior cruciate ligament injury: a prospective cohort study. Am J Sports Med. 2008;36(9):1717–1725. | |
Meuffels DE, Favejee MM, Vissers MM, Heijboer MP, Reijman M, Verhaar JA. Ten year follow-up study comparing conservative versus operative treatment of anterior cruciate ligament ruptures. A matched-pair analysis of high level athletes. Br J Sports Med. 2009;43(5):347–351. | |
Acevedo RF, Rivera-Vega A, Miranda G, Micheo W. Anterior cruciate ligament injury: Identification of risk factors and prevention strategies. Curr Sports Med Rep. 2014;13(3):186–191. | |
Frobell RB, Roos HP, Roos EM, Roemer FW, Ranstam J, Lohmander LS. Treatment for acute anterior cruciate ligament tear: Five year outcome of randomised trial. BMJ. 2013;346:f232. | |
Kessler MA, Behrend H, Henz S, Stutz G, Rukavina A, Kuster MS. Function, osteoarthritis and activity after ACL-rupture: 11 years follow-up results of conservative versus reconstructive treatment. Knee Surg Sports Traumatol Arthrosc. 2008;16(5):442–448. | |
Ageberg E, Thomeé R, Neeter C, Silbernagel KG, Roos EM. Muscle strength and functional performance in patients with anterior cruciate ligament injury treated with training and surgical reconstruction or training only: A two to five-year follow-up. Arthritis Rheum. 2008;59(12):1773–1779. | |
Streich NA, Zimmermann D, Bode G, Schmitt H. Reconstructive versus non-reconstructive treatment of anterior cruciate ligament insufficiency. A retrospective matched-pair long-term follow-up. Int Orthop. 2011;35(4):607–613. | |
Smith TO, Postle K, Penny F, McNamara I, Mann CJ. Is reconstruction the best management strategy for anterior cruciate ligament rupture? A systematic review and meta-analysis comparing anterior cruciate ligament reconstruction versus non-operative treatment. Knee. 2014;21(2):462–470. | |
Daniel DM, Stone ML, Dobson BE, Fithian DC, Rossman DJ, Kaufman KR. Fate of the ACL-injured patient: a prospective outcome study. Am J Sports Med. 1994;22(5):632–644. | |
Neuman P, Owman H, Muller G, Englund M, Tiderius CJ, Dahlberg LE. Knee cartilage assessment with MRI (dGEMRIC) and subjective knee function in ACL injured copers: a cohort study with a 20 year follow-up. Osteoarthritis Cartilage. 2014;22(1):84–90. | |
Potter HG, Jain SK, Ma Y, Black BR, Fung S, Lyman S. Cartilage injury after acute, isolated anterior cruciate ligament tear – immediate and longitudinal effect with clinical/MRI follow-up. Am J Sports Med. 2012;40(2):276–285. | |
Fink C, Hoser C, Hackl W, Navarro RA. Long-term outcome of operative or nonoperative treatment of anterior cruciate ligament rupture – Is sports activity a determining variable? Int J Sports Med. 2001;22(4):304–309. | |
Giove TP, Miller SJ, Kent BE, Sanford TL, Stanford MA, Garrick JG. Non-operative treatment of the torn anterior cruciate ligament. J Bone Joint Surg Am. 1983;65(2):184–192. | |
Kannus P, Jarvinen M. Conservatively treated tears of the anterior cruciate ligament – Long-term results. J Bone Joint Surg Am. 1987;69A(7):1007–1012. | |
Physiotherapy Evidence Database (Pedro). PEDro Scale. Available from: http://www.pedro.org.au/english/downloads/. Accessed May 29, 2015. | |
Kostogiannis I, Ageberg E, Neuman P, Dahlberg L, Friden T, Roos H. Activity level and subjective knee function 15 years after anterior cruciate ligament injury – a prospective, longitudinal study of nonreconstructed patients. Am J Sports Med. 2007;35(7):1135–1143. | |
Neuman P, Kostogiannis I, Friden T, Roos H, Dahlberg LE, Englund M. Knee laxity after complete anterior cruciate ligament tear: a prospective study over 15 years. Scand J Med Sci Sports. 2012;22(2):156–163. | |
Mihelic R, Jurdana H, Jotanovic Z, Madjarevic T, Tudor A. Long-term results of anterior cruciate ligament reconstruction: a comparison with non-operative treatment with a follow-up of 17–20 years. Int Orthop. 2011;35(7):1093–1097. | |
Fithian DC, Paxton EW, Stone ML, et al. Prospective trial of a treatment algorithm for the management of the anterior cruciate ligament – injured knee. Am J Sports Med. 2005;33(3):335–346. | |
Meunier A, Odensten M, Good L. Long-term results after primary repair or non-surgical treatment of anterior cruciate ligament rupture: a randomized study with a 15-year follow-up. Scand J Med Sci Sports. 2007;17(3):230–237. | |
Pattee, GA, Fox, JM, Del Pizzo W, Friedman, MJ. Four to ten year followup of unreconstructed anterior cruciate ligament tears. Am J Sports Med. 1989;17(3):430–435. | |
Hawkins RJ, Misamore GW, Merritt TR. Followup of the acute nonoperated isolated anterior cruciate ligament tear. Am J Sports Med. 1986; 14(3):205–210. | |
Cicuttini F, Ding C, Wluka A, Davis S, Ebeling P, Jones G. Association of cartilage defects with loss of knee cartilage in healthy, middle-aged adults. Arthritis Rheum. 2005;52(7):2033–2039. | |
Ding C, Cicuttini F, Scott F, Boon C, Jones G. Association of prevalent and incident knee cartilage defects with loss of tibial and patellar cartilage. Arthritis Rheum. 2005;52(12):3918–3927. | |
Uhorchak JM, Scoville CR, Williams GN, Arciero RA, St Pierre P, Taylor DC. Risk factors associated with noncontact injury of the anterior cruciate ligament: A prospective four-year evaluation of 859 west point cadets. Am J Sports Med. 2003;31(6):831–842. | |
Srikanth WK, Fryer JL, Zhai G, Winzenberg TM, Hosmer D, Jones G. A meta-analysis of sex differences prevalence, incidence and severity of osteoarthritis. Osteoarthritis Cartilage. 2005;13:769–781. | |
Felson DT. An update on the pathogenesis and epidemiology of osteoarthritis. Radiol Clin North Am. 2004;42:1–9. | |
Messier SP, Gutekunst DJ, Davis C, DeVita P. Weight loss reduces knee-joint loads in overweight and obese older adults with knee osteoarthritis. Arthritis Rheum. 2005;52(7):2026–2032. | |
Chan WP, Lang P, Stevens MP, et al. Osteoarthritis of the knee: comparison of radiography, CT, and MR imaging to assess extent and severity. AJR Am J Roentgenol. 1991;157:799–806. | |
Saarakkala S, Waris P, Waris V, et al. Diagnostic performance of knee ultrasonography for detecting degenerative changes of articular cartilage. Osteoarthritis Cartilage. 2012;20:376–381. | |
Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann Intern Med. 2009;151(4):264–249. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.