Back to Journals » Journal of Pain Research » Volume 14
A Systematic Review of the Prospective Relationship Between Bullying Victimization and Pain
Authors Marin TJ ![]() , Hayden JA
, Hayden JA ![]() , Lewinson R, Mahood Q
, Lewinson R, Mahood Q ![]() , Pepler D
, Pepler D ![]() , Katz J
, Katz J ![]()
Received 30 March 2021
Accepted for publication 21 May 2021
Published 23 June 2021 Volume 2021:14 Pages 1875—1885
DOI https://doi.org/10.2147/JPR.S313470
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Teresa J Marin,1 Jill A Hayden,2 Rebecca Lewinson,1 Quenby Mahood,3 Debra Pepler,1 Joel Katz1
1Department of Psychology, York University, Toronto, Ontario, Canada; 2Department of Community Health and Epidemiology, Dalhousie University, Halifax, Nova Scotia, Canada; 3SickKids Hospital, Hospital Library, Toronto, Ontario, Canada
Correspondence: Teresa J Marin Email [email protected]
Objective: This systematic review synthesized evidence about the relationship between childhood bullying victimization and chronic pain, with a focus on the temporal nature of the relationship and moderating factors, such as the type and intensity of victimization.
Method: We included prospective cohort studies that examined the relationship between childhood bullying victimization and pain measured at least three months later. We conducted electronic searches of Medline, EMBASE, PsycINFO, and CINAHL up to June 30, 2019. Standard methodological procedures consistent with Cochrane reviews of prognosis studies were used (PROSPERO record ID 133146).
Results: We included four longitudinal studies (6275 participants) in this review. The mean age of participants at baseline ranged from 10 to 14 years and the follow-up periods ranged from 6 months to 12 years. Two of the four studies were judged as having high risk of bias. Meta-analysis of results from four studies revealed increased risk of pain among victimized compared to non-victimized youth (adjusted OR [95% CI] = 1.45 [1.06– 1.97], but the effect size was small and not clinically important. Only one study examined the inverse association (ie, from pain to victimization), and there was not enough evidence to conduct a meaningful analysis of the proposed moderators.
Conclusions: Study findings were limited by few prospective studies. Meta-analytic findings suggested that victimization may incur some risk for later pain, although the evidence was judged to be very low quality. High-quality studies that measure and report the nuances of bullying victimization are needed to test the proposed moderator models.
Keywords: bullying, chronic pain, systematic review, meta-analysis
Bullying victimization is a common adversity in childhood and adolescence.1 Not only does the experience of being bullied have negative consequences for mental health and psychosocial functioning, both in childhood2–4 and adulthood,5–7 but there is mounting evidence of its negative physical health consequences,8,9 including increased risk of physical pain in school-aged children.10–12 This is important because pain problems in young people can be intense and disabling, with the potential to track across childhood and adolescence and into adulthood.13–15
Despite the growing literature pointing to a relationship between bullying victimization and chronic pain, there is still much we do not know about the nature of this association. In particular, the majority of studies that have examined this relationship have relied on cross-sectional data.10 Therefore, a positive association may indicate a causal relationship whereby bullying leads to chronic pain later in childhood or in adulthood, but it is also plausible that youth who experience pain are more likely to get bullied or that a third variable is driving the effect in which case the relationship between being bullied and chronic pain is indirect. Indeed, research evidence indicates that children who suffer from chronic health conditions are more vulnerable to being bullied,16,17 and the same may be true for youth with chronic pain.18 In regard to potential confounding variables, we need to rule out such factors as reporting biases and other individual differences, which could drive both reports of bullying exposure and pain experiences, thereby creating a spurious association between the two.
In addition, recent evidence shows that the association between bullying victimization and pain may depend on key moderating factors. First, given that physical victimization has the potential to cause bodily injury,19 it may contribute directly to the development of chronic pain.20,21 Therefore, it may be important to distinguish between victimization that does and does not have a physical component. Second, consistent with models of chronic stress and health,22 bullying victimization that is more frequent and/or stable over time may have a cumulative impact on pain outcomes.6 As such, the relationship between victimization and pain may depend on the “dose” of victimization. Third, critical period models point to the importance of timing of the exposure. Although early life models have received the most attention,20 it has been proposed that the adolescent years may represent a critical window during which youth experience heightened social vulnerability because of the importance of peer connections at this stage, as well as increased biological responses to stress related to pubertal maturation.23,24 In this regard, the relationship between victimization and pain may depend on the specific timing of the bullying exposure.
Objectives
This systematic review aimed to examine the relationship between childhood bullying victimization and the development of pain, with a focus on the temporal nature of this relationship, as well as potential moderating factors (ie, type of victimization, presence of physical injury, and the frequency, stability and developmental timing of victimization).
Method
Details of the protocol for this systematic review were registered on PROSPERO and can be accessed at https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=133146.25
Inclusion Criteria
We included prospective cohort studies that examined the relationship between childhood bullying victimization and chronic pain. We included studies when a clearly defined measure of victimization was obtained in childhood and/or adolescence (ie, 18 years or younger) and when pain-related outcomes were measured at least 3 months after (whether that was in childhood, adolescence or adulthood). The 3-month cut-off was used because we were interested in chronic pain outcomes (duration >3 months) as opposed to acute or subacute pain occurring in the aftermath of victimization. The 3-month cut-off is consistent with the definition of chronic pain provided by the International Association for the Study of Pain and the International Classification of Diseases 11th edition.26 We also included studies in which the measurement of pain preceded the measurement of bullying victimization, again with a minimum 3-month follow-up. We included studies when the full report was peer-reviewed.
Exclusion Criteria
We excluded 1) studies that induced pain in the laboratory; 2) intervention studies; and 3) case studies, review articles, dissertations, letters, editorials, book chapters, qualitative studies and conference abstracts; and 4) non-English articles.
Defining Bullying Victimization
Bullying victimization occurs when someone is the object of repeated aggression that is intentional and involves a disparity of power between the victim and perpetrators. For this review, we included bullying by peers and siblings, as well as cyberbullying. We included studies that measured bullying victimization using self-report questionnaires and interviews, other reports (eg, parents or teachers reporting bullying), and behavioral ratings (eg, being hit repeatedly).
We coded for specific features of the bullying exposure, including the type, frequency, stability, and developmental stage. See Supplemental Materials Appendix 1 for operational definitions used.
Defining Pain Outcomes
Our primary outcome was chronic pain, defined as pain lasting longer than 3 months. In addition to including studies that captured pain intensity or frequency, we included studies that reported the outcome as presence of a chronic pain condition (eg, migraine, chronic musculoskeletal, or abdominal pain). We included studies that measured pain in childhood, adolescence or adulthood via self-report (eg, visual analogue scale, numeric rating scale, McGill Pain Questionnaire,27 parental report, or clinician examination or interview. Many studies that report pain outcomes fail to specify the duration, thus it is unclear whether the study is actually measuring chronic pain. We therefore made an a priori decision to include studies regardless of duration, and if possible, account for any such measurement issues in our analysis. In regard to secondary outcomes, we included studies that reported pain-related outcomes, such as pain-related disability or interference. Where possible, we also coded for information regarding pain medication use.
Search and Screening Strategy
Electronic searches of Medline (OVID), EMBASE (OVID), PsycINFO (OVID, ProQuest [PsycInfo was originally run in OVID but due to an institutional change was only available through ProQuest when the search was last updated]), and CINAHL (EBSCO) were conducted by an experienced librarian (QM) and last updated June 30, 2019. The search strategy was adapted from a previous systematic review examining risk factors for chronic pain.28 Search terms cover three broad categories: 1) bullying victimization, 2) chronic pain, and 3) study design: captured by terms such as “risk” and “association” (see search terms for Medline presented in Supplemental Materials Appendix 2). The searches were customized for each database, using a combination of index and free text terms with no date or language restrictions. We did limit to human studies. To identify studies for inclusion, we screened the citations from these searches for relevance through title/abstract and full-text review. Recognizing potential limitations of electronic search strategies,29 we also searched references of previously published reviews of bullying victimization and pain10,11,18 and conducted a review of references for all included studies and citation searches of key articles in the field.6,30,31
Data Extraction
Two independent reviewers (TM and RL) extracted data and reached consensus using pre-defined electronic extraction forms. A third reviewer (JK) was consulted in the case of disagreements. See Supplemental Materials Appendix 3 for a list of variables extracted.
Assessing Risk of Bias
We assessed each study’s risk of bias using an approach based on the Quality in Prognosis Studies (QUIPS) tool32 for studies examining prognostic or risk factors. This involved consideration of six important domains: study participation, study attrition, measurement of the risk factor of interest, outcome measurement, confounding, and analysis/reporting. For each of the six domains, responses to the prompting items were taken together to inform the risk of bias judgment (low, moderate, or high). To judge risk of bias for the confounding domain, we considered whether statistical analyses were unadjusted, minimally adjusted (ie, controlled for participant age and sex) or adequately adjusted (ie, controlled for age, sex, baseline pain, a measure of social status, such as family income or parental education, and a measure of negative affect, such as neuroticism or symptoms of anxiety or depression). Unadjusted studies were rated as having high risk of bias, minimally adjusted studies were rated as having moderate risk of bias, and adequately adjusted studies were rated as having low risk of bias. Finally, we judged overall study validity by defining studies with a low risk of bias as those in which at least half of bias domains were rated to be low risk and there were no domains rated as high risk of bias. This assessment was conducted in duplicate by the first and last author, and any disagreements were resolved through discussion.
Measures of Association Extracted
Using methods described by Hayden and colleagues,33 we extracted unadjusted and adjusted measures of the association between bullying victimization and pain and used odds ratios (ORs) in the natural log scale as the common measure of the relationship. We converted effect sizes to the natural log scale and calculated standard errors (SEs) by log-transforming confidence intervals and then converting using an appropriate formula. We converted standardized regression coefficients for continuous outcomes to natural log ORs.34,35
Data Synthesis
We conducted a meta-analysis when three or more sufficiently homogenous studies assessed the relationship between bullying victimization or a proposed moderator variable and chronic pain. Data were analyzed using Review Manager software (RevMan version 5.3, the Cochrane Collaboration) with a random-effects generic inverse variance meta-analysis model, which allows for between-study heterogeneity in the exposure effect. The meta-analysis was summarized by the pooled estimate (the average exposure effect) and its 95% CI. We conducted these analyses separately using both unadjusted statistics and values adjusted for potential confounders.
To further test the proposed moderation models, we planned to use subgroup analyses to explore between-study differences in the specific nature of bullying victimization, including the type of victimization, presence of bodily injury and the frequency, stability and timing of exposure. We also planned to use subgroup analysis to explore the impact of differences in the timing of outcome measurement, specifically whether the assessment was conducted in early childhood (age 0–5 years), middle childhood (age 6–10 years), or adolescence (11–18 years).
We planned to use sensitivity analysis to explore the impact of other study factors on the relationship between victimization and chronic pain. In particular, we planned to examine the impact of the measurement of chronic pain, risk of bias, and adjustment for confounders by limiting our analyses to studies that 1) clearly captured chronic pain, 2) were assessed as having low risk of bias, and 3) adequately adjusted for confounders.
Interpretation of Results
The strength of observed associations was defined, for binary factors, based on effect size as small (OR < 1.5), moderate (1.5 ≥ OR ≤ 2), or large (OR > 2).33,36 We considered moderate or large effect sizes (OR ≥ 1.5) to be clinically important. Statistical heterogeneity between studies was assessed using the I2 test; heterogeneity was considered important if I2 was greater than 50%. In cases where it was not appropriate to combine results using meta-analysis due to the small number (fewer than 3) of sufficiently homogeneous studies with available data, the results were presented qualitatively.
We used an approach modified from the GRADE (Grading of Recommendations Assessment, Development and Evaluation) framework37,38 to assess the overall quality of evidence on the relationship between bullying victimization and chronic pain. We rated the overall strength of evidence as high, moderate, low or very low considering internal validity, size and precision of effect, heterogeneity, generalizability, and potential reporting bias.
Results
Description of Studies
Results of the Search
Our extensive literature search identified 2535 citations for appraisal against our inclusion and exclusion criteria. We retrieved 59 full-text articles for further assessment and study selection. We initially identified five longitudinal studies examining associations between bullying victimization and pain. Two of these studies reported findings based on cross-sectional aspects of the study data39,40; thus we requested additional data from the study authors to satisfy our inclusion criteria. Biebl and colleagues39 provided a subset of their data,1 whereas Lien and colleagues40 no longer had access. Ultimately, four studies were included. The search was last updated on June 30, 2019. See Figure 1 for the study flow diagram and Table 1 for the characteristics of included studies.
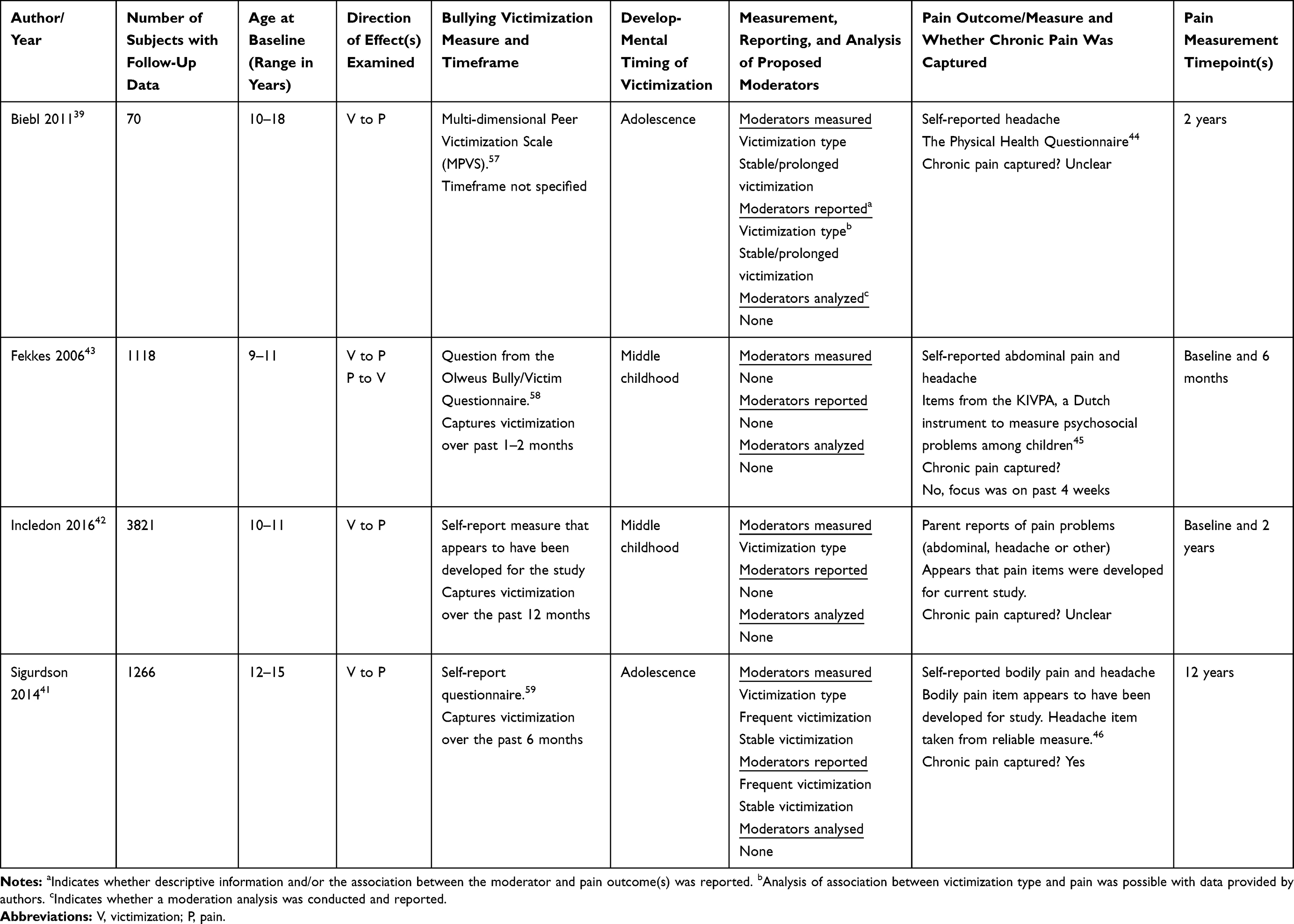 |
Table 1 Characteristics of Included Studies |
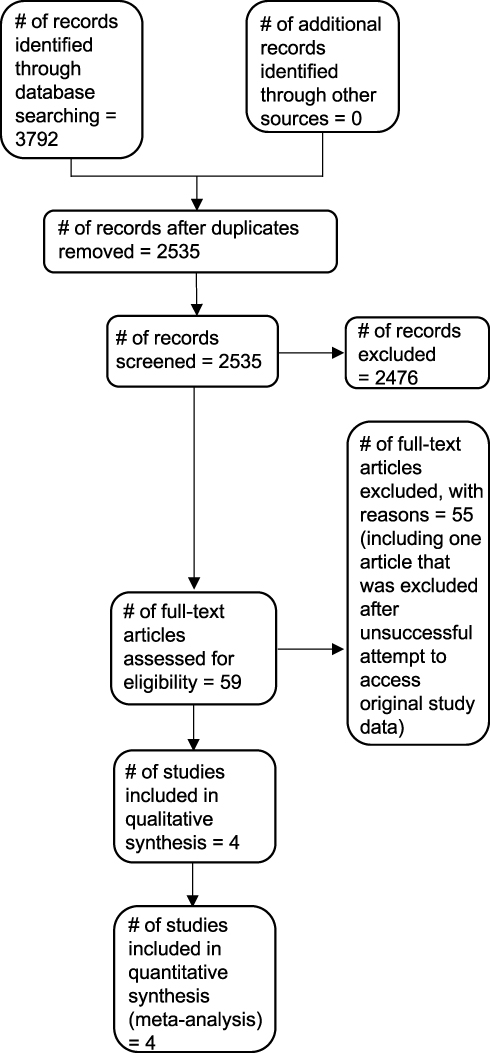 |
Figure 1 Study flow diagram. |
Included Studies
We included a total of four prospective cohort studies in the review. Two studies were conducted in Europe, one was conducted in Australia, and one was conducted in the United States of America. Sample sizes ranged from 70 to 3821. The studies included mixed samples of male and female participants (% female ranged from approximately 49 to 56.7). The mean age of participants at baseline ranged between 10 and 14 years. Follow-up periods ranged from 6 months to 12 years, with two studies following participants into adulthood.39,41
Three included studies examined peer victimization as a risk factor for pain,39,41,42 and one study examined bidirectional relations between victimization and pain.43
Measurement of Bullying Victimization
Each of the included studies measured bullying victimization using self-report questionnaires. One measure comprised a single question (eg, “How often did other children bully you in recent months?”,43 while others tapped the frequency of different types of bullying victimization, such as verbal insults, taunting and/or mocking, physical assault, and being frozen out of friendship groups.39,41 In contrast, Incledon et al37 tapped exposure to different types of bullying rather than frequency per se. One study also used behavioural observations of a 20-minute play session to capture early victim-type behaviours (eg, experiencing repetitive hitting, punching or kicking) among 5-year-olds,39 although these observational data were not available for meta-analysis. Biebl and colleagues provided a subset of their data (ie bullying victimization data from the second timepoint and pain data from the third timepoint), whereas Lien and colleagues no longer had access.
See Table 1 for information regarding the measurement of specific characteristics of bullying victimization, including its type, frequency, stability, and developmental timing.
The Measurement of Pain
Two studies measured site-specific pain, such as headache39,41,43 and abdominal pain,43 and two studies included a measure of bodily pain (ie, unspecified location of pain).41,42 They used self-report measures39,41,43 or parental report.42 Three studies measured pain using validated questionnaires,39,41,43 including The Physical Health Questionnaire,44 the Short Indicative Questionnaire for Psychosocial Problems among Adolescents (KIVPA)45 and the problem scale of the Adult Self Report,46 while other pain questions were developed specifically for the study.41,42
One study captured chronic pain (ie, pain lasting 3 months or more),41 one study reported pain over the past 4 weeks,43 and in the two remaining studies, either the duration or frequency of pain was not reported or it was unclear. Two studies included a measure of pain at baseline.42,43
The Risk of Bias in Included Studies
We judged two studies to have low risk of bias overall.42,43 Although both studies suffered from moderate risk of bias in up to three bias categories, they were determined to have low risk of bias across all other categories and in no case was a rating of high risk of bias made. Two studies were judged to have high risk of bias overall.41 See Supplemental Materials Appendix 4 for the QUIPS risk of bias summary.
Findings
Zero to four studies provided sufficiently similar data regarding each of our research questions, and zero to four studies were available for each of our planned meta-analyses. Given the small number of studies, we were unable to conduct the planned subgroup and sensitivity analyses. Overall, the level of evidence was assessed to be very low quality. See Supplemental Materials Appendix 5 for a summary of the GRADE analysis for each of the main analyses.
Is Baseline Exposure to Bullying Victimization Associated with Pain at Follow-Up?
Very low-quality evidence from four studies (total of 6275 participants) examined the relationship between baseline bullying victimization and pain outcomes at follow-up.39,41–43 Both unadjusted and adjusted results were available for each of these studies. When a study reported findings for more than one pain outcome (eg, abdominal pain and headache), the effect size was combined before inclusion in the meta-analysis.
Meta-analysis of unadjusted statistics showed that victimized individuals were 1.58 times more likely than non-victims to report pain at follow-up (OR [95% CI] = 1.58 [1.23–2.02], n = 4) (statistically significant and clinically important). See Supplemental Materials Appendix 6. There was notable heterogeneity across the studies, with an I2 of 57%. Meta-analysis revealed a similar finding for pooled adjusted results, but with a smaller effect size (OR [95% CI] = 1.45 [1.06–1.97], n = 4) (statistically significant but not clinically important). See Figure 2. Again, there was considerable heterogeneity across the studies (I2=68%). We had planned to explore heterogeneity across studies with a priori defined subgroup analyses, but this was not possible given the small number of included studies in the review. See Supplemental Materials Appendix 5 for GRADE summary.
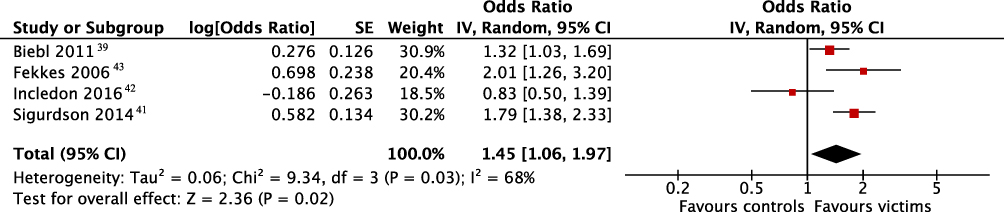 |
Figure 2 Forest plot depicting the results of a random-effects meta-analysis of longitudinal studies investigating the association between baseline bullying victimization and pain at follow-up, adjusted for potential confounders. |
Is Baseline Pain Associated with Bullying Victimization at Follow-Up?
There was very low-quality evidence from one study (947 participants) examining the relationship between baseline pain and bullying victimization at follow-up.43 Both unadjusted and adjusted analyses showed no difference in risk of bullying victimization at follow-up when comparing children with and without pain symptoms at baseline. This finding should be interpreted with caution given the limited evidence available.
Does the Type of Bullying Victimization and the Presence/Absence of Physical Harm Influence the Victimization–Pain Relationship?
There was very low-quality evidence from one study (70 participants) with information about the associations between different types of victimization and pain.39 In multiple regression models, including both relational and physical victimization, adjusted and unadjusted analyses showed that relational victimization but not physical victimization was significantly associated with pain at follow-up (p=0.002). This finding was in the expected direction, such that increased relational victimization at baseline was associated with more frequent headaches two years later even after statistically adjusting for sex and age. Although this analysis is not a direct test of moderation, it suggests that victimization type may influence the victimization–pain relationship. However, this finding should be interpreted with caution given the limited evidence available. In regard to physical injury as a potential moderator, there was no evidence available with information about the association between physical injury and pain.
Do the Frequency and/or Stability of Bullying Victimization Influence the Victimization–Pain Relationship?
There was not enough evidence available to conduct a meaningful synthesis of whether victimization frequency or stability was related to pain outcomes.
Does the Developmental Stage of Bullying Victimization Influence the Victimization–Pain Relationship?
Although the included studies captured victimization at different stages of development (early childhood, middle childhood and adolescence), there were too few included studies to conduct a meaningful analysis of the relationship between developmental stage of the exposure and later pain.
Discussion
The review included four longitudinal studies, with data from 6275 participants. Each of the included studies provided unadjusted and adjusted results for meta-analysis; however, these results were limited in scope and only provided evidence on the relationship between baseline bullying victimization and pain at follow-up. In contrast, only one included study examined the relationship between baseline pain and bullying victimization at follow-up, and for each of our questions about moderating factors, there was either no available evidence or evidence from only a single study. Of particular note, only one of the four included studies actually measured chronic pain, which was our primary outcome variable. The other studies either failed to specify the duration of pain or examined pain occurring for a shorter duration. Therefore, the applicability of our findings to chronic pain is unclear.
Summary of the Main Results
We found very low-quality evidence that bullying victimization was associated with increased risk of pain at follow-up. However, after adjusting for potential covariates, the effect size was small and not clinically important. Moreover, there was substantial heterogeneity across the studies, thereby limiting our ability to interpret the results. Indeed, the variability in effect sizes may be explained by between-study variability in clinical and/or methodological factors, including our pre-specified moderators and the timing of outcome measurement (ie, whether pain was assessed in early childhood, middle childhood, adolescence, or adulthood). However, we were unable to explore these factors due to the small number of included studies, and a dearth of information on the specific nature of bullying victimization. Additional high-quality studies are needed to identify factors that accentuate versus dampen the magnitude of this association.
We found very low-quality evidence from one study that youth who experience pain were at no greater risk of bullying victimization at follow-up compared to their pain-free counterparts. Additional high-quality studies are needed to delineate the temporal ordering of events.
Summary of Additional Findings
Regarding potential moderators of the victimization–pain relationship, we found very low-quality evidence from one study that relational victimization, but not physical victimization, was associated with pain at follow up. Additional work is needed to replicate this finding and to examine whether the relationship holds true when bullying-related bodily injury is accounted for. If so, it would add to mounting evidence showing that emotional injury can be more painful than physical injury.47
None of the included studies examined the association between the frequency, stability, or timing of victimization and pain outcomes, and there were too few studies to conduct comparisons across studies using subgroup analysis. Clearly, high-quality studies that measure and report the nuances of bullying victimization and the presence or absence of bodily harm are needed to test the proposed moderator models. None of the included studies measured secondary outcomes.
Strengths and Limitations of the Review
This review has a number of strengths. First, the methods were planned a priori. This included a pre-specified set of potential moderating variables related to the specific nature of bullying victimization and the presence or absence of physical injury, as well as other factors potentially related to heterogeneity, such as the timing of outcome measurement. Similarly, we considered what it would mean for a model to be minimally versus adequately adjusted and then accounted for the level of control in the risk of bias assessment. Second, we conducted a comprehensive literature search, including an electronic search and a review of references of key articles in the field (eg, previously published reviews) to identify included studies. Third, we judged the overall quality of the evidence, accounting for such factors as risk of bias, size and precision of effect, heterogeneity, generalizability, and potential reporting bias.
This review also has some limitations. First, there is unexplained heterogeneity with many potential sources. In addition to the proposed moderators (which we would expect to account for some of the heterogeneity), there is substantial 1) between-study variability in the measurement of bullying victimization and pain and 2) differences in covariate measurement and adjustment, thereby raising more questions than answers. For example, the Incledon et al42 findings differed from those of the other studies because they revealed no association between baseline bullying victimization and pain at follow-up. However, this pattern of findings could be interpreted in several ways. On the one hand, this is a lower risk of bias study that was well controlled in regard to potential confounders, so it may reflect the true state of affairs (ie, there is no direct relationship between victimization and pain). On the other hand, this study’s ability to detect an association between victimization and pain may have been limited by measurement issues, as we had some concerns about the validity of the bullying victimization measure used. In particular, children in this study were classified into the victimization group if they endorsed three or more types of bullying over the past 12 months. Although this construct is likely to correlate with the frequency of victimization, it fails to capture repeated victimization that is limited to one or two types (eg, repeated verbal victimization or repeated verbal and physical victimization). Clearly, there are many factors and too few studies to accurately pinpoint the sources of variation in the data.
Second, this review may not reflect the full body of work on this topic. Given that this is a prognostic factor review, we suspect the presence of reporting and publication biases due to difficulty publishing findings showing no connection between bullying victimization and pain. Moreover, we excluded non-English studies, thereby limiting the pool of published studies for inclusion in the review. Third, we had concerns about the internal validity (risk of bias) of included studies. In particular, we cannot rule out the impact of study attrition and potential confounding on the study results reported.
Agreements and Disagreements with Other Studies and Reviews
Other reviews in the field have also suggested a positive association between bullying victimization and pain,10,11 but these reviews have generally pointed to a more robust association compared to the current findings. There are a number of factors that may account for these inconsistencies, such as the inclusion of cross-sectional versus longitudinal studies and the particular outcome being studied (eg, pain versus somatic symptoms). Similar to the current findings, previous reviews in the field showed evidence of variability in results across studies. In addition to the potential moderators proposed in the current review, other reviews in the field have pointed to peer and family support, including having a best friend, as important moderating factors.6,18 Some reviews point to gender as a key moderator,10,11 while others suggest uniform associations across gender.6 These effects may be difficult to pin down due to interactions between various moderators. For example, the role of peer and family support may depend on the developmental stage,6 and gender may interact with the type of bullying to shape outcomes.48 Indeed, well-powered studies are needed to do a comprehensive test of theoretically grounded moderator models.
Implications for Research
The findings from this review suggest that there is a small but statistically significant longitudinal relationship between bullying victimization and pain in youth, yet there remain many unanswered questions about the nature of this relationship. For example, we cannot say whether victimization precedes pain, pain precedes victimization, or if there is a bidirectional relationship between the two. Moreover, not only were we unable to answer our questions about the proposed moderator models and whether there are specific contexts that magnify versus dampen the victimization–pain relationship, but the findings from our meta-analysis raised additional questions. For example, the attenuated effect in the adjusted compared to the unadjusted meta-analyses suggests that victimization may exert its effects through indirect pathways. Indeed, the findings reported by Incledon and colleagues42 suggest that factors such as “at-risk child mental health” and sleep difficulties are directly associated with children’s pain outcomes and may therefore represent key pathways from victimization to pain.
To further delineate the psychological and emotional pathways from victimization to pain, we recommend direct tests of mediation models, including symptoms of anxiety, depression, and post-traumatic stress disorder (PTSD). Symptoms of PTSD have been linked to both bullying victimization and chronic pain and therefore may be particularly relevant.49,50 Moreover, given that health behaviours may represent an important pathway to pain in youth, factors such as the sleep difficulties identified by Incledon and colleagues,42 as well as cigarette smoking and drug and alcohol use, should also be examined as potential mediators.51,52
Ideally, data from large prospective cohort studies with long follow-ups would be available to tackle these questions directly, but it is likely to be years or decades before such data become available. Therefore, we suggest the use of alternative methods to begin to illuminate the nature of the victimization–pain relationship. One possibility would be to use a postsurgical pain model to examine whether victimization status prior to surgery predicts pain trajectories across the recovery period and beyond.53 This type of study could shed light on the role of bullying victimization in the development of chronic pain following physical insult (ie, the surgical intervention). Another possibility would be to examine the relationship between bullying histories (taken retrospectively) and longitudinal pain outcomes, such as the emergence and persistence of pain in adolescence.
Acknowledgment
This work was supported by an Ontario Mental Health Foundation Studentship (TJM) and a Canadian Institutes of Health Research Canada Research Chair in Health Psychology (JK). The protocol for the review was registered with PROSPERO, record ID 133146. Teresa Marin is now at St. Joseph’s Healthcare Hamilton, 100 West 5th Campus, Hamilton, ON L8N 3K7.
Disclosure
The current article is part of the PhD dissertation of the lead author. The authors report no conflicts of interest in this work.
References
1. Arseneault L. Annual research review: the persistent and pervasive impact of being bullied in childhood and adolescence: implications for policy and practice. J Child Psychol Psychiatry. 2018;59:405–421. doi:10.1111/jcpp.12841
2. Bogart LM, Elliott MN, Klein DJ, et al. Peer victimization in fifth grade and health in tenth grade. Pediatrics. 2014;133:440. doi:10.1542/peds.2013-3510
3. Koyanagi A, Oh H, Carvalho AF, et al. Bullying victimization and suicide attempt among adolescents aged 12–15 years from 48 countries. J Am Acad Child Adolesc Psychiatry. 2019;58(907–918):e4. doi:10.1016/j.jaac.2018.10.018
4. Zwierzynska K, Wolke D, Lereya TS. Peer victimization in childhood and internalizing problems in adolescence: a prospective longitudinal study. J Abnorm Child Psychol. 2013;41:309–323. doi:10.1007/s10802-012-9678-8
5. Lereya ST, Copeland WE, Costello EJ, Wolke D. Adult mental health consequences of peer bullying and maltreatment in childhood: two cohorts in two countries. Lancet Psychiatry. 2015;2:524–531. doi:10.1016/S2215-0366(15)00165-0
6. McDougall P, Vaillancourt T. Long-term adult outcomes of peer victimization in childhood and adolescence: pathways to adjustment and maladjustment. Am Psychol. 2015;70:300. doi:10.1037/a0039174
7. Takizawa R, Maughan B, Arseneault L. Adult health outcomes of childhood bullying victimization: evidence from a five-decade longitudinal British birth cohort. Am J Psychiatry. 2014;171:777–784. doi:10.1176/appi.ajp.2014.13101401
8. Wolke D, Copeland WE, Angold A, Costello EJ. Impact of bullying in childhood on adult health, wealth, crime, and social outcomes. Psychol Sci. 2013;24:1958–1970. doi:10.1177/0956797613481608
9. Wolke D, Lereya ST. Long-term effects of bullying. Arch Dis Child. 2015;100:879–885. doi:10.1136/archdischild-2014-306667
10. Gini G, Pozzoli T. Bullied children and psychosomatic problems: a meta-analysis. Pediatrics. 2013;132:720–729. doi:10.1542/peds.2013-0614
11. Gini G, Pozzoli T, Lenzi M, Vieno A. Bullying victimization at school and headache: a meta‐analysis of observational studies. Headache. 2014;54:976–986. doi:10.1111/head.12344
12. Schacter HL. Effects of peer victimization on child and adolescent physical health. Pediatrics. 2021;147(1):147. doi:10.1542/peds.2020-003434
13. Brattberg G. Do pain problems in young school children persist into early adulthood? A 13‐year follow‐up. Eur J Pain. 2004;8:187–199. doi:10.1016/j.ejpain.2003.08.001
14. Stanford EA, Chambers CT, Biesanz JC, Chen E. The frequency, trajectories and predictors of adolescent recurrent pain: a population-based approach. Pain. 2008;138:11–21. doi:10.1016/j.pain.2007.10.032
15. Walker LS, Sherman AL, Bruehl S, Garber J, Smith CA. Functional abdominal pain patient subtypes in childhood predict functional gastrointestinal disorders with chronic pain and psychiatric comorbidities in adolescence and adulthood. Pain. 2012;153:1798–1806. doi:10.1016/j.pain.2012.03.026
16. Nordhagen R, Nielsen A, Stigum H, Köhler L. Parental reported bullying among Nordic children: a population‐based study. Child Care Health Dev. 2005;31:693–701. doi:10.1111/j.1365-2214.2005.00559.x
17. Van Cleave J, Davis MM. Bullying and peer victimization among children with special health care needs. Pediatrics. 2006;118:e1212–e1219. doi:10.1542/peds.2005-3034
18. Forgeron PA, King S, Stinson JN, McGrath PJ, MacDonald AJ, Chambers CT. Social functioning and peer relationships in children and adolescents with chronic pain: a systematic review. Pain Res Manage. 2010;15:27–41. doi:10.1155/2010/820407
19. Dukes RL, Stein JA, Zane JI. Gender differences in the relative impact of physical and relational bullying on adolescent injury and weapon carrying. J Sch Psychol. 2010;48:511–532. doi:10.1016/j.jsp.2010.08.001
20. Burke NN, Finn DP, McGuire BE, Roche M. Psychological stress in early life as a predisposing factor for the development of chronic pain: clinical and preclinical evidence and neurobiological mechanisms. J Neurosci Res. 2017;95:1257–1270. doi:10.1002/jnr.23802
21. Katz J, Pagé MG, Fashler S, Rosenbloom BN, Asmundson GJG. Chronic pain and the anxiety disorders: epidemiology, mechanisms and models of comorbidity, and treatment. In: Gaumond I, Saravane D, Marchand S, editors. Mental Health and Pain. New York: Springer; 2014:119–155.
22. McEwen BS. Stress, adaptation, and disease. Allostasis and allostatic load. Ann N Y Acad Sci. 1998;840:33–44. doi:10.1111/j.1749-6632.1998.tb09546.x
23. Bingham B, McFadden K, Zhang X, Bhatnagar S, Beck S, Valentino R. Early adolescence as a critical window during which social stress distinctly alters behavior and brain norepinephrine activity. Neuropsychopharmacology. 2011;36:896. doi:10.1038/npp.2010.229
24. Sumter SR, Bokhorst CL, Miers AC, Van Pelt J, Westenberg PM. Age and puberty differences in stress responses during a public speaking task: do adolescents grow more sensitive to social evaluation. Psychoneuroendocrinology. 2010;35:1510–1516. doi:10.1016/j.psyneuen.2010.05.004
25. Marin TJ, Katz J. Childhood bullying victimization and the development and persistence of chronic pain: a systematic review of prospective studies. PROSPERO. 2019.
26. Treede R-D, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP Classification of Chronic Pain for the: international Classification of Diseases: (ICD-11). Pain. 2019;160:19–27. doi:10.1097/j.pain.0000000000001384
27. Melzack R. The short-form McGill pain questionnaire. Pain. 1987;30:191–197. doi:10.1016/0304-3959(87)91074-8
28. Higgins KS, Birnie KA, Chambers CT, et al. Offspring of parents with chronic pain: a systematic review and meta-analysis of pain, health, psychological, and family outcomes. Pain. 2015;156:2256. doi:10.1097/j.pain.0000000000000293
29. Boulos L, Ogilvie R, Hayden JA. Search methods for prognostic factor systematic reviews: a methodologic investigation. J Med Lib Assoc. 2021;109:23. doi:10.5195/jmla.2021.939
30. Copeland WE, Wolke D, Lereya ST, Shanahan L, Worthman C, Costello EJ. Childhood bullying involvement predicts low-grade systemic inflammation into adulthood. Proc Natl Acad Sci. 2014;111:7570–7575. doi:10.1073/pnas.1323641111
31. Reijntjes A, Kamphuis JH, Prinzie P, Telch MJ. Peer victimization and internalizing problems in children: a meta-analysis of longitudinal studies. Child Abuse Negl. 2010;34:244–252. doi:10.1016/j.chiabu.2009.07.009
32. Hayden JA, van der Windt DA, Cartwright JL, Cote P, Bombardier C. Assessing bias in studies of prognostic factors. Ann Intern Med. 2013;158:280–286. doi:10.7326/0003-4819-158-4-201302190-00009
33. Hayden JA, Wilson MN, Riley RD, Iles R, Pincus T, Ogilvie R. Individual recovery expectations and prognosis of outcomes in non‐specific low back pain: prognostic factor review. Cochrane Database Syst Rev. 2019. doi:10.1002/14651858.CD011284.pub2
34. Borenstein M, Hedges L, Higgins J, Rothstein H. Introduction to Meta-Analysis. Chichester, West Sussex: John Wiley & Sons; 2009.
35. Peterson RA, Brown SP. On the use of beta coefficients in meta-analysis. J Appl Psychol. 2005;90:175. doi:10.1037/0021-9010.90.1.175
36. Hartvigsen J, Lings S, Leboeuf-Yde C, Bakketeig L. Psychosocial factors at work in relation to low back pain and consequences of low back pain; a systematic, critical review of prospective cohort studies. Occupational Environ Med. 2004;61:e2.
37. Guyatt GH, Oxman AD, Schünemann HJ, Tugwell P, Knottnerus A. GRADE guidelines: a new series of articles in the Journal of Clinical Epidemiology. J Clin Epidemiol. 2011;64:380–382. doi:10.1016/j.jclinepi.2010.09.011
38. Hayden JA, Tougas ME, Riley R, Iles. Individual recovery expectations and prognosis of outcomes in non-specific low back pain: prognostic factor exemplar review (Protocol). Cochrane Database Syst Rev. 2014;9.
39. Biebl SJW, DiLalla LF, Davis EK, Lynch KA, Shinn SO. Longitudinal associations among peer victimization and physical and mental health problems. J Pediatr Psychol. 2011;36:868–877. doi:10.1093/jpepsy/jsr025
40. Lien L, Welander-Vatn A. Factors associated with the persistence of bullying victimization from 10th grade to 13th grade: a longitudinal study. Clin Pract Epidemiol Mental Health. 2013;9:243. doi:10.2174/1745017901309010243
41. Sigurdson JF, Wallander J, Sund AM. Is involvement in school bullying associated with general health and psychosocial adjustment outcomes in adulthood. Child Abuse Negl. 2014;38:1607–1617. doi:10.1016/j.chiabu.2014.06.001
42. Incledon E, O’Connor M, Giallo R, Chalkiadis GA, Palermo TM. Child and family antecedents of pain during the transition to adolescence: a longitudinal population-based study. J Pain. 2016;17:1174–1182. doi:10.1016/j.jpain.2016.07.005
43. Fekkes M, Pijpers FIM, Fredriks AM, Vogels T, Verloove-Vanhorick SP. Do bullied children get ill, or do ill children get bullied? A prospective cohort study on the relationship between bullying and health-related symptoms. Pediatrics. 2006;117:1568–1574. doi:10.1542/peds.2005-0187
44. Schat ACH, Kelloway EK, Desmarais S. The Physical Health Questionnaire (PHQ): construct validation of a self-report scale of somatic symptoms. J Occup Health Psychol. 2005;10:363. doi:10.1037/1076-8998.10.4.363
45. Reijneveld SA, Vogels AGC, Brugman E, Van Ede J, Verhulst FC, Verloove‐Vanhorick SP. Early detection of psychosocial problems in adolescents: how useful is the Dutch short indicative questionnaire (KIVPA). Eur J Public Health. 2003;13:152–159. doi:10.1093/eurpub/13.2.152
46. Achenbach TM, Rescorla LA. Manual for the ASEBA Adult Forms & Profiles. 2003.
47. Atlas RS, Pepler DJ. Observations of bullying in the classroom. J Educ Res. 1998;92:86–99. doi:10.1080/00220679809597580
48. Kim S, Colwell SR, Kata A, Boyle MH, Georgiades K. Cyberbullying victimization and adolescent mental health: evidence of differential effects by sex and mental health problem type. J Youth Adolesc. 2018;47:661–672. doi:10.1007/s10964-017-0678-4
49. Idsoe T, Dyregrov A, Idsoe EC. Bullying and PTSD symptoms. J Abnorm Child Psychol. 2012;40:901–911. doi:10.1007/s10802-012-9620-0
50. Noel M, Wilson AC, Holley AL, Durkin L, Patton M, Palermo TM. Post-traumatic stress disorder symptoms in youth with versus without chronic pain. Pain. 2016;157:2277. doi:10.1097/j.pain.0000000000000642
51. Ghandour RM, Overpeck MD, Huang ZJ, Kogan MD, Scheidt PC. Headache, stomachache, backache, and morning fatigue among adolescent girls in the United States: associations with behavioral, sociodemographic, and environmental factors. Arch Ped Adolescent Med. 2004;158:797–803. doi:10.1001/archpedi.158.8.797
52. Hoftun GB, Romundstad PR, Rygg M. Factors associated with adolescent chronic non-specific pain, chronic multisite pain, and chronic pain with high disability: the Young-HUNT Study 2008. J Pain. 2012;13:874–883. doi:10.1016/j.jpain.2012.06.001
53. Katz J, Seltzer Z. Transition from acute to chronic postsurgical pain: risk factors and protective factors. Expert Rev Neurother. 2009;9(5):723–744. doi:10.1586/ern.09.20
54. Cleeland CS. Measurement of pain by subjective report. In: Chapman CR, Loeser JD, editors. 12. New York: Raven; 1989.
55. Cleeland CS, Ryan KM. Pain assessment: global use of the Brief Pain Inventory. Ann Acad Med Singapore. 1994;23:129–138.
56. Turk DC, Melzack R, eds. Handbook of Pain Assessment.
57. Mynard H, Joseph S. Development of the multidimensional peer‐victimization scale. Aggressive Behav. 2000;26:169–178. doi:10.1002/(SICI)1098-2337(2000)26:2<169::AID-AB3>3.0.CO;2-A
58. Olweus D. Bullying at school: basic facts and effects of a school based intervention program. J Child Psychol Psychiatry. 1994;35:1171–1190. doi:10.1111/j.1469-7610.1994.tb01229.x
59. Alsaker FD. Quälgeister und ihre Opfer. Mobbing unter Kindern-und wie man damit umgeht Bern: Hans Huber. 2003.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.