")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 17
A Systematic Review of the Economic Burden of Diabetes in Eastern Mediterranean Region Countries
Authors Arshad MS , Alqahtani F , Rasool MF
Received 14 September 2023
Accepted for publication 11 January 2024
Published 1 February 2024 Volume 2024:17 Pages 479—487
DOI https://doi.org/10.2147/DMSO.S440282
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Muhammad Subhan Arshad,1,2 Faleh Alqahtani,3 Muhammad Fawad Rasool1
1Department of Pharmacy Practice, Faculty of Pharmacy, Bahauddin Zakariya University, Multan, 60800, Pakistan; 2Department of Pharmacy, Southern Punjab Institute of Health Sciences, Multan, 60000, Pakistan; 3Department of Pharmacology and Toxicology, College of Pharmacy, King Saud University, Riyadh, 11451, Saudi Arabia
Correspondence: Muhammad Fawad Rasool; Faleh Alqahtani, Email [email protected]; [email protected]
Abstract: Diabetes Mellitus (DM) is a highly prevalent non-communicable disease with high mortality and morbidity, which imposes a significant financial impact on individuals and the healthcare system. The identification of various cost components through cost of illness analysis could be helpful in health-care policymaking. The current systematic review aims to summarize the economic burden of DM in the Eastern Mediterranean Region (EMR) countries. The original studies published in the English language between January 2010 and June 2023 reported the cost of DM was identified by searching four different databases (Google Scholar, PubMed, Science Direct, and Cochrane Central). Two reviewers independently screened the search results and extracted the data according to a predefined format, whereas the third reviewer’s opinion was sought to resolve any discrepancies. The costs of DM reported in the included studies were converted to USD dates reported in the studies. After the systematic search and screening process, only 10 articles from EMR countries met the eligibility criteria to be included in the study. There are substantial variations in the reported costs of DM and the methodologies used in the included studies. The mean annual cost per patient of DM (both direct and indirect cost) ranged from 555.20 USD to 1707.40 USD. The average annual direct cost ranged from 155.8 USD to 5200 USD and indirect cost ranged from 93.65 USD to 864.8 USD per patient. The studies included in the review obtained a median score of 8.65 (6.5 ─ 11.5) on the quality assessment tool based on Alison’s checklist for evaluation of cost of illness studies. There is a significant economic burden associated with DM, which directly affects the patients and healthcare system. Future research should focus on refining cost estimation methodologies, improving the understanding of study findings, and making it easier to compare studies.
Keywords: cost of illness, economic cost, healthcare cost, direct cost, indirect cost, diabetes
Introduction
Diabetes Mellitus (DM) has emerged as one of our era’s most common and severe non-communicable chronic illnesses with a leading cause of morbidity and mortality.1 DM entered the top 10 causes of death and disability in 2019, with 1.5 million deaths and 70.4 million disability-adjusted life years (DALYs).2 According to the first global report of the World Health Organization (WHO) on diabetes, approximately 422 million adults around the Globe had DM in 2014.3 As per the latest report by the International Diabetes Federation (IDF), around 537 million people had DM in 2021 worldwide, which was projected to increase to 783 billion in 2045.4 This rapid increase in the prevalence of DM is imposing a substantial economic burden on healthcare systems. In 2021, the DM was responsible for approximately 966 billion USD in global healthcare expenditure, which was expected to increase to 1045 billion USD by 2045.4
The Eastern Mediterranean Region (EMR) is one of six zones into which WHO classifies its member states, which includes 21 member countries from Pakistan to Morocco and a population of around 745 million people.5 EMR had the highest prevalence of DM (13.7%) among all WHO regions in 2014, according to the WHO’s global report on DM.3 Similarly, according to the latest IDF regional report, this region had the highest DM prevalence (16.2%) in 2021. At the same time, DM-related healthcare spending in the EMR was estimated to be 32.6 billion USD overall in 2021, projected to increase to 46.3 billion USD by 2045 due to rapidly growing prevalence in that region.4
The cost of illness (COI) analysis is the most common approach used to evaluate the economic burden of a disease on the individual patients, society, and healthcare system of a country. COI analysis identifies and quantifies all the costs related to the aspects of a disease, such as direct costs (medical and non-medical costs), indirect costs, and intangible costs that collectively contribute to the overall economic cost of that disease.6 Identifying the costs of a disease is crucial for national and international health-care policy-making to develop or improve a cost-effective solution for disease management.7
The various associated complications and the chronic nature of DM make it a costly disease.8 EMR had the highest regional prevalence of DM among WHO-classified regions and was also predicted to be the hot spot for DM in the future.4 In contrast, the healthcare financing systems of EMR countries are already facing challenges that require a strategic allocation of resources.9 There are few studies published from EMR countries addressing the COI of DM, but no systematic review has been conducted in EMR which tends to summarise the findings, methodologies, and gaps in published literature about the COI of DM. However, a meta-analysis was conducted in 2019 to estimate the cost of diabetes in EMR countries, which included only studies eligible for meta-analysis.10 Thus, the current systematic review aimed to summarize the findings of the studies published in EMR countries regarding the COI of DM and provide recommendations for the conduction of future studies.
Methods
Study Design
This systematic review followed the predefined protocol following Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines.11 The current systematic review was registered in the “International Prospective Register of Systematic Reviews (PROSPERO)” against registration number CRD42023453099.
Data Sources and Search Strategy
The relevant studies reporting the cost of DM were identified by searching the following electronic databases PubMed, Google Scholar, Science Direct, and Cochrane Central Library until 30 June 2023. The following keywords, including relevant terms along with Boolean operators, were used to find relevant articles in these databases (1) DM-related terms (“Diabetes” OR “Diabetic” OR “Diabetes Mellitus”) AND (2) terms related to costs “Cost of Illness” OR “Cost and Cost Analysis” OR “Direct and Indirect Costs” OR “Economic burden” OR “Cost of Disease.” Medical subject heading (MeSH) terms were used to search the PubMed database. The final search string used for PubMed was as follows: “Diabetes Mellitus”[Mesh] AND “Cost of Illness”[Mesh] OR “Cost and Cost Analysis”[Mesh] OR “Direct and Indirect Costs”[Mesh] OR “Economic burden”[Mesh] OR “Cost of Disease”[Mesh]. Whereas a similar string without Mesh terms was used to search in remaining databases ie Google Scholar, Science Direct, and Cochrane Central Library. The timeframe for the search was limited to studies published between January 2010 and June 2023. The reference lists of included articles were also searched to find more relevant articles.
Inclusion and Exclusion Criteria
The search results were assessed for relevance to be included in the present systematic review using the inclusion and exclusion criteria listed below. The studies were considered eligible for inclusion in this review if they met the following inclusion criteria: (1) original research, (2) English language (3) conducted in countries classified as EMR by WHO (4) reported the cost of illness (direct/indirect costs) for Type 1 or Type 2 DM. Exclusion criteria for studies were as follows: (1) Economic analysis of drugs or treatments (2) Gestational DM, (3) Only provided projected cost data (4) Only presented costs related to DM prevention, (5) Demonstrated poor methodology (6) Review papers, case reports, conference abstracts, editorials, comments, or letters (7) Involved animal studies.
Screening and Data Extraction
The search results identified during the database search were imported to Endnote software, and duplicates were removed using it. Only articles with the phrases “costs” and “diabetes” or similar words in the title were included in the first stage. Studies conducted outside EMR countries and mentioned in their titles were excluded during title screening. In the second step, the abstracts of studies retrieved after title screening were evaluated following inclusion and exclusion criteria. If necessary, the full text of the studies was also assessed. The whole process was conducted by two reviewers individually, and the opinion of a third reviewer was sought in case of any discrepancy or uncertainty between the two reviewers.
The included studies’ quality was evaluated per previously published reviews and guidelines.12–14 The quality assessment tool was comprised of 15 items and each item was rated with the highest score of 1, partial with 0.5, and lowest with a score of 0, whereas the studies having a total score of less than 5 were considered of poor quality. That tool was categorized into four sections (ie General, Sample, Costs, and Methods). The first section was comprised of two questions about a general description of the disease ie definition of diabetes and the inclusion of its complications. The second section was about the study sample, with two items regarding the reliability of data sources and the appropriateness of the evaluation period. The third section was comprised of five items about the cost evaluated in the studies like the inclusion of relevant costs, its appropriateness to the objectives of the study, documentation/justification for cost components, and limitations regarding cost calculation. The fourth section was regarding methodologies used for conducting the study with six items ie representation of study population (Prevalence/Incidence), the approach used (Bottom-Up/Top-down), cost estimation method (Incremental/Total cost), standard deviation/mean calculation, sensitivity analysis, and statistical methods used.
The two reviewers extracted important information regarding the methodology and findings of the included studies under the prescribed format presented in Tables 1–3. To summarize the characteristics of the included studies, data were extracted against the following variables ie study design (Prospective/Retrospective/Cross-sectional and Prevalence-based/Incidence-based), data sources (patient surveys/medical records/Ministry data), Sample size, study perspectives (Patient/Healthcare system/Societal/Third-party payers) type of costs (Direct medical cost/direct non-medical cost/Indirect cost/Intangible cost) that can be seen in Table 1. The findings of the included studies are summarized in Table 2 which includes the costs of diabetes (Direct cost/Indirect cost/Total cost) along with costing year, study population (based on the age of participants), and type of diabetes to compare the cost difference in those studies. To enable comparison across studies conducted at different times and in different countries, all reported costs were converted to USD (if in other currencies) using that year’s foreign exchange rates and then adjusted to USD 2023 rates using the Official Data Foundation’s consumer price index (CPI) inflation calculator.15 A third reviewer reviewed the extracted data. Any disagreement between two reviewers about the extracted data was resolved by discussion and additional opinion was obtained from third reviewer if necessary.
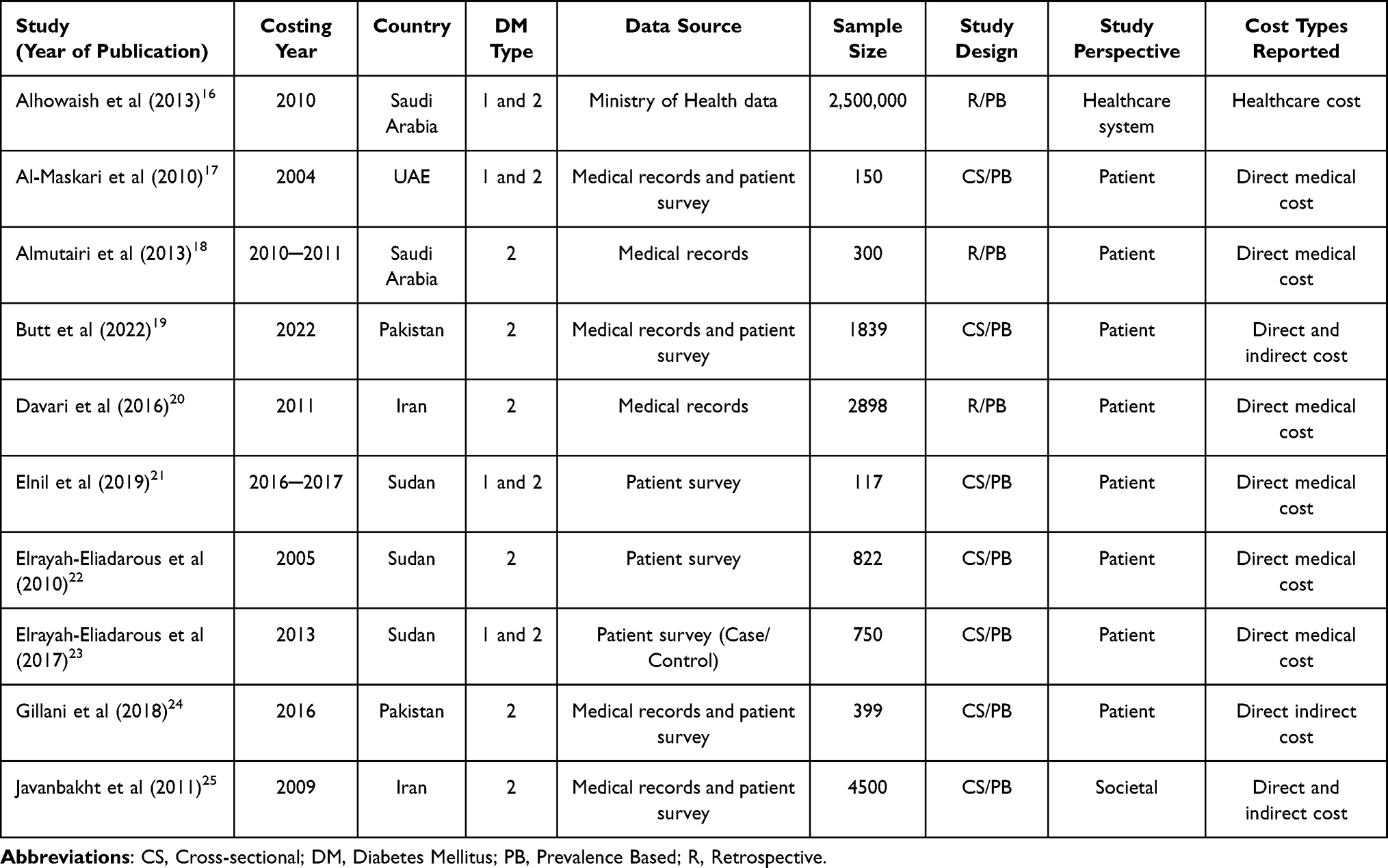 |
Table 1 Characteristics of the Studies Included in the Review from Eastern Mediterranean Region Countries Regarding the Economic Cost of Diabetes Mellitus |
 |
Table 2 The Findings of the Included Studies Regarding Mean Annual Costs of Diabetes Mellitus per Patient in Accordance with Reporting and Year of Costing |
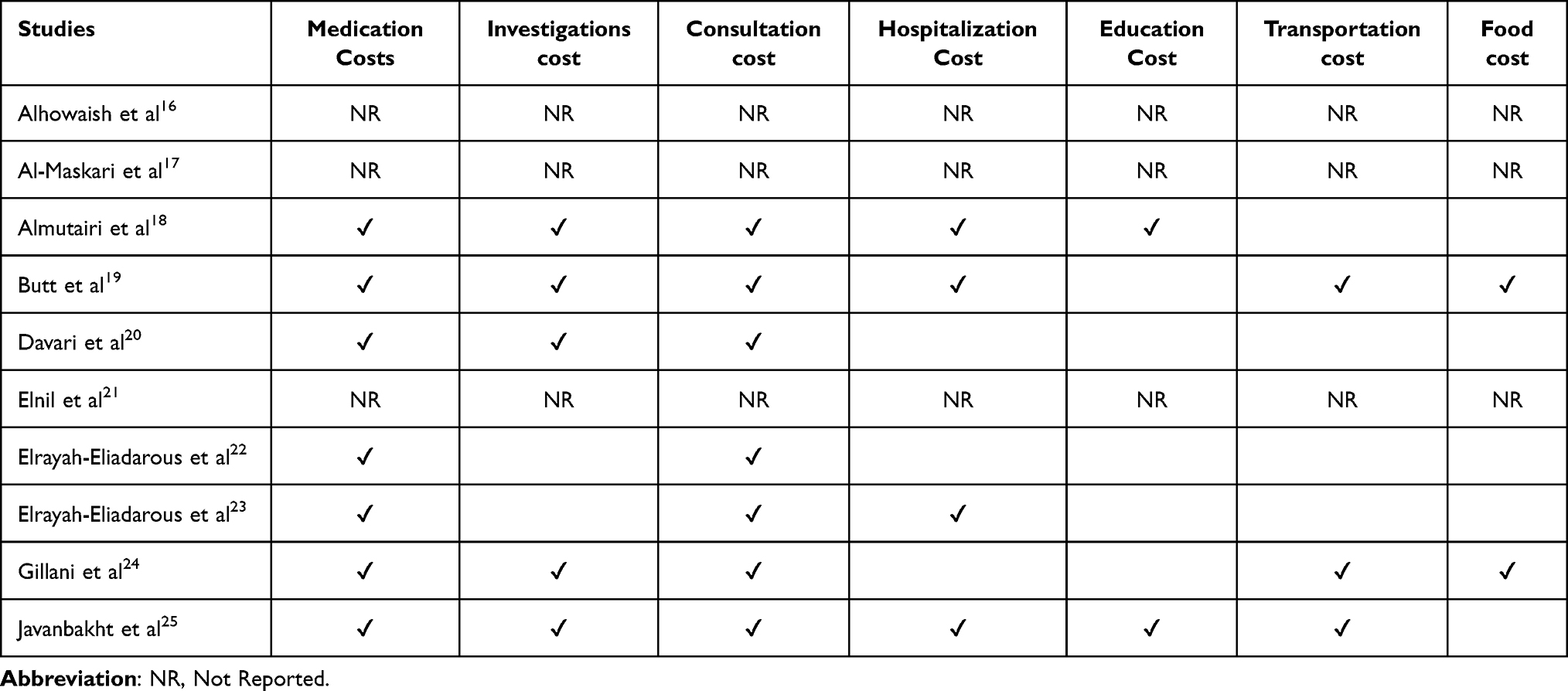 |
Table 3 Components of Direct Cost for Diabetes Mellitus Reported in Included Studies |
Results
The initial search from different databases yielded a total of 2816 articles, from which a total of 392 duplicates were removed. The remaining 2424 articles were screened based on the title in the first screening step, during which 2362 articles were excluded. From the remaining 62 articles, only 17 were retrieved during the second step of screening, which was conducted based on the abstract. In the end, only 10 articles were included in the study, although 7 articles were excluded during the articles’ full-text assessment as they did not meet eligibility criteria. Whereas among these excluded studies one was excluded due to poor quality whose details can be seen in Supplementary Table S1. The details of the study selection process can be seen in Figure 1.
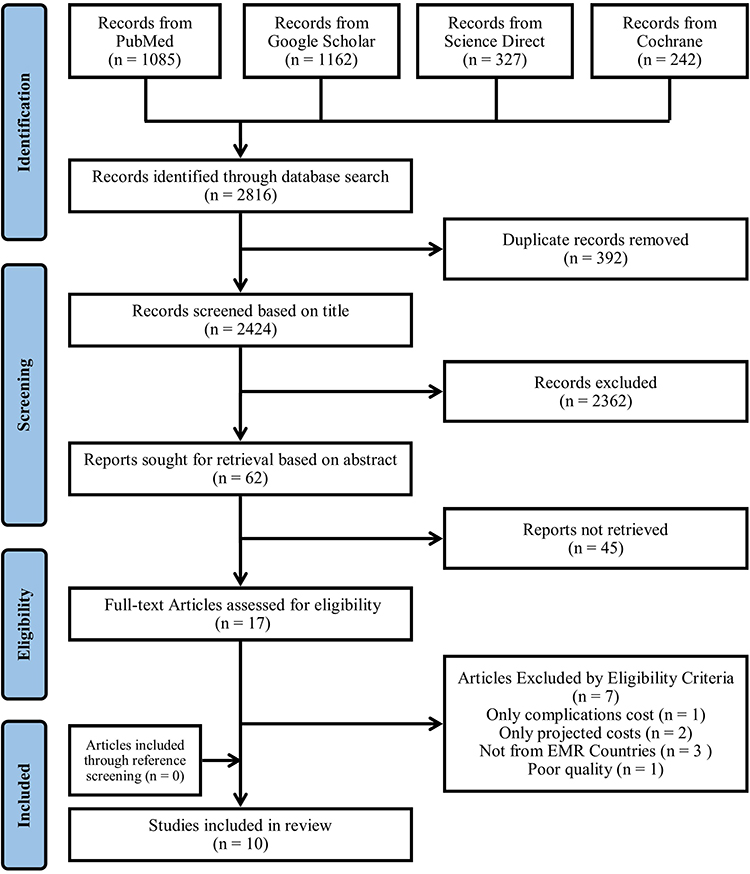 |
Figure 1 PRISMA flow chart of the study selection process. |
The summary of the characteristics of the included studies (n = 10) is presented in Table 1. Among these included studies three studies were conducted in Sudan.21–23 The remaining were completed in Pakistan,19,24 Iran,20,25 and Saudi Arabia16,18 (two studies in each country), and one study was conducted in the UAE.17 Only three studies calculated the overall cost of DM, including direct and indirect costs,19,24,25 while the remaining calculated only the direct medical cost of DM. However, the majority of the studies were conducted from the patient’s perspective (n = 8) with a cross-sectional study design (n = 7).
The costs of DM reported in the included studies are presented in Table 2. The total cost of DM, including direct and indirect costs, ranges from 1707.4 US$25 per patient per year (PPPY) in Iran to 555.20 US$24 and 740.10 US$19 PPPY in Pakistan. These studies reporting total costs also demonstrated that the direct cost was higher than the indirect cost. Even though the most increased direct medical cost was reported from UAE as 5200 US$ PPPY17 to the lowest in Iran as 155.80 US$ PPPY.20 The second highest direct costs of diabetes were reported in the studies from Saudi Arabia as 3686 US$ PPPY16 and 2,331.82 US$ PPPY.18 The Sudan studies reported median costs ranging from 579 US$ PPPY to 175 US$ PPPY. Only three studies reported the indirect cost of DM, ranging from 864 US$ PPPY in Iran to 223.2 US$ and 93.65 US$ PPPY in Pakistan.
The reported components of the costs of DM vary across studies (Table 3). Most of the studies included medication, investigations, consultations, and hospitalization costs as part of direct medical costs; however, transportation and food costs were included as direct non-medical costs. The average annual direct medical costs of DM per patient after adjusting according to the USD rate in 2023 by using the CPI method are presented in Figure 2. The mean direct cost was highest in the UAE at 8399 US$ PPPY followed by Saudi Arabia at 5158 US$ and 3163 US$ PPPY, whereas the lowest in Iran at 211 US$ PPPY.
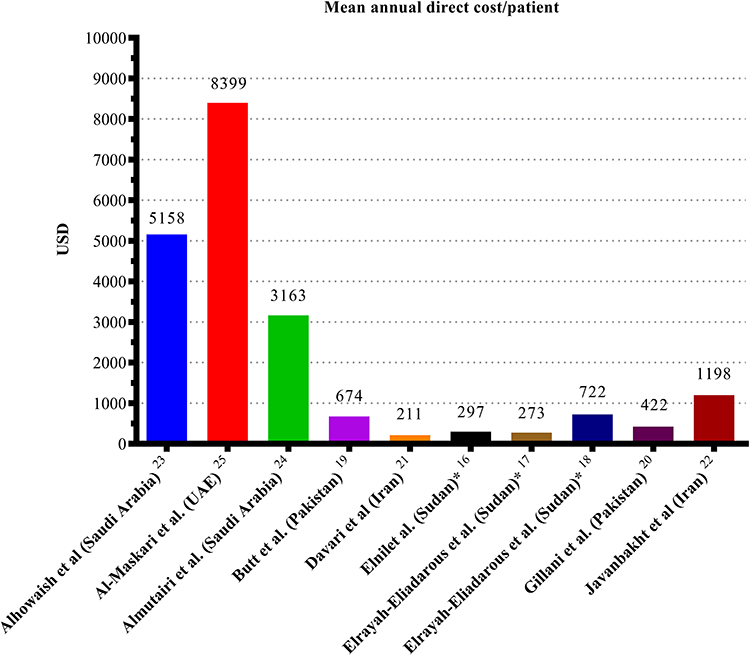 |
Figure 2 The mean annual direct cost of Diabetes Mellitus per patient according to USD rate in 2023. Notes: All costs are inflated to USD rate in 2023 by consumer price index method; *Median annual direct cost/patient. |
Quality assessment is necessary to conduct a good-quality review, especially focusing on the important components of the included studies. A quality assessment tool based on Alison’s checklist for critical evaluation for cost of illness studies with 15 items used to evaluate the included studies. The median score was 8.65 (Range: 6.5 ─ 11.5). The majority of the studies of this review lack a clear definition of diabetes and its types. While only three studies clearly defined diabetes and its types. There were only two studies considered and specified the complications of diabetes. Most of the studies were performed over a satisfactory period of 6 months, where only two studies did not meet this satisfactory period. The majority of studies used self-assessment/questionnaire to collect data and only four studies mentioned their verification through bills. The suitability of the cost components is also considered during quality assessment in accordance with the objectives of the included study as well as the minimum requirement of a COI study (ie cost components, data sources, approach, and use of sensitivity analysis) details can be seen in Supplementary Table S1. Considering the methodologies used by the included studies, all studies were prevalence-based with a bottom-up approach. Whereas only four studies performed linear regression analysis.
Discussion
The prevalence of DM is increasing enormously and causing a high economic burden to society, the healthcare system, and individuals. EMR has the highest prevalence among other regions in the world and was also predicted to be the hotspot for DM in the future. Therefore, the current systematic review aims to assess the economic burden of DM by appraising the studies published in EMR countries. This review revealed a variation in the methodology used to assess the cost of DM, and the majority of the studies only assessed the direct medical cost.
The availability of the data usually influences the methodology used by the authors to estimate the disease’s cost, affecting the results. Most of the studies in the current review used patient surveys to acquire data regarding the cost of DM, with sample sizes ranging from 11721 to 4500.25 In comparison, this is the most commonly employed method to collect data in LMICs.12 As a result, these studies are limited to specific diabetic population from particular centers in the country, rather than data from national-level registers. Only one study from Saudi Arabia used the Ministry of Health with the perspective of the healthcare system to calculate the cost of DM.16
Most reviewed studies reported only the direct medical cost of DM, whereas only three studies also reported the indirect cost of DM. Indirect costs reported by these studies were lesser than direct costs in contrast to common opinion.26,27 There was a variation in the costs reported by the studies, possibly due to differences in the inclusion of cost components, methodology, and study population. Therefore, comparisons between studies should be made with caution. Only four studies calculated the cost for both type 1 and 2 DM while the remaining calculated the cost for type 2 DM only, which could be a possible reason for this variation in the reported direct cost of DM. Because insulin replacement therapy is an expensive treatment option in comparison to oral hypoglycemic agents, patients with type 1 DM are only recommended with insulin replacement therapy that makes it more expensive than type 2 DM. On the other hand, there were differences even in the components of the direct cost calculated by included studies that could be a reason behind these significant differences between costs reported by different studies from the same country like Sudan and Saudi Arabia. The costs of DM reported by studies from high-income countries (HICs), ie Saudi Arabia and UAE, are higher than those from LMICs, ie Iran and Pakistan, and low-income countries ie Sudan. This could be due to the availability of healthcare infrastructure and high-cost diagnostic and treatment options available in HICs.
Various limitations must be considered for this review. The heterogeneity of the data and vast variation, as well as missing details about the methodologies used by included studies makes it challenging to compare the results even in the same country. Most of the included studies in this review failed to meet the goal of COI research due to inadequate study methods and calculated only direct medical cost of diabetes. First and foremost, the research lacked a comprehensive list of unit costs. Second, the cost components and data sources were not adequately explained and were not even addressed as limitations of the study, raising concerns about the study’s quality. The absence of these elements has rendered these studies less accurate in terms of data collection and cost computation.13 As the majority of included studies were performed with patients’ perspectives along with these methodological differences, it was difficult to compare the economic burden of diabetes and GDP across different countries of EMR. Despite these limitations, systematic search with the recommended methodology used in the conduction of this review could be counted as its strength like other systematic reviews. Two independent reviewers performed each step of the current review independently to avoid potential bias.
Conclusion
This systematic review adds to the growing body of evidence on the economic burden of DM, which significantly affects the patient and healthcare system. The current systematic review corroborates the significant variations in costs across countries and highlights the importance of considering direct and indirect costs in economic evaluations. Moving forward, future research should adopt standardized methodologies for assessing the economic burden of DM, incorporate longitudinal designs, and prioritize including indirect costs to obtain a more comprehensive understanding of the global impact of this prevalent chronic disease. These insights are vital for informing policymakers, health-care providers, and stakeholders to develop cost-effective DM management strategies and improve patient outcomes.
Acknowledgment
The authors extended their appreciation to the Distinguished Scientist Fellowship program at King Saud University, Riyadh, Saudi Arabia, for supporting the conduction of this study.
Funding
This work was funded by the Distinguished Scientist Fellowship program at King Saud University, Riyadh, Saudi Arabia, through research support project number (RSP2024R131).
Disclosure
No potential conflict of interest was reported by the authors.
References
1. Ong KL, Stafford LK, McLaughlin SA, et al. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the global burden of disease study 2021. Lancet. 2023;2023:203–234.
2. World Health Organization. Global health estimates: life expectancy and leading causes of death and disability. Available from: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates.
3. World Health Organization. World Health Organization Global Report on Diabetes. Geneva: World Health Organization. 2016.
4. Sun H, Saeedi P, Karuranga S, et al. IDF diabetes atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022;183:109119. doi:10.1016/j.diabres.2021.109119
5. World Health Organization. WHO regional offices. Available from: https://www.who.int/about/who-we-are/regional-offices.
6. Jo C. Cost-of-illness studies: concepts, scopes, and methods. Clin Mol Hepatol. 2014;20(4):327. doi:10.3350/cmh.2014.20.4.327
7. Durand-Zaleski I. Why Cost-of-Illness Studies are Important and Inform Policy. London, England: Sage Publications Sage UK; 2008:251–253.
8. Ettaro L, Songer TJ, Zhang P, Engelgau MM. Cost-of-illness studies in diabetes mellitus. Pharmacoeconomics. 2004;22:149–164. doi:10.2165/00019053-200422030-00002
9. Pourmohammadi K, Shojaei P, Rahimi H, Bastani P. Evaluating the health system financing of the Eastern Mediterranean Region (EMR) countries using grey relation analysis and Shannon entropy. Cost Eff Resour Allocation. 2018;16:1–9. doi:10.1186/s12962-018-0151-6
10. Ansari-Moghaddam A, Setoodehzadeh F, Khammarnia M, Adineh HA. Economic cost of diabetes in the Eastern Mediterranean region countries: a meta-analysis. Diabetes Metab Syndr. 2020;14(5):1101–1108. doi:10.1016/j.dsx.2020.06.044
11. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int j Surg. 2021;88:105906. doi:10.1016/j.ijsu.2021.105906
12. Afroz A, Alramadan MJ, Hossain MN, et al. Cost-of-illness of type 2 diabetes mellitus in low and lower-middle income countries: a systematic review. BMC Health Serv Res. 2018;18(1):1–10. doi:10.1186/s12913-018-3772-8
13. Larg A, Moss JR. Cost-of-illness studies: a guide to critical evaluation. Pharmacoeconomics. 2011;29:653–671. doi:10.2165/11588380-000000000-00000
14. Akobundu E, Ju J, Blatt L, Mullins CD. Cost-of-illness studies: a review of current methods. Pharmacoeconomics. 2006;24:869–890. doi:10.2165/00019053-200624090-00005
15. U.S. Official Inflation Data AF. CPI inflation calculator. Available from: https://www.officialdata.org/.
16. Alhowaish AK. Economic costs of diabetes in Saudi Arabia. J Fam Comm Med. 2013;20(1):1. doi:10.4103/2230-8229.108174
17. Al-Maskari F, El-Sadig M, Nagelkerke N. Assessment of the direct medical costs of diabetes mellitus and its complications in the United Arab Emirates. BMC Public Health. 2010;10(1):1–10. doi:10.1186/1471-2458-10-679
18. Almutairi N, Alkharfy KM. Direct medical cost and glycemic control in type 2 diabetic Saudi patients. Appl Health Econ Health Pol. 2013;11:671–675. doi:10.1007/s40258-013-0065-6
19. Butt MD, Ong SC, Wahab MU, et al. Cost of illness analysis of type 2 diabetes mellitus: the findings from a lower-middle income country. Int J Environ Res Public Health. 2022;19(19):12611. doi:10.3390/ijerph191912611
20. Davari M, Boroumand Z, Amini M, Aslani A, Hosseini M. The direct medical costs of outpatient cares of type 2 diabetes in Iran: a retrospective study. Int J Preventive Med. 2016;7. doi:10.4103/2008-7802.181758
21. Elnil M, Swaraldahab Z, Abdelaziz SI. Direct financial cost of diabetes mellitus among adult Sudanese patients in Khartoum State 2016–2017. Asian J Med Health. 2019;14(2):1–8. doi:10.9734/ajmah/2019/v14i230097
22. Elrayah-Eliadarous H, Yassin K, Eltom M, Abdelrahman S, Wahlström R, Östenson C-G. Direct costs for care and glycaemic control in patients with type 2 diabetes in Sudan. Exp Clin Endocrinol Diabetes. 2010;220–225. doi:10.1055/s-0029-1246216
23. Elrayah‐Eliadarous HA, Östenson CG, Eltom M, Johansson P, Sparring V, Wahlström R. Economic and social impact of diabetes mellitus in a low‐income country: a case‐control study in S udan. J Diabet. 2017;9(12):1082–1090. doi:10.1111/1753-0407.12540
24. Gillani AH, Aziz MM, Masood I, et al. Direct and indirect cost of diabetes care among patients with type 2 diabetes in private clinics: a multicenter study in Punjab, Pakistan. Expert Rev Pharmac Outcomes Res. 2018;18(6):647–653. doi:10.1080/14737167.2018.1503953
25. Javanbakht M, Baradaran HR, Mashayekhi A, et al. Cost-of-illness analysis of type 2 diabetes mellitus in Iran. PLoS One. 2011;6(10):e26864. doi:10.1371/journal.pone.0026864
26. Ng CS, Lee JY, Toh MP, Ko Y. Cost-of-illness studies of diabetes mellitus: a systematic review. Diabetes Res Clin Pract. 2014;105(2):151–163. doi:10.1016/j.diabres.2014.03.020
27. Dagenais S, Caro J, Haldeman S. A systematic review of low back pain cost of illness studies in the United States and internationally. Spine J. 2008;8(1):8–20. doi:10.1016/j.spinee.2007.10.005
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.