")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
A Systematic Review of Chronic Diseases and Their Prevalence Among the Population of Northern Borders Province (NBP) in Saudi Arabia
Authors Alenzi EO, Fatima W, Amara A, Imran M, Shah SSH , Elbilgahy AA, Fawzy MS , Abu-Negm LM, Mujtaba MA, Jacinto-Caspillo I, Al-Hazimi AM
Received 10 December 2022
Accepted for publication 17 March 2023
Published 17 April 2023 Volume 2023:16 Pages 1047—1056
DOI https://doi.org/10.2147/JMDH.S401001
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Ebtihag O Alenzi,1– 3 Waseem Fatima,3,4 Abdelbasset Amara,3,5 Mohd Imran,3,6 Syed Sajid Hussain Shah,3,7 Amal Ahmed Elbilgahy,3,8,9 Manal S Fawzy,3,10,11 Lobna M Abu-Negm,3,12,13 Md Ali Mujtaba,3,14 Ingrid Jacinto-Caspillo,3,15 Awdah M Al-Hazimi3,16
1Department of Family and Community Medicine, Faculty of Medicine, Northern Border University, Arar, Saudi Arabia; 2Clinical Sciences Department, College of Medicine, Princess Nourah bint Abdul Rahman University, Riyadh, Saudi Arabia; 3Health & Medical Research Unit, Deanship of Scientific Research, Northern Border University, Arar, Saudi Arabia; 4Department of Clinical Nutrition, Faculty of Applied Medical Sciences, Northern Border University, Arar, Saudi Arabia; 5Department of Medical Laboratory Technology, Faculty of Applied Medical Sciences, Northern Border University, Arar, Saudi Arabia; 6Department of Pharmaceutical Chemistry, Faculty of Pharmacy, Northern Border University, Rafha, Saudi Arabia; 7Department of Pathology, Faculty of Medicine, Northern Border University, Arar, Saudi Arabia; 8Maternal and Child Health Nursing Department, Faculty of Nursing, Northern Border University, Arar, Saudi Arabia; 9Pediatric Nursing, Faculty of Nursing, Mansoura University, Mansoura, Egypt; 10Department of Biochemistry, Faculty of Medicine, Northern Border University, Arar, Saudi Arabia; 11Department of Medical Biochemistry and Molecular Biology, Faculty of Medicine, Suez Canal University, Ismailia, Egypt; 12Emergency Nursing Department, Faculty of Nursing, Northern Border University, Arar, Saudi Arabia; 13Medical Surgical Nursing Department, Faculty of Nursing, Ain Shams University, Cairo, Egypt; 14Department of Pharmaceutics, Faculty of Pharmacy, Northern Border University, Rafha, Saudi Arabia; 15Medical and Surgical Nursing Department, Faculty of Nursing, Northern Border University, Arar, Saudi Arabia; 16Faculty of Medicine, Northern Border University, Arar, Saudi Arabia
Correspondence: Manal S Fawzy; Awdah M Al-Hazimi, Tel +966 583241944 ; +966 505375690, Fax +966 146640705, Email [email protected]; [email protected]
Abstract: Estimation of the prevalence of chronic conditions is pivotal to effective healthcare planning and management. Therefore, our objective was to systemically review previous literature about the prevalence of chronic diseases among residents of Northern Borders Province (NBP) in Saudi Arabia. The electronic search has been done using scientific databases (PubMed, Ebsco, SciFinder, and Web of Science) and search engines up to September 2021. The following main key terms: chronic disease OR chronic conditions AND prevalence AND Northern Borders Province OR Northern Borders AND Saudi Arabia were applied. Other related terms with a more specific search were done with names of the main cities in the province and the most common diseases in Saudi Arabia. Duplicates were removed electronically by Endnote and manually. Extracted data were tabulated in the literature matrix. The risk of bias and quality of included studies were assessed using the “Strengthening the Reporting of Observational Studies in Epidemiology” (STROBE) checklist. Out of 63 observational studies that were assessed for eligibility, 21 observational studies were included to synthesize the evidence. These studies were conducted on Arar (n=16), Turaif (n=2), and Rafha (n=1), while the remaining were national studies in which NBP was one of the included regions (n=2). The most frequently studied diseases were diabetes (4 records), psychological diseases (4 records), and obesity (3 records). The most prevalent disease was gastroesophageal reflux disease (GERD), with an estimated prevalence of 61% among adults in Arar city. In conclusion, although some research is conducted about chronic diseases somewhere in NBP, further studies are needed to study chronic diseases using a representative sample of the whole NBP population.
Keywords: chronic diseases, medical healthcare, northern borders province, systematic review
Introduction
Chronic diseases are the leading causes of disability and mortality and the main drivers of medical healthcare costs.1–4 Estimation of the prevalence of these diseases and determining their risk factors in any region could facilitate the implementation of health strategies to reduce the burden of chronic conditions.5
According to a national survey in Saudi Arabia, the estimated prevalence rates of chronic conditions, such as diabetes mellitus (DM), were 14.8% for males and 11.7% for females.6 The estimated prevalence rates of hypertension (HTN) were 17.7% for males and 12.5% for females in 2013.6 Other population-based studies demonstrated that the prevalence rate of chronic obstructive pulmonary disease (COPD) was 2.4%, while the prevalence of end-stage renal disease (ESRD) was 0.05.7,8
At regional levels, some studies were conducted to estimate the prevalence of chronic diseases, such as obesity, DM, and comorbid mental illness, in Hail, Jazan, and Eastern Province.9–11 A cross-sectional study showed that the prevalence of obesity in Hail was 63.6%.9 Another regional study estimated the prevalence of DM to be 17.2% in the Eastern Province.11
Concerning “Northern Borders Province” (NBP) in Saudi Arabia, the population is estimated to be about 383,051 out of 34,218,169 of the whole Saudi Arabia population, and it encompasses the four main areas: Arar, Rafha, Turaif, and Al Owaiqelah (Figure 1), along with many villages and towns.12 According to the report of the Ministry of Health (MoH), the largest health sector in Saudi Arabia;13 the NBP health utilities include 41 public health centers (PHC), six “Dialysis Units”, 3 “Diabetes and Endocrinology” centers, 10 “Smoking Cessation Clinics”, 1 “Cardiology center”, 1 “Rehabilitation center”, 1 “Central/regional Laboratory”, 1 “Forensic Medicine center” and 1 “Control Health center at entry points”.14 Some key health indicators of this region, according to the recently available resources (2021) at the MoH, are (1) this region has a total of 11 MoH hospitals, including 1460 beds with a rate of 38.1 hospital beds/10,000 population, (2) the number of physicians is 1133 with a rate of 78 physicians/100 beds, (3) the number of nurses, including the midwives is 2536 with a rate of 174 nurses/100 beds and 224 nurses/100 physicians, (4) a total number of 73 isolation beds and 135 emergency room (ER) beds is available, (5) there are 14 first aid centers with average service rate about 381cases/center as well as 45 ambulances with average service rate 119 cases/ambulance, and (6) the number of private medical complexes is 40.14 However, there has been no comprehensive list of epidemiological studies which include all potential chronic conditions in the region although previously national surveys had taken place in the country to estimate the prevalence of some chronic conditions. Also, many chronic diseases have not been studied yet among a population of NPB, such as hypertension, dyslipidemia, hepatitis, and cancer. With dramatic changes in lifestyle and sedentary behaviors of people along with the fact that consanguinity and endogamy are common in this region,15,16 comprehensive studies of a list of all potential chronic conditions, including genetic-related diseases, should be conducted.
 |
Figure 1 The geographical location of the Northern Border Province (green area) in Saudi Arabia. It includes four main areas, as indicated in the figure. Data source (Google Maps: https://www.google.com/maps). |
Therefore, the objective of our study is to systematically review observational studies about chronic diseases conducted in any area of NBP. This could help to have a preliminary estimation of the burden of chronic conditions in this area. Also, we could figure out the gap in the literature regarding this issue to plan for future research and healthcare management programs.
Methods
This systematic review has been conducted according to PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.17 The research team in the Health and Medical Research Unit (HMRU) in the Deanship of Scientific Research at Northern Border University (NBU) has conducted this systematic review through four stages: identification, screening, checking, eligibility, and inclusion.
Initially, the search was done mainly to identify all potentially relevant articles that reported the prevalence of any chronic disease (communicable and non-communicable diseases) in the NBP. For the geographic setting of the NBP, which has a class 2 (ie upper middle class) of socioeconomic status,18 it is located in the far Northwest of the kingdom of Saudi Arabia (Figure 1). It is surrounded from the inside by four administrative regions of the Kingdom (Eastern, Al Jouf, Hael, and Al Qassim), and outside by Iraq and Jordan.19
Scientific databases (PubMed, Ebsco, SciFinder, and Web of Science (WOS)) and search engines (Google Scholar) were thoroughly searched up to September 2021. A combination of specific terms and keywords related to the study aim was used. The research team used these words: chronic disease OR chronic conditions AND prevalence AND Northern Borders AND Saudi Arabia. Names of NBP cities were specified in the further search. A more specific search of certain common diseases, such as diabetes mellitus, hypertension, chronic liver disease, chronic kidney diseases, chronic obstructive pulmonary disease, obesity, and dyslipidemia, has been done. Also, manual screening was carried out for the relevant articles from the reference list. After that, total duplicates were removed electronically by Endnote, and records were rechecked to remove duplicates manually.
Identified articles underwent screening of titles and abstracts to have all regional or national studies that included participants from NBP and estimated prevalence of any chronic disease.
The screened articles were assessed for eligibility by three independent reviewers (the second author, the third author, and the sixth author) based on the following criteria: (1) the included study published in the last 10 years (2011–2021); (2) it conducted among the population of NBP, such as Arar, Rafha, Turaif or Owaiqelah or either a national study that included people from NBU; (3) original observational study; (4) the study reported the prevalence of studied chronic disease. No inclusion and exclusion criteria were made based on the language.
Extracted data were tabulated in the literature review matrix. Many variables were identified from the extracted data. The main variables of interest were the studied chronic diseases and their reported prevalence. Other reported variables included the first author’s name, year, study design, sampling technique, and the sample’s related variables (age, gender, sample size, city, and setting).
All included studies were assessed using Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) criteria which is a checklist of 22 items that must be reported in observational studies.20
Results
A flowchart outlining the search results is illustrated in Figure 2. A total of 9346 potentially relevant studies were retrieved through different databases. A total of 210 duplicate studies were removed initially, and 5400 identified records were screened based on titles and abstracts. Following the screening of titles and abstracts, several studies were excluded for being irrelevant publications (n = 5337). Only 63 full-text records were retrieved to assess the eligibility. Out of which, 42 were removed based on eligibility criteria (34 records were conducted in Saudi Arabia but did not cover Northern Border Provinces, 6 records missed the information about the outcome of interest, and 2 were review articles). Twenty-one full-text articles were retrieved and met our inclusion criteria for review.
 |
Figure 2 Flow chart of study selection according to PRISMA guidelines. Notes: Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. 2009;339:b2535. Creative Commons.17 |
Risk of Bias and Quality Evaluation
The STROBE instrument was used to assess the quality and risk of bias across all 21 selected articles. It is a checklist of 22 parameters: title and abstract, background/rationale of the study, objectives, study design, setting, participants, variables, data sources/measurement, bias, study size, quantitative variables, statistical methods, participants, descriptive data, outcome data, main results, other analyses, key results, limitations, interpretation, generalizability, and funding. The score results of all 21 studies ranged from 95% to 64%, and three articles got a score between 90% and 95%, four articles got a score between 80% and 90%, eight articles got a score between 70% and 80%, and six articles get a score between 60% and 70%. In our systematic review, 100% of the included studies reported the following parameters: background/rationale of the study, objectives, study design, setting, participants, data sources/measurement, study size, descriptive data, outcome data, key results, and interpretation. In contrast, few studies (10%) had described addressing any potential sources of bias. A complete summary of the risk of bias results using STROBE analysis is presented in Figure 3.
 |
Figure 3 A summary risk of bias results using the STROBE checklist.18 Note: Adapted from von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE)statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344-9. Creative Commons.20 |
Characteristics of Included Studies
The characteristics of all included studies are summarized in Table 1. The present review included studies published from January 2011 to September 2021. All the included papers were published within or after 2011.21–41 Most of the selected studies had a cross-sectional study design (n=20), and only one study conducted by Alenezi et al had a retrospective design.41
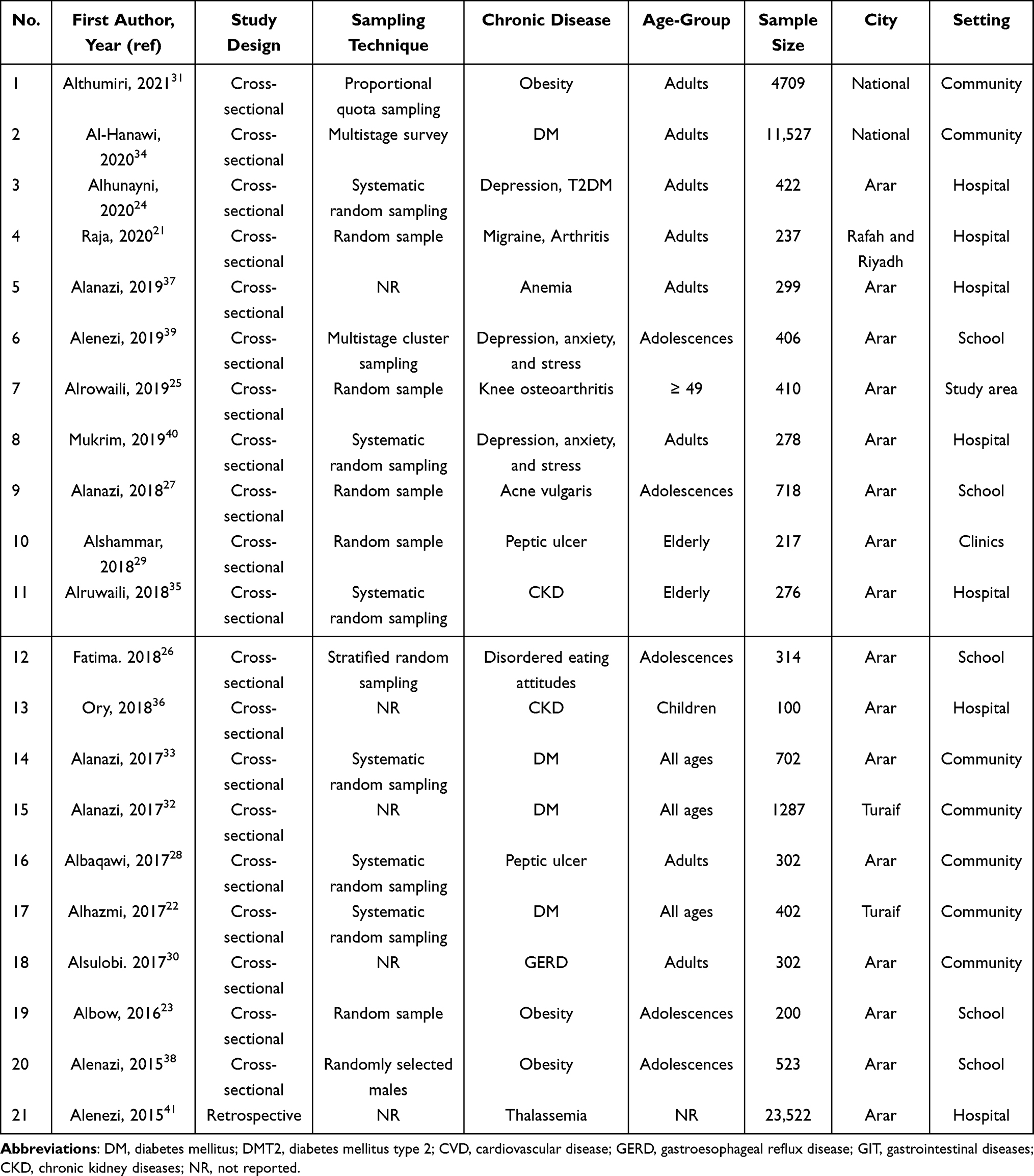 |
Table 1 Description of the Retrieved Studies Meeting the Inclusion Criteria of the Present Review |
Among these selected studies, 2 studies were national surveys,31,34 and 19 studies were regional studies conducted in some cities of NBP; 16 were from Arar,23–30,33,35–41 2 studies were from Turaif,22,32 and only 1 study from Rafha.21
Most of these studies (about 90%) rely on self-report chronic diseases gathered by interviews or questionnaires. Among included studies, seven studies were community-based,22,28,30–34 five studies were schools-based,23,26,27,38,39 and eight studies were hospital-based.21,24,29,35–37,40,41 The sample size of included studies ranged from 100 to 23,522.
The sample selection procedure and the variables are described sufficiently across all studies in Table 1.
Type of Studied Chronic Diseases
Table 2 demonstrates the general list of studied chronic diseases in the abstracted information and their prevalence. About 18 chronic diseases were found in the included studies, and these diseases were classified into seven categories: diabetes, obesity, psychological and mental, gastrointestinal (GIT), chronic kidney diseases (CKDs), musculoskeletal, and others. The highest crude prevalence among all reported diseases was the crude prevalence of gastroesophageal reflux (GERD) (61.8%) among adults in Arar city, and the lowest reported prevalence was the crude prevalence of kidney failures (1.4%) among the elderly in Arar. The most frequently studied chronic conditions were DM (4 records), mental disorders (4 records), obesity (3 records), GIT (3 records), musculoskeletal diseases (2 records), and CKDs (2 records). Based on participants’ gender, there were some studies conducted only among adolescent males38,39 which found that the prevalence rates of obesity, depression and anxiety were 30.%, 56.3%, and 56%, respectively. In contrast, there were some studies conducted only among adolescent females26,27 which showed that the prevalence of eating disorders and acne vulgaris were 25.5% and 34.8%, respectively.
 |
Table 2 A General List of Previously Studied Chronic Diseases and Their Prevalence in Northern Borders Province |
Discussion
The epidemiological data related to chronic diseases in any province or particular community promote the management of public health issues and facilitate improvements in health services in that community.42 Thus, members of HMRU in the Deanship of Scientific Research at NBU have systematically reviewed previously conducted observational studies about chronic disease in NBP of Saudi Arabia. The primary outcome of interest was the prevalence of the previously studied chronic diseases.
While it was evident from the retrieved data that DM has been the most studied chronic disease among the NBP population,22,32–34 it was not the highest estimated prevalence. The chronic disease with the highest prevalence was GERD (61.8%) among adults in Arar city, while it was 28.7% at the national rate.30,43 Although this was not a representative sample (the online questionnaire was conducted only in Arar city) of the whole NBP population, it showed that risk factors related to lifestyle and health behaviors, such as caffeine and nicotine consumption, psychological stress, fatty meals, and prolonged use of non-steroidal anti-inflammatory drugs (NSAID), were associated with the high prevalence of GERD.30
Concerning DM in NBP, its prevalence ranged from 4.5% among adults in Turaif to 11.6% among the total population of NBU, while it was about 8.5% at the national rate.15,27,44 The estimated prevalence of DM in other regions ranged from 6.7% in Tabuk to 17.8% in Hail.34 This prevalence could be attributed to modifiable risk factors, such as obesity, metabolic syndrome, lifestyle, and health behaviors.45,46 Non-modifiable factors, such as family history or genetic factors and age, could be associated with the prevalence of DM too.45,46 Thus, it is essential to launch educational campaigns which support public health and raise people’s awareness about modifiable risk factors of DM among the NBP population.
With regard to obesity, about 21% of the NBP population are obese, and this prevalence increased to 55% among adolescents in Arar.23,31 It is a significantly high percentage of DM among the general population of NBP, especially adolescents whose prevalence rate exceeded the national rate (24%).31 This indicates that those people are at high risk of other associated health issues and chronic diseases like diabetes and cardiovascular diseases.47 Other chronic diseases that have been studied among adolescents in NBP were eating disorders (25.5%), which was within the national range48 and acne vulgaris (14.3%) among females, depression (56.3%), and anxiety (56%) among males.23,26,27 For older people in Arar, it was estimated that peptic ulcer and renal insufficiency were prevalent in 21.2% and 6.5%, respectively.29,35 Two studies on the prevalence of inflammatory diseases (arthritis and knee-osteoarthritis) have been identified.21,25
All previously discussed results should be interpreted in light of the included studies’ limitations. First, most of the included studies were not representative of all populations of NBP. Only two included studies were representative of the whole population of NBP, which were national studies conducted among the Saudi population, including NBP.31,34 Based on these studies, it was demonstrated that 11.6% of the NBP population has diabetes and 21.1% are obese. Other results cannot be generalized to the whole population of NBP. Second, most of the included studies estimated the prevalence based on self-reported diseases not confirmed by diagnosis. Seven studies estimated the prevalence of chronic diseases based on the diagnosis of these diseases,25,27,29,32,37,38,41 while others were based on self-reported data, which could be prone to bias, underestimation, or overestimating.49,50 Finally, there was significant heterogeneity across all included studies in many of their observed characteristics. Some of these heterogenic characteristics include the targeted population, sampling technique, sample size, setting, and participants’ demographic.
To the best of our knowledge, this is the first study that sheds light on the chronic disease burden in a population of NBP. The retrieved data will provide insight to decision-makers in the health system about the burden of existing and foreseeable health problems.
Accordingly, further studies should be carried out on a larger sample that is representative of the whole population of NBP. As was discussed above, the prevalence rates of common chronic conditions, such as diabetes, obesity, and GERD in NBP, were different as compared with national averages. Therefore, there is an urgent need for a new population-wide study to estimate the prevalence of all potential chronic diseases among people in the NBP of Saudi Arabia.
In conclusion, our review shows that the most frequently studied diseases were diabetes, obesity, and psychological diseases, and the most prevalent disease among adults in Arar was gastroesophageal reflux disease. Educational campaigns and programs should be provided to the at-risk population to promote healthy behaviors and avoid modifiable risk factors of chronic diseases. Future research should be conducted among a representative sample of Northern Border Province, studying all chronic diseases, especially diseases that have not been previously studied in the area.
Acknowledgments
We would like to thank all the authors of the original articles enrolled in this study. Also, the authors extend their appreciation to the Deanship of Scientific Research at Northern Border University, Arar, KSA, for funding this research work through the project number “NBU-FFR-2023-0011.”
Author Contributions
All authors made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval for the version to be published; and agreed to be accountable for all aspects of the work.
Disclosure
The authors declare that there are no conflicts of interest in this work.
References
1. Centers for Disease, C.; Prevention. Chronic Diseases and Their Risk Factors: The Nation’s Leading Causes of Death. US Department of Health and Human Services, Centers for Disease Control and Prevention; 1999.
2. Joshi R, Cardona M, Iyengar S, et al. Chronic diseases now a leading cause of death in rural India—mortality data from the Andhra Pradesh rural health initiative. Int J Epidemiol. 2006;35(6):1522–1529.
3. Centers for Disease, C.; Prevention. The Burden of Chronic Diseases and Their Risk Factors: National and State Perspectives. Department of Health and Human Services, Centers for Disease Control and Prevention; 2002.
4. Hajat C, Stein E. The global burden of multiple chronic conditions: a narrative review. Prev Med Rep. 2018;12:284–293. doi:10.1016/j.pmedr.2018.10.008
5. Hajat C, Siegal Y, Adler-Waxman A. Clustering and healthcare costs with multiple chronic conditions in a US study. Front Public Health. 2020;8:607528. doi:10.3389/fpubh.2020.607528
6. Mokdad A Saudi health interview survey finds high rates of chronic diseases in the Kingdom of Saudi Arabia. Institute for Health Metrics and Evaluation (IHME); 2014. Available from: http://www.healthdata.org/news-release/saudi-health-interview-survey-finds-high-rates-chronic-diseases-kingdom-saudi-arabia.
7. Wali SO, Idrees MM, Alamoudi OS, et al. Prevalence of chronic obstructive pulmonary disease in Saudi Arabia. Saudi Med J. 2014;35(7):684–690.
8. Al-Sayyari AA, Shaheen FA. End stage chronic kidney disease in Saudi Arabia. Saudi Med J. 2011;32(4):339–346.
9. Ahmed HG, Ginawi IA, Elasbali AM, Ashankyty IM, Al-hazimi AM. Prevalence of obesity in Hail region, KSA: in a comprehensive survey. J Obes. 2014;2014:961861. doi:10.1155/2014/961861
10. Madkhali JM, Hakami AA, Dallak AH, et al. Prevalence and associated factors of depression among patients with diabetes at Jazan Province, Saudi Arabia: a cross-sectional study. Psychiatry J. 2019;2019:6160927. doi:10.1155/2019/6160927
11. Al-Baghli NA, Al-Ghamdi AJ, Al-Turki KA, Al Elq AH, El-Zubaier AG, Bahnassy A. Prevalence of diabetes mellitus and impaired fasting glucose levels in the Eastern Province of Saudi Arabia: results of a screening campaign. Singapore Med J. 2010;51(12):923.
12. Population Estimates: population Estimates in the Midyear of 2021; 2021. Available from: https://www.stats.gov.sa/en/43.
13. Zaher S, Ajabnoor SM, Cross Sectional A. Survey-based study to investigate the availability and utilisation of home nutrition support in Saudi Arabia. J Multidiscip Healthc. 2023;16:41–50. doi:10.2147/JMDH.S398569
14. Year book S. Statistical-Year book; 2021. Available from: https://www.moh.gov.sa/en/Ministry/Statistics/book/Documents/Statistical-Yearbook-2021.pdf.
15. Alenizi DA. Consanguinity pattern and heritability of Vitiligo in Arar, Saudi Arabia. J Family Community Med. 2014;21(1):13–16. doi:10.4103/2230-8229.128767
16. Ahmad Bahathig A, Abu Saad H, Md Yusop NB, Mohd Shukri NH, El-Din MME. Relationship between physical activity, sedentary behavior, and anthropometric measurements among Saudi female adolescents: a cross-sectional study. Int J Environ Res Public Health. 2021;18:1.
17. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535. doi:10.1136/bmj.b2535
18. AlOmar RS, Parslow RC, Law GR. Development of two socioeconomic indices for Saudi Arabia. BMC Public Health. 2018;18(1):791. doi:10.1186/s12889-018-5723-z
19. Arar City Profile. United Nations Human Settlements Programme (UN-Habitat). Available from: https://unhabitat.org/sites/default/files/2020/04/arar_0.pdf.
20. von Elm E, Altman DG, Egger M, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344–9. doi:10.1016/s0140-6736(07)61602-x
21. Raja MAG, Al-Shammari SS, Al-Otaibi N, Amjad MW. Public attitude and perception about analgesic and their side effects. J Pharm Res Int. 2020;2020:35–52.
22. Alhazmi RS, Ahmed AAB, Alshalan MH, et al. Prevalence of diabetes mellitus and its relation with obesity in Turaif (Saudi Arabia) in 2017. Electron Physician. 2017;9(10):5531.
23. Albow B, Alenezy A. Risk factors of type 2 diabetes and cardiovascular diseases among Saudi Arabian adolescents. Pak J Nutr. 2016;15(9):883–888.
24. Alhunayni NM, Mohamed AE, Hammad SM. Prevalence of depression among type-II diabetic patients attending the diabetic clinic at arar national guard primary health care center, Saudi Arabia. Psychiatry J. 2020;2020:1.
25. Alrowaili MG. Magnetic resonance evaluation of knee osteoarthritis among the Saudi Population. Pak J Med Sci. 2019;35(6):1575.
26. Fatima W, Ahmad LM. Prevalence of disordered eating attitudes among adolescent girls in Arar City, Kingdom of Saudi Arabia. J Health Psychol. 2018;6:1.
27. Alanazi MS, Hammad SM, Mohamed AE. Prevalence and psychological impact of Acne vulgaris among female secondary school students in Arar city, Saudi Arabia, in 2018. Electron Physician. 2018;10(8):7224.
28. Albaqawi ASB, El-Fetoh NMA, Alanazi RFA, et al. Profile of peptic ulcer disease and its risk factors in Arar, Northern Saudi Arabia. Electron Physician. 2017;9(11):5740.
29. Alshammari MJH, Ali OMB, Al-shamlani SK, et al. Peptic ulcer disease in elderly population of Arar City, Northern Saudi Arabia. Egypt J Hosp Med. 2018;73(4):6494–6501.
30. Alsulobi AM, El-Fetoh NMA, Alenezi SGE, et al. Gastroesophageal reflux disease among population of Arar City, Northern Saudi Arabia. Electron Physician. 2017;9(10):5499.
31. Althumiri NA, Basyouni MH, BinDhim NF, Alqahtani SA. Levels and associations of weight misperception with healthy lifestyle among adults in Saudi Arabia. Obes Facts. 2021;2021:1–7.
32. Alanazi NH, Alsharif MM, Rasool G, et al. Prevalence of diabetes and its relation with age and sex in Turaif city, northern Saudi Arabia in 2016–2017. Electron Physician. 2017;9(9):5294–5297. doi:10.19082/5294
33. Alanazi AM, Abo El-Fetoh NM, Alotaibi HK, et al. Survey of awareness of diabetes mellitus among the Arar population, Northern Border Region of Saudi Arabia. Electron Physician. 2017;9(9):5369–5374. doi:10.19082/5369
34. Al‐Hanawi MK, Chirwa GC, Pulok MH. Socioeconomic inequalities in diabetes prevalence in the Kingdom of Saudi Arabia. Int J Health Plann Manage. 2020;35(1):233–246.
35. Alruwaili ASM, Alrowili ASM, Alshammari MNO, et al. Prevalence and some of determinant factors of chronic kidney diseases among Saudi elderly in Arar, KSA. Egypt J Hosp Med. 2018;73(4):6522–6530.
36. Ory ZMI, Aboel-Fetoh NM, Mohammed NA, Hamoud A, Alruwaili AHA, Alenezi AM. Chronic kidney disease in children in arar, kingdom of Saudi Arabia. Int J Adv Res. 2016;4(8):1313–1321.
37. Alanazi WSG, Alshaibani FS, Alanazi AMR, et al. Anemia in pregnant women in Arar, Northern Saudi Arabia. Indo Am J Pharm Sci. 2019;6(1):1145–1151.
38. Alenazi SA, Koura HM, Zaki SM, Mohamed AH. Prevalence of obesity among male adolescents in Arar Saudi Arabia: future risk of cardiovascular disease. Indian J Community Med. 2015;40(3):182.
39. Alenazi SF, Hammad SM, Mohamed AE. Prevalence of depression, anxiety and stress among male secondary school students in Arar city, Saudi Arabia, during the school year 2018. Electron Physician. 2019;11:2.
40. Mukrim ME, Alshammari NMD, Alshammari WMD, et al. Prevalence of depression, anxiety, and stress among diabetes mellitus patients in Arar, Northern Saudi Arabia. Age. 2019;62:22–23.
41. Alenazi SA, Ali HW, Alharbi MG, Alenizi AF, Wazir F. Prevalence of thalassemia and sickle cell disease in northern border region of Saudi Arabia. Kashmir J Med Sci. 2015;1(1):3–6.
42. Bustami M, Matalka KZ, Mallah E, et al. The prevalence of overweight and obesity among women in Jordan: a risk factor for developing chronic diseases. J Multidiscip Healthc. 2021;14:1533–1541. doi:10.2147/JMDH.S313172
43. Alsuwat OB, Alzahrani AA, Alzhrani MA, Alkhathami AM, Mahfouz MEM. Prevalence of gastroesophageal reflux disease in Saudi Arabia. J Clin Med Res. 2018;10(3):221–225. doi:10.14740/jocmr3292w
44. Alqahtani B, Elnaggar RK, Alshehri MM, Khunti K, Alenazi A. National and regional prevalence rates of diabetes in Saudi Arabia: analysis of national survey data. Int J Diabetes Dev Ctries. 2022;2022:1. doi:10.1007/s13410-022-01092-1
45. Alanazi FK, Alotaibi JS, Paliadelis P, Alqarawi N, Alsharari A, Albagawi B. Knowledge and awareness of diabetes mellitus and its risk factors in Saudi Arabia. Saudi Med J. 2018;39(10):981–989. doi:10.15537/smj.2018.10.22938
46. Fawzy MS, Alshammari MA, Alruwaili AA, et al. Factors associated with diabetic foot among type 2 diabetes in Northern area of Saudi Arabia: a descriptive study. BMC Res Notes. 2019;12(1):51. doi:10.1186/s13104-019-4088-4
47. Ss MA. A review of prevalence of obesity in Saudi Arabia. J Obes Eat Disord. 2016;2(2):1–6.
48. Melisse B, de Beurs E, van Furth EF. Eating disorders in the Arab world: a literature review. J Eat Disord. 2020;8(1):59. doi:10.1186/s40337-020-00336-x
49. Maukonen M, Männistö S, Tolonen H. A comparison of measured versus self-reported anthropometrics for assessing obesity in adults: a literature review. Scand J Public Health. 2018;46(5):565–579. doi:10.1177/1403494818761971
50. Spitzer S, Weber D. Reporting biases in self-assessed physical and cognitive health status of older Europeans. PLoS One. 2019;14(10):e0223526. doi:10.1371/journal.pone.0223526
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.