Back to Journals » Medical Devices: Evidence and Research » Volume 19
A Systematic Review and Meta-Analysis of Diagnostic Test Accuracy for Human Toxoplasmosis: Performance, Populations, and Validation Gaps
Authors Suprianto D ![]() , Fitri LE
, Fitri LE ![]() , Sabarudin A, Mahmudy WF
, Sabarudin A, Mahmudy WF ![]() , Prabowo MH, Surareungchai W
, Prabowo MH, Surareungchai W
Received 22 September 2025
Accepted for publication 30 January 2026
Published 3 March 2026 Volume 2026:19 569457
DOI https://doi.org/10.2147/MDER.S569457
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mohamad Bashir
Dodit Suprianto,1,2 Loeki Enggar Fitri,3,4 Akhmad Sabarudin,5 Wayan Firdaus Mahmudy,6 Muhammad Hatta Prabowo,7 Werasak Surareungchai8
1Doctoral Program in Medical Science, Faculty of Medicine, Universitas Brawijaya, Malang, Indonesia; 2Department of Electrical Engineering, Politeknik Negeri Malang, Malang, Indonesia; 3Department of Clinical Parasitology, Faculty of Medicine, Universitas Brawijaya, Malang, Indonesia; 4AIDS, Toxoplasma, Opportunistic Disease and Malaria (ATOM) Research Group, Faculty of Medicine, Universitas Brawijaya, Malang, Indonesia; 5Department of Chemistry, Faculty of Science, Universitas Brawijaya, Malang, Indonesia; 6Department of Informatics Engineering, Faculty of Computer Science, Universitas Brawijaya, Malang, Indonesia; 7Department of Pharmacy, Faculty of Mathematics and Natural Sciences, Universitas Islam Indonesia, Yogyakarta, Indonesia; 8School of Bioresources and Technology, King Mongkut’s University of Technology Thonburi, Bangkok, Thailand
Correspondence: Loeki Enggar Fitri, Email [email protected]
Background: Accurate and timely diagnosis of toxoplasmosis is crucial for clinical management, particularly in high-risk populations. Despite a diverse diagnostic landscape spanning laboratory-based serology, molecular assays, point-of-care (POC) devices, and emerging technologies, a consolidated quantitative synthesis of their performance and clinical readiness is lacking.
Methods: This systematic review and diagnostic test accuracy meta-analysis employed a dual-method design, integrating evidence mapping and quantitative synthesis. We searched Embase, PubMed, Scopus, IEEE Xplore, and other databases from January 1, 2010, to December 31, 2025, for studies evaluating diagnostic tests for human toxoplasmosis. Evidence mapping classified technologies by target, specimen, and validation stage (Tiers 0– 3). Meta-analysis pooled sensitivity and specificity using bivariate random-effects models for subgroups with sufficient data. Risk of bias was assessed using QUADAS-2.
Results: Evidence mapping identified 175 studies yielding 309 diagnostic test evaluations across 37 target groups, 20 clinical populations, and 11 technological categories. Most studies evaluated conventional laboratory assays (75.9%), followed by point-of-care tests (20.9%) and emerging technologies (3.2%). Meta-analysis included 182 test evaluations (42,287 samples) and showed that accuracy differed by detection target, population, and platform. Among targets, IgG+IgM and IgG avidity demonstrated the strongest combined performance (IgG+IgM sensitivity 94.8% [95% CI 89.4– 97.5], specificity 96.7% [93.9– 98.3]; IgG avidity sensitivity 90.8% [84.9– 94.5], specificity 97.1% [91.7– 99.0]), whereas DNA assays showed a rule-in profile with lower sensitivity (66.0% [51.9– 77.7]) but high specificity (96.2% [94.3– 97.5]). Performance varied across clinical populations, with a notable diagnostic gap in other immunocompromised patients (sensitivity 55.7% [33.1– 76.2] despite specificity 97.7% [92.3– 99.3]). By platform, POCTs had high specificity (97.4% [95.4– 98.5]) and good sensitivity (87.7% [80.3– 92.6]) compared with conventional assays (84.7% [80.2– 88.3]; 95.5% [94.2– 96.6]).
Conclusion: Diagnostic accuracy for toxoplasmosis is highly context-dependent. Serology remains central, with IgG avidity (and high-performing IgG+IgM strategies) supporting infection dating, and POCTs offering rapid, high-specificity rule-in utility when embedded in appropriate clinical algorithms. The persistently reduced sensitivity in immunocompromised populations highlights an urgent unmet need for improved diagnostics and more rigorous, standardized real-world validation.
Keywords: toxoplasmosis, diagnostic accuracy, meta-analysis, point-of-care testing, IgG avidity, evidence mapping
Introduction
Toxoplasmosis, caused by the protozoan parasite Toxoplasma gondii (T. gondii), remains a globally important infectious disease due to its high prevalence and its potentially severe outcomes in high-risk populations, including pregnant women, fetuses/newborns, and immunocompromised individuals.1 In these groups, delayed recognition and treatment can lead to substantial clinical burden, including congenital disease and long-term neurological and ocular complications such as ocular toxoplasmosis (OT), a leading cause of infectious posterior uveitis.2 For this reason, diagnostics are central to clinical decision-making, prevention of vertical transmission, and effective patient management.
Despite long-standing availability of laboratory-based tests, diagnosing toxoplasmosis continues to present practical and methodological challenges. Serology and molecular techniques can provide robust evidence of exposure or active infection; however, they are influenced by various factors including the timing of infection, interpretation of antibody profiles, specimen type, and access to laboratory infrastructure. In ocular toxoplasmosis, for instance, diagnosis in atypical cases is complicated by phenotypic overlap with other retinochoroiditides and often depends on subjective expert interpretation of multimodal imaging, highlighting the limitations of serology alone in complex clinical presentations.3 In many contexts, testing is limited by cost, turnaround time, availability of trained personnel, and the need for specialized equipment, which can restrict timely diagnosis and delay interventions where rapid decision-making is critical.4
In parallel with established laboratory workflows, the diagnostic landscape has expanded to include a broad spectrum of platforms and device-enabled approaches, ranging from rapid immunoassays and portable molecular systems to biosensors, microfluidic devices, and reader-assisted formats. These approaches are increasingly reported across biomedical and engineering literature, resulting in a broad yet fragmented evidence base. Moreover, diagnostic performance claims are not always comparable across studies because evaluations vary in validation maturity, reference standards, specimen matrices, and whether testing is performed in clinical populations or under analytical/contrived conditions.
A key challenge for clinicians, researchers, and implementers is therefore not merely the abundance of technologies but also the lack of consolidated mapping of what has been evaluated, in which settings, using which specimens and targets, and with what level of clinical validity. Without an integrated view, it becomes challenging to judge readiness for clinical adoption, to compare diagnostic classes fairly, and to identify translational gaps where promising approaches remain limited by study design, bias risks, or insufficient field-relevant validation.
Accordingly, this study maps the evidence on toxoplasmosis diagnostics published between 2010 and 2025 across laboratory-based and device-enabled approaches. We classify diagnostic platforms by detection target, specimen matrix, and validation characteristics; summarize reported diagnostic performance using structured evidence mapping and diagnostic accuracy meta-analysis where feasible; and identify evidence gaps that inform future evaluation and implementation. Point-of-care technologies are regarded as an important subset of the overall diagnostic landscape, with their deployment implications emphasized primarily in the Discussion.
Materials and Methods
Study Design and Registration
This study was a systematic review and meta-analysis of diagnostic test accuracy (DTA) for human toxoplasmosis, with the primary aim of synthesizing and comparing the accuracy of available tests. The secondary aims were to analyze performance across key clinical populations and to map the validation maturity of the evidence base, thereby identifying critical gaps. The review was conducted according to the PRISMA-DTA 2020 statement.5 An internal protocol guided the process, informed by Cochrane and PRISMA-DTA guidelines; the protocol was not prospectively registered.
Information Sources and Search Strategies
A systematic search was performed across biomedical, engineering, and multidisciplinary databases to capture the full spectrum of diagnostic literature, from clinical evaluations to device-development reports. Databases included PubMed, Embase, Scopus, Web of Science Core Collection, ScienceDirect, IEEE Xplore, Engineering Village (Compendex/Inspec), ClinicalTrials.gov, and ProQuest Dissertations & Theses Global.
The search strategy combined core concepts of Toxoplasma gondii / toxoplasmosis with terms for diagnostic testing, point-of-care, and device-based detection. Controlled vocabularies (MeSH, Emtree) were used where available, supplemented by extensive free-text synonyms tailored to each database’s focus (eg, engineering terminology for IEEE Xplore). Searches were limited to January 1, 2010–December 31, 2025, with no initial language restrictions. One study accepted in 2025 but published online in early 2026 was included after manual screening. The complete search strings are provided in Supplementary Table S1.
Eligibility Criteria
Studies were eligible if they: (1) were original research evaluating a diagnostic test, device, or platform for T. gondii; (2) used human specimens or relevant matrices; (3) targeted antibodies (IgG, IgM, avidity), nucleic acids (DNA), antigens, or image-based patterns; (4) reported primary quantitative performance data (eg, 2×2 table, sensitivity/specificity, AUC, LOD); and (5) were published in English. For inclusion in meta-analysis, an acceptable reference standard and complete 2×2 data were required.
Exclusion criteria included: veterinary-only studies, reviews/editorials/case reports without primary data, studies focused on treatment/epidemiology/pathogenesis, insufficient methodological or quantitative data, and publications outside the date/language range.
Study Selection and Data Extraction
Study selection followed the PRISMA 2020 flow diagram (Figure 1). Two reviewers (D.S. and A.S.) independently screened titles/abstracts and full texts against eligibility criteria. Disagreements were resolved by consensus or a third reviewer (L.E.F).
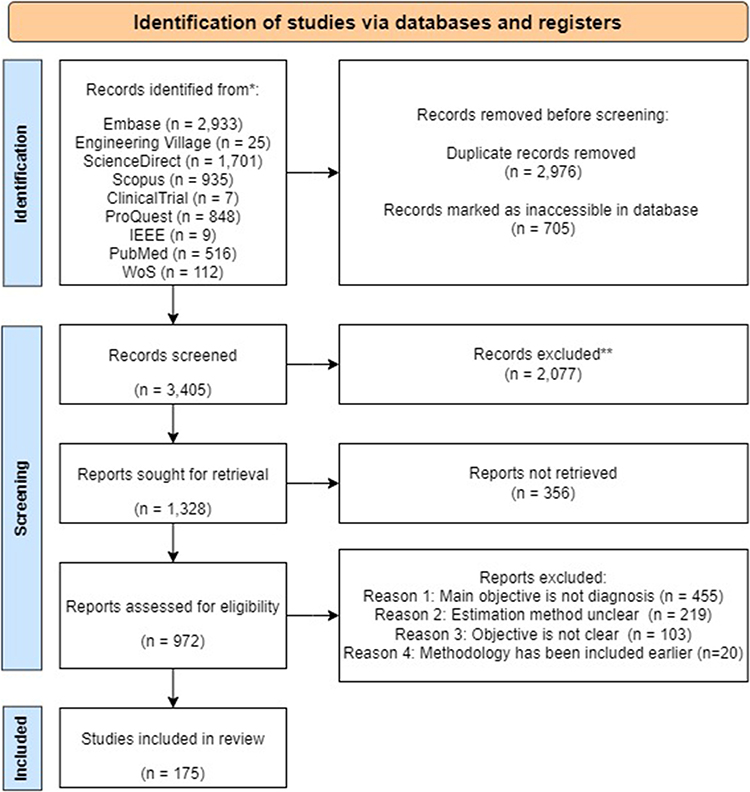 |
Figure 1 PRISMA flow diagram summarizing the study selection process. Of 7,086 records identified, 972 full-text articles were assessed; 797 reports were excluded (mainly not diagnostic evaluation, unclear estimation method, or unclear primary objective). A total of 175 studies were included in the systematic review, contributing 309 unique diagnostic test evaluations for evidence mapping, of which 182 evaluations with complete 2×2 data were included in the quantitative meta-analysis. |
Data were extracted in duplicates using a piloted, standardized form in Microsoft Excel. Extracted items included:
- Bibliographic/Contextual: Author, year, country, study design, clinical population, sample type, sample size.
- Index Test: Technology category (conventional/POCT/emerging), platform, detection target, specimen matrix, time-to-result.
- Reference Standard: Method used for comparison.
- Performance Data: TP, FP, FN, TN counts, sensitivity, specificity, limit of detection (LOD).
- Other: Funding and conflicts of interest.
For this classification, conventional tests were defined as established laboratory-based methods requiring centralized infrastructure and specialized personnel. Point-of-care (POCT) referred to rapid assays designed for use near the patient, while emerging technologies encompassed novel approaches such as biosensors and machine learning-based tools still in early validation stages.
Unit of Analysis and Data Handling
The study (publication) was the primary unit for descriptive analyses and characterization (n=175). Within studies, individual test evaluations (unique index test/cohort combinations) were the unit for accuracy assessment and validation staging. A single study could contribute multiple test evaluations (eg, evaluating both IgG and IgM). From the 175 included studies, 309 test evaluations were extracted.
For the diagnostic test accuracy (DTA) meta-analysis, we included only test evaluations with a complete 2×2 contingency table (true positives, false positives, false negatives, true negatives) derived from an appropriate reference standard. This resulted in 182 test evaluations eligible for quantitative synthesis. This dataset of 182 evaluations forms the basis for all subsequent pooled analyses and subgroup comparisons (by detection target, clinical population, and technology platform), unless otherwise specified (see Subgroup, Heterogeneity, and Sensitivity Analyses for details on the technology subgroup).
Validation Stage Classification (Tiered Framework)
To distinguish analytical feasibility from clinical readiness and to identify validation gaps, each test evaluation was classified into a validation tier:
- Tier 0 (Analytical): Contrived/spiked samples, benchtop feasibility without patient specimens.
- Tier 1 (Clinical-Lab): Human specimens tested under controlled laboratory conditions.
- Tier 2 (Near-Patient Pilot): Limited-site evaluations in workflows approximating intended use.
- Tier 3 (Field Validation): Multi-site deployment under real-world operational conditions.
Classification was based on specimen provenance and workflow description; the minimum defensible tier was assigned if details were unclear.
Risk of Bias Assessment
The methodological quality of studies providing accuracy data was assessed using QUADAS-2 across four domains: Patient Selection, Index Test, Reference Standard, and Flow & Timing. Two reviewers performed assessments independently, with disagreements resolved by consensus. Judgments (Low/High/Unclear risk) were based on pre-defined signaling questions regarding sampling, blinding, threshold pre-specification, the appropriateness of reference standard, timing, and participant flow.
Data Synthesis and Analysis
The synthesis was designed to address the three core aspects of the review: Diagnostic Performance, Population-Specific Analysis, and Evidence/Validation Mapping.
Descriptive Analysis and Evidence Mapping
Descriptive statistics summarized the landscape of evidence, including temporal/geographic trends, technology platforms, detection targets, sample types, operational metrics (time-to-result), and validation maturity (Tier distribution). Where available, reported analytical performance metrics—in particular the limit of detection (LOD)—were also extracted and mapped to characterize the methodological rigor and comparability of test evaluations. This mapping provides context for the quantitative synthesis and highlights key translational and standardization gaps in the evidence base.
Diagnostic Test Accuracy Meta-Analysis (Performance)
The primary quantitative synthesis estimated pooled sensitivity and specificity (with 95% CI) using a bivariate random-effects model (or HSROC model for threshold effects). Between-study heterogeneity was assessed using the bivariate random-effects variance components (τ²) and the estimated correlation (ρ), alongside visual inspection of study dispersion in ROC space and study-level forest plots.
Subgroup, Heterogeneity, and Sensitivity Analyses
To investigate heterogeneity and address the review’s secondary aims regarding population-specific performance, pre-planned analyses were conducted through subgroup meta-analyses, assessment of heterogeneity, sensitivity analyses, and investigation of reporting bias.
Separate bivariate random-effects models were fitted for clinically meaningful subgroups defined by:
- Detection Target (IgG, IgM, IgG Avidity, DNA)
- Clinical Population (pregnant women, immunocompromised patients)
- Technology Platform (conventional laboratory vs point-of-care)
For the technology platform comparison, the analysis focused on conventional versus point-of-care tests. Although the initial evidence mapping classified technologies into three broad categories—Conventional, Point-of-Care (POCT), and Emerging (machine learning, biosensors)—the “Emerging” category was pre-specified for exclusion from pooled subgroup analysis if fewer than 10 evaluations were available. This decision was based on the need for stable estimation and the profound methodological heterogeneity expected within this category.
Heterogeneity within each synthesis was assessed using the bivariate random-effects variance components for sensitivity and specificity (τ2_sens and τ2_spec) and their estimated correlation (ρ), alongside visual inspection of dispersion in ROC space and study-level forest plots. Between-subgroup differences were described by comparing pooled estimates and the extent of confidence interval overlap across stratified analyses.
To evaluate the robustness of key findings, sensitivity analyses were planned, including restriction to larger studies (sample size ≥ 50) for the most frequently evaluated target. For meta-analyses containing at least 10 studies, funnel plots were visually inspected to assess potential small-study effects or publication bias.
Software
Data management and evidence mapping used Microsoft Excel (Office 365). Statistical analyses and meta-analyses were conducted in R (v4.5.2) using the “mada” and “metafor” packages. All data and code are archived for reproducibility.
Result
Study Selection
The study selection process is summarized in the PRISMA flow diagram (Figure 1). From 7,086 initial records, 972 full-text articles were assessed. After eligibility screening, 797 reports were excluded, primarily because their main objective was not diagnostic evaluation (n=455), they had an unclear estimation method (n=219), or an unclear primary objective (n=103). A total of 175 studies met all inclusion criteria and were included in the systematic review.6–180 These 175 studies contributed 309 unique diagnostic test evaluations (ie, distinct index test/cohort combinations) for evidence mapping. Of these, 182 test evaluations provided complete dichotomous (2x2) data and were included in the quantitative meta-analysis. Further details are available in Supplementary Table S2 for full dataset characteristics.
Characteristics of Included Studies and Test Evaluations
Bibliometric and Temporal Trends
The 175 included studies were published between 2010 and 2025 (with one study accepted in 2025 published online in 2026).180 Publication output showed progressive growth, increasing from 7 studies in 20106–12 to a peak of 20 studies in 2021,115–134 indicating sustained and increasing research interest (Figure 2A).
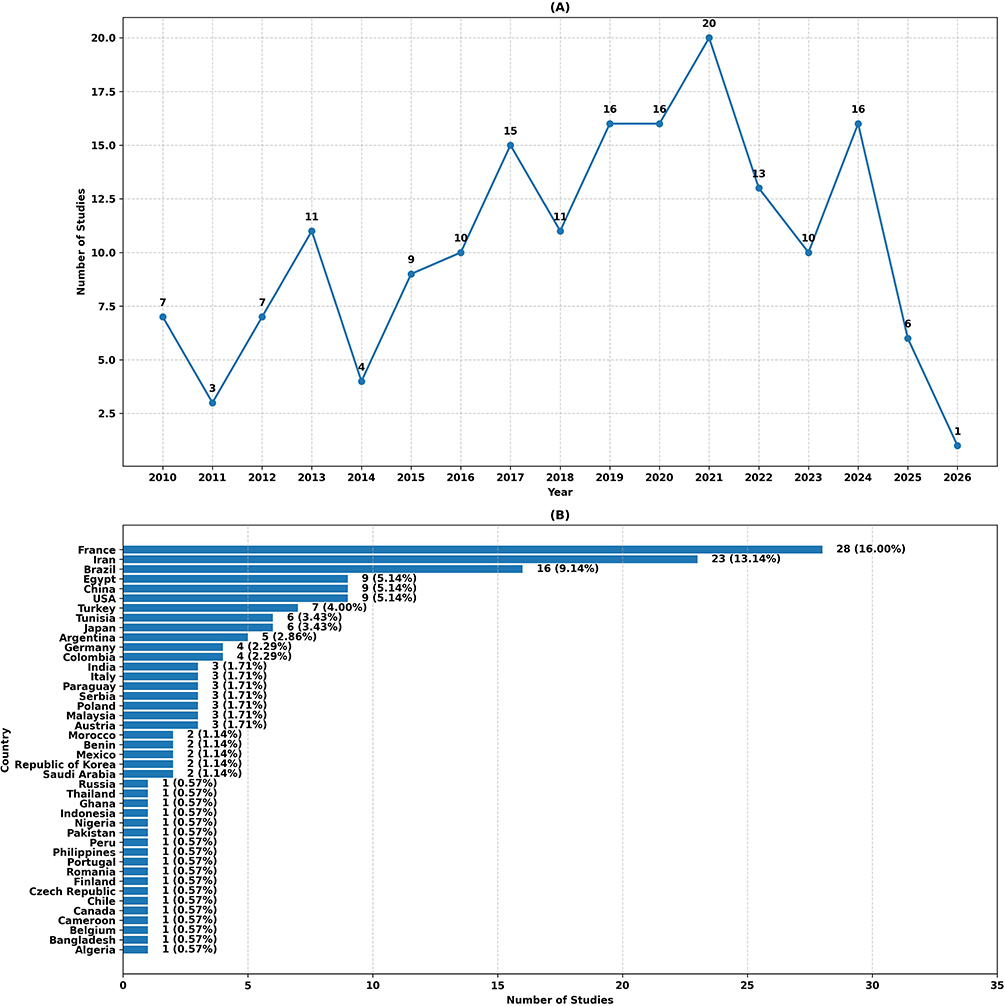 |
Figure 2 Temporal Trends and Geographic Distribution of Toxoplasmosis Diagnostic Studies (2010–2025). (A) Annual publication trend showing increasing research output, with peak activity in 2021. (B) Country Contribution to Publications, top 6 contributing countries: France (n=28), Iran (n=23), Brazil (n=16), Egypt (n=9), China (n=9) and USA (n=9). |
Research contributions were globally distributed across 42 countries. The top contributing countries were France (n=28 studies, 16.0%),22,30,31,33,37,40,45,57,61,68,76,82,83,86,88,100,102,107,110,111,116,125,135,137,138,141,142,162 Iran (n=23, 13.1%),12,18,20,47,53,62,63,66,81,87,91,92,94,108,112,119–121,124,127,136,143,154 Brazil (n=16, 9.1%),10,21,39,43,49,50,58,64,65,70,89,101,103,129,172 and the USA, Egypt, and China (each with n=9, 5.1%) (Table 1 and Figure 2B).
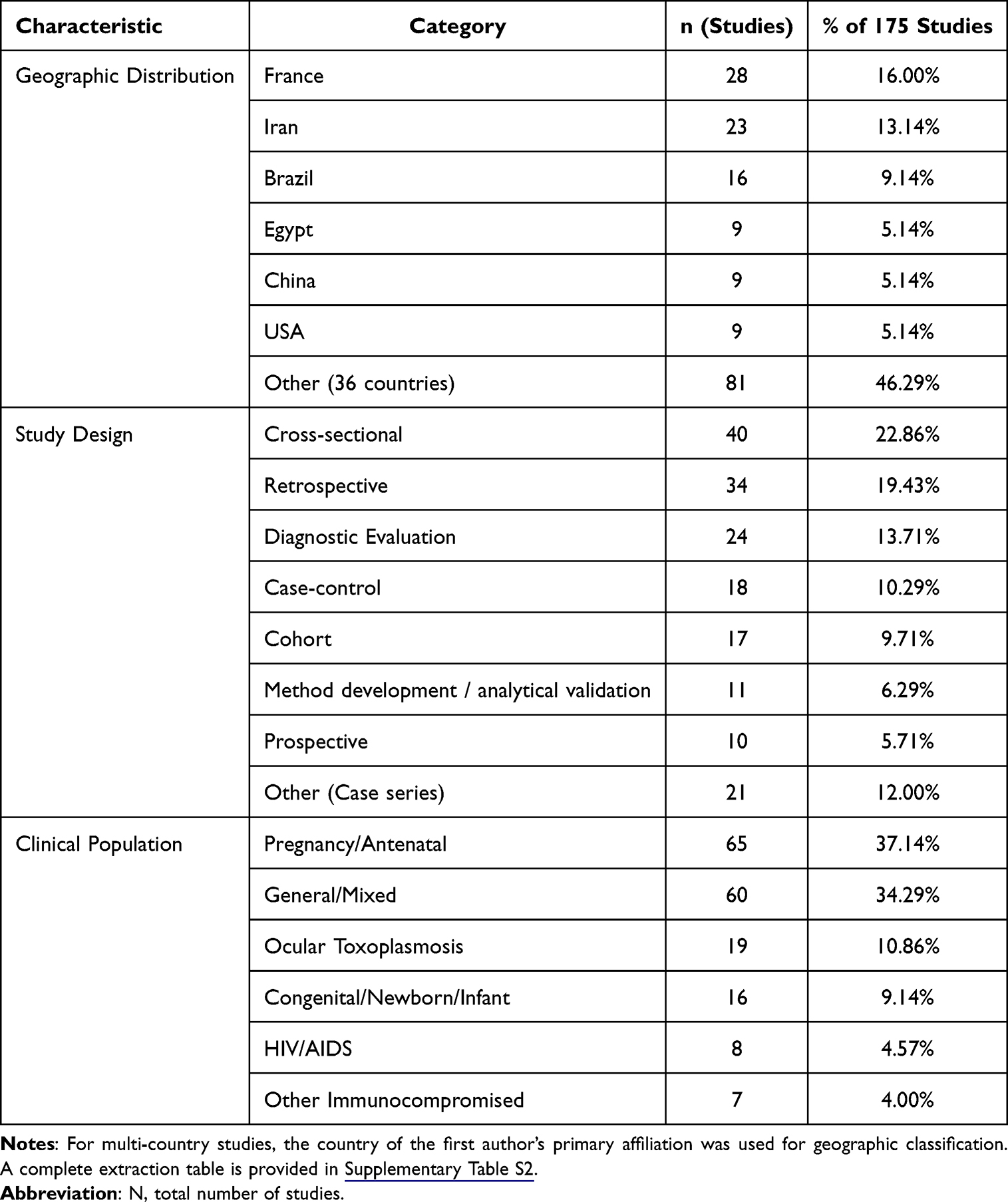 |
Table 1 Characteristics of Included Diagnostic Studies (N=175) |
Study Design and Clinical Populations
Cross-sectional design was the most common among the 175 included studies (n=40, 22.9%),25,28,32,34,36,49,52,55,62,63,69,73,74,84–86,90,91,96,98,99,102,105,106,109,113,114,117–119,121,123,133,134,136,140,144,146,147,152 followed by retrospective (n=34, 19.4%)13,16,22,29,33,45–49,56,60,62,65,67,68,72,76,78,80,82,83,100,107,110,111,115,125,130,135,137,138,141,142 and diagnostic evaluation studies (n=24, 13.7%)11,15,19,21,26,27,30,31,39,41,51,54,66,80,90,92,96,105,112,127,139,148,159,168,169,172 (Table 1 and Figure 3A).
 |
Figure 3 Bibliometric and temporal trends across included studies (N = 175). Panel (A) shows the distribution of study designs, and Panel (B) shows the distribution of clinical populations represented in the included evidence. |
The most frequently studied clinical population was pregnant/antenatal women, represented in 65 studies (37.1%),11,19,25–28,30,31,33–36,38,39,44,46,48,49,51,52,55–58,60–67,70–74,76–84,93,96–98,101,102,106–113,115,117,127,129,132,136,138,141,142,144,146,148–150,152,154,155,158,161,166,171 followed by general/mixed populations (60 studies,34.3%)6–9,12–14,17,18,20–24,32,34,35,37,40–42,45,47,49,50,53,54,59,68,69,72–75,80,85–90,92,95,97–100,104,105,108–114,118,120–123,126,128,130,131,133–135,138–140,145,147,148,150,151,153,156,157,160,162,163,165,167,168,170,172,173,176,178,179 and patients with ocular toxoplasmosis (19 studies, 10.9%) (Table 1 and Figure 3B). Studies on immunocompromised populations, particularly non-HIV groups, were less common (7 studies, 4.0%).
Diagnostic Technologies, Targets, and Specimens of Test Evaluations
The majority of the 309 test evaluations were based on conventional laboratory-based methods (245 evaluations; 79.3%).6–180 Point-of-care (POC) platforms accounted for 56 evaluations (18.1%),9,29,32,42,54,59,61,64,67,69,72,82,84,87,90,92,95,98,99,104,108,112,114,115,117,121,123,127,128,134,143,146–148,150,155,161,165,168–170,172,173 while emerging technologies (eg, machine learning, biosensors) were represented in only 8 evaluations (2.6%).13,104,126,128,131,151,160,178
Regarding detection targets, IgG was the most common (81 evaluations; 26.2%),6–8,10,12–14,19,21,24–26,28,30,34,35,39,42,47,58,59,68,70,71,73–78,80,81,83,84,86–90,92–180 followed by IgM (40 evaluations; 12.94%),6,10,18,20,26,30,36,42,53,65,73,77,84,91,113,142,146,162,172 parasite DNA (70 evaluations; 22.7%),9,15,16,23,29,37,40,41,44,45,48,56,68,69,72,75,76,79,81,82,85,88,94,99,100,107,110,112,113,116,118,119,121,124,125,128,130,131,133–135,137,140,143,145,149,150,154,156–158,161,163,164,167,169,172,175,177,179 combined IgG+IgM (52 evaluations; 16.8%),6,10,11,13,17,22,24,30–32,38,42,43,46,50,52,59,61,63,67,76,77,80,87,89,93,96,98–100,104,107,109–115,117,120,122,123,127,132,134,135,144,146,148,150,152,153,155,159,162,165,166,170,173,176 IgG Avidity (32 evaluations; 10.36%),7,21,27,33,49,51,54,55,58,60,65–67,70,76,78,91,113,122,129,136,158,171 Antigen (7 evaluations, 2.27%)73,97,103,116 and others (27 evaluations, 8.74%) encompassing a wide array of diagnostic approaches beyond standard serological and molecular targets. This category included the assessment of IgA antibodies and IgG subclasses for enhanced serological profiling, the evaluation of specific host biomarkers like anti-Hsp70.1 IgG, and the use of machine learning algorithms for the analysis of clinical images. It also captured studies focused on novel antigen-antibody interactions, such as those involving recombinant GRA7 and AMA1 proteins in experimental immunoassays.15,17,24,30,32,41,43,51,52,63,65,71,77,90,104,112,123,126,131,133,134,140,141,160,163,174
Serum was the predominant specimen type, used in 214 evaluations (69.3%).6–180 Other specimen types included unspecified blood (10.7%),16,43,45,56,63,69,76,77,79,81,82,85,88,94,107,112,119,121,124,125,133,135,137,140,145,156,164,167,169,172,177,179 whole blood (5.2%),9,65,99,100,107,110,112,119,149,155,161,169 plasma (2.91%)14,38,42,54,124,152,158 and specialized clinical matrices such as ocular fluid (8,4%),15,75,103,123,131,140,157,159,160,163,172,175 amniotic fluid (1.94%),37,40,48,68,132 and urine (1.62%)73,99,130 (Table 2 and Figure 4).
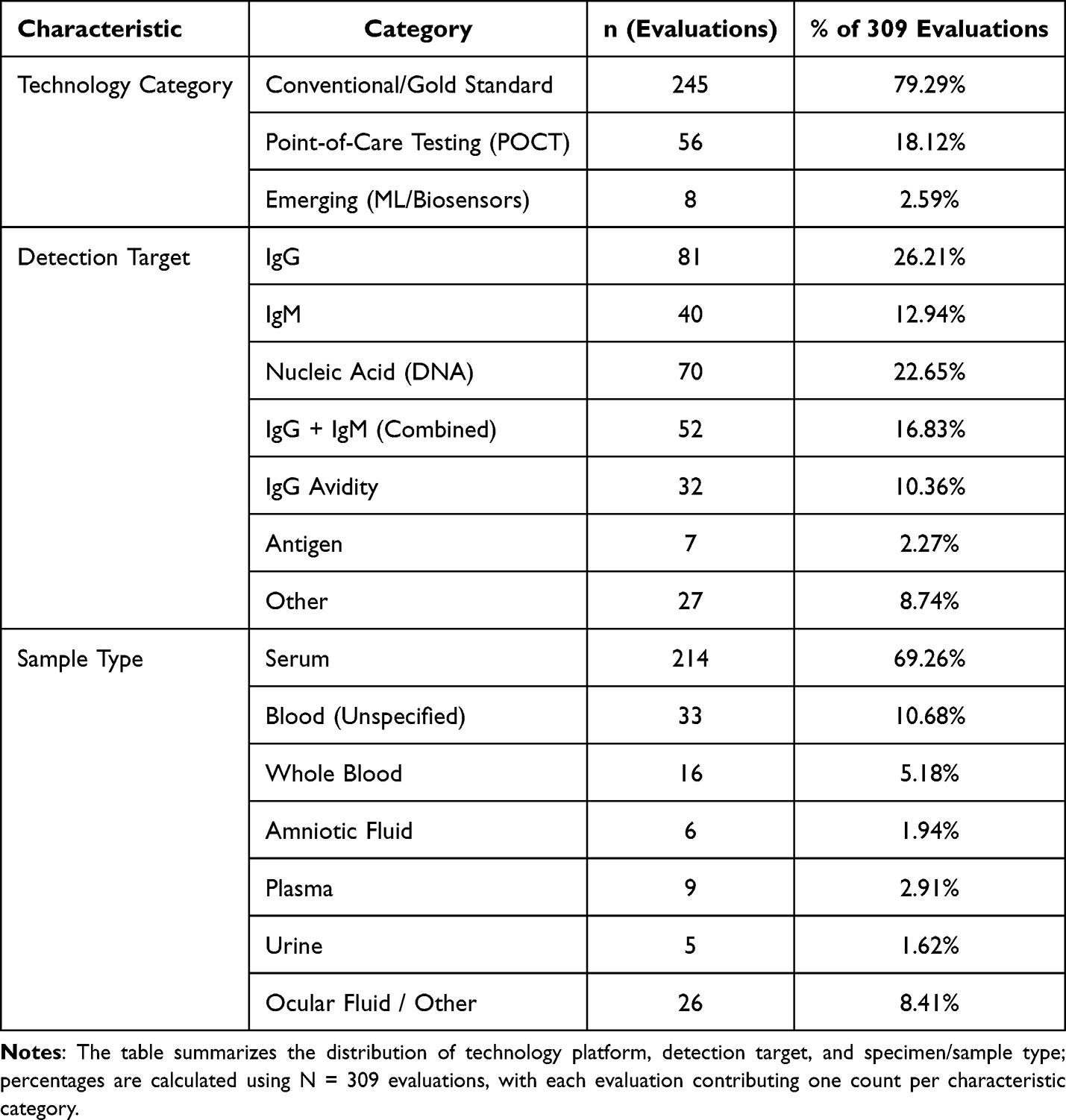 |
Table 2 Characteristics of Diagnostic Test Evaluations Included in Evidence Mapping (N = 309) |
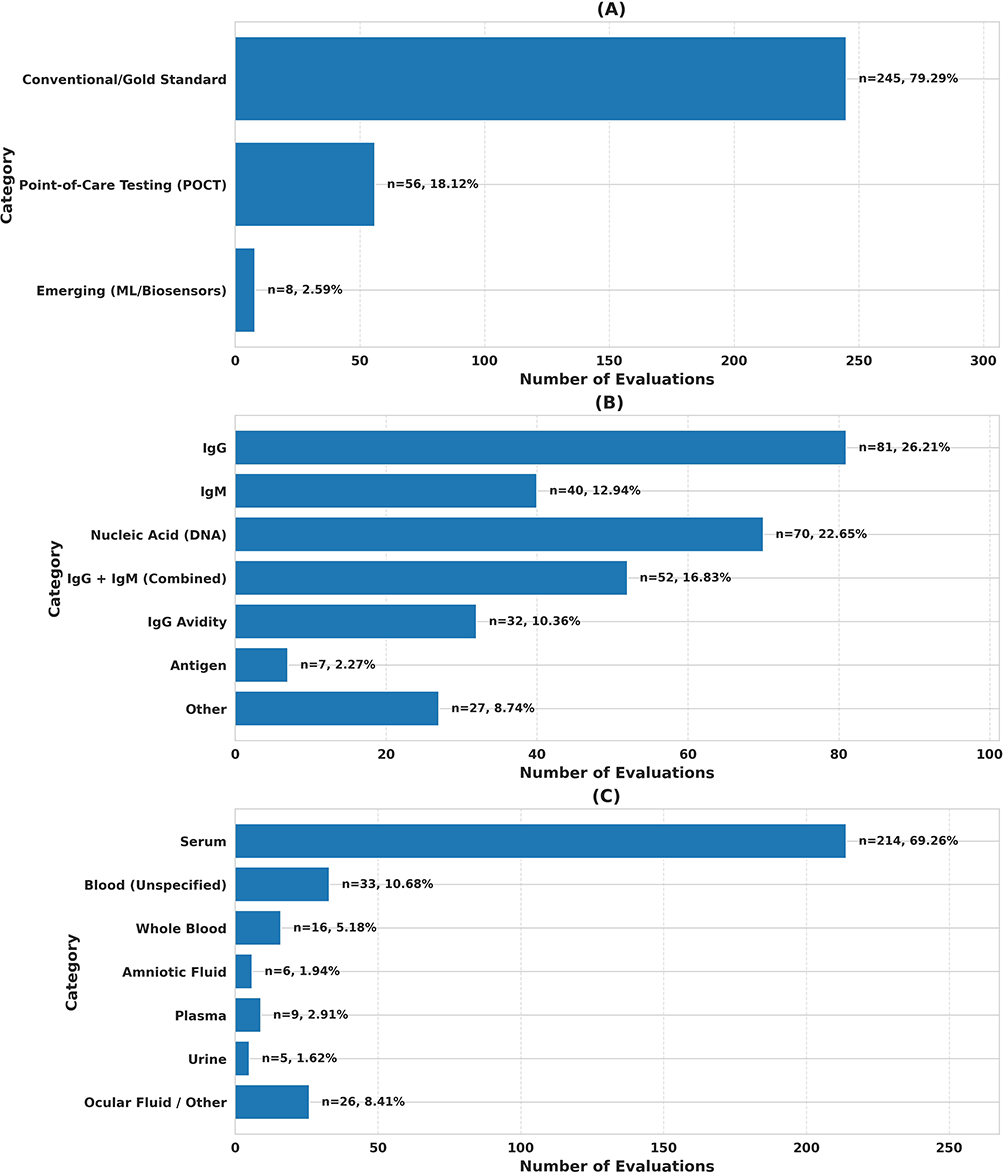 |
Figure 4 Distribution of diagnostic technologies (A), detection targets (B), and specimen/sample types (C) across included test evaluations (N = 309). Percentages are calculated based on total evaluations. |
Operational Readiness and Validation Maturity
Among the 309 test evaluations for which validation stage could be classified, only 71 (23%) reported quantitative time-to-result data.6,9,11,18,19,21,29,32,33,37,41,44,46,49,53–56,58,59,61,63,65,67–82,84–180 Among this subset of studies, the majority described rapid diagnostic protocols, with 74.7% delivering a result within 30 minutes and nearly half (45.1%) achieving a result in 10 minutes or less (Table 3). Reported assay times demonstrated substantial variation, ranging from 1 minute to 115 minutes. Further details are available in Supplementary Table S3.
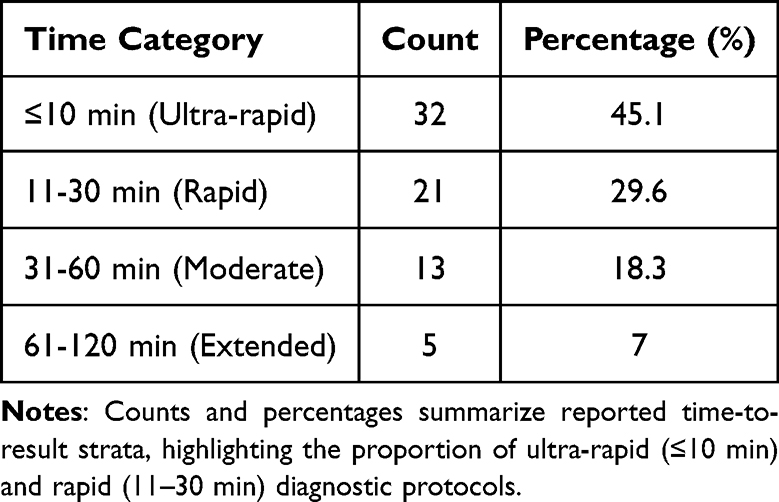 |
Table 3 Distribution of Time-to-Result Categories Among Evaluations Reporting Quantitative Assay Turnaround Time (n = 71) |
In contrast to the sparse temporal data, information on the validation stage was available for all 309 test evaluations. Analysis using a tiered validation framework revealed that the evidence base is predominantly composed of early-stage evaluations. A total of 115 evaluations (37.2%) were classified as Tier 0 (analytical/contrived samples only), representing proof-of-concept studies without clinical specimen testing. A further 100 evaluations (32.4%) were classified as Tier 1 (clinical laboratory validation), involving human specimens tested under controlled laboratory conditions. Another 87 evaluations (28.2%) involved general clinical sample testing without broader validation, corresponding to Tier 2 (near-patient pilot). In stark contrast, only 7 evaluations (2.3%) reached Tier 3, defined as large-scale field validation under real-world conditions. This distribution underscores a significant translational gap between initial test development and the generation of implementation-ready evidence.
Risk of Bias Assessment
Methodological quality, assessed using QUADAS-2 for the 175 included studies, revealed substantial concerns (Table 4 and Figure 5). The overall risk of bias was high in 139 studies (79.4%) and unclear in 36 studies (20.6%); no study was rated as low risk.
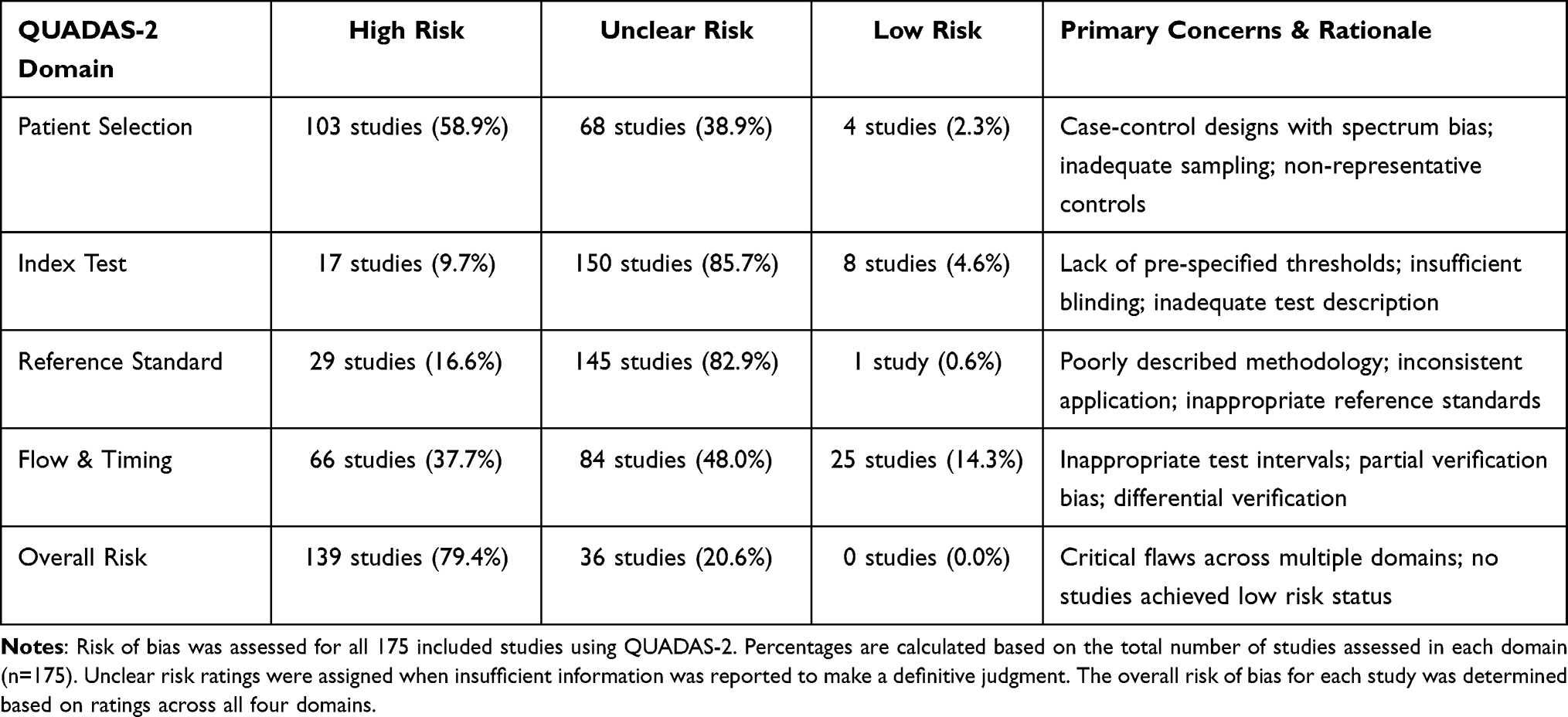 |
Table 4 Summary of Risk of Bias Assessment Using QUADAS-2 |
 |
Figure 5 Risk of Bias Assessment Using QUADAS-2 (n=175). Distribution of low, unclear, and high risk judgments across QUADAS-2 domains. Patient Selection had the highest high-risk proportion (58.9%), while Index Test and Reference Standard were dominated by unclear risk ratings (85.7% and 82.9%, respectively). The overall risk of bias was high in 139 studies (79.4%) and unclear in 36 studies (20.6%); no study achieved low risk status. |
Consistent with the overall rating, the domain with the highest proportion of high-risk judgments was Patient Selection (103 studies, 58.9%), primarily due to the prevalent use of case-control designs with non-representative controls and non-consecutive sampling.8,9,13,15,18–24,26,27,29,32–35,40,42,43,45–47,49,52–55,58–68,70,72–180 The Index Test and Reference Standard domains were dominated by unclear risk ratings (85.7% and 82.9%, respectively), reflecting a critical deficit in reporting of pre-specified thresholds, blinding procedures, and reference standard methodology.
Meta-Analysis of Diagnostic Accuracy and Associated Heterogeneity
Overall Accuracy by Detection Target
The quantitative synthesis included 182 (58.9%) test evaluations from the 309 identified in evidence mapping, comprising 42,287 total samples. Pooled sensitivity and specificity were estimated using a bivariate random-effects model (Reitsma), which jointly synthesizes sensitivity and specificity while accounting for their correlation across studies and enabling inference in ROC space. To ensure numerical stability in sparse strata with zero cells, a continuity correction (CC) of 0.5 was applied where required for estimation on the logit scale (Table 5).
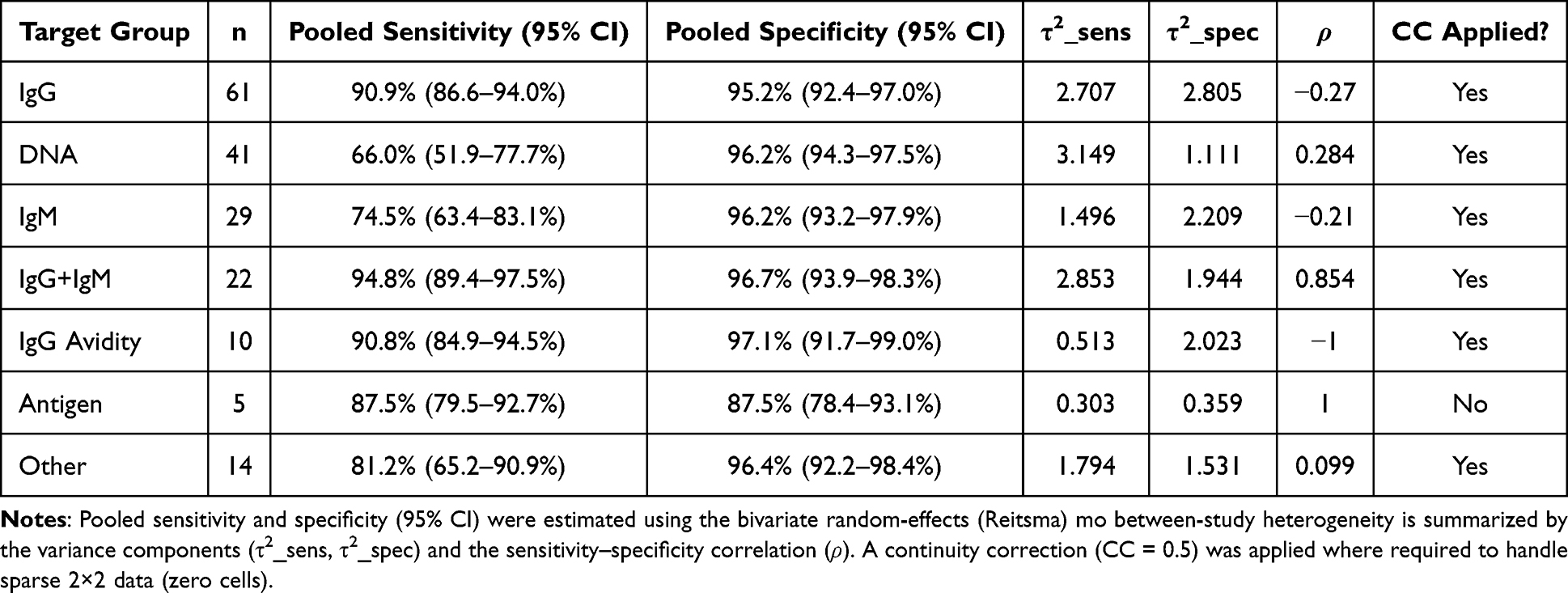 |
Table 5 Pooled Diagnostic Accuracy by Detection Target from the Quantitative Meta-Analysis (n = 182 Evaluations; 42,287 Total Samples) |
Across detection targets, pooled accuracy differed markedly (Table 5 and Figure 6). The highest combined performance was observed for IgG+IgM (combined) and IgG avidity, both demonstrating high pooled sensitivity and specificity. Specifically, IgG+IgM achieved pooled sensitivity 94.8% (95% CI: 89.4–97.5) and specificity 96.7% (93.9–98.3), while IgG avidity showed pooled sensitivity 90.8% (84.9–94.5) and specificity 97.1% (91.7–99.0) (Table 5 and Figure 6). In ROC space, IgG+IgM also exhibited substantial dispersion in study operating points, reflected by large bivariate variance components (τ2_sens = 2.853; τ2_spec = 1.944) and a strong positive correlation (ρ = 0.854), consistent with meaningful variation in thresholds and implementation across settings (Table 5). This pattern is visually supported by the SROC plot for IgG+IgM (Figure 7), with corresponding study-level dispersion evident in the paired forest plots (Supplementary Figures S1 and S2).
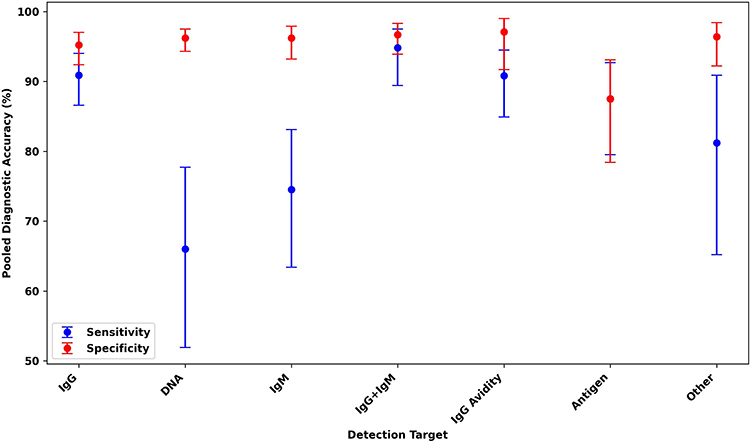 |
Figure 6 Pooled diagnostic accuracy by detection target, showing sensitivity and specificity with 95% confidence intervals estimated using the bivariate random-effects (Reitsma) model across included evaluations (n = 182; total samples = 42,287). |
 |
Figure 7 Summary ROC (SROC) plot for the IgG+IgM target group (Reitsma; n = 22 evaluations). Points represent individual study operating sensitivities/specificities, with the summary estimate and confidence region summarizing pooled performance and between-study dispersion. |
The most frequently evaluated target, IgG (n = 61), yielded robust pooled estimates—sensitivity 90.9% (86.6–94.0) and specificity 95.2% (92.4–97.0)—but with substantial between-study variability (τ2_sens = 2.707; τ2_spec = 2.805) and a modest negative correlation (ρ = −0.27), indicating heterogeneous operating points rather than a single consistent threshold (Table 5). This heterogeneity is apparent on the SROC representation (Figure 8) and is further illustrated by the study-level forest plots (Supplementary Figures S3 and S4).
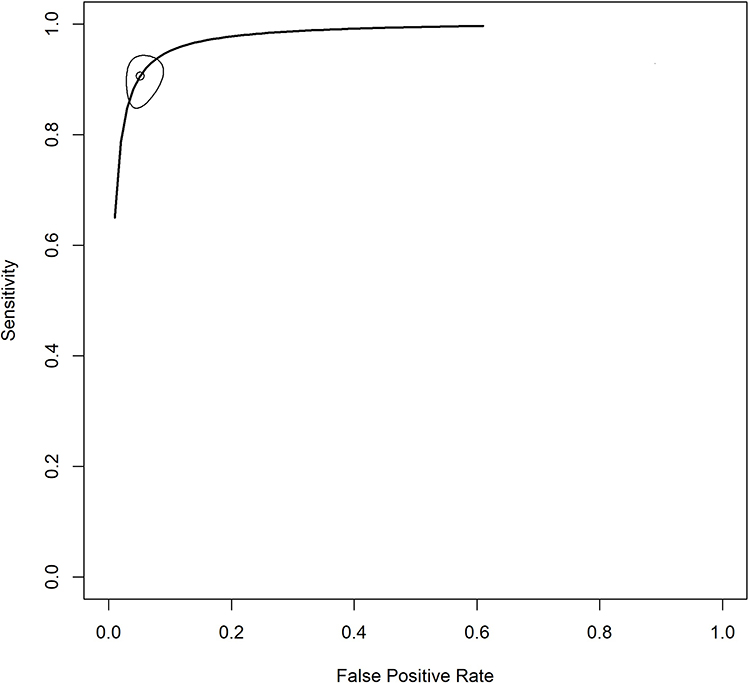 |
Figure 8 Summary ROC (SROC) plot for the IgG target group (Reitsma; n = 61 evaluations). Study-level operating points are displayed in ROC space, alongside the pooled summary estimate and its uncertainty to illustrate heterogeneity across evaluations. |
A clinically informative contrast was observed for DNA-based assays (n = 41), which showed the lowest pooled sensitivity (66.0%, 95% CI: 51.9–77.7) while maintaining high specificity (96.2%, 94.3–97.5), consistent with a “rule-in” profile in which false positives are uncommon, but missed detections remain an important limitation (Table 5 and Figure 6). Heterogeneity in sensitivity was considerable (τ2_sens = 3.149), while specificity variability was more moderate (τ2_spec = 1.111), suggesting that differences in assay protocols, specimen matrices, and reference standards may disproportionately affect sensitivity (Table 5). This trade-off and dispersion in ROC space are summarized in the SROC plot Figure 9, with complementary study-level patterns shown in forest plots (Supplementary: Figures S5 and S6).
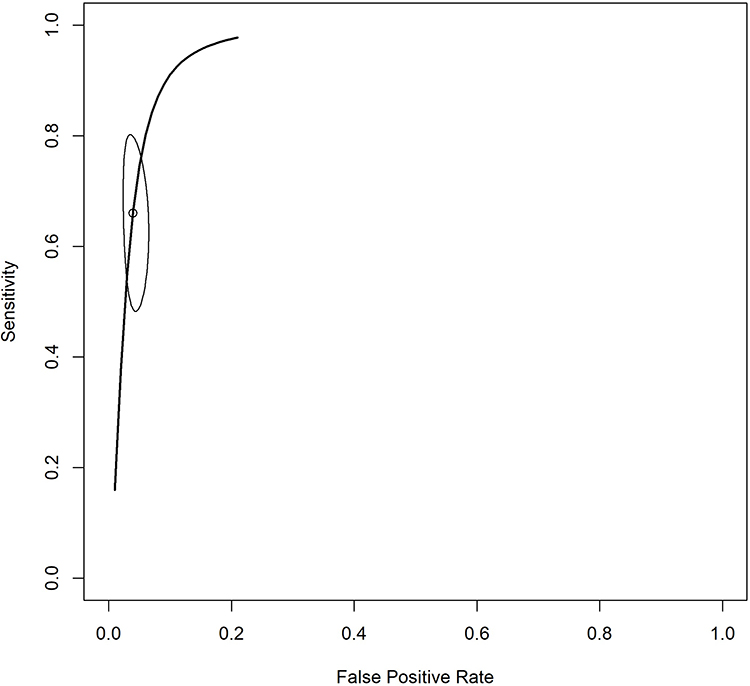 |
Figure 9 Summary ROC (SROC) plot for the DNA target group (Reitsma; n = 41 evaluations). The plot visualizes the trade-off between sensitivity and specificity across studies and the pooled summary operating point with associated confidence region. |
For IgM (n = 29), pooled sensitivity was lower (74.5%, 63.4–83.1) with high specificity (96.2%, 93.2–97.9), consistent with a confirmatory profile (Table 5 and Figure 6). The negative correlation (ρ = −0.21) and sizeable variance components (τ2_sens = 1.496; τ2_spec = 2.209) indicate heterogeneity in operating points that may reflect threshold effects and population spectrum differences across studies (Table 5). These patterns are captured visually in Figure S7 and the corresponding forest plots (Supplementary Figures S8 and S9).
Antigen detection (n = 5) demonstrated balanced pooled accuracy (sensitivity 87.5%, specificity 87.5) with comparatively smaller variance components (τ2_sens = 0.303; τ2_spec = 0.359), but inference remains limited by the small number of evaluations; notably, a continuity correction was not applied in this subgroup (Table 5). These findings are best treated as supportive and are presented with full visual context in Figure 10 and paired forest plots (Supplementary: Figures S10 and S11). Finally, the other target category showed intermediate sensitivity (81.2%) with high specificity (96.4%) and notable heterogeneity (τ2_sens = 1.794; τ2_spec = 1.531), reflecting the diversity of assays subsumed within this grouping (Table 5). The overall dispersion is summarized in Figure S12 with supporting forest plots (Supplementary: Figures S13 and S14).
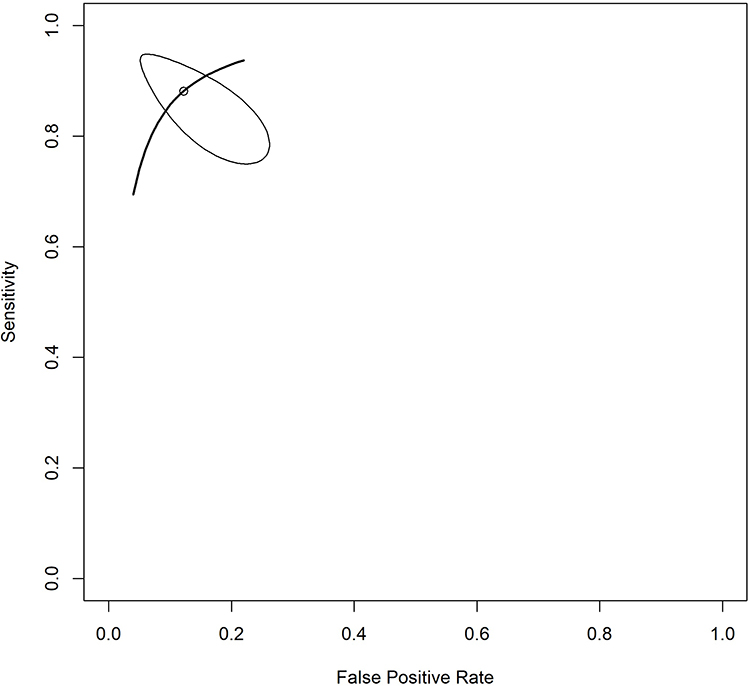 |
Figure 10 Summary ROC (SROC) plot for the Antigen target group (Reitsma; n = 5 evaluations). Study operating points and the pooled summary estimate are shown; interpretation should consider the limited number of evaluations. |
Subgroup Analysis by Clinical Population
Performance varied meaningfully across clinical populations (Table 6 and Figure 11). In general/mixed/other populations (n = 58), tests achieved the strongest overall performance with pooled sensitivity 90.6% (95% CI: 87.3–93.2) and specificity 96.6% (94.8–97.8), while heterogeneity remained substantial (τ2_sens = 1.296; τ2_spec = 1.951) and the correlation was modestly positive (ρ = 0.206), consistent with dispersion of operating points across heterogeneous real-world cohorts (Figures 11 and 12; Supplementary: Figures S15 and S16).
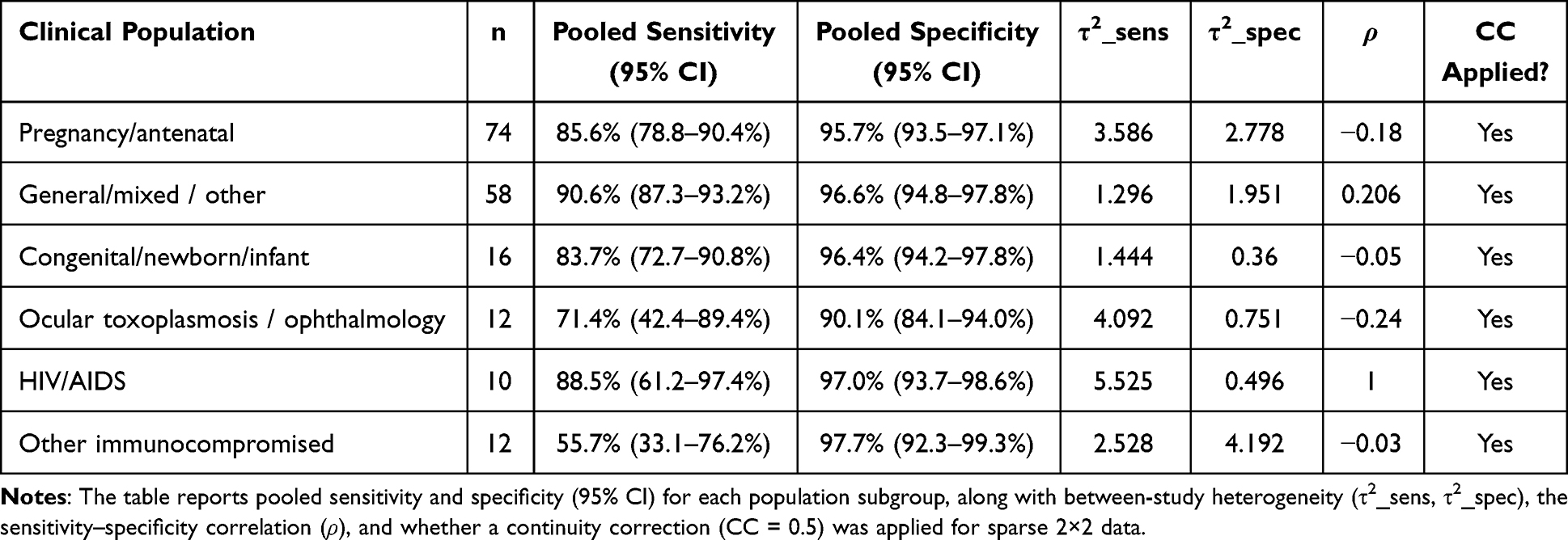 |
Table 6 Subgroup Meta-Analysis of Diagnostic Accuracy by Clinical Population Using the Bivariate Random-Effects (Reitsma) Model |
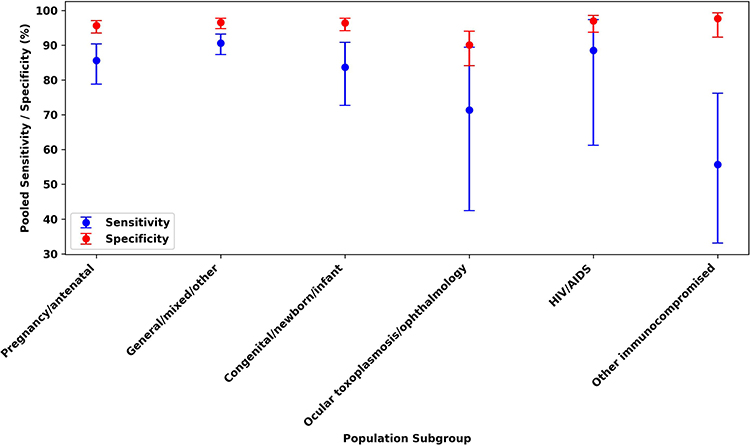 |
Figure 11 Pooled diagnostic accuracy by clinical population subgroup, showing sensitivity and specificity with 95% confidence intervals estimated using the bivariate random-effects (Reitsma) model. Subgroups are defined by clinical population, and pooled estimates summarize between-study variability in performance across settings. |
 |
Figure 12 Summary ROC (SROC) plot for the general/mixed/other population subgroup (Reitsma; n = 58 evaluations). Study operating points are displayed in ROC space together with the pooled summary estimate and its uncertainty, illustrating dispersion across heterogeneous real-world cohorts. |
In pregnancy/antenatal cohorts (n = 74), pooled sensitivity was lower at 85.6% (78.8–90.4) with similarly high specificity 95.7% (93.5–97.1). This subgroup exhibited among the largest bivariate variance components (τ2_sens = 3.586; τ2_spec = 2.778) and a negative correlation (ρ = −0.18), indicating wide dispersion in ROC space that is compatible with spectrum effects and differences in testing pathways (screening vs diagnostic work-up) across studies (Figure 11; Supplementary Figures S17, S18 and S32).
Across high-stakes groups, specificity remained consistently high. Congenital/newborn/infant populations (n = 16) showed pooled sensitivity 83.7% (72.7–90.8) and specificity 96.4% (94.2–97.8), with relatively lower specificity heterogeneity (τ2_spec = 0.360) and near-zero correlation (ρ = −0.05), suggesting more stable specificity across studies (Figure 11). HIV/AIDS populations (n = 10) demonstrated pooled sensitivity 88.5% (61.2–97.4) and specificity 97.0% (93.7–98.6); however, the very large sensitivity variance (τ2_sens = 5.525) indicates substantial instability in operating points, consistent with limited evidence and heterogeneous settings (Figure 11; Supplementary: Figures S19–S22).
Most notably, other immunocompromised populations (n = 12) revealed a pronounced diagnostic gap: pooled sensitivity was markedly reduced at 55.7% (33.1–76.2) despite very high specificity 97.7% (92.3–99.3). Variability was substantial for both components (τ2_sens = 2.528; τ2_spec = 4.192), with correlation near zero (ρ = −0.03), implying that sensitivity and specificity varied across studies without a consistent trade-off pattern (Figure 11). Clinically, this pattern is compatible with reduced performance of immune-response–dependent assays in vulnerable hosts, increasing the risk of missed diagnoses (Figure 13; Supplementary: Figures S23 and S24).
 |
Figure 13 Summary ROC (SROC) plot for the other immunocompromised population subgroup (Reitsma; n = 12 evaluations). The plot visualizes study-level operating points and the pooled summary estimate, highlighting the subgroup’s overall pattern of high specificity with reduced sensitivity and substantial heterogeneity. |
For ocular toxoplasmosis/ophthalmology (n = 12), pooled sensitivity 71.4% (42.4–89.4) and specificity 90.1% (84.1–94.0) were accompanied by very large heterogeneity (τ2_sens = 4.092), plausibly reflecting variation in case definitions, ocular specimen matrices, and reference standards (Figure 11; Supplementary: Figures S25–S27).
Subgroup Analysis by Technology Platform
This analysis compared the two major clinically operationalized technology categories (Table 7, Figure 14). Among the 182 evaluations eligible for quantitative synthesis, conventional assays (n = 140) and POCT (n = 40) provided sufficient data for bivariate estimation, whereas Emerging and Other categories were too sparse to pool (n = 1 each) and were therefore not meta-analytically summarized (Table 7).
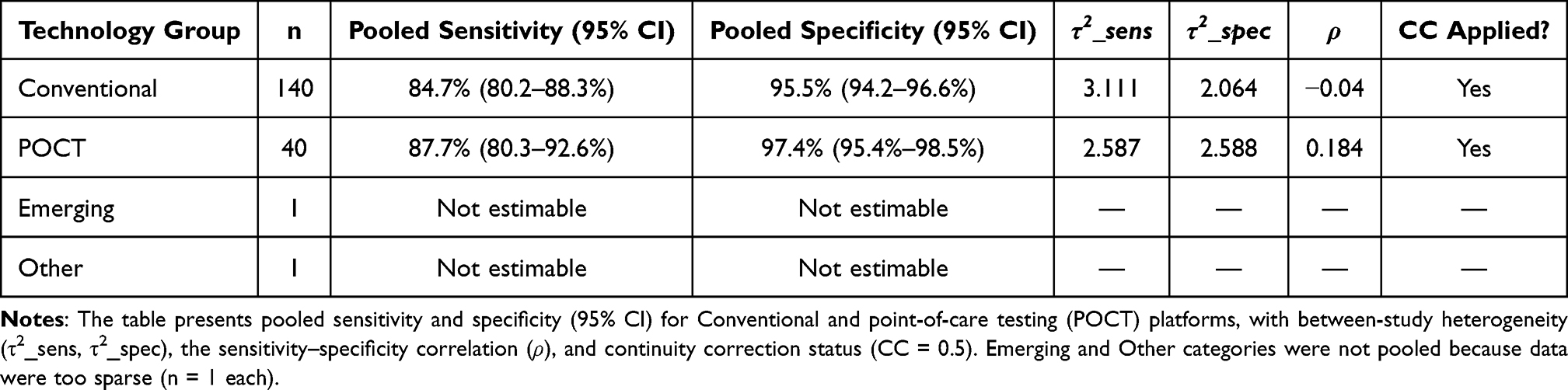 |
Table 7 Subgroup Meta-Analysis of Diagnostic Accuracy by Technology Platform Using the Bivariate Random-Effects (Reitsma) Model |
 |
Figure 14 Pooled diagnostic accuracy by technology platform, showing sensitivity and specificity with 95% confidence intervals estimated using the bivariate random-effects (Reitsma) model. Results are presented for Conventional laboratory assays (n = 140) and point-of-care testing (POCT) platforms (n = 40); Emerging and Other categories were not pooled due to insufficient data (n = 1 each). |
POCTs (including lateral flow assays and LAMP) demonstrated a favorable accuracy profile, with pooled sensitivity 87.7% (95% CI: 80.3–92.6) and specificity 97.4% (95.4–98.5), while Conventional laboratory assays achieved pooled sensitivity 84.7% (80.2–88.3) and specificity 95.5% (94.2–96.6) (Figures 14–16). Although confidence intervals overlapped, the consistently higher specificity for POCT supports their potential utility as rule-in tools, particularly in settings where rapid turnaround and decentralized testing are operational priorities (Figures 14 and 15).
 |
Figure 15 Summary ROC (SROC) plot for POCT platforms (Reitsma; n = 40 evaluations). Points represent individual study operating sensitivities/specificities in ROC space, with the pooled summary estimate and its uncertainty summarizing overall performance and between-study dispersion among point-of-care tests. |
 |
Figure 16 Summary ROC (SROC) plot for Conventional laboratory-based assays (Reitsma; n = 140 evaluations). Study operating points are shown in ROC space together with the pooled summary estimate and confidence region, illustrating heterogeneity and variability in diagnostic performance across conventional platforms. |
Heterogeneity remained notable in both groups (Conventional: τ2_sens = 3.111; τ2_spec = 2.064; POCT: τ2_sens = 2.587; τ2_spec = 2.588), indicating substantial dispersion in study operating points; this dispersion is visually reflected by the breadth of study-level estimates in the technology-stratified forest plots (Supplementary: Figures S28–S31).
Heterogeneity, Sensitivity Analysis, and Visual Synthesis
Between-study heterogeneity was evaluated within the bivariate framework using the random-effects variance components for sensitivity and specificity (τ2_sens and τ2_spec) and the estimated correlation (ρ) (Tables 5–7), alongside visual inspection of study dispersion in ROC space. Substantial heterogeneity was evident for multiple targets and subgroups—most notably IgG, DNA, and pregnancy/antenatal cohorts—where large τ2 values indicate wide variation in study operating points that likely reflects spectrum effects, assay thresholds, specimen types, reference standards, and differences in study conduct (eg, Supplementary: Figures S3–S6, S18 and S32).
Accordingly, robustness was judged primarily from the consistency of pooled estimates across subgroups and from concordance between model-based summaries and the observed dispersion of study operating points in ROC space, with visual support provided by the subgroup-specific forest plots of sensitivity and specificity and the corresponding SROC plots (Supplementary: Figures S7, S12, S17, S19, S20, S25, S33).
Visual synthesis complemented statistical pooling. Forest plots of study-level sensitivity and specificity illustrate the dispersion of estimates within each subgroup, while SROC plots provide an integrated depiction of sensitivity–specificity trade-offs across categories in ROC space. In these visualizations, IgG+IgM and IgG Avidity tend to lie closest to the desirable top-left corner (Figure 7; Supplementary: Figure S33), whereas DNA-based assays cluster in a high-specificity/low-sensitivity region, reinforcing their rule-in profile (Figure 9).
Publication bias was explored qualitatively through funnel plots as an assessment of potential small-study effects. Where available, two-panel funnel plots were reviewed for both sensitivity and specificity, but any asymmetry was interpreted cautiously because it may reflect threshold-related variation and clinical heterogeneity rather than selective reporting alone (Supplementary examples Figures S34–S37).
Between-subgroup differences were described by comparing pooled estimates and the extent of confidence interval overlap across stratified analyses (Tables 5–7, Figure 6, Figure 11, Figure 14). These comparisons are intended to support interpretation and hypothesis generation rather than to serve as formal interaction tests.
To complement the pooled bivariate estimates in Tables 5–7, supplementary figures provide full visual support by detection target, clinical population, and technology platform. Specifically, forest plots of study-level sensitivity and specificity (Supplementary Figures S1–S6, S8, S9, S10, S11, S13–S18, S21–S32, S38–S41) depict the spread of operating points contributing to the bivariate random-effects model in each subgroup, while SROC plots summarize the joint sensitivity–specificity trade-off in ROC space (Supplementary: Figures S7, S12, S17, S19, S20, S25, S33). Where the number of evaluations was sufficient, two-panel funnel plots (sensitivity and specificity) were included to explore potential small-study effects (Supplementary: Figures S34–S37, S42–S52), with interpretation tempered by the recognized influence of clinical and threshold-related heterogeneity in diagnostic accuracy meta-analyses.
Systematic Mapping of Analytical Performance Reporting
The reporting of analytical sensitivity, as measured by the Limit of Detection (LOD), was highly heterogeneous across the studies that reported it, presenting a major challenge for comparative evaluation.
For nucleic acid amplification tests (NAATs), LOD values were reported with wide variability—spanning over two orders of magnitude—even for the same technology. Values ranged from 0.01–1 parasite or genome equivalent per mL for optimized PCR/qPCR assays116,137,177 to 5–10 parasites or genome copies per reaction for many LAMP and some PCR protocols.9,69 This variability was exacerbated by the use of inconsistent and non-comparable units (eg, copies/µL, tachyzoite equivalents, genome equivalents/reaction),16,69,85 precluding a direct meta-analysis of analytical sensitivity.
For serological assays (IgG/IgM), the quantitative reporting of LOD was exceptionally rare. The field predominantly relied on qualitative cut-offs (eg, IU/mL for ELISA) or reported LOD as “Not Reported/Not Applicable” (NR/NA) or “Not Stated” (N/S)12,27,28,71 (Figure 8B). This represents a critical standardization gap, as it limits the objective assessment of an assay’s ability to detect low antibody titers, a parameter crucial for early infection diagnosis and avidity testing.
Together, these inconsistencies underscore the urgent need for standardized guidelines (eg, following CLSI protocols) for determining and reporting LOD in toxoplasmosis diagnostic studies to enable meaningful cross-assay comparisons.
Discussion
Synthesis of Key Findings
This systematic review and meta-analysis, integrating evidence from 175 studies (309 test evaluations) and over 42,000 samples, provides a definitive, stratified evaluation of diagnostic test accuracy for human toxoplasmosis.5,181 Our dual-method approach confirms that performance is intrinsically dependent on the diagnostic target, clinical population, and technological platform. Three pivotal findings emerge. First, serological strategies that capture both exposure and infection timing showed the strongest combined accuracy: IgG+IgM (combined) and IgG avidity demonstrated high pooled sensitivity and specificity (IgG+IgM: 94.8% and 96.7%; IgG avidity: 90.8% and 97.1%; Table 5), supporting their central role in clinical algorithms where dating infection is critical.2,182 Second, we identify a clinically important diagnostic blind spot: pooled sensitivity was substantially reduced in other immunocompromised (non-HIV) populations (55.7%) despite very high specificity (97.7%; Table 6), raising concern for missed diagnoses in vulnerable hosts.183 Third, POCTs demonstrate high specificity (97.4%) with good sensitivity (87.7%; Table 7), supporting rapid rule-in use within defined pathways, while acknowledging ongoing heterogeneity in study operating points.184
Interpretation of Dominant Technological Paradigms and Evolution
The evidence landscape remains dominated by conventional laboratory-based methods (79.3% of test evaluations), underscoring their entrenched role as reference standards (Table 2). This aligns with patterns in established infectious diseases, where innovation supplements rather than replaces validated workflows. The substantial representation of both serology (eg, ELISA for IgG/IgM) and molecular methods (eg, PCR for DNA) reflects their complementary roles—assessing immune status and detecting active infection, respectively.
The growth of POCTs to 18.1% of evaluations signals strong research interest in decentralized diagnostics.184 However, the diversity of platforms (LFIA, LAMP) presents both opportunity and standardization challenges. Emerging technologies (eg, machine learning, biosensors) remain nascent (2.6% of evaluations), primarily integrated with imaging, pointing to a future computational transformation.3,126,160,170,178
Most critically, our tiered validation analysis reveals a profound “validation chasm”: while 74.7% of assays with timing data are rapid (<30 min), a striking 97.7% of evaluations were limited to laboratory or early clinical validation (Tiers 0-2). Only 2.3% reached Tier 3 (large-scale field validation), highlighting a major translational gap between technological capability and proven real-world impact.185,186
Methodological and Analytical Landscape
A clear methodological dichotomy exists. Serological targets (IgG, IgM, Avidity) dominated the evidence base, accounting for the majority of evaluations, and were predominantly performed on serum (69.3% of evaluations). This reflects their well-established and accessible role in routine screening and exposure assessment (Table 2).25,26,33,53 In contrast, molecular detection of parasite DNA (22.7% of evaluations) was more frequently applied to clinically specialized matrices such as ocular fluid, amniotic fluid, and CSF (collectively categorized as “Ocular Fluid/Other,” 8.4% of evaluations) for direct pathogen detection in complex presentations like ocular and congenital toxoplasmosis.15,40,44,68,75 The substantial evaluation of IgG Avidity (10.4% of evaluations) confirms its recognized clinical importance for dating infection,30,33,67,129 whereas antigen detection remains a relatively unexplored avenue (2.3% of evaluations) despite its potential for diagnosing acute infection.73,97,103
Interpretation in Context of Clinical Scenarios
The clinical utility of a test is context-dependent, a principle starkly illustrated by our subgroup analyses.
Pregnancy: IgG avidity showed high pooled accuracy for infection dating (Table 5) and remains the key adjunct for interpreting serology in prenatal settings.2,30,33,58,129,182 However, pooled sensitivity in pregnancy/antenatal cohorts was lower than in general/mixed populations (85.6% vs 90.6%; Table 6), consistent with spectrum and pathway effects in screening contexts.
Ocular Toxoplasmosis (OT): Pooled performance was moderate (sensitivity 71.4%; specificity 90.1%; Table 6) with substantial heterogeneity, reaffirming that laboratory testing is often complementary and should be interpreted alongside clinical assessment and imaging, especially in atypical cases.101,103,123,131,140,157
Immunocompromised Patients (non-HIV): The reduced pooled sensitivity (55.7% with specificity 97.7%; Table 6) indicates a meaningful diagnostic vulnerability. Current tools may miss reactivation or atypical presentations, supporting the need for improved biomarkers and optimized sampling strategies.86,119,124,130,143
Confirmatory Role of Molecular Tests: DNA-based assays showed high specificity (96.2%) but limited sensitivity (66.0%; Table 5), reinforcing their established role as confirmatory tests in selected scenarios (eg, congenital infection work-up, ocular fluid sampling) rather than broad screening.110,116,137,156,164,177
The Translational Pathway, Validation Chasm, and Reporting Gaps
Our tiered validation framework maps a concerning pipeline: robust innovation at the analytical (Tier 0) and early clinical (Tier 1) stages, but a dramatic funnel narrowing at the point of real-world implementation.185 This “validation chasm” is particularly acute for promising POCTs and novel biosensors.61,98,114,117,146,155 Furthermore, reporting gaps fundamentally undermine evidence quality and comparability. While quantitative time-to-result data were reported in only 29.7% of relevant evaluations, the reporting of analytical sensitivity was critically deficient. As detailed in Systematic Mapping of Analytical Performance Reporting, quantitative Limit of Detection (LOD) data were highly inconsistent for molecular assays9,16,37,69,85,116,137,169,177 and virtually absent for serological tests,12,27,28,71 precluding any meaningful cross-assay comparison of analytical performance.
Implications for Clinical Practice and Policy
Beyond performance, fundamental methodological weaknesses plague the evidence base. The QUADAS-2 assessment found no studies rated as low overall risk of bias (high: 79.4%; unclear: 20.6%),5,181 with prevalent case-control designs and limited reporting of blinding and thresholds. In addition, large bivariate variance components (τ2) and wide dispersion in ROC space for several key subgroups (eg, IgG, DNA, pregnancy/antenatal, and combined IgG+IgM) limit certainty and suggest meaningful clinical and methodological diversity across studies. Geographic skew (with major contributions from Europe and South America) may also affect generalizability to other regions.22,34,45,58,132,146
To address this, we recommend:
- Test Selection & Algorithms: Prioritize IgG Avidity to support serological dating of infection (Table 5). Use POCTs as rapid rule-in tools given their high specificity (97.4%) and good sensitivity (87.7%) (Table 7), but interpret negative results in clinical context and, where appropriate, follow with conventional laboratory testing or molecular confirmation.59,61,98,117,146,155
- Guideline Update: National and international guidelines should be updated to reflect the established superiority of IgG Avidity over single or combined IgG/IgM tests for serological dating.2,182
- Standardization Mandate: The field must adopt international standards (eg, CLSI, STARD) for analytical validation (LOD, dynamic range) and transparent reporting to enable comparability.5,181,187–189
Strengths and Limitations
The primary strengths of this review include its comprehensive, dual-method design integrating evidence mapping (of studies and test evaluations) with diagnostic meta-analysis, rigorous application of PRISMA-DTA/QUADAS-2 guidelines,5,181 and extensive multi-database searches spanning biomedical and engineering literature. Our tiered validation framework provides novel insights into translational readiness beyond conventional accuracy metrics.185,186 However, our conclusions are constrained by important limitations in the primary literature: methodological quality was generally poor (high risk of bias in 79.4% of studies), and substantial between-study heterogeneity (large τ2 estimates and wide dispersion in ROC space) was observed for several key subgroups, reflecting clinical and methodological diversity across studies. Additional limitations include geographical concentration of studies and—as systematically mapped in Systematic Mapping of Analytical Performance Reporting—the extreme heterogeneity and frequent non-reporting of Limit of Detection (LOD) data for molecular assays, precluding a meta-analysis of analytical sensitivity and limiting conclusions about detection at low parasite burdens.9,12,16,27,28,37,69,71,85,116,137,169,177,188
Despite these limitations in the primary literature, this review itself was conducted with methodological rigor. Methodologically, this review adhered to its pre-specified analytic framework. All planned subgroup analyses were completed, and pre-defined exclusion criteria for the “Emerging” technology category were applied consistently. Heterogeneity was quantified and contextualized through both statistical parameters (τ2 and ρ) and visual assessment, supporting the stability of the key conclusions.
Implications for Future Research
Future efforts must bridge the identified gaps through transformative, implementation-focused science:
- Prospective, Multi-center Trials: Conduct large-scale, methodologically rigorous (low bias) studies in well-defined cohorts using standardized reference standards.5,181
- Implementation Research: Evaluate the real-world impact, cost-effectiveness, and feasibility of integrating high-accuracy tests (like IgG Avidity) and POCTs into clinical pathways.155,184,185
- Biomarker Discovery: Urgently invest in novel biomarkers to address the diagnostic crisis in non-HIV immunocompromised patients.86,119,124,130,143
- Standardization Initiatives: Develop an international reference panel and consensus protocols for analytical validation and reporting, led by organizations like WHO or FIND.4,187,189 These protocols must specifically address the severe heterogeneity in LOD determination and reporting documented in this review, mandating the use of standardized units and clinically relevant thresholds.188
- Computational Integration: Further validate and develop machine learning applications, particularly for image analysis in ocular and neurological toxoplasmosis.3,126,131,160,170,178
Conclusion
This systematic review and bivariate meta-analysis provide a nuanced, clinically actionable evidence base for toxoplasmosis diagnostics. It highlights that accuracy varies substantially by detection target, clinical population, and technology platform. IgG avidity and combined IgG+IgM strategies demonstrated the strongest combined pooled accuracy for serological assessment and infection dating, while DNA assays showed a high-specificity but lower-sensitivity profile consistent with confirmatory use. POCTs demonstrated high specificity with good sensitivity, supporting rapid rule-in utility when embedded in appropriate algorithms. Critically, performance remained suboptimal in immunocompromised (non-HIV) populations, underscoring an urgent unmet need for improved diagnostics. Across the field, inconsistent reporting and limited large-scale field validation—the identified “validation chasm”—remain key barriers to confident clinical adoption.
Abbreviations
AI, Artificial Intelligence; AUC, Area Under the Curve; CC, Continuity Correction; CI, Confidence Interval; CLSI, Clinical and Laboratory Standards Institute; CSF, Cerebrospinal Fluid; DNA, Deoxyribonucleic Acid; DTA, Diagnostic Test Accuracy; ECDC, European Centre for Disease Prevention and Control; ELFA, Enzyme-Linked Fluorescent Assay; ELISA, Enzyme-Linked Immunosorbent Assay; FIND, Foundation for Innovative New Diagnostics; FN, False Negative; FP, False Positive; GRA, Dense Granule Protein ; HIV, Human Immunodeficiency Virus; HIV/AIDS, Human Immunodeficiency Virus/Acquired Immunodeficiency Syndrome; HSROC, Hierarchical Summary Receiver Operating Characteristic; Ig, Immunoglobulin; IgG, Immunoglobulin G; IgM, Immunoglobulin M; IHA, Indirect Hemagglutination Assay; IIF, Indirect Immunofluorescence; ISAGA, Immunosorbent Agglutination Assay; LAMP, Loop-Mediated Isothermal Amplification; LFA, Lateral Flow Assay; LFD, Lateral Flow Dipstick; LFIA, Lateral Flow Immunoassay; LOD, Limit of Detection; MeSH, Medical Subject Headings; ML, Machine Learning; NA, Not Applicable; NAAT, Nucleic Acid Amplification Test; NR, Not Reported; N/S, Not Stated; OT, Ocular Toxoplasmosis; PCR, Polymerase Chain Reaction; POC, Point-of-Care; POCT, Point-of-Care Testing; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; PRISMA-DTA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses of Diagnostic Test Accuracy Studies; qPCR, Quantitative Polymerase Chain Reaction; QUADAS-2, Quality Assessment of Diagnostic Accuracy Studies-2; RAA, Recombinase-Aided Amplification; RNA, Ribonucleic Acid; ROC, Receiver Operating Characteristic; ROP, Rhoptry Protein; SAG, Surface Antigen; SROC, Summary Receiver Operating Characteristic; STARD, Standards for Reporting Diagnostic Accuracy Studies; TN, True Negative; TP, True Positive; TPP, Target Product Profile; WHO, World Health Organization; ρ, Estimated correlation between logit sensitivity and logit specificity across studies; τ2, Between-study variance component (random-effects variance) in the bivariate model.
Data Sharing Statement
All data generated or analyzed during this study are included in this article. Further inquiries can be directed to the corresponding author.
Ethics Declarations
All analyses were based on previous published studies; thus, no ethical approval and patient consent are required.
Acknowledgments
The authors sincerely thank the ATOM Research Group and Universitas Brawijaya Library for their support, insights, and assistance in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by the Directorate of Research and Community Services, Universitas Brawijaya, through the Strategic Research Grants Initiation towards CoE scheme under grant number 989.I3/UN 10.C20/2023.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chu KB, Quan FS. Advances in Toxoplasma gondii vaccines: current strategies and challenges for vaccine development. Vaccines. 2021;9(5):1–31. doi:10.3390/vaccines9050413
2. Márquez-Mauricio A, Caballero-Ortega H, Gómez-Chávez F. Congenital toxoplasmosis diagnosis: current approaches and new insights. Acta Parasitol. 2023;68(3):473–480. doi:10.1007/s11686-023-00693-y
3. Suprianto D, Fitri LE, Sofia O, et al. The evolution of artificial intelligence in ocular toxoplasmosis detection: a scoping review on diagnostic models, data challenges, and future directions. Infect Dis Rep. 2025;17(6):1–26. doi:10.3390/idr17060148
4. Ramasubramanian V, Surendran R, Bansal N, et al. Endemic parasitic disease ‑ expert group opinion for South Asia for solid-organ transplantation − leishmaniasis, malaria, toxoplasmosis, filariasis, and strongyloidiasis. Indian J Transplant. 2022;16(5):S57–S62. doi:10.4103/ijot.ijot_117_21
5. McInnes MDF, Moher D, Thombs BD, McGrath TA, Bossuyt PM, Group and the PD. Preferred reporting items for a systematic review and meta-analysis of diagnostic test accuracy studies: the PRISMA-DTA statement. JAMA. 2018;319(4):388–396. doi:10.1001/jama.2017.19163
6. Binnicker MJ, Jespersen DJ, Harring JA. Multiplex detection of IgM and IgG class antibodies to Toxoplasma gondii, rubella virus, and cytomegalovirus using a novel multiplex flow immunoassay. Clin Vaccine Immunol. 2010;17(11):1734–1738. doi:10.1128/CVI.00332-10
7. Marilena CR, Felipe NG, Marisa TH, et al. Evaluation of an IgG avidity commercial test: contribution to diagnosis of primary infection caused by Toxoplasma gondii. Rev Chil Infectol. 2010;27(6):499–504.
8. Holec-Gasior L, Kur J. Toxoplasma gondii: recombinant GRA5 antigen for detection of immunoglobulin G antibodies using enzyme-linked immunosorbent assay. Exp Parasitol. 2010;124(3):272–278. doi:10.1016/j.exppara.2009.10.010
9. Lau YL, Meganathan P, Sonaimuthu P, Thiruvengadam G, Nissapatorn V, Chen Y. Specific, sensitive, and rapid diagnosis of active toxoplasmosis by a loop-mediated isothermal amplification method using blood samples from patients. J Clin Microbiol. 2010;48(10):3698–3702. doi:10.1128/JCM.00462-10
10. Machado AS, Andrade GMQ, Januário JN, et al. IgG and IgM Western blot assay for diagnosis of congenital toxoplasmosis. Mem Inst Oswaldo Cruz. 2010;105(6):757–761. doi:10.1590/S0074-02762010000600005
11. Prusa AR, Hayde M, Unterasinger L, Pollak A, Herkner KR, Kasper DC. Evaluation of the Roche Elecsys Toxo IgG and IgM electrochemiluminescence immunoassay for the detection of gestational Toxoplasma infection. Diagn Microbiol Infect Dis. 2010;68(4):352–357. doi:10.1016/j.diagmicrobio.2010.07.011
12. Saraei M, Shojaee S, Esmaeli AR, Jahani-Hashemi H, Keshavarz H. Evaluation of confounders in toxoplasmosis indirect fluorescent antibody assay. Iran J Parasitol. 2010;5(4):55–62.
13. Liang L, Döşkaya M, Juarez S, et al. Identification of potential serodiagnostic and subunit vaccine antigens by antibody profiling of toxoplasmosis cases in Turkey. Mol Cell Proteomics. 2011;10(7). doi:10.1074/mcp.M110.006916
14. Okusaga O, Langenberg P, Sleemi A, et al. Toxoplasma gondii antibody titers and history of suicide attempts in patients with schizophrenia. Schizophr Res. 2011;133(1):150–155. doi:10.1016/j.schres.2011.08.006
15. Sugita S, Ogawa M, Inoue S, Shimizu N, Mochizuki M. Diagnosis of ocular toxoplasmosis by two polymerase chain reaction (PCR) examinations: qualitative multiplex and quantitative real-time. Jpn J Ophthalmol. 2011;55(5):495–501. doi:10.1007/s10384-011-0065-8
16. Busemann C, Ribback S, Zimmermann K, et al. Toxoplasmosis after allogeneic stem cell transplantation-a single centre experience. Ann Hematol. 2012;91(7):1081–1089. doi:10.1007/s00277-012-1406-5
17. Chiang E, Goldstein DA, Shapiro MJ, Mets MB. Branch retinal artery occlusion caused by toxoplasmosis in an adolescent. Case Rep Ophthalmol. 2012;3(3):333–338. doi:10.1159/000343262
18. Jalallou N, Bandehpour M, Khazan H, Haghighi A, Kazemi B. Evaluation of recombinant SAG1 protein for detection of Toxoplasma gondii specific immunoglobulin m by ELISA test. Iran J Parasitol. 2012;7(4):17–21.
19. Khammari I, Saghrouni F, Bougmiza I, et al. Evaluation of the immunoblotting for the detection of immunoglobulin G Toxoplasma antibodies in immunocompetent patients. Pathol Biol. 2012;60(3):160–165. doi:10.1016/j.patbio.2011.02.003
20. Selseleh M, Keshavarz H, Mohebali M, et al. Production and evaluation of Toxoplasma gondii recombinant GRA7 for serodiagnosis of human infections. Korean J Parasitol. 2012;50(3):233–238. doi:10.3347/kjp.2012.50.3.233
21. Silva-dos-Santos PP, Barros GB, Mineo JR, et al. Flow cytometry-based algorithm to analyze the anti-fixed Toxoplasma gondii tachyzoites IgM and IgG reactivity and diagnose human acute toxoplasmosis. J Immunol Methods. 2012;378(1–2):33–43. doi:10.1016/j.jim.2012.02.001
22. Villard O, Cimon B, Franck J, et al. Evaluation of the usefulness of six commercial agglutination assays for serologic diagnosis of toxoplasmosis. Diagn Microbiol Infect Dis. 2012;73(3):231–235. doi:10.1016/j.diagmicrobio.2012.03.014
23. Asai T. The diagnosis of toxoplasmic encephalitis by polymerase chain reaction. Clin Neurol. 2013;53(11):1194–1195. doi:10.5692/clinicalneurol.53.1194
24. Bhattacharyya S, Khurana S, Dubey M. Anti-Toxoplasma gondii antibody detection in serum and urine samples by enzyme-linked immunosorbent assay in HIV-infected patients. Indian J Pathol Microbiol. 2013;56(1):20–23. doi:10.4103/0377-4929.116143
25. Chemoh W, Sawangjaroen N, Nissapatorn V, et al. Toxoplasma gondii infection: what is the real situation? Exp Parasitol. 2013;135(4):685–689. doi:10.1016/j.exppara.2013.10.001
26. fang DJ, Jiang M, li QL, et al. Toxoplasma gondii: enzyme-linked immunosorbent assay based on a recombinant multi-epitope peptide for distinguishing recent from past infection in human sera. Exp Parasitol. 2013;133(1):95–100. doi:10.1016/j.exppara.2012.10.016
27. Deshpande PS, Kotresha D, Noordin R, et al. IgG avidity Western blot using Toxoplasma gondii rGRA-7 cloned from nucleotides 39-711 for serodiagnosis of acute toxoplasmosis. Rev Inst Med Trop Sao Paulo. 2013;55(2):79–83. doi:10.1590/S0036-46652013000200003
28. Khammari I, Saghrouni F, Yaacoub A, et al. IgG Western Blot for confirmatory diagnosis of equivocal cases of toxoplasmosis by EIA-IgG and fluorescent antibody test. KOREAN J Parasitol. 2013;51(4):485–488. doi:10.3347/kjp.2013.51.4.485
29. Mikita K, Maeda T, Ono T, Miyahira Y, Asai T, Kawana A. The utility of cerebrospinal fluid for the molecular diagnosis of toxoplasmic encephalitis. Diagn Microbiol Infect Dis. 2013;75(2):155–159. doi:10.1016/j.diagmicrobio.2012.10.015
30. Murat JB, Dard C, Hidalgo HF, Dardé ML, Brenier-Pinchart MP, Pelloux H. Comparison of the Vidas system and two recent fully automated assays for diagnosis and follow-up of toxoplasmosis in pregnant women and newborns. Clin Vaccine Immunol. 2013;20(8):1203–1212. doi:10.1128/CVI.00089-13
31. Prusa AR, Kasper DC, Olischar M, Husslein P, Pollak A, Hayde M. Evaluation of serological prenatal screening to detect Toxoplasma gondii infections in Austria. Neonatology. 2012;103(1):27–34. doi:10.1159/000342625
32. Song KJ, Yang Z, Chong CK, et al. A rapid diagnostic test for toxoplasmosis using recombinant antigenic N-terminal half of SAG1 linked with intrinsically unstructured domain of GRA2 protein. Korean J Parasitol. 2013;51(5):503–509. doi:10.3347/kjp.2013.51.5.503
33. Villard O, Breit L, Cimon B, et al. Comparison of four commercially available avidity tests for Toxoplasma gondii-specific IgG antibodies. Clin Vaccine Immunol. 2013;20(2):197–204. doi:10.1128/CVI.00356-12
34. Caballero-Ortega H, Castillo-Cruz R, Murrieta S, et al. Diagnostic-test evaluation of immunoassays for anti-Toxoplasma gondii IgG antibodies in a random sample of Mexican population. J Infect Dev Ctries. 2014;8(5):642–647. doi:10.3855/jidc.3858
35. Khammari I, Saghrouni F, Lakhal S, Bouratbine A, Ben Said M, Boukadida J. A new IgG immunoblot kit for diagnosis of toxoplasmosis in pregnant women. Korean J Parasitol. 2014;52(5):493–499. doi:10.3347/kjp.2014.52.5.493
36. Ogouyèmi-Hounto A, Agbayahoun-Chokki F, Sissinto Savi De Tove Y, et al. Evaluation of a rapid diagnostic test in the diagnosis of toxoplasmosis in pregnant women in Cotonou (Bénin). Bull la Soc Pathol Exot. 2014;107(2):85–89. doi:10.1007/s13149-014-0355-8
37. Varlet-Marie E, Sterkers Y, Brenier-Pinchart MP, et al. Characterization and multicentric validation of a common standard for Toxoplasma gondii detection using nucleic acid amplification assays. J Clin Microbiol. 2014;52(11):3952–3959. doi:10.1128/JCM.01906-14
38. Blay EA, Ghansah A, Otchere J, et al. Congenital toxoplasmosis and pregnancy malaria detection post-partum: effective diagnosis and its implication for efficient management of congenital infection. Parasitol Int. 2015;64(6):603–608. doi:10.1016/j.parint.2015.08.004
39. Capobiango JD, Pagliari S, Pasquali AKS, et al. Evaluation of a recombinant rhoptry protein 2 enzyme-linked immunoassay for the diagnosis of toxoplasmosis acquired during pregnancy. Mem Inst Oswaldo Cruz. 2015;110(6):732–738. doi:10.1590/0074-02760150069
40. Filisetti D, Sterkers Y, Brenier-Pinchart MP, et al. Multicentric Comparative assessment of the bio-evolution Toxoplasma gondii detection kit with eight laboratory-developed PCR assays for molecular diagnosis of congenital toxoplasmosis. J Clin Microbiol. 2015;53(1):29–34. doi:10.1128/JCM.01913-14
41. Hallur V, Sehgal R, Khurana S. Development of touch down-multiplex PCR for the diagnosis of toxoplasmosis. Indian J Med Microbiol. 2015;33(2):271–273. doi:10.4103/0255-0857.154874
42. Li XX, Zhang QL, Hou P, et al. Gold magnetic nanoparticle conjugate-based lateral flow assay for the detection of IgM class antibodies related to TORCH infections. Int J Mol Med. 2015;36(5):1319–1326. doi:10.3892/ijmm.2015.2333
43. Previato M, Frederico FB, Murata FHA, et al. A Brazilian report using serological and molecular diagnosis to monitoring acute ocular toxoplasmosis. BMC Res Notes. 2015;8:746. doi:10.1186/s13104-015-1650-6
44. Prusa AR, Kasper DC, Pollak A, Olischar M, Gleiss A, Hayde M. Amniocentesis for the detection of congenital toxoplasmosis: results from the nationwide Austrian prenatal screening program. Clin Microbiol Infect. 2015;21(2):191.e1–191.e8. doi:10.1016/j.cmi.2014.09.018
45. Robert-Gangneux F, Sterkers Y, Yera H, et al. Molecular diagnosis of toxoplasmosis in immunocompromised patients: a 3-year multicenter retrospective study. J Clin Microbiol. 2015;53(5):1677–1684. doi:10.1128/JCM.03282-14
46. Rodrigues JP, Andrade HF. Efficient duplex solid-phase fluorescent assay (dFISA) for the simultaneous detection of specific anti-T. gondii IgG and IgM due to refined conjugates. J Immunol Methods. 2015;420:11–17. doi:10.1016/j.jim.2015.03.007
47. Arab-Mazar Z, Fallahi S, Koochaki A, Haghighi A, Seyyed Tabaei SJ. Immunodiagnosis and molecular validation of Toxoplasma gondii-recombinant dense granular (GRA) 7 protein for the detection of toxoplasmosis in patients with cancer. Microbiol Res. 2016;183:53–59. doi:10.1016/j.micres.2015.11.006
48. Avci ME, Arslan F, Çiftçi Ş, et al. Role of spiramycin in prevention of fetal toxoplasmosis. J Matern neonatal Med Off J Eur Assoc Perinat Med Fed Asia Ocean Perinat Soc Int Soc Perinat Obstet. 2016;29(13):2073–2076. doi:10.3109/14767058.2015.1074998
49. Costa JG, Peretti LE, García VS, et al. P35 and P22 Toxoplasma gondii antigens abbreviate regions to diagnose acquired toxoplasmosis during pregnancy: toward single-sample assays. Clin Chem Lab Med. 2017;55(4):595–604. doi:10.1515/cclm-2016-0331
50. de Oliveira GB, da Silva MAL, Wanderley LB, et al. Cerebral toxoplasmosis in patients with acquired immune deficiency syndrome in the neurological emergency department of a tertiary hospital. Clin Neurol Neurosurg. 2016;150:23–26. doi:10.1016/j.clineuro.2016.08.014
51. El-Bali M, Zaglool DAM, Khodari YAW, Al-Harthi SA. Appraisal of prenatal anti-Toxoplasma gondii (IgG+IgM)- IHA/IgM-Elisa screening in single samples via IgG avidity test. J Egypt Soc Parasitol. 2016;46(1):201–208. doi:10.12816/0026165
52. Yun F, Hui-Fang L, Min-Yuan S. Investigation on Toxoplasma gondii infection and awareness of toxoplasmosis-related knowledge in women with poor pregnant outcomes in Wuxi City. Zhongguo Xue Xi Chong Bing Fang Zhi Za Zhi. 2016;28(6):664–668. doi:10.16250/j.32.1374.2016244
53. Mohammadpour N, Saki J, Rafiei A, Khodadadi A, Tavalla M, Cheraghian B. Design of indigenous elisa using tachyzoites from the rh strain of Toxoplasma gondii and comparison with commercial kits in ahvaz, Southwest of Iran, 2015. Jundishapur J Microbiol. 2016;9(10). doi:10.5812/jjm.36666
54. Poltavchenko AG, V NO, V FP, V EA, Gureyev VN. Multiplex method for initial complex testing of antibodies to blood transmitted diseases agents. J Virol Methods. 2016;236:231–236. doi:10.1016/j.jviromet.2016.08.003
55. Sroka J, Wójcik-Fatla A, Zając V, et al. Comparison of the efficiency of two commercial kits – ELFA and Western blot in estimating the phase of Toxoplasma gondii infection in pregnant women. Ann Agric Environ Med. 2016;23(4):570–575. doi:10.5604/12321966.1226848
56. Stajner T, Bobic B, Klun I, et al. Prenatal and Early Postnatal Diagnosis of Congenital Toxoplasmosis in a Setting With No Systematic Screening in Pregnancy. Medicine. 2016;95(9):e2979. doi:10.1097/MD.0000000000002979
57. Armengol C, Cassaing S, Roques-Malecaze C, et al. Time before anti-Toxoplasma IgG seroconversion detection by 7 commercial assays in French pregnant women. Diagn Microbiol Infect Dis. 2017;87(2):103–107. doi:10.1016/j.diagmicrobio.2016.10.020
58. Barros GB, Lemos EM, e Silva-dos-Santos PP, et al. Proposed panel of diagnostic tools for accurate temporal classification of symptomatic T. gondii infection. J Immunol Methods. 2017;451:61–70. doi:10.1016/j.jim.2017.08.010
59. Begeman IJ, Lykins J, Zhou Y, et al. Point-of-care testing for Toxoplasma gondii IgG/IgM using Toxoplasma ICT IgG-IgM test with sera from the United States and implications for developing countries. PLoS Negl Trop Dis. 2017;11(6). doi:10.1371/journal.pntd.0005670
60. Berredjem H, Aouras H, Benlaifa M, Becheker I, Djebar MR. Contribution of IgG avidity and PCR for the early diagnosis of toxoplasmosis in pregnant women from the North-Eastern region of Algeria. Afr Health Sci. 2017;17(3):647–656. doi:10.4314/ahs.v17i3.7
61. Chapey E, Wallon M, Peyron F. Evaluation of the LDBIO point of care test for the combined detection of toxoplasmic IgG and IgM. Clin Chim Acta. 2017;464:200–201. doi:10.1016/j.cca.2016.10.023
62. Laboudi M, Sadak A. Serodiagnosis of toxoplasmosis: the effect of measurement of IgG avidity in pregnant women in Rabat in Morocco. Acta Trop. 2017;172:139–142. doi:10.1016/j.actatropica.2017.04.008
63. Matin S, Shahbazi G, Namin ST, Moradpour R, Feizi F, Piri-Dogahe H. Comparison of Placenta PCR and maternal serology of aborted women for detection of Toxoplasma gondii in Ardabil, Iran. Korean J Parasitol. 2017;55(6):607–611. doi:10.3347/kjp.2017.55.6.607
64. Mazzu-Nascimento T, Morbioli GG, Milan LA, et al. Improved assessment of accuracy and performance indicators in paper-based ELISA. Anal Methods. 2017;9(18):2644–2653. doi:10.1039/c7ay00505a
65. Murata FHA, Ferreira MN, Pereira-Chioccola VL, et al. Evaluation of serological and molecular tests used to identify Toxoplasma gondii infection in pregnant women attended in a public health service in São Paulo state, Brazil. Diagn Microbiol Infect Dis. 2017;89(1):13–19. doi:10.1016/j.diagmicrobio.2017.06.004
66. Naghili B, Abbasalizadeh S, Tabrizi S, et al. Comparison of IIF, ELISA and IgG avidity tests for the detection of anti-Toxoplasma antibodies in single serum sample from pregnant women. Le Infez Med. 2017;25(1):50–56.
67. Peretti LE, Gonzalez VDG, Marcipar IS, Gugliotta LM. Diagnosis of toxoplasmosis in pregnancy. Evaluation of latex-protein complexes by immnunoagglutination. Parasitology. 2017;144(8):1073–1078. doi:10.1017/S0031182017000294
68. Robert-Gangneux F, Brenier-Pinchart MP, Yera H, et al. Evaluation of Toxoplasma ELITe MGB real-time PCR assay for diagnosis of toxoplasmosis. J Clin Microbiol. 2017;55(5):1369–1376. doi:10.1128/JCM.02379-16
69. Sun XM, Ji YS, Liu XY, et al. Improvement and evaluation of loop-mediated isothermal amplification for rapid detection of Toxoplasma gondii infection in human blood samples. PLoS One. 2017;12(1). doi:10.1371/journal.pone.0169125
70. Zacche-Tonini AD, Fonseca GSF, de Jesus L, et al. Establishing tools for early diagnosis of congenital toxoplasmosis: flow cytometric IgG avidity assay as a confirmatory test for neonatal screening. J Immunol Methods. 2017;451:37–47. doi:10.1016/j.jim.2017.08.005
71. Zhang K, Lin G, Han Y, Li J. The standardization of 5 immunoassays for anti-Toxoplasma immunoglobulin G(IgG). Clin Chim Acta. 2017;472:20–25. doi:10.1016/j.cca.2017.07.007
72. AA AEA, Nahnoush RK, Elmallawany MA, El-Sherbiny WS, Badr MS, Nasr GM. Isothermal PCR for feasible molecular diagnosis of primary toxoplasmosis in women recently experienced spontaneous abortion. Open Access Maced J Med Sci. 2018;6(6):982–987. doi:10.3889/oamjms.2018.227
73. Aly I, Taher EE, El Nain G, et al. Advantages of bioconjugated silica-coated nanoparticles as an innovative diagnosis for human toxoplasmosis. Acta Trop. 2018;177:19–24. doi:10.1016/j.actatropica.2017.09.024
74. Barakat AMA, Ahmed SO, Zaki MS, et al. New approach to differentiate primary from latent Toxoplasma gondii abortion through immunoglobulin and DNA interpretation. Microb Pathog. 2018;125:66–71. doi:10.1016/j.micpath.2018.09.001
75. Bispo PJM, Davoudi S, Sahm ML, et al. Rapid detection and identification of uveitis pathogens by qualitative multiplex real-time PCR. Invest Ophthalmol Vis Sci. 2018;59(1):582–589. doi:10.1167/iovs.17-22597
76. Boudaouara Y, Aoun K, Maatoug R, Souissi O, Bouratbine A, Ben AR. Congenital Toxoplasmosis in Tunisia: prenatal and Neonatal Diagnosis and Postnatal Follow-up of 35 Cases. Am J Trop Med Hyg. 2018;98(6):1722–1726. doi:10.4269/ajtmh.17-0580
77. Carral L Á, Kaufer F, Pardini L, et al. Congenital toxoplasmosis: serology, PCR, parasite isolation and molecular characterization of Toxoplasma gondii. Rev Chil Infectol. 2018;35(1):36–40. doi:10.4067/s0716-10182018000100036
78. Tanrıverdi E Ç, Kadıoğlu B G, Alay H, Özkurt Z. Retrospective evaluation of anti-Toxoplasma gondii antibody among first trimester pregnant women admitted to Nenehatun Maternity Hospital between 2013-2017 in Erzurum. Turkiye parazitolojii Derg. 2018;42(2):101–105. doi:10.5152/tpd.2018.5544
79. Masini G, Maggio L, Marchi L, et al. Isolated fetal echogenic bowel in a retrospective cohort: the role of infection screening. Eur J Obstet Gynecol Reprod Biol. 2018;231:136–141. doi:10.1016/j.ejogrb.2018.10.017
80. Roiko MS, LaFavers K, Leland D, Arrizabalaga G. Toxoplasma gondii-positive human sera recognise intracellular tachyzoites and bradyzoites with diverse patterns of immunoreactivity. Int J Parasitol. 2018;48(3):225–232. doi:10.1016/j.ijpara.2017.08.016
81. Sardarian K, Maghsood AH, Farimani M, et al. Detection of Toxoplasma gondii B1 gene in placenta does not prove congenital toxoplasmosis. Hum Antibodies. 2019;27(1):31–35. doi:10.3233/HAB-180346
82. Varlet-Marie E, Sterkers Y, Perrotte M, Bastien P. A new LAMP-based assay for the molecular diagnosis of toxoplasmosis: comparison with a proficient PCR assay. Int J Parasitol. 2018;48(6):457–462. doi:10.1016/j.ijpara.2017.11.005
83. Boquel F, Monpierre L, Imbert S, et al. Interpretation of very low avidity indices acquired with the Liaison XL Toxo IgG avidity assay in dating toxoplasmosis infection. Eur J Clin Microbiol Infect Dis off Publ Eur Soc Clin Microbiol. 2019;38(2):253–257. doi:10.1007/s10096-018-3421-5
84. Botein EF, Darwish A, El-Tantawy NL, El-Baz R, Eid MI, Shaltot AM. Serological and molecular screening of umbilical cord blood for Toxoplasma gondii infection. Transpl Infect Dis Off J Transplant Soc. 2019;21(4):e13117. doi:10.1111/tid.13117
85. Döşkaya M, Pullukçu H, Karakavuk M, et al. Comparison of an in house and a commercial real-time polymerase chain reaction targeting Toxoplasma gondii RE gene using various samples collected from patients in Turkey. BMC Infect Dis. 2019;19(1):1042. doi:10.1186/s12879-019-4666-z
86. Douet T, Armengol C, Charpentier E, et al. Performance of seven commercial automated assays for the detection of low levels of anti-Toxoplasma IgG in French immunocompromised patients. Parasite. 2019;26:51. doi:10.1051/parasite/2019052
87. Hanifehpour H, Samsam Shariat SK, Ghafari MS, Kheirandish F, Saber V, Fallahi S. Serological and molecular diagnosis of Toxoplasma gondii infections in thalassemia patients. Iran J Parasitol. 2019;14(1):20–28. doi:10.18502/ijpa.v14i1.714
88. Lévêque MF, Chiffré D, Galtier C, et al. Molecular diagnosis of toxoplasmosis at the onset of symptomatic primary infection: a straightforward alternative to serological examinations. Int J Infect Dis. 2019;79:131–133. doi:10.1016/j.ijid.2018.11.368
89. Martins HDD, Vaz BAS, da Silva Lins LS, Gondim BLC, Castellano LRC, Bonan PRF. Intraparotid lymph node toxoplasmosis diagnosis by fine needle aspiration cytology. J Oral Maxillofac Surgery, Med Pathol. 2019;31(5):369–371. doi:10.1016/j.ajoms.2019.04.003
90. Medawar-Aguilar V, Jofre CF, Fernández-Baldo MA, et al. Serological diagnosis of Toxoplasmosis disease using a fluorescent immunosensor with chitosan-ZnO-nanoparticles. Anal Biochem. 2019;564-565(December 2017):116–122. doi:10.1016/j.ab.2018.10.025
91. Moghaddas E, Hosseini SM, Sharifi K, et al. IgG avidity test for ocular toxoplasmosis diagnosis at a Tertiary Center, Northeast of Iran. Iran J Immunol. 2019;16(3):258–264. doi:10.22034/IJI.2019.80276
92. Morovati H, Seyyed Tabaei SG, Gholamzad M, et al. Development of a lateral flow immunoassay using recombinant dense granular antigen (GRA) 7 to detect anti-Toxoplasma gondii IgG antibodies. Arch Razi Inst. 2019;74(1):39–49.
93. Olariu TR, Blackburn BG, Press C, Talucod J, Remington JS, Montoya JG. Role of toxoplasma IgA as part of a reference panel for the diagnosis of acute toxoplasmosis during pregnancy. J Clin Microbiol. 2019;57(2). doi:10.1128/JCM.01357-18
94. Rahimi Esboei B, Kazemi B, Zarei M, et al. Evaluation of RE and B1 genes as targets for detection of Toxoplasma gondii by nested PCR in blood samples of patients with ocular toxoplasmosis. Acta Parasitol. 2019;64(2):384–389. doi:10.2478/s11686-019-00056-6
95. Takara EA, V PS, Scala-Benuzzi ML, Fernández-Baldo MA, Raba J, Messina GA. Novel electrochemical sensing platform based on a nanocomposite of PVA/PVP/RGO applied to IgG anti- Toxoplasma gondii antibodies quantitation. Talanta. 2019;195:699–705. doi:10.1016/j.talanta.2018.11.070
96. Thangarajah P, Hajissa K, Wong WK, Abdullah MA, Ismail N, Mohamed Z. Usefulness of paired samples for the Serodiagnosis of toxoplasmosis infection in a tertiary teaching Hospital in Malaysia. BMC Infect Dis. 2019;19(1):202. doi:10.1186/s12879-019-3830-9
97. Vargas-Montes M, Cardona N, Moncada DM, Molina DA, Zhang Y, Gómez-Marín JE. Enzyme-Linked Aptamer Assay (ELAA) for detection of Toxoplasma ROP18 protein in human serum. Front Cell Infect Microbiol. 2019;9. doi:10.3389/fcimb.2019.00386
98. Wassef R, Abdel-Malek R. Validity of a new immunochromatographic test in detection of Toxoplasma gondii in cancer patients. J Parasit Dis. 2019;43(1):83–86. doi:10.1007/s12639-018-1063-2
99. Ahmedani EI, Elagib AA, Mohamed K, et al. Detection of Toxoplasma gondii by loop-mediated isothermal amplification in blood and urine samples from women, Saudi Arabia. J Clin Diagnostics Res. 2020;14(9). doi:10.7860/JCDR/2020/44550.14026
100. Ammar NA, Yera H, Bigot J, Botterel F, Hennequin C, Guitard J. Multicentric evaluation of the bio-evolution Toxoplasma gondii assay for the detection of Toxoplasma DNA in immunocompromised patients. J Clin Microbiol. 2020;58(2). doi:10.1128/JCM.01231-19
101. Brandão-de-resende C, Santos HH, Rojas Lagos AA, et al. Clinical and multimodal imaging findings and risk factors for ocular involvement in a presumed waterborne toxoplasmosis outbreak, Brazil1. Emerg Infect Dis. 2020;26(12):2922–2932. doi:10.3201/EID2612.200227
102. Chiquet C, Chumpitazi B, Vilgrain I, et al. Prospective study of serum and aqueous humour anti-Hsp70.1 IgG antibody levels in ocular toxoplasmosis. Parasite Immunol. 2020;42(10). doi:10.1111/pim.12771
103. de Oliveira Dias JR, Campelo C, Novais EA, et al. New findings useful for clinical practice using swept-source optical coherence tomography angiography in the follow-up of active ocular toxoplasmosis. Int J Retin Vitr. 2020;6:1–10. doi:10.1186/s40942-020-00231-2
104. Echeverri D, Garg M, Varón Silva D, Orozco J. Phosphoglycan-sensitized platform for specific detection of anti-glycan IgG and IgM antibodies in serum. Talanta. 2020;217:121117. doi:10.1016/j.talanta.2020.121117
105. Ferra B, Holec-Gąsior L, Gatkowska J, Dziadek B, Dzitko K. Toxoplasma gondii recombinant antigen AMA1: diagnostic utility of protein fragments for the detection of IgG and IgM antibodies. Pathogens. 2020;9(1). doi:10.3390/pathogens9010043
106. Hegazy MM, Hegazy MK, Azab MS, Nabih N. Validation of dried blood spots in monitoring toxoplasmosis. Pathog Glob Health. 2020;114(5):242–250. doi:10.1080/20477724.2020.1765125
107. Leroy J, Houzé S, Dardé ML, et al. Severe toxoplasmosis imported from tropical Africa in immunocompetent patients: a case series. Travel Med Infect Dis. 2020;35:101509. doi:10.1016/j.tmaid.2019.101509
108. Khamsi HM, Javad SS, Gholamzad M. Evaluation of a newly designed immunochromatographic test using Gold nanoparticles and recombinant antigen gra7 for rapid diagnosis of human toxoplasmosis. Iran J Med Microbiol. 2020;14(1):101–115. doi:10.30699/ijmm.14.1.101
109. Ozcelik S, Alim M, Ozpinar N. Detection of Toxoplasma gondii infection among diabetic patients in Turkey. Clin Epidemiol Glob Heal. 2020;8(3):899–902. doi:10.1016/j.cegh.2020.02.020
110. Pomares C, Estran R, Press CJ, et al. Is real-time PCR targeting rep 529 suitable for diagnosis of toxoplasmosis in patients infected with non-type II strains in North America? J Clin Microbiol. 2020;58(2). doi:10.1128/JCM.01223-19
111. Simon L, Fillaux J, Guigon A, et al. Serological diagnosis of Toxoplasma gondii: analysis of false-positive IgG results and implications. Parasite. 2020;27:7. doi:10.1051/parasite/2020006
112. Soltani Tehrani B, Mirzajani E, Fallahi S, et al. Challenging TaqMan probe-based real-time PCR and loop-mediated isothermal amplification (LAMP): the two sensitive molecular techniques for the detection of toxoplasmosis, a potentially dangerous opportunistic infection in immunocompromised patients. Arch Microbiol. 2020;202(7):1881–1888. doi:10.1007/s00203-020-01903-1
113. Wang Y, Hedman L, Nurmi V, et al. Microsphere-based IgM and IgG avidity assays for human Parvovirus B19, human cytomegalovirus, and Toxoplasma gondii. mSphere. 2020;5(2). doi:10.1128/mSphere.00905-19
114. Ybañez RHD, Nishikawa Y. Serological detection of T. gondii infection in humans using an immunochromatographic assay based on dense granule protein 7. Parasitol Int. 2020;76. doi:10.1016/j.parint.2020.102089
115. Rym BA, Yasmine K, Hedia B, et al. Contribution of the Toxoplasma ICT IgG IgM(®) test in determining the immune status of pregnant women against toxoplasmosis. J Clin Lab Anal. 2021;35(5):e23749. doi:10.1002/jcla.23749
116. Brenier-Pinchart MP, Robert-Gangneux F, Accoceberry I, et al. Multicenter comparative assessment of the TIB MolBiol Toxoplasma gondii detection kit and four laboratory-developed PCR assays for molecular diagnosis of toxoplasmosis. J Mol Diagn. 2021;23(8):1000–1006. doi:10.1016/j.jmoldx.2021.05.010
117. El Mansouri B, Amarir F, Peyron F, et al. High performance of a novel point-of-care blood test for Toxoplasma infection in women from diverse regions of Morocco. Emerg Microbes Infect. 2021;10(1):1675–1682. doi:10.1080/22221751.2021.1948359
118. El-Sayad MH, Salem AI, Fazary H, Alzainny HN, Abd El-Latif NF. Detection of toxoplasmosis in aborted women in Alexandria, Egypt using ELISA and PCR. J Parasit Dis off Organ Indian Soc Parasitol. 2021;45(2):539–545. doi:10.1007/s12639-020-01327-0
119. Hashemi SM, Mahmoodi S, Mehravaran A, et al. Serological and molecular evaluation of toxoplasmosis in patient undergoing chemotherapy for malignancies in southeast of Iran. Gene Rep. 2021:23. doi:10.1016/j.genrep.2021.101163
120. Pour EK, Riazi-Esfahani H, Ebrahimiadib N, Esteghamati VZ, Zarei M. Acquired immunodeficiency syndrome presented as atypical ocular toxoplasmosis. Case Rep Ophthalmol Med. 2021;2021. doi:10.1155/2021/5512408
121. Kheirandish F, Fallahi S, Mahmoudvand H, et al. A loop-mediated isothermal amplification (LAMP) assay for detection of Toxoplasma gondii infection in women with spontaneous abortion. Arch Microbiol. 2021;203(2):763–769. doi:10.1007/s00203-020-02081-w
122. Lijeskić O, Štajner T, Srbljanović J, et al. Postnatal ocular toxoplasmosis in immunocompetent patients. J Infect Dev Ctries. 2021;15(10):1515–1522. doi:10.3855/jidc.14824
123. Logroño Wiese PE, Seeber F, Endres AS, Brockmann C, Pleyer U. Screening for common eye diseases in the elderly with Optos ultra-wide-field scanning laser ophthalmoscopy: a pilot study with focus on ocular toxoplasmosis. Int Ophthalmol. 2021;41(5):1573–1584. doi:10.1007/s10792-020-01683-z
124. Mirahmadi H, Nozari B, Raissi V, Alijani E, Etemadi S. Frequency and parasite load of Toxoplasma gondii in hemodialysis patients based on RE gene by real-time PCR. Gene Rep. 2021;23. doi:10.1016/j.genrep.2021.101145
125. Nourrisson C, Moniot M, Poirier P, Sterkers Y. Evaluation of two commercial kits on the automated ELITe InGenius PCR platform for molecular diagnosis of toxoplasmosis. J Mol Diagn. 2021;23(7):865–871. doi:10.1016/j.jmoldx.2021.04.004
126. Parra R, Ojeda V, Vázquez Noguera JL, et al. Automatic diagnosis of ocular toxoplasmosis from fundus images with residual neural networks. Stud Health Technol Inform. 2021;281:173–177. doi:10.3233/SHTI210143
127. Safarpour H, Pourhassan-Moghaddam M, Spotin A, et al. A novel enhanced dot blot immunoassay using colorimetric biosensor for detection of Toxoplasma gondii infection. Comp Immunol Microbiol Infect Dis. 2021:79. doi:10.1016/j.cimid.2021.101708
128. Sousa S, Castro A, Da Costa JMC, Pereira E. Biosensor based immunoassay: a new approach for serotyping of Toxoplasma gondii. Nanomaterials. 2021;11(8). doi:10.3390/nano11082065
129. de SJY, Gomes TC, Rezende HHA, Storchilo HR, Rodrigues PG, de CAM. IgG avidity in samples collected on filter paper: importance of the early diagnosis of congenital toxoplasmosis. Rev Bras Ginecol e Obstet Rev da Fed Bras Das Soc Ginecol e Obstet. 2021;43(12):887–893. doi:10.1055/s-0041-1740272
130. Steinberg HE, Bowman NM, Diestra A, et al. Detection of toxoplasmic encephalitis in HIV positive patients in urine with hydrogel nanoparticles. PLoS Negl Trop Dis. 2021;15(3). doi:10.1371/journal.pntd.0009199
131. Jabs DA, Belfort R, Bodaghi B, et al. Classification criteria for Toxoplasmic retinitis. Am J Ophthalmol. 2021;228:134–141. doi:10.1016/j.ajo.2021.03.042
132. Trotta M, Trotta A, Spataro E, et al. Primary toxoplasmosis acquired during early pregnancy: is it currently overestimated? Eur J Obstet Gynecol Reprod Biol. 2021;267:285–289. doi:10.1016/j.ejogrb.2021.11.019
133. Wu Y, Wang F, Wang C, et al. Detection of Pneumocystis jirovecii and Toxoplasma gondii in patients with lung infections by a duplex qPCR assay. PLoS Negl Trop Dis. 2021;15(12). doi:10.1371/journal.pntd.0010025
134. Zhao J. A novel rapid visual detection of Toxoplasma gondii by combining recombinase polymerase amplification and lateral flow dipstick coupled with CRISPR-Cas13a fluorescence (RAA-Cas13a-LFD). Parasite. 2022;29:21. doi:10.1051/parasite/2022021
135. Aerts R, Mercier T, Beckers M, Schoemans H, Lagrou K, Maertens J. Toxoplasmosis after allogeneic haematopoietic cell transplantation: experience using a PCR-guided pre-emptive approach. Clin Microbiol Infect. 2022;28(3):440–445. doi:10.1016/j.cmi.2021.09.033
136. Azimi A, Parsaei M, Soleymani E, Mehranzadeh E, Maghsood AH. Diagnosis of acute toxoplasmosis in the first trimester of pregnancy by IgG avidity. Avicenna J Clin Med. 2022;29(1):50–56. doi:10.52547/ajcm.29.1.50
137. Brenier-Pinchart MP, Filisetti D, Cassaing S, et al. Molecular diagnosis of Toxoplasmosis: multicenter evaluation of the Toxoplasma RealCycler Universal PCR assay on 168 characterized human samples. J Mol Diagn. 2022;24(6):687–696. doi:10.1016/j.jmoldx.2022.03.009
138. Jean-Pierre V, Miozzo J, Fricker-Hidalgo H, et al. Serological diagnosis of toxoplasmosis: evaluation of the commercial test recomLine Toxoplasma IgG immunoblot (Mikrogen) based on recombinant antigens. Parasite. 2022;29:52. doi:10.1051/parasite/2022050
139. Kim MJ, Chu KB, Mao J, et al. Recombinant AMA1 virus-like particle antigen for serodiagnosis of Toxoplasma gondii infection. Biomedicines. 2022;10(11). doi:10.3390/biomedicines10112812
140. Ksiaa I, Khochtali S, Mefteh M, et al. Distinguishing swept-source optical coherence tomography findings in active toxoplasmic retinochoroiditis. Eye. 2022;36(6):1222–1230. doi:10.1038/s41433-021-01491-4
141. Lévêque MF, Albaba S, Arrada N, et al. Diagnosis of congenital toxoplasmosis: no benefit of IgA antibody detection by platelia ELISA in a tricentric evaluation. J Clin Microbiol. 2022;60(5):e0011622. doi:10.1128/jcm.00116-22
142. Meroni V, Genco F, Scudeller L, et al. Diagnostic accuracy of LDBIO-Toxo II IgG and IgM western blot in suspected seroconversion in pregnancy: a multicentre study. Pathogens. 2022;11(6). doi:10.3390/pathogens11060665
143. Mirahmadi H, Nozari B, Metanat M, et al. Evaluating the performance of LAMP diagnostic test in the detection of toxoplasmosis in hemodialysis patients. Gene Rep. 2022:26. doi:10.1016/j.genrep.2021.101430
144. Rodrigues JP, Junior HFA. Efficiency of a single well IgG, IgM and IgA Anti T. gondii fluorimetric assay for pre-natal screening for congenital toxoplasmosis. J Fluoresc. 2022;32(2):661–667. doi:10.1007/s10895-022-02892-8
145. Štajner T, Vujić D, Srbljanović J, et al. Risk of reactivated toxoplasmosis in haematopoietic stem cell transplant recipients: a prospective cohort study in a setting withholding prophylaxis. Clin Microbiol Infect. 2022;28(5):733.e1–733.e5. doi:10.1016/j.cmi.2021.09.012
146. Yéngué JF, Essomba CMN, Ndzengue GEA, et al. Performance of immunochromatographic and immunoenzymatic techniques in the diagnosis of toxoplasmosis in pregnant women in Cameroon: need for harmonization. Pan Afr Med J. 2022;43:195. doi:10.11604/pamj.2022.43.195.36996
147. Zhao J, Li Y, Xue Q, Zhu Z, Zou M, Fang F. A novel rapid visual detection assay for Toxoplasma gondii combining recombinase-Aided amplification and lateral flow dipstick coupled with CRISPR-Cas13a fluorescence (RAA-Cas13a-LFD). Parasite. 2022;29. doi:10.1051/parasite/2022021
148. Abraham S, Piarroux R, Zhou Y, et al. Performances of ICT Toxoplasma IgG-IgM test in comparison with Vidas® toxo competition to determine the immune status against Toxoplasma gondii. Eur J Clin Microbiol Infect Dis. 2023;42(11):1327–1335. doi:10.1007/s10096-023-04669-8
149. Aly NSM, Kim HS, Marei YM, et al. Diagnosis of toxoplasmosis using surface antigen grade 1 detection by ELISA, Nano-Gold ELISA, and PCR in pregnant women. Int J Nanomed. 2023;18:1335–1345. doi:10.2147/IJN.S401876
150. Cañedo-Solares I, Correa D, Luna-Pastén H, et al. Maternal anti-Toxoplasma gondii antibodies IgG2, IgG3 and IgG1 are markers of vertical transmission and clinical evolution of toxoplasmosis in the offspring. Acta Trop. 2023;243:106943. doi:10.1016/j.actatropica.2023.106943
151. Cardozo O, Ojeda V, Parra R, et al. Dataset of fundus images for the diagnosis of ocular toxoplasmosis. Data Br. 2023:48. doi:10.1016/j.dib.2023.109056
152. Dambrun M, Sare N, Vianou B, et al. Serological diagnosis of toxoplasmosis in pregnancy: comparison between a manual commercial ELISA assay and the automated VIDAS® kit. Eur J Clin Microbiol Infect Dis off Publ Eur Soc Clin Microbiol. 2023;42(6):759–769. doi:10.1007/s10096-023-04603-y
153. Dragomir A, Lupu MA, Lighezan R, Paduraru AA, Olariu TR. Toxoplasma gondii Infection in patients with cardiovascular diseases from Western Romania: a case–control study. Life. 2023;13(7):1575. doi:10.3390/life13071575
154. Hosseini SA, Sharif M, Sarvi S, et al. Identification and multilocus genotyping of Toxoplasma gondii isolates from congenital infection in north of Iran. Parasitol Res. 2023;122(1):177–184. doi:10.1007/s00436-022-07714-1
155. Londoño-Martinez JC, Velasco-Velasquez S, Cordero-Lopez S, et al. Evaluation of the acceptability of point of care diagnostic test for prenatal toxoplasmosis (translational research Phase III). J Infect Public Health. 2023;16(1):15–24. doi:10.1016/j.jiph.2022.11.023
156. Nabet C, Brossas JY, Poignon C, et al. Assessment of droplet digital PCR for the detection and absolute quantification of Toxoplasma gondii: a comparative retrospective study. J Mol Diagn. 2023;25(7):467–476. doi:10.1016/j.jmoldx.2023.03.006
157. Sofia O, Wahyudi INSA, Susianti H, Fitri LE, Prayitnaningsih S. Optical coherence tomography angiography findings in ocular toxoplasmosis with multiple recurrences. Int Med Case Rep J. 2023;16(January):35–43. doi:10.2147/IMCRJ.S395600
158. Abedian R, Esboei BR, Kordi S, et al. Efficacy of amniotic fluid, blood and urine samples for the diagnosis of toxoplasmosis in pregnant women candidates for amniocentesis using serological and molecular techniques. BMC Pregnancy Childbirth. 2024;24(1). doi:10.1186/s12884-024-06979-x
159. Aktas K. Presumed acute unilateral toxoplasma papillitis without vitritis: a case report. Eur Eye Res. 2024;4(3):233–236. doi:10.14744/eer.2024.05924
160. Cifuentes-González C, Rojas-Carabali W, Mejía-Salgado G, et al. is automated machine learning useful for ocular toxoplasmosis identification and classification of the inflammatory activity? AJO Int. 2024;1(4):1–7. doi:10.1016/j.ajoint.2024.100079
161. Datta P, Garg P, Rattan D, et al. Comparison of B1 and RE 529 gene targets by real time PCR and LAMP assay for diagnosis of toxoplasmosis in pregnant females. Indian J Med Microbiol. 2024:47. doi:10.1016/j.ijmmb.2023.100481
162. Deleplancque AS, Fricker-Hidalgo H, Pomares C, et al. Comparative performance of ISAGA IgM and ELISA assays for the diagnosis of maternal and congenital Toxoplasma infections: which technique could replace ISAGA IgM? Parasite. 2024;31:7. doi:10.1051/parasite/2024004
163. Eraghi AT, Garweg JG, Pleyer U. The role of age in ocular toxoplasmosis: clinical signs of immunosenescence and inflammaging. Front Med. 2024;11:1311145. doi:10.3389/fmed.2024.1311145
164. Guitard J, Brenier-Pinchart MP, Varlet-Marie E, et al. Multicenter evaluation of the Toxoplasma gondii Real-TM (Sacace) kit performance for the molecular diagnosis of toxoplasmosis. J Clin Microbiol. 2024;62(4). doi:10.1128/jcm.01428-23
165. Gulshan JE, Lira SS, Qusar M, et al. Association between Toxoplasma gondii infection and serum neurotransmitter levels in major depressive disorder patients: a case-control study in Bangladesh. J Parasitol Res. 2024;2024. doi:10.1155/japr/7054920
166. Hurt K, Kodym P, Stejskal D, Cihar M, Rakovic J, Zikan M. Correlation of toxoplasmosis with small‑for‑gestational‑age newborns. Bratisl Lek Listy. 2024;125(2):92–95. doi:10.4149/BLL_2024_014
167. Kamel NA, Abdalla MS, Al Ali A, Alshahrani MY, Aboshanab KM, El Borhamy MI. Effectiveness of pre-transplant screening for high-priority multidrug-resistant pathogens on pre-engraftment infections after hematopoietic stem cell transplantation. Infect Drug Resist. 2024;17:2249–2260. doi:10.2147/IDR.S463868
168. Li X, Wang Q, Li X, et al. Carbon nanospheres dual spectral-overlapped fluorescence quenching lateral flow immunoassay for rapid diagnosis of toxoplasmosis in humans. J Pharm Biomed Anal. 2024:241. doi:10.1016/j.jpba.2024.115986
169. Mikita K, Mori T, Komine T, et al. Development of a LAMP method with lateral flow DNA chromatography to diagnose toxoplasmosis in immunocompromised patients. Trop Med Health. 2024;52(1). doi:10.1186/s41182-024-00613-4
170. Milad D, Antaki F, Bernstein A, Touma S, Duval R. Automated machine learning versus expert-designed models in ocular toxoplasmosis: detection and lesion localization using fundus images. Ocul Immunol Inflamm. 2024;32(9):2061–2067. doi:10.1080/09273948.2024.2319281
171. Ota H, Yamada H, Wada S, et al. Toxoplasma gondii IgG avidity for the diagnosis of primary infection in pregnant women: comparison between chemiluminescent microparticle immunoassay and enzyme-linked immunosorbent assay. J Infect Chemother. 2024;30(5):434–438. doi:10.1016/j.jiac.2023.11.019
172. Ramos RCF, Barbosa AS, Aleixo ALQC, Arruda IF, Amendoeira MRR. Comparison of immunological and molecular methods for laboratory diagnosis of ocular toxoplasmosis in blood, serum and tears in Brazil. PLoS One. 2024;19(2):e0298393. doi:10.1371/journal.pone.0298393
173. Zhou Y, Leahy K, Grose A, et al. Novel paradigm enables accurate monthly gestational screening to prevent congenital toxoplasmosis and more. PLoS Negl Trop Dis. 2024;18(5). doi:10.1371/journal.pntd.0011335
174. Adebakin BB, Atima MO, Idakwo U, et al. Comparative evaluation of funduscopy, PCR and serology in the diagnosis of ocular toxoplasmosis at ECWA Eye Hospital, Kano. BMJ Open Ophthalmol. 2025;10(1). doi:10.1136/bmjophth-2024-002023
175. Marchese A, L’Abbate G, Bandello F, Miserocchi E. Chronic retinal necrosis associated with Toxoplasma gondii. Ocul Immunol Inflamm. 2025;33(2):210–213. doi:10.1080/09273948.2024.2362876
176. Naseem M, Khan S, Alshaya DS, et al. ToRCH pathogens-induced histopathological changes in placental tissues and associated post obstetric complications. Acta Trop. 2025;261:107466. doi:10.1016/j.actatropica.2024.107466
177. Nourrisson C, Varlet E, Guitard J, et al. Multicenter performance evaluation of the “quanty TOXO (RH region)” kit (Clonit) for molecular diagnosis of toxoplasmosis. J Clin Microbiol. 2025;63(11):e0053825. doi:10.1128/jcm.00538-25
178. Umer L, Iqbal J, Ayaz Y, et al. Interpretable multi-model deep learning framework for automated four-class diagnosis of ocular toxoplasmosis using fundus imaging. Sci Reports. 2025;15(1):44012. doi:10.1038/s41598-025-29768-8
179. Usluca S, Bakir A, Arikok AT, Korkut G, Yagiz GC, Alper M. Detection of Toxoplasma gondii and high-risk human papillomaviruses in FFPE malignant and benign breast lesions using real-time PCR. Infect Drug Resist. 2025;18:3149–3155. doi:10.2147/IDR.S523180
180. Hoshina T, Miyamoto T, Miyajima M, et al. Longitudinal monitoring of Toxoplasma gondii antibodies in people with HIV in Japan. J Infect Chemother. 2026;32(1):102867. doi:10.1016/j.jiac.2025.102867
181. Reitsma JB, Bruns DE, Gatsonis CA, et al. Original Research & Special Stard 2015: an updated list of essential items for reporting diagnostic accuracy studies 1. Radiology. 2015;277(3).
182. Kortbeek LM, Villena I, Costache C, Petersen E. Toxoplasma gondii-specific IgG avidity testing in pregnant women. Clin Microbiol Infect. 2020;26:4–9. doi:10.1016/j.cmi.2020.04.014
183. Wang ZD, Liu HH, Ma ZX, et al. Toxoplasma gondii infection in immunocompromised patients: a systematic review and meta-analysis. Front Microbiol. 2017;8(MAR):1–12. doi:10.3389/fmicb.2017.00389
184. Alrubayyi A, Fahimi R, Hassan M, Madan J, Uthman OA. Current clinical practices and future perspectives for primary healthcare use of point-of-care devices: a scoping review. Int J Clin Pract. 2025;2025. doi:10.1155/ijcp/4742851
185. Vroom EB, Albizu A, Oliver J. Evaluating an implementation science training program: impact on professional research and practice. Glob Implement Res Appl. 2021;1(3):147–159. doi:10.1007/s43477-021-00017-0
186. Ibnidris A, Liaskos N, Eldem E, et al. Facilitating the use of the target product profile in academic research: a systematic review. J Transl Med. 2024;1:1–14.
187. Lippi G, Plebani M, Favaloro EJ. The model list of essential in vitro diagnostics: nuisance or opportunity ? Diagnosis. 2019;6(3):187–188.
188. Lange B, Roberts T, Cohn J, et al. Diagnostic accuracy of detection and quantification of HBV-DNA and HCV-RNA using dried blood spot (DBS) samples – a systematic review and meta-analysis. BMC Infect Dis. 2017;17(Suppl 1). doi:10.1186/s12879-017-2776-z
189. Moussy FG, Berumen AV, Pai M. EBioMedicine The WHO list of essential in vitro diagnostics: development and next steps. EBioMedicine. 2018;37:1–2. doi:10.1016/j.ebiom.2018.10.070
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.