Back to Journals » Infection and Drug Resistance » Volume 17
A Study on Risk Factors for Readmission of Elderly Patients with Pulmonary Tuberculosis Within One Month Using Propensity Score Matching Method
Authors Feng Y, Guo J, Luo S, Zhang Z, Liu Z
Received 12 January 2024
Accepted for publication 19 April 2024
Published 26 April 2024 Volume 2024:17 Pages 1625—1632
DOI https://doi.org/10.2147/IDR.S459260
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Yinping Feng, Jing Guo, Shuirong Luo, Zunjing Zhang, Zhongda Liu
Department of Tuberculosis, Lishui Hospital of Traditional Chinese Medicine Affiliated to Zhejiang University of Traditional Chinese Medicine, Lishui Tuberculosis Clinical Medical Research Center, Lishui, Zhejiang, People’s Republic of China
Correspondence: Zhongda Liu, Email [email protected]
Objective: Exploring the risk factors for readmission of elderly patients with pulmonary tuberculosis (PTB) within one month using the propensity score matching(PSM).
Methods: A retrospective analysis was conducted on the clinical data of elderly patients with PTB who were admitted to the Tuberculosis Department of Lishui Hospital of Traditional Chinese Medicine from January 2020 to October 2023. The patients were divided into two groups: non-readmission group and readmission group based on whether they were readmitted within one month after discharge. The PSM method was used to match the baseline data of the two groups of patients, and multivariate logistic regression analysis was conducted to explore the risk factors for readmission of elderly patients with PTB within one month after discharge.
Results: A total of 1268 hospitalized elderly patients with PTB were included in the study, comprising 977 readmitted patients and 291 newly admitted patients (22.95%). Using the PSM, 288 pairs of patients were successfully matched. Following matching, there were no statistically significant differences between the two groups in terms of gender, age, occupation, body mass index(BMI), past medical history, etc. (all P> 0.05). Multivariate logistic regression analysis indicated that infection, drug-induced liver injury(DILI), acute heart failure(AHF), chronic kidney disease(CKD), and extrapulmonary tuberculosis(EPTB) were all identified as risk factors for readmission of elderly patients with PTB.
Conclusion: After controlling for confounding factors through PSM, the study revealed that infection, DILI, AHF, CKD, and EPTB are risk factors for readmission among elderly patients with PTB, highlighting the need for early intervention.
Keywords: elderly patients with pulmonary tuberculosis, aged, readmission, propensity score matching, risk factors
Introduction
As the body undergoes degenerative changes, the vulnerability of elderly individuals increases and their immune system’s defense weakens, resulting in a higher risk of contracting tuberculosis.1 Research indicates that as individuals age, their lungs become more vulnerable to inflammation, which heightens the risk of tuberculosis infection in elderly individuals.2 Due to the decline in immune function, malnutrition, and other mechanisms and factors, the elderly are more susceptible to new tuberculosis infections and reactivation of latent tuberculosis infection. Therefore, they are more likely to suffer from tuberculosis compared to non-elderly individuals. With the further intensification of the aging population, PTB remains a disease that cannot be ignored, and more attention needs to be devoted to the prevention and control of PTB in the elderly. The positivity rate of sputum smear in elderly patients with PTB is low, which hinders diagnosis and often leads to delays in diagnosis. Moreover, elderly individuals exhibit lower immune function, more chronic complications, and increased susceptibility to treatment-related adverse drug reactions, all of which contribute to poorer treatment outcomes and higher mortality rates.3 The elderly, due to their weakened physique, underlying diseases, and medication side effects, are at risk of repeated hospitalization due to tuberculosis, which can reduce their quality of life and increase the economic burden. This study analyzes and explores the risk factors for rehospitalization of elderly patients with PTB one month after discharge in order to intervene early, improve the quality of life of patients, and reduce medical expenses.
Materials and Methods
Research Object Selection
Retrospective analysis was conducted on clinical data from elderly PTB patients hospitalized in our department from January 2021 to October 2023. The data included information on age, gender, occupation, BMI, and past medical history. This study received approval from the hospital’s Medical Ethics Committee (Approval number:LW-2024009).
Patients Inclusion and Exclusion Criteria
Inclusion criteria: (1) Patients who meet the diagnostic criteria for PTB;4 (2) Elderly hospitalized patients aged ≥ 60 years old; (3) The clinical data are complete. Exclusion criteria: (1) Patients with severe illness leading to death; (2) Patients who are readmitted due to other factors; (3) Patients with severe missing clinical data.
Patients Data Collection
The age, gender, occupation, BMI, past medical history (hypertension, diabetes, chronic obstructive pulmonary disease(COPD), bronchiectasis, tumor), and diagnoses after admission of patients were collected through the inpatient management information system.
Case Grouping
According to whether the patient has been readmitted within one month after discharge, they are categorized into two groups: the non-readmission group and the readmission group.
Statistical Analysis
All data were analyzed using SPSS 26.0 software. Count data are expressed as percentages (%), and differences between groups are compared using chi-square (χ2) test. Measurement data that conforms to a normal distribution are represented by the mean ± standard deviation ( ) and t-test is used. Measurement data that do not conform to a normal distribution are represented by the median (M) and interquartile range (P25, P75). Inter-group comparisons are performed using the Mann–Whitney U-test. The PSM extension program was utilized to perform propensity score matching between two groups of patients using the 1:1 nearest neighbor matching method, and the quality of the matching results was ensured by defining clamp values. Multiple logistic regression analysis was used to investigate the influencing factors of anxiety in elderly hospitalized patients with PTB, and the difference was statistically significant (P<0.05).
) and t-test is used. Measurement data that do not conform to a normal distribution are represented by the median (M) and interquartile range (P25, P75). Inter-group comparisons are performed using the Mann–Whitney U-test. The PSM extension program was utilized to perform propensity score matching between two groups of patients using the 1:1 nearest neighbor matching method, and the quality of the matching results was ensured by defining clamp values. Multiple logistic regression analysis was used to investigate the influencing factors of anxiety in elderly hospitalized patients with PTB, and the difference was statistically significant (P<0.05).
Results
Case Screening
A total of 1360 elderly patients hospitalized with PTB were included in the study. Of these, 36 patients had incomplete clinical data, 40 were readmitted for reasons unrelated to tuberculosis, and 16 patients had died. This resulted in a total of 1268 patients being included in the analysis. Patients were then categorized based on readmission status within one month after discharge, with 977 patients not being readmitted and 291 patients being readmitted. Following propensity score matching, a total of 288 pairs of patients were successfully matched (Figure 1).
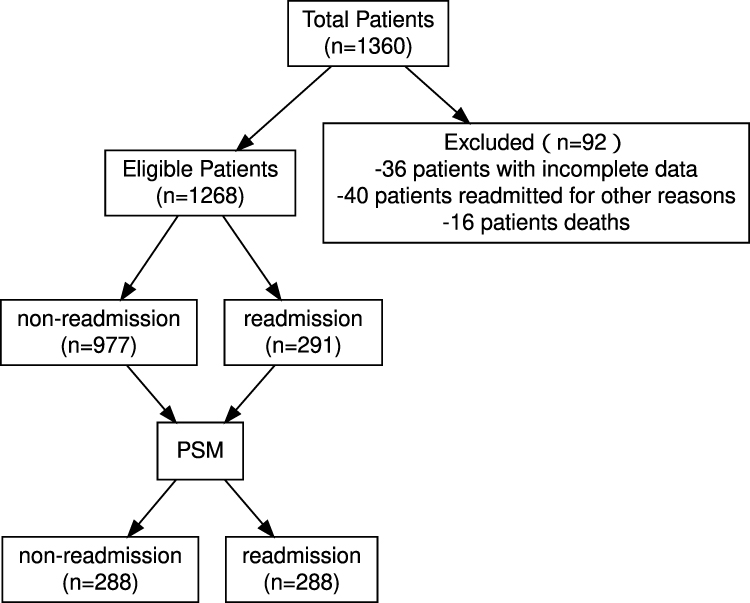 |
Figure 1 A flow chart for screening eligible studies. |
Comparison of Clinical Features Between Two Groups of Patients Before PSM
There were no significant differences in age, sex, occupation, BMI, diabetes history, and tumor history between the two groups (P>0.05). However, there were significant differences in the history of hypertension, COPD, and bronchiectasis (P<0.05) (Table 1).
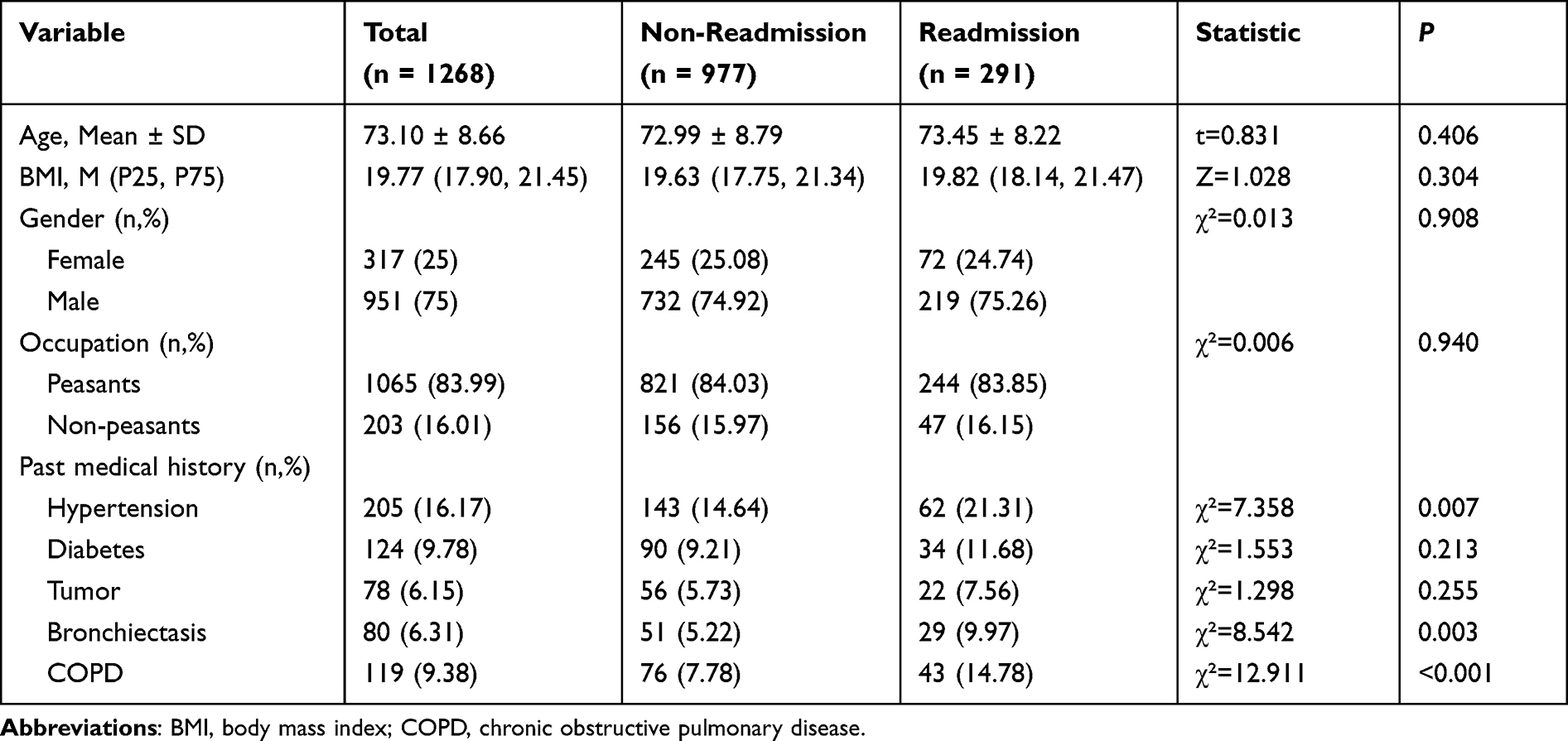 |
Table 1 Comparison of Clinical Features Between Two Groups of Patients Before PSM |
Clinical Characteristics of Two Groups of Patients After PSM
The age, sex, occupation, BMI, and past medical history (including hypertension, diabetes, tumor, bronchiectasis, and COPD) of the patients were used as matching variables for 1:1 propensity score matching. This resulted in 288 pairs of successfully matched patients, and there was no statistically significant difference in any of the variables after matching (P>0.05) (Table 2).
 |
Table 2 Clinical Characteristics of Two Groups of Patients After PSM |
Single Factor Analysis After PSM
After balancing the two sets of covariates using PSM, a further comparison was conducted between the non-readmission group and the readmission group with respect to other factors. The analysis revealed statistically significant differences between the two patient groups in terms of complications with infection, DILI, AHF, CKD, and EPTB (all P<0.05)(Table 3).
 |
Table 3 Single Factor Analysis After PSM |
Multivariate Logistic Regression Analysis After PSM
Using the variables that showed statistical differences (P<0.05) in the above univariate analysis as independent variables and readmission as the dependent variable, a binary logistic regression analysis was conducted. The results indicated that co-infection (OR=4.62, 95% CI: 3.08–6.92), DILI (OR=4.14, 95% CI: 2.09–8.19), AHF (OR=3.40, 95% CI: 1.86–6.21), CKD (OR=2.29, 95% CI: 1.06–4.95), and EPTB (OR=2.85, 95% CI: 1.83–4.42) are risk factors for readmission within one month in elderly patients with PTB (P<0.05) (Table 4).
 |
Table 4 Multivariate Logistic Regression Analysis After PSM |
Discussion
The most recent global tuberculosis report, released by the World Health Organization in 2023, indicates that there were 10.6 million tuberculosis patients worldwide in the past year, with the number of deaths due to tuberculosis reaching 1.2 million.5 Compared to the non-elderly population, the reported incidence rate of tuberculosis in the elderly population is higher. Japan has nearly 60% of tuberculosis patients aged 70 years or above, making it one of the countries with the highest incidence rates of tuberculosis among developed countries.6 A study conducted in our country indicates that the risk of developing PTB in the elderly is 2.4–2.9 times higher than that of the population under 65 years of age.7 Elderly individuals experience a reduction in thymus output of T lymphocytes due to impaired immune system function. Consequently, their ability to produce cytokines and other effector factors is reduced.8 The immune protection against tuberculosis infection is primarily achieved through the coordinated action of phagocytic cells and T lymphocytes in order to establish cell-mediated immunity.9 In addition, elderly patients are more likely to have structural lung diseases, such as bronchiectasis and COPD, which can also reduce the clearance rate of Mycobacterium tuberculosis in the lower respiratory tract, leading to PTB.10 The etiology of PTB in elderly individuals is thought to involve both exogenous reinfection and reactivation of latent infections.11 Elderly patients with PTB present unique challenges for diagnosis due to the low pathogen positivity rate, as well as the presence of multiple underlying diseases. As a result, treatment outcomes are often less effective, leading to a higher mortality rate.12 As the population continues to age, there is a need to strengthen research on tuberculosis in the elderly, which also contributes to the achievement of global tuberculosis control goals.13 Readmission within one month after discharge refers to a situation in which a patient is readmitted due to the same or a related illness within one month of their initial discharge.14 Research indicates that factors such as gender, age, place of residence, smoking status, history of COPD, history of chronic hepatitis, non-compliance with standard anti-tuberculosis treatment, and adverse drug reactions are associated with an increased risk of unplanned readmission for tuberculosis.15 There are also studies indicating that the median readmission time for patients with PTB is 24 days, primarily due to fever, worsening breathing difficulties, and hemoptysis.16 Additionally, being aged ≥ 65 years old is significantly correlated with readmission of tuberculosis patients within one month after discharge.17 Readmission after discharge imposes a substantial economic burden on patients and medical resources.18 In 2004, the cost of readmission for medical insurance in the United States was approximately $1.7 billion, representing around one-fifth of the total hospital expenses nationwide.19 Therefore, conducting research on the readmission of elderly hospitalized patients with pulmonary tuberculosis after discharge can play an important role in improving their quality of life and reducing medical expenses.
This study collected clinical data on elderly patients hospitalized with PTB and used propensity score matching to balance out confounding bias for the analysis of risk factors for readmission after discharge. Co-infection, DILI, AHF, CKD, and EPTB were identified as risk factors for readmission of elderly patients with PTB. Due to the decline in immune function and structural changes in the lungs, elderly patients with PTB are susceptible to secondary infections from other pathogens, with bacterial infections being the most common. The co-occurrence of PTB and other pathogen infections can prolong the treatment duration of tuberculosis, induce resistance to tuberculosis, and is also a contributing factor to recurrent hospitalization for PTB. At the same time, malnutrition in older adults also increases the risk of pulmonary bacterial infections in elderly patients with PTB. Additionally, fungal infections, such as Aspergillus and Cryptococcus, are also more commonly observed. In this study, 53.12% of readmitted patients had other infections, which was the primary cause following matching. Logistic analysis indicated that this was a risk factor for readmission within one month of discharge (OR=4.62, 95% CI: 3.08–6.92). During the course of anti-tuberculosis treatment, it is important for clinical doctors to be mindful of potential liver function damage caused by anti-tuberculosis drugs. This can not only extend the treatment period and cause interruptions, but also significantly impact the prognosis of patients. An epidemiological survey on drug-induced liver injury in the Chinese population revealed that anti-tuberculosis drugs are the main cause of liver injury in China, accounting for approximately 21.99%.20 The incidence of drug-induced liver damage in the matched readmission patients in this study was 15.97%, which represents a risk factor for readmission of elderly PTB patients (OR=4.14, 95% CI: 2.09–8.19). AHF significantly impacts the health of the population in China and increases the socio-economic burden. Early diagnosis and intervention can reduce the risk of readmission. The prognosis for heart failure patients is extremely poor, with a readmission rate of up to 24.8% within 90 days.21 Therefore, the average annual hospitalization cost for AHF patients exceeds 20,000 yuan.22 The incidence of AHF in matched readmission patients in this study was 18.40%, which represents a risk factor for readmission of elderly PTB patients (OR=3.40, 95% CI: 1.86–6.21).In recent years, the number of patients with CKD has been increasing, along with the prolonged survival years of those on dialysis. As a result, there has been a gradual increase in the number of patients with CKD who also have tuberculosis.23 CKD can lead to a reduction in the success rate of treatment and an increase in mortality due to the impact of tuberculosis drug dosage on the adjustment of renal function.24 The incidence of adverse reactions to anti-tuberculosis treatment in patients with CKD is significantly higher than in the general population. It is important to avoid drugs with known nephrotoxic effects and to utilize liver metabolism drugs whenever possible. This study also demonstrated that renal dysfunction is a significant risk factor for readmission in elderly patients with PTB (OR=2.29, 95% CI: 1.06–4.95). PTB is the most prevalent form of tuberculosis. However, in recent years, there has been a steady increase in the incidence of combined pulmonary and EPTB. This dual manifestation of the disease is associated with more severe symptoms than those of simple PTB, as well as a poorer prognosis.25 Over a 10-year period, Beijing Chest Hospital tracked hospitalized tuberculosis patients and found that EPTB accounted for 33.4% of all tuberculosis cases. This suggests a serious prevalence of EPTB at present.26 EPTB is typically caused by the spread of Mycobacterium tuberculosis through the blood or lymphatic system, or by direct spread from adjacent organs. Studies have also shown that a relatively high proportion of inpatients with PTB experience complications with EPTB, and approximately one-fifth of EPTB cases occur in two or more locations. This can lead to worsening of the condition, prolonged treatment, a low cure rate, and increased economic burden.27 In this study, following matching, the incidence rate of EPTB in elderly patients with readmission for pulmonary tuberculosis was 37.15%, representing a significant risk factor for readmission in this patient group (OR=2.85, 95% CI: 1.83–4.42).
Conclusions
In summary, the PSM method effectively balanced confounding bias and revealed that co-infection, DILI, AHF, CKD, EPTB were significant risk factors for readmission within one month after discharge in elderly patients with PTB. Early evaluation and intervention should be prioritized based on these findings. However, it is important to note that this study has certain limitations. It is hoped that future prospective studies with larger sample sizes will be conducted to further determine the risk factors for readmission of elderly hospitalized PTB patients after discharge.
Institutional Review Board Statement
This study was conducted with approval from the Ethics Committee of Lishui Hospital of Traditional Chi- nese Medicine (LW-2024009). This study was conducted in accordance with the declaration of Helsinki.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Informed Consent Statement
Written informed consent was obtained from all participants.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Zhejiang Provincial Administration of Traditional Chinese Medicine Co built Science and Technology Plan Project (No.GZY-ZJ-KJ-23096).
Disclosure
The authors declare no competing interests in this work.
References
1. Gupta S, Arora V, Sharma OP, et al. Prevalence & pattern of respiratory diseases including tuberculosis in elderly in ghaziabad - Delhi - NCR. Indian J Tuberc. 2016;63(4):236–241. doi:10.1016/j.ijtb.2016.09.012
2. Piergallini TJ, Turner J. Tuberculosis in the elderly: why inflammation matters. Exp Gerontol. 2018;105:32–39. doi:10.1016/j.exger.2017.12.021
3. Velayutham BRV, Nair D, Chandrasekaran V, et al. Profile and response to anti-tuberculosis treatment among elderly tuberculosis patients treated under the TB control programme in South India. PLoS One. 2014;9(3):e88045. doi:10.1371/journal.pone.0088045
4. Lyon SM, Rossman MD, Schlossberg D. Pulmonary Tuberculosis. Microbiol Spectr. 2017;5(1). doi:10.1128/microbiolspec.TNMI7-0032-2016
5. Word Health Organization. Global Tuberculosis Report 2023. Geneva: World Health Organization; 2023.
6. Hase I, Toren KG, Hirano H, et al. Pulmonary tuberculosis in older adults: increasedmort ality related to tuberculosis within two months of treatment initiation. Drugs Aging. 2021;38(9):807–815. doi:10.1007/s40266-021-00880-4
7. Zhang CY, Chen H, Zhang H, et al. Analysis of the reported incidence of pulmonary tuberculosis in the elderly aged 65 and over in China, 2011–2020. Chin J Dis Control Prevent. 2022;26(11):1252–1258.
8. Akbar AN, Henson SM. Are senescence and exhaustion intertwined or unrelated processes that compromise immunity? Nat Rev Immunol. 2011;11(4):289–295. doi:10.1038/nri2959
9. Byng-Maddick R, Noursadeghi M. Does tuberculosis threaten our ageing populations? BMC Infect Dis. 2016;16(1):119. doi:10.1186/s12879-016-1451-0
10. Kan T, Komiya K, Yamasue M, et al. Comparison of chest computed tomography features between pulmonary tuberculosis patients with culture-positive and culture-negative sputum for non-mycobacteria: a retrospective observational study. Medicine. 2021;100(31):e26897. doi:10.1097/MD.0000000000026897
11. Di Gennaro F, Vittozzi P, Gualano G, et al. Active pulmonary tuberculosis in elderly patients: a 2016–2019 retrospective analysis from an Italian referral hospital. Antibiotics. 2020;9(8):489. doi:10.3390/antibiotics9080489
12. Negin J, Abimbola S, Marais BJ. Tuberculosis among older adults – time to take notice. Int J Infect Dis. 2015;32:135–137. doi:10.1016/j.ijid.2014.11.018
13. Li SJ, Li YF, Song WM. Population aging and trends of pulmonary tuberculosis incidence in the elderly. BMC Infect Dis. 2021;21(1):302. doi:10.1186/s12879-021-05994-z
14. Duggal R, Zhang Y, Diana ML. The association between hospital ACO participation and readmission rates. J Healthc Manag. 2018;63(5):e100–e114. doi:10.1097/JHM-D-16-00045
15. Ye X, Su X, Shi J, et al. Incidence, causes, and risk factors for unplanned readmission in patients admitted with pulmonary tuberculosis in China. J Infect Dev Ctries. 2023;17(7):1007–1013. doi:10.3855/jidc.17190
16. Cao J, Liu S, Huang J. Risk factor for 31-day unplanned readmission to hospital in patients with pulmonary tuberculosis in China. Saudi Med J. 2021;42(9):1017–1023. doi:10.15537/smj.2021.42.9.20210281
17. Anaam MS, Alrasheedy AA, Alsahali S, et al. Rate and risk factors of recurrent tuberculosis in Yemen: a 5-year prospective study. Infect Dis. 2020;52(3):161–169. doi:10.1080/23744235.2019.1690162
18. Finlayson K, Chang AM, Courtney MD, et al. Transitional care interventions reduce unplanned hospital readmissions in high-risk older adults. BMC Health Serv Res. 2018;18(1):956. doi:10.1186/s12913-018-3771-9
19. Daras LC, Deutsch A, Ingber MJ, et al. Inpatient rehabilitation facilities’ hospital readmission rates for medicare beneficiaries treated following a stroke. Top Stroke Rehabil. 2021;28(1):61–71. doi:10.1080/10749357.2020.1771927
20. Shen T, Liu Y, Shang J, et al. Incidence and etiology of drug-induced liver injury in mainland China. Gastroenterology. 2019;156(8):2230–2241.e11. doi:10.1053/j.gastro.2019.02.002
21. Zhang Z, Cao L, Chen R, et al. Electronic healthcare records and external outcome data for hospitalized patients with heart failure. Sci Data. 2021;8(1):46. doi:10.1038/s41597-021-00835-9
22. Huang J, Yin H, Zhang M, et al. Understanding the economic burden of heart failure in China: impact on disease management and resource utilization. J Med Econ. 2017;20(5):549–553. doi:10.1080/13696998.2017.1297309
23. Hill NR, Fatoba ST, Oke JL, et al. Global prevalence of chronic kidney disease- A systematic review and meta-analysis. PLoS One. 2016;11(7):e0158765. doi:10.1371/journal.pone.0158765
24. Igari H, Imasawa T, Noguchi N, et al. Advanced stage of chronic kidney disease is risk of poor treatment outcome for smear-positive pulmonary tuberculosis. J Infect Chemother. 2015;21(8):559–563. doi:10.1016/j.jiac.2015.04.008
25. Natarajan A, Beena PM, Devnikar AV, et al. A systemic review on tuberculosis. Indian J Tuberc. 2020;67(3):295–311. doi:10.1016/j.ijtb.2020.02.005
26. Pang Y, An J, Shu W, et al. Epidemiology of Extrapulmonary Tuberculosis among Inpatients, China, 2008–2017. Emerg Infect Dis. 2019;25(3):457–464. doi:10.3201/eid2503.180572
27. Xu ZH, Liu LQ, Wang QZ, et al. Study on epidemiological characteristics and influencing factors of pathogen positive hospitalized pulmonary tuberculosis patients with extrapulmonary tuberculosis. Chin J Antitubercul. 2021;43(11):1164–1170.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.