Back to Journals » Advances in Medical Education and Practice » Volume 10
A study of clinical teachers’ attitude to teaching and perceived learning needs in a medical college in Nigeria
Authors Olasoji HO, Mu'azu AB ![]() , Garba MH
, Garba MH ![]()
Received 18 April 2018
Accepted for publication 30 June 2018
Published 12 August 2019 Volume 2019:10 Pages 605—617
DOI https://doi.org/10.2147/AMEP.S171550
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
HO Olasoji, Ahmad Bilyamini Mu’azu, Mairo Hassan Garba
Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, College of Medical Sciences, University of Maiduguri, Maiduguri, Borno State, Nigeria
Background and purpose: Debates on medical educational reform initiatives in Nigeria have gradually shifted from access to medical colleges to improving learning quality. Understandably, clinical teachers are being encouraged to acquire basic teaching pedagogical knowledge through learning activities. Considering the fact that the concept of faculty development for medical teachers’ is still evolving in Sub-Saharan Africa, this study aims to explore clinical teachers’ attitude to teaching and perceptions of continuing education in teaching knowledge and skills in a medical college in Nigeria.
Methods: Using a mixed-method research approach, quantitative data were collected from a sample of teachers through survey questionnaires, and qualitative data were obtained through face-to-face individual semi-structured interviews of teachers from the same institution.
Results: Sixty-one survey questionnaires (response rate of 88%) and 10 interviews were completed and analyzed. Findings revealed that teachers’ derived satisfaction from teaching and maintain a strong commitment to teaching. Bedside teachings (64%) and lectures (21%) were reported to be the most frequent mode of teaching. Although four out of every five respondents (80%) reported not having previous training in teaching, a large proportion (97%) self-assessed their teaching abilities to be average or above average, with most indicating that the experience of teaching observed during undergraduate medical training may be sufficient preparation for their teaching roles. The majority of the teachers’ were of the opinion that there is a need to improve their individual teaching skill. However, in the absence of formal faculty development programs in the college, most of the teachers indicated that their teaching skills are currently being improved through sporadic informal community of practice involving interested colleagues and modeling identified good teachers.
Conclusion: A catalyst of learning by teachers’ may come from their belief and self-rating of teaching ability. In this under-resourced context, explicit classifications of existing informal learning opportunities coupled with greater institutional support could improve teaching and teachers’ development.
Keywords: clinical teachers, attitudes, teaching, faculty development, Nigeria
Introduction
Globally, the role of teachers in medical colleges is multi-dimensional. Clinical teachers have competing and increasing demands placed upon them to be creative and effective teachers, successful researchers and productive patient caregiver.1 For some, there is the further challenge of leadership and administrative duties. Balancing busy clinical, research and teaching workload continues to be a challenge for clinical teachers worldwide, and this has resulted in an ongoing debate on the role of doctors as teachers in medical education. A major concern in doctors’ teaching role is that teaching expertise has traditionally been assumed to be part of clinical or scientific expertise, yet, unlike the preparation provided for their roles as clinicians and despite their expertise in what they teach, majority of clinical teachers have little or no training in their teaching role.2–4
Previous studies on the subject have identified two schools of thought; those who dismiss teacher training as inessential for doctors’ teaching roles and those who argue that they should be trained in teaching skills so as to meet the expectations of the teaching job. The main premise for the first school of thought is that medical doctors selected to teach at this level should have the competence and inherent aptitude required to figure out what is required of them and do it well.5
Key arguments for the formal training of doctors in teaching skills are that: (1) quality teaching requires effective pedagogical skills; however, many doctors gain expertise in fields of specialization that are not related to these pedagogical competencies.6 (2) Notwithstanding their qualifications, some academic doctors feel inadequately prepared to teach at a higher institutional level and lack the confidence to do so.6,7 This camp further argues that the modern academic medical workplace is characterized by changing social expectations, new technologies and a shift in emphasis toward the learner.
Over the years, much work has been directed at faculty development program in teaching skills for medical educators in Western countries. For instance, in the United Kingdom, the General Medical Council (GMC) publication, “The Doctor as Teacher“ and “Good Medical Practice“ state that “ … those who accept special responsibilities for teaching should take steps to ensure that they develop and maintain teaching skills.”8,9 In contrast, literature indicate that faculty development program has not gained wide acceptance in medical colleges in sub-Saharan Africa. This is despite the fact that majority of medical teachers in this part of the world are insufficiently prepared for their teaching role.10,11 Current studies have concluded that without formal preparation for the teaching role, teachers may not be able to offer quality training programs for students.12
More recently, debates on medical educational reform initiatives in Nigeria have gradually shifted from access to medical colleges to improving learning quality. Understandably, increasing attention is now being paid to the quality of medical teachers, more importantly their teaching skills.13,14 This is more so in a country, as in most other developing countries, where education means teachers. In the face of a dearth of essential teaching aids, library facilities and texts, teachers invariably become the key sources of knowledge, skills and appropriate orientation.15,16 Consequently, the medical teacher is central to facilitating the processes that lead to effective teaching, and as well, students’ learning outcomes are affected by teachers quality.
Subsequently, there has been a growing demand and support for embedding teacher training courses in postgraduate medical training curriculum in Nigeria13,16,17 and for the implementation of teacher-development activities as a standard part of the program in medical colleges.13,14,16 However, intricately linked with the issues around the teaching role of clinical teachers are teachers’ attitudes toward teaching. Interpreting attitude as a complex interweaving of beliefs and effective responses that influence individual’s worldviews, their decisions and judgments, and their choice to act in certain conscious or subconscious ways,18 the resulting effective load will have repercussions on the developed behavior. Attitudes therefore play an important role in guiding teachers’ thoughts and behaviors.19,20
Although research on the correspondence of teachers’ attitude and behavior regarding faculty development has produced mixed results,20 an analysis combining the design features of faculty development initiatives and teachers’ attitude toward these initiatives probably accounts for more of the variance in the effectiveness of faculty development program than either of these sets of factors alone. These studies however espouse some influence that attitudes and beliefs have on teachers’ decision regarding teaching and learning. For example, studies suggest that the availability of professional learning activities in medical schools is not a guarantee that clinical teachers will participate.21 Furthermore, substantial amounts of time and financial resources are invested at universities in many countries worldwide to stimulate the professional development of medical teachers,7 which means that explicit examination of factors that foster or interfere with learning and development of clinical teachers is merited, particularly in resource-limited environments. In addition, scarcity of resources continues to pose a major challenge to medical education in sub-Saharan Africa.15,16 Successful implementation of educational programs therefore depends on the availability of essential data and strategic planning in this setting.
In view of the fact that the whole concept of faculty development for medical teachers’ is still evolving in Nigeria and across Africa,11,13,14 it is important to understand the perceptions of this issue by clinical teachers themselves. Also, in strengthening faculty development initiatives (which largely involves participation in learning activities) in medical colleges, there is the need to explore the attitudes of clinical teachers to teaching and development. This study aims to explore clinical teachers’ attitude to teaching and their perceptions of continuing education in relation to developing their knowledge and abilities as teachers in a medical college in Nigeria. Establishing a clear understanding of these concepts and the relationship among them will accomplish an important first step in the planning and implementation of sustainable faculty development programs in medical colleges in Sub-Saharan Africa.
Method and data sources
Research context
The College of Medicine, University of Maiduguri, the site of this research is located in the North-Eastern region of Nigeria and it is presently the only accredited medical college in this geopolitical zone. The North-Eastern region has a population of 19 million making up 13.52% of the total population of Nigeria.22 The college has an annual intake of 140 students and attracts students and teachers from all the 6 geopolitical zones of the country. Similar to other medical colleges in Nigeria, the curriculum typifies the ‘traditional’ curriculum model described by Harden et al,23 as course delivery is mostly instructive lectures, bedside demonstration and an emphasis on information gathering as a learning strategy.
Participants
Participants were clinical teachers with postgraduate medical qualifications in relevant specialties and are primarily employed by the university to provide teaching to undergraduate medical students during the clinical program. In addition, they are given honorary appointments as consultant specialists by the teaching hospital where the students undergo clinical attachments. Hence, apart from their teaching roles, the clinical teachers pursue research (in area of clinical specialty) and provide specialist clinical care. The University pays monthly salary for teaching roles and the hospital pays monthly honorarium for clinical care.
Data collection
A mixed-methods approach was used for gathering data because it was understood that while some attributes of the teachers’ attitudes to teaching and learning needs may be amenable to quantitative analysis, other attributes might require qualitative approach. In other words, gathering facts and figures through survey questionnaire and also seeking “clarifications, and elaborations of the results from the quantitative method” through participants’ interview to produce a bigger picture behind those data.24
The study population for the quantitative data is defined as clinical teachers at the College of Medicine, University of Maiduguri, Nigeria. This population as listed in the College handbook of the university, numbered 138. The handbook groups clinical teachers according to their respective departments and in order of rank. In selecting a study sample, 50% sample was chosen by randomly selecting the first name and subsequently alternate names from the list. This ensured that different departments and grades of the staff were equitably represented. In a situation where a selected individual was discovered not to be currently in post, the next person on the list was selected as a replacement.
Participants completed an adapted version (following a pilot study) of pre-existing survey questionnaire which was previously used for measuring medical teachers’ attitudes to teaching and teacher training in a British medical school25 and in an Australian medical school.26 The questionnaire consisted of a 16-item Likert scale questions, of which 10 items (items: 1, 2, 3, 4, 7, 8, 9, 11, 14 and 16) explored aspects of teaching and 6 items (items: 5, 6, 10, 12, 13 and 15) addressed attitudes to teacher training. In part A of the survey, all participants were expected to select from a Likert scale 5-point rating: “strongly disagree”, “disagree”, “neutral”, “agree” and “strongly agree”. Part B consisted of 12 items to obtain demographic attributes of participants.
However, for the purposes of criteria of ambiguity, relevance and internal consistency reliability, the original survey questionnaire was piloted with a group of 12 volunteers drawn from clinical teachers in the faculty of dentistry. This pilot survey lasted 15 mins and participants’ comments, both positive and negative, were very constructive and provided the researchers with extremely useful feedback. Some of the suggestions led to appropriate modifications of the survey instrument. An internal mailing system was used to send numbered questionnaires to the 61 members of the study group. Each questionnaire was enclosed within an envelope specifically addressed to respondents, and respondents were asked to use this when returning the completed questionnaire via the internal mail. Those who had not responded after 2 weeks were again sent a copy of the questionnaire within the envelope as a form of reminder.
Using a purposeful sampling technique,27 10 clinical teachers known for their keen interest in medical education and who were willing give about 40–60 mins of their time to be interviewed, were selected for the qualitative data. To enhance objectivity, a sufficiently diverse group was chosen from both genders. Interviews were conducted in each participant’s office for their convenience and to de-emphasize other working relationships they might have with the researcher. An in-depth individual semi-structured approach to interview was adopted to lead the discussion, with open-ended questions aimed at enriching data. Unstructured follow-up questions were used to encourage further elaboration. These questions commonly took the form of, “What do you mean by that?”, “Could you tell me a bit more about that?”, “Why is that important to you?”, “Could you explain that further?” In many cases, the follow-up questions were more important in eliciting underlying meanings than the predetermined questions. All interviews were audio-recorded.
Data analysis
Qualitative data collected were coded and entered using SPSS version 16. The analysis carried out was univariate (summary statistics; frequencies and percentages) and bivariate (cross-tabulations, chi-square test). For all statistical analyses of relationships, p-value of less than 0.05 was accepted as level of statistical significance.
Contents of audio recordings during the interview were transcribed verbatim and analyzed to attribute codes to recurring utterances in order to categorize contents.28 Additional codes for newly emerging topics were created as needed. To examine the authenticity and credibility of the findings of the interview data, participants’ validation process was used. Main themes from the initial coding of the interview were drawn together and woven into individual narratives, which were given to each interviewee for comment on the text in terms of accuracy, balance and omissions, thereby generating further data for analysis.29
Ethics
Ethical approval for this research was granted by the ethics committees of the Cardiff University, United Kingdom and the University of Maiduguri Teaching Hospital, Nigeria. Accordingly, all participants consented to participate and elected to have pseudonyms to protect their identities. Participants’ written informed consent was obtained and confidentiality was ensured.
Results
The survey questionnaire was sent to 69 teachers (50% of the total clinical teachers). Seven questionnaires were not returned and one questionnaire was discarded as the respondent did not complete any of the items in Section B of the questionnaire (demographic attributes data). The data obtained from 61 completed and usable questionnaires were analyzed, thus giving a response rate of 88%.
Profile and attributes of respondents
A profile of the respondents is as presented in Table 1. A large proportion (n=47) of the respondents fell within the age range of 36–55 years. With 92% being male, the sex distribution of the respondents correlated with that of the population sampled. The majority of the teachers (71%) have been employed for teaching their roles for the last 15 years. Most had considerable teaching experience, with more than half (56%) indicating teaching more than twice a week. Bedside teachings were reported to be the most frequent mode of teaching (64%), followed by lectures (21%). Only 4 (7%) respondents frequently involved in small group teaching such as tutorials and seminars. A predominantly large proportion of respondents (97%) self-assessed their teaching ability to be average or above average. Only 2 respondents rated personal teaching ability as below average.
 |
Table 1 Respondents’ profile (N=61) |
Four out of every 5 (78.6%) respondents reported not having previous training in teaching methods and skills, while only 9 (14.7%) had attended a teacher training course in the last 5 years. More than half (57%) had previously heard of medical education department and 8 (13%) claimed membership of Medical Education Society. When attributes of the clinical teachers were analyzed in relation to gender, frequency of teaching and previous training in teaching, there were no significant differences in attributes between the sexes. Although only 4 (7%) of the respondents were female, just like the male population, they were more likely to have been employed in the previous 15 years, frequently undertook bedside teaching and taught more than twice per week. However, no female occupied Readership or Professorship posts, any had previous training in teaching and none had attended any teacher training course in the previous 5 years.
Rates of respondents with previous training in teaching fell progressively with the length of period since appointment in the medical college (see Table 2). Based on self-reported teaching abilities of below average and average and above, results show a significant difference between those who had previous teacher training and those who did not (p=0.003). Out of the 10 respondents who had previously been trained in education methods, workshop/seminar (n=7) was the most frequent method of training followed by postgraduate diploma in general education (n=2) and certificate program in general education (n=1). No teacher reported having formal training in medical education (see Table 3). Clinical teachers that rated personal teaching ability as above average tended to be in the higher academic cadre (professors =67%; associate professors=60%). There was no significant difference in the proportions across the different academic ranks and personal rating of teaching activity (p=0.094).
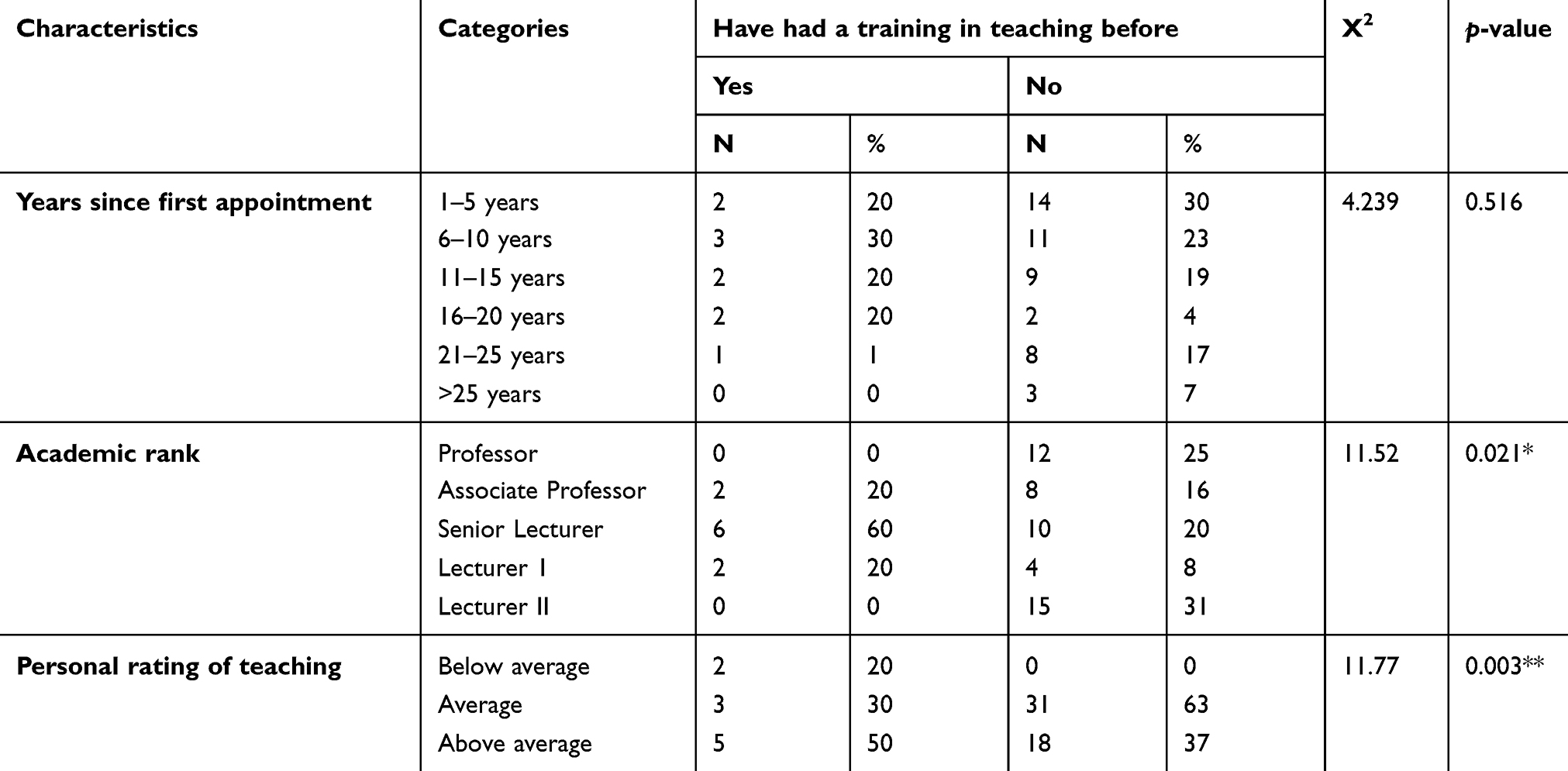 |
Table 2 Attributes of teacher training course attendees and non-attendees |
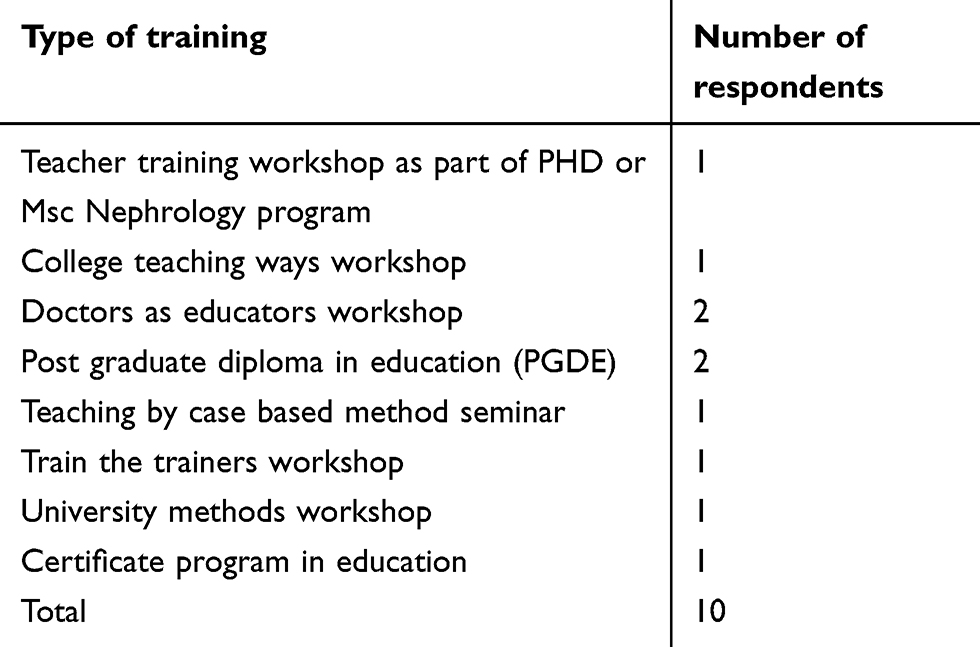 |
Table 3 Types of teacher training program attended |
Attitudes to teaching and perceived learning needs
Data indicating responses to all attitudinal statements are presented in Table 4.
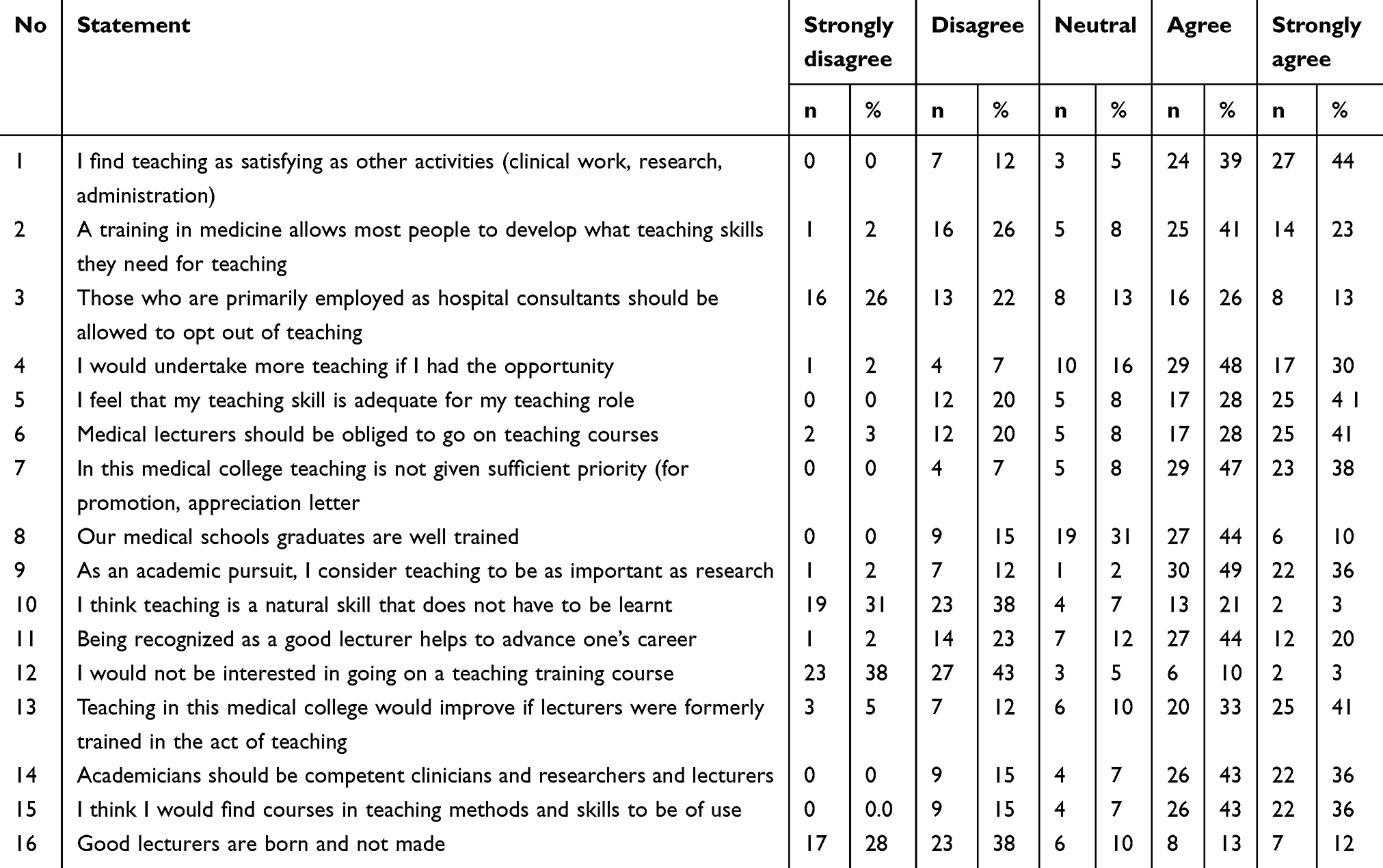 |
Table 4 Distribution of responses to attitudinal statements |
Enthusiasm for teaching
Analyses of the survey results reveal that a high level of enthusiasm to teaching was demonstrated by the respondents, with a large majority (84%) indicating pleasure in teaching and satisfaction with teaching roles (see Table 5). Furthermore, 3 out of every 4 participants indicated their willingness to take additional teaching responsibilities. Ten respondents (17%) were however undecided in terms of undertaking more teaching activities.
 |
Table 5 Distribution of responses to statements measuring enthusiasm for teaching |
Attitudes of complacency toward teaching
Statements measuring the attitude of complacency indicated that most clinical teachers felt that the experience of seeing how teaching was done during medical professional training may be sufficient preparation for teaching roles (see Table 6). Majority (66%) of the teachers believed that good teachers were not ‘born that way’ but developed into the role. About two-thirds (63%) of the clinical teachers were however of the opinion that such development can take place during general medical training.
 |
Table 6 Distribution of responses to statements measuring attitude of complacency toward teaching |
Overall, about half, or 54% of the respondents, felt that medical students in the college were well trained, though almost a third (31%) had no opinion on this.
Status of teaching
The vast majority of respondents (85%) valued teaching just like research, as an academic pursuit, with 80% also indicating that academic doctors should be competent in research, teaching and patient care (see Table 7). However, the perceived status of teaching within academia was low, with about 5 out of every 6 respondents (85%) feeling that teaching was awarded little value in academic promotion processes. Furthermore, only 15 respondents (25%) reported that recognition of good teaching contributed to career advancement.
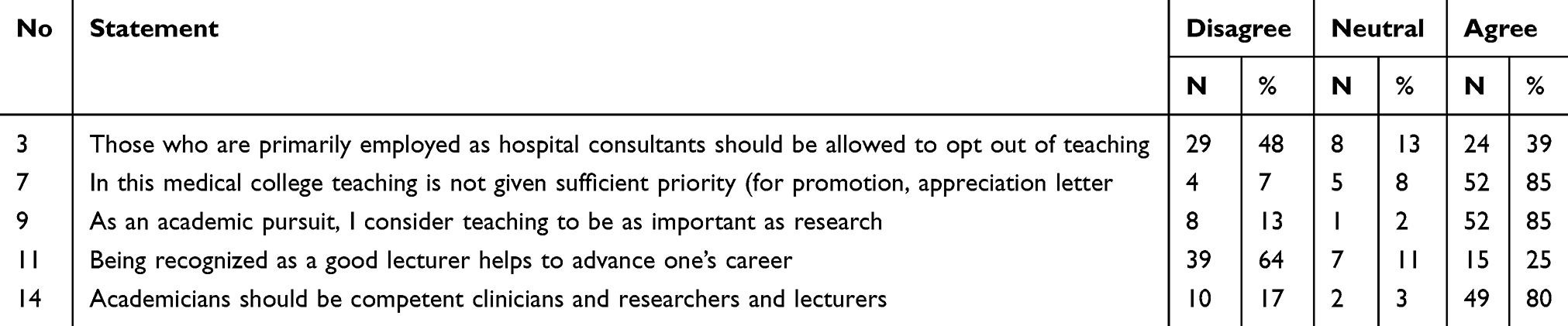 |
Table 7 Distribution of responses to statements measuring status of teaching |
The respondents were divided in their opinion as to whether or not those primarily employed as hospital consultants should be allowed to opt out of teaching. As high as 47% of the respondents indicated agreement with this statement, while 48% of the respondents did not.
Perceived learning needs
Majority of the clinical teachers were favorably disposed to the need to improve teaching skills through the concept of training courses, given that they agreed that teaching in the college would be improved by such courses (see Table 8). They considered such courses useful and disagreed with the statement that they would not be interested in participating (Thus indicating their willingness to undertake a teaching training course).
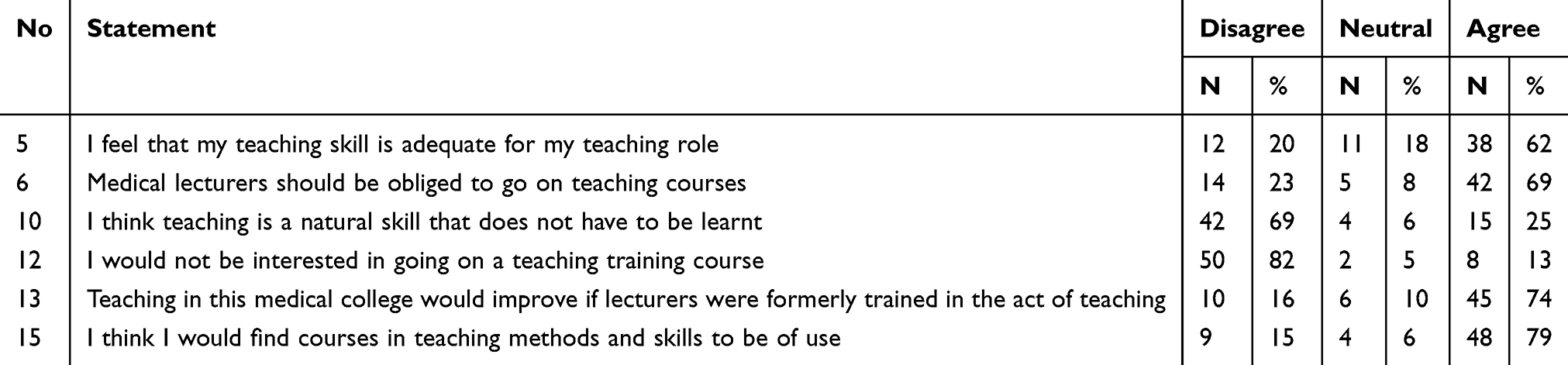 |
Table 8 Distribution of responses to statements measuring perceived learning needs |
As shown by correlation matrix, the answers to these three questions were strongly correlated (see Table 9). However, it is pertinent to note that 10 (16%) teachers felt that teaching would not be improved by training courses and 6 (10%) had no opinion on this statement. In addition, 9 (15%) teachers felt that training programs would not be of personal use and 8 (13%) reported that they would not wish to attend. In general, 2 out of every 3 (69%) respondents indicated that teacher training courses should be made compulsory. However, 14 (23%) felt that they should not.
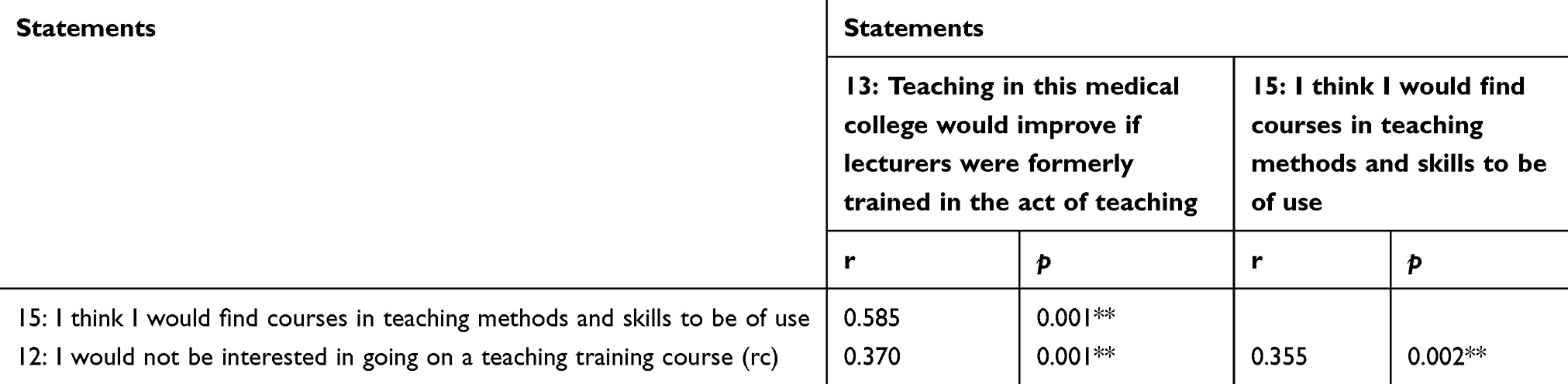 |
Table 9 Correlation of responses to statements 12, 13 and 15 (Kendall’s Tau-b correlation) |
Discussion
Attributes of clinical teachers
Regarding the gender distribution of teachers in this medical college, it is worth noting that there is a relatively low population of female teachers compared with male teachers as the male to female ratio of 14 to 1 signifies. This correlates with the findings from previous studies in the country.30 The low recruitment of females in academic positions in Nigerian universities has been of major concern in education literature. One reason suggested is that females are particularly disadvantaged in enrolment into vocational fields such as medical sciences and engineering, and this has been attributed to prevailing social, cultural and economic factors in the country.31 In addition, these factors tend to limit females’ participation in formal education. Equal access to ensure the attainment of educational qualification is necessary if more females are to fully participate in medical academia. Furthermore, it is vital that these individuals are encouraged to enter a career in clinical academia and receive the support necessary to maintain them on an academic track.32
There is evidence which suggests that staff retention is a major challenge in this college, considering the fact that it was established more than 40 years ago and presently has clinical staff strength of only 138 members, with 7 out of every 10 of these teachers employed in the last 15 years. Also, only 3 teachers have teaching experience in the college for 25 years or more. Studies indicate that recruiting and retaining health professionals who wish to build a teaching career is often challenging.33 However, this issue may have even more significance in resource-limited environments. In a recent large-scale study to determine the challenges for medical education in sub-Saharan Africa, Mullan et al34 estimated that the number of teaching staff (salaried full-time or part-time and volunteer) at 51 of 98 medical colleges was fewer than 100. Major impediments to recruitment and retaining of faculty according to the research include inadequate salaries, limited career options, full teaching workload, growing enrolment and lack of equipment and support staff. This shortage is further amplified by brain drain.35
An important observation is the efforts made to reduce this trend. Some countries in sub-Saharan Africa are known to have initiated creative strategies, usually in the form of incentives to retain medical teachers. Such strategies included housing and communication allowances in Tanzania, targeted effort to promote and train medical faculty in Mozambique and payment of special clinical teaching and supplementation allowances in Nigeria.33 Despite these strategic innovations, substantial and long-term faculty scarcity remains a challenge.
The assessment of the teaching activities of the teachers surveyed produced some essential findings. In contrast to previous studies,25,36 this study revealed heavy teaching workload of majority of the clinical teachers. About 50% of the survey participants indicated being actively involved in one form of teaching activity twice a week. The fact that majority are primarily employed by the university to teach undergraduate students and are therefore answer to the university might have contributed to the trend. This may lend weight to the argument that teachers in medical education be selected for roles as either teacher/clinician or teacher/researchers.6
Another possible explanation for the heavy teaching load of most of the participants could be the substantial increase in the number of undergraduate medical students in Nigerian universities in recent times,37 coupled with the limited academic staffing. This might have required many teachers to take on or increase existing teaching responsibilities. This claim deserves a closer look and it is a reflection of one of the major challenges faced by medical education in sub-Saharan Africa as noted by Mkony et al.38 On the one hand, halting expansion of student admissions limits availability of professional care for a large portion of the populace and restricts the pool of potential faculty recruits. On the other hand, when universities admit larger cohorts without training and employing more teachers, the standard of medical education will decline and invariably limit the quality of care students can provide upon qualification.
Attitudes to teaching and perceived learning needs
Despite the multiple challenges for medical education in Nigeria, this study has shown that clinical teachers in the College of Medicine, University of Maiduguri, derive satisfaction from and maintain a strong commitment to teaching. Studies from medical education literature suggest that factors that motivate clinical teachers to teach include intrinsic satisfaction of being involved in education, feeling a sense of responsibility to teach medicine and seeing students succeed.21,39 This view is echoed by the findings in this study. Most perceived attitudinal factors that positively influence teaching in this study are found primarily at the personal level, including both intrinsic and altruistic factors. The following quote illustrates this:
I really enjoy teaching personally. I think that imparting information to the younger ones, bringing them up gives me joy. In fact I enjoy it because that is just one of the my passion even at home to my children I like telling them stories and teaching them and the fact that I tell them stories, I also want them to do what is good for them in the stories. (Lecturer 1)
Regarding the status of teaching in this College, it is clear from the study that clinical educators consider teaching to be as important as research in their academic pursuit. On the other hand, similar to previous reports,26,40 there is a perception that teaching does not receive sufficient importance or recognition as evidenced by the fact that 85% of the respondents believe that teaching is not accorded necessary priority and only 15% believing that recognition as a good teacher helps with career advancement. The quote below illustrates this:
Let me tell you, promotion of lecturers is a big problem, it’s only publications and research, publications that take you to the next level, no matter how good you are as a lecturer, that one is between you and your students. So how do they expect one to use extra time to go for training in teaching? Let them include teaching as part of promotion, and then I will know it is important. Now it is not. (Lecturer 10)
Conventional wisdom dictates that those activities or skills which an educational institution values should be adequately rewarded. Until the status of teaching is comparable to research, it is unrealistic to expect those involved to devote the necessary time and effort to teaching and show greater commitment to professional development.41
Studies have investigated the different ways in which doctors have learned to teach, with most of the recent findings relating to acquisition and improvement of pedagogical skills by attendance at formal teacher training program.6 In contrast, a major finding in this study is that while majority of the teachers are primarily employed by the university to teach undergraduate medical students, only 16% had previously attended formal training program in teaching roles. Analyses of the qualitative data suggest that clinical teachers in this college developed their present teaching skills through two major formats: personal learning experiences and informal interaction with fellow colleagues. The following quote illustrates this category:
You see, some of my lecturers in medical college are talented teachers and I tried to take some of their own aspects, even from some senior colleagues. So I have brought a lot of good aspects from many places altogether and that is what I use in teaching now. That is actually all that I try to do, to copy all that I think my former lecturers have been doing well. (Lecturer 5)
This raises concerns about the quality of the teaching, especially when it is taken into account that changes in medical education might have rendered obsolete some of the methods by which their teachers taught them. Accordingly, this study noted that the absence of formal teachers’ training program presents as an important gap in the deployment of doctors as academia at this medical college.
Furthermore, the experience of being taught in medical schools as students influences respondents’ teaching styles and preferences. For example, similar to majority of medical colleges in sub-Saharan Africa,15,16,18 majority of teachers surveyed use lectures and bedside teaching as the predominant approach to teaching, indicating the way they were taught as learners. According to Asani,42 such bedside teaching, however, often involves a large number of students. Even though the issue of bedside teaching has generated a lot of debate in the literature, with some studies in favor of42,43 and some against,44 it is inevitable that in the absence of clinical skills centers, bedside teaching seems to be the only readily available method of transmitting clinical skills to learners at most medical colleges in Africa. Only a few of the clinical teachers surveyed are frequently involved in small group teaching such as seminars and tutorials. Despite its strengths, the considerable burden small group teaching places on manpower resources needs to be acknowledged,45 and may therefore be challenging to readily implement in environments with very little resources.
Role models have been documented as important sources of medical teachers’ development.46,47 Most of the teachers interviewed acknowledged acquiring knowledge and improving skills by observing how known excellent and ‘natural’ teachers in the college teach and also by discussing teaching issues with colleagues. Important features of such community of practice that were mentioned include, among others, involvement of diverse cadres of academic staff in discussions with often varying topics depending on the individuals involved. However, such discussions are usually sporadic and informal. The following quote illustrates this conception:
Am of the opinion that lecturers in this college learn from each other, how far this is the case, I cannot say. But when we mark students scripts together, discuss on the corridor about our problems in classes with each other and with some senior colleagues, I think we gain something from each other. Maybe not always. (Lecturer 2)
This draws attention to the learning that takes place during or between professional tasks, and in some instances without the individual being aware of what is being learned.48 Taking advantage of the current informal peer learning opportunities and overcoming some of the documented limitations (eg, possible assembling of inappropriate knowledge and limited access to appropriate expertise)49 in the implementation of professional development for teachers remains a challenge in this college.
Based on research in higher education, it would be worthwhile to help medical educators see their everyday experiences as “learning experiences” and to make the invisible visible through structured (or formal) faculty development programs. Community of practice provides a well-theorized and practiced framework for collaborative learning in individual, organizational and has been implemented in a wide range of educational and institutional settings.50
Few articles have specifically explored the processes and roles of formal communities of practice in teachers’ development in the field of medical education. In a related profession, Sherer et al51 describe the development of an online community of practice of college teachers through a faculty development portal and cite several benefits of participation, including opportunity to access educational materials and enhance knowledge of teaching through collaboration with colleagues. Furthermore, Jippes et al52 demonstrate how social networks (in a community) can enhance the adoption of an educational innovation.
Taking advantage of current technological options, faculty developers can enhance the opportunity for the entire faculty to learn through the use of online communities. Designing a faculty development portal using community of practice concepts can be an effective means to jump-start, facilitate, develop and sustain a faculty development program in this medical college. Often, clinicians are confronted with several competing tasks, including teaching, research and patient care. As a milieu for professional socialization, van Lankveld et al53 found that communities of practice in medical schools may be particularly helpful in validating and strengthening members professional identity as teachers.
In accordance with findings from other studies,25,26 this study documented support for faculty development program. Despite the fact that about two-thirds of the respondents indicated that their present teaching skills are adequate for their teaching role, majority still felt that formal training would improve the quality of teaching in the College; that they would find training courses useful and would participate in such program. This attitude of double standard suggests that teachers in this college perceive knowledge gained from such training program as an addition to their existing knowledge and not necessarily for personal improvement. Research has shown that faculty may underestimate both their own potential for improvement and that participation may be necessary for a true understanding of the benefits of such program.25 Faculties are therefore encouraged not to rule out participation in a program without careful consideration.
Limitations of the study
This study was conducted in a particular context, namely, a medical college located in one of the six geopolitical regions of Nigeria, which makes generalization of the findings difficult. However, the study may be broadly applicable to similar settings, as the participants provided rich descriptions of their experiences.
Second, the methodological issue regarding the use of self-report and interviews to measure teachers’ own attitude to teaching and perceptions of learning. Although person-bound factors can be well assessed by the clinical teachers themselves to gain insight into teachers’ actions and perceptions, the use of more data sources, such as classroom observations and reflective writings, would benefit further research.
Conclusion and practical implications
Despite these limitations, the findings of this study have some key implications. A significant value of this study lies in the voice it gives the Nigerian medical educators to talk about their experiences of teaching and need for learning. In particular, the existing informal teachers’ development program revealed, represent important findings from the perspective of implementing sustainable formal faculty development activities in this setting. The main question that arises despite clinical teachers’ high enthusiasm for teaching is how to develop and foster participation in learning activities in a situation marked by limited resources. While this study has gone some way in uncovering existing informal learning activities, its greatest value, as one would argue, is the importance of tapping into this in the development of teachers’ formal professional program. The continuous medical education (CME) literature has pointed out that much of the clinical learning of doctors arises from their practice – and must be integrated with it. The same is true for staff development.
Second, a catalyst of learning by teachers’ in this college may come from their belief and self-rating of teaching ability. Because beliefs tend to be implicit, clinical teachers need support to make their beliefs explicit, such as through opportunities to confront the potential inadequacy of those beliefs, and the provision of new information that they can examine, elaborate on and integrate into their existing systems of knowledge and beliefs. Such an examination and adjustment of beliefs could begin through the commencement of formal, structured, learning activities such as workshops and seminars.
Finally, faculty development program can only succeed in settings or contexts that support it. It is recommended that in order to ensure effective clinical teachers’ development program, college leadership must cultivate and develop conditions which are conducive to clinical teachers’ working collaboratively as part of faculty development, as well as encourage the continuous display of a positive attitude toward teaching and faculty development. According to Olasoji,14 faculty development should be a high priority on the medical education agenda of a developing country like Nigeria to improve the skills and knowledge of clinical academia and promote lifelong learning.
Acknowledgments
Warmest thanks are extended to the clinical teachers who were involved in the data collection process, without which this study would not have been possible. The information contained in this article was extracted from a Master’s thesis by the first author, HOO for the award of MSc Medical Education degree program at Cardiff University, UK. Sincere appreciation goes to Lynne Allery, the research supervisor.
Author contributions
All authors contributed towards data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wilkerson L, Irby DM. Strategies for improving teaching practices: a comprehensive approach to faculty development. Acad Med. 1998;73(4):387–396.
2. Biggs JSG, Agger SK, Dent TH, Allery LA, Coles C. Training for medical teachers; a UK survey. Med Educ. 1994;28:99–106.
3. Gibson DR, Campbell RM. Promoting effective teaching and learning: hospital consultants identify their needs. Med Educ. 2000;34:126–130.
4. MacDougall J, Drummond MJ. The development of medical teachers: an enquiry into the learning histories of 10 experienced medical teachers. Med Educ. 2005;39:1213–1220. doi:10.1111/j.1365-2929.2005.02335.x
5. Towle A. Staff development in UK medical schools. In: Jolly B, Ress L, editors. Medical Education in Millennium. Oxford: Oxford Medical Publications; 1998:205–210.
6. Steinert Y, Mann K, Centeno A, et al. A systematic review of faculty development initiatives designed to improve teaching effectiveness in medical education: BEME guide no. 8. Med Teach. 2006;28(6):497–526. doi:10.1080/01421590600902976
7. Mclean M, Cilliers F, Van Wyk J. Faculty development: yesterday, today and tomorrow. Med Teach. 2008;30(6):555–584. doi:10.1080/01421590802109834
8. General Medical Council. The Doctor as Teacher. London: GMC; 1999.
9. General Medical Council. Good Medical Practice. London: GMC; 2001.
10. Kiguli-Malwadde E, Olapade-Oluwabunmi O, kiguli S, et al. Competency-based medical education in two Sub-Saharan African medical schools. Adv Med Educ Prac. 2014;5:483–489. doi:10.2147/AMEP.S68480
11. Malu AO. University and medical education in Nigeria. Nig Med J. 2010;52(2):84–88.
12. Schofield SJ, Bradley S, Macrae C, Nathwani D, Dent J. How we encourage faculty development. Med Teac.h. 2010;32(11):883–886. doi:10.3109/0142159X.2010.506564
13. Olasoji HO. Addressing the issue of faculty development for clinical teachers in Nigeria. Nig J Clin Pract. 2014;17(2):265–266. doi:10.4103/1119-3077.127576
14. Olasoji HO. Feedback after continuous assessment: an essential element of students’ learning in medical education. Nig J Clin Pract. 2016;19(5):692–694. doi:10.4103/1119-3077.188696
15. Gukas ID. Global paradigm shift in medical education: issues of concern for Africa. Med Teach. 2007;29:887–892. doi:10.1080/01421590701814286
16. Ibrahim M. Medical education in Nigeria. Med Teach. 2007;29:901–905. doi:10.1080/01421590701832130
17. Olukoya A. Teaching medical teachers how to teach in Lagos, Nigeria. Med Teach. 1986;8(2):145–148.
18. Jarrett JL. The Teaching Values: Caring and Appreciation. London: Routledge; 1991.
19. Borg M. Teachers’ beliefs. ELT Journal. 2001;55(2):186–188. doi:10.1093/elt/55.2.186
20. Çiğdem H. Determine the attitudes of teachers towards professional activities. Prosedia Tech. 2012;1:420–425. doi:10.1016/j.protcy.2012.02.094
21. Dybowski C, Harendza S. “Teaching is like nightshifts … .” A focus group study of teaching motivations of clinicians. Teach Learn Med. 2014;26(4):393–400. doi:10.1080/10401334.2014.910467
22. National Population Commission (NPC). (2013). Available From: http://www.mdcnigeria.org/.
23. Harden RM, Snowden S, Dunn WR. Some educational strategies in curriculum development: the SPICES model. Med Educ. 1984;18:284–297.
24. Greene JC, Caracelli VJ, Graham WF. Toward a conceptual framework for mixed method education designs. Educ Eval Policy Anal. 1989;11(3):255–274. doi:10.3102/01623737011003255
25. Finucane P, Allery LA, Hayes TM. Attitudes to teaching among teachers at a british medical school. Med Educ. 1994;28:213–219.
26. Finucane P, Allery LA, Hayes TM. Comparison of teachers at a ‘traditional’ and ‘innovative’ medical school. Med Educ. 1995;29:104–109.
27. Bernard HR. Research Methods in Anthropology: Qualitative and Quantitative Methods.
28. Miles MB, Huberman AM. Data management and analysis methods. In: Denzin NK, Lincoln YS, editors. Collecting and Interpreting Qualitative Materials. Thousand Oaks, CA: Sage; 1998:179–210.
29. Cook DT, Cook DT. Knowing the child consumer: historical and conceptual insights on qualitative children’s consumer research. Young Consumers. 2009;10:269–282. doi:10.1108/17473610911007111
30. Adegun OA. Gender factor and labour participation among academic staff in tertiary institutions in Ekiti State, Nigeria. Eur J Educ Stud. 2012;4(2):249–258.
31. Egun AC, Tibi EU. The gender gap in vocational education: increasing girls access in the 21st century in Mid Western states of Nigeria. Int J Voc Tech Educ. 2012;2(2):18–21.
32. Medical School Council. Women in Clinical Academia: Attracting and Developing the Medical and Dental Workforce of the Future. London: MSC; 2007.
33. World Health Organization. Transforming and Scaling up Health: Professional Education and Training Policy Brief on Faculty Development. Geneva: WHO; 2013.
34. Mullan F, Frehywot S, Omaswa F, et al. Medical schools in Sub-Saharan Africa. Lancet. 2011;377:1113–1121. doi:10.1016/S0140-6736(10)61961-7
35. Bundred P, Gibbs T. Medical migration and Africa: an unwanted legacy of educational change. Med Teach. 2007;29:893–896. doi:10.1080/01421590701814278
36. Masters PH, Nester C. A study of primary care teaching comparing academic and community –based settings. J Gen Intern Med. 2001;16(1):9–13. doi:10.1111/j.1525-1497.2001.91126.x
37. Anyaehie USB, Nwobodo E, Oze G, et al. Medical students’ evaluation of physiology learning environment in two Nigerian medical schools. Adv Physiol Educ. 2011;35:146–148. doi:10.1152/advan.00106.2010
38. Mkony CA, Kaaya EE, Goodell AJ, Macfarlane SA. Where teachers are few: documenting available faculty in five tanzanian medical schools. Glob Health Action. 2016;9(1):32717. doi:10.3402/gha.v9.32717
39. Starr S, Ferguson WJ, Haley HL, Quirk M. Community preceptors’ views of their identities as teachers. Acad Med. 2003;78:820–825.
40. Hendry RG, Kawai GK, Moody WE, et al. Consultant attitudes to undertaking undergraduate teaching duties: perspectives from hospitals serving a large medical school. Med Educ. 2005;39:1129–1139. doi:10.1111/j.1365-2929.2005.02320.x
41. Hanson PA, Roberts KB. Putting teaching back at the center. Teach Learn Med. 1992;4:136–139. doi:10.1080/10401339209539551
42. Asani M. Bedside teaching: an indispensable model of patient-centred teaching in undergraduate medical education. Niger J Basic Clin Sci. 2014;11(2):57–61. doi:10.4103/0331-8540.140305
43. Wang-Cheng RM, Barnas GP, Sigmann P, Riendl PA, Young MJ. Bedside case presentation: why patients like them but learners don’t. J Gen Intern Med. 1989;4:284–287. doi:10.1007/bf02597397
44. Nair B, Coughlan J, Hensley M. Student and patient perspective on bedside teaching. Med Educ. 1997;31:341–346.
45. Meo SA. Basic steps in establishing effective small group teaching sessions in medical schools. Pak J Med Sci. 2013;29:1071–1076.
46. Bligh J. Learning by example. Med Educ. 1999;33:234–235.
47. Wright SM, Kern DE, Kolodner K, Howard DM, Brancati FL. Attributes of excellent attending physicians role models. N Engl J Med. 1998;339:1986–1993. doi:10.1056/NEJM199812313392706
48. Eraut M. Informal learning in the workplace. Stud Cont Educ. 2004;26(2):247–273. doi:10.1080/158037042000225245
49. Billet S. Workplace learning: its potential and limitations. Educ and Train. 1995;37(5):20–27. doi:10.1108/00400919510089103
50. Churchman D, Stehlik T. Transforming academic work: communities of practice in Australian universities. J Organ Trans Soc Change. 2007;4(3):263–278. doi:10.1386/jots.4.3.263_1
51. Sherer P, Shea D, Kristensen T. Online communities of practice: a catalyst for faculty development. Innov High Educ. 2003;27(3):183–194. doi:10.1023/A:1022355226924
52. Jippes E, Steinert Y, Pols J, Achterkamp MC, van Engelen JM, Brand PL. How do social networks and faculty development courses affect clinical supervisors’ adoption of a medical education innovation? An exploratory study. Acad Med. 2013;88(3):398–404. doi:10.1097/ACM.0b013e318280d9db
53. van Lankveld T, Schoonenboom J, Kusurkar R, Beishuizen J, Croiset G, Volman M. Informal teacher communities enhancing the professional development of medical teachers: a qualitative study. BMC Med Educ. 2016;16:109. (Retrieved June 14, 2018). doi:10.1186/s12909-016-0632-2
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.