Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
A Structured Educational Intervention Aims to Improve Pneumococcal Vaccination Practices in Primary Healthcare Centers
Authors Alqifari SF ![]() , Binswelim MA
, Binswelim MA ![]() , Atia TH, Alzaaq RB, Mouzhir R, Amirthalingam P
, Atia TH, Alzaaq RB, Mouzhir R, Amirthalingam P ![]()
Received 8 October 2022
Accepted for publication 9 January 2023
Published 19 January 2023 Volume 2023:16 Pages 175—179
DOI https://doi.org/10.2147/JMDH.S392685
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Saleh F Alqifari,1,2 Mohammed A Binswelim,3 Tasneem H Atia,4 Renad B Alzaaq,4 Rim Mouzhir,4 Palanisamy Amirthalingam1
1Faculty of Pharmacy, University of Tabuk, Tabuk, Kingdom of Saudi Arabia; 2College of Dentistry & Pharmacy, Buraydah Colleges, AlQassim, Kingdom of Saudi Arabia; 3College of Medicine, Qassim University, AlQassim, Kingdom of Saudi Arabia; 4College of Medicine, Sulaiman Alrajhi University, AlQassim, Kingdom of Saudi Arabia
Correspondence: Saleh F Alqifari, Department of Pharmacy Practice, Faculty of Pharmacy, University of Tabuk, Tabuk, Kingdom of Saudi Arabia, Email [email protected]
Objective: The Centers for Disease Control and Prevention (CDC) provide evidence-based recommendations on vaccine use in the US Current CDC recommendations for the two available pneumococcal vaccine types can be confusing for providers and nursing staff, introducing the potential for administering the wrong product to patients. The pneumococcal vaccine products come with specific recommendations and target-specific patient groups. This intervention aims to improve pneumococcal vaccine practices per CDC recommendations, at primary health-care centers in Saudi Arabia.
Materials and Methods: This intervention is conducted with nursing staff and mid-level providers. An educational intervention consisting of a five-question assessment questionnaire and containing brief scenario cases on pneumococcal vaccine indication. The assessment questionnaire was administered twice separated by a brief educational session on proper vaccine use by a clinical pharmacist. The educational intervention and the pre/post assessment required 15 min to complete. Assessments were collected, and a pre-intervention assessment was compared with a post-intervention assessment to capture the effect of the educational intervention. Test score changes from the baseline were analyzed via a paired Student’s t-test.
Results: Eighty-five nursing staff and mid-level providers completed the assessment. Questionnaire scores signaled an improvement trend in both centers, but the results were not statistically significant in center 1 (p=0.767) and center 2 (p=0.125).
Conclusion: Focusing education on nursing staff by clinical pharmacists on proper vaccine use does not appear to be as effective as previously thought. The desire for improvement in practices was evident in the overwhelming desire to participate in the educational session by nursing staff and mid-level providers. However, the results reflect the complex nature of vaccine practices and the need for further training on proper vaccine use for nursing and mid-level providers.
Keywords: pneumococcal vaccine, vaccines, public health, primary care, clinical pharmacy
Introduction
Pneumococcal infection accounts for around 30% of all adult pneumonia infections in developed nations, including a fatality percentage ranging from 11% to 40%. In recognition of this infection’s risk of morbidity and mortality in adults and children, healthcare efforts over the last 30 years have concentrated on immunizations to minimize the rate of pneumococcal infections.1 Thus, the Centers for Disease Control and Prevention (CDC) offer recommendations on vaccine use in the US Current CDC recommendations for the two pneumococcal vaccine products can be confusing for providers and nursing staff, introducing the potential for administering the wrong product. The pneumococcal vaccine products come with specific recommendations and target-specific patient groups. PCV13 (Prevnar 13®) is active against 13 strains of pneumococcal bacteria and is indicated for adults 65 years or older or adults with conditions such as human immunodeficiency virus (HIV) infection, organ transplantation, leukemia, lymphoma, and kidney disease. PPSV23 (Pneumovax®) is active against 23 strains of pneumococcal bacteria and is indicated for adults 65 years or older and smoker adults 19 to 64 years and individuals with asthma. Considering two distinct vaccines are in circulation, special caution is urged as documented incidents of wrong administration have been documented. Therefore, education on vaccination among healthcare providers is warranted. Furthermore, the intervention was sought because of an organizational-wide report that spanned 12 months of data and included all pneumococcal vaccine encounters. The report captured approximately 2000 pneumococcal vaccine encounters. After careful evaluation of each encounter, investigators noted around 100 inappropriate vaccine encounters that did not follow CDC recommendations for pneumococcal vaccines. Vaccine encounters were deemed inappropriate due to inappropriate indications based on the patient’s risk factors, inappropriate vaccine interval, or inappropriate vaccine product selection. Investigators designed this study to better identify a follow-up action plan to improve adherence to vaccine practices at primary health centers. This study aims to improve practices in prescribing PCV13 or Prevnar 13® and the subsequent PPSV23 or Pneumovax® per CDC guidelines in primary healthcare centers.
Materials and Methods
The targeted population includes nursing staff and mid-level providers in two different primary healthcare centers. The intervention is only done with nursing staff and mid-level providers, and no interaction between investigators and patients occurred. Inclusion criteria included nursing staff and mid-level providers who handle or administer vaccines, attended educational sessions, and provided written consent. The educational intervention consists of a five-question assessment questionnaire that contains brief scenario cases about the proper use of pneumococcal vaccine products (Supplement 1). The same assessment was administered twice, labeled as pre-test and post-test, where the two trials were separated by a brief educational session on the CDC's pneumococcal vaccine recommendations. The educational intervention and the pre/post assessment required 15 min to complete. The assessment questions were developed by investigators and validated by expert reviews for face validity. Assessment cases were repeated in a scrambled fashion in the post-test assessment. Assessments were collected, and pre-intervention assessments were compared with a post-intervention assessment to capture any potential changes in vaccine prescribing trends. All raw scores were added for pre- and post-intervention and then converted to percentages and the mean ± standard deviation values were used to describe normally distributed continuous data. A two-sample t-test was used to compare the means between groups. Both pre- and post-assessments were printed on a two-sided page to pair the results of pre/post-assessment for each participant. Assessments were anonymous with no subject identifiers collected. Collected information included only the level/rank of practice for subjects (Licensed Practical Nurse (LPN), Medical Assistance (MA), and Registered Nurse (RN)). The results of this study will help improve practices in prescribing various pneumococcal vaccine products at primary care centers.
Results
Eighty-five total nursing staff and mid-level providers completed the assessment in two separate centers. The demographics of study participants are comparable in centers 1 and 2 (p=0.386). In center 1, the participants were 3 Licensed Practitioner Nurses (LPN), 13 Registered Nurses (RN), and 24 Medical Assistants (MA). Meanwhile, for center 2, the participants were 8 Licensed practitioner nurses (LPN), 14 Registered nurses (RN), and 24 Medical Assistants (MA).
The paired t-test which is used to compare pre- and post-results for centers 1 and 2 respondents is represented in (Table 1). It indicates that the pre-test score of centers 1 for LPN, RN, and MA (M=3.02, SD=1.07) are higher than that of the post-test scores (M=2.98, SD=1.31), but not significantly different (p=0.767). A similar pattern is observed in center 2 as it reveals that the pre-test result for LPN, RN, and MA (M=3.96, SD=0.90) is higher than that of the post-test (M=3.72, SD=1.07) but not statistically significant (p=0.125) showing a general trend of reduction in post-test scores in both centers.
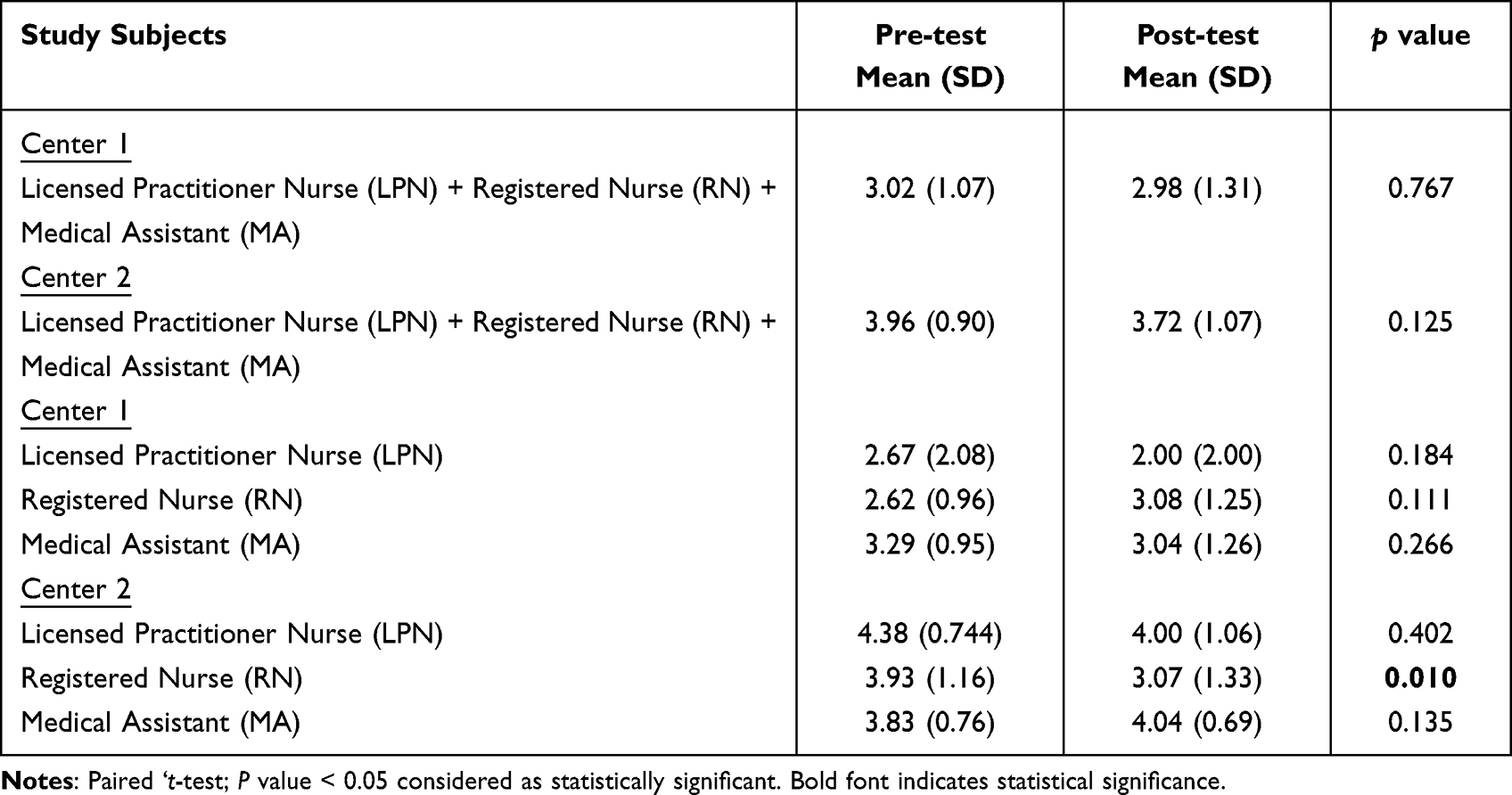 |
Table 1 Pre- and Post-Test Scores of the Study Population |
Furthermore, data analysis revealed that the pre-test score is higher for most cases than the post-test but not statistically significant in both centers.
Discussion
Educational interventions were adapted by several studies measuring the effectiveness of various educational modalities for healthcare providers and staff. The study sought to measure the effect of multidisciplinary educational activity in private pediatrics and family medicine practices. The study noted a noticeable increase in the urge to dispense vaccines to patients’ post-educational activity. Furthermore, the rate of vaccination records checking for patients who sought medical help for reasons other than vaccination has shown some growth (p=<0.05). Small offices were markedly influenced by the educational activity compared to larger centers.2
Berenson et al investigated whether a 30 min structured presentation could improve physicians, non-physician healthcare workers, and medical students’ practice related to the human papillomavirus (HPV) vaccination. Similar to our protocol, a few cases were administered separated by an educational intervention. The sample consisted of 208 medical students, 144 nurses or other healthcare workers, and 75 physicians. The post-lecture scores significantly improved in comparison to the pre-lecture score (p=<0.001), regardless of specialty, race, gender, and age. Scores of younger participants and non-physician healthcare workers showed more improvement than other groups. The team concluded that a brief, structured presentation increased HPV knowledge among a variety of healthcare workers, even when their baseline knowledge was low.3
Unfortunately, this study showed that an educational program for nurses regarding protocols for administering pneumococcal vaccines was not as effective as expected. After analysis, no significant difference was shown between participants’ pre- and post-assessment overall scores. This raises concerns about educational interventions among healthcare practitioners and whether more novel methods should be initiated. Similar results were found by Huizing et al in a study conducted in the Netherlands investigating the role of educational intervention proposed by nursing staff to reduce the use of physical restraints with psychogeriatric nursing home residents. It showed similar results to this study, as the educational intervention was not effective as aimed.4 It is debatable whether the intervention was ineffective or whether the targeted group, which was nursing staff and mid-level providers, needed a different method of education. Education methods come in different types such as visual, active, auditory, or innovative. This ideology was adopted by numerous studies debating the preferred style of education for nurses. Alharbi et al suggested a more visual route is preferred among nursing staff after they surveyed 56 respondents out of 130 nursing students selected, resulting in 67.9% of the respondents preferring visual education.5 Also, Mangold et al performed a similar study focusing on the preferred style of education among nursing staff with a larger sample of 2071 and 1399 respondents, revealing a pattern of visual education preference.6 Considering the importance of educational methods used, we believe that multiple methods are critical to achieving the desired outcome. Nevertheless, our study highlights the knowledge gaps to be filled regarding vaccine education. Contrary to our results, vaccine administration education secured improvement in vaccination knowledge. Similar to a study from Jordan, which recommended enrollment of pharmacists in immunization education and prescription to improve pneumococcal vaccine coverage among the elderly. In the study, after pharmacists-led educational activity to elderly patients regarding pneumococcal vaccines, an improvement in vaccine coverage by 1.9% (p= 0.008) was observed.7 Another study from the US aimed to identify nurse practitioner (NP) barriers to herpes zoster vaccine (HZV) administration and then use these results to develop and evaluate the outcomes of an educational program. In Phase 1 of a two-phase design, primary care (NPs) with practice years ranging from 1 to 24 possessed limited knowledge of the vaccine, especially the financial aspects. In Phase 2, there was a statistically significant difference in the knowledge survey, demonstrating (NPs’) improved understanding of HZV.8
Our study revealed an interesting finding in our selected group as we observed a consistent decline in post-exam results. With similar findings in different studies, we noted the urge to improve the methodology of our structured learning in future interventions. We propose a multi-approach educational system that covers visual, active, auditory, and innovative methods. We believe simple changes like adding picture-based boards on the walls of nurse stations or halls could perhaps provide a significant improvement in vaccine practices.
Conclusions
In conclusion, focused educational intervention on proper vaccine use does not appear to be as effective as previously thought. The desire for improvement in practices was evident in the overwhelming desire for participation in educational sessions by nursing staff and mid-level providers. However, the results reflect the complex nature of vaccine practices and the need for further training on proper vaccine use for nursing and mid-level providers.
Data Sharing Statement
All the provided data of this study are available by contacting the corresponding authors upon request.
Ethical Consideration
Study protocol #1443-1-12 is approved by the Research Ethics Committee at Buraydah Colleges – Qassim, Saudi Arabia.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The corresponding author declares former affiliation to the College of Dentistry & Pharmacy, Buraydah Colleges, AlQassim, Kingdom of Saudi Arabia. The authors report no conflicts of interest in this work.
References
1. Bridy-Pappas AE, Margolis MB, Center KJ, Isaacman DJ. Streptococcus pneumoniae: description of the pathogen, disease epidemiology, treatment, and prevention. Pharmacotherapy. 2005;25(9):1193–1212. doi:10.1592/phco.2005.25.9.1193
2. Boom JA, Nelson CS, Laufman LE, Kohrt AE, Kozinetz CA. Improvement in provider immunization knowledge and behaviors following a peer education intervention. Clin Pediatr. 2007;46(8):706–717. doi:10.1177/0009922807301484
3. Berenson AB, Rahman M, Hirth JM, Rupp RE, Sarpong KO. A brief educational intervention increases providers’ human papillomavirus vaccine knowledge. Hum Vaccin Immunother. 2015;11(6):1331–1336. doi:10.1080/21645515.2015.1022691
4. Huizing AR, Hamers JP, Gulpers MJ, Berger MP. A cluster-randomized trial of an educational intervention to reduce the use of physical restraints with psychogeriatric nursing home residents. J Am Geriatr Soc. 2009;57(7):1139–1148. doi:10.1111/j.1532-5415.2009.02309.x
5. Alharbi HA, Almutairi AF, Alhelih EM, Alshehry AS. The learning preferences among nursing students in the King Saud University in Saudi Arabia: a cross-sectional survey. Nurs Res Pract. 2017;2017:3090387. doi:10.1155/2017/3090387
6. Mangold K, Kunze KL, Quinonez MM, Taylor LM, Tenison AJ. Learning style preferences of practicing nurses. J Nurses Prof Dev. 2018;34(4):212–218. doi:10.1097/NND.0000000000000462
7. Abu-Rish EY, Barakat NA. The impact of pharmacist-led educational intervention on pneumococcal vaccine awareness and acceptance among elderly in Jordan. Hum Vaccin Immunother. 2021;17(4):1181–1189. doi:10.1080/21645515.2020.1802973
8. O’Donnell M, Shurpin K, Janotha B. Improving herpes zoster vaccine rates: the impact of a targeted educational program. J Am Assoc Nurse Pract. 2018;30(8):435–440. doi:10.1097/JXX.0000000000000039
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.