Back to Journals » International Journal of Women's Health » Volume 15
A Strategy for Reducing Maternal Mortality in Rural Kenya
Authors Masaba BB ![]() , Mmusi-Phetoe R
, Mmusi-Phetoe R ![]()
Received 16 December 2022
Accepted for publication 13 March 2023
Published 3 April 2023 Volume 2023:15 Pages 487—498
DOI https://doi.org/10.2147/IJWH.S396257
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Brian Barasa Masaba, Rose Mmusi-Phetoe
Department of Health Studies, University of South Africa (UNISA), College of Human Sciences, School of Social Sciences, Pretoria, South Africa
Correspondence: Brian Barasa Masaba, Email [email protected]
Background: Migori County is categorized among regions with worst maternal survival rates in Kenya. The county’s current maternal mortality ratio (MMR) is 673 deaths per 100 000 live births. A need exists for a context-specific strategy to mitigate the persistent high maternal mortalities in rural Kenya. The researchers aimed to develop a strategy for reducing the maternal mortality ratio (MMR) in Migori, Kenya.
Methods: An explanatory sequential mixed methods design was utilised. The design was characterised by two separate studies, an initial quantitative followed by a qualitative study. The final phase entailed integration of data from the two separate studies. The findings, extensive literature review and three delays of maternal mortality theoretical framework informed the development of the strategy.
Results: The strategy for implementation considered three strategic areas, namely, interventions targeting first delays, interventions targeting second delays, interventions targeting third delays.
Conclusion: The priority interventions needed are those that enable: 1) Pregnant mothers to receive quality peripartum care in Migori hospitals, 2) Strengthened and efficient referral systems of obstetric emergencies and 3) Community knowledge empowerment on safe pregnancy and culture shift. These interventions would significantly transform the health-care system towards maternal mortality reduction. The Kenyan government and non-profit organisations should be involved in the implementation of the proposed strategy.
Keywords: community empowerment, determinants, health systems, interventions, maternal delays, maternal mortality, obstetric care, obstetric complications, pregnancy, quality care, referral, strategy
Introduction
Current worldwide estimates indicate that,295000 mothers die annually.1 In 2017, sub-Sahara was the leading region with very high maternal mortality ratio (MMR) of 542/100 000 live births.2 In the same region, South Sudan, Chad and Sierra Leone are countries that had extremely high MMR of 1150, 1140 and 1120, respectively.2 In 2015, Kenya was categorised among 18 sub-Saharan countries with very high MMR.1 The country’s reduction of MMR has been slow with a decline of 432 in 2010 to 353/100 000 live births in 2015.1 The current Kenya’s MMR is 362/100,000 live births.3 The UNDP4 note that, in 2015, world leaders envisioned reducing maternal mortality ratio to less than 70/100,000 live births by the year 2030 through Sustainable Development Goals (SDG).4 The current global MMR is 210/100,000.4 In order for Kenya to meet the MMR target of 140/100,000 by 2030 an annual rate reduction (ARR) of at least 8.6% is needed.5
In 1987, WHO held an international conference in Nairobi, Kenya, to advocate for global maternal mortality reduction through the introduction of Safe motherhood Initiative.6 The initiative’s visionary goal was to end preventable maternal mortality.7,8 A better knowledge of distal and proximal causes of maternal mortality has resulted in the current global shift from SMI to “Ending Preventable Maternal Mortality (EPMM)” in 2014 in Bangkok.7 The current EPMM strategy champions beyond clinical care to address socio-economic and political determinants of maternal survival.7 A Consensus Statement by United Nations member states was that they recognised EPMM as an achievable strategy. Its progress could be further accelerated through anchoring maternal survival across lifespan of women’s health and their right to healthcare.9,10
Theoretical Underpinning
Notable empirical conceptual frameworks on factors specifically influencing maternal mortality and their related causes are the frameworks proposed by McCarthy and Maine and Thaddeus and Maine.11 Despite the fact that the Thaddeus and Maine framework was developed a long time ago, it was found to still be relevant and inclusive of most determinants pertinent to maternal health outcomes in rural settings like Migori County.12 Thaddeus and Maine framework proposed three phases of delays that hinder a woman in need of maternal care from receiving optimal treatment. The delays range from; delays in decision-making by the family, reaching hospital to delays in receiving care upon hospital admission.13 The three delays framework helps identify maternal deaths across the pathway from home (community) to hospital. The researchers posit that, designing a strategy to mitigate these context-specific delays can help reduce maternal mortalities.14 In the present study, the first delay factors included factors such as socio-demographic and maternal health variables; maternal age, parity, marital status, educational level, residence, antenatal clinic attendance and gestation. The second delay factors informed analysis of factors such as affordability of care, availability of transport and distance to the hospital. The third delay factors of the model were used to help the researchers assess the quality of care and availability of staff and equipment, and healthcare system factors contributing to maternal deaths. Based on this, researchers developed a strategy for reducing the maternal mortality ratio (MMR) in Migori, Kenya, along the three delay factor pathway.
Methodology
An explanatory sequential mixed methods design was utilised for this study conducted between January 2020 and November 2022 (Table 1). The design was characterised by two separate studies, an initial quantitative – Masaba et al’s study15 followed by a qualitative – Masaba et al’s survey.16,17 The final step entailed integration or linking of data from the two separate strands of studies.18 The findings and an extensive literature review informed the development of a strategy for reducing the MMR in Migori, Kenya. The two study findings were anchored on the three delays of maternal mortality theoretical framework (Table 1). In regard to study setting; three hospitals that are referral centers in Migori County were purposively selected. The selection criterion of the hospitals was based on the referral capacity and number of admissions in their respective peripartum units. Only those with a referral capacity and had high admissions among the 19 hospitals in the county were utilised.19 The two aforementioned studies were conducted in the three hospitals of which two were public while one was private. Based on integration of the results of quantitative and qualitative studies, summary statements were made. For each summary, an interim strategy statement was formulated, and an intervention stated. Thereafter, review forms of the interim strategy statements were emailed to five reproductive health experts for validation (see Table 2). Reproductive health experts were purposefully sampled. The researchers requested a detailed list of reproductive health experts from Migori County Ministry of Health. The reproductive health experts were selected based on the following considerations: they 1) were consultants in reproductive health, 2) had experience in policy formulation on maternal health, and 3) were managers in their respective organisations. The reproductive health experts were oriented on the present study’s purpose and protocols before participating in the review process (Table 3). The researchers requested to be provided with feedback of the completed review and validation forms by email. The experts (Table 3) in maternal health reviewed the developed strategy by focusing on the following elements: acceptability, applicability, clarity, effectiveness, feasibility, relevance, sustainability and validity (Table 2). A strategy was accepted in reference to the review comments and score ratings. An average score of >6 of a strategy by all experts participating in the review was considered. Additionally, review comments were used to revise and improve the formulated strategy. Table 4 illustrates the outcome of the validation feedback by the selected reviewers. The least (32/40) scored strategy was 1.6, while the highest strategy 1.7 scored 38 points. Further analysis reveals that all the strategic areas met the inclusion criteria that had been predetermined. The reviewers gave insightful comments against each strategy that were incorporated in the presented proposed strategy.
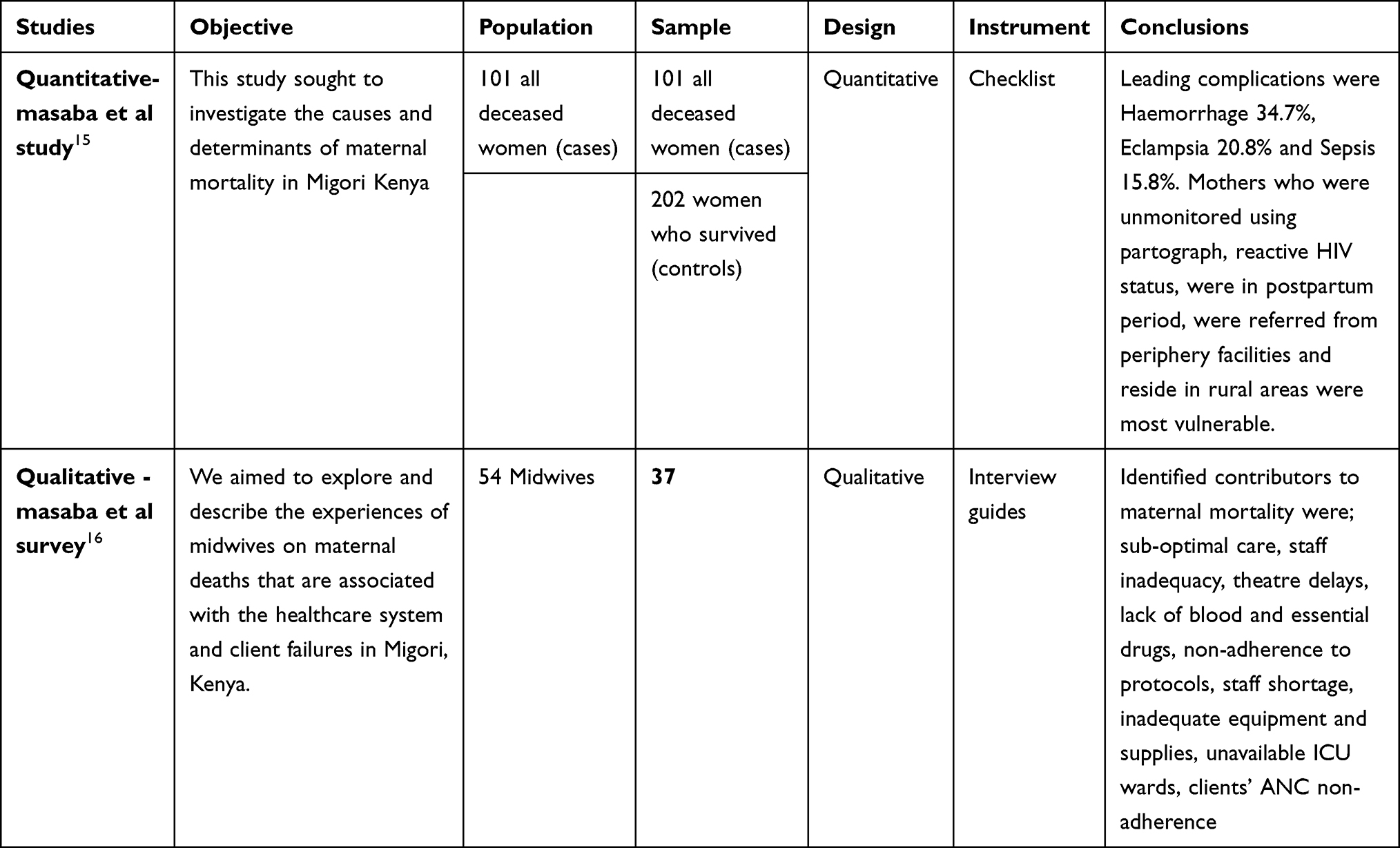 |
Table 1 Description of the Two Studies, Objectives, Populations and Sample Sizes |
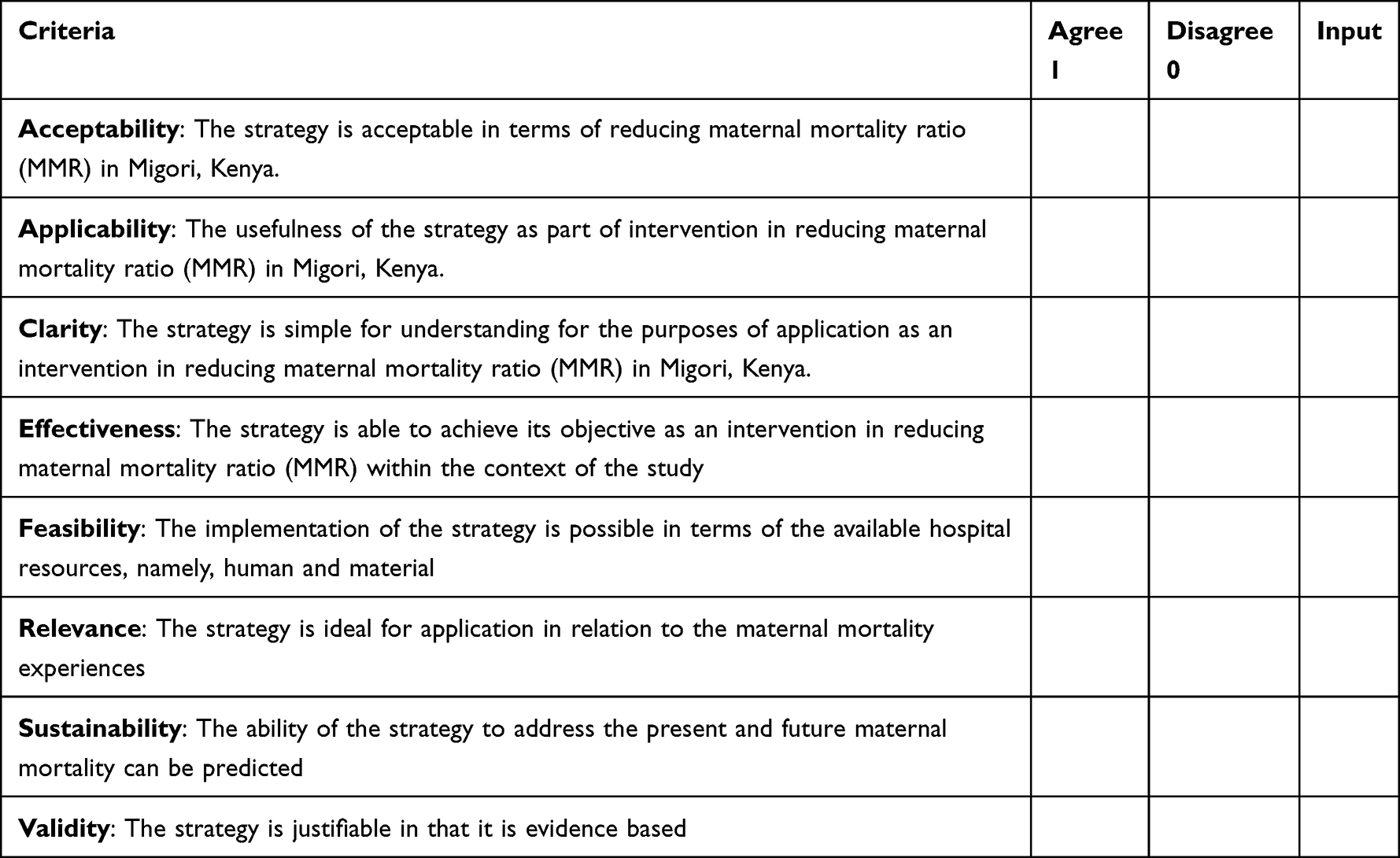 |
Table 2 Scoring Criteria and Description of Validating Each Strategy |
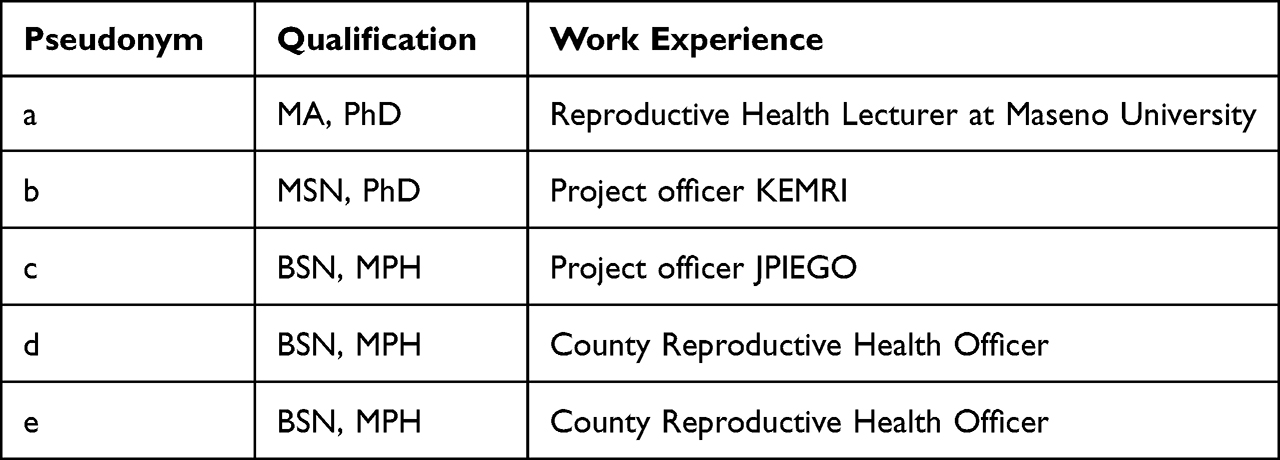 |
Table 3 Health Experts’ Demographics |
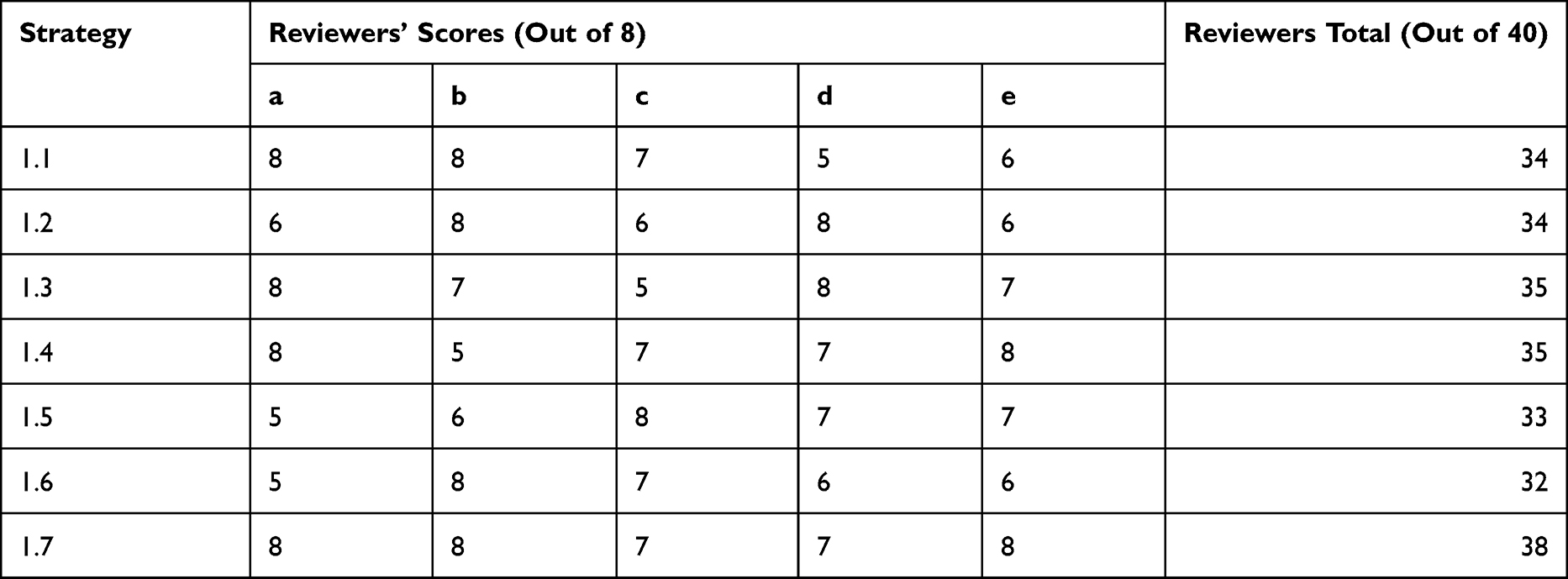 |
Table 4 Outcome of Validation by Reviewers |
Ethical Considerations
The study was approved (Registration: Rec-240816-052) by the Ethical Review Board of the University of South Africa (UNISA). Anonymity was ensured by pseudonym labelling of all participants and hospitals. Further, participation was by voluntary. All the mentioned participants were requested to sign informed consents. This study conforms to the principles outlined in the Declaration of Helsinki.
Findings
The researchers integrated the quantitative masaba et al study’s data15 and the qualitative – Masaba et al survey’s data.16 This was through juxtaposing the respective summarised results by a side-by-side joint display in order to draw meta-inferences.18,20,21 The major findings noted upon integration are the causes and three delay factors of maternal deaths in Migori County.
Causes of Maternal Mortality
The researchers found that the leading causes of maternal mortalities in the selected hospitals were haemorrhage 34.7%, eclampsia 20.8% and sepsis 15.8%. The findings also indicated that the Migori region has chronic blood shortages. This can mean that the cases that developed haemorrhage were inadequately managed. In-depth interviews indicated that drug shortages, inadequate patient monitoring, and slowness in management of cases with eclampsia might have contributed to their poor outcome (death). For sepsis cases, they were vulnerable to inappropriate care, and erratic drug supply in the hospitals.
Factors Contributing to First Delays
The study findings noted causes of first delays and non-utilisation of maternal health-care interventions. Medical records’ review revealed that most (44.6%) of the cases had a primary level of education, while 32.7% had attained secondary education. Although the study was facility based, 7.9% of women had home deliveries. Most (93.1%) of the reviewed cases were Christian, 71.3% were married, and 21.8% were single. In-depth interviews indicated that most vulnerable mothers were ignorant of obvious danger signs and poorly schooled; they were negatively influenced by old traditions, myths, perceptions and culture. This caused them to opt for home deliveries with the use of traditional birth attendants (TBAs) and herbal drugs. Patriarchy’s decision-making power hindered some mothers in need from getting prompt services. Participants further noted negative influences of Roman Catholic and Legio religions that are dominant in the county. It can be concluded that both data sets reveal that most mothers vulnerable to first delays are those poorly educated and those negatively influenced by religion, culture and traditional practices and beliefs.
Factors Contributing to Second Delays
Findings demonstrate that once a mother decides to get hospital interventions, she is vulnerable to second delays (challenges of access to maternal health care interventions). Quantitative data indicated that most cases (68.3%) were from rural regions, 44.6% were unemployed, and 37.6% were working in the informal sector. On the other hand, participants’ interviews revealed that most mothers were from remote residences (spending more than two hours on road), the region has a poor road network, the cost of transport is prohibitive and public vehicles are limited. Both data sets therefore illustrate that rural residence and unaffordable transport due to poor roads are major causes of second delays.
Factors Contributing to Third Delays –Hospital System Failures
Mothers with obstetric emergencies need prompt referral services to tertiary hospitals for the appropriate care. Quantitative data showed that most (66.3%) of the cases were referrals. Additionally, 52.5% of the cases spent less than 24 hours in the hospital upon admission, whilst the qualitative data revealed several referral challenges mothers face, including protocol delays, poorly staffed ambulances, inadequate and out of service ambulances. It can therefore be concluded that both sets of results revealed that mothers were vulnerable to referral delays.
The findings indicate that multiple hospital system challenges and failures are hindering maternal care interventions. Quantitative data reveal that 75.2% of the cases at least attended antenatal care (ANC). Interviews demonstrated that there are gaps in ANC care, such as inadequate birth plan preparedness, non-adherence to ANC visits, and unaffordable service cost of ANC profiles. The qualitative data sets explain (quantitative data) that the majority of cases (deceased mothers) who attended ANC visits were vulnerable to suboptimal ANC care and associated unaffordable direct charges.
Quantitative data show that 44.6% had caesarean section (C/S), 38.6% had spontaneous vertex delivery (SVD), 1% had vacuum-assisted delivery. In addition, qualitative study yielded sub-themes such as inadequate resuscitation supplies, theatre-related delays, inappropriate care and lack of blood. The qualitative data sets explain (quantitative data) that although most of the cases had complications warranting C/S, the hospitals were poorly prepared to handle the emergencies.
In regard to point of care, most (64.4%) of the cases were in the postpartum period compared to 18.8% in intrapartum. This emphasises the need for more efforts during postpartum care, where most mothers are vulnerable.
Further, quantitative data reveal that 67.3% were not monitored using a partograph, the latter was used for only 32.7%. Qualitative data illustrated non-adherence to patient management guidelines and poor monitoring. It can therefore be concluded that both sets of results revealed that hospitalised mothers were poorly monitored.
Lastly, quantitative data illustrate that delivery of the majority (48.5%) of the cases was cared for by nurses, 44.6% by doctors and 6.9% by TBAs. The qualitative data demonstrates staff shortages, health-care providers with negative attitudes, staff slowness in service, and demotivated staff. The qualitative data sets explain (quantitative data) that although the cases were cared for by Skilled Birth Attendants (SBAs), they were vulnerable to suboptimal care caused by staff challenges.
Discussion
The researchers believe that the proposed interventions are not mutually exclusive. Addressing one could lead to a beneficial direct or indirect impact on multiple other interventions. In addition, a delay or a challenge to maternal care in Migori County can be mitigated by either one or multiple interventions. Figure 1 illustrates the framework of interventions to be implemented for the proposed strategy.
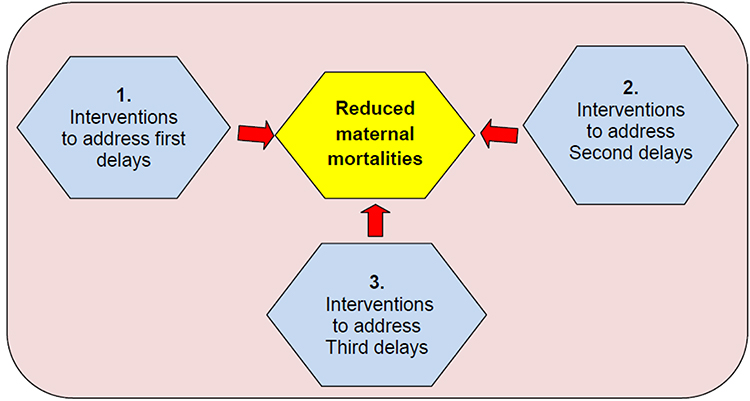 |
Figure 1 Diagrammatic presentation of interventions proposed to address maternal delays. |
Interventions Targeting First Delays
The mother and her family need to be knowledgeable for recognition of maternal complications and be motivated to take prompt action. Community initiatives increase families’ access to healthcare and enable mitigation of first delays of maternal mortality.22 Community health-care workers, volunteers, herbalists and TBAs are an essential workforce in developing countries that are faced with limited human resources in their health-care systems.23 This community workforce can be involved to support programmes that improve healthy maternal and household behaviours, including the seeking of care for uncomplicated pregnancy, referrals, culture shift and prompt treatment of complications.24 For instance, in a rural Ethiopian study, the introduction of the Health Development Army (HDA) (a community voluntary group) successfully identified and encouraged antenatal mothers to attend clinics and have hospital deliveries rather than home deliveries.25 In urban slums in a Bangladesh study, time taken for (women with maternal complications) referred by community health workers (CHWs) and community health volunteers (CHVs) was shorter compared to self referred women from homes. This indicates that, CHWs and CHVs could make better judgement of maternal complications, hence reducing the time taken for decision-making to the hospital for the particular women.26
The researchers posit that, TBAs, whether trained or not, should be excluded from offering direct SBA-related care services. However, they can provide crucial linkages (indirect services) into an integrated strategy of the Migori community and the hospital (Table 5). Further, empowering and incentivising the TBAs is part of provision of an enabling environment needed in the community. Of note is that, TBAs have been delivering mothers in developing countries for years and they are part of a trusted socio-cultural system in the community. It is therefore essential to involve them into community reproductive services.27 This strategy could promote the rural community’s uptake of SBA-related services such as TBAs (who are routinely first point of contact for clients in rural settings) would guide, inform and refer mothers appropriately.28
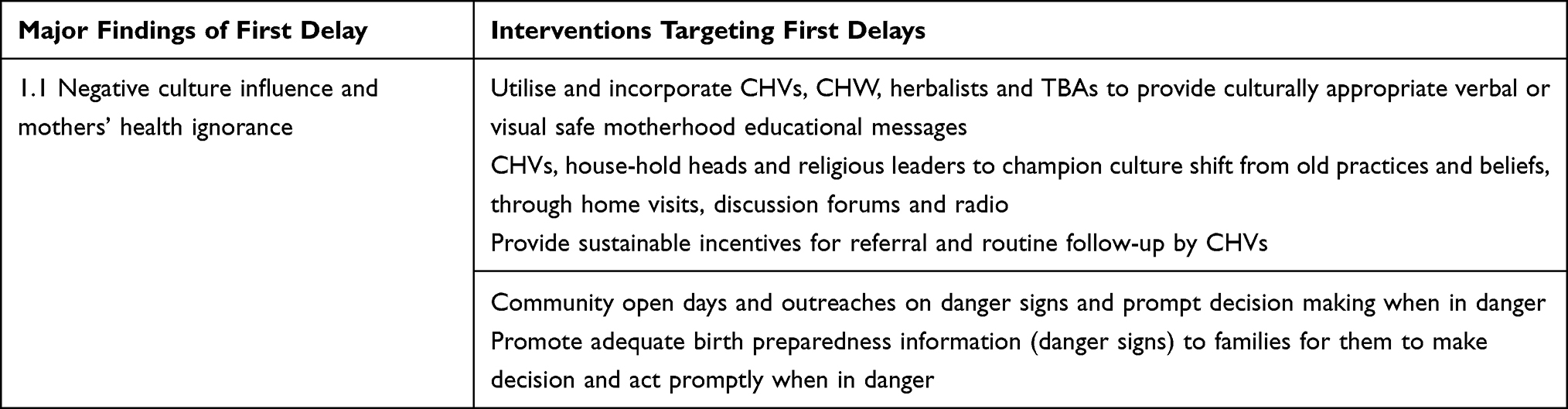 |
Table 5 Description of Interventions Targeting First Delays |
Lastly, at the facility level adequate and quality ANC education (birth preparedness) is provided to mothers to reduce their vulnerability to first delay. Antenatal care education provides knowledge to the family about pregnancy-related complications and need for prompt action.29
Interventions Targeting Second Delays
Pregnant women who develop pregnancy complications (emergencies) need to be transported urgently to Emergency Obstetric & Newborn Care (EmONC) facilities to receive optimal care. This reduces mortality vulnerability of both the mother and her fetus.30 Bhandari and Dangal31 advocate for strong and functional integration between community and health facilities to address the second delays in maternal care – reaching the hospital promptly. It is crucial to encourage local (community) transport initiatives (such as motorbikes for referral) and improvement of road network systems in developing countries to enable efficient access to health-care services.32 United Nations Children’s Fund (UNICEF) introduced a Boda Boda (motorcycle) referral transport system to reduce the barriers related to distance, lack of transport means and cost of travel in West Nile Uganda.33 The project observed that the motorcycle (Boda Boda) referral system saves mothers’ lives in hard-to-reach areas.33 The UNICEF system supports referrals from communities to health centres and from health centres to hospitals.33 Both monetary and non-monetary incentives as a motivation to the Boda Boda riders can be incorporated into the initiative to have increased deliveries at health centres.34
In the present study, mothers delayed the decision to seek skilled birth attendance or did not seek help at all (as some returned home when indicated for referral), possibly due to financial reasons and referral charges. To mitigate this, free ambulance services should be a high priority (Table 6). In a Tanzanian study, researchers assessed the impact of introducing ambulance fees in a rural hospital.35 After the introduction of ambulance fees, an increase in labour complications and C/S was observed.35 In contrast, in Uganda increased uptake of maternal care services to include caesarean section deliveries upon implementation of a free 24-hr ambulance referral system.36
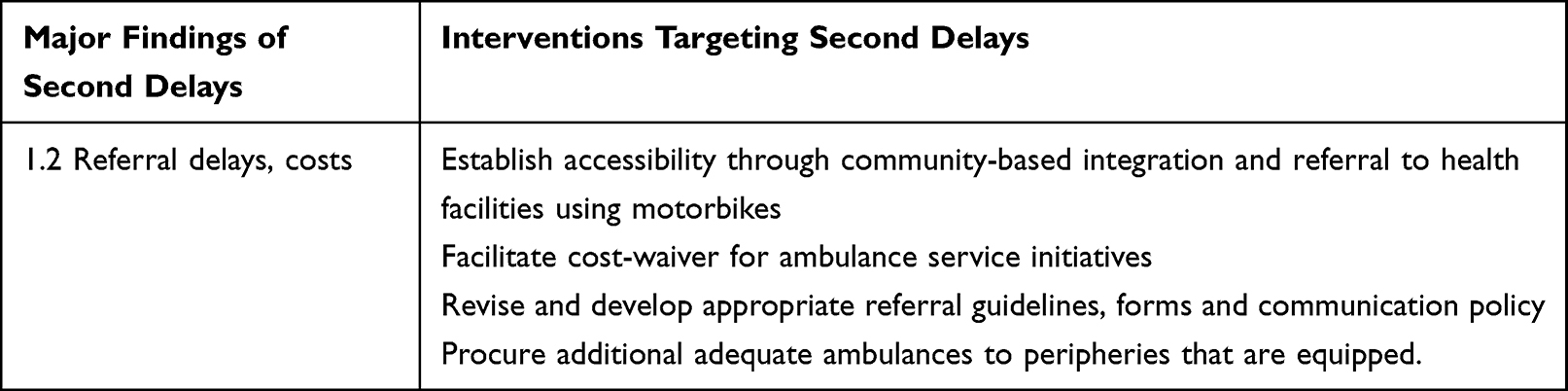 |
Table 6 Description of Interventions Targeting Second Delays |
Time is crucial in saving mothers with emergency complications. In Sierra Leone, a countrywide study demonstrated that maternal risk of death increased concurrently with National Emergency Medical Service (NEMS) operational times.37 This implies that, improved maternal outcomes are likely to be noted with reduced delays of reaching the hospital.37,38 The emergency system should be effective, affordable and adequate.39
Interventions Targeting Third Delays
Mothers with pregnancy-related complications are likely to survive if managed in a hospital that is well equipped with skilled health professionals, emergency supplies and drugs.40 This is defined as an enabling environment in the healthcare system.40 However, in the present study, participants’ interviews indicated suboptimal care contributed by water challenges, erratic supplies, stockout of drugs and inadequate emergency equipment. Improvements (Table 7) in these challenges enable provision of quality care, thus increasing maternal survival in the hospitals.41,42 Ethiopian study43 and Tanzanian interventional study44 demonstrated how equipping hospitals helped to reduce maternal mortality ratios.43 In particular, the Ethiopian findings showed that it was possible to achieve substantial reductions in maternal mortality ratios over a short period of time if effective coverage of well-known interventions is implemented.43
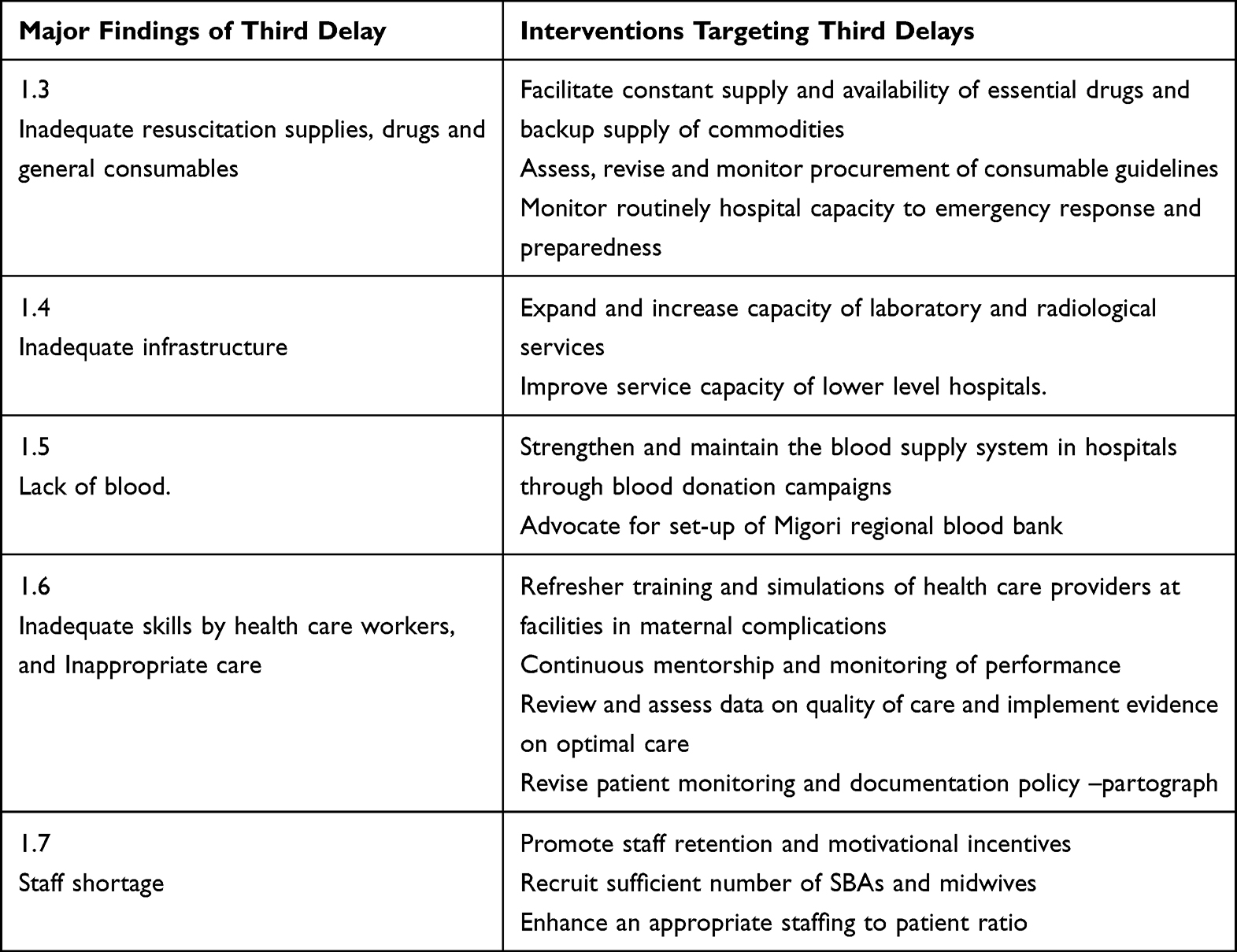 |
Table 7 Description of Interventions Targeting Third Delays |
The present findings further revealed long waiting theatre lists and congested wards. Decentralisation (Table 7) of services – providing comprehensive emergency obstetric care (CEmOC) services near the home of patients is an important strategy to mitigate this challenge.43 This could reduce the burden of potentially life-threatening complications that overwhelms the tertiary health-care system.45,46
The need for blood is universal;47 however, present findings in Migori region indicate that access for all those who need it is not hence the urgent need for blood availability initiatives (Table 7). Literature shows an inverse relationship between the availability of blood and maternal deaths: in countries with the lowest availability of blood, maternal mortality is higher.48 Women who suffer severe bleeding during pregnancy, delivery or after childbirth can die within two hours if untreated.49 Sustainable blood donation initiatives are highly needed to enable adequate blood availability in the Migori region.50,51 For instance, on 11th November 2017, in Kenya, the Maternal and New-born Improvement (MANI) project and the Rotary Club launched a blood campaign organised by E4A-MamaYe in collaboration with Bungoma County Department of Health to reduce the high rates of maternal mortality.52 The initiative set a target of collecting at least 800 units of blood per month and is committed to raising this through organised community groups with the support of all interested parties.52 Elsewhere, media campaigns to motivate blood donations in higher-income countries have become more direct and imaginative, mentioning maternal mortality both in the context of saving women’s lives but also the importance to the newborn of the mother surviving.53 This includes video clips on Facebook and YouTube of recipients thanking donors for having saved their lives, thus giving the process a human face.53
Efficient obstetric emergency care is dependent upon midwives’ knowledge, skills-competencies and the availability of essential supplies needed for a particular intervention.54 However, present findings indicated that some of the cases were inappropriately managed or mismanaged. Training (refresher) programmes (Table 7) improve health-care provider (HCP) knowledge, skills and attitudes as well as care delivery and outcomes for women and their newborns55. In northern Bangladesh, a study was conducted to explore the current knowledge and skills of health-care providers already trained by SIMESON (simulation for essential skills for obstetrical and neonatal care).56 There were improvements in the quality of care for maternal and neonatal health services at the intervention – government health-care facilities.56,57
Improving health workers’ performance through supervision and mentoring would be advantageous to minimise the variation of quality of care and improve maternal outcomes.58 In case of unexpected incidences or complications, the event is evaluated using a no-blame culture.43 This could reduce the poor partograph charting, inadequate patient monitoring and providers’ incompetence that was observed in the present study.
Inequitable access to quality maternal childbirth in sub-Saharan Africa (SSA) is exacerbated by acute shortage and unequal distribution of skilled and specialised health personnel such as physicians, midwives and nurses.36 Improving human resource strategies (Table 7) including recruiting adequate health professionals and improving terms and conditions is essential for reducing maternal mortality in Migori region. This would mitigate the increased demand for services and understaffed maternity wards in the present study.59 It has been hypothesised that adequate provider staffing influences the quality of patient surveillance because it allows health providers to spend more time in direct care.60 Insufficient staffing leads to the rationing of time to care, which has an important impact on the occurrence of missed care.60 Further, delays in receiving timely and appropriate care on reaching a health facility (third maternal care delays) can be directly caused by having too few skilled staff available to carry out adequate care.61 Staff shortages may also cause delays in initiating emergency interventions.61 Recently in Nigeria, researchers investigated the association between client-provider ratios for antenatal and delivery care and the risk of maternal mortality in eight referral hospitals.62 Okonofua et al62 concluded that the maternal mortality ratios in Nigeria’s referral hospitals were worsened by high client provider ratios, with few providers attending a large number of pregnant women experiencing complications.62–65
Recommendations for Hospital Management
Provision of quality obstetric care is proportional to better maternal outcomes. However, findings indicated that some cases were inappropriately and suboptimally managed. This calls for strengthening of continuous quality improvement measures in the peripartum units. Hospitalised mothers expect that drugs and consumables are constantly available. Erratic supply, as indicated by the findings, contributes to inequality of access to hospital interventions by poor mothers. An efficient procurement procedure that minimises delays and ensures adequate stocks of supplies is needed. Adequate staffing (optimal human resource recruitment) is needed in peripartum units. The findings indicate high midwife to patient ratios that contribute to poor patient monitoring and demotivation among staff. Hospitals should recruit adequate staffs that match patient admissions. Hospital managements should organise for continuous refresher trainings for their midwives. Some midwives noted that they had never undergone trainings in the last three years. Further data revealed some cases were vulnerable to negligence of care. Drills and continuous on-job training would improve the level of skills and competencies among the health-care providers.
Recommendations for Governments and Policy Makers
The findings indicated persistent lack of blood. Also, the top pregnancy complication that caused death was haemorrhage. This means that most cases needed blood that was rarely available. The stakeholders should establish blood campaigns teams and set up a Migori regional blood bank centre. The government should set up more comprehensive emergency obstetric care hospitals, especially at the sub-county level. The findings indicated that the existing county hospitals were overwhelmed with demand. In addition, most cases in quantitative study were referrals from periphery-based hospitals. Decentralisation of obstetric care would likely reduce second and third delays.
Procure adequate ambulance vehicles and revise the existing referral system protocol. The findings indicate that mothers were exposed to referral delays due to limited availability of ambulances. Atleast two ambulances should be stationed in each sub-county.
Recommendations for Communities
The researchers recommend strengthening the integration of community systems and hospital care systems. Present data illustrated absence of community referral systems and delays of stipends payments to CHVs. To enable pregnant mothers with obstetric conditions to reach hospital promptly, community motorbikes could be utilised to transport the mother to the nearest health centre. Motivated CHVs are likely to improve referral of mothers to hospital. Organising community health promotion and education on safe pregnancy is needed. Findings illustrate that some Migori families were ignorant of obvious obstetric danger signs. This could be improved through community outreaches that involve all women of reproductive age, household heads, village elders and community traditional healers. Transformation of culture in the community is needed. The researchers observed that Migori women were negatively influenced by traditional practices that encourage home deliveries. Also, they were vulnerable to the negative influences of patriarchy. Initiatives that promote positive cultural practices that involve in-laws, male partners and TBAs as culture champions are recommended.
Conclusion
The researchers believe that priority interventions needed are those that enable: 1) Pregnant mothers to receive quality peripartum care in Migori hospitals, 2) Strengthened and efficient referral systems of obstetric emergencies and 3) Community knowledge empowerment on safe pregnancy and culture shift. These interventions would significantly transform the health-care system towards maternal mortality reduction. Notably, the present strategy’s success depends on the stakeholders’ commitment and availability of resources to enable its full-scale implementation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. UNPD. Trends in Maternal Mortality: 2000 to 2017. United Nations Statistics Division; 2018.
2. World Health Organization. Trends in Maternal Mortality 2000 to 2017. World Health Organization; 2019.
3. Ministry of Health. Reducing Maternal Deaths in Kenya. Ministry of Health; 2019.
4. UNDP. Fact Sheets on Sustainable Development Goals. UNDP; 2018.
5. Keats EC, Macharia W, Singh NS, et al. Accelerating Kenya’s progress to 2030: understanding the determinants of under-five mortality from 1990 to 2015. BMJ Glob Heal. 2018;3:1–15.
6. Santora E. The impact of the safe motherhood initiative from 1987 to 2000; 2020.
7. Stanton ME, Kwast BE, Shaver T, Mccallon B, Koblinsky M. Beyond the safe motherhood initiative: accelerated action urgently needed to end preventable maternal mortality. Glob Heal Sci Pract. 2018;6:408–412. doi:10.9745/GHSP-D-18-00100
8. Anoldis T, Christine K, Gladys M, Clara H, Abigail K. Concept paper: safe motherhood. J Res Pharm Sci. 2018;4:48–53.
9. World Health Organization. Targets and Strategies for Ending Preventable Maternal Mortality Consensus Statement. World Health Organization; 2015.
10. Jolivet RR, Moran AC, O’Connor M, Chou D, Bhardwaj N. Ending preventable maternal mortality: Phase II of a multi-step process to develop a monitoring framework, 2016–2030. BMC Pregnancy Childbirth. 2018;18:1–13.
11. Gebremedhin S. Development of a new model for estimating maternal mortality ratio at national and sub-national levels and its application for describing sub-national variations of maternal death in Ethiopia. PLoS One. 2018;13:e0201990. doi:10.1371/journal.pone.0201990
12. Agena A. Trends and Determinants of Intrapartum Stillbirth in the Public Health Facilities of Addis Ababa, Ethiopia. University of South Africa; 2018.
13. Win T, Vapattanawong P, Vong-ek P. Three delays related to maternal mortality in Myanmar: a case study from maternal death review, 2013. J Heal Res. 2015;29:179–187.
14. Serbanescu F, Goodwin MM, Binzen S, Morof D, Asiimwe AR. Addressing the first delay in saving mothers, giving life Districts in Uganda and Zambia: approaches and results for increasing demand for facility delivery services. Glob Heal Sci Pract. 2019;7:48–67. doi:10.9745/GHSP-D-18-00343
15. Masaba BB. Maternal mortality determinants in Rural Kenya; an audit of three hospitals. Iran J Nurs Midwifery Res. 2023;28:1–9.
16. Masaba BB, Mmusi-Phetoe R, Rono B, et al. The healthcare system and client failures contributing to maternal mortality in rural Kenya. BMC Pregnancy Childbirth. 2022;22:1–13. doi:10.1186/s12884-022-05259-w
17. Polit DF, Beck CT. Essentials of Nursing Research. Wolters Kluwer/Lippincott Williams & Wilkins; 2017.
18. Creswell JW, Creswell JD. Research Design Qualitative, Quantitative, and Mixed Approaches. SAGE Publications; 2018.
19. KDHS. Kenya Demographic and Health Survey. Kenya National Bureau of Statistics; 2020.
20. McCrudden MT, McTigue EM. Implementing integration in an explanatory sequential mixed methods study of belief bias about climate change with high school students. J Mix Methods Res. 2018;13:381–400. doi:10.1177/1558689818762576
21. Bazeley P. Integrating Analyses in Mixed Methods Research. Sage Publications Ltd; 2018. doi:10.4135/9781526417190
22. Elmusharaf K, Byrne E, Donovan DO. Strategies to increase demand for maternal health services in resource-limited settings: challenges to be addressed. BMC Public Health. 2015;15:1–10. doi:10.1186/s12889-015-2222-3
23. Nishimwe C, Mchunu GG, Mukamusoni D. Community-based maternal and newborn interventions in Africa: systematic review. J Clin Nurs. 2021;30:2514–2539. doi:10.1111/jocn.15737
24. USAID. Reducing the burden of the three delays on maternal health in Timor-Leste; 2015.
25. Jackson R, Tesfay FH, Gebrehiwot TG, Godefay H. Factors that hinder or enable maternal health strategies to reduce delays in rural and pastoralist areas in Ethiopia. Trop Med Int Heal. 2017;22:148–160. doi:10.1111/tmi.12818
26. Nahar S, Banu M, Nasreen HE. Women-focused development intervention reduces delays in accessing emergency obstetric care in urban slums in Bangladesh: a cross-sectional study. BMC Pregnancy Childbirth. 2021;11:1–10.
27. Choguya NZ. Traditional birth attendants and policy ambivalence in Zimbabwe. J Anthropol. 2014;2014:1–9. doi:10.1155/2014/750240
28. Kitui JE, Dutton V, Bester D, Ndirangu R, Wangai S. Traditional Birth Attendant reorientation and Motherpacks incentive’ s effect on health facility delivery uptake in Narok County, Kenya: an impact analysis. BMC Pregnancy Childbirth. 2017;17:1–12. doi:10.1186/s12884-017-1307-7
29. Danna VA, Bedwell C. Utility of the three-delays model and its potential for supporting a solution-based approach to accessing intrapartum care in low- and middle-income countries. A qualitative evidence synthesis. Glob Health Action. 2020;13:1–23.
30. Alaofe H, Lott B, Kimaru L, Okusanya B, Chebet J. Emergency transportation interventions for reducing adverse pregnancy outcomes in low- and middle-income countries: a systematic review. Ann Glob Heal. 2020;86:1–18.
31. Bhandari T, Dangal G. Emergency obstetric care: strategy for reducing maternal mortality in Developing Countries. Emerg Obstet Care. 2014;9:8–16.
32. Amosse F, Boene H, Kinshella MW, Drebit S, Sharma S. Implementation of a community transport strategy to reduce delays in seeking obstetric care in Rural Mozambique. Glob Heal Sci Pract. 2021;9:122–136. doi:10.9745/GHSP-D-20-00511
33. UNICEF. Motorcycle (Boda Boda) Referral System Saves Mothers and Babies in Hard-to-Reach Areas in West Nile Uganda. United Nations Children’s Fund (UNICEF); 2022.
34. Muluya KM, Mugisha JF, Kithuka P, Kibaara KR, Muwanguzi DG. Incentives for mothers, health workers and ‘boda – boda’ riders to improve community ‑ based referral process and deliveries in the rural community: a case of Busoga Region in Uganda. Reprod Health. 2022;19:1–9. doi:10.1186/s12978-022-01334-9
35. Vossius C, Mduma E, Moshiro R, Mdoe P, Kvaløy JT. The impact of introducing ambulance and delivery fees in a rural hospital in Tanzania. BMC Health Serv Res. 2021;21:1–10. doi:10.1186/s12913-021-06107-x
36. Wekesah FM, Mbada CE, Muula AS, Kabiru CW, Muthuri SK. Effective non-drug interventions for improving outcomes and quality of maternal health care in sub-Saharan Africa: a systematic review. Syst Rev. 2016;5:1–18. doi:10.1186/s13643-016-0305-6
37. Caviglia M, Putoto G, Conti A, Tognon F, Jambai A. Association between ambulance prehospital time and maternal and perinatal outcomes in Sierra Leone: a countrywide study. BMJ Glob Heal. 2021;6:1–8.
38. Oguntunde O, Yusuf FM, Nyenwa J, Dauda DS, Salihu A. Emergency transport for obstetric emergencies: integrating community-level demand creation activities for improved access to maternal, newborn, and child health services in northern Nigeria. Int J Women’s Heal. 2018;10:773–782. doi:10.2147/IJWH.S180415
39. Zachariah R, Manzi M, Van Den BW, Nyandwi G, Reid T. An ambulance referral network improves access to emergency obstetric and neonatal care in a district of rural Burundi with high maternal mortality. Trop Med Int Heal. 2013;18:993–1001. doi:10.1111/tmi.12121
40. World Health Organization. Maternal Mortality - UNICEF DATA2020. World Health Organization; 2022.
41. Barker P, Nynke V-B, Dickson K, Hanson C, Hill K. Standards for Improving Quality of Maternal and Newborn Care in Health Facilities. World Health Organization; 2016.
42. Hou X, Khan MM, Pulford J, Saweri OPM. Readiness of health facilities to provide emergency obstetric care in Papua New Guinea: evidence from a cross- - sectional survey. BMJ Open. 2022;12:1–10. doi:10.1136/bmjopen-2021-050150
43. Lindtj B, Mitiku D, Zidda Z, Yaya Y. Reducing maternal deaths in Ethiopia: results of an intervention programme in Southwest Ethiopia. PLoS One. 2017;12:e0169304. doi:10.1371/journal.pone.0169304
44. Otolorin E, Gomez P, Currie S, Thapa K, Dao B. Essential basic and emergency obstetric and newborn care: from education and training to service delivery and quality of care. Int J Gynecol Obstet. 2015;130:S46–S53. doi:10.1016/j.ijgo.2015.03.007
45. Tukur J, Lavin T, Adanikin A, Abdussalam M, Bankole K. Articles quality and outcomes of maternal and perinatal care for 76, 563 pregnancies reported in a nationwide network of Nigerian referral-level hospitals. Lancet. 2022;47:1–16.
46. Prasad N, Mwakatundu N, Dominico S, Masako P, Mongo W. Improving maternal and reproductive health in Kigoma, Tanzania: a 13-year initiative. Glob Heal Sci Pract. 2022;10:1–17.
47. Mohammed AS, Yassin A, Aliyi AA. Voluntary blood donation practice and its associated factors among civil servants in Bale Robe town, Southeast Ethiopia, 2021. SAGE Open Med. 2022;10:1–10. doi:10.1177/20503121221102099
48. Pan-American-Health-Organization. WHO urges blood donation to save mothers’ lives; 2022.
49. World Health Organization. Drop in blood donations add to maternal health threats in Africa WHO Regional Office for Africa; 2021.
50. Melku M, Melku M, Asrie F, Shiferaw E, Woldu B. Knowledge, attitude and practice regarding blood donation among graduating undergraduate health science students at the University of Gondar, Northwest Ethiopia. Ethiop J Heal Sci. 2018;28:571–575.
51. Zanin TZ, Hersey DP, Cone DC, Agrawal P. Tapping into a vital resource: understanding the motivators and barriers to blood donation in Sub-Saharan Africa. African J Emerg Med. 2016;6:70–79. doi:10.1016/j.afjem.2016.02.003
52. Bungoma-County-Govt. Show your love, donate blood to save a Mama na Mtoto E4A-MamaYe; 2022.
53. Ray S, Madzimbamuto F, Fonn S. Activism: working to reduce maternal mortality through civil society and health professional alliances in sub-Saharan Africa. Reprod Health Matters. 2012;20:40–49. doi:10.1016/S0968-8080(12)39617-1
54. Mgawadere F, Unkels R, Kazembe A, Van Den BN. Factors associated with maternal mortality in Malawi: application of the three delays model. BMC Pregnancy Childbirth. 2017;17:1–9. doi:10.1186/s12884-017-1406-5
55. Banke-Thomas A, Maua J, Madaj B, Ameh C, Van Den BN. Perspectives of stakeholders on emergency obstetric care training in Kenya: a qualitative study. Adv Access Publ. 2020;12:11–18.
56. Das R, Dil F, Zakia F, Kallol S, Baayo A. Evaluation of SIMESON, a training program to improve access to quality health care for pregnant women and newborn in different healthcare facilities of northern Bangladesh. Nurs Open. 2022;9:801–815. doi:10.1002/nop2.1131
57. Baumgartner JN, Headley J, Kirya J, Guenther J, Kaggwa J. Impact evaluation of a maternal and neonatal health training intervention in private Ugandan facilities. Health Policy Plan. 2021;37:1103–1115. doi:10.1093/heapol/czab072
58. Raru TB, Ayana GM, Bahiru N, Deressa A, Alemu A. Quality of antenatal care and associated factors among pregnant women in East Africa using Demographic and Health Surveys: a multilevel analysis. Women’s Heal. 2022;18:1–9.
59. Kim C, Erim D, Natiq K, Salehi AS, Zeng W. Combination of interventions needed to improve maternal healthcare utilization: a multinomial analysis of the inequity in place of childbirth in Afghanistan. Front Glob Women’s Heal. 2020;1:1–12.
60. Haegdorens F, Van, Meester BP, De K, Monsieurs KG. The impact of nurse staffing levels and nurse’ s education on patient mortality in medical and surgical wards: an observational multicentre study. BMC Health Serv Res. 2019;7:1–9.
61. Bradley S, Kamwendo F, Chipeta E, Chimwaza W, Pinho HD. Too few staff, too many patients: a qualitative study of the impact on obstetric care providers and on quality of care in Malawi. BMC Pregnancy Childbirth. 2015;15:1–10. doi:10.1186/s12884-015-0492-5
62. Okonofua F, Ntoimo L, Ogu R, Galadanci H, Abdus-salam R. Association of the client-provider ratio with the risk of maternal mortality in referral hospitals: a multi-site study in Nigeria. Reprod Health. 2018;15:1–9. doi:10.1186/s12978-018-0464-0
63. Thi N, Thu H, Wilson A, Mcdonald F. Motivation or demotivation of health workers providing maternal health services in rural areas in Vietnam: findings from a mixed-methods study. Hum Resour Health. 2015;13:1–11. doi:10.1186/1478-4491-13-1
64. Nabi R, Karimi D, Senkubuge F, Hongoro C. Determinants of motivation among healthcare workers in the East African community between 2009 – 2019: a systematic review. Healthcare. 2020;8:1–24.
65. Lagarde M, Huicho L, Papanicolas I. Motivating provision of high quality care: it is not all about the money. BMJ Open. 2019;366:1–5.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.