")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
A Single-Center Study Using IVUS to Guide Rotational Atherectomy for Chronic Renal Disease’s Calcified Coronary Artery
Authors Hu G, Qi X, Li B, Ge T, Li X, Liu Z, Li J , Zhang X, Li Y, Zhang S, Wang Y, Zhao T, Zhang B, Xu Q
Received 6 February 2023
Accepted for publication 31 March 2023
Published 19 April 2023 Volume 2023:16 Pages 1085—1093
DOI https://doi.org/10.2147/JMDH.S405174
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Guangxin Hu,1,* Xijuan Qi,1,* Ben Li,1 Ting Ge,1 Xi Li,1 Zhijun Liu,1 Jiaxing Li,1 Xuemei Zhang,1 YinPing Li,1 Shichang Zhang,1 Yajuan Wang,2 Tingting Zhao,3 Botao Zhang,1 Qingbin Xu1
1Department of Cardiology, General Hospital of Ningxia Medical University, Yinchuan, 750002, People’s Republic of China; 2Department of Pharmacy, General Hospital of Ningxia Medical University, Yinchuan, 750002, People’s Republic of China; 3Department of Respiratory Medicine, General Hospital of Ningxia Medical University, Yinchuan, 750002, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guangxin Hu, Email [email protected]
Objective: To assess the effectiveness and safety of an IVUS-guided rotational atherectomy (RA) percutaneous coronary intervention (PCI) in chronic renal patients with complex coronary calcification who are at risk for contrast-related acute kidney injury (AKI).
Methods: From October 2018 to October 2021, 48 patients with chronic renal disease who were receiving PCI with RA at the General Hospital of NingXia Medical University were informed for data collection for this research. They were randomly assigned to the IVUS-guided RA group and the Standard RA group, which did not use IVUS. According to a clinical expert consensus document on rotational atherectomy in China, both PCI procedures were performed. The intravascular ultrasound (IVUS) results from the study group were used to describe the morphology of the lesion and to guide the selection of burrs, balloons, and stents. IVUS and angiography were used to evaluate the outcome in the end. IVUS-guided RA PCI and Standard RA PCI groups’ effects and results were contrasted.
Results: There were no appreciable differences in the clinical baseline characteristics between the IVUS-guided RA PCI group and the Standard RA PCI group. The average estimated glomerular filtration rate (eGFR) of two groups was (81.42 ± 20.22 vs 82.34 ± 22.19) mL/min/1.73 m2. Most of them (45.8% vs 54.2%) was in stage 60– 90 mL/min/1.73m2. When compared to the standard RA PCI group, RA in IVUS-Guided group was more performed electively (87.5% vs 58.3%; p = 0.02). The IVUS-guided RA PCI group was associated with shorter fluoroscopy time (20.6 ± 8.4 vs 36 ± 22; p< 0.01) and less contrast amount (32 ± 16 vs 184 ± 116mL; p< 0.01) than Standard-RA group. Five patients in the Standard RA PCI group developed contrast-induced nephropathy, which was 5 times than the IVUS-guided RA PCI group (20.8% VS 4.1%; p=0.19).
Conclusion: In chronic renal patients with complex coronary calcification, an IVUS-guided RA PCI technique is effective and safe. It can also lower the volume of contrast and perhaps the incidence of contrast-related AKI.
Keywords: rotational atherectomy, chronic renal disease, contrast-associated acute kidney injury, intravascular ultrasound
Introduction
Atherosclerosis and the calcification of the coronary arteries have both been found to progress more quickly in individuals with chronic kidney disease (CKD).1 Since its introduction more than 20 years ago, the rotational atherectomy (RA) technique has become increasingly popular for the treatment of severely calcified coronary lesions.2–4 The technically challenging procedure known as percutaneous coronary intervention (PCI) of severely calcified coronary lesions is typically linked with a high contrast volume consumption, which raises the risk of contrast-related acute renal injury.5
The increased utilization of intravascular ultrasonography has contributed to the rise in the incidence of RA (IVUS).6–8 IVUS-guided rotational atherectomy (RA) percutaneous coronary intervention (PCI) in patients with complex coronary calcification who already had CKD is supported by a smaller number of studies.9–11
In order to evaluate the efficacy and safety of the procedure, the purpose of this research is to compare IVUS-guided RA PCI with standard-RA PCI in patients with CKD who have complicated calcified coronary lesions and a serious potential for contrast-related AKI.
Methods
Patient Selection
The data for this study came from a collection of 48 chronic renal patients who underwent PCI with RA at the General Hospital of NingXia Medical University between the months of October 2018 and October 2021. They were randomly split up into two groups after being separated. The first group consisted of 24 patients and was treated with standard RA without IVUS. The second group consisted of 24 patients and was treated with IVUS-guided RA. Both PCI procedures were carried out in accordance with the clinical expert consensus document on atherectomy rotational in China.12 Mild, moderate, severe, or kidney failure (according to the Kidney Disease: Improving Global Outcomes guideline, these stages are referred to as G2-G5). According to the modification of diet in renal disease equation, patients who had an estimated glomerular filtration rate (eGFR) of less than 90 mL/min/1.73m2 were all considered to be at a high risk for contrast-related acute kidney injury (AKI), or a previous history of acute kidney injury caused by contrast (AKI), which is defined as an increase in serum creatinine of 0.5 mg/dl or 25% over baseline that occurs between 48 and 72 hours after being exposed to iodinated contrast media).13–15
Patients with chronic total occlusion (CTO), acute coronary syndrome with ST-elevation, or cardiogenic shock were excluded from this study. The ethical committee of the General Hospital of Ningxia Medical University gave their stamp of approval to the collection and use of the data after receiving written consent from each patient (KYLL-2021-498). The principles outlined in the Declaration of Helsinki were adhered to throughout the course of the research.
Procedure of IVUS-Guided RA PCI and Standard RA PCI
In order to reduce the risk of contrast-related acute kidney injury (AKI), PCI was performed as soon as possible after the diagnostic angiography in stable patients who had chronic coronary syndrome, and it was performed 48 hours later in stable patients who had non-ST-elevation acute coronary syndrome. Every single patient received the appropriate amount of hydration. Access through either the radial or the femoral artery was chosen by the operator depending on the peripheral vascular conditions. Systematic echocardiography was performed both before and after the PCI procedure in order to look for any pericardial effusion. After the decision to perform PCI was made, patients were given a loading dose of a P2Y12 inhibitor orally (either Clopidogrel 600 mg or Ticagrelor 180 mg), along with aspirin (300 mg). Intraprocedural anticoagulation was accomplished with a dose of unfractionated heparin that was set at 100 U/kg in order to maintain an active clotting time (ACT) that was greater than 250 seconds. During PCI, the previous angiography was shown as needed for procedural direction. On the basis of the prior diagnostic angiography without contrast injection, workhorse wire manipulation and guiding catheter placement were completed.
Before deciding whether to use a burr, balloon, or stent, the IVUS-guided RA PCI group performed a baseline IVUS to analyze the morphology of the lesion, as well as the distribution of calcium throughout the vessel. The length of the stent was determined by taking the distance between the two reference points into account. The use of small burrs (burrs measuring 1.25 or 1.5 mm) is recommended for IVUS lesions that cannot be crossed. The operator could choose either 1.25- or 1.5-mm burrs at their own discretion. After that, imaging data from the IVUS would be collected. During the IVUS pullback, the lesion limits were determined by comparing the IVUS data to the position of the catheter as seen on fluoroscopy. In the group that received IVUS guidance for RA PCI, contrast was only administered before and after the procedure. Baseline angiography was performed in different views showing the target lesion for the Standard RA PCI group. This was done to avoid foreshortening and overlap by visual estimation, which is why IVUS examination was not performed. Depending on the findings of the IVUS or previous angiographic procedures, RA was either performed as a planned strategy or as a bailout choice in situations involving lesions that could not be crossed or deleted. The micro-catheter was moved forward over the workhorse guide wire in order to make room for a wire exchange using the Rota Wire on both of them.
The equipment known as RotaPro or Rotablator was utilized in the RA procedure (Boston Scientific Scimed Inc, USA). The size of the burr was determined in order to achieve a burr/vessel ratio of 0.5. And 140,000–200,000 revolutions per minute were within RA speed’s capabilities. Continuous intracoronary infusion of heparin at a dose of 5000 IU was performed without the use of nitroglycerin or verapamil. During the atherectomy procedure, the patient’s symptoms, as well as their heart rate, blood pressure, and ST-segment, were all carefully monitored. Ablation runs were restricted to 20 seconds, and a pecking action, which consisted of a slow push forward and a quick pullback movement of the burr, was the most frequently used technique for burr manipulation in RA. It was essential for effective RA to avoid making a floppy bend in the Rota Wires because doing so significantly increased the amount of friction force that existed between the burr and the Rota Wire. When using non-compliant balloons, balloon pre-dilation was performed with a 1:1 sizing target. The distal part of the treated segment was used as a reference to ensure that the balloon did not become oversized. Before the stent could be implanted, the balloon had to be expanded to its full capacity, and the lesion had to be properly prepared. It was recommended that the patient’s balloon be downsized to reduce the risk of dissection in the event that additional pre-dilatation with a modified balloon (scoring/cutting/Lacrosse NSE) was required.
After the lesion was prepared, an IVUS was carried out once more in order to reassess its boundaries and decide whether it should be combined with a myocardial bridge in order to circumvent vascular dissection. After the stent was implanted, IVUS was performed to check for mal-apposition, under-expansion, and edge dissection in the stent, as well as to make sure that the lesion was completely covered. In order to monitor coronary flow and observe any complications such as distal embolization, perforation, or hematoma, the final outcome was evaluated angiographically by minimum dosage contrast injection following PCI and with satisfactory findings from IVUS. This was done in order to determine the ultimate outcome.
Study Endpoints
Angiographic success was measured by TIMI 3 flow with less than 30% of residual stenosis after the treatment. To determine feasibility and safety, it was necessary to rule out intraprocedural and in-hospital issues such slow/no-flow, coronary perforation, pericardial effusion, peri-procedural death, cardiac arrest, and target vessel revascularization. After PCI, the absence of contrast-related AKI was used to assess the procedure’s success. Following PCI, we clinically examined the patients to evaluate renal function and cardiovascular events.
Statistical Methods
An overview of quantitative variables is provided by their median or mean (inter-quartile range [IQR]). Counts and percentages are used to summarize category variables. Independent variables included age, gender, diabetes mellitus, baseline GFR, and the overall length of stented arteries. There was no calibration. There were a total of 26 patients matched. The Student’s t-test was used to compare continuously regularly distributed continuous variables, while the Mann–Whitney U-test was used for continuously non-normally distributed data. The chi-squared and Fisher’s exact tests were used where needed to compare categorical variables. A two-sided 0.05 p value was used to establish statistical significance. Version 24.0 of the propensity score plug-in (version 1) for IBM SPSS, was used to conduct the PSM. Utilizing Stata SE 14, the remaining statistical analysis was carried out (StataCorp LP, Texas, USA).
Results
Baseline Clinical Characteristics
Forty-eight patients were included at General Hospital of NingXia Medical University with chronic renal disease who were undergoing PCI with RA from October 2018 to October 2021. Twenty-four patients were divided into the IVUS-guided RA PCI group. The study’s participants had an average age of 72.3 ± 7.1 years, and 80.9% of them were male. The mean BMI of the IVUS-guided RA PCI Group was 26.9 ± 4.8. Hypertension was presented in 95.8% patients and 58.3% of the cases involved type 2 diabetes mellitus. Moreover, 79.2% of the patients had dyslipidemia and 80.9% of them had a history of smoking. The average ejection fraction was 41 ± 13%, PCI was performed in 19/24 (79.2%) patients diagnosed chronic coronary syndrome. The creatinine was 163[129–348] µmol/l. The mean eGFR was 81.42 ± 20.22mL/min/1.73 m2, 45.8% of them was in eGFR stage 60–90 mL/min/1.73m2. Seven patients (29.2%) had a history of contrast-related AKI. Similar results were obtained in the Standard-RA PCI group, and the differences were not statistically significant (P>0.05). The baseline clinical characteristics of the IVUS-guided RA group and Standard RA group with PCI are summarized in Table 1.
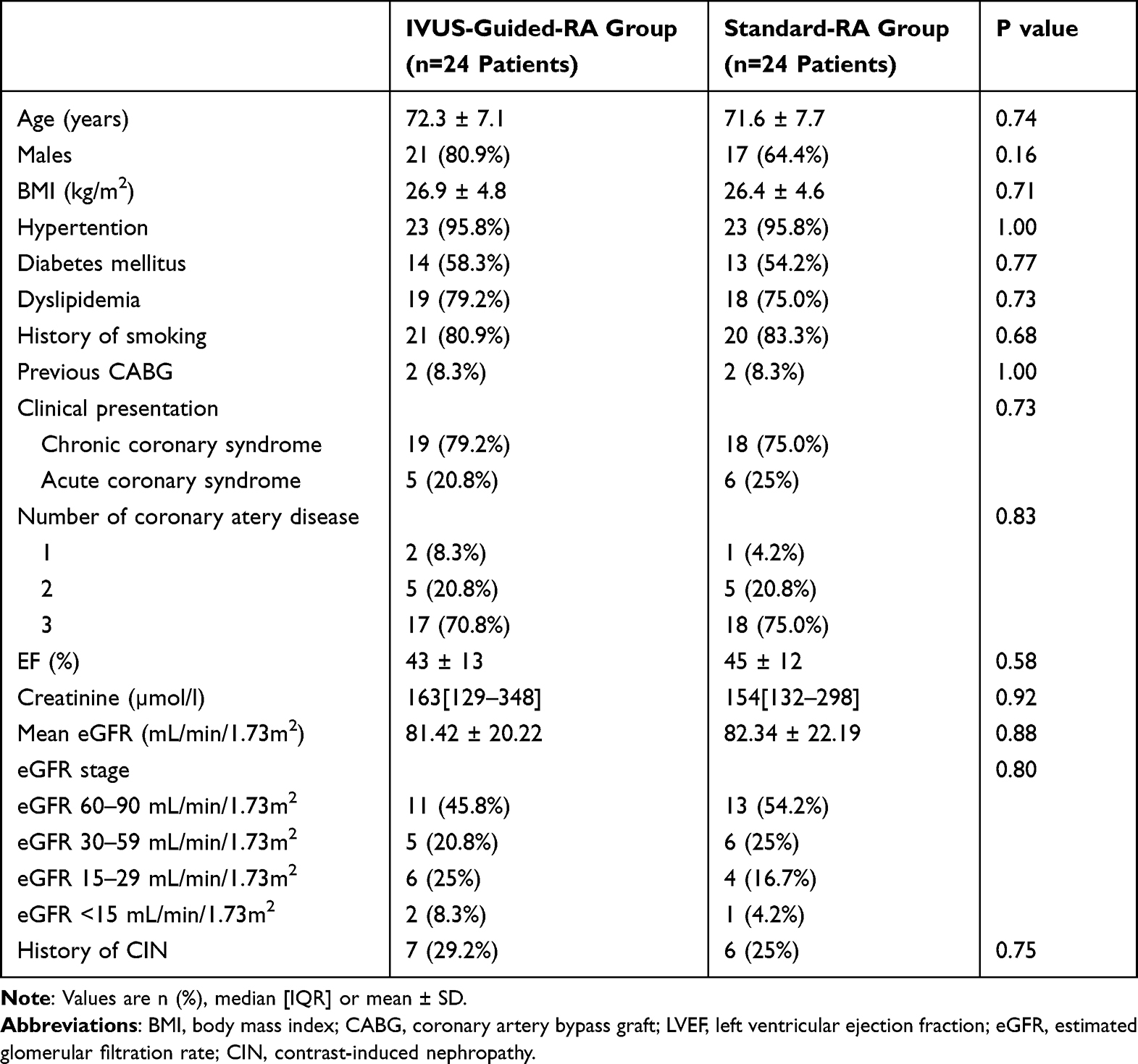 |
Table 1 Baseline Clinical Characteristics of the IVUS-Guided RA PCI Group and Standard-RA PCI Group |
Baseline Angiographic and RA PCI Procedural Characteristics
Table 2 shows the baseline angiographic and procedural features. The most frequently targeted vascular in both the IVUS-guided RA PCI group and the conventional RA PCI group was the left anterior descending artery (LAD) (50% vs 54.1%). The diameter stenosis in the two groups was nearly identical (88 8% vs 89 9%) during RA PCI under IVUS guidance. A bifurcation was present in 54.1% of the lesions, and the two-stent approach was used to treat 20.8% of them (2 culotte technique cases, 3 crush technique cases). And 61.5% employed a preliminary approach. In order to offer robust back-up support in the event of a significant tortuosity and calcification, a 7F guide catheter (87.5%) was placed during the PCI. In five cases, a Guidezilla extension catheter was employed (20.8%). Both the IVUS-guided RA group and the Standard-RA group made extensive use of radial access (83.3% vs 75%). Target RA PCI vascular prevalence, diameter stenosis, bifurcation lesion, bifurcation approach, epidural access, and guiding diameter did not differ significantly between the two groups.
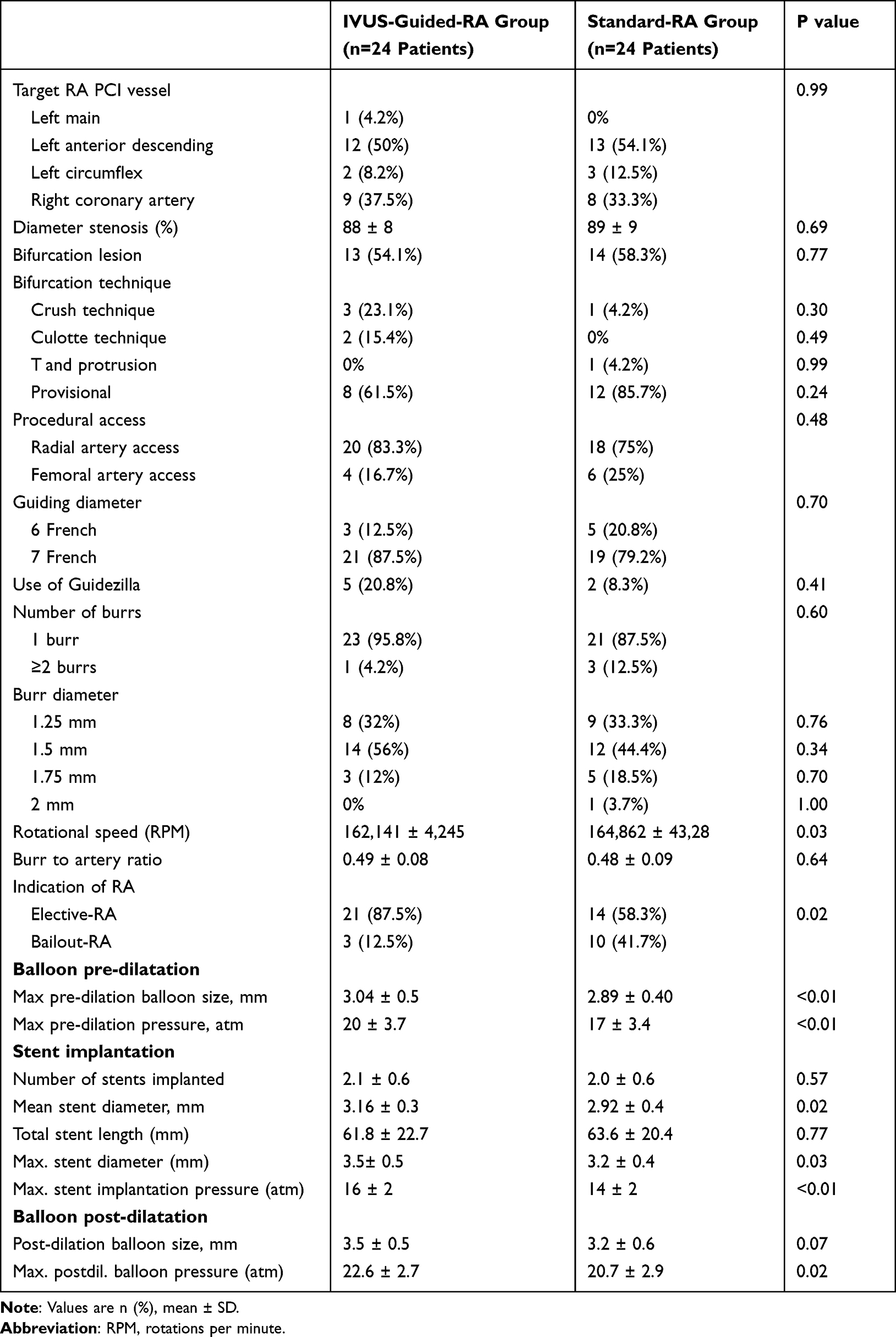 |
Table 2 Angiographic and Procedural Characteristics of the IVUS-Guided RA Group and Standard-RA Group |
The majority of experts in RA technique advocated a 1.5 mm burr size for the second group (56% vs 44.4%). Two burrs were treated instead of as many patients (4.2% vs 12.5%). Operators decided to perform elective RA in 94.4% of the patients in the IVUS-guided RA PCI group and 58.3% in the Standard RA PCI group (P0.05) based on IVUS or angiographic results. The ratio of burrs to arteries in the two groups was nearly identical (0.49 0.08 vs 0.48 0.09). In contrast, the rotational speed (RPM) was different (162, 141 4, 245 vs 164, 862 43, 28bpm, P 0.05). There was no discernible difference in the number of stents implanted, the overall length of the stent, or the size of the post-dilation balloon (P > 0.05). The maximum pre-dilation balloon size (3.04 0.5 vs 2.89 0.40; p 0.01), the maximum pre-dilation pressure (20 3.7 vs 17 3.4; p 0.01), the mean stent diameter (3.16 0.3 vs 2.92 0.4; p = 0.02), the maximum stent diameter (3.5 0.5 vs Table 2 contains more details).
Intravascular Imaging Finding
In the IVUS-guided RA PCI group, there were three IVUS acquisitions on average in each procedure. The IVUS catheter was unable to across the lesion in around 25% of the instances, and baseline IVUS lesion analysis was not accessible. The measurements of maximum calcium angle, proximal reference, distal reference, post-stent implantation, are showed in Table 3. The average stent expansion rate was (75 ± 8)%, 3(12.5%) patients got edge dissection. One patient (4.1%) had under-expansion and 3(12.5%) patients had mal-apposition.
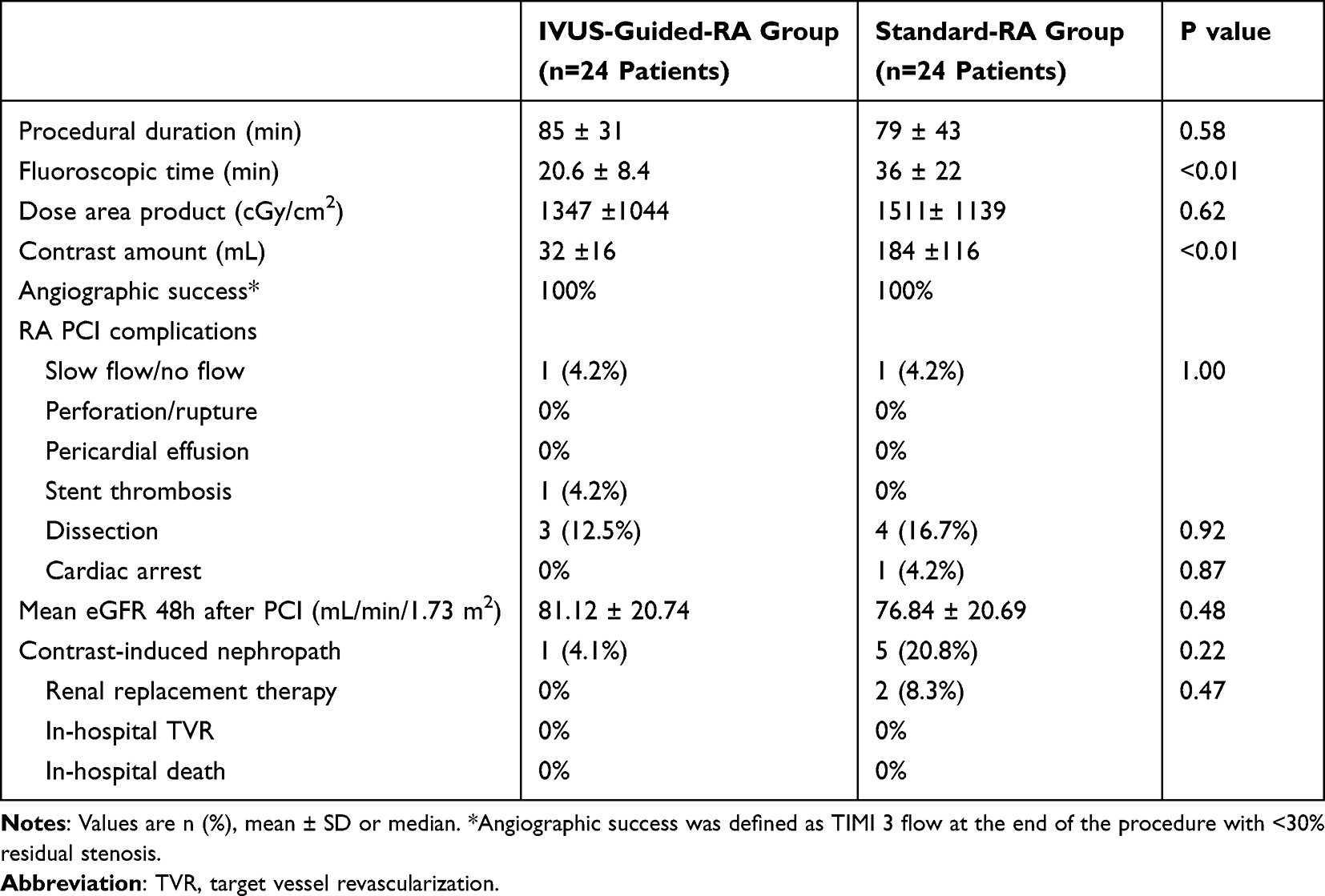 |
Table 3 Procedural and In-Hospital Outcome of the IVUS-Guided RA Group and Standard RA Group |
Procedural, Complications and In-hospital Outcome
In comparison to the Standard-RA group, the IVUS-guided RA PCI group had shorter fluoroscopy times (20.6 8.4 vs 36 22min; p 0.01) and less contrast (32 16 8.4 vs 184 116; p 0.01). Although there was no discernible distinction in the mean eGFR between the two groups following PCI. Contrast-induced nephropathy occurred in five patients in the Standard RA PCI group, which is 5 times more patients than in the IVUS-guided RA PCI group (20.8% VS 4.1%). Procedure length, dosage area product, RA PCI problems (slow flow/no flow, pericardial effusion, dissection, cardiac arrest), in-hospital TVR, and in-hospital death (P0.05) did not differ significantly from one another (see Table 3).
Discussion
Cardiovascular disease is the leading cause of mortality and morbidity in CKD patients, especially those with complex calcified lesions.15–17 They are so resistant to insufficient balloon dilatation or stent placement, and coronary highly calcified lesions can present a significant obstacle for PCI18–20 additionally, stent thrombosis and in-stent restenosis may occur as a result of inadequate stent implantation.21–23 Therefore, adequate stent expansion depends in particular on sufficient preparation of severely calcified lesions. RA is effective at modifying calcified plaques and enabling the stent deployment.24–26
Observational trials showed RA was safe and appropriate in terms of peri-procedural and in-hospital consequences in most patients.27 Our research revealed that IVUS-guided RA PCI may be a useful strategy to prevent contrast-associated AKI. A shorter fluoroscopy duration and lower radiation dosage were linked with IVUS-guided RA PCI, which did not increase procedural time.
Since contrast-induced nephropathy is linked to an independent risk of peri-procedural mortality, acute myocardial infarction, hemorrhage, and RRT after PCI.28–30 It is a significant issue in the management of patients with CKD. As a result, minimizing contrast use to reduce contrast-related AKI and attaining outstanding stent results to improve long-term outcomes are two therapy goals that should be pursued concurrently.
Prior research had established the viability and safety of minimal-contrast IVUS-guided rotational atherectomy in terms of the prevalence of peri-procedural and in-hospital problems. This could be successful in preventing contrast-related AKI.5 In a cohort of 31 patients with severe CKD, Ali et al31–33 showed that intravascular imaging guidance allowed for safe PCI with zero contrast. The later series, however, excluded individuals with significant calcification in tortuous vessels and only performed RA on two lesions. It also only included patients with CCS. Patients with advanced CKD were more likely to present with acute coronary syndrome than stable angina according to a prior case-control study.34 Our study included 79.2% chronic coronary syndrome 20.8% acute coronary syndrome, which is more consistent in real world. Similar results could be found in Abd et al’s trial.5
Previous research had shown that elective RA saves surgery time, radiation, and, most critically, contrast use when compared to bailout RA.35,36 In our study, 87.5% patients in study group performed RA electively, not only basing on IVUS findings but also because some IVUS catheters failed to pass through the lesion. Additionally, we discovered that the IVUS catheter enables a detailed assessment of the lesion and side branch to decide whether a one- or two-stent strategy could improve the effect of procedural and clinical outcomes. There were no statistically significant differences in the occurrence of complications such as slow flow/no flow, perforation/rupture, pericardial effusion, and stent thrombosis of two groups.
Our study found that IVUS catheterization did not extend the operation or expose patients to a higher radiation dosage. This is due to the fact that calcified lesions make it more difficult for the balloon and stent to pass through them, and IVUS catheterization enables clinicians to choose the best balloon size, burr diameter, and stent size for PCI. All of these elements would aid in making the PCI process quicker and more precise. Because their doctors were concerned that they would develop contrast nephropathy, which had a negative effect on their clinical outcomes, some patients with coronary artery disease and chronic renal insufficiency even did not have PCI. Because the contrast was only utilised before and during coronary angiography, with an average dose of just 32 mL, we found that the risk of contrast-associated acute kidney damage (AKI) was exceedingly low in patients with chronic renal insufficiency having IVUS-guided RA PCI.
Some limitations exist in our research. First of all, it was a single-center study with a tiny sample size. Second, those who have persistent complete occlusions are excluded. Third, our investigation did not include any physiological evaluations like fractional flow reserves. Fourth, there may be a selection bias on bur size, one- or two-stent strategies due to the fact that different operators had different experiences using the RA approach. Therefore, larger prospective multicenter trials must be conducted in order to show the clinical value of IVUS-guided RA in chronic renal illness. However, our investigation showed that in high-risk CKD patients, low-contrast IVUS-guided PCI supported by RA is safe and feasible.
Conclusion
An IVUS-guided RA PCI method in chronic renal patients with complex coronary calcification is efficient and safe, and can also reduce the contrast volume and possibly the rate of contrast-related AKI. In conclusion, this single-center study suggests that using IVUS to guide rotational atherectomy for calcified coronary artery lesions in patients with chronic renal disease may be a safe and effective approach. The use of IVUS allowed for more precise sizing of the rotational atherectomy burrs and identification of the extent of calcification, which may have contributed to improved procedural outcomes. However, the study’s findings should be interpreted with caution, given its limitations, including the small sample size, short-term follow-up, and lack of a control group. Further research is needed to confirm these findings and assess the long-term clinical outcomes of this approach.
Abbreviations
PCI, percutaneous coronary intervention; AKI, acute kidney injury; CKD, chronic kidney disease; IVUS, intravascular ultrasound; RA, rotational atherectomy; TVR, target vessel revascularization.
Informed Consent Statement
The participants were fully informed about the purpose of the study and written informed consent has been obtained from them to publish this paper.
Funding
This study was funded by the application of intravascular coronary ultrasound (IVUS) in coronary rotational atherectomy technique (No. XM2021016).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nakamura S, Ishibashi-Ueda H, Niizuma S, Yoshihara F, Horio T, Kawano Y. Coronary calcification in patients with chronic kidney disease and coronary artery disease. Clin J Am Soc Nephrol. 2009;4(12):1892–1900. doi:10.2215/CJN.04320709
2. Sakakura K, Ito Y, Shibata Y, et al. Clinical expert consensus document on rotational atherectomy from the Japanese Association of Cardiovascular Intervention and therapeutics. Cardiovasc Interv Ther. 2021;36(1):1–18. doi:10.1007/s12928-020-00715-w
3. Lu L, Dong J, Liu Y, et al. New insights into natural products that target the gut microbiota: effects on the prevention and treatment of colorectal cancer. Front Pharmacol. 2022;13:964793. doi:10.3389/fphar.2022.964793
4. Zhang C, Li J, Xiao M, et al. Oral colon-targeted mucoadhesive micelles with enzyme-responsive controlled release of curcumin for ulcerative colitis therapy. Chin Chem Letters. 2022;33(11):4924–4929. doi:10.1016/j.cclet.2022.03.110
5. Allali A, Traboulsi H, Sulimov DS, et al. Feasibility and safety of minimal-contrast IVUS-guided rotational atherectomy for complex calcified coronary artery disease. Clin Res Cardiol. 2021;110(10):1668–1679. doi:10.1007/s00392-021-01906-y
6. Klersy C, Ferlini M, Raisaro A, et al. Use of IVUS guided coronary stenting with drug eluting stent: a systematic review and meta-analysis of randomized controlled clinical trials and high quality observational studies. Int J Cardiol. 2013;170(1):54–63. doi:10.1016/j.ijcard.2013.10.002
7. Maehara A, Mintz GS, Witzenbichler B, et al. Relationship between intravascular ultrasound guidance and clinical outcomes after drug-eluting stents. Circ Cardiovasc Interv. 2018;11(11):e006243. doi:10.1161/CIRCINTERVENTIONS.117.006243
8. Xu H, Van der Jeught K, Zhou Z, et al. Atractylenolide I enhances responsiveness to immune checkpoint blockade therapy by activating tumor antigen presentation. J Clin Invest. 2021;131(10). doi:10.1172/JCI146832
9. Dobrzycki S, Reczuch K, Legutko J, et al. Rotational atherectomy in everyday clinical practice. Association of Cardiovascular Interventions of the Polish Society of Cardiology (Asocjacja Interwencji Sercowo-Naczyniowych Polskiego Towarzystwa Kardiologicznego - AISN PTK): expert opinion. Kardiol Pol. 2018;76(11):1576–1584. doi:10.5603/KP.2018.0225
10. Aziz A, Bhatia G, Pitt M, et al. Intravascular lithotripsy in calcified-coronary lesions: a real-world observational, European multicenter study. Catheter Cardiovasc Interv. 2021;98(2):225–235. doi:10.1002/ccd.29263
11. Yu Y, Wang L, Ni S, et al. Targeting loop3 of sclerostin preserves its cardiovascular protective action and promotes bone formation. Nat Commun. 2022;13(1):4241. doi:10.1038/s41467-022-31997-8
12. Ge J, Wang W, Huo Y. Chinese expert consensus on coronary internal rotational surgery. Chin J Intervent Cardiol. 2017;25(2):61–66.
13. Mehran R, Nikolsky E. Contrast-induced nephropathy: definition, epidemiology, and patients at risk. Kidney Int Suppl. 2006;100:S11–S15. doi:10.1038/sj.ki.5000368
14. Inker LA, Astor BC, Fox CH, et al. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am J Kidney Dis. 2014;63(5):713–735. doi:10.1053/j.ajkd.2014.01.416
15. Zhang X, Qu Y, Liu L, et al. Homocysteine inhibits pro-insulin receptor cleavage and causes insulin resistance via protein cysteine-homocysteinylation. Cell Rep. 2021;37(2):109821. doi:10.1016/j.celrep.2021.109821
16. Matsushita K, Ballew SH, Coresh J, et al. Measures of chronic kidney disease and risk of incident peripheral artery disease: a collaborative meta-analysis of individual participant data. Lancet Diabetes Endocrinol. 2017;5(9):718–728. doi:10.1016/S2213-8587(17)30183-3
17. Matsushita K. Chronic Kidney Disease Prognosis Consortium: これまでの成果と今後の方向性 [Chronic kidney disease prognosis consortium: achievements and future directions]. Nihon Jinzo Gakkai Shi. 2015;57(8):1290–1296. Japanese.
18. Charytan DM, Natwick T, Solid CA, Li S, Gong T, Herzog CA. Comparative effectiveness of medical therapy, percutaneous revascularization, and surgical coronary revascularization in cardiovascular risk subgroups of patients with CKD: a retrospective cohort study of medicare beneficiaries. Am J Kidney Dis. 2019;74(4):463–473. doi:10.1053/j.ajkd.2019.04.018
19. Liu F, Zhao X, Zhu Z, Zhai Z, Liu Y. Dual-microphone active noise cancellation paved with Doppler assimilation for TADS. Mech Syst Signal Process. 2023;184:109727. doi:10.1016/j.ymssp.2022.109727
20. Duan C, Deng H, Xiao S, et al. Accelerate gas diffusion-weighted MRI for lung morphometry with deep learning. Eur Radiol. 2022;32(1):702–713. doi:10.1007/s00330-021-08126-y
21. Fujii K, Carlier SG, Mintz GS, et al. Stent underexpansion and residual reference segment stenosis are related to stent thrombosis after sirolimus-eluting stent implantation: an intravascular ultrasound study. J Am Coll Cardiol. 2005;45(7):995–998. doi:10.1016/j.jacc.2004.12.066
22. Lu S, Yang B, Xiao Y, et al. Iterative reconstruction of low-dose CT based on differential sparse. Biomed Signal Process Control. 2023;79:104204. doi:10.1016/j.bspc.2022.104204
23. Ban Y, Wang Y, Liu S, et al. 2D/3D multimode medical image alignment based on spatial histograms. Appl Sci. 2022;12(16):8261. doi:10.3390/app12168261
24. Moussa I, Di Mario C, Moses J, et al. Coronary stenting after rotational atherectomy in calcified and complex lesions. Angiograph Clin Follow Up Results Circ. 1997;96(1):128–136.
25. Qin X, Ban Y, Wu P, et al. Improved image fusion method based on sparse decomposition. Electronics. 2022;11(15):2321. doi:10.3390/electronics11152321
26. Liu H, Liu M, Li D, Zheng W, Yin L, Wang R. Recent advances in pulse-coupled neural networks with applications in image processing. Electronics. 2022;11(20). doi:10.3390/electronics11203264
27. Kinnaird T, Gallagher S, Sharp A, et al. Operator volumes and in-hospital outcomes: an analysis of 7740 rotational atherectomy procedures from the BCIS national database. JACC Cardiovasc Interv. 2021;14(13):1423–1430. doi:10.1016/j.jcin.2021.04.034
28. Nikolsky E, Mehran R, Lasic Z, et al. Low hematocrit predicts contrast-induced nephropathy after percutaneous coronary interventions. Kidney Int. 2005;67(2):706–713. doi:10.1111/j.1523-1755.2005.67131.x
29. Dangas G, Iakovou I, Nikolsky E, et al. Contrast-induced nephropathy after percutaneous coronary interventions in relation to chronic kidney disease and hemodynamic variables. Am J Cardiol. 2005;95(1):13–19. doi:10.1016/j.amjcard.2004.08.056
30. Giacoppo D, Madhavan MV, Baber U, et al. Impact of contrast-induced acute kidney injury after percutaneous coronary intervention on short- and long-term outcomes: pooled analysis from the HORIZONS-AMI and ACUITY trials. Circ Cardiovasc Interv. 2015;8(8):e002475. doi:10.1161/CIRCINTERVENTIONS.114.002475
31. Ali ZA, Karimi Galougahi K, Nazif T, et al. Imaging- and physiology-guided percutaneous coronary intervention without contrast administration in advanced renal failure: a feasibility, safety, and outcome study. Eur Heart J. 2016;37(40):3090–3095. doi:10.1093/eurheartj/ehw078
32. Yang B, Li Y, Zheng W, et al. Motion prediction for beating heart surgery with GRU. Biomed Signal Process Control. 2023;83:104641. doi:10.1016/j.bspc.2023.104641
33. Pan Z, Zhong H, Huang D, Wu L, He X. Beneficial effects of repeated washed microbiota transplantation in children with autism. Front Pediatr. 2022;10. doi:10.3389/fped.2022.928785
34. Go AS, Bansal N, Chandra M, et al. Chronic kidney disease and risk for presenting with acute myocardial infarction versus stable exertional angina in adults with coronary heart disease. J Am Coll Cardiol. 2011;58(15):1600–1607. doi:10.1016/j.jacc.2011.07.010
35. Allali A, Abdel-Wahab M, Sulimov DS, et al. Comparison of bailout and planned rotational atherectomy for heavily calcified coronary lesions: a single-center experience. J Interv Cardiol. 2017;30(2):124–133. doi:10.1111/joic.12361
36. Kawamoto H, Latib A, Ruparelia N, et al. Planned versus provisional rotational atherectomy for severe calcified coronary lesions: insights From the ROTATE multi-center registry. Catheter Cardiovasc Interv. 2016;88(6):881–889. doi:10.1002/ccd.26411
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.