Back to Journals » Journal of Blood Medicine » Volume 14
A Single Center Study Investigating Clinical Outcomes of Testing for Multiple Myeloma and Immune Deficiency at Low Globulin Levels
Authors Ramasamy I ![]()
Received 6 March 2023
Accepted for publication 23 May 2023
Published 30 May 2023 Volume 2023:14 Pages 345—358
DOI https://doi.org/10.2147/JBM.S409234
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Indra Ramasamy
Department of Blood Sciences, Worcester Royal Hospital, Worcester, UK
Correspondence: Indra Ramasamy, Worcester Royal Hospital, Charles Hastings Way, Worcester, WR51DD, United Kingdom, Email [email protected]
Background: Both primary (e.g. common variable immune deficiency, CVID) and secondary immune deficiency as well as multiple myeloma (MM) require medical intervention and treatment delay can exacerbate morbidity. This study investigated the potential importance of low levels of calculated globulin to detect immune deficiency and MM associated with immunoparesis (light chain, non-secretory MM).
Methods: One hundred and thirty-nine patient serum samples from community physicians and outpatient clinics for liver function tests with low calculated globulin (< 16 g/L, RR 18– 37 g/L) levels were screened for immunoglobulins and protein electrophoresis. Further, 110 patients with globulin levels ≤ 16 g/L with screening for immunoglobulin levels and protein electrophoresis, requested through routine clinical care, were included in the analysis.
Results: Approximately 47% of patients in this cohort had secondary antibody deficiency as a result of hematological malignancy. Secondary iatrogenic (immunosuppressants, antiepileptic drugs) immune deficiency was detected in 20% of patients and a significant percentage of the patients were found by reflex testing at globulin levels < 16 g/L. During the study period the screening detected new light chain and non-secretory MM in 2.2% of patients. Three patients with CVID and six patients with light chain myeloma were previously detected by screening, consequently alerting clinicians and reducing delay in treatment. A further 23% with several co-morbid conditions showed unexpected hypogammaglobulinemia; in this category, the study identified a subgroup that required further investigation.
Conclusion: Investigation of low globulin levels detects patients with primary and secondary immune deficiency and MM. Optimizing treatment for decreased immunoglobulins in patients with other clinical co-morbidities may require increased clinician awareness and watchful clinical and laboratory assessment.
Keywords: calculated globulin, primary immune deficiency, common variable immune deficiency, secondary immune deficiency, light chain myeloma, non-secretory myeloma
Highlights
- We investigated the value of low globulin levels in the diagnosis of immune deficiency and multiple myeloma in a routine clinical laboratory.
- Low globulin levels identified patients with (i) immune deficiency, (ii) multiple myeloma, (iii) iatrogenic secondary immune deficiency (SID), (iv) SID in hematological malignancies and (v) idiopathic hypogammaglobulinemia.
- Patients with hematological malignancies were more likely to be monitored for SID than those on antiepileptic or immunosuppressant treatment.
- A subgroup of patients with unexpected hypogammaglobulinemia will benefit from further clinical evaluation.
Introduction
Calculated globulin (total protein-albumin) is part of the liver function test profile. The main use of calculated globulin is to determine paraprotein concentrations at high levels. There are few studies to investigate the use of globulin values below the reference range to detect both antibody deficiencies or new minor paraproteins associated with hypogammaglobulinemia (immunoparesis) e.g. light chain myeloma or non-secretory multiple myeloma. Both diagnoses are important because of the requirement for medical intervention and morbidity associated with delay in diagnosis which requires the use of health resources. Diagnostic and consequent treatment delay occurs when there is a failure to consider immune deficiency or multiple myeloma (MM) in patients with appropriate clinical presentation.
Approximately 15% of patients with myeloma have light chain myeloma. Light chain multiple myeloma has a more aggressive disease course and poor outcome. Renal failure, bone disease and amyloidosis appear to be more frequent in these patients.1 Non-secretory multiple myeloma is a rare variant of multiple myeloma, because of its rarity there is a paucity of data regarding prognosis, though it appears to be less aggressive than light chain multiple myeloma.2
A comprehensive process for the detection of primary immune deficiency (PID) and secondary immune deficiency (SID) has not been explored. The genetics of PID is complex. The clinical presentation of PID, and one of the most common symptomatic primary immune deficiency disorders, common variable immune deficiency (CVID) is broad and may present as predominantly recurrent infections or may present with autoimmune, inflammatory conditions or malignancy.3,4 Secondary immune deficiency is more common than PID, and may present within a wider range of specialties and is associated with an increased risk of infection.5 Calculated globulin may be low in hypogammaglobulinemia. However, there is possibility for changes in other proteins to mask hypogammaglobulinemia e.g. acute phase proteins, such as complement and alpha1-antitrypsin can increase during inflammatory conditions causing an increase in calculated globulins. Transient hypogammaglobulinemia has been associated with respiratory infections; as the infection resolved, serum immunoglobulins returned to normal.6
Previous studies, in the UK, have indicated that calculated globulins facilitate early diagnosis of patients with unsuspected hypogammaglobulinemia and that the use of calculated globulin in screening for antibody deficiency may shorten the latency period for correct management of patients with immune deficiency.7,8 Both studies reviewed the detection of immune deficient patients using information from calculated globulin levels. An Australian study assessed the sensitivity and specificity of detection of hypogammaglobulinemia at low calculated globulin values, though the underlying clinical conditions for low immunoglobulin levels were not explored.9
New evidence suggests that patients with SID and PID are at greater risk of morbidity and mortality during pandemic periods such as during the Covid-19 pandemic.10 Identification of patients with immune deficiency at increased risk of co-morbidities during pandemics is relevant as public health guidelines to protect this group of vulnerable patients and to decrease adverse outcomes in PID and SID patients are required.
We report here on real life experience in the detection of immune deficiency or MM associated with immunoparesis in a district general hospital when protein electrophoresis and immunoglobulins were either requested by the physician or analysed as a result of opportunistic screening of serum samples with calculated globulin levels below the reference range. Unlike previous studies, this study evaluates the utility of investigating calculated globulins below the reference range for MM, PID and SID in a non-teaching hospital setting. In Worcestershire, UK, patients with globulin values outside the reference range are screened for protein electrophoresis and immunoglobulins. The screening service was started in 1977.11 Worcester Royal Hospital (WRH) provides pathology services to a population of approximately 500,000 in both primary and secondary care. Opportunistic screening (or reflex testing) is part of the service offered by the laboratory, which in addition carries out protein electrophoresis requested through routine clinical care. In this cross-sectional observational study we investigated the advantages and disadvantages of low globulin values for the detection of both immune deficiency and MM with immunoparesis. We further review the cost implications to the health-care system of the protocol used at the WRH.
Materials and Methods
Selection of Patients and Primary Outcome
Serum samples sent for liver function tests were reflex tested for protein electrophoresis and immunoglobulins at globulin values <16 g/L (reference range 18–37 g/L) in patients ≥30 years of age. Calculated globulin values were derived from liver function tests by subtracting albumin from total protein. Opportunistic screening (reflex testing) was performed if previous protein electrophoresis results were not available for a period of 12 months. Reflex testing was discretionary as hospital inpatients and outpatient patients from rheumatology, gastroenterology and non-hematologic oncology clinics were excluded from reflex testing since changes in immunoglobulin levels in these patients were likely to be due to other pathology or treatment and monitoring of patients was carried out by their individual specialties.
The study was designed as a retrospective cross-sectional observational study with data collected during the period January 1, 2019 to December 31, 2019. The laboratory information management system (WinPath, Clinisys, UK) enabled the reflex testing and automatic addition for immunoglobulin and protein electrophoresis analysis based on globulin levels, using a comprehensive WinPath code system. In addition, protein electrophoresis and immunoglobulin requested through routine clinical care in patients with globulin ≤16 g/L were incorporated in the study. Data on patient samples reflex tested for protein electrophoresis and immunoglobulins as well as patient samples with globulin ≤16 g/L with routine requests for immunoglobulin and protein electrophoresis were collected using the laboratory information management system. Discretionary reflex testing was carried out on all samples with globulin levels <16 g/L every 12 months. The protocol was designed to include all patients with globulin levels ≤16 g/L with immunoglobulin and protein electrophoresis results during 2019 (Flow chart, Figure 1). Decrease in diagnostic delay was defined if the onset of symptoms preceded the diagnosis of myeloma/primary immune deficiency and the globulin levels were identified by reflex testing other than by routine requests for immunoglobulins. The primary end point of the study was the detection rate of both immune deficiency and MM as well as the diagnosis of patients with globulin values ≤ 16 g/L who were identified by both opportunistic screening and routine requests.
 |
Figure 1 Flow chart of analysis of patient samples. |
Analytical Methods
Patients with immunoglobulin levels below the limit of quantitation were assigned the lower limit of quantitation for calculation purposes. Total protein was measured using the biuret method and albumin using the bromocresol green method (Roche, UK). The analytical method for detection, typing and quantitation of paraprotein was capillary electrophoresis and immunosubtraction using Capillarys or immunofixation carried out using Hydragel (Sebia, UK). Serum free light chains were measured using Optilite (Binding site, UK) and immunoglobulins were measured on Cobas (Roche, UK).
Clinical comment was added if IgG <6 g/L or if two or more immunoglobulin classes were below the reference range and a known cause of hypogammaglobulinemia was excluded. The clinical comment stated “exclude the following causes of low immunoglobulins, immunosuppressive drugs, antiepileptic drugs, hematological malignancies and renal/gastrointestinal protein loss. If the above causes excluded functional antibody studies suggested as a first step to investigate for primary immune deficiency states”. In patients <30 years of age reflex testing for protein electrophoresis was excluded as MM was unlikely in this group. The comment “Persistent decrease in globulin levels may require the measurement of immunoglobulin” was added to results with globulin levels below the reference range in patients ≥ 18 to <30 years of age. Clinical information for patients was obtained from electronic notes. If the information in patient electronic notes was incomplete, community physicians were contacted either by email or by telephone, for further clinical details.
Statistical Analysis
After exclusion of duplicates a total of 249 samples were tested for both immunoglobulin and protein electrophoresis, 139 were reflex tested at globulin levels <16 g/L. One hundred and ten patient samples with globulin levels ≤16 g/L and protein electrophoresis and immunoglobulin requested through routine clinical care were included in the analysis. Statistical analysis was performed and graphs constructed using GraphPad Prism (UK). All patient data were analysed and patient confidentiality maintained in accordance with NHS data protection policy12,13 and the Declaration of Helsinki.
Results
The mean age of the 249 patients was 70 years (range 33–97), and 50% were females. The IgG concentration according to globulin levels is given in Figure 2. The mean IgG values differed significantly (ρ<0.001) between each group. The diagram shows a wide distribution of IgG values at each globulin level. It is significant that low IgG levels of <3 g/L are found at globulin values of 16 g/L, suggesting that the distribution of decreased IgG levels will extend to globulin levels >16 g/L and that a higher cut-off level may be indicated. A globulin cut-off level of 16 g/L was considered cost effective and practical as it resulted in reflex testing of 2–3 patient sera for protein electrophoresis and immunoglobulin measurements per week. In this group 26% of samples had IgG values ≤3 g/L, 49% had IgG values ≤4 g/L and 86% had IgG values ≤6 g/L, indicating a high positive predictive value for hypogammaglobulinemia. A summary of results according to diagnosis are in Table 1. Follow-up of patients during the year following the first diagnostic sample identified 15/249 patients (globulin values 14–16 g/L) who died (causes varied from co-existing morbidities, n = 7; light chain myeloma n = 3; hemato-oncology, n = 5) during the year of the study.
 |
Table 1 Diagnosis of Patients with Globulin Levels ≤ 16 g/L |
 |
Figure 2 IgG levels at different globulin concentrations. The lower reference range of IgG = 7 g/L is indicated by the horizontal line in the figure. IgG <3 g/L has been converted to 3 g/L in the graph. |
Patient Subgroup Clinical Details
Hematology Patients
The specialty with highest number samples (116/249, 46.5%) with low globulins was hematology (Figure 3). The diagnostic groups were chronic lymphocytic leukemia (CLL), multiple myeloma, follicular lymphoma, non-Hodgkin lymphoma (NHL), mantle cell lymphoma, marginal zone lymphoma, T-cell lymphoma, Waldenström’s macroglobulinemia (WM), IgD myeloma, acute myeloid leukemia (AML), polycythemia rubra vera, acute lymphoid leukemia (ALL) and chronic myeloid leukemia (CML) (Figure 4).
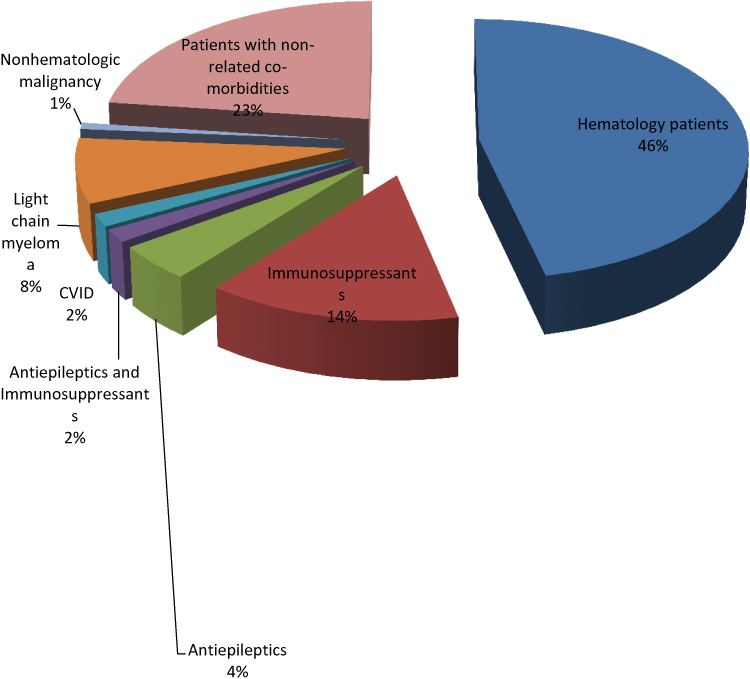 |
Figure 3 Diagnosis of patients with globulin levels ≤ 16 g/L. |
 |
Figure 4 Hematology subgroups. |
Thirty-six percent of the patients were reflex tested for immunoglobulins and protein electrophoresis based on low globulin values. In these patients with SID those who showed an increased predisposition to infection were treated either with prophylactic antibody or intravenous immunoglobulin. Twelve percent of NHL patients, 20% of CLL patients, 11% of lymphoma patients, and 1 of 3 patients with WM were under prophylactic treatment for SID.
Reflex testing (globulin = 14 g/L) showed a minor paraprotein band (<3 g/L) in a patient who presented with nausea and weight loss. Bone marrow showed extensive plasma cell infiltration and review showed lytic bone lesions. The patient’s serum free light chains were kappa = 5.52 mg/L (reference range (RR) 3.3–19.4), lambda = 3.74 mg/L (RR 5.7–26.3) and immunoglobulins IgG 3.1 g/L (RR 7–16), IgA 0.19 g/L (RR 0.7–4.0) and IgM 0.1g/L (RR 0.4–2.3). The patient was diagnosed with non-secretory myeloma. In this patient (1/139) screening identified significant disease and the finding of non-secretory myeloma was made following investigation prompted by the detection of immunoparesis.
Immunosuppressant Treatment
Clinical details on patients treated with immunosuppressants were ulcerative colitis, vasculitis, polymyalgia rheumatica, nephrotic syndrome, asthma, giant cell arteritis, rheumatoid arthritis, renal transplant and Crohn’s disease. Of the 35 patients on immunosuppressant treatment, 16 were treated with glucocorticoids, 13 were treated with both corticosteroid and immunosuppressants (methotrexate, azathioprine, sulfasalazine, tacrolimus), five were treated with immunosuppressants only and a single patient was on clozapine. Low immunoglobulins were detected by reflex testing in 89% of patients.
Of the 16 patients on glucocorticoid treatment two were under observation for increased infections and possible prophylactic treatment.
Antiepileptic Drugs
Immunoglobulin levels below the reference range were detected in 11 patients treated with antiepileptic drugs. Antiepileptic drugs associated with a reduction in immunoglobulin levels were carbamazepine, phenytoin, gabapentin, lamotrigine, levetiracetam and pregabalin. Four patients were on combined treatment with both antiepileptic drugs and immunosuppressants. Decreased immunoglobulins were detected by reflex testing in 80% and 75% of patients who were on antiepileptic drugs or combined treatment. A single patient on combined treatment with a diagnosis of multiple sclerosis was under the observational care of a specialist in immunology following the report of SID.
Unlike SID linked to hematological malignancies, the approach described here highlights the challenges in identifying and assessing patients with SID secondary to iatrogenic causes and associated with other co-morbidities. In the study cohort, the number of immune deficiency patients identified by automated reflex testing was increased in the latter groups when compared with immunosuppressed patients with hematological malignancies (Table 1, p <0.001). In addition patients were less likely to be referred for immunology/hematology review and further treatment (p <0.001).
Oncology Patients Undergoing Treatment
Low immunoglobulins were detected in two patients with breast or renal cancer and on treatment. Of these one patient was detected with low immunoglobulins by reflex testing with an IgG = 3.1 g/L. Neither patient was under investigation for SID.
Primary Immune Deficiency
Four patients with CVID were seen during the study, three of whom were detected in the previous 9 years by reflex testing and the fourth patient by routine diagnostic request. All three patients were diagnosed by reflex testing prior (globulin levels < 16 g/L) to the study, within the same screening program, and were included in the study as they presented with persistent total globulin values ≤16 g/L in 2019. Review by a specialist in immunology and initiation of treatment followed the detection of immunoparesis by reflex testing. Delay in recognition of the underlying diagnosis can result in recurrent infections and irreversible end organ damage such as bronchiectasis. The impact of screening at low globulin levels for the diagnosis of clinically significant disease and the effect of diagnostic delay is shown in example 1 (Supplementary Materials).
Abnormal Serum Free Light Chains
Of the 20 patients with abnormal serum free light chains six were reported by reflex testing, in the 9 years prior to the start of the study (by the same screening program, globulin levels <16 g/L), four with light chain monoclonal gammopathy of undetermined significance (MGUS) and two with light chain myeloma. All six patients were reviewed by hematologists following the detection of immunoparesis and abnormal serum free light chains. Treatment was commenced on the two patients diagnosed with light chain myeloma. Of the 20 patients 1/20 was treated with prophylactic antibody to prevent infection. Two patients with light chain myeloma were detected following routine requests for immunoglobulin and protein electrophoresis during the study period. A single patient was identified by reflex testing (globulin =14 g/L) with abnormal serum free light chains kappa =11.62 mg/L (RR 3.3–19.4), lambda = 250.14 mg/L (RR 5.7–26.3), during the course of the study, a detection rate of 0.7% (1/139) for patients with abnormal serum free light chains. The patient presented with severe back pain treated with morphine. The patient died prior to hematology follow-up. Patient review shows that early diagnosis of myeloma patients can alter the performance status of the patient and define fit versus frail patients and consequent selection for treatment.14 A further case study (Example 2 is included in Supplementary Materials) shows the impact of diagnostic delay on treatment. In this patient, there was a delay in diagnosis of light chain myeloma and the patient was found to have vertebral lesions, which can cause severe morbidity.
Patients with Low Globulin Values of Unknown Cause: “Idiopathic” Hypogammaglobulinemia
The study found unsuspected antibody deficiency in 57 (57/249 = 22.9%) patients with other co-morbidities (Figure 5). Low globulins were transient in 11 patients. Eleven patients (11/57, 19%) were referred by community physicians for further review by either hematology or immunology specialist medical practitioners; review of patient notes suggest that myelodysplastic syndrome was suspected in one of these patients and advice was to keep up to date with vaccines in a second patient. A further patient presented with persistently low immunoglobulins from 2014, with immunoglobulin levels: IgG = 3.9 g/L, IgA = 0.43 g/L, IgM = 0.37 g/L. The patient had a past history of heart failure, chronic kidney disease, hypertension and osteoarthritis. The patient treatment included thyroxine, amlodipine, fluoxetine, warfarin, bisoprolol and simvastatin. The patient did not present with clinical symptoms of increased infection or night sweats and was assigned to monitoring.
 |
Figure 5 Follow-up details on patients with globulin ≤ 16 g/L, idiopathic hypogammaglobulinemia. |
Eight patients (8/57, 14%) were tested for specific antibody response to vaccines, and 5/57 (9%) showed a decreased antibody response to tetanus, hemophilus and pneumococcus challenge. Immunology advice was requested for 1/5 patients, with subnormal vaccine response and IgG <3 g/L. Advice from specialist immunologist was to keep up to date with vaccinations, and for further specialist immunology opinion if there was an increase in rate of infections. A patient with IgG = 4.3 g/L, was not followed up further. Three further patients with IgG = 4.0 g/L, IgG = 4.8 g/L and IgG = 4.7 g/L with several co-morbidities (depression, frailty, Alzheimer’s disease) were assigned to monitoring should symptoms develop.
The remaining 27 patients presented with several co-morbidities (myocardial infarction, hemochromatosis, Parkinson’s disease). This cohort included the following: two patients who presented with recurrent UTI, with an IgG 5.4 g/L and antibody response to vaccines within reference range, and IgG 4.8 g/L who were not examined further. A further patient with a prior history of testicular and colorectal cancer and low calculated globulin was found to have low immunoglobulins by reflex testing in 2019 (IgG = 3.3 g/L, IgA = 0.77 g/L, IgM = 0.43 g/L). The patient’s immunoglobulins remained below reference range in 2021, and serum free light chains and antibody response to tetanus, hemophilus and pneumococcus challenge were within reference range. The incidence of malignancy has been stated as increased in CVID, regular follow-up may be advantageous in this patient should new problems arise.15 It is likely that in patients who during the period of observation were asymptomatic, potential interventions such as antibiotic prophylaxis and treatment and vaccination were not indicated. Treatment may depend on progressive decline in antibody levels and the development of symptoms.16
However, examples 3 and 4 in Supplementary Materials demonstrate the complexity of clinical presentation among the patients classified as idiopathic hypogammaglobulinemia and are examples of patients who would have benefited from earlier as well as more extensive investigation. The examples include a further 1/139 patients in the detection of new, previously unsuspected non-secretory MM during the course of the study.
The study shows the difficulty associated with the diagnosis of “idiopathic hypogammaglobulinemia”. This cohort of patients includes those with transient hypogammaglobulinemia as well as patients with comorbidities who were placed on surveillance should symptoms develop and treatment necessitated. Nineteen of the 57 patients (33%) were further investigated either by referral to hematologists/immunologists or by antibody response to vaccines. Patients were placed under observation for further review should symptoms develop. In these patients presentation is less defined and it is a challenge to determine whether or not to treat. Of the 57 patients two more patients were identified, one of whom with a possible diagnosis of Good syndrome who presented with sepsis would have benefitted from further investigation and treatment. The second patient underwent further investigation for anemia and gastroenterology review prior to diagnosis of non-secretory myeloma. Additional investigation was prompted by this study, following a detection of immunoparesis in 2019 by reflex testing. A summary of diagnostic conclusions in the distinct groups is given in Table 2.
 |
Table 2 Summary of Diagnostic Outcomes |
Discussion
Calculated globulin values have previously been suggested as a useful screening tool for detection of antibody deficiency or small paraprotein bands with immunoparesis,17 however real life evidence supporting this practice is lacking. In WRH protein electrophoresis and measurement of immunoglobulin levels at globulin levels below the reference range were carried out both as a reflex test and as requests through routine clinical care. Both approaches were used to complement each other in the diagnosis of immune deficiency and MM with immunoparesis. The main findings of this study are that both MM with immunoparesis and primary immune deficiency can be detected by this approach. This study further demonstrates that the program detected previously unsuspected secondary antibody deficiencies.
The current cut-off for screening is globulin values <16 g/L. The current study suggests low values of IgG <3 g/L are found at globulin value of 16 g/L, suggesting a higher cut-off value may detect low values of IgG. The value of 16 g/L was considered a practical solution in that 2–3 patient samples were detected per week and 86% of the IgG values detected were below 6 g/L. In WRH selective reflex testing of samples sent to the laboratory in conjunction with requests for investigation of low globulin levels through routine clinical care was considered a practical and cost-effective investigative approach. One previous study suggests that the use of the first percentile of the globulin fraction improved the detection of hypogammaglobulinemia.17
Screening identified approximately 2.2% of the 139 patients screened during 2019 with previously undiagnosed MM. Myeloma is characterized by bone lesions, anemia, renal impairment and immune deficiency. The patients may require prophylaxis and supportive treatment for osteolytic pain, anemia, renal insufficiency, peripheral neuropathy and thromboembolic events. Delay in diagnosis may lead to impairment in quality of life, life expectancy as well as increased health-care costs.14
The study identified three patients with CVID and six patients with light chain myeloma detected by reflex testing, within the same screening program, prior to the start of the study period. This data suggests that both CVID and MM are detected by reflex testing, and that clinically significant disease can be detected by the screening criteria. The patients presented with globulin levels ≤16 g/L and were detected during the study period by the study protocol. It is possible that additional patients diagnosed with CVID or light chain myeloma, by the WRH screening program, prior to the start of the study were under treatment and may no longer present with globulin levels ≤16 g/L. Previous reviews using screening based on globulin cut-off levels, serum electrophoresis and immunofixation detected small paraproteins associated with immunoparesis in 1.2% of samples.7
CVID is one of the common primary immune deficiency disorders encountered in clinical practice. CVID can present with chronic infections of the sinopulmonary tract, however clinical manifestations can be broad and include autoimmunity, splenomegaly, lymphadenopathy as well as an increased incidence of cancers. Genomic studies have revealed an increasing number of genetic causes of the CVID phenotype.18 In studies with CVID patients a mean diagnostic delay of 7.46 years has been observed. As the presentation of CVID may include non-infectious autoimmune or inflammatory conditions diagnostic delay can result in inappropriate treatment.19 Identification and investigation of patients with low globulin values has the potential to decrease the delay in making the diagnosis.
Secondary immune deficiency caused by hematological malignancies was identified in 46.6% of patients, a significant proportion of the patients were identified by routine clinical requests and a noteworthy number of patients were under treatment for SID. In contrast, a substantial number of patients with SID as a result of antiepileptic or immunosuppressant therapy or a combination of both were identified by reflex testing and an insignificant number of patients were under treatment for SID. Neither of the two patients with non-hematological malignancy and low immunoglobulins were investigated further. With the growth of new treatments for non-hematological oncology patients monitoring of immunoglobulins for SID with a possibility of non-neutropenic sepsis may be indicated. The current study excluded non-hematology oncology patients from reflex testing for protein electrophoresis and immunoglobulins; inclusion of these patients may detect patients at increased risk of hypogammaglobulinemia. It remains to be seen if patients with hypogammaglobulinemia at increased risk of malignancy can be identified by this approach.
Clinical routine requests for immunoglobulins and protein electrophoresis were less likely if the patients were treated with immunosuppressive drugs, antiepileptic drug therapy or clozapine. Patients on clozapine can display clinical patterns resembling CVID.20 In patients with iatrogenic SID, investigation to assess response to vaccination and a trial of prophylactic antibiotic treatment may be indicated. This study suggests limitations in the current response to iatrogenic SID. Further studies are required to define adequacy and type of treatment needed in these patients.21
A further 22.9% with several co-morbidities and non-specific symptoms were identified with hypogammaglobulinemia and a significant number were detected by reflex testing. Transient hypogammaglobulinemia was identified in 19% of this cohort and further advice for a second 19% of the cohort from either hematologists/immunologists identified patients with myelodysplasia or who required up to date vaccination. Of the 9% of the cohort who showed a subnormal response to vaccines, immunology advice was requested for a single patient. There may be instances where patients are assigned to monitoring, however if patients develop symptoms, treatment (e.g. antibiotic administration) may be altered in light of the observed hypogammaglobulinemia. Review of the remaining patients in this cohort identified patients with decreased immunoglobulins (possible Good syndrome, a second with malignancy and a further patient with non-secretory myeloma) who would have benefitted from further investigation.
A number of approaches can be taken to raise the awareness of community physicians to immune deficiency and MM as part of the differential diagnosis of hypogammaglobulinemia as early patient encounters will be with non-specialist community physicians. Coded comments attached to the results can direct the physician to appropriate testing. Another approach is to use direct comments in results to increase awareness of immune deficiency and draw the clinician’s attention to documents (Jeffrey Modell Foundation (JMF) “10 Warning Signs of Immune deficiency” which are widely available; http://www.info4pi.org/library/educational-materials/10-warning-signs)22,23 and describe symptoms associated with immune deficiency. Additionally, the UK myeloma forum has guidelines for the diagnosis and treatment of myeloma (https://www.ukmf.org.uk/guidelines-page/bshukmf-guidelines/).
In WRH, the cost of screening using protein electrophoresis and immunoglobulins is £5:00/test at 2–3 patient requests per week. The study suggests a detection rate of approximately 2.2% for MM during 2019. A review of patients in the study suggests that both CVID and light chain MM were identified by reflex testing in the years prior to 2019. In addition, patients with SID who required further investigation were identified. The economic impact of the screening method has to be balanced by the possibility of decrease in time delay in diagnosis and detection of disease before the onset of end-organ damage which can affect long-term prognosis and the quality of life in patients with immune deficiency and multiple myeloma.14,24 A strong case for detecting antibody deficiency using discretionary laboratory testing at calculated globulin levels below the reference range has been suggested,7 though there are few studies in routine laboratories to investigate its effectiveness. Previous reviews have emphasized the necessity of early diagnosis to prevent complications for both immune deficiency25 and MM.26 Cost-analysis of renal dialysis, should end-organ damage occur in MM, estimates an annual cost of approximately £30,000 per patient for hospital-based hemodialysis in the UK.27 In the USA pneumonia is a major cause of mortality and morbidity and the immunocompromised population can experience a disproportionate burden of pneumonia-related hospitalization. In the USA the annual charge for pneumonia-related hospitalization is over $84 billion.28 On average the cost of reflex testing for immunoglobulins and protein electrophoresis at globulin levels was approximately 136*5=£680 per year. The burden on finite health-care budgets was an important consideration in devising the screening program. The annual detection rate of 2.2%, with an estimated cost of £227 (680/3)/patient detected, suggests an economic benefit to the health-care system.
This is a single center study and bias may have been introduced due to referral characteristics. A limitation of this study is that it evaluated patients ≥30 years of age. Potential further studies would be to assess the value of investigating globulin values ≤16 g/L at <30 years. In the current economic environment the challenge is to appraise an acceptable detection rate without a substantial increase in service cost. The practice at WRH is to use both discretionary screening tests as well as routine requests for immunoglobulins and protein electrophoresis for the diagnosis of both immune deficiency and multiple myeloma at globulin values below the reference range. Screening programs differ in their protocol and the procedure at WRH can be compared with other programs to assist future decisions on the best method to aid in the diagnosis of both MM and immunodeficiency by following globulin levels below the reference range. To our knowledge, this is the first study to include the two different diagnoses within the same program.
Conclusion
The current globulin cut-off value of ≤16 g/L identified both immune deficiency and MM patients. The results show that this approach can detect patients with immunoparesis, thus contributing to inappropriate investigation and delay in treatment. The study identified patients with secondary immune deficiency as well as idiopathic hypogammaglobulinemia. The latter patients were a heterogeneous group who needed close clinical and laboratory assessment for the development of optimal treatment strategies.
Data Sharing Statement
The data are stored in the Laboratory Quality Management System of The Worcester Royal Hospital, and are available following anonymization of patient identifiable information. The full data set can be requested from the corresponding author upon approval of the paper proposal using the data.
Ethics Approval and Consent to Participate
The study was an audit carried out according to the Declaration of Helsinki and the NHS Data Protection Act. Approval for the study was granted by the Research and Ethics Committee of the Worcester Acute Hospitals NHS Trust as per NHS Data Protection Act. Informed verbal consent was obtained from patients and approved by the Research and Ethics Committee of the Worcester Acute Hospitals NHS Trust.
Consent for Publication
The study is a service audit (carried out as a cross-sectional observational study, according to STROBE guidelines). Informed verbal consent was obtained from patients and approved by the Research and Ethics Committee of the Worcester Acute Hospitals NHS Trust.
Author Contributions
I am the sole author of the manuscript and made a significant contribution to the work reported, in the conception, study design, execution, acquisition of data, analysis and interpretation; took part in drafting, revising and critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The author reports no competing interests in this work.
References
1. Zhang J, Sun W, Huang Z, et al. Light chain multiple myeloma, clinic features, responses to therapy and survival in a long-term study. World J Surg Oncol. 2014;12:234. doi:10.1186/1477-7819-12-234
2. Dupuis MM, Tuchman SA. Non-secretory multiple myeloma: from biology to clinical management. Once Targets There. 2016;9:7583–7590. doi:10.2147/OTT.S122241
3. Dilley M, Wangberg H, Noone J, Geng B. Primary immunodeficiency diseases treated with immunoglobulin and associated comorbidities. Allergy Asthma Proc. 2021;42(1):78–86. doi:10.2500/aap.2021.42.200113
4. Cunningham-Rundles C. Common variable immune deficiency: dissection of the variable. Immunol Rev. 2019;287(1):145–161. doi:10.1111/imr.12728
5. Patel SY, Carbone J, Jolles S. The expanding field of secondary antibody deficiency: causes, diagnosis, and management. Front Immunol. 2019;10:33. doi:10.3389/fimmu.2019.00033
6. Greenberger PA, Walker CL, Fitzsimons TE, Roberts M. Hypogammaglobulinemia associated with cytomegalovirus pneumonia. J Infect Dis. 1991;163(3):631–633. doi:10.1093/infdis/163.3.631
7. Holding S, Jolles S. Current screening approaches for antibody deficiency. Curr Opin Allergy Clin Immunol. 2015;15(6):547–555. doi:10.1097/ACI.0000000000000222
8. Jolles S, Borrell R, Zouwail S, et al. Calculated globulin (CG) as a screening test for antibody deficiency. Clin Exp Immunol. 2014;177(3):671–678. doi:10.1111/cei.12369
9. Hoo T, Lim EM, John M, D’Orsogna L, McLean-Tooke A. Calculated globulin as a screening tool for hypogammaglobulinaemia or paraproteins in hospitalized patients. Ann Clin Biochem. 2021;58(3):236–243. doi:10.1177/0004563221989737
10. Shields AM, Burns SO, Savic S, Richter AG; UK PIN COVID-19 Consortium. COVID-19 in patients with primary and secondary immunodeficiency: the United Kingdom experience. J Allergy Clin Immunol. 2021;147(3):870–875. doi:10.1016/j.jaci.2020.12.620
11. Adams RA, Smith L, Pickering PE. The incidence of monoclonal proteins during 7 years of screening in a district general hospital. Immunology. 1984;51(3):451–454.
12. Twycross A, Shorten A. Service evaluation, audit and research: what is the difference? Evid Based Nurs. 2014;17(3):65–66. doi:10.1136/eb-2014-101871
13. NHS England and NHS Improvement. Data Protection Policy. Available from: https://www.england.nhs.uk/wp-content/uploads/2019/10/data-protection-policy-v5.1.pdf.
14. Terpos E, Kleber M, Engelhardt M, et al.; European Myeloma Network. European Myeloma Network guidelines for the management of multiple myeloma-related complications. Haematologica. 2015;100(10):1254–1266. doi:10.3324/haematol.2014.117176
15. Cunningham-Rundles C. How I treat common variable immune deficiency. Blood. 2010;116(1):7–15. doi:10.1182/blood-2010-01-254417
16. Ameratunga R, Ahn Y, Steele R, Woon ST. The natural history of untreated primary hypogammaglobulinemia in adults: implications for the diagnosis and treatment of Common Variable Immunodeficiency Disorders (CVID). Front Immunol. 2019;10:1541. doi:10.3389/fimmu.2019.01541
17. Holding S, Khan S, Sewell WA, Jolles S, Dore PC. Using calculated globulin fraction to reduce diagnostic delay in primary and secondary hypogammaglobulinaemias: results of a demonstration project. Ann Clin Biochem. 2015;52(Pt 3):319–326. doi:10.1177/0004563214545791
18. Maffucci P, Filion CA, Boisson B, et al. Genetic diagnosis using whole exome sequencing in common variable immunodeficiency. Front Immunol. 2016;7:220. doi:10.3389/fimmu.2016.00220
19. Cunningham-Rundles C. Common variable immune deficiency: case studies. Blood. 2019;134(21):1787–1795. doi:10.1182/blood.2019002062
20. Ponsford MJ, Steven R, Bramhall K, et al. Clinical and laboratory characteristics of clozapine-treated patients with schizophrenia referred to a national immunodeficiency clinic reveals a B-cell signature resembling common variable immunodeficiency (CVID). J Clin Pathol. 2020;73(9):587–592. doi:10.1136/jclinpath-2019-206235
21. Jolles S, Chapel H, Litzman J. When to initiate immunoglobulin replacement therapy (IGRT) in antibody deficiency: a practical approach. Clin Exp Immunol. 2017;188(3):333–341. doi:10.1111/cei.12915
22. Arkwright PD, Gennery AR. Ten warning signs of primary immunodeficiency: a new paradigm is needed for the 21st century. Ann N Y Acad Sci. 2011;1238:7–14. doi:10.1111/j.1749-6632.2011.06206.x
23. Subbarayan A, Colarusso G, Hughes SM, et al. Clinical features that identify children with primary immunodeficiency diseases. Pediatrics. 2011;127(5):810–816. doi:10.1542/peds.2010-3680
24. Graziano V, Pecoraro A, Mormile I. Delay in diagnosis affects the clinical outcome in a cohort of CVID patients with marked reduction of IGA serum levels. Clin Immunol. 2017;180:1–4. doi:10.1016/j.clim.2017.03.011
25. Sánchez-Ramón S, Bermúdez A, González-Granado LI, Rodríguez-Gallego C, Sastre A, Soler-Palacín P; ID-Signal Onco-Haematology Group. Primary and secondary immunodeficiency diseases in oncohaematology: warning signs diagnosis, and management. Front Immunol. 2019;10:586. doi:10.3389/fimmu.2019.00586
26. Rajkumar SV. Evolving diagnostic criteria for multiple myeloma. Hematol Am Soc Hematol Educ Program. 2015;2015:272–278. doi:10.1182/asheducation-2015.1.272
27. Roberts G, Holmes J, Williams G, et al. Current costs of dialysis modalities: a comprehensive analysis within the United Kingdom. Perit Dial Int. 2022;42(6):578–584. doi:10.1177/08968608211061126
28. Hayes BH, Haberling DL, Kennedy JL, Varma JK, Fry AM, Vora NM. Burden of pneumonia-associated hospitalizations: United States, 2001–2014. Chest. 2018;153(2):427–437. doi:10.1016/j.chest.2017.09.041
29. Kelleher P, Misbah SA. What is Good’s syndrome? Immunological abnormalities in patients with thymoma. J Clin Pathol. 2003;56(1):12–16. doi:10.1136/jcp.56.1.12
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.