Back to Journals » Journal of Pain Research » Volume 16
A Secondary Analysis: Comparison of Experimental Pain and Psychological Impact in Individuals with Carpometacarpal and Knee Osteoarthritis
Authors Ordonez Diaz T ![]() , Fillingim RB, Cruz-Almeida Y
, Fillingim RB, Cruz-Almeida Y ![]() , Nichols JA
, Nichols JA ![]()
Received 2 June 2023
Accepted for publication 24 October 2023
Published 4 December 2023 Volume 2023:16 Pages 4139—4149
DOI https://doi.org/10.2147/JPR.S421689
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Tamara Ordonez Diaz,1,2 Roger B Fillingim,2,3 Yenisel Cruz-Almeida,2,3,* Jennifer A Nichols1,2,4,*
1J. Crayton Pruitt Family Department of Biomedical Engineering, University of Florida, Gainesville, FL, USA; 2Pain Research & Intervention Center of Excellence, University of Florida, Gainesville, FL, USA; 3Department of Community Dentistry and Behavioral Science, University of Florida, Gainesville, FL, USA; 4Department of Orthopaedics & Sports Medicine, University of Florida, Gainesville, FL, USA
*These authors contributed equally to this work
Correspondence: Jennifer A Nichols, J. Crayton Pruitt Family Department of Biomedical Engineering, University of Florida, 1275 Center Drive, BMS JG-56, PO Box 116131, Gainesville, FL, 32611, USA, Tel +1(352)294-8803, Email [email protected]
Purpose: Evaluate sensory and psychological differences in individuals with thumb carpometacarpal (CMC) and/or knee osteoarthritis (OA) pain. This secondary analysis focuses on comparing the effects of OA at large and small joints in community-dwelling adults.
Patients and Methods: A total of 434 individuals were recruited from communities in Gainesville, FL and Birmingham, AL. Each participant completed health and clinical history questionnaires, quantitative sensory testing, and physical functional tests. Participants were divided into four groups based on their pain (“CMC pain” (n = 33), “knee pain” (n = 71), “CMC + knee pain” (n = 81), and “pain-free” controls (n = 60)). ANCOVAs were performed to identify significant differences in experimental pain and psychological variables across groups.
Results: The “CMC + knee pain” group had lower pressure pain thresholds (lateral knee site, p < 0.01) and higher temporal summation of mechanical pain (knee, p < 0.01) when compared to “CMC pain” and “pain-free” groups. The “knee pain” group had lower heat pain tolerance at the forearm site (p = 0.02) and higher mechanical pain (p < 0.01) at both tested sites in comparison to the “CMC pain” group. Lastly, the “CMC + knee pain” group had the highest self-reported pain (p < 0.01) and disability (p < 0.01) compared to all other groups.
Conclusion: Results suggest knee OA compounded with CMC OA increases disease impact and decreases emotional health compared to OA at either the CMC or knee joint alone. Results also support a relationship between the number of painful joints and enhanced widespread pain sensitivity. Measuring pain at sites other than the primary OA location is important and could contribute to more holistic treatment and prevention of OA progression.
Keywords: thumb, trapeziometacarpal, multi-site OA, generalized OA, quantitative sensory testing
Introduction
Osteoarthritis (OA) is a multifactorial musculoskeletal and degenerative disease that can affect any joint.1 Yet, most studies focus solely on large joints, namely the hip or knee. A systematic review that compared knee, hip, and hand OA found that the hand exhibits the highest radiographic prevalence of OA but is included in the lowest number of studies.2 Moreover, studies typically focus on single-site OA, but OA can affect multiple joints within an individual. For example, it is common for individuals with knee OA to also suffer from hand OA.3,4 The similarities and differences in factors contributing to the clinical presentation of OA at a single, large lower extremity joint; a single, small hand joint; or across multiple joints in the body are unknown, highlighting important knowledge gaps in our understanding of OA phenotypes.
An important aspect of the clinical presentation of OA at any joint is pain. The complexity of osteoarthritic pain is attributed to the combined influences of psychological factors,5 disease pathophysiology,6 and multiple aspects of nociceptive processing, including changes in nociceptive receptors,7,8 presence of neuropathic pain,9–11 and altered pain modulation.12 Notably, recent clinical and experimental studies have shown sensitization of pain pathways during OA, involving changes in joint nociceptors and central nervous system pain processing.13–15 Most of these experimental studies have evaluated pain mechanisms through a combination of psychological assessments and quantitative sensory testing (QST). For example, studies of knee OA have used psychological assessments to inform targeted treatments16–18 and QST to identify clinically meaningful characteristics.19,20
In comparison, although the body of work on hand OA is growing, investigation of somatosensory disparities and phenotypes in individuals with hand OA remains limited.21–26 The few studies that measured pain phenotypes at the hand showed that participants with symptomatic hand OA demonstrated higher self-reported hand pain as well as peripheral26 and central15 sensitization in comparison to healthy or control participants. Similarly, few studies have evaluated alterations in nociceptive processing and/or pain phenotypes in symptomatic, multi-joint OA.27–29 This limited literature means that to our knowledge, no studies focused on hand OA or multi-joint OA with hand involvement include a complete sensory assessment (eg, mechanical and thermal); instead, most studies focus solely on pressure stimulus,25,30 or report clinical or psychological characteristics without QST measures.31 Examining measures of self-reported pain, psychological, and somatosensory function simultaneously may allow more general conclusions regarding altered pain processing in these populations. Further study could also elucidate to what extent results from research examining large joint OA generalize to the small non-load-bearing joints of the hand and/or multi-joint OA.
As a step toward understanding the impact of small, large, and multi-joint involvement on the multidimensional pain experience, this study aimed to evaluate sensory and psychological differences in individuals with carpometacarpal (CMC) OA and/or knee OA compared to “pain-free” controls. CMC OA was chosen as a representative form of small joint OA because it occurs in isolation more frequently than OA at other joints in the hand.32 Knee OA was chosen as a representative form of large joint OA due to its wide study and the fact that it is known to occur concomitantly with hand OA.33 In this secondary analysis of previous studies focused on osteoarthritic disease,34,35 we specifically examined differences in somatosensory (ie, QST) and psychological function across four groups of individuals (ie, only “CMC pain”, only “knee pain”, “CMC + knee pain”, and “pain-free” controls). Given the population demographics, physical examination, and reported symptoms, OA was the most likely cause of pain in the pain groups. We hypothesized that the “CMC + knee pain” group would have significantly higher experimental pain and worse functional impact than the only CMC, only knee, and “pain-free” groups.
Materials and Methods
Study Design
The primary objective of the study was to elucidate differences in pain and psychological limitations in individuals with only “CMC pain”, individuals with only “knee pain”, “CMC + knee pain”, and “pain-free” individuals. This study is a secondary data analysis from community-dwelling individuals that participated in the Understanding Pain and Limitations in OsteoArthritic Disease-1 (UPLOAD1) and Understanding Pain and Limitations in OsteoArthritic Disease-2 (UPLOAD2) studies at the University of Florida (UF) and the University of Alabama Birmingham (UAB). Each of these studies featured distinct cohorts, comprising individuals with knee OA as well as a corresponding control group. These cohorts were merged and analyzed together for the purposes of this study given similarities in inclusion/exclusion criteria, recruitment methods, and study procedures.17,36 Briefly, participants in both studies provided informed consent and completed a series of questionnaires that assessed demographics, functional factors, and psychosocial characteristics. In addition, participants attended a quantitative sensory session (QST) undergoing thermal, mechanical, and temporal summation of pain assessments. Institutional Review Boards at the UF and UAB approved both studies (IRB# 201400209, IRB# 201500906), and a preliminary version of this secondary analysis was published as a conference abstract.37
Participants
Both UPLOAD1 and UPLOAD2, included individuals between 45 and 85 years of age, who self-identified as non-Hispanic Black/African American or non-Hispanic White/Caucasian or European. Posteroanterior and lateral radiographs of the knee were taken to clinically diagnose participants with bilateral or unilateral knee OA.38 Participants were excluded if they had any of the following: 1) clinically significant surgery to the affected (ie, most painful) knee including total joint replacement; 2) systematic rheumatic disorders including rheumatoid arthritis, lupus erythematosus, and fibromyalgia; 3) peripheral neuropathy; 4) psychiatric illness requiring hospitalization within the previous year; 5) cognitive impairment; 6) daily opioid use; 7) uncontrolled hypertension, heart failure, or history of acute myocardial infarction. All participants underwent a physical exam by a clinician, including assessment of pain evoked by manual palpation of carpal and metacarpal joints bilaterally. Given this physical exam and the strict exclusion of rheumatic disorders, the most likely explanation for reported CMC pain is OA; however, presence of CMC OA was not confirmed via radiograph.
Description Quantitative Sensory Testing Procedure
Mechanical
Pressure pain thresholds were evaluated at the medial and lateral aspects of the affected knee, ipsilateral quadriceps, and trapezius using a calibrated algometer (AlgoMed, Medoc). The order of testing sites was randomized for all participants. For each site, a handheld algometer was applied at a constant rate of 30 kPa/second until the participant indicated the sensation “first became painful.” An average pressure pain threshold of three trials was determined for each site. As a safety measure, the maximum pressure that can be applied for the knee sites was 600 kPa and 1000 kPa at the other sites.39
Thermal
Thermal stimuli were applied to the affected knee (or a randomly selected knee for “pain-free” individuals) and ipsilateral ventral forearm using a computer-controlled Medoc PATHWAY Pain & Sensory Evaluation System. Heat pain thresholds and tolerances were assessed using a 16×16 mm thermode. The baseline temperature started at 32C and increased at a rate of 0.5°C/second. For the heat pain threshold, temperature was recorded when participant stated the sensation “first became painful”. Similarly, the temperature was recorded for heat pain tolerance when the participant was no longer able to tolerate the pain.
Temporal Summation (TS)
TS of heat pain was evaluated at the dorsal forearm and the affected knee or randomly selected knee for “pain-free” individuals. Participants were asked to rate the intensity of peak pain during a series of 5 brief and repetitive heat pulses (CHEPS, Medoc). During the trials, 3 different temperatures were used (44°C, 46°C, and 48°C). The difference between the fifth trial and first trial pain rating was used as an indicator of temporal summation of heat pain.
TS of punctate pain was evaluated using a calibrated Von Frey monofilament with a target force of 300 grams. This test was performed at the affected patella or right patella for “pain-free” individuals and back of the left hand in randomized order. Using the pain scale of 0 to 100, participants reported their pain rating after a single contact and after 10 consecutive contacts. The difference between the pain rating after 10 contacts and the pain rating after a single contact was used as an indicator of TS for each site.
Pain Characteristics
Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) was used to assess symptoms of knee OA in the past 48 hours.40 The WOMAC has 3 categories, including pain during activities (5 items), stiffness during the day (2 items), and impairments in physical function (17 items), with higher scores indicating worse outcomes.
Graded Chronic Pain Scale (GCPS) was used to analyze global pain severity and pain-related interference over the past 6 months. Participants were asked to complete a series of 7 items related to pain intensity and pain interference using a 0–10 numeric rating scale. Scores were averaged and multiplied by 10 to generate a GCPS characteristic pain intensity score and GCPS disability score, with higher scores indicating greater pain.
Number of Pain Sites was collected from all participants. They were asked to self-report body site where they experienced pain on most days over the past 3 months. The sum of all areas reported represents the total number of pain sites.
Psychological and Physical Function
Coping Strategies Questionnaire-Revised (CSQ-R) was used to evaluate passive and active coping techniques related to pain.41 Using a 7-point scale, participants rated the frequency with which they engage in various coping techniques (ie, ignoring, praying, catastrophizing). A higher score indicating a greater use of that coping strategy.
Life Orientation Test- Revised (LOT-R) was used to measure how optimistic or pessimistic people feel about the future through a 10-item scale.42 Optimism has been shown to improve physical and mental health and work performance,43 with higher scores indicating more optimism.
Positive and Negative Affect Schedule (PANAS) was used to characterize different feeling and emotions through a set of 20 words associated with positive and negative affect.44 Participants were asked to choose how they generally feel that way on a 1–5-point scale from very slightly to extremely. Higher scores on positive affect demonstrate positive feelings (eg, enthusiasm, energy), while high scores on negative affect demonstrate negative feelings (eg, distress).
Short Physical Performance Battery (SPPB) was used to assess physical function. This battery is a reliable and valid performance-based measure of physical function commonly used for patients with knee OA.34 It evaluates standing balance, 4-meter gait speed, and chair rising tasks. Scores ranging from 0 to 12 are calculated, with lower scores indicating greater functional limitations.
Statistical Methods
Individuals were categorized into four groups based on the baseline questionnaires and health history assessment (Table 1). In addition to indicating no joint pain during their physical examination, the “pain-free” group only included individuals that also scored 0 on the WOMAC-pain and GCPS questionnaires. Definition of these groups enabled testing of our hypothesis that individuals with multi-site OA (“CMC + knee pain” group) would have significantly higher experimental pain and worse psychological impact in comparison to single-site OA (“CMC pain” only and “knee pain” only groups) and “pain-free” individuals.
 |
Table 1 Joint Pain Indicated During Physical Examination |
Data analysis was performed using IBM SPSS software v.28. Values convey the mean ± standard deviation (SD), unless stated otherwise. Demographic characteristics were examined using chi-square for nominal variables and t-tests for continuous/discrete ordinal variables. To assess differences across the four groups, analysis of covariance (ANCOVA) was conducted. Effect sizes are reported as partial eta squared (η2) where η2 = 0.01 indicates a small effect, η2 = 0.06 indicates a medium effect, and η2 = 0.14 indicates a large effect. Fisher's Least Significant Difference (LSD) post hoc tests were performed to compare group means. Location of primary pain differences in QST and psychological measures was examined in a model with no covariates (ie, unadjusted model) and a second model with sex, education, and income as covariates given previous literature45–47 (ie, fully adjusted model). The unadjusted model serves as a baseline, while the adjusted model accounts for significant differences in demographics between groups. Statistical significance was set at p values less than or equal to 0.05.
Results
Demographic and Descriptive Statistics
Two hundred and forty-five of 434 subjects met the eligibility criteria of having either CMC, knee, or CMC and knee pain in this secondary analysis. Significant sex, education, and annual income differences were shown across groups (p < 0.05) (Table 2). There were no significant differences in age or race across groups.
 |
Table 2 Subject Demographics by Location of Primary Pain Groups |
Pain Group Differences in Experimental Pain Measures
The “CMC + knee pain” had significantly lower pressure pain thresholds at the lateral knee site and mechanical TS at the knee in comparison to the only “CMC pain” group and “pain-free” group in the fully adjusted model (all p’s < 0.01) (Table 3). For the unadjusted model, the “CMC + knee pain group” had significantly lower pressure pain threshold at all body sites with exception of the trapezius (all p’s < 0.01), and lower heat pain tolerance (forearm, p < 0.01; knee, p = 0.02) when compared to the only “CMC pain” and “pain-free” groups. The “CMC + knee pain” group also had higher heat induced TS at the forearm (at 46 °C, p < 0.01) in comparison to all other pain groups (Figure 1).
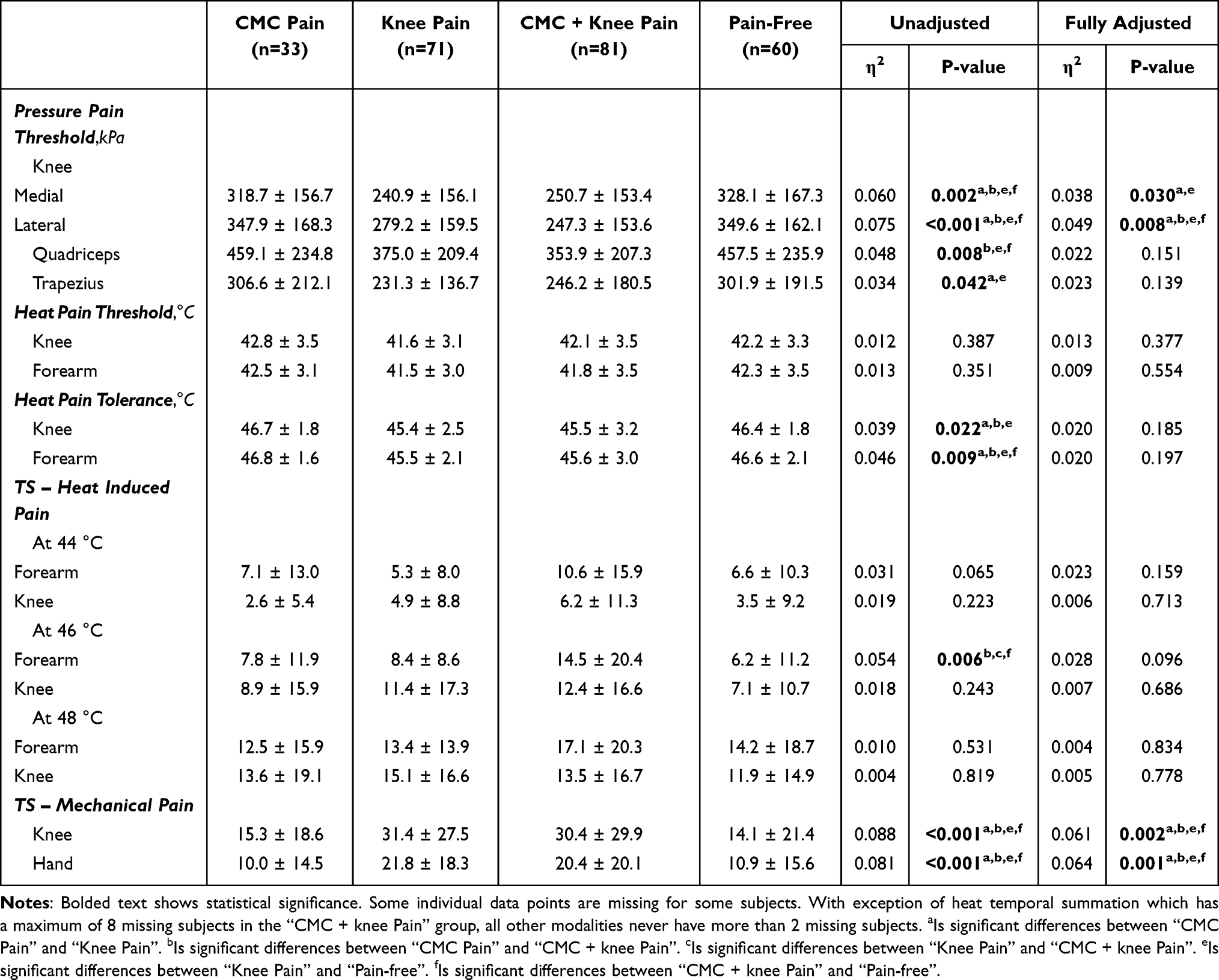 |
Table 3 Results of Quantitative Sensory Testing by Location of Primary Pain Groups (Mean ± SD) and Comparison Across Groups |
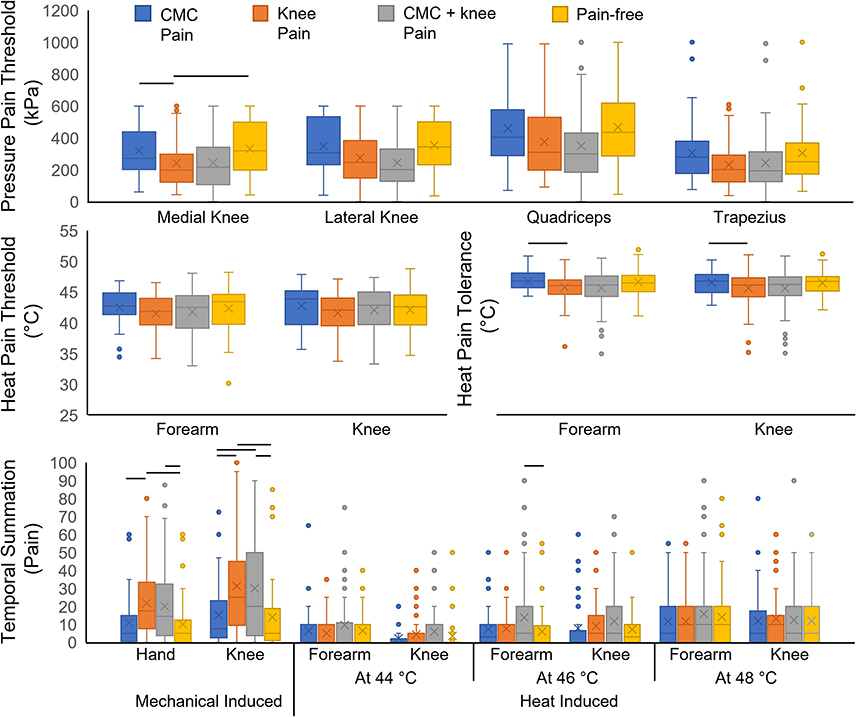 |
Figure 1 Results of quantitative sensory testing by location of primary pain groups. Boxplots represent the distribution of the data, where “x” represents the mean, “—” represents the median, and dots represent outliers. Black lines represent statistically significant differences between cohorts. |
When comparing the only “CMC pain” and “knee pain” groups, the “knee pain” individuals had significantly lower pressure pain threshold at the knee sites (medial, p = 0.03 and lateral, p < 0.01) and higher mechanical TS pain at both sites (p’s < 0.01) in the fully adjusted model. Differences between only “CMC pain” and only “knee pain” were also observed in the unadjusted model during the heat pain tolerance, mechanical TS, and pressure pain threshold at all sites with exception of the quadriceps. No significant differences were observed for heat pain thresholds across groups in either model.
Pain Group Differences in Psychological Variables
The “CMC + knee pain” group had the highest self-reported pain, disability, and emotional distress compared to all other groups (Figure 2). Specifically, the “CMC + knee pain” group had significantly higher pain intensity, disability, and stiffness per the GCPS and WOMAC questionnaires and lower outcomes during the SPPB (p < 0.01) in comparison to the only “CMC pain” group in the fully adjusted model (all p’s < 0.01) (Table 4). Similarly, the “CMC + knee pain” group was also significantly different from the only “knee pain” group in the disability portion of the GCPS questionnaire and SPPB outcomes. We also observed significant differences in number of pain sites between the only “knee pain” group and “CMC + knee pain” group, but no significant differences were observed across only “knee pain” and “CMC pain” or “CMC pain” and “CMC + knee pain” in the fully adjusted model. When comparing coping strategies, the “CMC + knee pain” group used reinterpretation more commonly than the only “CMC pain” and “knee pain” groups. Interestingly, the sole distinction in coping strategies between the “CMC pain” and “knee pain” groups, within the fully adjusted model, emerged during praying, where the “knee pain” group demonstrated higher scores. Although no comparisons were made within-groups for the coping strategies, the raw values show that the only ‘CMC pain’ and ‘CMC + knee pain’ groups had higher scores for coping self-statements, while the only ‘knee pain’ group chose praying as a coping mechanism more often.
 |
Table 4 Results of Function and Psychological Variables by Location of Primary Pain Groups (Mean ± SD) and Comparison Results |
 |
Figure 2 Results of function and psychological variables by location of primary pain groups. Error bars represent standard deviations. Black lines represent statistically significant differences between cohorts. |
Discussion
The primary finding of this secondary analysis is that individuals with “CMC + knee pain” had higher functional disability and greater psychological symptoms than individuals with “CMC pain” or “knee pain”. Both pain intensity and the overall self-perceived disability were significantly higher, or more severe, when knee OA was compounded with “CMC pain”. This finding is in agreement with previous studies that showed pain severity and the feeling of helplessness directly affect self-perceived disability48,49 as well as studies that have shown that individuals with multi-joint pain have worse self-reported function and physical performance than those with single-joint pain.28
To our knowledge, even though hand OA is commonly diagnosed in conjunction with knee OA,29,50 this is the first study to explicitly compare pain and psychological factors in “CMC pain” and “knee pain” groups. When comparing pain groups, we found significant differences in pressure pain threshold, heat pain tolerance, and mechanical temporal summation. Our results showed that the only “CMC pain” group experienced less pain during mechanical TS and had higher pressure pain threshold at the knee sites when compared to the only “knee pain” group in the fully adjusted model. However, in contrast to previous studies reporting that individuals with CMC OA experience pressure pain hyperalgesia25 in comparison to a healthy cohort, our study identified no differences between the “CMC pain” and “pain-free” groups. Remarkably, the “CMC + knee pain” group had the highest pain ratings during TS at the forearm at all temperatures in comparison to all other groups, but was only significantly different in the unadjusted model at 46 °C. These results suggest that individuals with knee pain exacerbated with CMC pain may experience hyperalgesia in the arm more frequently than individual with either just “CMC pain” or “knee pain”.
This study also provides novel insights into the psychological symptoms and functional disability experienced by individuals with hand and/or knee OA. Functional limitation scores during the SPPB of the “CMC + knee pain” group were significantly lower than those in the “CMC pain” and “knee pain” group in the fully adjusted model. These results can be related to their pain scores during the assessment, unfortunately due to missing data this type of analysis was not completed. Furthermore, coping mechanisms used in response to disability varied across groups. The “CMC + knee pain” and “CMC pain” groups demonstrated a preference for using coping statements, while the “knee pain” group dealt with the pain by praying. Interestingly, the second most common coping mechanism chosen by the “CMC pain” group, which also had the highest raw scores in comparison to all other groups, was ignoring. Given that the thumb accounts for over 50% of hand function,51 these results imply individuals with “CMC pain” are ignoring pain during a wide variety of activities of daily living, thereby highlighting the need for future work to identify effective treatments for CMC pain, so that pain is eliminated and coping is no longer necessary.
This study was a secondary analysis of existing datasets collected to understand pain characteristics in patients with knee OA. As such, there are several limitations. Because the focus of the original study was characterizing knee pain, most of the QST assessments did not include the CMC joint or the hand as a testing site. Despite this limitation, the results highlighted differences in clinical and experimental pain across individuals with only “CMC pain”, only “knee pain”, and “CMC + knee pain”. Additionally, significant differences in self-perceived pain intensity and functional limitations were identified across groups. For example, although psychological questionnaires for hand OA were not assessed (eg, AUSCAN or DASH), the higher scores in the WOMAC of the “CMC + knee pain” group and only “knee pain” group highlights the severity of disability in individuals with multi-site OA, particularly OA compounded with CMC joint pain. Another limitation was the absence of medical images confirming the presence of OA. However, given the demographics of the population and exclusion criteria (eg, presence of rheumatoid OA, fibromyalgia, lupus) and the physical examination performed, it is likely that pain in the hand was the result of OA. The self-reported number of pain sites and the fact that only “CMC pain” and “knee pain” groups included individuals with bilateral joint pain might be reflective of the participants age52 and may render our findings more representative of the broader community. Moreover, our groups were created based on their most painful joint and excluding as necessary pain at the hand or knee joints. Lastly, the study includes groups with different numbers of individuals. However, due to the large overall number of individuals studied, our analyses were powered to detect group differences that are moderate in magnitude.
Conclusion
The differences in experimental pain and psychological variables found in this study highlight the importance of studying the pain experience across OA in both large and small joints. Given the “CMC + knee pain” group had the worst psychophysical outcomes, this highlights the importance of understanding CMC OA as a compounding factor for osteoarthritic pain at other joints. Given these findings, future studies should control how hand pain affects function and well-being. The results of this study also motivate future work to specifically study individuals with only CMC OA. Quantifying their experience thoroughly (eg, assessing pain thresholds at the CMC joint) could further our understanding of hand pain phenotypes and inform treatment.53 Hand OA remains understudied despite its high prevalence.54 Thus, expanding research of small joints is critical for fully elucidating their role in modulating the experimental and clinical pain experience.
Abbreviations
CMC, carpometacarpal; OA, osteoarthritis; QST, quantitative sensory testing; TS, temporal summation; WOMAC, western Ontario and McMaster universities osteoarthritis index; GCPS, graded chronic pain scale; CSQ-R, coping strategies questionnaire-revised; LOT-R, life orientation test-revised; PANAS, positive and negative affect schedule; SPPB; short physical performance battery; SD, standard deviation.
Ethics Approval of Research on Humans
The procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000.
Acknowledgments
Funding from the National Institutes of Health (F31 AG074645, KL2 TR001429, and R37 AG033906) and from the University of Florida Graduate Student Preeminence Award is acknowledged. Funding sources were not involved in the preparation of this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. March L, Cross M, Arden N, Hawker G. Osteoarthritis: a Serious Disease, Submitted to the U. S. Food and Drug Administration. Oarsi. 2016;1–103.
2. Pereira D, Peleteiro B, Araújo J, Branco J, Santos RA, Ramos E. The effect of osteoarthritis definition on prevalence and incidence estimates: a systematic review. Osteoarthritis Cartilage. 2011;19(11):1270–1285. doi:10.1016/j.joca.2011.08.009
3. Forestier R, Francon A, Briole V, Genty C, Chevalier X, Richette P. Prevalence of generalized osteoarthritis in a population with knee osteoarthritis. Joint Bone Spine. 2011;78(3):275–278. doi:10.1016/j.jbspin.2010.09.024
4. Günther KP, Stürmer T, Sauerland S, et al. Prevalence of Generalised Osteoarthritis in Patients with Advanced Hip and Knee Osteoarthritis: the Ulm Osteoarthritis Study. Ann Rheumatic Dis. 1998;57.:717–723. doi:10.1136/ard.57.12.717
5. Vitaloni M, Botto-van Bemden A, Sciortino Contreras RM, et al. Global management of patients with knee osteoarthritis begins with quality of life assessment: a systematic review. BMC. 2019;2.
6. Iannone F, Lapadula G. The pathophysiology of osteoarthritis. Aging Clin Exp Res. 2003;15(5):364–372. doi:10.1007/BF03327357
7. Miller RE, Tran PB, Obeidat AM, et al. The Role of Peripheral Nociceptive Neurons in the Pathophysiology of Osteoarthritis Pain. Curr Osteoporosis Rep. 2015;13(5):318–326. doi:10.1007/s11914-015-0280-1
8. Eitner A, Hofmann GO, Schaible HG, Kress M, Cunha TM. Mechanisms of Osteoarthritic Pain. Studies in Humans and Experimental Models. Front Mol Neurosci. 2017;10. doi:10.3389/fnmol.2017.00349
9. Ohtori S, Orita S, Yamashita M, et al. Existence of a neuropathic pain component in patients with osteoarthritis of the knee. Yonsei Med J. 2012;53(4):801–805. doi:10.3349/YMJ.2012.53.4.801
10. French HP, Smart KM, Doyle F. Prevalence of neuropathic pain in knee or Hip osteoarthritis: a systematic review and meta-analysis. Semin Arthritis Rheum. 2017;47(1):1–8. doi:10.1016/J.SEMARTHRIT.2017.02.008
11. Villafañe JH, Valdes K, Pedersini P, Berjano P. Osteoarthritis: a call for research on central pain mechanism and personalized prevention strategies. Clin Rheumatol. 2019;38(2):583–584. doi:10.1007/s10067-018-4270-4
12. Carlesso LC, Law LF, Wang N, Nevitt M, Lewis CE, Neogi T. Association of Pain Sensitization and Conditioned Pain Modulation to Pain Patterns in Knee Osteoarthritis. Arthritis Care Res. 2021;107. doi:10.1002/acr.24437
13. Schaible HG. Mechanisms of chronic pain in osteoarthritis. Curr Rheumatol Rep. 2012;14(6):549–556. doi:10.1007/s11926-012-0279-x
14. Graven-Nielsen T, Arendt-Nielsen L. Peripheral and central sensitization in musculoskeletal pain disorders: an experimental approach. Curr Rheumatol Rep. 2002;4(4):313–321. doi:10.1007/s11926-002-0040-y
15. Steen Pettersen P, Neogi T, Magnusson K, et al. Peripheral and Central Sensitization of Pain in Individuals With Hand Osteoarthritis and Associations With Self-Reported Pain Severity. Arthritis Rheumatol Hoboken NJ. 2019;71(7):1070–1077. doi:10.1002/art.40850
16. Wylde V, Palmer S, Learmonth ID, Dieppe P. Somatosensory abnormalities in knee OA. Rheumatology. 2012;51(3):535–543. doi:10.1093/rheumatology/ker343
17. Cardoso JS, Riley JL, Glover T, et al. Experimental pain phenotyping in community-dwelling individuals with knee osteoarthritis. Pain. 2016;157(9):2104–2114. doi:10.1097/j.pain.0000000000000625
18. Frey-Law LA, Bohr NL, Sluka KA, et al. Pain sensitivity profiles in patients with advanced knee osteoarthritis. Pain. 2016;157(9):1988–1999. doi:10.1097/j.pain.0000000000000603
19. Cruz-Almeida Y, King CD, Goodin BR, et al. Psychological profiles and pain characteristics of older adults with knee osteoarthritis. Arthritis Care Res. 2013;65(11):1786–1794. doi:10.1002/acr.22070
20. Moore RL, Clifford AM, Moloney N, Doody C, Smart KM, O’Leary H. The Relationship Between Clinical and Quantitative Measures of Pain Sensitization in Knee Osteoarthritis. Clin J Pain. 2020;36(5):336–343. doi:10.1097/AJP.0000000000000798
21. Westermann A, Rönnau A-K, Krumova E. Pain-associated mild sensory deficits without hyperalgesia in chronic non-neuropathic pain. Clin J Pain. 2011;27(9):782–789. doi:10.1097/AJP.0B013E31821D8FCE
22. Villafañe JH, Silva GB, Fernandez-Carnero J. Effect of thumb joint mobilization on pressure pain threshold in elderly patients with thumb carpometacarpal osteoarthritis. J Manipulative Physiol Ther. 2012;35(2):110–120. doi:10.1016/j.jmpt.2011.12.002
23. Themelis K, Newport R. An investigation of contextual factors in the application of multisensory illusions for analgesia in hand osteoarthritis. Rheumatol Adv Pract. 2018;2(2):1–10. doi:10.1093/RAP/RKY019
24. Chiarotto A, Fernandez-de-las-Peñas C, Castaldo M, Negrini S, Villafañe JH. Widespread pressure pain hypersensitivity in elderly subjects with unilateral thumb carpometacarpal osteoarthritis. Hand. 2013;8(4):422–429. doi:10.1007/s11552-013-9537-2
25. Chiarotto A, Fernandez-de-las-Peñas C, Castaldo M, Villafañe JH. Bilateral Pressure Pain Hypersensitivity over the Hand as Potential Sign of Sensitization Mechanisms in Individuals with Thumb Carpometacarpal Osteoarthritis. Pain Med. 2013;14(10):1585–1592. doi:10.1111/pme.12179
26. Wajed J, Ejindu V, Heron C, Hermansson M, Kiely P, Sofat N. Quantitative sensory testing in painful hand osteoarthritis demonstrates features of peripheral sensitisation - PubMed. Int J Rheumatol. 2012;2012:1–8. doi:10.1155/2012/703138
27. Nelson AE, Golightly YM, Renner JB, et al. Brief Report: differences in multijoint symptomatic osteoarthritis phenotypes by race and sex: the Johnston County Osteoarthritis Project. Arthritis Rheum. 2013;65(2):373–377. doi:10.1002/art.37775
28. Guérard O, Dufort S, Forget Besnard L, Gougeon A, Carlesso L. Comparing the association of widespread pain, multi-joint pain and low back pain with measures of pain sensitization and function in people with knee osteoarthritis. Clin Rheumatol. 2020;39(3):873–879. doi:10.1007/s10067-019-04828-3
29. Badley EM, Zahid S, Wilfong JM, Perruccio AV. The relationship between body mass index and osteoarthritis for single and multi‐site osteoarthritis of the hand, Hip, or knee: findings from the CLSA. Arthritis Care Res. 2021. doi:10.1002/ACR.24729
30. Pedersini P, Negrini S, Cantero-Tellez R, Bishop MD, Villafañe JH. Pressure algometry and palpation of the upper limb peripheral nervous system in subjects with hand osteoarthritis are repeatable and suggest central changes. J Hand Ther. 2020;33(1):103–111. doi:10.1016/j.jht.2018.06.003
31. Hoogendam L, van der Oest MJW, Tsehaie J, et al. Psychological factors are more strongly associated with pain than radiographic severity in non-invasively treated first carpometacarpal osteoarthritis. Disabil Rehabil. 2021;43(13):1897–1902. doi:10.1080/09638288.2019.1685602
32. van der OMJW, Duraku LS, Andrinopoulou ER, et al. The prevalence of radiographic thumb base osteoarthritis: a meta-analysis. Osteoarthritis Cartilage. 2021;29(6):785–792. doi:10.1016/j.joca.2021.03.004
33. Perruccio AV, Badley EM, Antflek D, Power JD, Baltzer H. Frequency of multisite non-hand joint involvement in patients with thumb-base osteoarthritis, and associations with functional and patient-reported outcomes. Osteoarthr Cartil Open. 2023;5(4):100397. doi:10.1016/j.ocarto.2023.100397
34. Fowler-Brown A, Wee CC, Marcantonio E, Ngo L, Leveille S. The mediating effect of chronic pain on the relationship between obesity and physical function and disability in older adults. J Am Geriatr Soc. 2013;61(12):2079–2086. doi:10.1111/jgs.12512
35. Deshpande N, Metter EJ, Guralnik J, Bandinelli S, Ferrucci L. Predicting 3-year incident mobility disability in middle-aged and older adults using physical performance tests. Arch Phys Med Rehabil. 2013;94(5):994–997. doi:10.1016/j.apmr.2012.10.032
36. Johnson AJ, Sibille KT, Cardoso J, et al. Patterns and correlates of self‐management strategies for osteoarthritis related pain among older non‐Hispanic Black and non‐Hispanic White adults. Arthritis Care Res. 2020. doi:10.1002/ACR.24396
37. Ordonez Diaz T, Cruz-Almeida Y, Fillingim RB, Nichols JA. Comparison of Experimental Pain and Functional Impact in Individuals with Single- and Multi-site Osteoarthritis - ScienceDirect. J Pain. 2022;23:41. doi:10.1016/j.jpain.2022.03.156
38. Altman R, Asch E, Bloch D, et al. Development of criteria for the classification and reporting of osteoarthritis: classification of osteoarthritis of the knee. Arthritis Rheum. 1986;29(8):1039–1049. doi:10.1002/art.1780290816
39. Johnson AJ, Laffitte Nodarse C, Peraza JA, et al. Psychological profiles in adults with knee OA-related pain: a replication study. Ther Adv Musculoskelet Dis. 2021;13:1759720X211059614. doi:10.1177/1759720X211059614
40. Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the Hip or knee. J Rheumatol. 1988.
41. Robinson ME, Riley JL, Myers CD, et al. The coping strategies questionnaire: a large sample, item level factor analysis. Clin J Pain. 1997;13(1):43–49. doi:10.1097/00002508-199703000-00007
42. Glaesmer H, Rief W, Martin A, et al. Psychometric properties and population-based norms of the Life Orientation Test Revised (LOT-R). Br J Health Psychol. 2012;17(2):432–445. doi:10.1111/j.2044-8287.2011.02046.x
43. Rasmussen HN, Scheier MF, Greenhouse JB. Optimism and physical health: a meta-analytic review. Ann Behav Med. 2009;37(3):239–256. doi:10.1007/s12160-009-9111-x
44. Watson D, Clark LA, Tellegen A. Development and validation of brief measures of positive and negative affect: the PANAS scales. J Pers Soc Psychol. 1988;54(6):1063–1070. doi:10.1037/0022-3514.54.6.1063
45. Lee JY, Han K, Park YG, Park SH. Effects of education, income, and occupation on prevalence and symptoms of knee osteoarthritis. Sci Rep. 2021;11:13983. doi:10.1038/s41598-021-93394-3
46. O’Connor MI. Sex differences in osteoarthritis of the Hip and knee. J Am Acad Orthop Surg. 2007;15 Suppl 1:S22–S25.
47. Srikanth VK, Fryer JL, Zhai G, Winzenberg TM, Hosmer D, Jones G. A meta-analysis of sex differences prevalence, incidence and severity of osteoarthritis. Osteoarthritis Cartilage. 2005;13(9):769–781. doi:10.1016/j.joca.2005.04.014
48. Creamer P, Lethbridge-Cejku M, Hochberg MC. Factors associated with functional impairment in symptomatic knee osteoarthritis. Rheumatology. 2000;39(5):490–496. doi:10.1093/RHEUMATOLOGY/39.5.490
49. Horgas AL, Yoon SL, Nichols AL, Marsiske M. The Relationship Between Pain and Functional Disability in Black and White Older Adults. Res Nurs Health. 2008;31(4):341–354. doi:10.1002/nur.20270
50. Prieto-Alhambra D, Judge A, Javaid MK, Cooper C, Diez-Perez A, Arden NK. Incidence and risk factors for clinically diagnosed knee, Hip and hand osteoarthritis: influences of age, gender and osteoarthritis affecting other joints. Ann Rheum Dis. 2014;73(9):1659–1664. doi:10.1136/annrheumdis-2013-203355
51. Luker KR, Aguinaldo A, Kenney D, Cahill-Rowley K, Ladd AL. Functional task kinematics of the thumb carpometacarpal joint. In: Clinical Orthopaedics and Related Research. Vol. 472. New York LLC: Springer;2014:1123–1129. doi:10.1007/s11999-013-2964-0
52. Donald IP, Foy C. A longitudinal study of joint pain in older people. Rheumatology. 2004;43(10):1256–1260. doi:10.1093/rheumatology/keh298
53. Cedraschi C, Delézay S, Marty M, et al. Let’s Talk about OA Pain”: a Qualitative Analysis of the Perceptions of People Suffering from OA. Towards the Development of a Specific Pain OA-Related Questionnaire, the Osteoarthritis Symptom Inventory Scale (OASIS). PLoS One. 2013;8(11):e79988. doi:10.1371/journal.pone.0079988
54. Snyder EA, Alvarez C, Golightly YM, Renner JB, Jordan JM, Nelson AE. Incidence and Progression of Hand Osteoarthritis in a Large Community-Based Cohort: the Johnston County Osteoarthritis Project. Osteoarthritis Cartilage. 2020;28(4):446–452. doi:10.1016/j.joca.2020.02.028
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.