Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
A Scoping Review of Psychoeducational Interventions for Managing Type 2 Diabetes Mellitus in Asian Countries
Authors Setyowati R, Haroen H, Yosep I ![]() , Agustina HR
, Agustina HR ![]()
Received 17 September 2025
Accepted for publication 19 December 2025
Published 30 December 2025 Volume 2025:18 Pages 8333—8350
DOI https://doi.org/10.2147/JMDH.S568155
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
Rahayu Setyowati,1 Hartiah Haroen,2 Iyus Yosep,3 Hana Rizmadewi Agustina4
1Doctoral Program, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia; 2Department of Community Health Nursing, Faculty of Nursing, Universitas Padjadjaran, Bandung, West Java, Indonesia; 3Department of Mental Health Nursing, Faculty of Nursing, Universitas Padjadjaran, Bandung, West Java, Indonesia; 4Department of Fundamental Nursing, Faculty of Nursing, Universitas Padjadjaran, Bandung, West Java, Indonesia
Correspondence: Rahayu Setyowati, Doctoral Program, Faculty of Medicine, Universitas Padjadjaran, Bandung, West Java, Indonesia, Email [email protected]
Background: Diabetes mellitus (DM) is a chronic disease that significantly affects patients’ quality of life and mental health. Psychoeducational approaches have been recognized as an effective strategy to improve knowledge and self-care skills and to reduce psychological burden. However, scoping reviews focusing on psychoeducational interventions and their outcomes in patients with type 2 diabetes mellitus in Asian contexts remain limited.
Purpose: This scoping review aimed to identify, map, and synthesize existing evidence on psychoeducational interventions for adults with type 2 diabetes mellitus in Asian countries.
Methods: A scoping review was conducted in accordance with the Arksey and O’Malley framework and reported in accordance with PRISMA guidelines. Literature searches were conducted across CINAHL, PubMed, Scopus, and Taylor & Francis databases through July 28, 2025, complemented by manual searches in Google Scholar. Eligible studies were randomised controlled trials (RCTs) published in English that involved patients with diabetes types 2 in Asian countries. Methodological quality was appraised using the Joanna Briggs Institute (JBI) checklist, and data were synthesised through thematic analysis.
Results: There were 13 RCT articles analyzed in this review. The psychoeducational interventions identified could be classified into three main models: cognitive-behavioral and acceptance-based interventions, mindfulness and stress-reduction interventions, and educational and coaching-based interventions. The reported outcomes also clustered into three domains: psychological, behavioral/self-management, and clinical. The most consistent improvements were observed in psychological and behavioural outcomes, while clinical outcomes, such as reduced HbA1c, cortisol levels, and PAI-1, also improved.
Conclusion: Psychoeducational interventions are diverse and effective in improving psychological well-being and self-management among patients with diabetes in Asia. Culturally-based adaptation and integration into primary healthcare systems are essential to ensure sustainability and long-term effectiveness.
Keywords: Asia, diabetes mellitus, intervention, psychoeducation, quality of life
Introduction
Diabetes mellitus (DM) is a public health burden that continues to increase globally, particularly in the Asian region. Globally, the International Diabetes Federation (IDF) estimates that 451 million adults worldwide had diabetes in 2017, which is projected to increase to 852.5 million by 2050.1 More than 95% of people with diabetes have type 2 diabetes.2 In Asia, the IDF projects that the number of people with diabetes in the Southeast Asia Region will increase by 73%, reaching 185 million by 2050.3 The proportion of undiagnosed diabetes is the third highest of all Regions at 42.7%.3 Asia faces a significant and growing diabetes burden, with high prevalence rates and a trend of earlier onset and diagnosis in younger individuals compared to other regions.4,5
The increasing prevalence rate in the DM population is in line with rapid urbanization, population aging, increasing obesity, and unequal access to prevention and treatment, especially in low- to middle-income countries.6,7 Social determinants of health, such as socioeconomic status, education, physical environment, and access to care, substantially influence diabetes risk and outcomes.8,9 This trend is also exacerbated by the existing high proportion of undiagnosed cases in many Asian countries, resulting in delayed glycemic control and increased risk of complications.3 This condition indicates the need for more comprehensive diabetes management.
People with type 2 diabetes show higher levels of depression and anxiety compared to the general population.10 Depression and anxiety are related to poor glycemic control,11,12 diabetes complications,13 and lower prognosis and quality of life.14–17 Psychological distress triggers activation of the sympathetic nervous system, increased cortisol and catecholamines, which ultimately increases the risk of metabolic syndrome.18,19 Furthermore, patients who experience psychological distress tend to experience difficulties in diabetes self-care,20 so that glycemic control worsens and triggers serious complications.12 In the long term, microvascular complications (eg, retinopathy, neuropathy) and macrovascular (eg, myocardial infarction, angina pectoris, and stroke) frequently occur and have been shown to reduce health-related quality of life (HRQoL) significantly.21–24 In addition, depression and diabetes distress often accompany DM and are associated with low self-care (drug compliance, diet, physical activity, glucose monitoring) in sufferers, which in turn increases the high level of morbidity and reduces the quality of life.22,24,25
To achieve optimal disease control, patients need to understand the importance of diet and medication and be able to adapt them to their physical activity routine.23 Therefore, education is an essential component of diabetes management.26 However, formal health education is often less than optimal due to the lack of active patient participation, short consultation times, and minimal integration of psychological support.27,28 These limitations highlight the need for innovative approaches that can deliver education more effectively. Psychoeducational interventions, which integrate disease education with psychosocial support, represent one such strategy that may enhance patient engagement and improve both clinical and psychological outcomes without necessarily requiring additional consultation time. Previous reviews reported that psychoeducation-based interventions can reduce emotional distress and glycemic control.29 Psychoeducational interventions integrating disease education and self-care skills with psychological components are key strategies for improving glycemic control, care behaviors, and psychosocial outcomes.30–34
Although numerous studies report significant effects of psychoeducational interventions, their implementation in patients with diabetes mellitus is often hampered. The barriers include a lack of knowledge and skills among healthcare workers, time constraints, and minimal policy support and incentives from healthcare institutions.35,36 Furthermore, cultural factors that emphasize physical aspects over psychological ones contribute to low awareness of the importance of mental support in diabetes management.36 Other barriers arise from low health literacy and patient motivation, variations in psychoeducation delivery methods, and limited access to technology for specific groups.34,37 These barriers indicate that successful implementation of psychoeducation in diabetes requires increased capacity of health workers, policy support, and an adaptive approach to patient culture and technology.
To date, no scoping review has comprehensively identified and synthesised existing evidence on psychoeducational interventions for diabetes mellitus in Asian countries, nor has it evaluated their impact on clinical, behavioural, and psychosocial outcomes. Existing review studies conducted among Asian populations include lifestyle-tailored interventions,38 culturally based interventions in self-management,39 diabetes self-management education,40,41 dietary interventions,42 and psychoeducation for pregnant women.43 However, none specifically and systematically examine psychoeducational interventions for diabetes across Asian settings. Given Asia’s unique culture, languages, family structures, and diverse healthcare systems, there is a critical need for a rigorous review of psychoeducational interventions in this context, assessing their feasibility and effectiveness within real-world resource constraints. In addition, health expenditure related to diabetes care in Asian countries has shown a steady and significant rise over recent decades, reflecting both the growing prevalence of diabetes and the economic strain on healthcare systems.44,45 Therefore, this scoping review aimed to systematically identify, map, and synthesize psychoeducational interventions implemented for adults with type 2 diabetes mellitus in Asian countries.
Materials and Method
Study Design
This study adopted a scoping review design to map psychoeducational interventions for the management of type 2 diabetes mellitus in Asian countries. The review followed the Arksey and O’Malley framework and was reported in accordance with the PRISMA extension for scoping reviews (PRISMA-ScR).
Eligibility Criteria
Screening and selection were performed independently by three reviewers (RS, HH, and IY) using the PRISMA flow (see Figure 1). Research questions and inclusion thresholds were structured with the PICOT framework:
- Population (P): Individuals with diabetes mellitus (type 2) living in Asian countries.
- Intervention (I): Psychoeducational programs.
- Comparator (C): Usual care or standard education.
- Outcomes (O): Patient-reported and clinical outcomes related to diabetes self-management (eg, HbA1c and other glycemic indicators, diabetes knowledge, self-efficacy, medication adherence, lifestyle behaviours, diabetes distress/depression, quality of life, etc).
- Type of study (T): Randomized controlled trials (RCTs) studies.
 |
Figure 1 PRISMA Flow Diagram. Adapted from Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Creative Commons.46 |
Inclusion criteria in this study were full-text, English-language studies employing RCT designs that evaluated psychoeducational interventions for diabetes management in Asian settings. Although this review was conducted as a scoping review with the primary aim of mapping and describing the range of psychoeducational interventions, delivery formats, and outcome measures, we focused on studies with stronger internal validity. Therefore, we restricted inclusion to randomized controlled trials (RCTs), which are generally considered the most robust design for evaluating intervention effects, and synthesized their findings narratively.
Articles were excluded if the full text was unavailable, not in English, or were secondary research (eg, reviews, commentaries). No date limits were applied to maximize coverage. Full-text availability was required to enable detailed extraction of intervention components, outcome measures, and methodological characteristics, as well as to allow a comprehensive critical appraisal. Articles were classified as “full text unavailable” only when the complete manuscript could not be obtained despite attempts through institutional subscriptions, inter-library access, and/or direct contact with the corresponding authors.
Search Strategy
A literature search was carried out by three independent reviewers (RS, HH, and IY) comprehensively through six databases: CINAHL, PubMed, Scopus, and Taylor & Francis on 28 July 2025. Core search keywords combined controlled terms and keywords for diabetes, psychoeducation, and outcomes, restricted to Asian contexts. The keywords used were:
diabetes type 2[MeSH Terms]) OR (diabetes mellitus[MeSH Terms] AND psychoeducational intervention OR psychoeducation OR psycho education[MeSH Terms] OR cognitive behavior therapy[MeSH Terms] OR cognitive behavioral therapies[MeSH Terms] OR CBT AND clinical outcome OR patients outcome OR Psychologycal distress OR depression[MeSH Terms] OR anxiety[MeSH Terms] OR mental health[MeSH Terms] OR mental illness[MeSH Terms] OR quality of life[MeSH Terms] OR psychologycal well being.
Boolean operators AND/OR were used to refine and broaden retrieval across databases. The authors also performed hand searching (backward/forward citation tracking of included papers and relevant reviews) on Google Scholar to identify additional eligible studies.
Study Selection and Quality Appraisal
All records were de-duplicated in Mendeley before independent title/abstract and full-text screening against the eligibility criteria. Methodological quality was assessed by two reviewers (RS and HH) using the Joanna Briggs Institute (JBI) critical appraisal tools: 13 items for RCTs. Each item was rated Yes/No/Unclear/Not applicable; “Yes” scored 1, and other responses scored 0. Studies with a JBI score <70% were excluded. Discrepancies were discussed, and a consensus was reached among all authors. In this study, no unresolved disagreements remained.
Data Extraction and Synthesis
Data were extracted by two reviewers (RS and HRA) into standardised tables capturing: author/year, country, design, sample size, participant characteristics, intervention model, comparator, outcomes, and main findings, and rechecked by HH and IY. For transparency and comparability, extracted information was organized into four summary tables: Table 1 (JBI score of included studies), Table 2 (Study Characteristics such as study, country, design, participants, measures, intervention, and control, Table 3 (Patient Characteristics such as mean age, education, female, HbA1c, and comorbidity, and Table 4 (Intervention Characteristics include intervention, method, content, follow-up and frequency, and outcome.
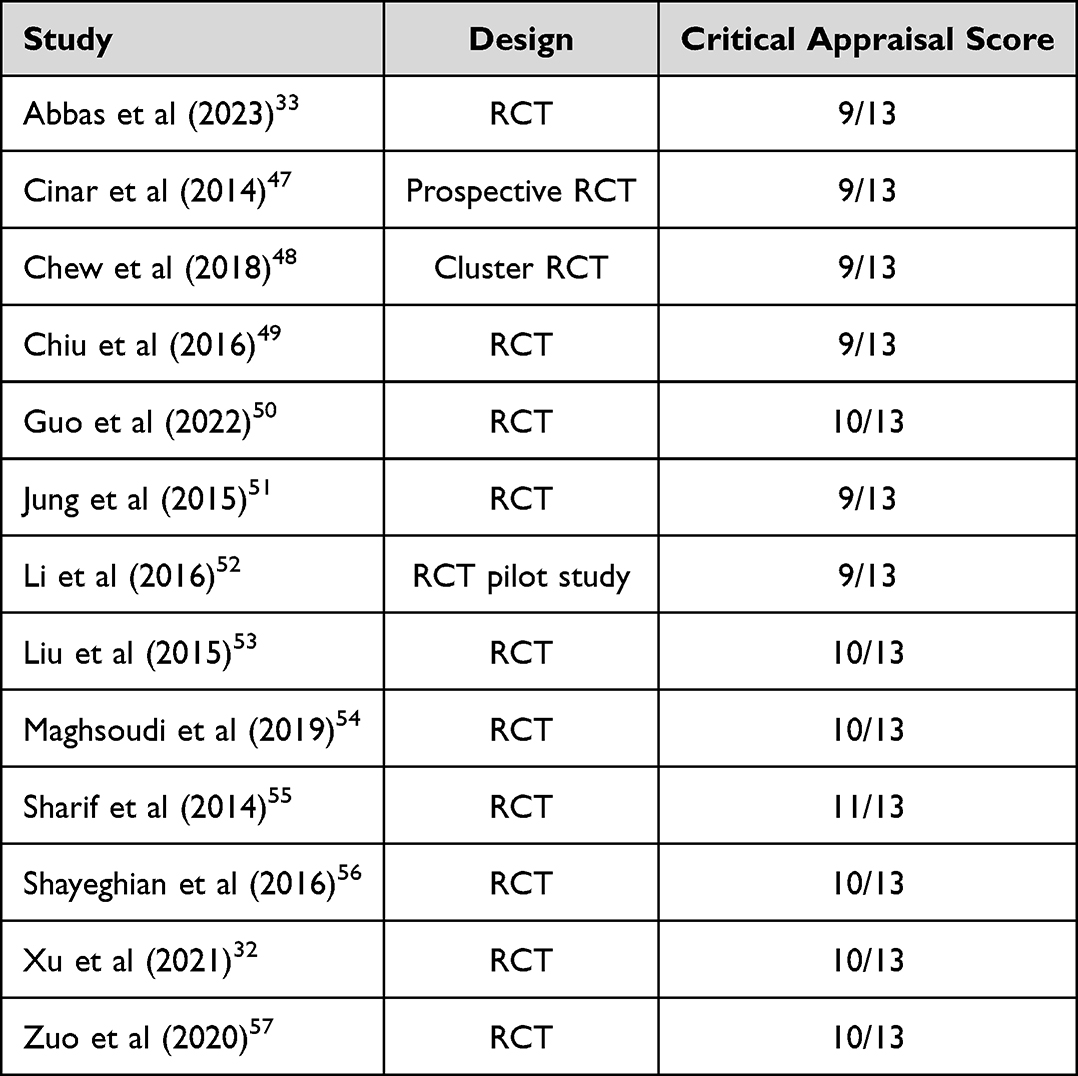 |
Table 1 Critical Appraisal Results |
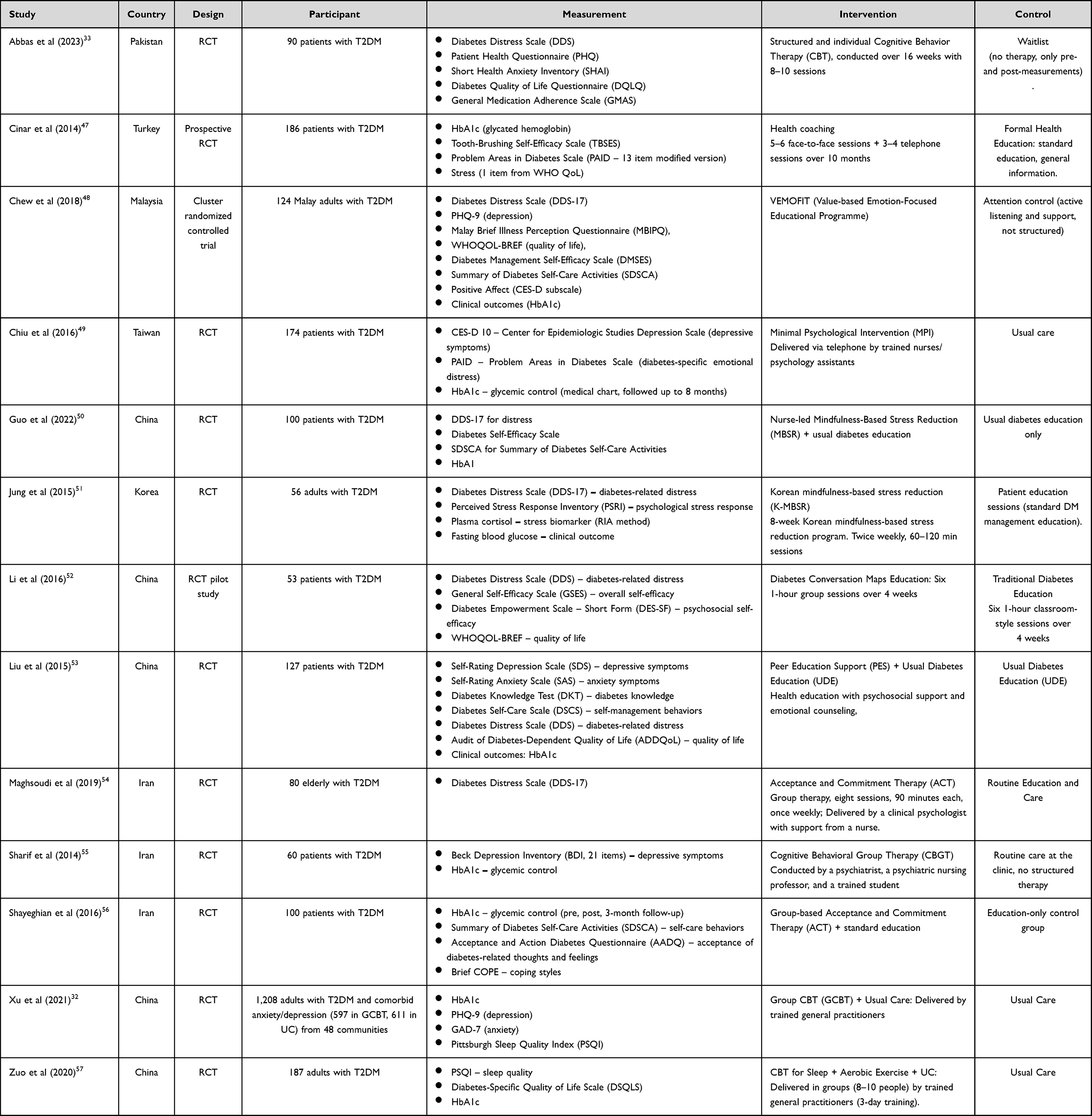 |
Table 2 Characteristic of Studies |
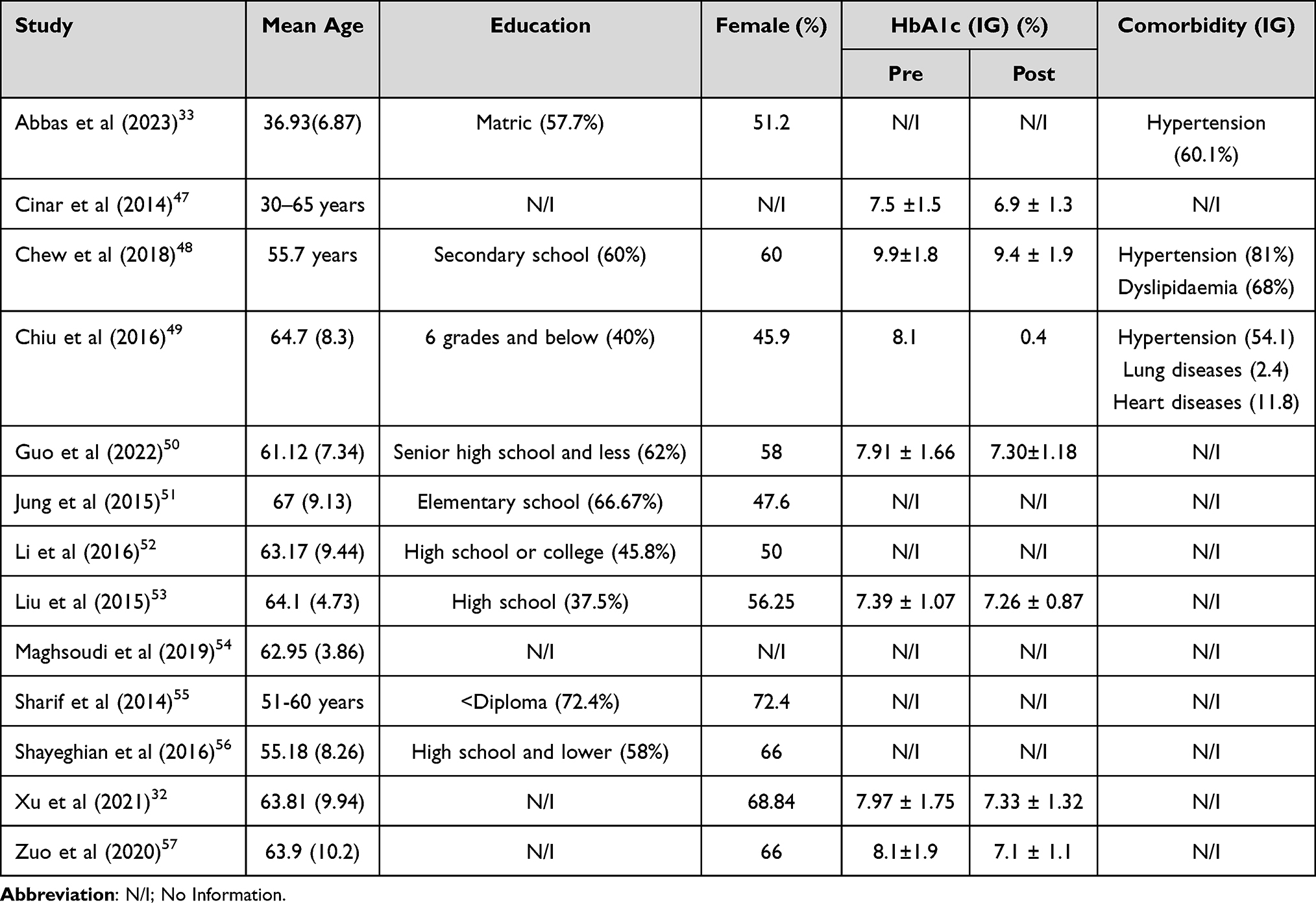 |
Table 3 Patient Characteristics of the Included Studies |
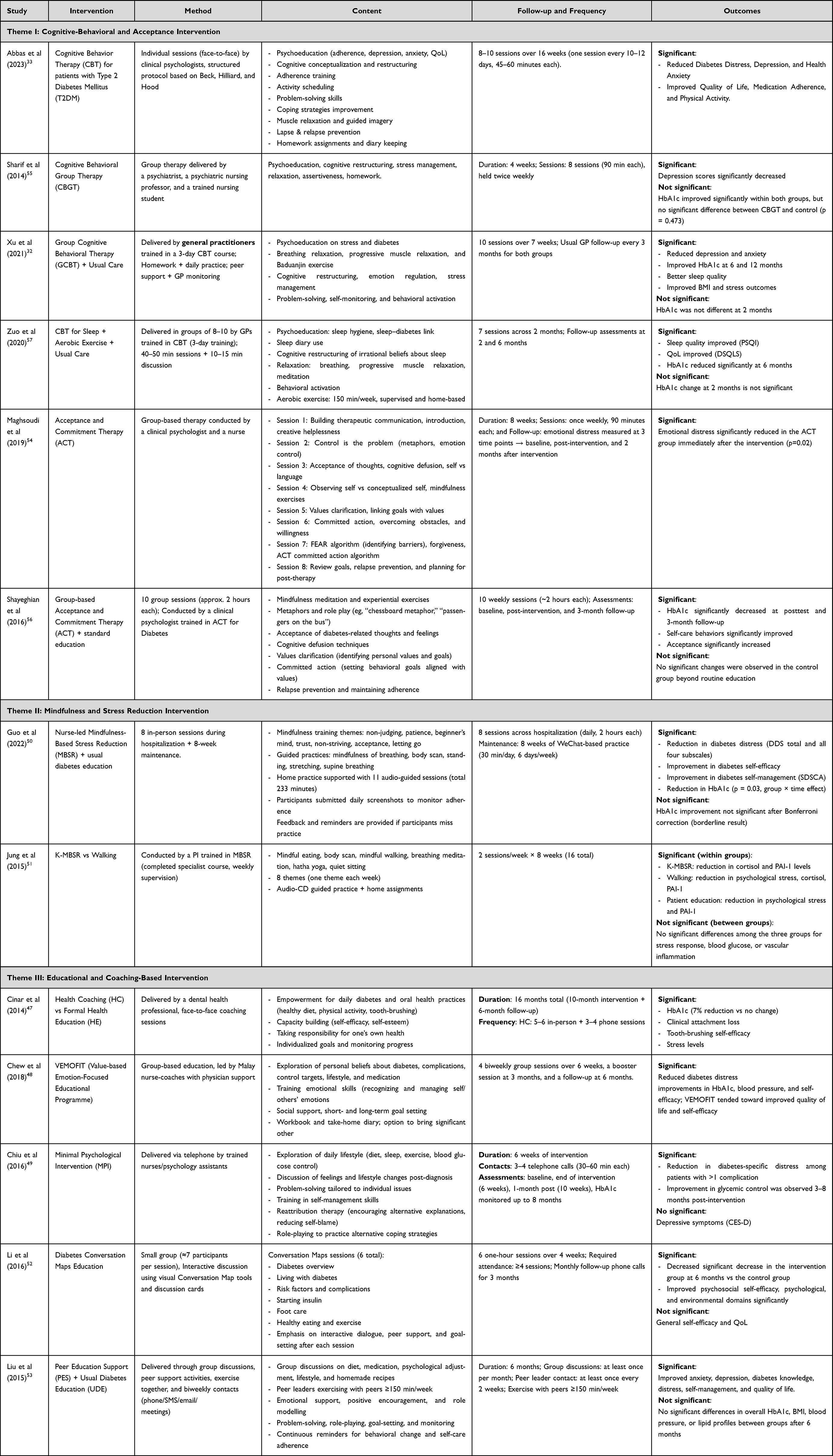 |
Table 4 Characteristic of Intervention, Content, and Outcomes |
All extracted data were verified in a final cross-check to minimize errors prior to synthesis. The analytic procedure commenced with the systematic organization and tabular display of extracted data by study. Each finding was then examined and explicated in depth, strictly aligned with the extracted variables. To safeguard accuracy and mitigate extraction error, the authors conducted a final audit of all included studies. Given heterogeneity in intervention models and outcomes, the authors undertook a thematic, exploratory narrative synthesis rather than meta-analysis.
Results
Study Selection
The initial database search identified 1,321 records (PubMed: 298, Scopus: 489, CINAHL: 234, and Google Scholar: 300). An additional four records were obtained through hand searching. After removing 122 duplicates, a total of 1,199 records were screened based on title and abstract. Of these, 1,170 records were excluded for failing to meet the inclusion criteria. Subsequently, 29 full-text articles were retrieved for eligibility assessment, of which 13 were unavailable in full text. Sixteen studies underwent full-text review, of which seven were excluded due to factors such as non-Asian context (n=4), inappropriate study design (n=1), heterogeneous samples (n=1), and interventions that did not include psychoeducation (n=1). The hand-searched studies (n=4) all met eligibility criteria. In total, 13 studies were included in this review, comprising nine from database searches and four from hand searching.
Critical Appraisal Results
The critical appraisal using the JBI checklist demonstrated that the majority of studies achieved relatively high methodological quality, with scores ranging from 9/13 to 11/13 (see Table 1). This indicates that most trials fulfilled the key criteria for randomized controlled trials, although some limitations prevented them from reaching the maximum score. Meanwhile, the remaining studies generally scored between 9 and 10 out of 13, which still represents good quality but suggests a minor risk of bias, particularly in aspects related to blinding. This challenge is inherently difficult to achieve in psychoeducational interventions. Overall, the appraisal results indicate that the included studies are methodologically robust and can be considered reliable.
Characteristics of Studies
In this review, the majority of studies analyzed were RCTs conducted in several Asian countries, focusing on psychoeducational and psychosocial interventions for patients with type 2 diabetes mellitus (T2DM) (see Table 2). Most of the studies identified in this review originated from China,32,50,52,53,57 with a total of six studies evaluating various forms of psychoeducational interventions in patients with type 2 diabetes mellitus. In addition, Iran (n=3) was in second place with three studies,54–56 Pakistan, Turkey, Malaysia, Taiwan, and Korea each contributed only one study. In general, these studies recruited adult and elderly patients with sample sizes ranging from 53 participants in the pilot study to over 1,200 in the community-scale trial.32,52 This variation in sample sizes demonstrates efforts to assess the effectiveness of interventions not only on a small clinical scale, but also in a broader community setting.
The measurement instruments used are varied, reflecting the research’s multidimensional focus on clinical, psychological, and behavioral aspects of self-care. Most studies measure diabetes distress using the Diabetes Distress Scale (DDS). At the same time, symptoms of depression and anxiety are assessed using standard instruments such as the PHQ-9, CES-D, SDS, and GAD-7.32,33,49,53 In addition, clinical indicators, such as HbA1c levels, are the primary measures of glycemic control.47,56,58 Some studies also added instruments for quality of life,48,52 self-efficacy,50,52 self-care,53,56 and sleep aspects using the Pittsburgh Sleep Quality Index (PSQI).32,57
Characteristics of Participants
The characteristics of the patients included in the study showed a wide age range (see Table 3), from a mean of 36.9 years in Pakistan33 to 67 years in Korea.51 Most studies involved middle-aged and elderly participants, reflecting the highest burden of diabetes in these age groups.32,48,49
In terms of education and gender, the majority of patients have a lower secondary education background, with a large proportion only completing elementary to high school.49–51 A small proportion of studies involved participants with higher education, such as high school or college graduates.52 Meanwhile, the proportion of women tends to be higher, ranging from 45.9% to 72.4%, with some studies reporting a predominance of female participants.32,56
The mean HbA1c levels in the intervention group ranged from around 7.3% to almost 10%, indicating that the study participants had varying glycemic control, from relatively well controlled to poor.48,53,57 The most frequently reported comorbidity was hypertension, followed by dyslipidemia, heart disease, lung disease, and other chronic conditions, indicating a high burden of multimorbidity in the diabetes population.33,48,49
Characteristics of Intervention
The analysis of intervention characteristics revealed considerable variation in both format and delivery across the included studies (see Table 4). Although the interventions were diverse, they could be systematically grouped into three major themes based on their theoretical foundation, delivery method, and educational content. The first theme encompasses cognitive-behavioural and acceptance-based interventions, which focus on cognitive restructuring, emotional regulation, and value-based behavioural change. The second theme highlights mindfulness and stress-reduction intervention, emphasizing awareness, relaxation, and stress management. Finally, the third theme captures educational- and coaching-based interventions that integrate health education, counseling, peer support, and coaching strategies. These three themes provide a structured framework for understanding how psychoeducational interventions have been designed and implemented in Asian settings.
Theme I: Cognitive-Behavioral and Acceptance Intervention
Cognitive-behavioral and acceptance-based interventions were the most dominant categories in this study. Cognitive Behavioural Therapy (CBT), both in individual and group formats, is widely used to improve emotional regulation, reduce distress, and enhance self-management in patients with diabetes.
Cognitive and acceptance-based interventions are generally delivered with structured modules and a consistent schedule. Abbas et al (2023) conducted 16 weeks of individual CBT (8–10 sessions, 45–60 minutes), consisting of psychoeducation on depression, anxiety, and quality of life, as well as skills training such as cognitive restructuring, problem-solving, scheduled activities, and relaxation.33 Sharif et al (2014) provided group CBT over 8 sessions (2 times per week, 90 minutes) that included psychoeducation, cognitive restructuring, stress management, relaxation exercises, and homework.55 In China, Xu et al (2021) developed a group CBT guided by trained general practitioners, consisting of 10 sessions over 7 weeks, encompassing stress and diabetes psychoeducation, breathing relaxation, progressive muscle relaxation, Baduanjin exercises, and cognitive restructuring, plus routine monitoring every 3 months.32 Meanwhile, Zuo et al (2020) adapted CBT for sleep problems through 7 group sessions (40–50 minutes plus a short discussion) with materials on sleep hygiene, cognitive restructuring related to sleep, use of a sleep diary, relaxation exercises, and 150 minutes of aerobic exercise per week.57
Meanwhile, Acceptance and Commitment Therapy (ACT)-based interventions focus more on accepting diabetes, mindfulness, clarifying life values, and committing to behavioral change. Maghsoudi et al (2019) conducted 8 group ACT sessions (90 minutes each week) that included an introduction to ACT, mindfulness exercises, cognitive defusion, values clarification, and relapse prevention.54 Shayeghian et al (2016) presented 10 group ACT sessions (2 hours per week) led by trained psychologists, including meditation, role-play, metaphors, acceptance of diabetes-related thoughts, and values-based action planning.56
Theme II: Mindfulness and Stress Reduction Intervention
Mindfulness-based programs typically integrate mindfulness exercises, meditation, and gentle yoga into a psychoeducational curriculum. Guo et al (2022) implemented Nurse-led Mindfulness-Based Stress Reduction for 8 intensive sessions during hospitalization, followed by an 8-week WeChat-based maintenance phase.50 The material includes mindfulness of breathing, body scans, mindful stretching, and exercises to accept thoughts without judgment. Participants also engage in independent practice for 30 minutes per day, six days a week, with monitoring through the submission of daily practice logs.50 Then, Jung et al (2015) adapted the Korean version of MBSR (K-MBSR) with an emphasis on mindful eating, body scan, mindful walking, breathing, hatha yoga, and silent meditation. The intervention consisted of 16 sessions (2 per week for 8 weeks), guided by trained facilitators, and included audio CDs and homework.51 With this structure, patients are taught to become more aware of the relationship between stress, emotions, and diabetes management through consistent, repetitive practice.
Theme III: Educational and Coaching-Based Intervention
Interventions in this theme centre on health education, coaching, and social support, using a variety of methods, from individual counselling to educational groups to peer support. Cinar et al (2014) implemented health coaching through 5–6 face-to-face sessions plus 3–4 telephone sessions over 10 months, accompanied by a 6-month follow-up. The coaching material focuses on patient empowerment in diet, physical activity, oral health, and self-health responsibility.47 Chew et al (2018) implemented the VEMOFIT program as 4 group sessions (every 2 weeks for 6 weeks) led by nurses, with support from doctors.48 The content emphasizes exploring patients’ beliefs about diabetes, emotional skills, social support, and setting short- and long-term goals. The program includes a workbook, diary, booster session at month-3, and follow-up at month-6.48
Chiu et al (2016) used Minimal Psychological Intervention (MPI) through 3–4 telephone calls lasting 30–60 minutes over 6 weeks.49 The content includes exploration of daily lifestyle, discussion of feelings after diagnosis, problem solving, self-management exercises, and reattribution therapy.49 In addition, Li et al (2016) developed Diabetes Conversation Maps Education, comprising 6 group sessions (1 hour each week for 4 weeks), based on visual tools and interactive discussions. Participants were invited to engage in a dialogue about diabetes, insulin, the risk of complications, foot care, diet, and physical activity, with monthly telephone follow-ups for 3 months.52 Liu et al (2015) emphasized Peer Education Support (PES) with group discussions, joint activities such as sports ≥150 minutes per week, role-playing, goal-setting, and regular communication via SMS/telephone.53 This intervention lasted 6 months, with meetings at least once a month and contact with a peer leader every 2 weeks.
Study Outcomes
The outcomes reported across the included studies can be broadly categorised into three domains: psychological, behavioural and self-management, and clinical and functional.
Theme I: Psychological Outcomes
Psychological outcomes were the most frequently assessed and demonstrated consistent benefits across different psychoeducational approaches. Significant reductions in diabetes-related distress were observed in several trials.33,48–50,53 Improvements in depression and anxiety symptoms were reported in multiple studies,32,33,55 while broader reductions in emotional distress, stress responses, and health anxiety were also documented.33,54 Furthermore, acceptance of illness improved significantly following acceptance-based interventions.56 Importantly, several studies also reported enhancements in quality of life (QoL) as part of the psychological outcomes.32,33,48,53,57 Collectively, these findings emphasize the strong role of psychoeducational interventions in improving psychological well-being among individuals with diabetes.
Theme II: Behavioral and Self-Management Outcomes
Behavioral and self-management outcomes formed the second domain, highlighting changes in self-care behaviors and daily disease management. Interventions consistently led to improvements in self-efficacy and diabetes self-care, as reported across multiple trials.33,48,50,52,56 Among group and peer-based interventions, patients also showed enhanced diabetes knowledge and adherence, which facilitated better disease management in everyday life.32,53 These results suggest that psychoeducation not only improves psychological functioning but also strengthens patients’ confidence and skills for long-term diabetes management.
Theme III: Clinical and Functional Outcomes
Clinical outcomes were frequently evaluated using objective biomedical indicators. Glycemic control (HbA1c) was the most commonly assessed parameter, with significant improvements reported in several studies, although results were not universally consistent.32,47–49,56,57 Stress-related biomarkers, such as cortisol and PAI-1, were also reduced in one trial,51 while oral health outcomes improved in another.47 Beyond these, some interventions demonstrated additional benefits such as better sleep quality and physiological resilience.32,57 These findings suggest that psychoeducational interventions may contribute not only to psychosocial health but also to tangible biomedical improvements.
Discussion
This review aims to identify and synthesize psychoeducational interventions in the management of diabetes mellitus in Asia. From the results of the literature search, 13 RCTs were successfully included. These interventions can be grouped into three main models: (1) cognitive-behavioral and acceptance interventions, (2) mindfulness and stress reduction interventions, and (3) educational and coaching-based interventions. The outcomes achieved vary, but in general can be grouped into three major domains: psychological (diabetes distress, depression, anxiety, acceptance, quality of life), behavioral (self-care, self-efficacy, adherence, knowledge), and clinical (HbA1c, BMI, stress biomarkers).
Overall, the results of this review show that psychological outcomes are the domain that most consistently shows improvement, confirming the relevance of psychoeducation as a primary intervention strategy to reduce the emotional burden of diabetes patients. Behavioral and clinical outcomes also show positive results, but with greater variation. Differences likely influence this in intervention intensity, facilitator competency, and the extent to which the program is adapted to the local cultural context. These findings align with global studies showing that psychoeducational interventions often have a faster impact on behavioural and psychosocial outcomes than on clinical indicators.26,29,59
CBT and ACT-based interventions are the most widely studied models, with high consistency in improving psychological outcomes. CBT is effective because it focuses on cognitive restructuring and emotion regulation skills, which directly reduce distress and increase adherence.33,55 ACT emphasises acceptance of chronic conditions and a commitment to the value of life, both of which are relevant in the context of diabetes requiring long-term care.54,56 The theoretical justification is that psychological burdens such as depression and distress often inhibit self-care behaviors, so interventions that address cognitive-emotional barriers may produce indirect effects on glycemic control.54,56 However, the limitations of this model include the need for trained personnel (psychologists/psychiatrists) and the high intensity of sessions, which may make it less practical for primary care settings with limited resources.54,56
Mindfulness-based interventions, although fewer in number, are unique in that they focus on mindfulness and physiological stress regulation.50,51 Guo et al (2022) showed that nurse-led MBSR with digital support reduced diabetes distress and increased self-efficacy.50 Mindfulness increases self-regulation, decreases physiological activation of stress (cortisol), and improves perception of illness.51 This model is easier to implement in the community because it does not always require specialist staff, but can be trained to nurses or facilitators or health workers.60–62 The challenge is maintaining patient self-practice consistency, which often decreases over time.60–62 Compared to CBT/ACT, mindfulness may be technically simpler, but its effects tend to be more optimal and depend on adherence to practice.63,64
Education and coaching models are the most varied and easily adaptable across cultures. Interventions such as health coaching,47 VEMOFIT,48 Conversation Maps,52 and peer support53 emphasizes increased knowledge, self-management skills, and social support. The outcomes achieved varied: some studies reported clinical improvements (HbA1c, blood pressure), while others focused more on psychological and behavioral outcomes. Rationally, this model works through a patient empowerment mechanism. When patients understand their disease, receive emotional support, and engage in group settings, their motivation and self-efficacy increase, ultimately influencing self-care behaviors.58 The advantage of this model is its scalability, which can be implemented in primary care at a relatively low cost, using nurses, peer leaders, or community educators. However, its clinical effectiveness tends to be more variable than that of CBT or ACT, as it depends on the intensity of implementation and the level of patient involvement.
When comparing models, CBT/ACT has the most substantial evidence for psychological outcomes; mindfulness offers a more straightforward yet more effective approach to stress regulation; and education and coaching excel in affordability, sustainability, and cultural adaptability.50 In the Asian context, education- and coaching-based models have the potential to be more widely adopted due to their alignment with primary care capacity and the needs of large populations. However, their clinical outcomes are less consistent. Conversely, CBT/ACT is more appropriate for patients with high distress or significant psychological problems. Therefore, the choice of intervention model should be tailored to the patient’s profile, clinical goals, and available resources.
Although most psychoeducational interventions show positive results, some studies report insignificant outcomes, particularly in clinical settings. For example, Chiu et al (2016) found that while diabetes distress was reduced, depressive symptoms did not show significant improvement.49 Liu et al (2015) also reported that HbA1c, blood pressure, body mass index, and lipid profile were not significantly different between the intervention and control groups, although knowledge and quality of life increased.53 Similar findings were reported by Sharif et al (2014), where a decrease in HbA1c occurred in both groups but did not differ significantly between groups.55 Even in a mindfulness study in Korea, Jung et al (2015) found no differences between groups for stress response, blood glucose levels, and vascular inflammation.51 These results indicate that although psychoeducation has a positive impact on psychological and behavioral dimensions, the effects on clinical indicators tend to be more variable and may be influenced by the duration of the intervention, sample size, patient baseline, and ongoing follow-up.
In general, the most widely used and proven effective content includes: psychoeducation about diabetes and its complications, cognitive restructuring, relaxation techniques (breathing, progressive, mindfulness), clarification of life values, problem solving, goal setting, social support, and relapse prevention strategies.33,50,52,57 Tools such as workbooks, diaries, interactive discussions, and traditional physical exercises (Tai Chi, Ba Duan Jin) are widely used. This confirms that the success of psychoeducation lies not only in the intervention’s format, but also in the combination of knowledge transfer, strengthening psychological skills, and social empowerment.
The psychoeducational interventions identified in this review share many similarities with those implemented in non-Asian settings. Cognitive–behavioral and acceptance-based approaches, mindfulness-based stress reduction, and structured educational or coaching programs have all been widely described in Western populations, targeting standard mechanisms such as maladaptive cognitions, emotional regulation, self-efficacy, and health-related behavior change. However, several features of the Asian trials reflect culturally specific adaptations. Many interventions explicitly integrated local cultural and religious values, relied on group-based formats that capitalize on peer and family support, and were delivered by nurses or general practitioners within resource-constrained primary care systems. These characteristics suggest that, while the theoretical foundations of psychoeducational interventions are broadly comparable across regions, cultural tailoring in Asian countries may enhance acceptability, engagement, and feasibility without changing the core psychological mechanisms targeted.
Several barriers to implementing psychoeducation still need to be addressed. The main challenge is maintaining long-term patient engagement, particularly with high-frequency interventions or self-paced practice that requires discipline.50,53 In addition, limited trained personnel, competing health service priorities, and uneven digital infrastructure are broad-scale obstacles.65–68 To address this, integrating psychoeducation into routine diabetes services, training healthcare workers such as nurses and community workers, utilizing digital platforms, and adapting content to suit local culture and language can be effective strategies to increase the sustainability and impact of interventions.69–71
Strengths and Limitations
This review is among the first to comprehensively map psychoeducational interventions for diabetes management specifically within Asian countries. The study applied rigorous methodology guided by the Cochrane Handbook and reported in accordance with PRISMA standards, ensuring transparency and reproducibility. A structured eligibility framework (PICOT) was used, and methodological quality was appraised with the Joanna Briggs Institute (JBI) checklist, strengthening the reliability of the included evidence. The review also captured a broad spectrum of outcomes, psychological, behavioural, and clinical, providing a holistic understanding of intervention effects. Moreover, categorising interventions into three distinct models (cognitive-behavioural/acceptance, mindfulness or stress reduction, and educational/coaching) provides a practical framework for clinicians, researchers, and policymakers to design and implement culturally tailored programs.
Despite the strengths, several limitations must be acknowledged. First, the review included only randomised controlled trials published in English, potentially excluding relevant studies in local Asian languages and introducing language bias. Second, the heterogeneity of interventions, outcomes, and follow-up durations precluded meta-analysis, limiting the ability to draw pooled quantitative conclusions. Third, most included studies had relatively short follow-up periods, which constrained understanding of the long-term sustainability of psychoeducational benefits. Fourth, many interventions were conducted in controlled research settings, raising concerns about generalizability to real-world clinical practice, where resources and training may be limited.
Conclusion
This review demonstrates that psychoeducational interventions play a crucial role in the management of type 2 diabetes mellitus in Asian settings. All included studies were conducted among patients with type 2 diabetes, and three major models were identified: cognitive-behavioral and acceptance-based approaches, mindfulness and stress-reduction programs, and educational or coaching-based strategies. Across these studies, outcomes consistently indicated improvements in psychological well-being and self-management behaviours, whereas clinical outcomes, such as glycemic control, showed mixed results. These findings suggest that psychoeducation is highly effective in addressing the psychosocial and behavioral dimensions of type 2 diabetes care, although its impact on biomedical outcomes is more variable.
Although the current evidence is limited to type 2 diabetes, the psychological and behavioral mechanisms targeted by these interventions (eg, coping skills, emotional regulation, and self-management competencies) are also relevant to other types of diabetes. Future research should therefore not only include long-term evaluations and comparative effectiveness studies within type 2 diabetes, but also rigorously test psychoeducational interventions in other diabetes populations (such as type 1 diabetes and gestational diabetes) and in diverse age groups. In addition, greater use of digital and hybrid delivery models, along with evaluations of cost-effectiveness and implementation strategies, is needed to support broader integration of psychoeducation into routine diabetes care.
Acknowledgments
All authors thank Universitas Padjadjaran, Bandung, West Java, Indonesia, for facilitating the database for this study.
Disclosure
The authors declare that they have no conflicts of interest related to this study. There are no financial, personal, or professional relationships that could have influenced the design, conduct, analysis, or reporting of this review.
References
1. International Diabetes Federation. Facts & figures of Diabetes Melitus. 2025 Available from: https://idf.org/about-diabetes/diabetes-facts-figures/.
2. World Health Organization [WHO]. Diabetes. 2024.
3. International Diabetes Federation. Diabetes regional report 2000 — 2050 [Internet]. 2025. Available from: https://diabetesatlas.org/data-by-location/region/south-east-asia/.
4. Shahid S, Ajeel AA, Marsool AD, et al. Trends and regional disparities in the diabetes burden across Asia, 1990–2021: insights from the global burden of disease study. Diabetes Epidemiol Manag. 2025;19–20:100287. doi:10.1016/j.deman.2025.100287
5. Wang R, Lip GYH, Liu Y, et al. Disease burden of type 2 diabetes among young adults in asia: an analysis from the global burden of disease study 2021. J Diabetes Res. 2025;2025:5521613. doi:10.1155/jdr/5521613
6. Ong KL, Stafford LK, McLaughlin SA, et al. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the global burden of disease study 2021. Lancet. 2023;402(10397):203–234.
7. Alinaghian SA, Hamidzadeh S, Badrizadeh A, et al. Burden of type 2 diabetes and its relationship with human development index in Asian countries: global Burden of Disease Study in 2019. BMC Public Health. 2025;25(1).
8. Sung K, Lee SH. Social determinants of health and type 2 diabetes in Asia. J Diabetes Investig. 2025;16(6):971–983. doi:10.1111/jdi.70024
9. Hill-Briggs F, Adler NE, Berkowitz SA, et al. Social Determinants of Health and Diabetes: A Scientific Review. Vol. 44. Diabetes care. United States; 2020:258–279
10. Huang CJ, Chiu HC, Lee MH, Wang SY. Prevalence and incidence of anxiety disorders in diabetic patients: a national population-based cohort study. Gen Hosp Psychiatry. 2011;33(1):8–15. doi:10.1016/j.genhosppsych.2010.10.008
11. Bellomo R. Acute glycemic control in diabetics. how sweet is optimal? pro: sweeter is better in diabetes. J Intensive Care. 2018;6(1):71. doi:10.1186/s40560-018-0336-2
12. Bin Rakhis SAS, AlDuwayhis NM, Aleid N, AlBarrak AN, Aloraini AA. Glycemic control for type 2 diabetes mellitus patients: a systematic review. Cureus. 2022;14(6):e26180.
13. Farmaki P, Damaskos C, Garmpis N, Garmpi A, Savvanis S, Diamantis E. Complications of the type 2 diabetes mellitus. Curr Cardiol Rev. 2020;16(4):249–251. doi:10.2174/1573403X1604201229115531
14. Wicaksana A, Hertanti NS. Concept analysis of diabetes-related quality of life. Health Qual Life Outcomes. 2025;23. doi:10.1186/s12955-025-02354-2
15. Jing X, Chen J, Dong Y, et al. Related factors of quality of life of type 2 diabetes patients: a systematic review and meta-analysis. Health Qual Life Outcomes. 2018;16. doi:10.1186/s12955-018-1021-9
16. Mróz M, Sadowska D, Zarychta M, Iwanowicz-Palus G, Kretowski A, Cybulski M. Assessment of the quality of life of patients with diabetes and prediabetes in poland: a cross-sectional study. J Clin Med. 2025;14.
17. Gebremedhin T, Workicho A, Angaw D. Health-related quality of life and its associated factors among adult patients with type II diabetes attending Mizan Tepi University Teaching Hospital, Southwest Ethiopia. BMJ Open Diabetes Res Care. 2019;7:e000577. doi:10.1136/bmjdrc-2018-000577
18. Lamounier-Zepter V, Ehrhart-Bornstein M, Bornstein SR. Metabolic syndrome and the endocrine stress system. Horm Metab Res = Horm Und Stoffwechselforsch = Horm Metab. 2006;38(7):437–441. doi:10.1055/s-2006-947837
19. Rosmond R. Role of stress in the pathogenesis of the metabolic syndrome. Psychoneuroendocrinology. 2005;30(1):1–10. doi:10.1016/j.psyneuen.2004.05.007
20. Das-Munshi J, Stewart R, Ismail K, Bebbington PE, Jenkins R, Prince MJ. Diabetes, common mental disorders, and disability: findings from the UK National Psychiatric Morbidity Survey. Psychosom Med. 2007;69(6):543–550. doi:10.1097/PSY.0b013e3180cc3062
21. Akinci F, Yildirim A, Gözü H, Sargin H, Orbay E, Sargin M. Assessment of health-related quality of life (HRQoL) of patients with type 2 diabetes in Turkey. Diabet Res Clin Pract. 2008;79(1):117–123. doi:10.1016/j.diabres.2007.07.003
22. Kordi Z, Khosravi A, Fotouhi A. Depression and self-care in diabetes; adjustment for misclassification bias: application of predictive weighting method. BMC Public Health. 2023;23(1):2540. doi:10.1186/s12889-023-17412-x
23. Huang JP, Chen HH, Yeh ML. A comparison of diabetes learning with and without interactive multimedia to improve knowledge, control, and self-care among people with diabetes in Taiwan. Public Health Nurs. 2009;26(4):317–328. doi:10.1111/j.1525-1446.2009.00786.x
24. Emad S, Elawad S, Elawad SOM, et al. Prevalence of depression among diabetic patients and its relationship to diabetes self-care activities, disease profile, and social factors in Khartoum State, Sudan: a cross-sectional study. Medicine. 2025;104(19):e42350. doi:10.1097/MD.0000000000042350
25. Al-Ozairi A, Taghadom E, Irshad M, Depression A-OEAB. Diabetes Self-care activity and glycemic control in an Arab population with type 2 diabetes. Diabetes Metab Syndr Obes. 2023;16:321–329. doi:10.2147/DMSO.S377166
26. Didarloo A, Shojaeizadeh D, Alizadeh M. Impact of educational intervention based on interactive approaches on beliefs, behavior, hemoglobin a1c, and quality of life in diabetic women. Int J Prev Med. 2016;2016.
27. Schäfer I, Pawels M, Küver C, et al. Strategies for improving participation in diabetes education. A qualitative study. PLoS One. 2014;9(4):e95035. doi:10.1371/journal.pone.0095035
28. Strine TW, Okoro CA, Chapman DP, Beckles GLA, Balluz L, Mokdad AH. The impact of formal diabetes education on the preventive health practices and behaviors of persons with type 2 diabetes. Prev Med. 2005;41(1):79–84. doi:10.1016/j.ypmed.2004.10.009
29. Perrin N, Bodicoat DH, Davies MJ, Robertson N, Snoek FJ, Khunti K. Effectiveness of psychoeducational interventions for the treatment of diabetes-specific emotional distress and glycaemic control in people with type 2 diabetes: a systematic review and meta-analysis. Prim Care Diabetes. 2019;13(6):556–567. doi:10.1016/j.pcd.2019.04.001
30. Supriyanto M, Miadi AAA, Fadilah N. The effect of psychoeducation with a health coaching method on HbA1c levels among patients with type 2 diabetes mellitus. Healthc Low-Resource Settings. 2024;12(s1).
31. Yuniartika W, Dwidiyanti M, Mu’in M. Reducing depression level of diabetes mellitus patient by psychoeducation by means of poster. Int J Res Med Sci. 2016;4(8):3348–3353. doi:10.18203/2320-6012.ijrms20162292
32. Xu C, Dong Z, Zhang P, et al. Effect of group cognitive behavioural therapy on psychological stress and blood glucose in people with type 2 diabetes mellitus: a community-based cluster randomized controlled trial in China. Diabet Med. 2021;38(2):1–15. doi:10.1111/dme.14491
33. Abbas Q, Latif S, Ayaz Habib H, et al. Cognitive behavior therapy for diabetes distress, depression, health anxiety, quality of life and treatment adherence among patients with type-II diabetes mellitus: a randomized control trial. BMC Psychiatry. 2023;23(1):86. doi:10.1186/s12888-023-04546-w
34. Mahmoud SS, El MMH, Mahfouz MS, et al. Effects of a psychoeducational program on hemoglobin a1c level and health-related quality of life in patients with type 2 diabetes mellitus, Jazan, Saudi Arabia. Biomed Res Int. 2018;2018:6915467. doi:10.1155/2018/6915467
35. Chapman A, Yang H, Thomas S, Searle K, Browning C. Barriers and enablers to the delivery of psychological care in the management of patients with type 2 diabetes mellitus in China: a qualitative study using the theoretical domains framework. BMC Health Serv Res. 2016;16. doi:10.1186/s12913-016-1358-x
36. Paduch A, Kuske S, Schiereck T, et al. Psychosocial barriers to healthcare use among individuals with diabetes mellitus: a systematic review. Prim Care Diabetes. 2017;11(6):495–514. doi:10.1016/j.pcd.2017.07.009
37. Berking M, Lehr D, Ebert DD, et al. Efficacy and cost-effectiveness of a web-based intervention with mobile phone support to treat depressive symptoms in adults with diabetes mellitus type 1 and type 2: design of a randomised controlled trial. BMC Psychiatry. 2013;13(1):1–24. doi:10.1186/1471-244X-13-1
38. Ballotari P, Ferrari F, Ballini L, Chiarenza A, Manicardi V, Rossi G. Lifestyle-tailored interventions for South Asians with type 2 diabetes living in high-income countries: a systematic review. Acta Diabetol. 2017;54:785–794. doi:10.1007/s00592-017-1008-8
39. Navodia N, Wahoush O, Tang T, Yost J, Ibrahim S, Sherifali D. Culturally tailored self-management interventions for south asians with type 2 diabetes: a systematic review. Can J Diabetes. 2019;43(6):445–452. doi:10.1016/j.jcjd.2019.04.010
40. Alharbi T, Alhumaidi B, Alharbi M, et al. Diabetes education self-management intervention in improving self-efficacy for people with type 2 diabetes in the Gulf Cooperation Council countries: a systematic review. Diabetes Metab Syndr. 2023;17(12):102906. doi:10.1016/j.dsx.2023.102906
41. Riangkam C, Ruksakulpiwat S, Jariyasakulwong P, Panichpathom V, Phianhasin L. Educational interventions for individuals with insulin-treated type 2 diabetes mellitus: a systematic review. Patient Prefer Adherence. 2024;18:1831–1843. doi:10.2147/PPA.S482882
42. Subhan F, Fernando D, Thorlakson J, Chan C. Dietary interventions for type 2 diabetes in south asian populations—a systematic review. Curr Nutr Rep. 2022;12:39–55. doi:10.1007/s13668-022-00446-9
43. Alshammari M, Lee RLT, Stubbs M, Chan SWC. Effectiveness of psychoeducation interventions for pregnant women with gestational diabetes mellitus: an integrative review. BMC Public Health. 2024;24(1):2929. doi:10.1186/s12889-024-20428-6
44. Dong L. Association between out-of-pocket health expenditure and the disease burden of diabetes mellitus: insights from GBD 2021. Front Public Health. 2025;13.
45. J DRF, Ogurtsova K, Linnenkamp U, et al. IDF Diabetes Atlas estimates of global health expenditures on diabetes in 2014. Diabet Res Clin Pract. 2016;117:48–54. doi:10.1016/j.diabres.2016.04.016
46. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:1–11.
47. Basak Cinar A, Schou L. Health promotion for patients with diabetes: health coaching or formal health education? Int Dent J. 2014;64(1):20–28. doi:10.1111/idj.12058
48. Chew BH, Vos RC, Stellato RK, Ismail M, Rutten GEHM. The effectiveness of an emotion-focused educational programme in reducing diabetes distress in adults with Type 2 diabetes mellitus (VEMOFIT): a cluster randomized controlled trial. Diabet Med. 2018;35(6):750–759. doi:10.1111/dme.13615
49. Chiu CJ, Hu YH, Wray LA, et al. Dissemination of evidence-base minimal psychological intervention for diabetes management in Taiwan adults with type 2 diabetes. Int J Clin Exp Med. 2016;9(7):14489–14498.
50. Guo J, Wang H, Ge L, Valimaki M, Wiley J, Whittemore R. Effectiveness of a nurse-led mindfulness stress-reduction intervention on diabetes distress, diabetes self-management, and HbA1c levels among people with type 2 diabetes: a pilot randomized controlled trial. Res Nurs Heal. 2022;45(1):46–58. doi:10.1002/nur.22195
51. Jung HY, Lee H, Park J. Comparison of the effects of Korean mindfulness-based stress reduction, walking, and patient education in diabetes mellitus. Nurs Heal Sci. 2015;17(4):516–525. doi:10.1111/nhs.12229
52. Li F, Yao P, Hsue C, Xu J, Lou Q. Impact of “Conversation Maps” on diabetes distress and self-efficacy of Chinese adult patients with type 2 diabetes: a pilot study. Patient Prefer Adherence. 2016;10:901–908. doi:10.2147/PPA.S95449
53. Liu Y, Han Y, Shi J, et al. Effect of peer education on self-management and psychological status in type 2 diabetes patients with emotional disorders. J Diabetes Investig. 2015;6(4):479–486. doi:10.1111/jdi.12311
54. Maghsoudi Z, Razavi Z, Razavi M, Javadi M. Efficacy of acceptance and commitment therapy for emotional distress in the elderly with type 2 diabetes: a randomized controlled trial. Diabetes Metab Syndr Obes. 2019;12:2137–2143. doi:10.2147/DMSO.S221245
55. Sharif F, Masoudi M, Ghanizadeh A, Dabbaghmanesh MH, Ghaem H, Masoumi S. The effect of cognitive-behavioral group therapy on depressive symptoms in people with type 2 diabetes: a randomized controlled clinical trial. Iran J Nurs Midwifery Res. 2014;19(5):529–536.
56. Shayeghian Z, Hassanabadi H, Aguilar-Vafaie ME, Amiri P, Besharat MA. A randomized controlled trial of acceptance and commitment therapy for type 2 diabetes management: the moderating role of coping styles. PLoS One. 2016;11(12):1–14. doi:10.1371/journal.pone.0166599
57. Zuo X, Dong Z, Zhang P, et al. Effects of cognitive behavioral therapy on sleep disturbances and quality of life among adults with type 2 diabetes mellitus: a randomized controlled trial. Nutr, Metab Cardiovasc Dis. 2020;30(11):1980–1988. doi:10.1016/j.numecd.2020.06.024
58. Shi M, lan LZ, bo ZY, et al. Effect of health education based on integrative therapy of chinese and western medicine for adult patients with type 2 diabetes mellitus: a randomized controlled study. Chin J Integr Med. 2018;24(2):94–102. doi:10.1007/s11655-015-2113-6
59. Bergmame L, Shaw S. Clinical utility of psychoeducational interventions for youth with type 1 diabetes: a scoping review. Contin Educ. 2021;2(1):76–108. doi:10.5334/cie.28
60. Ni YX, Ma L, Li JP. Effects of mindfulness-based intervention on glycemic control and psychological outcomes in people with diabetes: a systematic review and meta-analysis. J Diabetes Investig. 2021;12(6):1092–1103. doi:10.1111/jdi.13439
61. Ee CC, Al-Kanini I, Armour M, et al. Mindfulness-based interventions for adults with type 2 diabetes mellitus: a systematic review and meta-analysis. Integr Med Res. 2025;14(2):101138. doi:10.1016/j.imr.2025.101138
62. Jiang S, Pan X, Li H, Su Y. Global trends and developments in mindfulness interventions for diabetes: a bibliometric study. Diabetol Metab Syndr. 2024;16(1):43. doi:10.1186/s13098-024-01288-x
63. Cahyono I, Sulaeman R, Hanum L, Karyono SM, Mubarok AS. Comparison of the effectiveness between mindfulness therapy and cognitive behavioral therapy in treating anxiety disorders. J World Futur Med Heal Nurs. 2024;2(2):203–215. doi:10.70177/health.v2i2.756
64. Christodoulou V, Flaxman PE, Morris EMJ, Oliver JE. Comparison of mindfulness training and acceptance and commitment therapy in a workplace setting: results from a randomized controlled trial. Eur J Work Organ Psychol. 2024;33(3):368–384. doi:10.1080/1359432X.2024.2314934
65. Preechasuk L, Sriussadaporn P, Likitmaskul S. The obstacles to diabetes self-management education and support from healthcare professionals’ perspectives: a nationwide survey. Diabetes Metab Syndr Obes. 2019;12:717–727. doi:10.2147/DMSO.S195916
66. Adu MD, Malabu UH, Malau-Aduli AEO, Malau-Aduli BS. Enablers and barriers to effective diabetes self-management: a multi-national investigation. PLoS One. 2019;14(6):e0217771. doi:10.1371/journal.pone.0217771
67. Young-Hyman D, De Groot M, Hill-Briggs F, Gonzalez J, Hood K, Peyrot M. Psychosocial care for people with diabetes: a position statement of the American diabetes association. Diabetes Care. 2016;39:2126–2140. doi:10.2337/dc16-2053
68. Ghoreishi MS, Vahedian-Shahroodi M, Jafari A, Tehranid H. Self-care behaviors in patients with type 2 diabetes: education intervention base on social cognitive theory. Diabetes Metab Syndr. 2019;13(3):2049–2056. doi:10.1016/j.dsx.2019.04.045
69. Yakubu TI, Pawer S, West NC, Tang TS, Görges M. Impact of digitally enabled peer support interventions on diabetes distress and depressive symptoms in people living with type 1 diabetes: a systematic review. Curr Diab Rep. 2024;25(1):1. doi:10.1007/s11892-024-01560-4
70. Caballero Mateos I, Morales Portillo C, Lainez López M, Á V-A. Efficacy of a digital educational intervention for patients with type 2 diabetes mellitus: multicenter, randomized, prospective, 6-month follow-up study. J Med Internet Res. 2025;
71. Puspitasari Y, Kusumawati PD. Digital-based education and counseling on self-care behaviors in patients with type 2 diabetes mellitus as a prevention strategy for neuropathy complications. Int.J. Nurs. Pract. 2025;8(4):965–977.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Investigating the Feasibility, Acceptability, and Impact of a Brief Dementia Awareness for Caregivers (DAC) Course: A Mixed Methods Study
Patel R, Evans I, Stoner CR, Spector A
Clinical Interventions in Aging 2023, 18:1923-1935
Published Date: 21 November 2023
Assessment of Health-Related Quality of Life Among Patients with Chronic Diseases and Its Relationship with Multimorbidity: A Cross-Sectional Study from Saudi Arabia
Alzarea AI, Khan YH, Alzarea SI, Alanazi AS, Alsaidan OA, Alrowily MJ, Al-Shammari M, Almalki ZS, Algarni MA, Mallhi TH
Patient Preference and Adherence 2024, 18:1077-1094
Published Date: 4 June 2024
Psychometric Impact of Diabetic Retinopathy-Induced Visual Impairment: A Hospital-Based Study, Al Buraimi, Sultanate of Oman
Vankudre GS, Mohamed ZD, Ayyappan JP, Alrasheed SH
Clinical Optometry 2025, 17:3-10
Published Date: 13 January 2025
A Systematic Review of Continuity of Care Strategies for Enhancing Diabetes Self-Management in Older Adults in Asian Countries
Sari CWM, Haroen H, Juniarti N, Amalia L, Pardosi JF
Journal of Multidisciplinary Healthcare 2025, 18:5441-5459
Published Date: 2 September 2025
Medication Adherence Interventions Among People Living with Diabetes: A Systematic Review
Wang M, Lee K, Thew HZ, Sowtali SN, Jiang Q, Cao Y, Lim PY
Patient Preference and Adherence 2025, 19:3095-3112
Published Date: 7 October 2025