Back to Journals » Journal of Pain Research » Volume 19
A Scoping Review of Flotation-REST (Restricted Environmental Stimulation Therapy) for Chronic Pain and Associated Comorbidities
Authors Stuart SJ ![]() , Achury LK, Kline M, Bair MJ
, Achury LK, Kline M, Bair MJ
Received 5 September 2025
Accepted for publication 17 January 2026
Published 11 February 2026 Volume 2026:19 565238
DOI https://doi.org/10.2147/JPR.S565238
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Sam J Stuart,1 Lizeth K Achury,2 Matthew Kline,3 Matthew J Bair4
1Indiana University School of Medicine – Terre Haute, Terre Haute, IN, USA; 2Indiana University School of Medicine, Indianapolis, IN, USA; 3VA Center for Health Information and Communication, Indianapolis VA Medical Center Indianapolis, Indianapolis, IN, USA; 4VA Center for Health Information and Communication, Indiana University School of Medicine, and Regenstrief Institute, Indianapolis, IN, USA
Correspondence: Sam J Stuart, Email [email protected]
Background: Flotation-Restricted Environmental Stimulation Therapy (flotation-REST) is a novel nonpharmacologic intervention for chronic pain. Previous reviews have examined the effects of flotation-REST on other outcomes, but a comprehensive review centered on chronic pain has not been conducted.
Objective: To describe the extent, range, and nature of research evaluating flotation-REST for chronic pain and associated comorbidities, including psychological, physiological, and biomarker outcomes.
Eligibility Criteria: No restrictions were placed on study design or setting. Studies conducted in animals, not published in English, or assessing outcomes outside the scope of the review were excluded.
Sources of Evidence: Ovid MEDLINE, the Cochrane Library, Embase, and PsycINFO were searched from inception to January 2025. Reference lists of relevant studies and reviews were screened.
Charting Methods: Two reviewers independently screened titles, abstracts, and full texts. One reviewer extracted data. Variables included study design, population, controls, outcomes, and intervention parameters. Risk of bias for randomized trials was assessed using the Cochrane RoB 2 tool.
Results: Eight studies (6 randomized controlled trials, and 2 single-arm pre/post) comprising 401 participants met inclusion criteria. Studies consistently reported improvements in pain intensity and frequency, fewer pain locations, and greater pain tolerance and detection. Anxiety and depression were substantially reduced in most studies. Sleep quality and latency improved in some studies, though others reported no benefit. Stress consistently declined, and optimism increased. Physiological outcomes were variable. Biomarker analysis demonstrated a post-treatment reduction in 3 methoxy-4-hydroxyphenylethyleneglycol (MHPG), a norepinephrine metabolite, and increased prolactin. Considerable heterogeneity in study designs, intervention protocols, outcome measures, and follow-up duration precluded meta-analysis.
Conclusion: Flotation-REST appears promising for reducing chronic pain and enhancing psychological well-being. Physiological and biomarker effects remain unclear. High-quality randomized trials with standardized interventions and longitudinal follow-up are needed to confirm efficacy, sustainability, and clinical applicability.
Keywords: flotation-REST, float therapy, flotation therapy, sensory deprivation, relaxation therapy, chronic pain
Introduction
Pain is one of the most common reasons for seeking medical care in the United States, accounting for nearly one in four outpatient clinic visits and affecting more than 100 million adults.1,2 As of 2023, 24.3% of US adults live with chronic pain; 8.5% experience high-impact chronic pain – chronic pain that restricts life or work activities.3 Chronic pain is frequently comorbid with mental health concerns, such as depression, anxiety, stress, and sleep disturbances, which exacerbate patient suffering and complicate treatment.4,5 The societal and economic burdens of chronic pain are immense, often hindering one’s ability to work and function in society effectively.6 The estimated annual healthcare cost of acute and chronic pain is $735 billion and $725 billion per year, respectively.
Pain medications account for more than 12% of all prescriptions,7 costing $17.8 billion annually in the United States.8 Opioid analgesics are commonly prescribed for chronic pain; however, they are associated with major risks of abuse, misuse, and dependence.9 In 2022, 76% of the nearly 108,000 drug overdose deaths in the United States involved an opioid.10 Consequently, primary care physicians often struggle to treat chronic, non-cancer pain while preventing opioid misuse, abuse, and addiction.11,12
The development and integration of effective tools for non-pharmacological pain management remains one of the most urgent and unmet needs. Patients are increasingly turning to complementary and integrative health options to treat their pain either instead of, or concurrently with, prescribed pharmaceuticals.13 Recent consensus clinical guidelines recommend multi-modal chronic pain treatments focused on reducing reliance on prescription medications, with an emphasis on non-pharmacological pain treatment modalities.14 As a result, research to identify safe and effective non-pharmacological treatments to improve pain management is critical.
One such emerging modality is flotation-REST (Restricted Environmental Stimulation Therapy), which induces a deep relaxation response through sensory isolation while floating in a water-filled tank.15 This relaxation technique alleviates pain by reducing muscle tension and improves overall well-being by calming the mind and reducing stress.16,17 During a flotation-REST session, an individual floats supine in a tank filled with warm water and saturated Epsom salts (Mg2SO4). Flotation tanks are dark, soundproof environments resembling large bathtubs with lids, and an average flotation session lasts approximately 45 minutes.17 Early evidence suggests that Flotation-REST could be readily implemented in clinical or therapeutic settings due to its relatively short treatment time, ease of use, cost-effectiveness and safety.18 Reported adverse effects are minimal or completely absent.17
Despite the potential flotation-REST holds, its therapeutic applications have been incompletely characterized. Two reviews of flotation-REST have been previously published, but the effects of flotation-REST on chronic pain and its common comorbidities have not been comprehensively summarized. A meta-analysis of 27 studies (1980–2002) gathered from Medline and PsycINFO reported that flotation-REST can be a valuable stress management tool, either as primary or adjunctive therapy. The review further described its positive effects on physiology, well-being, and performance during activities involving a physiological component.17 More recently, a 2017 systematic review of 9 full-text articles, extracted from PubMed, Google Scholar, Web of Science and PsycINFO demonstrated the beneficial effects of flotation-REST on sleep, even 4 to 6 months post-treatment.19 Chronic pain was outside the scope of both previously published reviews. The current study is not reported as a systematic review due to the high levels of variability in outcomes measures, patient populations, flotation session duration and number, and control environments.
This scoping review aims to map the evidence on flotation-REST for chronic pain in human populations, focusing on pain-related, mental health, physiological, and biomarker outcomes.
Methods
A comprehensive search of Ovid MEDLINE, the Cochrane Library, Embase, and PsycINFO was conducted from database inception to May 22, 2020, with guidance from a medical librarian. The search was updated in January 2025 to capture recent publications. Results are reported in accordance with PRISMA guidelines for scoping reviews.20 Additional articles were identified through a manual reference screening of relevant articles. We used the combined search terms “pain AND flotation-REST” along with broader umbrella terms including “sensory deprivation” and “relaxation therapy”. Studies were eligible for inclusion if they involved human participants, were published in English, and reported on outcomes related to pain or its associated comorbidities (e.g., anxiety, depression, stress, or sleep disturbances) in populations with chronic pain. No restrictions were placed on study design, setting, or country of origin. Studies were excluded if they were conducted in animals, published in languages other than English, or assessed outcomes outside the scope of the review. The inclusion/exclusion criteria were purposely broad to ensure a comprehensive collection of relevant evidence regarding flotation-REST. All variables relevant to the outcomes of interest were extracted by one reviewer (S.S. or L.A)., along with country, study design, sample size, study population, control, and duration. Missing or unclear data was noted on the extraction sheet. No attempts were made to contact authors regarding missing data. All data extracted from the included studies are presented in the manuscript tables and Supplemental Table A.1.
Titles and abstracts were screened independently by two reviewers, and full texts were retrieved for potentially relevant studies. Discrepancies were resolved by consensus or adjudicated by a third reviewer. Given the heterogeneity of study designs and outcome measures, a qualitative synthesis was performed. No review protocol was registered.
Results
Literature Search
A total of 9,027 texts were identified as possibly relevant. Of these, 6,600 studies were screened, and 41 studies either met the inclusion criteria or could not be evaluated from abstract alone. 33 studies were excluded at the full text stage, most often for the wrong indication (n=12) or wrong outcomes (n=12). Eight studies met the inclusion criteria and were included (Figure 1). The outcomes were grouped by category below. Of the 8 papers, 6 were randomized controlled trials (RCTs), while the remaining papers were single-arm (pre/post) studies (n=2). Risk of bias was assessed using the Cochrane Risk of Bias 2.0 tool (RoB 2) for RCTs; no validated RoB 2 tool is available for single-arm studies.21 Overall, 66% (4/6) of the RCTs were rated as having “some concerns” regarding risk of bias, most often resulting from a lack of blinding of outcome assessors. Otherwise, these studies were low risk. As most outcomes were derived from self-reported instruments, the potential impact of assessor blinding on outcome measurement was likely minimal. Study assessments are provided in Supplemental Table A.1.
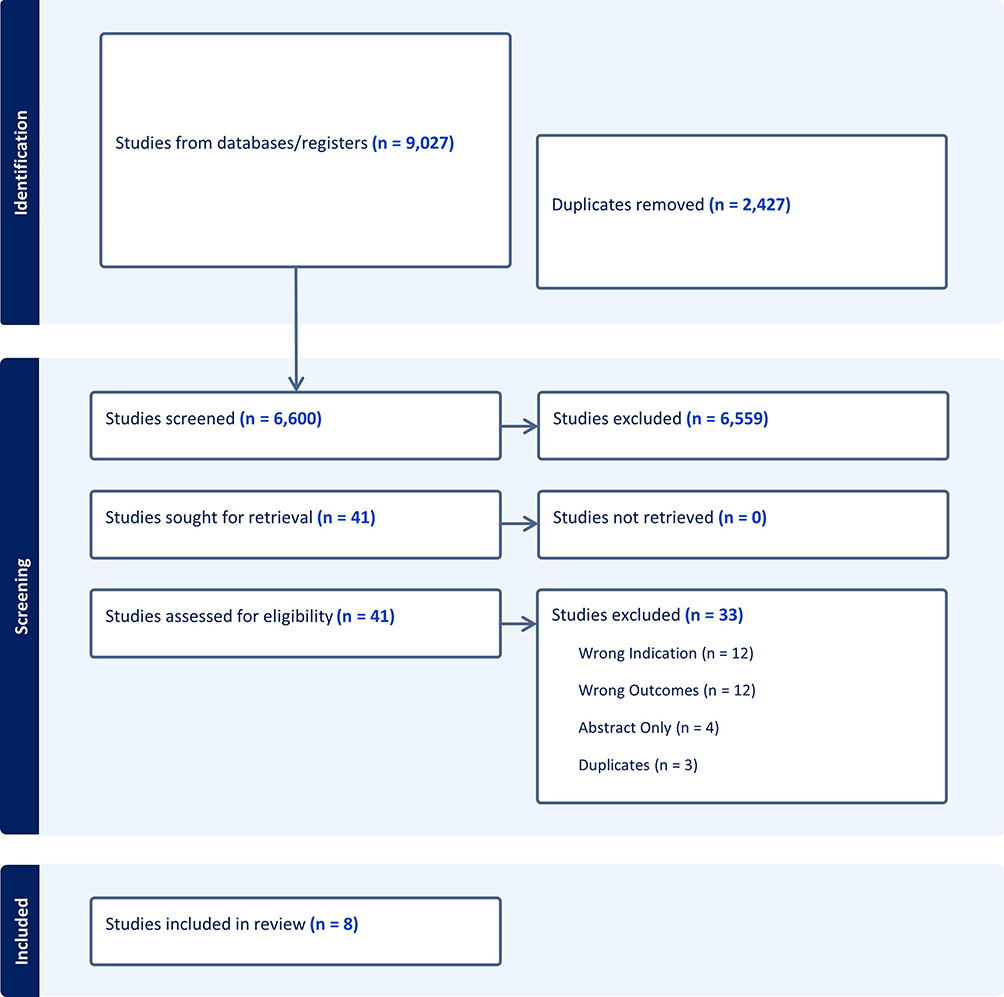 |
Figure 1 PRISMA flow diagram of included studies. |
 |
Table 1 Study Details and Patient Demographics |
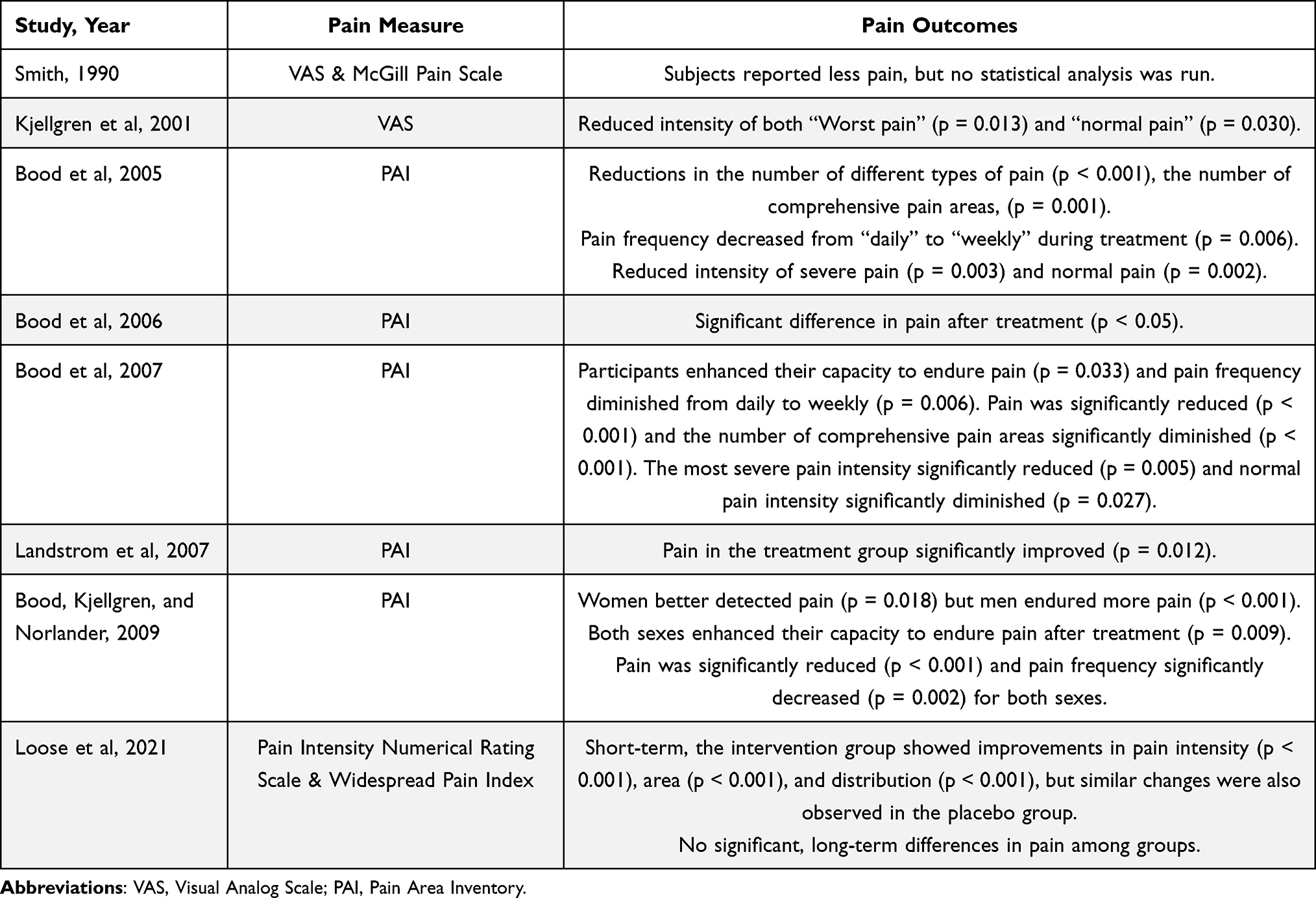 |
Table 2 Pain Measures and Outcomes from Clinical Trials of Flotation-REST |
 |
Table 3 Anxiety and Depression Measures and Outcomes from Clinical Trials of Flotation-REST |
 |
Table 4 Sleep and Stress Measures and Outcomes from Clinical Trials of Flotation-REST |
 |
Table 5 Other Mood and Disposition Health Measures and Outcomes from Clinical Trials of Flotation-REST |
 |
Table 6 Physiological and Biomarker Measures and Outcomes from Clinical Trials of Flotation-REST |
Study Details and Patient Demographics
The included studies cumulatively evaluated 401 participants (Table 1). Most ranged between 30 and 50 years old. Sample populations include those with chronic neck, back, or muscular pain. Half of the studies reported outcomes of patients with stress-related pain.
Control conditions varied across studies. Some studies had no control group, while others consisted of a Wait-List Control (WLC) in which no intervention or treatment was applied.16,22–25 Another study used a sensory controlled space; participants sat in a chair and read magazines.26
The flotation environment was likewise variable, as different flotation facilities across various cities and countries were used. Most studies did not specify using an open vs closed tank. One study specified that 13% of participants requested to float with an open lid (either fully opened or opened less than 5cm) while others floated with a closed lid.25 Most studies reported similar tank sizes (± 0.4m per dimension), most commonly measuring 2.7m x 1.5m x 1.3m, with a water depth between 0.2m and 0.3m.16,24,26–28 Some tanks had reduced light and noise, some were noiseless but had reduced light, and others had total darkness and total silence.16,24,26–28
The frequency and duration of treatment varied, with studies reporting at least 5 sessions over 20 days.25 Frequently, studies delivered a higher number of sessions, including eight sessions with no time frame specified or nine sessions over 3 weeks.16,22 Half of the studies included in this review consisted of 12 flotation-REST sessions over 6–7 weeks, with one study uniquely performing 33 flotation sessions over 35 weeks.23,24,26–28 Furthermore, flotation sessions ranged from 45 to 90 minutes, most commonly 45 minutes.16,24–28
Pain
Across the included studies, flotation-REST was associated with significant improvements in multiple pain-related outcomes (Table 2). Participants reported reductions in pain frequency and intensity, lower sensitivity to induced pain, fewer reported pain areas, and increased pain tolerance and detection.16,22–24,26–28 Short-term improvements in widespread pain were also reported, although the duration of pain improvement is uncertain.25 A 2021 study reported no significant differences in pain in the long-term (6 months post-treatment), but previous studies reported positive effects 4 months and 6 months after treatment.25,26
Anxiety and Depression
All articles that reported anxiety outcomes for patients with chronic pain found improvements in symptoms both during and after flotation-REST (Table 3). One study reported significant benefit up to 4 months post-treatment.26 Results were similarly positive for depression, though one contradictory study found no significant effect.25
Sleep and Stress
Results related to sleep and stress outcomes were mixed (Table 4). After flotation-REST sessions, some participants reported improved sleep latency (time elapsed to fall asleep), without significant differences in sleep duration or quality.16,25 Other studies revealed improvements in sleep quality immediately following a session, with one study showing the positive effect lasting up to 4 months post-treatment.24,28 Most studies observed significant stress reduction both during and after treatment sessions, with the effect likewise lasting 4 months after treatment.26–28 One contradictory study found no significant change in stress.22
Mood and Disposition
Flotation-REST was also associated with positive effects on broader mood and dispositional traits (Table 5). Optimism scores increased both during and after the treatment period, with effects maintained for 4 months after treatment.16,26–28 One study reported a significant increase in positive affect and a decrease in negative affect.27 Others reported a reduction in negative affectivity only, with no effect on positive affect, or no significant effects or interactions for either positive or negative affectivity.26,28 The treatment groups of flotation-REST reported greater relaxation, and increased mindfulness.16,26
Physiological and Biomarker Outcomes
Several studies also examined physiological and biomarker responses to flotation-REST (Table 6). Small or inconsistent changes in cardiovascular parameters were observed. Several studies reported no significant effect on systolic blood pressure, but a decrease in diastolic blood pressure.16,27,28 Studies reported either no significant difference, or small- to medium-sized reductions in heart rate.25,27 Small effects in heart rate variability parameters were also reported.25
Endocrine and neurochemical biomarkers yielded mixed findings. Prolactin concentrations increased immediately following treatment but returned to baseline at 4 months follow-up.26 Beta-endorphin concentrations did not significantly change pre- to post-treatment and were paradoxically higher in control participants than in the flotation group.16 In contrast, levels of 3-methoxy-4-hydroxyphenylethyleneglycol (MHPG) - a norepinephrine metabolite - were significantly reduced post-treatment.16 Electrophysiological data from electromyography (EMG) revealed a reduction from pre-test to post-test and sporadic improvements after treatment.22 No adverse events were reported in any of the included studies, either during treatment, immediately post-treatment, or at follow-up assessments.
Discussion
While most studies included in this review were randomized controlled trials, there were also a few single arm pre/post studies. All studies included in this review exhibited substantial heterogeneity in terms of study design, participant populations, flotation equipment, number and duration of flotation sessions, control conditions, and follow-up periods. There is no consensus on the optimal number and length of flotation sessions.
Despite heterogeneity, reductions in pain, anxiety, and stress were relatively consistent across studies. Several physiological and psychological processes may account for these similarities. Flotation-REST reduces sensory input and increases mindfulness, potentially facilitating deep relaxation responses. Sympathetic downregulation may also occur through decreased stimulation, which could in turn reduce muscle tension, pain perception, and stress-related autonomic arousal. Additionally, the warm, buoyant environment may stimulate parasympathetic activity.
Findings involving biomarkers were markedly inconsistent. These discrepancies may stem from differences in baseline stress physiology, variability in timing of biomarker collection, and the generally small sample sizes used in these studies. Heterogeneity in disease severity, medication use, and psychological traits across study samples may further complicate the interpretation of biomarker responses, leading to inconsistent or attenuated effects.
Differences in tank type (open vs closed), size, lighting, sound insulation, and participant control over sensory input may have also contributed to inconsistent findings. The importance of water immersion, tank size and type, and the presence of swimwear are unclear; these physical and environmental factors remain understudied and may modulate therapeutic outcomes.29 Previous research showed that the presence of light inside the floating tank has no effect on treatment outcome, but this has not been reevaluated in several decades.30 Studies analyzing the effects of a noiseless versus noise-reduced tank have not been conducted.
A rigorous study by Loose et al attempted to isolate the effects of floating and restricted environmental stimulation by designing a modified control environment that adjusted buoyancy and added multisensory inputs. Despite these efforts, both the control and experimental groups experienced positive results established in previous studies of flotation-REST, including reduced pain and improved anxiety, depression, sleep, and stress. This study raises questions about flotation-REST’s efficacy in the context of placebo effects, expectancy, and non-specific relaxation responses.25
Another possibly confounding factor is the variability in follow-up time, with studies reporting anywhere from 0 days follow-up (ie immediately after the float session) to 6 months follow-up.16,22–27 Few studies had a follow-up period greater than one day, limiting understanding of long-term effects of flotation-REST. Despite these limitations, none of the articles reported any adverse events during, directly after, or in follow-up of flotation-REST treatments, supporting the safety of the intervention.
Limitations
This review has many limitations. First, most studies relied on self-reported outcomes, which are vulnerable to bias and may be influenced by participant expectations. Reportedly, some participants were already familiar with flotation-REST or with the treatment facility and its staff, which could have influenced expectations about treatment efficacy. A few studies lacked control groups or randomization, limiting causal inference, and introducing a confounding placebo effect. The absence of standardized protocols across studies (e.g., session number, tank type, environmental controls) further complicates comparisons and synthesis. No conclusions about the optimal number of sessions, session duration, or sensory control of light and sound can be made in aggregate. Some studies were intrinsically limited by using a within-subject randomized controlled design. Many only focused on the immediate effects following a single flotation-REST session, without exploring the cumulative effects of multiple sessions; sustained long-term benefits or adverse effects are poorly understood. Many of the participants included in these studies continued to receive their concomitant medications and therapies for the study’s target disease or condition, which may have confounded results in studies focused on populations with chronic pain.
This review is not a systematic review, rather it is a scoping review that summarizes the current scope of studies on flotation-REST and its effects on pain and its comorbid conditions. A meta-analysis was not performed due to the heterogeneity of study designs, targeted diseases and study conditions, study measures and outcomes, and treatment and control conditions. Although a broad search strategy was used, some relevant articles may have been missed due to language and database limitations.
Conclusions
This scoping review summarized the effects of flotation-REST on pain and its common comorbid mental health conditions. The results suggest that flotation-REST is a safe, well-tolerated, and potentially effective non-pharmacological treatment for reducing chronic pain and associated symptoms such as anxiety, depression, stress, and sleep difficulties. Further improvements were noted in positive affect and optimism. Findings related to physiological and biomarker outcomes were more variable and often limited by small effect sizes.
Moving forward, high-quality RCTs with standardized flotation protocols, control conditions, biomarker outcomes, and long-term follow-up are essential to better assess the clinical efficacy and sustainability of this intervention. Evaluating larger sample sizes and longer treatment durations will be integral to determine the optimal number and frequency of flotation-REST sessions to produce and sustain these effects over time.
Studies should also explore mechanistic pathways, including neuroendocrine and autonomic markers, such as serotonin metabolite 5-hydroxyindole acetic acid and oxytocin. Tools to incorporate include EEG and fMRI to examine effects on central nervous system function. One study explored possible sex differences among patients with stress-related pain undergoing flotation-REST, though further research should evaluate predictors of response potency, such as age, psychological traits, or health behaviors (eg, smoking or alcohol use).27 Finally, comparative effectiveness studies should examine flotation-REST for pain reduction alongside or in combination with other mind-body interventions, such as mindfulness meditation, yoga, or tai-chi.
Flotation-REST holds promise as a complementary therapy in the management of chronic pain, but its integration into routine clinical practice will require a stronger evidence base, especially regarding long-term outcomes and physiological mechanisms.
Abbreviations
Flotation-REST, Flotation-Restricted environmental stimulation therapy; RCT, Randomized controlled trial; EMG, Electromyography; MHPG, 3-methoxy-4-hydroxyphenylethyleneglycol.
Data Sharing Statement
The authors confirm that the data supporting the findings and conclusion of this study are available within the article and its supplementary material. All articles cited are available online.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Schappert SM, Burt CW. Ambulatory care visits to physician offices, hospital outpatient departments, and emergency departments: United States, 2001-02. Vital Health Stat 13. 2006;(159):1–12.
2. Gaskin DJ, Richard P. The economic costs of pain in the United States. J Pain. 2012;13(8):715–724. doi:10.1016/j.jpain.2012.03.009
3. Lucas JW, Sohi I. Chronic pain and high-impact chronic pain in U.S. adults, 2023. In: NCHS Data Brief, No 518. Hyattsville, MD: National Center for Health Statistics; 2024. doi:10.15620/cdc/169630
4. Bair MJ, Robinson RL, Katon W, Kroenke K. Depression and pain comorbidity: a literature review. Arch Intern Med. 2003;163(20):2433–2445. doi:10.1001/archinte.163.20.2433
5. Fishbain DA, Cutler R, Rosomoff HL, Rosomoff RS. Chronic pain-associated depression: antecedent or consequence of chronic pain? A review. Clin J Pain. 1997;13(2):116–137. doi:10.1097/00002508-199706000-00006
6. Dahlhamer J, Lucas J, Zelaya C, et al. Prevalence of chronic pain and high-impact chronic pain among adults - United States, 2016. MMWR Morb Mortal Wkly Rep. 2018;67(36):1001–1006. doi:10.15585/mmwr.mm6736a2
7. Turk DC. Clinical effectiveness and cost-effectiveness of treatments for patients with chronic pain. Clin J Pain. 2002;18(6):355–365. doi:10.1097/00002508-200211000-00003
8. Rasu RS, Vouthy K, Crowl AN, et al. Cost of pain medication to treat adult patients with nonmalignant chronic pain in the United States. J Manag Care Spec Pharm. 2014;20(9):921–928. doi:10.18553/jmcp.2014.20.9.921
9. Edlund MJ, Steffick D, Hudson T, et al. Risk factors for clinically recognized opioid abuse and dependence among veterans using opioids for chronic non-cancer pain. Pain. 2007;129(3):355–362. doi:10.1016/j.pain.2007.02.014
10. Spencer MR, Garnett MF, Miniño AM. Drug overdose deaths in the United States, 2002–2022. In: NCHS Data Brief, No 491. Hyattsville, MD: National Center for Health Statistics; 2024. doi:10.15620/cdc:135849
11. Rose ME. Are prescription opioids driving the opioid crisis? Assumptions vs facts. Pain Med. 2018;19(4):793–807. doi:10.1093/pm/pnx048
12. Harle CA, Bauer SE, Hoang HQ, et al. Decision support for chronic pain care: how do primary care physicians decide when to prescribe opioids? A qualitative study. BMC Fam Pract. 2015;16(1):48. doi:10.1186/s12875-015-0264-3
13. Dhanani NM, Caruso TJ, Carinci AJ. Complementary and alternative medicine for pain: an evidence-based review. Curr Pain Headache Rep. 2011;15(1):39–46. doi:10.1007/s11916-010-0158-y
14. Becker WC, Dorflinger L, Edmond SN, et al. Barriers and facilitators to use of non-pharmacological treatments in chronic pain. BMC Fam Pract. 2017;18(1):41. doi:10.1186/s12875-017-0608-2
15. Suedfeld P, Ballard EJ, Murphy M. Water immersion and flotation: from stress experiment to stress treatment. J Environ Psychol. 1983;3(2):147–155. doi:10.1016/S0272-4944(05)80153-7
16. Kjellgren A, Sundequist U, Norlander T, Archer T. Effects of flotation-REST on muscle tension pain. Pain Res Manag. 2001;6(4):181–189. doi:10.1155/2001/768501
17. Van Dierendonck D, Te Nijenhuis J. Flotation restricted environmental stimulation therapy (REST) as a stress-management tool: a meta-analysis. Psychol Health. 2005;20(3):405–412. doi:10.1080/08870440412331337093
18. Barabasz A, Barabasz M, Dyer R, et al. Clinical and Experimental Restricted Environmental Stimulation. New York: Springer-Verlag; 1993.
19. Kjellgren A, Norell-Clarke A, Jonsson K, Tillfors M. Does flotation-rest (restricted environmental stimulation technique) have an effect on sleep? Eur J Integr Med. 2020;1(33):101047. doi:10.1016/j.eujim.2019.101047
20. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMAScR): checklist and explanation. Ann Intern Med. 2018;169:467–473. doi:10.7326/M18-0850
21. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:14898. doi:10.1136/bmj.l4898
22. Smith DD. The Effectiveness of Restricted Environmental Stimulation Therapy (REST) on Reducing Chronic Low Back Pain. Western Michigan University; 1990.
23. Landstrom A, Bood SA, Kjellgren A, Norlander T. Treating stress-related pain in a clinical sample with flotation-rest: a further report on improvements in pain assessed by the pain area inventory (pai). Soc Behav Pers. 2007;35(9):1279–1280. doi:10.2224/sbp.2007.35.9.1279
24. Bood SA, Kjellgren A, Norlander T. Treating stress-related pain with the flotation restricted environmental stimulation technique: are there differences between women and men? Pain Res Manag. 2009;14(4):293–298. doi:10.1155/2009/298935
25. Loose LF, Manuel J, Karst M, et al. Flotation restricted environmental stimulation therapy for chronic pain: a randomized clinical trial. JAMA Network Open. 2021;4(5):e219627. doi:10.1001/jamanetworkopen.2021.9627
26. Bood SA, Sundequist U, Kjellgren A, et al. Eliciting the relaxation response with the help of flotation-rest (restricted environmental stimulation technique) in patients with stress-related ailments. Int J Stress Manag. 2006;13(2):154–175.
27. Bood SA, Sundequist U, Kjellgren A, et al. Effects of flotation-restricted environmental stimulation technique on stress-related muscle pain: what makes the difference in therapy--attention-placebo or the relaxation response? Pain Res Manag. 2005;10(4):201–209. doi:10.1155/2005/547467
28. Bood SA, Sundequist U, Kjellgren A, et al. Effects of flotation rest (restricted environmental stimulation technique) on stress related muscle pain: are 33 flotation sessions more effective than 12 sessions? Soc Behav Pers. 2007;35(2):143–156. doi:10.2224/sbp.2007.35.2.143
29. Forgays DG, Forgays DK, Pudvah M, Wright D. A direct comparison of the ‘wet’ and ‘dry’ flotation environments. J Environ Psychol. 1991;11(2):179–187. doi:10.1016/S0272-4944(05)80075-1
30. Turner JW, Fine T, Ewy G, et al. The presence or absence of light during flotation restricted environmental stimulation: effects on plasma cortisol, blood pressure, and mood. Biofeedback Self Regul. 1989;14(4):291–300. doi:10.1007/BF00999120
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.