")
Back to Journals » Journal of Pain Research » Volume 15
A Review of Current Perspectives on Facial Presentations of Primary Headaches
Authors Peng KP , Benoliel R, May A
Received 18 January 2022
Accepted for publication 30 May 2022
Published 3 June 2022 Volume 2022:15 Pages 1613—1621
DOI https://doi.org/10.2147/JPR.S294404
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Alexandre F DaSilva
Kuan-Po Peng,1 Rafael Benoliel,2 Arne May1
1Department of Systems Neuroscience, University Medical Center Hamburg-Eppendorf, Hamburg, Germany; 2Department of Diagnostic Sciences, Rutgers School of Dental Medicine, Rutgers University, Newark, NJ, USA
Correspondence: Arne May, Department of Systems Neuroscience, University Medical Center Hamburg-Eppendorf, Martinistr. 52, D-20246, Hamburg, Germany, Tel +49-40-7410-59189, Fax +49-40-7410-59955, Email [email protected]
Abstract: Orofacial pain (OFP) has recently been classified and subdivided into a number of groups, similar to headache disorders in the International Classification of Headache Disorders (ICHD). A novel group of OFP has been established whose major feature is that they resemble primary headache disorders occurring in the V2 or V3 dermatomes. These follow the clinical criteria and associated symptoms of the eponymous headache syndromes. Following the recent International Classification of Orofacial Pain (ICOP), three types are differentiated: Headache which spread into the face (type 1), facial pain which replaced headache but maintained the same characteristics and associated symptoms of the former headache (type 2), and de-novo orofacial pain that resembles primary headache types without any involvement of the ophthalmic trigeminal branch (type 3). The epidemiology is unclear: type 1 and 2 are not exactly common, they certainly exist in a notable proportion of headache patients, whereas type 3 may be rather rare. Since effective treatment options are available, it is important for clinicians to recognize such syndromes early to avoid misdiagnosis and unnecessary treatment, which most of these patients still experience. This review gives an up-to-date summary of diagnosis, pathophysiology and treatment of attack-like non-dental facial pain disorders.
Keywords: facial pain, classification, migraine, cluster headache, treatment
Introduction
Headache is a universal experience and occurs at least once in nearly all human beings. It has been estimated that 40–50% of the adult population may have an active headache disorder, among which most are primary headache disorders.1 According to the definition of the International Classification of Headache Disorders, 3rd edition (ICHD-3), headache refers to pain located in the head or in the face above the orbitomeatal line; pain below this line will be regarded as facial pain2 although this has recently been challenged.3 This arbitrary border, the orbitomeatal line, roughly corresponds to the border between the ophthalmic (V1) and maxillary (V2) branches of the trigeminal nerve. This differentiation also reflects the intracranial anatomy: the supratentorial dura mater is primarily innervated by the V1 branch of the trigeminal nerve, which is the same branch responsible for “pain in the face” above the orbitomeatal line.4 In the clinical practice of pain, these anatomical borders are less relevant, regional pain clearly ignores these borders and “facial pains” spread to the “head” and vice versa.
According to ICHD-3, the primary headaches consist of migraines, tension-type headaches, trigeminal autonomic cephalalgias (TACs) and a mixed group termed other primary headaches disorders (Table 1). Each of these groups is subdivided into separate entities if relevant and subsequently into temporally dependent subgroups defined by the frequency of attacks. A primary headache is a disorder, not caused by or attributed to another disorder. This is in sharp contrast to a secondary headache which is caused by another underlying disorder. Thus, in theory, and often in practice, a headache may have the characteristics of a primary headache, but a causative disorder is detected. Therefore, it would be diagnosed as a secondary headache.
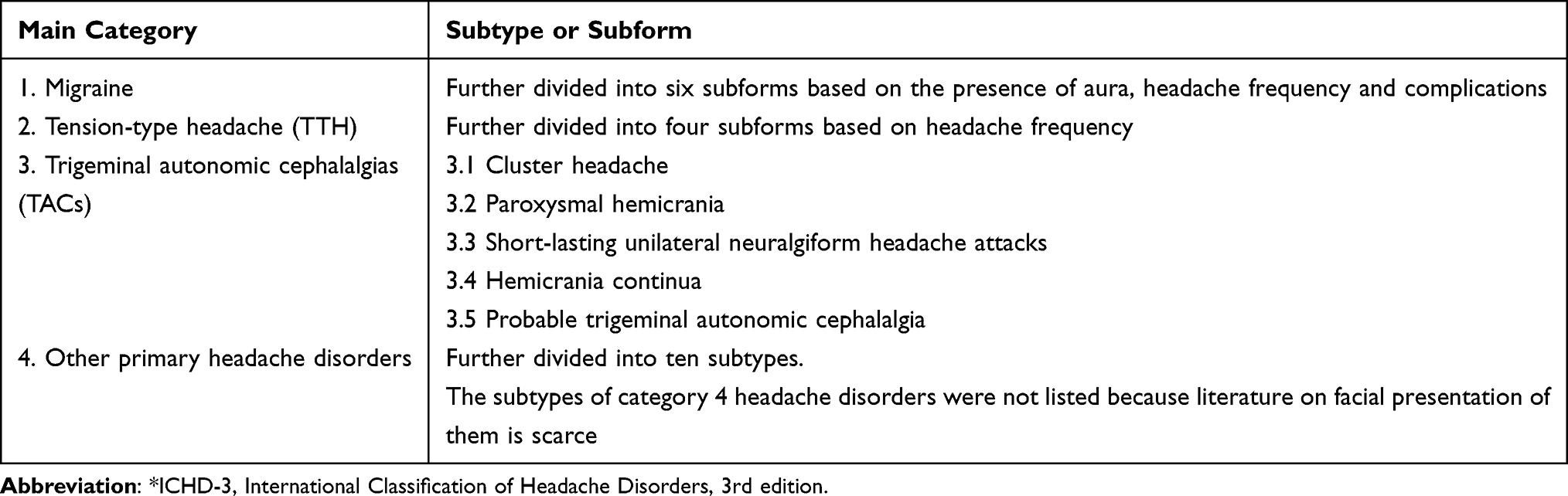 |
Table 1 Classification of Primary Headache Disorders Based on the ICHD-3* |
Relative to headache, the prevalence of facial pain is much lower, with an incidence rate of 38.7 per 100,000 person-years.5 The anatomical definition of headache (V1) vs facial pain (V2, V3) is clear and seems internationally accepted. However, the clinical borders between headache and facial pain are often blurred, questioning the exact prevalence of each discrete disorder. Migraine pain may extend to V2, sometimes even to the mandibular branch (V3) of the trigeminal nerve.6,7 Even rarer, some patients experience facial migraine – defined as attacks fulfilling the criteria for migraine located exclusively in the V2/V3 dermatomes.8 In these patients, the atypical (V2 or V3) location of a “headache” may lead to misdiagnosis or unnecessary treatment.9 On the other hand, myofascial pain in a temporomandibular disorder is considered to be the most common cause of chronic facial pain, featured by ongoing pain that can be reproduced by pressure over at least the masseter and temporalis muscle.10 Pain in the temporalis muscle is clearly a “headache” and pain in the masseter a “facial pain”. Is myofascial pain then a head or facial pain?11
One hypothesis for the involvement of the non-V1 dermatome is the initiation and establishment of central sensitization, which leads to the spread of pain beyond the primary region into the lower trigeminal branches, or in some cases even outside the cranium (eg, arm).12 Alternatively, the neurovascular activation of the V1 branch during certain headache types may lead to coactivation of the adjacent trigeminal branches, which subsequently leads to facial pain.13,14 A third possibility is that neurovascular activation occurs in V2 and/or V3 without the involvement of V1. We aim to provide an overview of the facial presentations of primary headache disorders, including their possible pathophysiology, and how to differentiate the “facial pain presentations” of headache disorders from primary facial pain disorders.
Historical Perspective and Development
Migraine is probably the first primary headache that ignited interest in the involvement of the face and the relationship between head and facial pain. That migraine involved orofacial structures is not new. In 1963 Wolff wrote “The sites of migraine headache are notably temporal, supraorbital, frontal, retrobulbar, parietal, auricular, and occipital. However, they may occur as well in the malar region, the upper and lower teeth, at the base of the nose, or in the medial wall of the orbit”.15 Although an astute and diagnostically important observation, it caused surprisingly little interest. In many ways, the fact that the phenomenon was “revived” primarily in orofacial pain and to some degree in otolaryngologic clinics is not surprising. Pain over the jaws, maxillary sinuses and adjacent structures would certainly drive patients to seek care in these specialties.
There have been several reports of migraine-like pain in the lower two-thirds of the face beginning in the 1990s.6,8,16,17 There were no clear criteria for the diagnosis and different terms were assigned such as orofacial migraine, lower half migraine, or migraine with isolated facial pain.14 Lately, with the publication of the International Classification of Orofacial Pain (ICOP), a series of migraine presenting as isolated facial pain has appeared,18 and the patients have adhered to clear diagnostic criteria. The presentation of V2 migraine is often throbbing, accompanied by mild rhinorrhea, and pain on head movement has led to extensive misdiagnosis as sinusitis. This is of significant clinical implications. Migraine patients may receive antibiotic treatment and ENT procedures unnecessarily.19–22
Facial Presentations of Primary Headache: Beyond Migraine
Benoliel et al reported 26 (47%) of 55 patients seen in an orofacial pain clinic with orofacial symptoms, diagnosable as migraine, cluster headache and paroxysmal hemicrania.6 This was followed up with cases and case series6,23–25 and together established that the TACs could, like migraine, present in the orofacial region (V2 and/or V3). These findings linked perfectly with other research reports such as “lower face cluster”,26 and reports of short-lasting unilateral neuralgiform headache with conjunctival injection and tearing (SUNCT) presenting equally in the three trigeminal dermatomes.27 In a later report, Benoliel et al reported on 328 consecutive patients seen in an orofacial pain clinic. Employing ICHD criteria, they were only able to accurately diagnose 184 (56%) of patients, including paroxysmal hemicrania, and migraines with prominent orofacial characteristics.16 This and other studies16,28,29 underscore the shortcomings of ICHD when applied to the diagnosis of orofacial pain.
In a population-based study of 517 patients with migraine, facial presentation of pain attacks were identified in 8.9% of patients;7 another study reported 6% of 973 migraine patients with isolated pain in the second trigeminal division.8 Facial pain may be more common in patients with cluster headaches (CH): Bahra and Goadsby reported that every other CH patient had been seen by a dentist, suggesting the similarities in clinical presentation. Indeed, 40% underwent (unnecessary) dental treatment, suggesting that the involvement of V2 and V3 dermatome may be more common in CH compared to migraine.30 A recent large-scaled tertiary center study confirmed this early hypothesis. Ziegeler et al investigated 2912 patients with primary headache disorders, among which 291 (10%) reported facial presentation. The prevalence of facial pain presentations differs among various primary headache diagnoses: Facial involvement was found in 2.3% in patients with migraine, and 14.8% in cluster headache or other TACs,31 suggesting that facial pain may be more common in TAC-spectrum headaches than migraine. Very recently the spectrum has been widened to cover ultra-short facial attacks reminiscent of stabbing headache disorders.32 Facial presentation of headaches can mimic idiopahitc facial pain syndromes. The topic of chronic idiopathic facial pain syndromes have been covered elsewhere.33
One problem emerged from these studies: the definition of “facial involvement” differs among studies. Some included those with headaches that extended to the V2/V3 dermatomes;7 others looked into those with pain exclusively in the V2/V3 dermatome.8 A common definition for the facial presentation of headache disorders remains missing.3 Therefore, in the recently published ICOP, a specific section (Diagnosis, orofacial pains resembling presentations of primary headaches) was dedicated to the establishment of common terminology for the facial presentation of headache disorders.34 According to ICOP, three types of facial pain presentation of headache disorders exist:
- Type 1: Headache patients with additional facial pain during the headache attacks
- Type 2: Headache patients whose headache attacks have stopped and been replaced by facial pain attacks of the same characteristics and associated symptoms
- Type 3: Headache naïve patients with de novo orofacial pain attacks that resemble primary headache types.
All these entities are interesting scientifically and diagnostically in their own right. Since ICOP was published in 2020, such differentiation has only been put in the field test in one study: Among 44 patients with a facial presentation of migraine, type 1 accounted for 86.4%, followed by type 2 (11.4%) and type 3 (2.3%). Among 63 patients with TAC (including CH), type 1 was 82.5%, followed by type 3 (17.5%), and none had type 2 phenotypes.31 Notably, the proportion of Type 3 among all patients with a facial presentation of primary headaches is based on a recent report from a headache clinic,31 but some patients may consult other specialties, such as otolaryngological practices because of the pain location.8,35 Therefore, the prevalence of type 3 orofacial pain may in fact be underestimated. Besides, type 3 patients can be difficult to demarcate from primary orofacial pain patients because of the lack of headache. Noteworthy, ICHD-3 allows facial pain to be diagnosed as a primary headache disorder if the pain otherwise fulfills the diagnostic criteria of the corresponding primary headache disorder.2 It follows that pain exclusively above the orbitomeatal line is not necessary for diagnosing a headache disorder. Therefore, both the type 1 and type 2 presentations should be coded under their corresponding headache disorders according to ICHD-32 whereas type 3 cannot easily be coded using ICHD-3. All three presentation types can be coded under ICOP, Diagnosis.34
Clinical Presentations
Common associating symptoms of primary headache disorders are also present in patients with the facial presentation of primary headache disorders, such as photo- and/or phonophobia and nausea in migraine, and cranial autonomic symptoms in facial TACs.6,17 This is not surprising since these symptoms are listed in the diagnostic criteria of the respective primary headache disorders. Without them, it is difficult to fulfill the diagnostic criteria. However, the frequency of certain accompanying symptoms, such as photo- and phonophobia, nausea, or vomiting were comparably low in migraine patients with facial pain, compared to those without facial pain, and sometimes absent in facial TACs.31 The mechanism remains unknown, but painful stimulation on the V1 dermatome increased the rating of photophobia36 and the ophthalmic (V1) branch is involved in the sensory innervation of the eyes, providing a potential link between photophobia and pain in the V1 dermatome, and this link may be missing in pain predominately in the V2 branch. It is interesting that in migraine patients with a facial presentation, the occurrence of cranial autonomic symptoms (CAS) is more common compared to those without facial presentation (47.8% vs 7.9%, p<0.001).7 CAS suggests the activation of the trigeminal-autonomic reflex and includes conjunctival injection and/or lacrimation, nasal congestion and/or rhinorrhoea, eyelid oedema, forehead and facial sweating, or miosis and/or ptosis. CAS is usually ipsilateral to the side of headache2 and is one key feature of TAC headaches, although these symptoms may also (less commonly) be present in patients with migraine, particularly when severe and unilateral.37 The high prevalence of CAS in facial pain presentations of migraine could be interpreted in that these patients share some features of TAC. Indeed, TAC patients were more likely to have facial pain presentation than migraine patients (14.8–45% vs 2.3%). In our opinion, the bidirectional association between CAS and facial pain presentation suggests a possible (specific) role of the trigeminal-autonomic reflex behind both conditions, regardless of the primary headache diagnosis. In short, primary headache patients with facial pain presentation have a somewhat different clinical presentation of the associated symptoms, which can be summarized as less migraine-like symptoms and more TAC-like symptoms.
Migraine is known to be associated with the menstrual cycle. More than 50% of female migraine patients have menstrually-associated attacks or worsening of attacks and fulfill the diagnostic criteria of menstrually-related migraine.38 A recent case report described a 47-year-old woman with paroxysmal facial pain associated with her menstruation. The pain lasted for 15–20 minutes and was accompanied by ipsilateral lacrimation and conjunctival injection. The patient responded completely to a therapeutic trial with indomethacin. A final diagnosis of facial pain presentation of paroxysmal hemicrania was given.39 An association between headache and menstruation is common in migraine but rare in other primary headache disorders such as TAC.40 Together with the exceptionally frequent CAS in migraine patients with facial pain presentation, both clinical issues may suggest that primary headache patients with facial pain presentation have a somewhat different and possibly mixed (both migraine and TAC) phenotype compared to their “pure” headache counterparts.
Another specific feature of facial presentation of headache disorders is intraoral involvement. Benoliel et al reported 29 (53%) of 55 patients with “neurovascular orofacial pain”, a term used to describe facial presentation of headache disorders with primarily intraoral pain.6 Some patients demonstrated signs that mimic dental pulpitis, including thermal allodynia or hypersensitivity of the teeth and these presentations often lead to diagnostic confusion or unnecessary therapeutic intervention.9,26 However, changes in levels of sensitivity are not specific to a disease entity but reflect an altered physiological state that may be similar to the allodynia seen in migraine patients. An aseptic neurogenic inflammation, as occurs in migraine, may also contribute to the symptoms in facial presentations of headache disorders. Central sensitization is an additional candidate for these symptoms. The proper diagnosis may be challenging: these patients should be carefully examined to exclude an intraoral pathology. Additionally, the presence of accompanying CAS may suggest a broader activation of the trigeminal nociceptive system beyond the intra-oral branches of the trigeminal nerve and provides diagnostic cues suggestive of a non-oral pathology.
Pathophysiology
The mechanisms underlying facial pain presentations of headache disorders remain unknown. One common hypothesis relies on the intracranial and extracranial innervation of the trigeminal nerves. The intracranial structures for pain perception, ie, the dura mater, are primarily innervated with the V1 branch. There is direct anatomical communication between the intra- and extracranial innervations of the trigeminal nerve: In both rat and human dura mater, some intracranial fibers leave the skull through emissary canals and fissures to innervate the periosteum and extracranial tissue such as the pericranial muscles.41 Therefore, the anatomical connection between the intracranial and extracranial fibers provides a route of how trigeminovascular activation of the dura extends to their extracranial counterpart, the V1 dermatome in the face.42 However, the dura mater in the posterior cranium is innervated by V2, V3 and cervical branches.43 Intracranial activation of V2/V3 fibers is, therefore, more likely to evoke posterior head pain whereas intracranial activation of V1 would evoke frontal headache. Extracranial activation of the trigeminal nerves may also lead to the intracranial activation of their counterparts. Neurogenic inflammation via intranasal administration of capsaicin and formalin increased plasma protein extravasation not only in the nasal mucosa but also in the dura mater.44 Based on the anatomical and functional connection between different branches of the trigeminal system, it is surprising that facial presentation of headache disorders remains so rare.
When peripheral anatomy remains insufficient to explain a low prevalence of facial pain presentation, such somatotopic segregation may be rather central. The central somatotopy of trigeminal nucleus caudalis (sTN) is onion-ring shaped with the center being the perioral region. However, fibers from the V1 branch project more to the caudal part of the trigeminal nucleus caudalis (sTN), whereas those from the V2 and V3 branches more to the rostral part of the sTN.45 This distribution also provides the anatomical basis of why cervical modulation, eg, greater occipital nerve (GON) block, may be effective in aborting headache disorders since the V1 dermatome projects to the most caudal part of the sTN and locates directly adjacent to the secondary sensory neuron of the C2/C3 branches in the spinal cord.46,47 It has recently been demonstrated that the stimulation of the V1 dermatome via capsaicin was able to modulate the pain threshold in the V2, V3, and GON dermatome; similarly, stimulation at the GON was able to change the pain threshold on all three branches of the trigeminal nerve, but with a stronger effect on V1, compared to V2/V3.48 This study provided evidence that the functional interaction between different branches of the trigeminal nerve takes place at the pontomedullary level. We have demonstrated that the functional connection between the limbic system and the ophthalmic branch exists in migraine and explains the attack-like behavior;49,50 this functional connection explains why such attack-like pains are predominately in the head.51 Following this thought the facial presentations would be a simple “spread” of the pontomedullary activation in type 1 and type 2 facial presentations of headache, whereas the isolated facial attacks resembling headaches (type 3) are due to an (extremely rare) direct functional connection between the limbic system and the maxillary or mandibular brainstem nuclei. Further studies into this subject are clearly needed.
Functional imaging studies for headache and facial pain disorders suggested possible different mechanisms behind headache and facial pain. Brain activation in the sTN via trigeminal nociception was decreased in migraine52 but increased in primary facial pain disorders (ie, persistent idiopathic facial pain),53 suggesting a role of hyperresponsive secondary sensory neurons in facial pain. Patients with an orofacial presentation of primary headache disorders have yet to be investigated using neuroimaging methods.
Diagnosis
The diagnosis of a facial presentation of primary headache disorders is based on the diagnostic criteria of the corresponding headache disorders.2,34 Of note, known associations between facial presentation and primary headache disorders stem exclusively from patient cohorts with either migraine or TAC. These types of headache disorders are well recognized/defined by their attack duration: 4–72 hours for migraine, 15–180 minutes for CH, 2–30 minutes for paroxysmal hemicrania, and 1–600 seconds for SUNCT or short-lasting unilateral neuralgiform headache attacks with cranial autonomic symptoms (SUNA).2 This non-neuralgic attack-like nature differentiates facial pain presentation of headache disorders rather easily from persistent primary facial pain disorders like persistent idiopathic facial pain or neuropathic facial pain. Notably, as a headache disorder transforms from episodic to a chronic subform, the attack may change its clinical features and duration.54 Some patients with chronic headache disorders, such as chronic migraine, may experience persistent headaches without remission, which further increases the diagnostic difficulty in those with an orofacial presentation. It is noteworthy that pain characteristics provide less power than attack length to differentiate facial presentations of primary headache disorders. For example, the presence of associated photo- and phonophobia, nausea, or vomiting provide additional diagnostic tips (for migraine) but remain relatively uncommon in the facial presentation of migraine31 and are not very specific.55 The presence of CAS usually prompts the consideration of TAC-spectrum disorders. However, as we discussed above, CAS is also disproportionally prevalent in patients with migraine and facial presentations. Diagnostic trials are not part of the diagnostic criteria for primary headache disorders with the exception of indomethacin-responsive headaches, such as paroxysmal hemicrania.2 Such specific responses have not yet been shown in facial pain disorders, possibly due to low numbers.31 The diagnosis flowchart is summarized in Figure 1.
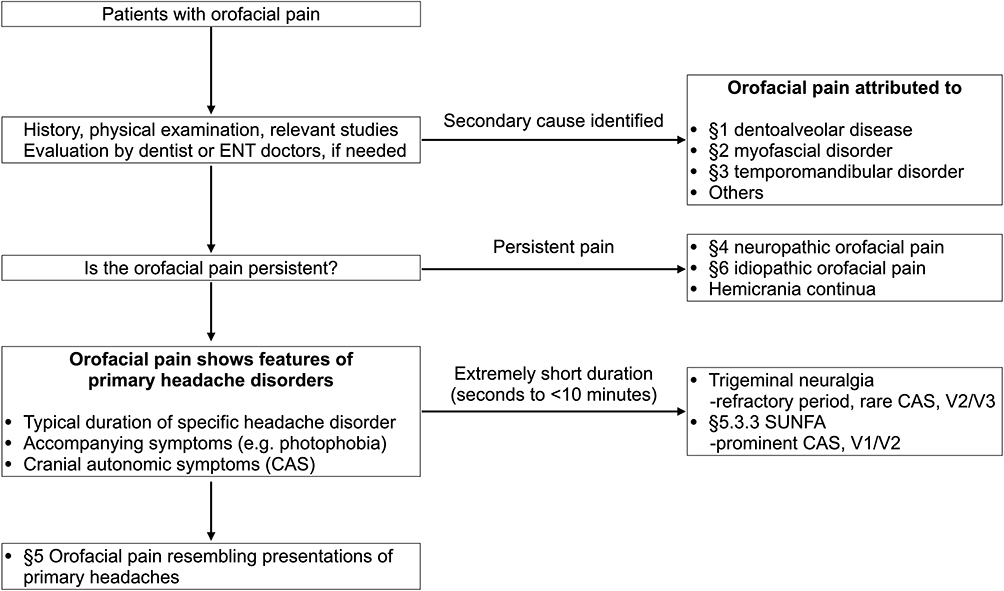 |
Figure 1 Diagnosis flowchart of orofacial pain resembling presentations of primary headaches. Abbreviations: §, corresponding chapter in the International Classification of Orofacial Pain; ENT, otorhinolaryngologist; SUNFA, short-lasting unilateral neuralgiform facial pain attacks with cranial autonomic symptoms; V1/V2/V3, first/second/third branch of the trigeminal nerve. |
Treatment
The treatment of facial pain presentation is in principle based on the primary headache diagnosis. Patients usually respond well to acute therapy used for the corresponding headache disorders. For example, in migraine patients with facial pain presentation, the attacks usually responded to triptans.31 Nonsteroidal anti-inflammatory drugs are commonly used to treat migraine and are reasonable choices in patients with facial presentations, but the individual response to a specific medication varies. In patients with CAS presentation, particularly of short duration, a trial of indomethacin may provide diagnostic insights. In one recent study, nearly all patients with a facial presentation of indomethacin-responsive TAC, eg, paroxysmal hemicrania, responded well to indomethacin.31 A thorough overview of acute treatment of migraine and cluster headache and indomethacin-responsive headaches is beyond the scope of this review and has been reviewed in detail elsewhere.56–58 Similar to acute treatment, preventive treatment for migraine and cluster headache should be effective in patients with facial pain presentations of primary headaches.57,59 Of note, a facial equivalent of medication-overuse headache was recently suggested, even though the topic remains largely under-investigated.60 Other migraine treatment options, including neurostimulation, have not been investigated in patients with facial pain presentation.
Conclusion and Future Perspective
Orofacial presentation accounts for 6–10% of patients with primary headache disorders. Proper recognition of these syndromes not only prevents unnecessary examination and treatment trials but directly benefits the patients since effective treatment is already available. Nonetheless, the understanding of the disease mechanisms remains insufficient. Neurophysiological and functional imaging studies targeting orofacial presentation of headache disorders remain lacking. Besides, calcitonin gene-related peptide (CGRP) treatments are emerging options in preventing migraine or cluster headache attacks,61,62 but their roles in facial pain disorders, both primary facial pain disorders and facial presentation of headache disorders, remain unknown. Such studies are necessary, however, since they may provide new insight into our understanding of the disease mechanisms in order to lay the foundation for future treatment possibilities.
Funding
There is no funding to report.
Disclosure
Dr Kuan-Po Peng reports personal fees from Teva Pharmaceuticals, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Stovner L, Hagen K, Jensen R, et al. The global burden of headache: a documentation of headache prevalence and disability worldwide. Cephalalgia. 2007;27(3):193–210. doi:10.1111/j.1468-2982.2007.01288.x
2. Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202
3. Ziegeler C, May A. The ICHD definition of “facial pain” should be revised. Cephalalgia. 2020;40(12):1398–1399. doi:10.1177/0333102420928080
4. Witten A, Marotta D, Cohen‐Gadol A. Developmental innervation of cranial dura mater and migraine headache: a narrative literature review. Headache. 2021;61(4):569–575. doi:10.1111/head.14102
5. Koopman JS, Dieleman JP, Huygen FJ, de Mos M, Martin CG, Sturkenboom MC. Incidence of facial pain in the general population. Pain. 2009;147(1–3):122–127. doi:10.1016/j.pain.2009.08.023
6. Benoliel R, Elishoov H, Sharav Y. Orofacial pain with vascular-type features. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;84(5):506–512. doi:10.1016/S1079-2104(97)90267-5
7. Yoon MS, Mueller D, Hansen N, et al. Prevalence of facial pain in migraine: a population-based study. Cephalalgia. 2010;30(1):92–96. doi:10.1111/j.1468-2982.2009.01899.x
8. Daudia AT, Jones NS. Facial migraine in a rhinological setting. Clin Otolaryngol Allied Sci. 2002;27(6):521–525. doi:10.1046/j.1365-2273.2002.00628.x
9. Czerninsky R, Benoliel R, Sharav Y. Odontalgia in vascular orofacial pain. J Orofac Pain. 1999;13(3):196–200.
10. Schiffman E, Ohrbach R, Truelove E, et al. Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: recommendations of the international RDC/TMD consortium network and orofacial pain special interest group. J Oral Facial Pain Headache. 2014;28(1):6–27. doi:10.11607/jop.1151
11. Exposto FG, Renner N, Bendixen KH, Svensson P. Pain in the temple? Headache, muscle pain or both: a retrospective analysis. Cephalalgia. 2021;41(14):1486–1491. doi:10.1177/03331024211029234
12. Burstein R, Cutrer MF, Yarnitsky D. The development of cutaneous allodynia during a migraine attack clinical evidence for the sequential recruitment of spinal and supraspinal nociceptive neurons in migraine. Brain. 2000;123(8):1703–1709. doi:10.1093/brain/123.8.1703
13. Hoffmann J, Baca SM, Akerman S. Neurovascular mechanisms of migraine and cluster headache. J Cereb Blood Flow Metab. 2019;39(4):573–594. doi:10.1177/0271678X17733655
14. Obermann M, Mueller D, Yoon MS, Pageler L, Diener H, Katsarava Z. Migraine with isolated facial pain: a diagnostic challenge. Cephalalgia. 2007;27(11):1278–1282. doi:10.1111/j.1468-2982.2007.01413.x
15. Wolff H. Headache and Other Head-Pain.
16. Benoliel R, Birman N, Eliav E, Sharav Y. The international classification of headache disorders: accurate diagnosis of orofacial pain? Cephalalgia. 2008;28(7):752–762. doi:10.1111/j.1468-2982.2008.01586.x
17. Peñarrocha M, Bandrés A, Peñarrocha M, Bagán JV. Lower-half facial migraine: a report of 11 cases. J Oral Maxillofac Surg. 2004;62(12):1453–1456. doi:10.1016/j.joms.2004.01.027
18. Lambru G, Elias LA, Yakkaphan P, Renton T. Migraine presenting as isolated facial pain: a prospective clinical analysis of 58 cases. Cephalalgia. 2020;40(11):1250–1254. doi:10.1177/0333102420933277
19. Eross E, Dodick D, Eross M. The Sinus, Allergy and Migraine Study (SAMS). Headache. 2007;47(2):213–224. doi:10.1111/j.1526-4610.2006.00688.x
20. Foroughipour M, Sharifian SMR, Shoeibi A, Ebdali Barabad N, Bakhshaee M. Causes of headache in patients with a primary diagnosis of sinus headache. Eur Arch Otorhinolaryngol. 2011;268(11):1593–1596. doi:10.1007/s00405-011-1643-6
21. Kari E, DelGaudio JM. Treatment of sinus headache as migraine: the diagnostic utility of triptans. Laryngoscope. 2008;118(12):2235–2239. doi:10.1097/MLG.0b013e318182f81d
22. Schreiber CP, Hutchinson S, Webster CJ, Ames M, Richardson MS, Powers C. Prevalence of migraine in patients with a history of self-reported or physician-diagnosed “sinus” headache. Arch Intern Med. 2004;164(16):1769–1772. doi:10.1001/archinte.164.16.1769
23. Benoliel R, Robinson S, Eliav E, Sharav Y. Hemicrania continua. J Orofac Pain. 2002;16(4):317–325.
24. Benoliel R, Sharav Y. Paroxysmal hemicrania. Case studies and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998;85(3):285–292. doi:10.1016/s1079-2104(98)90010-5
25. Benoliel R, Sharav Y. SUNCT syndrome: case report and literature review. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1998;85(2):158–161. doi:10.1016/s1079-2104(98)90419-x
26. Cademartiri C, Torelli P, Cologno D, Manzoni GC. Upper and lower cluster headache: clinical and pathogenetic observations in 608 patients. Headache. 2002;42(7):630–637. doi:10.1046/j.1526-4610.2002.02150.x
27. Cohen AS, Matharu MS, Goadsby PJ. Short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) or cranial autonomic features (SUNA)–a prospective clinical study of SUNCT and SUNA. Brain. 2006;129(Pt 10):2746–2760. doi:10.1093/brain/awl202
28. Zebenholzer K, Wöber C, Vigl M, Wessely P, Wöber-Bingöl C. Facial pain and the second edition of the international classification of headache disorders. Headache. 2006;46(2):259–263. doi:10.1111/j.1526-4610.2006.00304.x
29. Zebenholzer K, Wöber C, Vigl M, Wessely P, Wöber-Bingöl C. Facial pain in a Neurological Tertiary Care Centre — evaluation of the international classification of headache disorders. Cephalalgia. 2005;25(9):689–699. doi:10.1111/j.1468-2982.2004.00936.x
30. Bahra A, Goadsby PJ. Diagnostic delays and mis-management in cluster headache. Acta Neurol Scand. 2004;109(3):175–179. doi:10.1046/j.1600-0404.2003.00237.x
31. Ziegeler C, May A. Facial presentations of migraine, TACs, and other paroxysmal facial pain syndromes. Neurology. 2019;93(12):e1138–e1147. doi:10.1212/WNL.0000000000008124
32. Ziegeler C, Daneshkhah S, May A. Stabbing facial pain reminiscent of primary stabbing headache. Cephalalgia. 2020;40(10):1079–1083. doi:10.1177/0333102420923643
33. Ziegeler C, Brauns G, May A. Characteristics and natural disease history of persistent idiopathic facial pain, trigeminal neuralgia, and neuropathic facial pain. Headache. 2021;61(9):1441–1451. doi:10.1111/head.14212
34. Orofacial Pain Classification Committee. International Classification of Orofacial Pain, 1st edition (ICOP). Cephalalgia. 2020;40(2):129–221. doi:10.1177/0333102419893823
35. Agius AM, Jones NS, Muscat R. Prospective three-year follow up of a cohort study of 240 patients with chronic facial pain. J Laryngol Otol. 2014;128(6):518–526. doi:10.1017/S0022215114000929
36. Drummond PD, Woodhouse A. Painful stimulation of the forehead increases photophobia in migraine sufferers. Cephalalgia. 1993;13(5):321–324. doi:10.1046/j.1468-2982.1993.1305321.x
37. Lai TH, Fuh JL, Wang SJ. Cranial autonomic symptoms in migraine: characteristics and comparison with cluster headache. J Neurol Neurosurg Psychiatry. 2009;80(10):1116–1119. doi:10.1136/jnnp.2008.157743
38. Vetvik KG, MacGregor EA. Menstrual migraine: a distinct disorder needing greater recognition. Lancet Neurol. 2021;20(4):304–315. doi:10.1016/S1474-4422(20)30482-8
39. Ziegeler C, May A. Facial paroxysmal hemicrania associated with the menstrual cycle. Cephalalgia Rep. 2019;2:251581631985707. doi:10.1177/2515816319857070
40. Maggioni F, Palmieri A, Viaro F, Mainardi F, Zanchin G. Menstrual paroxysmal hemicrania, a possible new entity? Cephalalgia. 2007;27(9):1085–1087. doi:10.1111/j.1468-2982.2007.01374.x
41. Schueler M, Neuhuber WL, De Col R, Messlinger K. Innervation of rat and human dura mater and pericranial tissues in the parieto-temporal region by meningeal afferents. Headache. 2014;54(6):996–1009. doi:10.1111/head.12371
42. Edvinsson JCA, Viganò A, Alekseeva A, et al. The fifth cranial nerve in headaches. J Headache Pain. 2020;21(1):65. doi:10.1186/s10194-020-01134-1
43. Kemp WJ, Tubbs RS, Cohen-Gadol AA. The innervation of the cranial dura mater: neurosurgical case correlates and a review of the literature. World Neurosurg. 2012;78(5):505–510. doi:10.1016/j.wneu.2011.10.045
44. Lovrenčić L, Matak I, Lacković Z. Association of intranasal and neurogenic dural inflammation in experimental acute rhinosinusitis. Front Pharmacol. 2020;11:586037. doi:10.3389/fphar.2020.586037
45. Kamitani T. Isolated hypesthesia in the right V2 and V3 dermatomes after a midpontine infarction localised at an ipsilateral principal sensory trigeminal nucleus. J Neurol Neurosurg Psychiatry. 2004;75(10):1508–1509. doi:10.1136/jnnp.2004.038026
46. Ashkenazi A, Levin M. Greater occipital nerve block for migraine and other headaches: is it useful? Curr Pain Headache Rep. 2007;11(3):231–235. doi:10.1007/s11916-007-0195-3
47. Lambru G, Abu Bakar N, Stahlhut L, et al. Greater occipital nerve blocks in chronic cluster headache: a prospective open-label study. Eur J Neurol. 2014;21(2):338–343. doi:10.1111/ene.12321
48. Basedau H, Nielsen T, Asmussen K, et al. Experimental evidence of a functional relationship within the brainstem trigeminocervical complex in humans. Pain. 2022;163(4):729–734. doi:10.1097/j.pain.0000000000002417
49. Schulte LH, Jürgens TP, May A. Photo-, osmo- and phonophobia in the premonitory phase of migraine: mistaking symptoms for triggers? J Headache Pain. 2015;16(1):14. doi:10.1186/s10194-015-0495-7
50. Schulte LH, May A. The migraine generator revisited: continuous scanning of the migraine cycle over 30 days and three spontaneous attacks. Brain. 2016;139(Pt7):1987–1993. doi:10.1093/brain/aww097
51. May A. The exceptional role of the first division of the trigeminal nerve. Pain. 2018;159(Suppl 1):S81–S84. doi:10.1097/j.pain.0000000000001239
52. Stankewitz A, Aderjan D, Eippert F, May A. Trigeminal nociceptive transmission in migraineurs predicts migraine attacks. J Neurosci. 2011;31(6):1937–1943. doi:10.1523/JNEUROSCI.4496-10.2011
53. Ziegeler C, Schulte LH, May A. Altered trigeminal pain processing on brainstem level in persistent idiopathic facial pain. Pain. 2021;162(5):1374–1378. doi:10.1097/j.pain.0000000000002126
54. Bigal ME, Lipton RB. Clinical course in migraine: conceptualizing migraine transformation. Neurology. 2008;71(11):848–855. doi:10.1212/01.wnl.0000325565.63526.d2
55. Digre KB, Brennan KC. Shedding light on photophobia. J Neuroophthalmol. 2012;32(1):68–81. doi:10.1097/WNO.0b013e3182474548
56. Becker WJ. Acute migraine treatment in adults. Headache. 2015;55(6):778–793. doi:10.1111/head.12550
57. Hoffmann J, May A. Diagnosis, pathophysiology, and management of cluster headache. Lancet Neurol. 2018;17(1):75–83. doi:10.1016/S1474-4422(17)30405-2
58. VanderPluym J. Indomethacin-responsive headaches. Curr Neurol Neurosci Rep. 2015;15(2):516. doi:10.1007/s11910-014-0516-y
59. Schwedt TJ. Preventive therapy of migraine. Continuum. 2018;24(4):1052–1065. doi:10.1212/CON.0000000000000635
60. Debruyne F, Herroelen L. Migraine presenting as chronic facial pain. Acta Neurol Belg. 2009;109(3):235–237.
61. Diener HC, Förderreuther S, Gaul C, et al. Prevention of migraine with monoclonal antibodies against CGRP or the CGRP receptor: addition to the S1 guideline: therapy of migraine attacks and prevention of migraine. Recommendations of the Germany Society of Neurology and the German Migraine and Headache Society. Neurol Res Pract. 2020;2(1):1–6. doi:10.1186/s42466-020-00057-1
62. Yuan H, Spare NM, Silberstein SD. Targeting CGRP for the prevention of migraine and cluster headache: a narrative review. Headache. 2019;59(S2):20–32. doi:10.1111/head.13583
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.