Back to Journals » International Journal of General Medicine » Volume 18
A Retrospective Study to Determine the Preoperative Bilirubin Level for Conducting Preoperative Biliary Drainage to Reduce Pancreaticoduodenectomy Complications
Authors Chu X, Tong K, Liu K, Wu H, Li H, Liu J, Li Z, Zhang M, Guo W ![]()
Received 11 June 2025
Accepted for publication 31 October 2025
Published 7 November 2025 Volume 2025:18 Pages 6769—6781
DOI https://doi.org/10.2147/IJGM.S546424
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Xudong Zhu
Xiangyu Chu,* Kuinan Tong,* Kun Liu, Hongwei Wu, Haonan Li, Jie Liu, Zhonghao Li, Mingcheng Zhang, Wei Guo
Department of General Surgery, Beijing Friendship Hospital, Capital Medical University, State Key Laboratory of Digestive Health, National Clinical Research Center for Digestive Diseases, Beijing, 100050, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wei Guo, Email [email protected]
Background: Preoperative biliary drainage is used to alleviate obstructive jaundice before pancreaticoduodenectomy in jaundiced patients, but its effect on reducing the short-term postoperative complications is still controversial.
Methods: Data were collected retrospectively from patients (n = 292) with benign and malignant diseases around the ampulla who underwent pancreaticoduodenectomy in this study. Intergroup comparisons were performed using statistical methods such as t-tests and chi-square tests. The optimal preoperative total bilirubin was identified through receiver operating characteristic curve analysis.
Results: A total of 292 patients (jaundiced patients:141, non-jaundice:151) were collected in this study. Compared with non-jaundice patients, the incidence of postoperative bleeding events (P = 0.004), short-term complications (P = 0.038), and severe short-term complications (P = 0.025) was significantly increased in jaundiced patients. The incidence of short-term postoperative complications in patients with severe jaundice was not statistically different from that in patients with mild jaundice after preoperative biliary drainage. In patients with mild jaundice, there was no statistically significant difference between the direct surgery group and the preoperative biliary drainage group. When the preoperative total bilirubin in preoperative biliary drainage patients decreased to 151.8μmol/L, the incidence of severe short-term postoperative complications was significantly reduced (P = 0.047).
Conclusion: Preoperative biliary drainage can effectively improve liver function and decrease the short-term complications after pancreaticoduodenectomy for severe jaundiced patients. Routine preoperative biliary drainage is not recommended in patients with mild jaundice. It is recommended to reduce the total bilirubin to less than 151.8μmol/L, which can effectively decrease the severe short-term postoperative complications.
Keywords: pancreaticoduodenectomy, jaundice, preoperative biliary drainage, postoperative complications, target total bilirubin
Introduction
Pancreatic duodenectomy (PD) is the standard surgical procedures for treating benign and malignant diseases around the ampulla. PD is known for its extensive surgical resection, complex gastrointestinal reconstruction, and difficult postoperative management. Short-term complications after PD surgery include clinically relevant pancreatic fistula (CR-POPF), biliary leak, postoperative bleeding, postoperative infection, delayed gastric emptying (DGE), etc.1,2 The incidence of CR-POPF is reported to between 10% and 25.9%.3 Once short-term complications occur after PD surgery, it will seriously affect the patient’s prognosis. Therefore, it’s necessary to identify how to prevent and decrease the postoperative short-term complications before surgery.
Patients with benign and malignant diseases around the ampulla often suffered from the obstructive jaundice, and severe obstructive jaundice can affect the patient’s liver and kidney function, leading to pathological and physiological changes such as coagulation dysfunction, hypoalbuminemia, and decreased immunity, which can increase the incidence of short-term postoperative complications.4 Preoperative biliary drainage (PBD) is the common treatment for obstructive jaundice in clinical practice. Although PBD can alleviate obstructive jaundice, there is controversy over whether PBD should be performed routinely before PD in patients with obstructive jaundice. The current mainstream PBD methods include percutaneous transhepatic cholangial drainage (PTCD), endoscopic nasobiliary drainage (ENBD), and endoscopic retrograde biliary drainage (ERBD). All involve invasive procedures and carry the risk of infection associated with drainage tubes. The traditional opinion is that patients with total bilirubin (TB) below 250 μmol/L do not need to undergo PBD because it increases the risk of infectious complications.5–7 Some studies have shown that PBD can provide benefits such as improving liver function, restoring physiological mechanisms of obstructive jaundice changes, and increasing patient tolerance to surgery.8–12 On the contrary, other studies have reported postoperative adverse outcomes, including CR-POPF and even patient mortality.13–15
In the previous studies, ERBD or ENBD were predominantly preferred PBD approaches, with a typical duration of approximately 4 weeks for jaundice relief. This approach is somewhat inconsistent with the current clinical landscape in China. In China, PTCD holds a place as a method of PBD. Moreover, to prevent tumor progression to an unresectable state, surgery is typically performed around 2 weeks after PBD. The differing disease spectrum necessitates new research to validate more appropriate PBD strategies. Moreover, current research has not yet definitively identified an appropriate PBD endpoint. Therefore, this study intends to retrospectively analyze whether PBD can reduce short-term postoperative complications and the target TB of PBD in patients with obstructive jaundice undergoing PD.
Materials and Method
Research Object
This study retrospectively collected patients who underwent PD at Capital Medical University Affiliated Beijing Friendship Hospital from January 1, 2016, to January 31, 2022. The research plan has been approved by the Bioethics Committee of Capital Medical University Affiliated Beijing Friendship Hospital, with ethics approval number 2025-P2-118-01. The research flowchart is shown in Figure 1.
 |
Figure 1 The cohort of the study. |
Inclusion Criteria
(1) Benign and malignant diseases around the Vater ampulla: including malignant tumors of the pancreatic head, distal bile duct, duodenum papilla and Vater ampulla; Intraductal papillary mucinous malignant tumor, as well as chronic pancreatitis; (2) No metastasis to distant organs as confirmed by preoperative evaluation; (3) Clear pathological diagnosis and complete clinical data.
Exclusion Criteria
(1) Preoperative neoadjuvant therapy; (2) Combined with other organ resections; (3) Patients with repeated PBD.
Clinical Information Collection
Demographic Information: gender, age, body mass index (BMI), chronic comorbidities (such as diabetes and hypertension).
Preoperative laboratory tests: preoperative hemoglobin (HGB), preoperative and pre-PBD biochemical indicators (including alanine aminotransferase, TB), preoperative coagulation indicators (prothrombin time and activated partial thromboplastin time).
Clinical information: whether biliary drainage was performed, the method of biliary drainage, the duration of biliary drainage, the duration of surgery, the method of surgery, the amount of bleeding, and the occurrence of short-term postoperative complications.
Observation outcome: The main observation outcome is the occurrence of short-term postoperative complications (Clavien Dindo grade I or above), and the secondary observation outcome is severe short-term postoperative complications (Clavien Dindo grade III or above), CR-POPF, postoperative bleeding events (including abdominal or gastrointestinal bleeding), and postoperative biliary leak. Observation period until the patient completes postoperative recovery and is discharged.
Diagnostic Criteria
According to the current mainstream view of relevant research, patients with the highest TB during preoperative course between 34.2 and 250μmol/L are defined as mild jaundice, while those exceeding 250μmol/L are defined as severe jaundice.5–7 According to the postoperative laboratory tests and course records of the patient, the Clavien Dindo classification of complications was performed. A grade I or higher was considered as the occurrence of complications, while a grade III or higher was considered as the occurrence of severe complications.16 Postoperative biliary leak is defined by the International Group of Liver Surgeons (ISGLS) as a condition where the bilirubin concentration in the drainage material is at least three times the normal serum bilirubin concentration at least 3 days after surgery, or intervention or surgical treatment is required due to bile aggregation or biliary peritonitis. Specific clinical manifestations include unexplained perihepatic fluid accumulation, peritonitis stimulation, or bile-like ascites visible in puncture drainage fluid.17 According to the definition of postoperative pancreatic fistula by the International Group of Pancreatic Surgeons (ISGPS) in 2016, if the amylase concentration in the drainage material is at least three times that of the serum amylase concentration at least 3 days after surgery, and whether it affects the normal clinical course of the patient, it is divided into grades A, B, and C18. Of these, classes B and C are CR-POPF. According to the ISGPS, postoperative gastric emptying delay is defined as the need for or re-insertion of a nasogastric tube on the third day after surgery or failure to resume oral diet on the seventh day after surgery.19 Postoperative infections include abdominal infection, thoracic infection, or combined infection, and the diagnostic criteria are clear imaging findings of pleural effusion and ascites accompanied by elevated infection indicators or positive pathogen culture in body fluids.
Surgical Procedure
All PD procedures are performed by our center’s experienced pancreatic surgeon (W.G). Open or laparoscopic PD is performed on patients. The conventional resection range includes the distal stomach, duodenum, gallbladder, common bile duct, partial jejunum, and regional lymph nodes. Child reconstruction is performed on the digestive tract, and the biliary pancreatic loop is reconstructed in the posterior position of the colon. Pancreatic intestinal anastomosis is a continuous mucosal to mucosal end-to-end anastomosis, in which a stent tube is routinely inserted into the pancreatic duct. Bile intestinal anastomosis involves continuous outward rotation of the anterior and posterior walls, while gastrointestinal anastomosis is performed using a stapler. During the operation, drainage tubes are routinely placed next to the biliary enteric anastomosis and pancreatic enteric anastomosis, and in some patients, drainage tubes are placed next to the gastrointestinal anastomosis. All surgeries are performed by experienced pancreatic surgeons.
Statistical Methods
According to a previous randomized controlled trial study, the overall complication rate was 74% in the PBD group and 39% in the direct surgery group.5 Using the sample size calculation formula for retrospective cohort studies, with a Type I error (α) of 0.05, power of 0.8, a 1:1 group ratio, and a two-tailed test, the required sample size per group was calculated to be 31. To avoid bias from confounding factors, we conducted subgroup analyses based on different clinical issues (such as mild jaundice subgroup and PBD subgroup). SPSS V27.0 (IBM Corp, Armonk, NYS, USA) was used for data analysis.
The quantitative data is subjected to normality test, and the quantitative data that conforms to the normality distribution is described by mean ± standard deviation. T-test is applied for difference analysis. The quantitative data of non-normal distribution is described using the median (1st quartile, 3rd quartile). Qualitative data is described using examples (percentages). Nonparametric rank sum test (Mann Whitney test) is applied to skewed quantitative data and ordered qualitative data, while chi-square test is used to analyze differences in unordered qualitative data. If the ideal frequency is too low, Fisher’s exact probability method is used.
Clinical characteristics with significant results in univariate binary logistic regression were incorporated into multivariate binary logistic regression. The regression method employed input variables, with an entry probability of 0.05, an exit probability of 0.10, a classification cutoff value of 0.5, and a maximum iteration count of 20. P-values less than 0.050 were statistically significant.
The ROC curve is used to identify an appropriate cut-off value. Specifically, by predicting the occurrence of short-term severe postoperative complications using preoperative total bilirubin levels, the specificity and sensitivity at each point are determined. The Youden index is then calculated, with the maximum Youden index value representing the optimal cut-off point.
Youden Index = Sensitivity + Specificity − 1
Results
Clinical Characteristics of the Patients
Total 292 patients who underwent PD at Beijing Friendship Hospital affiliated with Capital Medical University from January 1, 2016, to January 31, 2022, were included in this study. The clinical characteristics are summarized in Table 1. The incidence of jaundice in patients is about 48.3%, and the methods of PBD are PTCD (31.9%), ENBD (28.4%) and ERBD (7.8%). The main surgical method was open surgery (177/292, 60.6%), and percentage of laparoscopic transfer opening was 7.9% (23/292), while the percentage of laparoscopic surgery was 31.5% (92/292). Postoperative pathological examination indicated that 79 (27.1%) were diagnosed as the malignant tumors of the common bile duct, 56 (19.2%) were diagnosed as the Vater’s ampullary carcinoma, 56 (19.2%) were diagnosed as the intraepithelial neoplasia, and 31 (10.6%) patients were diagnosed as pancreatic adenocarcinoma. Overall, 164 of 292 (56.2%) patients experienced short-term complications, and 42 of 292 (14.4%) patients experienced severe short-term postoperative complications. The incidence of CR-POPF was 20.2%, the incidence of biliary leak was 7.9%, and the perioperative mortality rate was 3.1%.
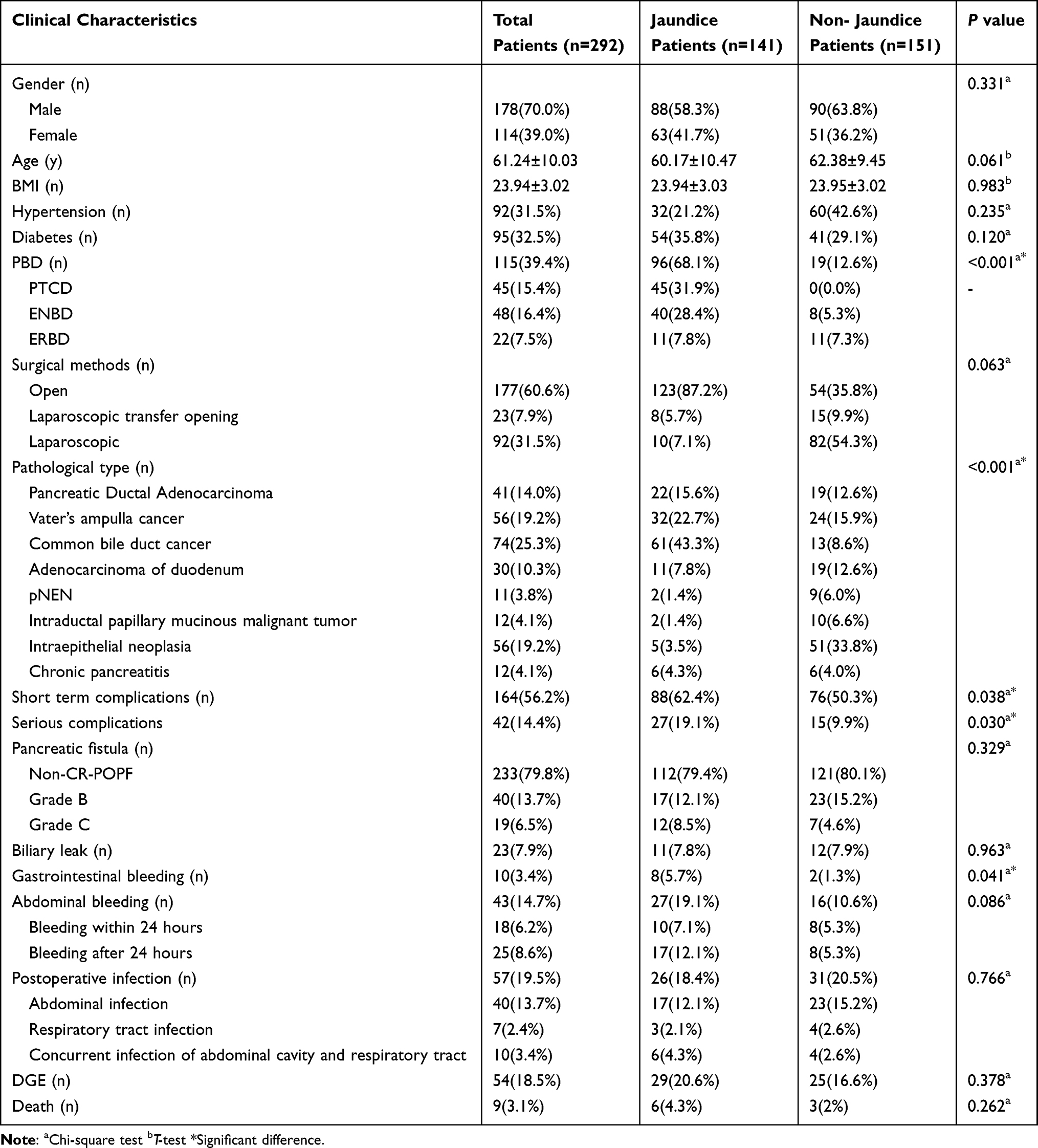 |
Table 1 Clinical Characteristics of Patients |
The Impact of Preoperative Jaundice on Short-Term Postoperative Complications
We conducted univariate binary logistic regression analysis on the clinical features before and during surgery. The clinical features with P-values less than 0.050 were included in the multivariate binary logistic regression analysis. The results showed that severe jaundice (P = 0.043) and male (P = 0.042) were independent risk factors for short-term severe postoperative complications (Table 2). Subsequently, patients were divided into jaundice group (n = 141) and non-jaundice group (n = 151) based on whether the preoperative TB was greater than 34.2μmol/L. The comparison of preoperative baseline data of patients showed significant differences in preoperative TB (P < 0.001), preoperative alanine aminotransferase (ALT, P < 0.001), preoperative albumin (ALB, P < 0.001), and preoperative HGB (P < 0.000) (Table S1). There were no significant differences in age, preoperative coagulation function, duration of surgery, and surgical methods. This indicates that jaundiced patients have poorer liver function, poorer nutritional status, and higher surgical risks compared to those without jaundice. The complications results showed that the jaundiced patients were easy to suffer from the postoperative bleeding events (P = 0.004), short-term complications (P = 0.038), and severe short-term complications (P = 0.025) (Table 3). Therefore, it’s necessary to PBD to reduce the short-term postoperative complications after PD.
 |
Table 2 Univariate and Multivariate Binary Logistic Regression to Identify Risk Factors for Short-Term Severe Postoperative Complications |
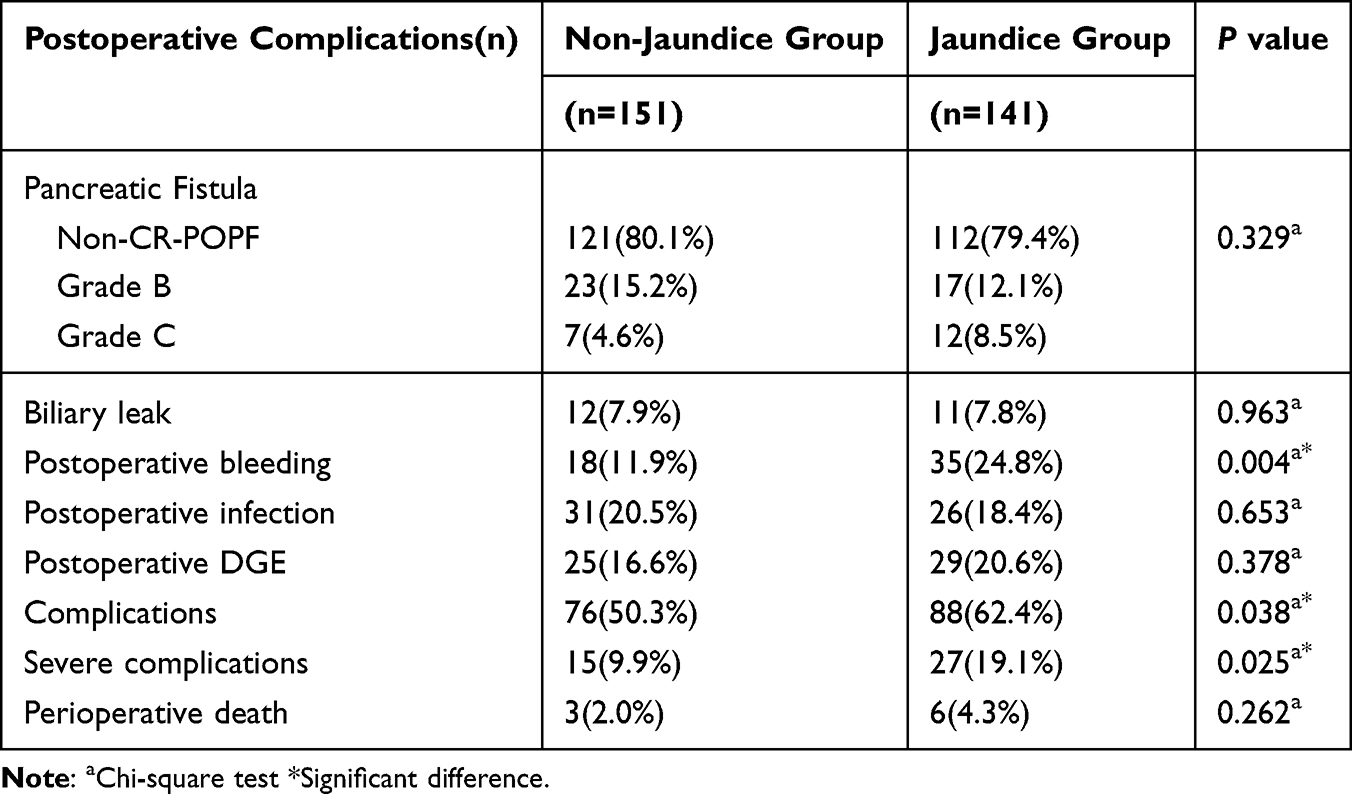 |
Table 3 Comparison of Short-Term Postoperative Complications Between Non-Jaundice Group and Jaundice Group |
The 141 jaundiced patients were divided into mild jaundice group (n = 85) and severe jaundice group (n = 56) based on whether the highest TB exceeded 250μmol/L, to further investigate the impact of severity of jaundice on short-term postoperative complications. The comparison of preoperative clinical data between the mild jaundice group and the severe jaundice group is shown in Table 4. The results show that there are significant differences in the highest TB (P < 0.001), preoperative TB (P < 0.001), preoperative HGB (P = 0.024), preoperative PT (P = 0.001), and whether there is PBD (P < 0.001). However, patients with severe jaundice have better preoperative liver function (P = 0.003) (Table S2). The finding is indeed counter-intuitive but can be explained by the differential application of PBD. The key is to distinguish between the severity of the initial obstruction and the functional state of the liver at the time of surgery. The severe jaundice group, due to their critical condition, underwent PBD much more frequently (89.3% vs 54.1% in the mild jaundice group, P < 0.001). This intervention effectively reversed the ongoing hepatocellular injury, leading to a marked improvement in ALT levels. Consequently, by the time of surgery, their liver function had recovered to a degree that surpassed that of the mild jaundice group. As shown in Table S3, there was no significant difference in the incidence of short-term postoperative complications between the two groups, which indicated that patients with severe jaundice could benefit from the PBD. This observation underscores the potent reversibility of obstructive liver injury and highlights the benefit of PBD in optimizing preoperative status in severely jaundiced patients.
 |
Table 4 Comparison of Short-Term Postoperative Complications Between Direct Surgery Group and PBD Group in Mild Jaundiced Patients |
The Relationship Between Preoperative Biliary Drainage and Postoperative Complications in Jaundiced Patients
In order to investigate whether PBD brings significant benefits to jaundiced patients, the subgroup of jaundiced patients was divided into the direct surgery group (n = 45) and the PBD group (n = 96). The comparison of preoperative baseline data showed significant differences in age (P = 0.005), highest TB (P < 0.001), and preoperative ALT (P < 0.001) (Table S4). The majority of patients in the preoperative biliary drainage group have severe jaundice, and PBD can effectively alleviate the preoperative ALT of jaundice patients, which was even better than direct surgery patients. The results showed no significant difference in the occurrence of short-term postoperative complications (Table S5), which indicated that jaundiced patients could benefit from the effective PBD, especially severe jaundice patients.
To identify the controversial issue that whether mild jaundice patients need the PBD, the mild jaundice patients were divided into the mild direct surgery group (n = 39) and mild PBD group (n = 46). The results showed significant differences in age (P = 0.022) and preoperative ALT (P = 0.001) (Table S6). There exists no significant difference between two groups on the postoperative complications (Table 4). PBD in patients with mild jaundice relieves preoperative ALT but does not reduce the complication rate and is not recommended routinely.
Identity the Optimal Target Preoperative Total Bilirubin in Preoperative Biliary Drainage Patients
To investigate the optimal target preoperative TB, we conducted a subgroup analysis on 86 patients who underwent PBD (10 patients were excluded because their pre-PBD biochemical data could not be obtained due to PBD performed at other hospitals). The ROC curve of preoperative TB was drawn based on the occurrence of severe short-term postoperative complications and calculated the Youden index for each preoperative TB. The results showed that the maximum Youden index was obtained when the preoperative TB was 151.8μmol/L, with the Youden index of 0.266 (Figure 2). When the preoperative TB was more than 151.8 μ mol/L, the sensitivity to predict the occurrence of severe complications was 57.9%, and the specificity was 68.7%. The 151.8μmol/L was set as the cut-off value to divide the patients with PBD into two groups: the ineffective PBD group (n = 33) and the effective PBD group (n = 53). The results showed the highest TB (P = 0.001) in the ineffective PBD group was higher than the effective PBD group (Table 5). Patients in the ineffective PBD group had a higher risk of developing severe short-term postoperative complications (P = 0.047) (Table 6), which supported the feasibility of the cut-off value for the preoperative TB.
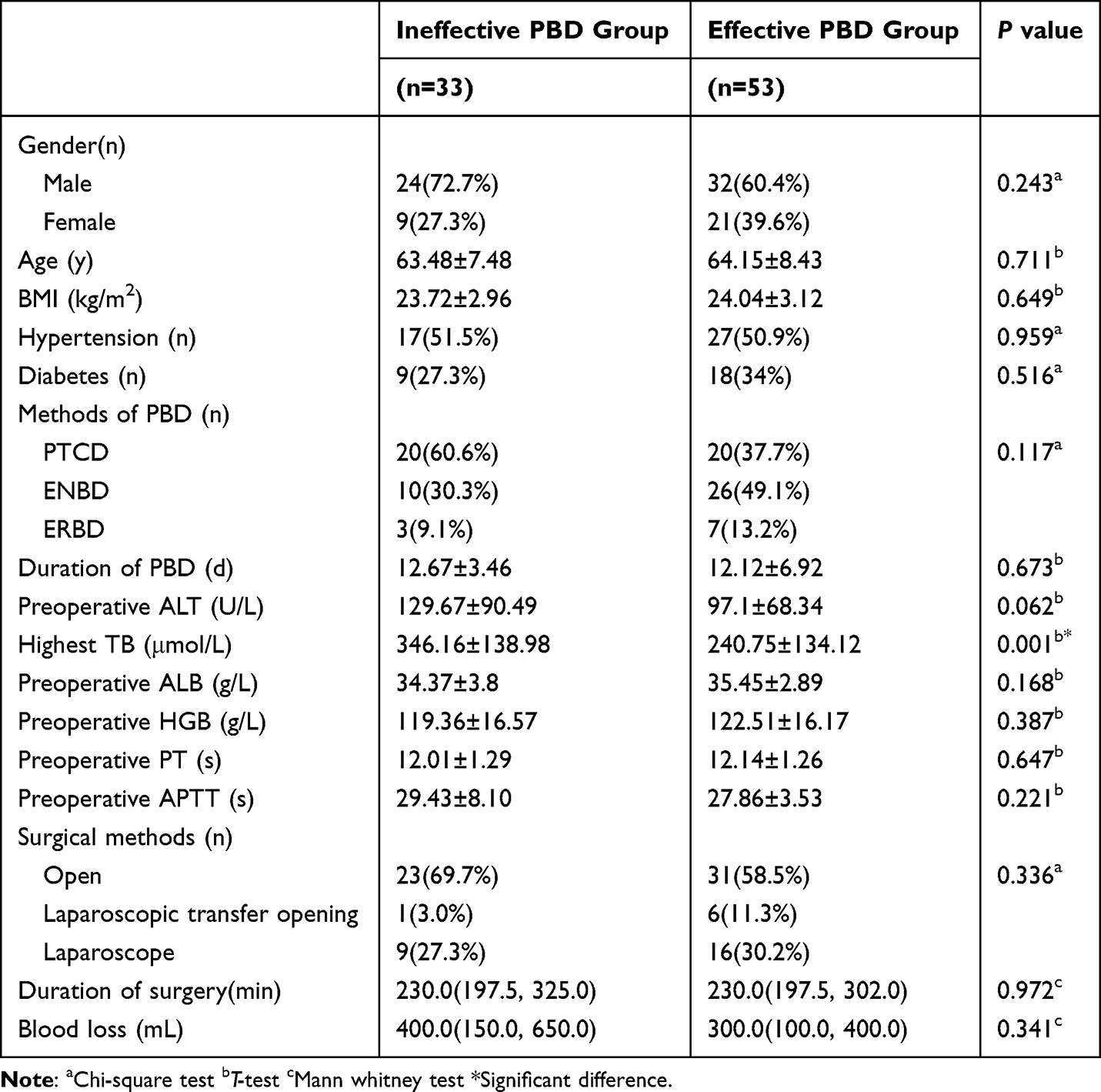 |
Table 5 Preoperative Baseline Data of Ineffective PBD Group and Effective PBD Group |
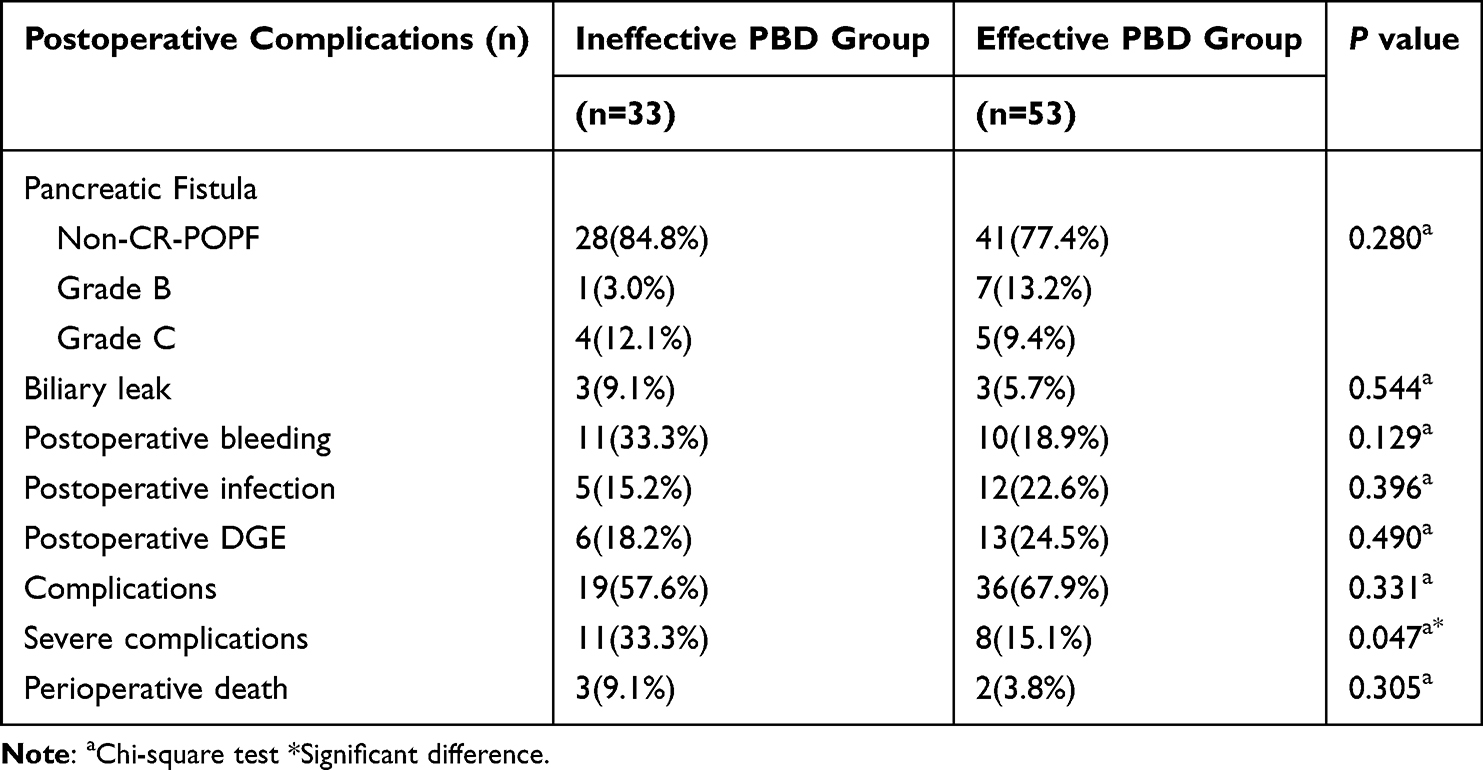 |
Table 6 Comparison of Short-Term Postoperative Complications Between Ineffective PBD Group and Effective PBD Group |
 |
Figure 2 The ROC curve of preoperative total bilirubin to predict the occurrence of severe complications. |
Discussion
The hydrostatic pressure inside the human bile duct is 5–10 cmH2O, and the internal pressure gradually increases as the tumor obstructs the outflow tract of the bile duct.20 When the hydrostatic pressure in the bile duct rises to 15–30cm H2O, liver cells will gradually stop secreting bile due to impaired function, resulting in increased aminotransferase, elevated serum bilirubin, and induction of liver cell apoptosis.20 High bile salt can inhibit the activity of liver cytochrome P450, thereby inducing inflammatory response and liver cell apoptosis, affecting the liver and systemic immune response.21 It is confirmed that the function of kupffer cells in jaundiced patients is impaired, and the function can be restored when the obstruction is relieved.22 Patients with obstructive jaundice are prone to postoperative infections due to three major factors: abnormal immune function, bacterial translocation, and damage to the intestinal mucosal barrier.23 Obstructive jaundice can lead to pathological and physiological changes such as hypoalbuminemia, coagulation dysfunction, decreased liver reserve function, and kidney dysfunction in patients, which can affect the occurrence of surgical complications.4
Given these pathophysiological consequences, PBD has been employed to alleviate obstructive jaundice before PD in jaundiced patients. However, its effect on reducing short-term postoperative complications remains controversial. Some studies suggest that even with severe jaundice, PBD may not be necessary. A case-control study showed that PBD in patients with severe jaundice (TB exceeding 15 mg/dl) increased the incidence of postoperative abdominal infection (P = 0.020), prolonged surgical duration (P < 0.001), and intraoperative bleeding (P = 0.002).24 Another research suggests that direct surgery can reduce the incidence of postoperative incision infection (P < 0.001) and infectious ascites (P = 0.040), and severe preoperative jaundice does not seem to be a risk factor for postoperative complications.25 In contrast, our study provides evidence supporting the utility of PBD in a specific patient population.
However, a retrospective study in China included 200 patients with severe jaundice and found that direct surgery for severe jaundice increased the incidence of postoperative complications (P = 0.005), bleeding events (P = 0.032), and CR-POPF (P = 0.045).26 Our findings clearly demonstrate that obstructive jaundiced patients have decreased preoperative liver function, poorer nutritional status, and higher anesthesia risk. They are more likely to experience postoperative bleeding events (P = 0.004), short-term complications (P = 0.038), and severe short-term complications (P = 0.025). Severe jaundice is an independent risk factor for severe short-term postoperative complications, and effective PBD can significantly alleviate preoperative liver function and reduce postoperative complications for severe jaundice.
Having established the value of PBD for patients with severe jaundice, we next sought to determine if this benefit extends to patients with only mild jaundice. The current controversial issue is the PBD strategy for the mild jaundice patients with preoperative TB ranging from 34.2 to 250 μmol/L. A randomized controlled trial from the Netherlands showed that for patients with mild jaundice, PBD increases the overall risk of complications (P < 0.001), with PBD-related complications being the main cause.5 In our study, PBD in patients with mild jaundice relieves preoperative ALT but does not reduce the complication rate and is not recommended routinely. However, PBD may be performed at the discretion of some patients with special conditions (long preoperative preparation time or rapid progression of jaundice), as it does not cause adverse postoperative complications.
Beyond identifying which patient subgroups benefit from PBD, our study further provides a definable objective for the procedure. The PBD treatment for patients with severe obstructive jaundice has gradually become standardized, but there exists no clinical research to identify the optimal efficacy jaundice should be reduced before surgery. This study found that the incidence of severe postoperative complications was lower in patients with PBD who had preoperative TB reduced to below 151.8μmol/L (P = 0.047).
The rationale for this specific threshold may be partially explained by the need for sufficient time to restore physiological function. In this study, the PT (P = 0.001) of patients with severe jaundice was longer than that of patients with mild jaundice, at the upper limit of normal (12.42 ± 1.4s), but there was no difference in intraoperative bleeding and postoperative complications. This reveals the problem that current clinical indicators may not truly reflect the coagulation, nutritional and immune status of patients after PBD. The current view that PBD requires at least 4 weeks, which is necessary to fully restore the patient’s liver function, originates from an animal study.5,27,28 However, it is worth thinking about how long we need to PBD before surgery. Our previous study has already suggested that duration of PBD longer than 2 weeks will increase the rate of complications and serious complications.7 Prolonged PBD also leads to a risk of tumor progression.29 More studies are needed to investigate the appropriate biomarkers or scoring system to guide the end of PBD.
Finally, it is important to consider how the specific PBD method might influence outcomes, as this could explain discrepancies between our findings and some previous studies. The reason why this conclusion differs from previous research findings may be related to the methods of PBD. In our center, ENBD and ERBD accounted for 53.1%, and PTCD accounted for 46.9%. The proportion of PTCD was higher than in other studies. Although ERBD can ensure the flow of bile to the intestine and restore normal physiological structure, it also has drawbacks, such as damage to the papillary muscles during endoscopic procedures and the risk of intestinal fluid reflux and bacterial translocation caused by stent placement. In addition, due to the biliary stent, continuous stimulation of the end of the bile duct can lead to inflammatory reactions in the surrounding area, which may have an impact on the PD surgical area and may be more likely to cause postoperative complications. This viewpoint has been verified by animal experiments, and our center has also found this clinical phenomenon.30 A study has shown that PTCD, as a PBD method for obstructive jaundice, can reduce intraoperative bleeding and the incidence of postoperative complications.31 Another meta-analysis shows that PTCD has a lower incidence of PBD-related complications (P = 0.010) and postoperative complications (P = 0.020) compared to ENBD and ERBD.32
This study also has certain limitations. Although our study met the minimum sample size requirement, it must be acknowledged that the sample size was insufficient. Consequently, we were unable to specifically explore the advantages and disadvantages of PTCD, ENBD, and ERBD as three distinct PBD methods. Moreover, this study was unable to further investigate the impact of PBD on long-term prognosis through follow-up. As this is a retrospective study, it inevitably involves certain confounding factors and suffers from missing data due to incomplete hospital records. High-capacity, multicenter prospective studies are needed to further optimize preoperative PBD strategies for patients with jaundice undergoing PD.
Conclusion
In conclusion, this retrospective study demonstrates that obstructive jaundice significantly increases the risk of postoperative bleeding and severe complications following pancreaticoduodenectomy. Preoperative biliary drainage effectively mitigates this risk in patients with severe jaundice (TB > 250 μmol/L) by improving liver function, whereas routine PBD is not supported for patients with mild jaundice (TB 34.2–250 μmol/L) as it did not reduce complication rates. Crucially, our study proposes a specific preoperative TB level of 151.8 μmol/L as a potential target. The data demonstrate that reducing TB below this threshold before surgery is associated with a significant decrease in severe postoperative complications. These findings support a PBD strategy, recommending its application in severely jaundiced patients with the objective of reducing TB to <151.8 μmol/L to optimize surgical outcomes.
Acknowledgment
None
Ethics Statement
The studies involving humans were approved by Bioethics Committee of Capital Medical University Affiliated Beijing Friendship Hospital (ethics approval number: 2025-P2-118-01). This study complies with the Declaration of Helsinki. Research conducted in this study was in accordance with local regulations and institutional requirements. The written informed consent of the participants was provided in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the “Seed Program” in Beijing Friendship Hospital Affiliated Capital Medical University (No.YYZZ202419), National Key Technologies R&D Program (No. 2015BAI13B09) and National Key Clinical Specialist Construction Programs.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Simon R. Complications after pancreaticoduodenectomy. Surg Clin North Am. 2021;101(5):865–874. doi:10.1016/j.suc.2021.06.011
2. Wang M, Cai H, Meng L, et al. Minimally invasive pancreaticoduodenectomy: a comprehensive review. Int J Surg. 2016;35:139–146. doi:10.1016/j.ijsu.2016.09.016
3. Russell TB, Aroori S. Procedure-specific morbidity of pancreatoduodenectomy: a systematic review of incidence and risk factors. ANZ J Surg. 2022;92(6):1347–1355. doi:10.1111/ans.17473
4. Liu JJ, Sun Y-M, Xu Y, et al. Pathophysiological consequences and treatment strategy of obstructive jaundice. World J Gastrointest Surg. 2023;15(7):1262–1276. doi:10.4240/wjgs.v15.i7.1262
5. van der Gaag NA, Rauws EAJ, van Eijck CHJ, et al. Preoperative biliary drainage for cancer of the head of the pancreas. N Engl J Med. 2010;362(2):129–137. doi:10.1056/NEJMoa0903230
6. De Pastena M, Marchegiani G, Paiella S, et al. Impact of preoperative biliary drainage on postoperative outcome after pancreaticoduodenectomy: an analysis of 1500 consecutive cases. Dig Endosc. 2018;30(6):777–784. doi:10.1111/den.13221
7. Wang D, Lin H, Guan C, et al. Impact of preoperative biliary drainage on postoperative complications and prognosis after pancreaticoduodenectomy: a single-center retrospective cohort study. Front Oncol. 2022;12:1037671. doi:10.3389/fonc.2022.1037671
8. Gouma DJ, Coelho JCU, Fisher JD, et al. Endotoxemia after relief of biliary obstruction by internal and external drainage in rats. Am J Surg. 1986;151(4):476–479. doi:10.1016/0002-9610(86)90107-8
9. Kawasaki S, Imamura H, Kobayashi A, et al. Results of surgical resection for patients with hilar bile duct cancer: application of extended hepatectomy after biliary drainage and hemihepatic portal vein embolization. Ann Surg. 2003;238(1):84–92. doi:10.1097/01.SLA.0000074984.83031.02
10. Roughneen PT, Gouma DJ, Kulkarni AD, et al. Impaired specific cell-mediated immunity in experimental biliary obstruction and its reversibility by internal biliary drainage. J Surg Res. 1986;41(2):113–125. doi:10.1016/0022-4804(86)90016-8
11. Abdullah SA, Gupta T, Jaafar KA, et al. Ampullary carcinoma: effect of preoperative biliary drainage on surgical outcome. World J Gastroenterol. 2009;15(23):2908–2912. doi:10.3748/wjg.15.2908
12. Kloek JJ, Heger M, van der Gaag NA, et al. Effect of preoperative biliary drainage on coagulation and fibrinolysis in severe obstructive cholestasis. J Clin Gastroenterol. 2010;44(9):646–652. doi:10.1097/MCG.0b013e3181ce5b36
13. Greig JD, Krukowski ZH, Matheson NA. Surgical morbidity and mortality in one hundred and twenty-nine patients with obstructive jaundice. Br J Surg. 1988;75(3):216–219. doi:10.1002/bjs.1800750309
14. Sewnath ME, Karsten TM, Prins MH, et al. A meta-analysis on the efficacy of preoperative biliary drainage for tumors causing obstructive jaundice. Ann Surg. 2002;236(1):17–27. doi:10.1097/00000658-200207000-00005
15. Singhirunnusorn J, Roger L, Chopin-Laly X, et al. Value of preoperative biliary drainage in a consecutive series of resectable periampullary lesions. From randomized studies to real medical practice. Langenbecks Arch Surg. 2013;398(2):295–302. doi:10.1007/s00423-012-1000-2
16. Téoule P, Bartel F, Birgin E, et al. The clavien-dindo classification in pancreatic surgery: a clinical and economic validation. J Invest Surg. 2019;32(4):314–320. doi:10.1080/08941939.2017.1420837
17. Koch M, Garden OJ, Padbury R, et al. Bile leakage after hepatobiliary and pancreatic surgery: a definition and grading of severity by the international study group of liver surgery. Surgery. 2011;149(5):680–688. doi:10.1016/j.surg.2010.12.002
18. Bassi C, Marchegiani G, Dervenis C, et al. The 2016 update of the International Study Group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 years after. Surgery. 2017;161(3):584–591. doi:10.1016/j.surg.2016.11.014
19. Wente MN, Bassi C, Dervenis C, et al. Delayed gastric emptying (DGE) after pancreatic surgery: a suggested definition by the International Study Group of Pancreatic Surgery (ISGPS). Surgery. 2007;142(5):761–768. doi:10.1016/j.surg.2007.05.005
20. Pavlidis ET, Pavlidis TE. Pathophysiological consequences of obstructive jaundice and perioperative management. Hepatobiliary Pancreat Dis Int. 2018;17(1):17–21. doi:10.1016/j.hbpd.2018.01.008
21. Fukushima S, Okuno H, Shibatani N, et al. Effect of biliary obstruction and internal biliary drainage on hepatic cytochrome P450 isozymes in rats. World J Gastroenterol. 2008;14(16):2556–2560. doi:10.3748/wjg.14.2556
22. Okaya T, Nakagawa K, Kimura F, et al. The alterations in hepatic microcirculation and Kupffer cell activity after biliary drainage in jaundiced mice. J Hepatobiliary Pancreat Sci. 2012;19(4):397–404. doi:10.1007/s00534-011-0435-0
23. Assimakopoulos SF, Tsamandas AC, Louvros E, et al. Intestinal epithelial cell proliferation, apoptosis and expression of tight junction proteins in patients with obstructive jaundice. Eur J Clin Invest. 2011;41(2):117–125. doi:10.1111/j.1365-2362.2010.02379.x
24. Arkadopoulos N, Kyriazi MA, Papanikolaou IS, et al. Preoperative biliary drainage of severely jaundiced patients increases morbidity of pancreaticoduodenectomy: results of a case-control study. World J Surg. 2014;38(11):2967–2972. doi:10.1007/s00268-014-2669-x
25. Pamecha V, Sadashiv Patil N, Kumar S, et al. Upfront pancreaticoduodenectomy in severely jaundiced patients: is it safe? J Hepatobiliary Pancreat Sci. 2019;26(11):524–533. doi:10.1002/jhbp.671
26. Shen Z, Zhang J, Zhao S, et al. Preoperative biliary drainage of severely obstructive jaundiced patients decreases overall postoperative complications after pancreaticoduodenectomy: a retrospective and propensity score-matched analysis. Pancreatology. 2020;20(3):529–536. doi:10.1016/j.pan.2020.02.002
27. Yang F, Jin C, Zou C, et al. Delaying surgery after preoperative biliary drainage does not increase surgical morbidity after pancreaticoduodenectomy. Surgery. 2019;166(6):1004–1010. doi:10.1016/j.surg.2019.07.012
28. Koyama K, Takagi Y, Ito K, et al. Experimental and clinical studies on the effect of biliary drainage in obstructive jaundice. Am J Surg. 1981;142(2):293–299. doi:10.1016/0002-9610(81)90296-8
29. Sanjeevi S, Ivanics T, Lundell L, et al. Impact of delay between imaging and treatment in patients with potentially curable pancreatic cancer. Br J Surg. 2016;103(3):267–275. doi:10.1002/bjs.10046
30. Karsten TM, Davids PH, van Gulik TM, et al. Effects of biliary endoprostheses on the extrahepatic bile ducts in relation to subsequent operation of the biliary tract. J Am Coll Surg. 1994;178(4):343–352.
31. Wang HB, Peng F, Wang M, et al. Impact of percutaneous transhepatic biliary drainage on clinical outcomes of patients with malignant obstructive jaundice undergoing laparoscopic pancreaticoduodenectomy. Curr Med Sci. 2021;41(2):375–380. doi:10.1007/s11596-021-2357-7
32. Dorcaratto D, Hogan NM, Muñoz E, et al. Is percutaneous transhepatic biliary drainage better than endoscopic drainage in the management of jaundiced patients awaiting pancreaticoduodenectomy? A Systematic Review Meta-Analysis J Vasc Interv Radiol. 2018;29(5):676–687. doi:10.1016/j.jvir.2017.12.027
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.