Back to Journals » Journal of Pain Research » Volume 18
A Retrospective Study of Ultrasound-Guided C2 Transverse Process Injection with Myofascial Release for Cervicogenic Headache
Authors Hao L ![]() , Guo Y, Song L
, Guo Y, Song L ![]() , Zhang L, Mi J
, Zhang L, Mi J
Received 25 July 2025
Accepted for publication 5 November 2025
Published 11 November 2025 Volume 2025:18 Pages 6037—6044
DOI https://doi.org/10.2147/JPR.S556139
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rune Häckert Christensen
Lijun Hao,1 Yinnan Guo,1 Liping Song,1 Lin Zhang,2 Jun Mi1
1Department of Pain Medicine, Shanxi Provincial People’s Hospital, Taiyuan, People’s Republic of China; 2Department of Anesthesiology, Shanxi Medical University, Taiyuan, People’s Republic of China
Correspondence: Lijun Hao, Department of Pain Medicine, Shanxi Provincial People’s Hospital, No. 29 Shuangtasi Street, Yingze District, Taiyuan, Shanxi, 030001, People’s Republic of China, Tel +8618835120933, Email [email protected]
Objective: To evaluate the efficacy and safety of ultrasound-guided myofascial hydrodissection between the obliquus capitis inferior and semispinalis capitis muscles combined with C2 transverse process injection in patients with cervicogenic headache (CGH).
Methods: This retrospective study analyzed 80 patients with CGH who received four sessions of ultrasound-guided treatment from January to December 2024. Each session consisted of hydrodissection of the obliquus capitis inferior and semispinalis capitis muscles along with C2 transverse process injections of lidocaine and corticosteroids. Pain intensity, disability, and headache impact were assessed using the numeric rating scale (NRS), neck disability index (NDI), and headache impact test-6 (HIT-6) at baseline, 1 week, 1 month, 3 months, and 6 months.
Results: All patients completed the treatment without serious complications. Notable and consistent reductions in NRS, NDI, and HIT-6 scores were observed at all follow-up points (P < 0.05). Minor transient adverse events, including dizziness and mild discomfort, resolved spontaneously.
Conclusion: This retrospective study suggests that ultrasound-guided myofascial hydrodissection combined with C2 transverse process injection may provide potentially meaningful pain relief and functional improvement in patients with CGH. However, given the uncontrolled retrospective design, the findings should be interpreted with caution and require confirmation in prospective controlled trials.
Keywords: cervicogenic headache, ultrasound-guided injection, myofascial hydrodissection, C2 transverse process, retrospective study, pain management
Introduction
Cervicogenic headache (CGH) is a secondary headache arising from disorders of the upper cervical spine (C1–C3), typically presenting as unilateral, dull, or radiating pain extending from the occiput to the vertex and frontal region.1 The underlying pathophysiology involves cervical facet joint dysfunction, myofascial adhesion, nerve entrapment, and central sensitization, with irritation or compression of the C2 spinal nerve and its dorsal branch—the greater occipital nerve (GON)—recognized as a key contributor.2–4 Although prevalence estimates vary widely from 0.4% to 42% depending on study design and diagnostic criteria, CGH may account for up to 15–20% of headaches and imposes a substantial burden by impairing daily functioning and quality of life.5
Fluoroscopy-guided interventions, such as high cervical epidural injections and C2/C3 facet joint blocks, are standard CGH treatments.6,7 However, they are limited by soft tissue visualization, ionizing radiation exposure, and potential risks related to vertebral artery injury or dural puncture due to needle trajectories.8 Non-pharmacological approaches such as physiotherapy and manual therapy have also been explored, and recent studies highlight their potential to improve symptoms and quality of life.9,10 Nevertheless, given the mechanical and neurogenic mechanisms underlying CGH, interventional techniques remain indispensable.
Ultrasound-guided interventions provide a real-time, radiation-free, and anatomically precise alternative, enabling dynamic visualization of cervical musculature, neurovascular structures, and the GON. Fascial entrapment of the GON between the obliquus capitis inferior and semispinalis capitis has been increasingly recognized as a major contributor to CGH.11,12 To address both mechanical compression and neurogenic inflammation, we developed a dual-target approach: ultrasound-guided myofascial hydrodissection between these muscles, combined with C2 transverse process injection of local anesthetics and corticosteroids, the latter being anatomically equivalent to a C2 nerve block.13 Unlike conventional protocols that typically employ single nerve blocks or facet joint injections, this method incorporates the myofascial component to address fascial adhesion, offering a novel strategy for simultaneous decompression and neuromodulation. Moreover, ultrasound guidance not only reduces procedural risk but also enhances therapeutic precision through real-time visualization of fascial planes and neural structures, underscoring its advantages beyond safety.
To date, no clinical study has systematically evaluated the safety and efficacy of this combined approach. Therefore, this retrospective study aims to assess the therapeutic outcomes of ultrasound-guided C2 transverse process injection with myofascial release in patients with CGH, and to provide preliminary evidence for its clinical applicability.
Materials and Methods
Study Design and Participants
This retrospective observational study included patients diagnosed with CGH who were treated at our pain clinic from January to December 2024. A total of 110 patients were initially identified based on a clinical diagnosis of CGH and treatment with ultrasound-guided C2 transverse process injection combined with myofascial hydrodissection between the obliquus capitis inferior and semispinalis capitis muscles.
To ensure homogeneity and data completeness, all cases were further screened according to predefined inclusion and exclusion criteria.
Concomitant medications such as NSAIDs or simple analgesics were permitted if kept stable during the study period, but no additional interventional procedures or structured physiotherapy programs were allowed during follow-up.
The inclusion criteria were as follows:
- age between 18 and 65 years;
- duration of symptoms ≥ 3 months;
- diagnosis of CGH confirmed by clinical assessment and imaging;
- no prior history of invasive headache treatment; and
- at least one documented follow-up evaluation within 6 months after treatment.
The exclusion criteria were as follows:
- presence of other primary or secondary headache disorders (for example, migraine, cluster headache);
- history of cervical spine surgery;
- incomplete clinical or follow-up data.
The diagnosis of CGH was based on established clinical criteria,14 including: (1) Headache provoked by neck movement or poor posture; (2) restricted cervical range of motion; (3) unilateral headache without side-shifting; (4) significant symptom relief following diagnostic nerve block. These diagnostic features were consistent with the criteria of the Cervicogenic Headache International Study Group (CHISG).
After applying these criteria, 30 patients were excluded; 12 for not meeting the inclusion criteria, 10 for incomplete clinical records, and 8 for missing imaging or procedural documentation. Ultimately, 80 patients met the eligibility criteria and were included in the final analysis (Figure 1).
 |
Figure 1 Flowchart of patient enrollment and follow-up in this retrospective study. |
Treatment Protocol
All procedures were performed by a senior pain physician with more than 10 years of experience in ultrasound-guided interventional techniques.
All 80 patients underwent four ultrasound-guided treatment sessions, administered twice weekly. Each session included myofascial hydrodissection between the obliquus capitis inferior and semispinalis capitis muscles, combined with C2 transverse process injection. The specific procedures were as follows:
Myofascial Hydrodissection of Obliquus Capitis Inferior and Semispinalis Capitis
Patients were positioned laterally with the affected side up and a pillow under the head for slight cervical flexion. A low-frequency convex ultrasound probe (6–15 MHz) was placed between C1 transverse process and C2 spinous process to visualize the obliquus capitis inferior (boat-shaped, deep to the semispinalis capitis muscle). Using an in-plane technique, a needle was advanced laterally to medially, and 20 mL of 0.5% lidocaine with 6 mg of prednisolone was injected for hydrodissection between the two muscles (Figure 2).
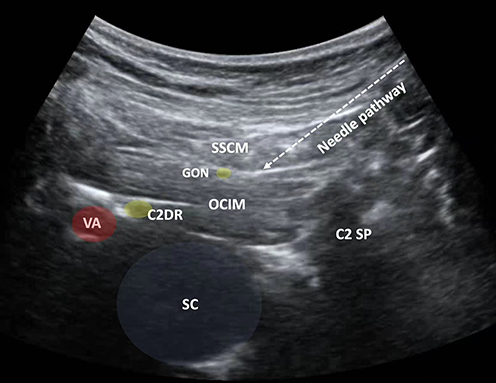 |
Figure 2 Ultrasound image at the level of the obliquus capitis inferior muscle (OCIM) in the long-axis view. Abbreviations: SSCM, semispinalis capitis muscle; OCIM, obliquus capitis inferior muscle; GON, greater occipital nerve; C2SP, C2 spinous process; SC, spinal canal; VA, vertebral artery; C2DR, C2 dorsal root. |
C2 Transverse Process Injection
With the same patient position, the probe was aligned sagittally to locate the C2 spinous process and moved laterally to identify the C2 transverse process as a hyperechoic hump. Under ultrasound guidance, 8 mL of 0.5% lidocaine with 2 mg of prednisolone was injected into the target area (Figure 3).
 |
Figure 3 Ultrasound image at the level of the C2 transverse process in the short-axis view. Abbreviations: SCM, sternocleidomastoid muscle; SpCM, splenius capitis muscle; SpCvM, splenius cervicis muscle; SM, scalenus medius muscle; C2TP, C2 transverse process. |
Outcome Measures
Numeric rating scale (NRS) for pain intensity: 0 = no pain; 10 = worst pain imaginable.
Neck disability index (NDI): 0–50; higher scores indicate greater disability.
Headache Impact Test-6 (HIT-6): 36–78; higher scores reflect greater impact on quality of life.
All outcome assessments were performed by an independent physician who was not involved in the intervention; however, formal blinding was not feasible in this retrospective study.
Assessments were conducted at baseline, and at 1 week, 1 month, 3 months, and 6 months post-treatment.
Statistical Analysis
Statistical analyses were performed using the Statistical Package for the Social Sciences software (version 22.0; IBM Corp., Armonk, NY, USA). Continuous variables are presented as mean ± standard deviation. Normality was assessed using the Shapiro–Wilk test. Repeated measures analysis of variance was used to compare outcome scores across time points, with Bonferroni correction for post hoc pairwise comparisons. A P < 0.05 was considered statistically significant. Missing data imputation was not required. As this was a retrospective study, no a priori sample size calculation was performed, which may limit statistical power.
Results
Baseline Characteristics
Baseline demographic and clinical characteristics of the 80 patients are summarized in Table 1. The mean age was 42.9 ± 7.4 years, with 35 males and 45 females. The average symptom duration was 9.2 ± 3.6 months. Pain was right-sided in 51 patients and left-sided in 29. All patients underwent four sessions of ultrasound-guided myofascial hydrodissection combined with C2 transverse process injection (Table 1).
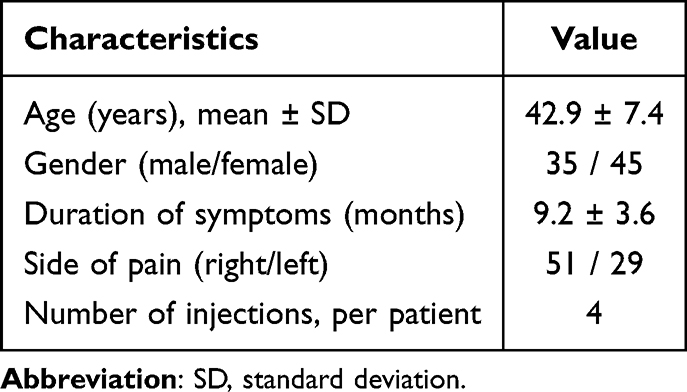 |
Table 1 Baseline Characteristics of Patients with Cervicogenic Headache (n = 80) |
Clinical Outcomes
All patients tolerated the procedures well. Nine experienced transient dizziness immediately post-injection, resolving within minutes of rest. Six reported mild neck or shoulder discomfort post-treatment, requiring no medical intervention. No serious complications such as infection, hematoma, or nerve injury were observed.
Reductions in pain intensity, functional disability, and headache impact were noted. The NRS score showed a statistically decrease at 1 week post-treatment, with continued improvement at 1, 3, and 6 months. Similarly, NDI and HIT-6 scores demonstrated a trend of improvement at each follow-up, reflecting better neck function and reduced headache impact (Table 2).
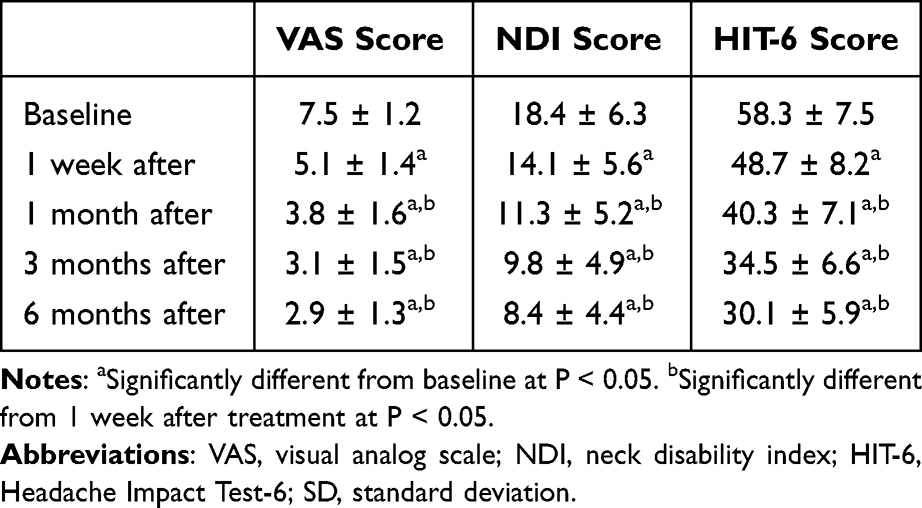 |
Table 2 Change in VAS, NDI, and HIT-6 Scores After Intervention (Mean ± SD) |
These findings indicate the potential effectiveness and safety of the dual-target ultrasound-guided treatment for CGH in a real-world clinical setting.
Discussion
This study demonstrated that ultrasound-guided myofascial separation of the obliquus capitis inferior and semispinalis capitis, combined with C2 transverse process injection, may provide sustained clinical benefits for CGH. It is hypothesized that this dual-target intervention may improve cervical mobility and quality of life through mechanical decompression and modulation of neuroinflammation; however, these mechanisms require confirmation in further studies.
CGH pathogenesis primarily stems from dysfunction in the upper cervical spine (C1–C3) segments.15 GON, a dorsal branch of the C2 spinal nerve, passes between the obliquus capitis inferior and semispinalis capitis muscles.16 Chronic muscle tension, fascial adhesions, or local inflammation in this region can cause nerve compression or irritation, leading to characteristic unilateral, radiating headache.17
In this study, ultrasound-guided hydrodissection appeared to separate the two muscles by injecting fluid into the interfascial space, thereby possibly alleviating nerve compression. This mechanism is plausible but should be interpreted cautiously, as no objective imaging confirmation was performed. The intervention may also improve local circulation and lymphatic drainage, which might contribute to reducing inflammation and pain.18
We hypothesize that injectate delivered at the C2 transverse process may diffuse to nearby structures, including C1–C3 dorsal rami and the C2–3 facet joints; however, this remains speculative in the absence of direct anatomical or imaging evidence. Anatomical studies suggest that the C2 transverse process lies near these structures,19,20 but further radiographic or cadaveric validation is warranted. The pharmacological action of lidocaine and corticosteroids may contribute to both nociceptive blockade and suppression of neuroinflammation, consistent with prior reports of benefit from C2/C3 injections lasting up to 6 months.21
Importantly, this is the first study to preliminarily evaluate a combined protocol of ultrasound-guided hydrodissection and C2 transverse process injection. While previous research has demonstrated the efficacy of fascial release22 and C2 injections individually,21 our results provide preliminary clinical evidence for their integration. Nonetheless, as a retrospective study without a control group, these findings should be interpreted as hypothesis-generating rather than conclusive.
Additionally, ultrasound guidance offers distinct advantages over fluoroscopy: real-time dynamic imaging, absence of ionizing radiation, portability, and enhanced safety. Notably, the injection path in this study is relatively superficial and visualized, avoiding critical structures such as the dura mater and spinal canal. Using the Doppler mode ensures accurate localization of the vertebral artery, reducing the risks of vascular injury or epidural mis-injection often associated with fluoroscopic guidance. Compared to dorsal root ganglion (DRG) block at the C2, injection at the C2 transverse process is considered significantly safer. The C2 DRG lies near critical structures such as the vertebral artery, spinal cord, and spinal canal, increasing the risk of complications such as vascular puncture, intrathecal injection, or nerve injury.23 By contrast, the C2 transverse process target is more superficial and accessible, making it a practical option for outpatient use, though prospective comparative studies are required to confirm its relative safety profile.
Finally, while interventional techniques remain indispensable for patients with refractory CGH, recent evidence also highlights physiotherapy and manual therapy as complementary strategies in headache management,9,10 integrating such approaches into future studies could provide a more comprehensive perspective on multimodal management of CGH.
This study has limitations. First, the diagnosis of cervicogenic headache was based on the criteria proposed by the Cervicogenic Headache International Study Group (CHISG), rather than the International Classification of Headache Disorders (ICHD). The use of CHISG criteria is common in interventional pain research but does not fully align with the ICHD system, which is more widely applied in clinical and research settings. Cervicogenic headache is a particularly complex condition, and ongoing debate persists between the two diagnostic frameworks.24 Consequently, some included participants may also meet the diagnostic criteria for other ICHD categories, such as migraine, which may affect the generalizability of our findings. Second, as a single-arm retrospective study without a control group, the interpretation of efficacy should be cautious. Finally, outcome evaluation relied mainly on patient-reported measures without blinding or objective assessments, raising the possibility of placebo effects or overestimation. Future prospective controlled studies are warranted to validate these findings.
Conclusion
This retrospective study suggests that ultrasound-guided myofascial hydrodissection combined with C2 transverse process injection may provide pain relief and functional improvement in patients with CGH. Importantly, this dual-target protocol has the potential to serve as a radiation-free alternative to fluoroscopic methods, indicating possible clinical relevance. However, given the absence of a control group, reliance on subjective outcomes, and potential selection bias, these findings should be interpreted with caution. Future randomized controlled trials with objective endpoints are needed to confirm efficacy, clarify mechanisms, and define the role of this approach within broader multimodal headache management strategies, including physiotherapy and manual therapy.
Data Sharing Statement
The data supporting the results reported in this manuscript are available from the corresponding author upon reasonable request. Data can be accessed by contacting Dr. LiJun Hao at [email protected]. Please note that due to confidentiality agreements, some data may not be available for public sharing.
Ethics Approval and Informed Consent
This study was approved by the Institutional Review Board (IRB) of Shanxi Provincial People’s Hospital, Taiyuan, China (Reference No: 2025510). Informed consent was obtained from all individual participants included in the study. Each participant was provided with a detailed explanation of the study procedures, potential risks, and benefits, and they provided written informed consent before participating in the study. This study complies with the principles of the Declaration of Helsinki.
Consent for Publication
Consent for publication was obtained from all participants. They were informed that the details of their clinical data, including images, would be published in this manuscript. Signed consent forms are available upon request from the journal editorial office.
Author Contributions
Lijun Hao conceived and designed the study. Yinnan Guo and Jun Mi performed the procedures and collected the clinical data. Lin Zhang analyzed the data and interpreted the results. Liping Song contributed to the literature review and manuscript drafting. Lijun Hao and Yinnan Guo wrote the main manuscript text.
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no competing interests. No author has any financial or non-financial interests related to the study.
References
1. Pöllmann W, Keidel M, Pfaffenrath V. Headache and the cervical spine: a critical review. Cephalalgia. 1997;17(8):801–816. doi:10.1046/j.1468-2982.1997.1708801.x
2. Janjua MB, Reddy S, El Ahmadieh TY, et al. Occipital neuralgia: a neurosurgical perspective. J Clin Neurosci. 2020;71:263–270. doi:10.1016/j.jocn.2019.08.102
3. Piovesan EJ, Utiumi MAT, Grossi DB. Cervicogenic headache - How to recognize and treat. Best Pract Res Clin Rheumatol. 2024;38(1):101931. doi:10.1016/j.berh.2024.101931
4. Chowdhury D, Datta D, Mundra A. Role of greater occipital nerve block in headache disorders: a narrative review. Neurol India. 2021;69(Suppl 1):S228–s256.10.4103/0028–3886.315993. doi:10.4103/0028-3886.315993
5. Xu Y, Gao Y, Jiang L, et al. Global trends in research on cervicogenic headache: a bibliometric analysis. Front Neurol. 2023;14:1169477. doi:10.3389/fneur.2023.1169477
6. Zhou L, Hud-Shakoor Z, Hennessey C, Ashkenazi A. Upper cervical facet joint and spinal rami blocks for the treatment of cervicogenic headache. Headache. 2010;50(4):657–663. doi:10.1111/j.1526-4610.2010.01623.x
7. Wang E, Wang D. Treatment of cervicogenic headache with cervical epidural steroid injection. Curr Pain Headache Rep. 2014;18(9):442. doi:10.1007/s11916-014-0442-3
8. Shim E, Lee JW, Lee E, Ahn JM, Kang Y, Kang HS. Fluoroscopically guided epidural injections of the cervical and lumbar spine. Radiographics. 2017;37(2):537–561. doi:10.1148/rg.2017160043
9. Tedeschi R, Pillastrini P, Pierangeli G, Favoni V, Cortelli P, Cevoli S. Is physiotherapy in migraines known to sufferers? A cross-sectional study. Neurol Sci. 2024;45(4):1669–1674. doi:10.1007/s10072-023-07195-9
10. Tedeschi R. Integrating manual therapy into headache management: bridging the evidence gap. Neurol Sci. 2025;46(7):3287–3289. doi:10.1007/s10072-025-08093-y
11. Djavaherian DM, Guthmiller KB. Occipital Neuralgia. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538281.
12. Saglam L, Gayretli O, Coskun O, Kale A. Morphological features of the greater occipital nerve and its possible importance for interventional procedures. J Anat. 2024;244(2):312–324. doi:10.1111/joa.13959
13. Bogduk N. The anatomy of occipital neuralgia. Clin Exp Neurol. 1981;17:167–184.
14. Verma S, Tripathi M, Chandra PS. Cervicogenic headache: current perspectives. Neurol India. 2021;69(Suppl 1):S194–s198.10.4103/0028–3886.315992. doi:10.4103/0028-3886.315992
15. Al Khalili Y, Ly NK, Murphy PB. Cervicogenic headache. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507862.
16. Yu M, Wang SM. Anatomy, head and neck, occipital nerves. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK546640.
17. Bogduk N. The clinical anatomy of the cervical dorsal rami. Spine. 1982;7(4):319–330. doi:10.1097/00007632-198207000-00001
18. Buntragulpoontawee M, Chang KV, Vitoonpong T, et al. The effectiveness and safety of commonly used injectates for ultrasound-guided hydrodissection treatment of peripheral nerve entrapment syndromes: a systematic review. Front Pharmacol. 2020;11:621150. doi:10.3389/fphar.2020.621150
19. Baek IC, Park K, Kim TL, O J, Yang HM, Kim SH. Comparing the injectate spread and nerve involvement between different injectate volumes for ultrasound-guided greater occipital nerve block at the C2 level: a cadaveric evaluation. J Pain Res. 2018;11:2033–2038. doi:10.2147/jpr.S172692
20. Zhang Y, Li H, Xu S, Guo R, Ma D, Wang Y. Understanding the anatomy of posterior cervical interfascial space: implications for regional blocks and pain management. a narrative review. Pain Ther. 2025;14(4):1203–1222. doi:10.1007/s40122-025-00754-2
21. Wan Q, Yang H, Li X, et al. Ultrasound-guided versus fluoroscopy-guided deep cervical plexus block for the treatment of cervicogenic headache. Biomed Res Int. 2017;2017:4654803. doi:10.1155/2017/4654803
22. Lam KHS, Su DC, Wu YT, Janze A, Reeves KD. Novel ultrasound-guided hydrodissection with 5% dextrose for the treatment of occipital neuralgia targeting the greater occipital nerve. Diagnostics. 2024;14. doi:10.3390/diagnostics14131380
23. He L, Zhao W, Su PP, et al. A novel ultrasonographic method to quickly and accurately access the C2 dorsal root Ganglion. Pain Physician. 2024;27(8):E927–e935. doi:10.36076/ppj.2024.7.E927
24. Robinson CL, Christensen RH, Al-Khazali HM, et al. Prevalence and relative frequency of cervicogenic headache in population- and clinic-based studies: a systematic review and meta-analysis. Cephalalgia. 2025;45(3):3331024251322446. doi:10.1177/03331024251322446
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.