")
Back to Journals » International Journal of General Medicine » Volume 16
A Retrospective Study of Pneumococcal Pneumonia in Hospitalized Patients Aged ≥65 Years in Izumo, Japan: 2010 to 2014
Authors Hamaguchi M , Tsubata Y , Yoshihara K, Nakao M, Amano Y, Nakashima K, Hotta T , Okimoto T, Hamaguchi S, Sutani A, Isobe T
Received 27 February 2023
Accepted for publication 26 May 2023
Published 30 May 2023 Volume 2023:16 Pages 2125—2132
DOI https://doi.org/10.2147/IJGM.S407732
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mihajlo Jakovljevic
Megumi Hamaguchi,1 Yukari Tsubata,1 Ken Yoshihara,1 Mika Nakao,1 Yoshihiro Amano,1 Kazuhisa Nakashima,1 Takamasa Hotta,2 Tamio Okimoto,1 Shunichi Hamaguchi,3 Akihisa Sutani,4 Takeshi Isobe1
1Division of Medical Oncology and Respiratory Medicine, Department of Internal Medicine, Shimane University, Izumo, Shimane, Japan; 2Department of Respiratory Medicine, Shimane Prefectural Central Hospital, Izumo, Shimane, Japan; 3Department of General Medicine, Shimane University, Izumo, Shimane, Japan; 4Sutani Respiratory Clinic, Izumo, Shimane, Japan
Correspondence: Megumi Hamaguchi, Division of Medical Oncology and Respiratory Medicine, Department of Internal Medicine, Shimane University, 89-1, Enyacho, Izumo-shi, Shimane, Japan, Tel/Fax +81-853-20-2581, Email [email protected]
Purpose: In Japan, both a 23-valent pneumococcal polysaccharide vaccine (PPSV23) and a 13-valent pneumococcal conjugate vaccine (PCV13) are available. Although randomized controlled trials have examined the effects of pneumococcal vaccines, few epidemiological studies have investigated the onset of pneumococcal pneumonia in general practice. In Izumo, Shimane Prefecture, Japan, a public subsidy for PPSV23 inoculation began in November 2012.
Patients and Methods: The subjects were pneumonia patients aged 65 and over who were admitted to a hospital in Izumo. This retrospective study analyzed the following data extracted from medical records: pneumococcal pneumonia prevalence, pneumonia severity, mortality rate, PPSV23 vaccination rate, and length of hospital stay. The 2 years before the start of the public subsidy were defined as the early phase, and the 2 years after the subsidy initiation were defined as the late phase. We compared the two phases in terms of PPSV23 vaccination rate, prevalence and severity of pneumococcal pneumonia, and mortality rate.
Results: We investigated data from a total of 1188 and 1086 patients in the early and late phases, respectively. The prevalence of pneumococcal pneumonia was 21.0% and 21.3% in the early and late phases, respectively. The mortality rate from pneumococcal pneumonia was 10.4% and 5.4% in the early and late phases, respectively (p = 0.080), indicating a 50% reduction. The PPSV23 vaccination rate (p < 0.001) and the comorbidity rates of chronic respiratory disease (p = 0.022) and chronic renal disease (p < 0.001) were significantly different between the early and late phases.
Conclusion: This study showed that the rate of in-hospital deaths due to pneumococcal pneumonia was halved after the PPSV23 vaccine was subsidized. The causal relationship between the pneumococcal vaccination rate and the mortality rate of pneumococcal disease was unclear. Further investigation is deemed necessary.
Keywords: Streptococcus pneumoniae, pneumococcal pneumonia, vaccine, PPSV23, PCV13
Introduction
Streptococcus pneumoniae causes otitis media, sinusitis, and pneumonia in children and adults. This organism is the most common cause of community-acquired pneumonia (CAP) and nursing and healthcare-associated pneumonia (NHCAP) in Japan,1,2 and it is responsible for a high pneumonia-related mortality rate of 16–55%3,4 in older people, defined here as aged 65 and over. Furthermore, Streptococcus pneumoniae causes invasive pneumococcal diseases (IPDs), such as meningitis and pneumonia with bloodstream infection, that have a mortality rate of over 20% in older people.5 Preventing the worsening of pneumococcal infections in older adults is an important issue. In Japan, two types of pneumococcal vaccines are available for older individuals: the 23-valent pneumococcal excipient vaccine (PPSV23) and the 13-valent pneumococcal conjugate vaccine (PCV13). PPSV23 is a polysaccharide vaccine, which means it contains portions of the outer polysaccharide capsule of 23 different strains of the pneumococcus bacteria. When a person receives PPSV23, their immune system produces antibodies against these polysaccharides, which can help fight off infection if they are later exposed to the actual bacteria. PCV13, on the other hand, is a conjugate vaccine, which means it contains components of the pneumococcus bacteria that are chemically conjugated to a carrier protein. This conjugation enhances the immune response. A meta-analysis performed under the 2013 Cochrane Joint Plan showed that PPSV23 reduced the incidence of IPDs caused by all serotypes by 74%, and the incidence of those caused by vaccine serotypes by 82%.6 PPSV23 was also shown to lower medical expenses.7 Based on these results, a public subsidy for PPSV23 vaccination was started in October 2014 in Japan. This subsidy is designed to provide financial assistance to eligible individuals who receive the PPSV23 vaccine. People are eligible if they are 65 years of age or older or if they have certain medical conditions that put them at higher risk of developing pneumococcal infections. The subsidy is intended to cover most of the cost of the vaccine. It is also important to suppress the onset and prevent the worsening of pneumococcal pneumonia without associated IPD. Morimoto et al reported that from September 2011 to January 2013, only 2.9% of pneumococcal pneumonia cases were associated with bloodstream infection,8 and most cases of pneumonia in Japan are pneumococcal without bacteremia.8 A randomized control trial (RCT) by Maruyama et al9 reported the effects of PPSV23 on the onset of both pneumococcal and non-pneumococcal pneumonia. They reported that the incidence of pneumococcal pneumonia during follow-up was significantly higher in the placebo group than in the vaccine group: 9.8% vs 13.3%, respectively. Also, significantly more participants with pneumococcal pneumonia died in the placebo group than in the vaccine group: 35.1% vs 0%, respectively. The limitation of this research is that it was conducted on patients in a limited situation, namely elderly care facilities. Recently, Suzuki et al10 investigated the effectiveness of the 23-valent pneumococcal polysaccharide vaccine (PPV23) against pneumococcal pneumonia in adults aged 65 years or older. They found no significant effect of PPSV23 vaccination on pneumococcus-associated mortality.
In Izumo, Shimane Prefecture, Japan, a public subsidy for PPSV23 vaccination began in November 2012, approximately 2 years prior to the public subsidy in Japan that was initiated in October 2014. Naito et al11 previously reported on the effect of improving vaccination rates through public subsidies. It was expected that PPSV23 vaccination rates and awareness of the vaccines were improved in Shimane Prefecture since the start of public subsidies in 2012. In this study, we targeted older inpatients aged 65 and over who had mainly moderate to severe pneumonia in Izumo, and analyzed pneumococcal pneumonia prevalence, pneumonia severity, mortality rate, PPSV23 inoculation rate, and length of hospital stay. We examined the changes in pneumonia severity, prevalence of pneumococcal pneumonia, and mortality among hospitalized pneumonia patients before and after the public subsidy. A RCT9 investigated the effect of PPSV23 inoculation on pneumococcal pneumonia without associated bloodstream infection, but only one report12 has assessed the PPSV23 vaccination rate or the prevalence and mortality of pneumococcal pneumonia in daily practice over several years.
Materials and Methods
Patients
We conducted a retrospective survey before and after the start of the public subsidy for PPSV23 inoculation in Izumo, Japan. We defined the 2 years before the start of the subsidy (October 2010 to September 2012) as the early phase, and the 2 years after the start of the subsidy (November 2012 to October 2014) as the late phase. Patients aged 65 and over who were admitted to any of the five acute care hospitals in Izumo (Shimane University Hospital, Shimane Prefectural Central Hospital, Izumo Tokushukai Hospital, Izumo Municipal Hospital, and Izumo Municipal General Medical Center) were enrolled if they were clinically diagnosed with bacterial pneumonia by an emergency doctor or internal medicine doctor and required hospitalization for more than 1 day. The doctors clinically diagnosed bacterial pneumonia based on a comprehensive assessment that included the following: physical findings such as fever, cough, sputum, chest pain, shortness of breath, and fatigue; examination findings such as abnormal chest sounds, elevated inflammatory markers in blood tests, and decreased oxygenation or increased respiratory rate; and the presence of infiltration shadows or ground-glass opacities on chest X-ray or CT. Patients without these findings were excluded from the analysis.
Data Collection
We collected data from the medical records of each hospital. First, we checked whether the findings in patients who were clinically diagnosed with bacterial pneumonia were consistent with those typical of this condition. Then, we collected data on patient age, gender, comorbidities, pneumonia type (see below), causative organism, vaccination status, length of hospital stay, and in-hospital mortality. Vaccination status was not routinely recorded, and physicians only inquired about it if necessary. Vaccination status was self-reported.
We classified pneumonia types into community-acquired pneumonia (CAP), hospital-acquired pneumonia, and nursing and health care–associated pneumonia (NHCAP) based on the guidelines13–15 of the Japanese Respiratory Society. According to Japanese guidelines,13 CAP is defined as pneumonia acquired in the community by patients who have not been hospitalized. Specifically, it refers to pneumonia acquired within the patient’s daily living environment, excluding outbreaks and cases in nursing homes or other elderly care facilities. The definition of NHCAP in the Japanese guidelines15 is as follows: (1) pneumonia that occurs within 48 hours of hospital admission in patients with a history of hospitalization or outpatient visits to healthcare facilities, or (2) pneumonia that develops within 2 weeks after surgery, hemodialysis, chemotherapy, radiation therapy, immunosuppressant use, or in patients who have resided in healthcare facilities for an extended period, even if they have no history of hospitalization or outpatient visits. We scored pneumonia severity according to the CAP severity classification (A-DROP),13 with each of the following assigned one point: 1) Age: male ≥ 70, female ≥ 75; 2) Dehydration: blood urea nitrogen ≥ 21, or dehydration findings; 3) Respiration: SpO2 < 90%, PaO2 < 60%, or RR ≥ 30; 4) Orientation: disturbance of consciousness; and 5) Blood pressure: sBP < 90 mmHg. We then categorized severity as follows: 0 points, mild; 1–2 points, moderate; 3 points, severe; and 4–5 points, extremely severe. As for comorbidities, we investigated chronic respiratory disease, chronic heart disease, chronic renal disease, chronic liver disease, diabetes, and splenic dysfunction. For bacteriological diagnosis, we determined whether sputum cultures, blood cultures, and the pneumococcal urinary antigen test were performed. If any of these were positive for a single bacterium, or if the urinary pneumococcal antigen was positive, we judged the relevant bacterium to be causative.
Statistical Analysis
Statistical analysis was outsourced to APO PLUS STATION (former Qol RD). We used the chi-square test to assess mortality during hospitalization and that caused by pneumococcal pneumonia, and to compare proportions of patients with PPSV23 vaccination, pneumococcal pneumonia, comorbid diseases, and different pneumonia severities. We used Wilcoxson’s rank sum test to evaluate length of hospital stay. We considered a p-value of <0.05 to be statistically significant.
Ethical Considerations
This study was approved by the Medical Research Ethics Committee, Shimane University Faculty of Medicine, Japan, in accordance with the Declaration of Helsinki (study number: 1531). The study involved only the collection and use of existing information (including personal information requiring special care) from our institution and other institutions. The subjects of this study were patients who were hospitalized at our institution and other institutions in the past, and it was difficult to obtain informed consent from these patients. Therefore, we provided an opportunity for research subjects and their representatives to refuse the implementation or continuation of the research by accessing each hospital’s website. The content posted on the websites included the following: 1) the purpose and method of the use of information; 2) items of information to be used; 3) the name of the period for which information is provided and the name of the head of that period; 4) the method of obtaining information; 5) the name of the principal investigator and the name of the affiliated research institution; 6) notification that at the request of the research subject or his/her agent, the suspension of use of information that will be destroyed by the research subject, and the method of accepting such a request. Informed consent was waived by the Ethical Guidelines for Medical and Biological Research Involving Human Subjects, and this exemption was approved by the Medical Research Ethics Committee, Shimane University Faculty of Medicine.
Results
Patient Background
Table 1 shows patient background information. A total of 2274 patients were investigated during the 4-year study period, and the number of patients was almost the same in the early and late phases. In both phases, the median age was 84 years and the proportion of males was high. Available medical records data showed that the PPSV23 vaccination rate was 0.76% in the early phase and 3.80% in the late phase, indicating a significant difference between the two phases.
 |
Table 1 Patient Background |
Regarding comorbid diseases (Table 2), the numbers of patients with chronic respiratory disease (p = 0.022) and chronic kidney disease (p < 0.001) were significantly lower in the late group compared to the early group. Splenic dysfunction (splenectomy) was identified in only 0.4% of patients in the early phase and 0.7% in the late phase. The total number of patients with no comorbidities was 192 (8.4%): 110 in the early phase and 82 in the late phase.
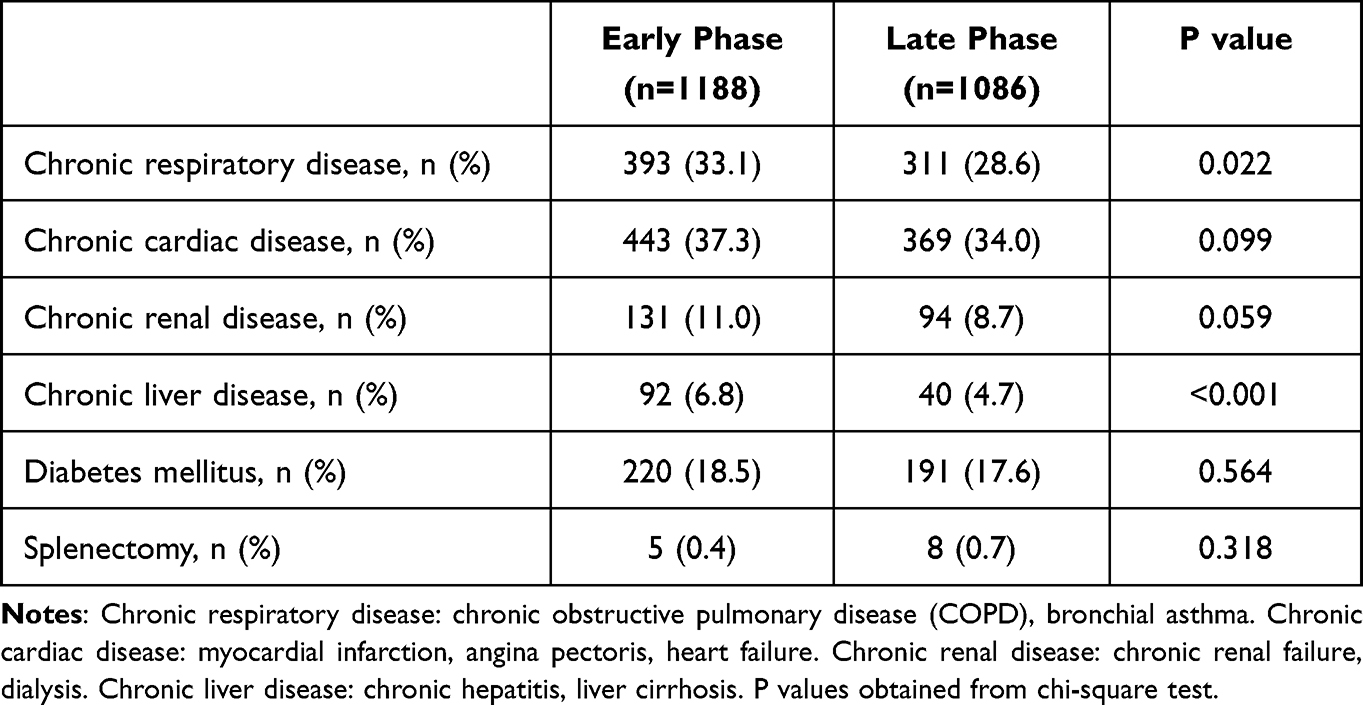 |
Table 2 Patients Comorbidities |
Pneumonia Characteristics
In terms of pneumonia type, NHCAP was the most common, accounting for 58.0% of cases in the early phase and 72.7% in the late phase (Figure 1). Regarding pneumonia severity, moderate was most common in both early and late phases, with moderate and severe cases accounting for nearly 90% of the total (early phase, 86.8%; late phase, 88.3%). Patients with extremely severe pneumonia comprised 9.8% of cases in the early phase and 9.3% in the late phase (Figure 2). There was no significant change (p = 0.427) in the proportion of any severity grade between the early and late phases.
 |
Figure 1 Types of pneumonia. Abbreviations: CAP, community-acquired pneumonia; HAP, hospital-acquired pneumonia; NHCAP, nursing and healthcare-associated pneumonia. Notes: There was no significant difference in pneumonia severity grades (p = 0.427, chi-square test) between the early and late phases. |
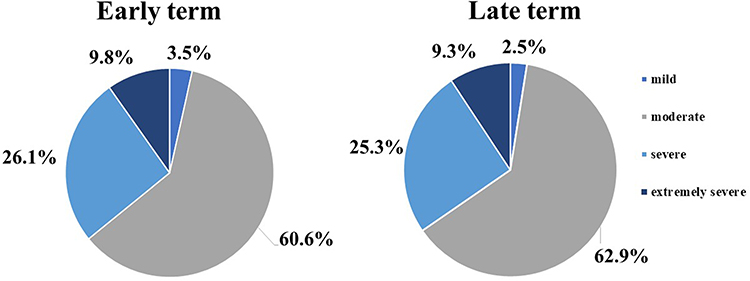 |
Figure 2 Pneumonia severity. Notes: Pneumonia of moderate severity was most common in both early and late phases, with moderate and severe cases accounting for nearly 90% of the total (early phase, 86.8%; late phase, 88.3%). Patients with extremely severe pneumonia comprised 9.8% of cases in the early phase and 9.3% in the late phase. |
Causative Bacteria
Figure 3 shows the percentages of bacteria suspected of causing pneumonia in the early and late phases. Streptococcus pneumoniae was the most common cause in both phases, accounting for 12.2% of cases in the early phase and 9.7% in the late phase. The percentages of cases due to Klebsiella pneumoniae and Staphylococcus aureus were also high. No culture tests were performed in 16.8% (381) of cases.
 |
Figure 3 Causative bacteria. Notes: Streptococcus pneumoniae was the most common cause in both phases, accounting for 12.2% of cases in the early phase and 9.7% in the late phase. |
Characteristics of Hospitalized Pneumonia Patients
The prevalence of pneumococcal pneumonia in hospitalized patients was 21.0% in the early phase and 21.3% in the late phase (p = 0.943). In patients with pneumonia, the average length of the hospital stay was 29.3 days in the early phase and 24.8 days in the late phase (p = 0.193), while in patients with pneumococcal pneumonia it was 29.6 days in the early phase and 26.2 days in the late phase (p = 0.101). The in-hospital mortality rate due to pneumonia was 20.3% in the early phase and 18.7% in the late phase (p = 0.341), and the mortality rate due to pneumococcal pneumonia was 10.4% in the early phase and 5.4% in the late phase (p = 0.079) (Table 3).
 |
Table 3 Characteristics of Hospitalized Pneumonia Patients |
Discussion
We investigated differences in pneumonia prevalence and mortality before and after the PPSV23 public subsidy in Izumo, Japan. The most notable finding was that the mortality rate due to pneumococcal pneumonia was halved after the start of the public subsidy.
There are five acute care hospitals in Izumo, and if a patient in Izumo develops pneumonia that requires hospitalization, they will be admitted to one of these hospitals. Therefore, the survey we conducted provides a comprehensive overview of pneumococcal pneumonia in the entire community of Izumo. Although previous RCTs9 reported the effects of PPSV23 on the onset of pneumococcal and non-pneumococcal pneumonia, no reports have investigated changes in the prevalence and mortality of pneumococcal pneumonia in a group of patients in daily clinical practice.
Shimane Prefecture has one of the oldest populations in Japan, and the median age in our study was 84 years in both the early and late phases. This is about 20 years older than in past overseas reports16,17 that examined the effectiveness of PPSV23, and about 10 years older than in the report by Kawakami et al.7 The age is similar to that in the report by Maruyama et al9 involving facility residents. However, the proportion of patients with comorbidities was higher in our study than in two of the aforementioned studies,7,9 and we consider that our study enrolled patients who were generally at high risk of experiencing worsening of pneumococcal pneumonia. In fact, nearly 90% of patients in our study had moderate or severe pneumonia, both in the early and late phases. In addition, the patients with extremely severe pneumonia accounted for almost 10% in both phases. In-hospital mortality from pneumonia of all etiologies and mortality from pneumococcal pneumonia were also higher in our study than previously reported,7,9,17 reflecting the high severity.
The early and late phases were similar in terms of median age, pneumonia severity, and the proportion of pneumococcal patients. The mortality rate of pneumococcal pneumonia was halved in the late phase compared with the early phase, but the difference was not statistically significant. The PPSV23 vaccination rate and the comorbidity rates of chronic respiratory disease and chronic renal disease were significantly different between the early phase and the late phase. It is considered that these differences may have an impact on the mortality rate of pneumococcal pneumonia.
This study has several limitations. First, pneumococcal vaccination was not documented for many patients in this study, and we were unable to establish a causal relationship between pneumococcal vaccination coverage and mortality from pneumococcal pneumonia. Regarding the vaccination status, it is necessary to standardize the contents of pneumonia-related medical records in Izumo, such as by determining the vaccination status at the initial pneumonia diagnosis and recording it in the medical records. Second, our determination of whether the pneumococcal vaccination rate in Izumo differed between the early and late phases was based only on medical records. Regarding this issue, we plan to clarify the causal relationship between the pneumococcal vaccination rate and pneumococcal mortality in cooperation with local governments. Finally, various risk factors are involved in the mortality rate of older patients with pneumonia. We were unable to investigate several important parameters, such as changes in patient demographics (smoking rate, nutritional status, activities of daily living, etc.), that might be associated with pneumonia mortality.
This study did not take into account PCV13 vaccination. PCV13 was approved for use in adults in Japan in June 2014, and can be administered as a voluntary vaccination to people aged 65 and over. Furthermore, beginning in May 2020, the indication for PCV13 was expanded to high-risk persons aged 6–64 years. It is also worth noting that the introduction of PCV13 for infants in 2013 may have an additional impact. It is expected that administering PPSV23 after PCV13 will have a booster effect regarding specific antigens on the 12 serotypes common to both vaccines,18 and we plan to examine this issue in the future.
Conclusion
This study showed that the mortality rate due to pneumococcal pneumonia was halved after the start of the public subsidy for PPSV23 in Izumo, Japan. We are conducting additional research to determine the pneumococcal vaccine rate and the mortality rate of pneumococcal pneumonia based on data collected since 2014, when PCV13 vaccination became available for elderly people aged 65 and over. We aim to elucidate methods to reduce the mortality rate caused by pneumococcal pneumonia in Japan’s super-aging society.
Acknowledgments
We would like to express our sincere gratitude to each of the following for their cooperation in this research: Dr. Kiyoshi Kikuchi, Director of Shimane Prefectural Central Hospital; Dr. Takashige Kuraki and Dr. Kiyotaka Miura of the Department of Respiratory Medicine, Shimane Prefectural Central Hospital; Dr. Taisuke Komatsu, Director of Izumo City Hospital; Dr. Toshihiro Shizuku, Director of Izumo City General Medical Center; and Dr. Hideki Tabara, Director of Izumo Tokushukai Hospital. We would also like to thank the clerical staff of each hospital for their help in obtaining medical records.
Funding
This study was funded by the Japan Association of Health Services.
Disclosure
Dr Kazuhisa Nakashima reports personal fees from TAIHO Pharmaceutical Co., Ltd., Chugai Pharmaceutical Co., Ltd., AstraZeneca K.K., and Eli Lilly Japan K.K., outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Ishida T, Tachibana H, Ito A, et al. Clinical characteristics of nursing and healthcare-associated pneumonia: aJapanese variant of healthcare-associated pneumonia. Intern Med. 2012;51(18):2537–2544. doi:10.2169/internalmedicine.51.7987
2. Shindo Y, Ito R, Kobayashi D, et al. Risk factors for drug-resistant pathogens in community-acquired and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2013;188:985–995. doi:10.1164/rccm.201301-0079OC
3. Tleyieh IM, Tlaygeh HM, Hejal R, et al. The impact of penicillin resistance on short-term mortality in hospitalized adults with pneumococcal pneumonia: a systematic review and meta-analysis. Clin Infect Dis. 2006;42:788–797. doi:10.1086/500140
4. Aspa J, Rajas O, Rodriguez de Castro F, et al. Impact of initial antibiotic choice on mortality from pneumococcal pneumonia. Eur Respir J. 2006;27:1010–1019. doi:10.1183/09031936.06.00126004
5. Fedson DS. Pneumococcal conjugate vaccination for older adults. Hum Vaccine Immunother. 2013;10:47–51. doi:10.4161/hv.26422
6. Moderley S, Holden J, Tatham DP, et al. Vaccines for preventing pneumococcal infection in adults. Cochrane Database Syst Rev. 2013;1:CD000422.
7. Kawakami K, Ohkusa Y, Kuroki R, et al. Effectiveness of pneumococcal polysaccharide vaccine against pneumonia and cost analysis for the elderly who receive seasonal influenza vaccine in Japan. Vaccine. 2010;28(43):7063–7069. doi:10.1016/j.vaccine.2010.08.010
8. Morimoto K, Suzuki M, Ishifuji T, et al. The burden and etiology of community-onset pneumonia in the aging Japanese population: a multicenter prospective study. PLoS One. 2015;10:e0122247. doi:10.1371/journal.pone.0122247
9. Maruyama T, Taguchi O, Niederman MS, et al. Efficacy of 23-valent pneumococcal vaccine in preventing pneumonia and improving survival in nursing home residents: double blind randomized and placebo controlled trial. BMJ. 2010;340:c1004. doi:10.1136/bmj.c1004
10. Suzuki M, Dhoubhadel BG, Ishifuji T, et al. Adult Pneumonia Study Group-Japan (APSG-J). Serotype-specific effectiveness of 23-valent pneumococcal polysaccharide vaccine against pneumococcal pneumonia in adults aged 65 years or older: a multicentre, prospective, test-negative design study. Lancet Infect Dis. 2017;17:313–321. doi:10.1016/S1473-3099(17)30049-X
11. Naito T, Matsuda N, Tanei M, et al. Relationship between public subsidies and vaccination rates with the 23-valent pneumococcal vaccine in elderly persons, including the influence of the free vaccination campaign after the Great East Japan Earthquake. J Infect Chemother. 2014;20(7):450–453. doi:10.1016/j.jiac.2014.03.004
12. Jung SM, Lee H, Nishiura H. The impact of pneumococcal vaccination on pneumonia mortality among the elderly in Japan: a difference-in-difference study. PeerJ. 2018;12;6:e6085. doi:10.7717/peerj.6085
13. Committee for the Japanese Respiratory Society guidelines for the management of respiratory infections. The JRS guidelines for the management of community-acquired pneumonia in adults. Tokyo. Japanese Respiratory Society; 2007. Japanese.
14. Committee for the Japanese Respiratory Society guidelines for the management of respiratory infections. The JRS guidelines for the management of hospital-acquired pneumonia in adults. Tokyo: Japanese Respiratory Society; 2008. Japanese.
15. Committee for the Japanese Respiratory Society guidelines for the management of nursing and healthcare-associated pneumonia (NHCAP). The JRS guidelines for the management of nursing and healthcare-associated pneumonia.Tokyo: Japanese Respiratory Society; 2011. Japanese.
16. Alfageme I, Vazquez R, Reyes N, et al. Clinical efficacy of anti-pneumococcal vaccination in patients with COPD. Thorax. 2006;61:189–195. doi:10.1136/thx.2005.043323
17. Ortqvist A, Hedlund J, Burman LA; Swedish Pneumococcal Vaccination Study Group, et al. Randomized trial of 23-valent pneumococcal capsular polysaccharide vaccine in prevention of pneumonia in middle-aged and elderly people. Lancet. 351;1998:399–403. doi:10.1016/S0140-6736(97)07358-3
18. Greenberg RN, Gurtman A, Frenck RW, et al. Sequential administration of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine in pneumococcal vaccine-naïve adults 60–64 years of age. Vaccine. 2014;32:2364–2374. doi:10.1016/j.vaccine.2014.02.002
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.