Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
A Retrospective Study of Hepatic Arterial Infusion Chemotherapy Combined with Tyrosine Kinase Inhibitors and PD-1 Inhibitors in Hepatocellular Carcinoma Patients with Main Portal Vein Tumor Thrombus (VP4)
Authors Wang X ![]() , Chen S
, Chen S ![]() , Yu W, Liu W, Fang Z
, Yu W, Liu W, Fang Z
Received 27 September 2025
Accepted for publication 14 December 2025
Published 7 January 2026 Volume 2026:13 562766
DOI https://doi.org/10.2147/JHC.S562766
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Mohamed Shaker
Xiaolong Wang, Shiguang Chen, Wenchang Yu, Weifu Liu, Zhuting Fang
Department of Oncology and Vascular Interventional Therapy, Clinical Oncology School of Fujian Medical University, Fujian Cancer Hospital, Fuzhou, 350014, People’s Republic of China
Correspondence: Zhuting Fang, Department of Oncology and Vascular Interventional Therapy,Clinical Oncology School of Fujian Medical University, Fujian Cancer Hospital, Fuzhou, 350014, People’s Republic of China, Email [email protected]
Background: Patients with hepatocellular carcinoma (HCC) involving main portal vein tumor thrombosis (Vp4) face a dismal prognosis with limited treatment options. While combination therapy comprising hepatic arterial infusion chemotherapy (HAIC), tyrosine kinase inhibitors (TKIs), and PD-1 inhibitors has emerged as a potential strategy, real-world clinical data regarding its efficacy and safety in this subset of patients remain scarce.
Methods: This retrospective study enrolled 35 Vp4 HCC patients who received HAIC combine with TKI and PD-1 inhibitor. Treatment response was evaluated according to mRECIST and RECIST1.1. Survival outcomes including progression-free survival (PFS) and overall survival (OS) were analyzed using the Kaplan–Meier method, and independent prognostic factors were identified via Cox regression analyses.
Results: Of 35 patients (mean age 52.7 ± 8.3 years, 97.1% male, 97.1% HBV-infected), 37.1% had extrahepatic metastasis and 57.1% had ≥ 4 tumors. After a median follow-up of 313 days (IQR, 177.5– 464.5), the objective response rate (ORR) by mRECIST was 60.0%. Median OS and PFS were 313 days (95% CI: 257.5– 368.5) and 204 days (95% CI: 153.9– 254.1) respectively. Hepatic vein tumor thrombus/inferior vena cava tumor thrombus (HVTT/IVCTT) independently predicted worse PFS (HR = 2.860, p = 0.023) and OS (HR = 3.482, p = 0.007), and tumor number ≥ 4 predicted inferior OS (HR = 2.454, p = 0.020). Grade 3– 4 AEs occurred in 45.7% of patients, most commonly elevated AST (34.3%), with no grade 5 events.
Conclusion: The combination of HAIC, TKI, and PD-1 inhibitor demonstrates encouraging antitumor activity and a manageable safety profile in patients with Vp4 HCC, indicating its potential as an effective treatment option for this clinically challenging population.
Keywords: hepatocellular carcinoma, hepatic arterial infusion chemotherapy, portal vein
Introduction
Hepatocellular carcinoma (HCC) ranks as the fourth most common malignancy and the second leading cause of cancer-related mortality in China.1 More than 70% of HCC patients are diagnosed at an advanced stage, precluding curative treatment options such as liver transplantation, surgical resection, or ablation.2 Since the global SHARP trial in 2008 demonstrated that sorafenib—a tyrosine kinase inhibitor (TKI)—could modestly improve survival with a median overall survival (OS) of 10.7 months, it was approved as the first-line systemic therapy for advanced HCC.3 However, a subsequent Phase 3 study conducted in the Asia-Pacific region, where hepatitis B virus (HBV) infection is the predominant etiology, showed a lower response rate and a median OS of only 6.5 months.4 Portal vein tumor thrombus (PVTT) is a particularly poor prognostic factor, present in approximately 10–60% of HCC patients at diagnosis, and is associated with a median survival of 2.7–4.0 months in the absence of treatment.3
Recent advances in systemic therapy, including tyrosine kinase inhibitors (TKIs) and immune checkpoint inhibitors (ICIs), have led to the development of combination regimens such as bevacizumab plus atezolizumab, durvalumab plus tremelimumab, sintilimab plus bevacizumab biosimilar, and apatinib plus camrelizumab, which have shown promising efficacy in HCC.4–7Nevertheless, outcomes remain modest, with median OS ranging from 10 to 23 months in these studies. It should be noted that the proportion of patients with macrovascular invasion enrolled in these trials typically ranged from 15% to 38%. Extensive evidence has consistently identified macrovascular invasion as a significant adverse prognostic factor associated with poorer outcomes in HCC,8–10 and the efficacy of current systemic therapies in this subgroup remains unsatisfactory.
Among all types of PVTT, invasion of the main portal vein (designated as Vp4 in the Japanese Vp classification system) represents the most advanced and aggressive form.11–13 Patients with Vp4 PVTT face an extremely dismal prognosis due to rapid intrahepatic dissemination, impaired portal venous flow leading to deteriorating liver function and portal hypertension, and limited treatment options. Although novel combination systemic therapies represent a considerable advancement, their efficacy specifically in Vp4 patients remains suboptimal and poorly defined, often resulting in survival outcomes considerably lower than the median OS reported in broader advanced HCC cohorts.14
HAIC delivers high concentrations of cytotoxic agents directly into the liver via the tumor-feeding hepatic artery, potentially offering superior locoregional control, especially for tumors with vascular involvement.15,16 Emerging exploratory studies suggest that combining HAIC with systemic agents—such as TKIs and ICIs (particularly PD-1 inhibitors) that enhance antitumor immunity—may yield synergistic effects and improve outcomes.17,18 Preliminary reports have indicated promising efficacy and acceptable safety profiles for this triple combination (HAIC + TKI + PD-1 inhibitor) in advanced HCC, including subsets with vascular invasion.19 However, real-world evidence systematically evaluating the outcomes of this regimen specifically in the challenging subgroup of HCC patients with main portal vein invasion remains limited and insufficient to robustly guide clinical practice.
Therefore, we conducted this retrospective study to evaluate the efficacy and survival outcomes of triple therapy with HAIC, TKI, and PD-1 inhibitor in patients with hepatocellular carcinoma complicated by main portal vein tumor thrombus treated at our institution. We aimed to assess the objective response rate (ORR), progression-free survival (PFS), and overall survival (OS) associated with this combination strategy in this high-risk population.
Methods
Study Design and Patients
We retrospectively reviewed the medical records of patients with unresectable hepatocellular carcinoma (HCC) who were treated with transarterial interventional therapy—either HAIC or transcatheter arterial chemoembolization (TACE)—in combination with TKIs and PD-1 inhibitors at our institution between February 2019 and October 2023. Inclusion criteria: (1) age 18–75 years; (2) HCC diagnosis per AASLD criteria;20 (3) Vp4 portal vein invasion; (4) ≥1 measurable lesion (≥1 cm); (5) receipt of ≥1 cycle of HAIC + TKI + PD-1 inhibitor; (6) Child-Pugh class A or B; (7) ECOG PS 0–2; (8) adequate organ function, defined as: white blood cell count ≥ 3.0 × 109/L, platelet count ≥ 70 × 109/L, aspartate aminotransferase (AST) and alanine aminotransferase (ALT) ≤ 5 times the upper limit of normal, and serum creatinine ≤ 2.0 mg/dL. (9) Presence of extrahepatic metastasis was allowed. Exclusion criteria: (1) prior systemic therapy; (2) prior local therapy (eg, RFA, EBRT) within 4 weeks of initiating combination therapy; (3) lack of baseline imaging; (4) history of other malignancies; (5) interval >6 weeks between combination cycles; (6) active autoimmune disease requiring systemic treatment; (7) incomplete follow-up data.
By querying the Hospital Information System, we identified 169 consecutive patients with unresectable HCC(uHCC) who received transarterial interventional therapy combined with TKI and PD-1 inhibitor treatment during the specified period. The follow-up data cutoff was December 31, 2024. After applying the exclusion criteria, 134 patients were excluded, resulting in a final cohort of 35 patients Figure 1.Treatment strategies were discussed and recommended by a multidisciplinary team comprising hepatologists, surgeons, medical oncologists, radiation oncologists, radiologists, and pathologists. Final treatment decisions were made jointly by physicians and patients after detailed discussion.
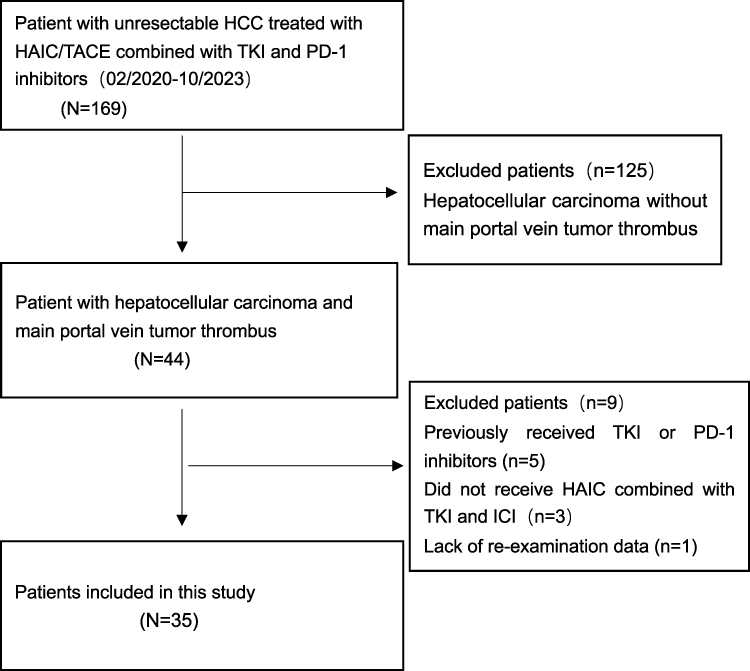 |
Figure 1 Flowchart of patient selection. Abbreviations:HCC, hepatocellular carcinoma; HAIC, hepatic arterial infusion chemotherapy; TACE, transarterial chemoembolization; TKI, tyrosine kinase inhibitor; PD-1, programmed cell death protein. |
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Specifically, the clinical study protocol of this research was reviewed and approved by the Ethics Committee of Fujian Cancer Hospital (K2025-380-01). The requirement for written informed consent was waived owing to the retrospective nature of the study and was approved by the Ethics Committee of Fujian Cancer Hospital.
The TKIs and PD-1 inhibitors used in this study included: Lenvatinib (Beacon Pharmaceuticals Ltd., Japan); Sorafenib (Bayer Healthcare Pharmaceuticals Inc., Germany); Donafenib (Suzhou Zelgen Biopharmaceuticals Co., Ltd., China); Apatinib (Jiangsu Hengrui Medicine Co., Ltd., China); Sintilimab (Innovent Biologics Inc., China); Camrelizumab (Jiangsu Hengrui Medicine Co., Ltd., China); Tislelizumab (BeiGene Ltd., China); Pembrolizumab (Merck Sharp & Dohme Corp., USA).
Hepatic Arterial Infusion Chemotherapy
HAIC procedures were performed by experienced interventional radiologists. In brief, each procedure involved the temporary placement of an arterial catheter. Using the Seldinger technique, the coaxial microcatheter was superselectively positioned within the tumor-feeding artery to cover the distribution of the hepatic tumors.In patients with dual blood supply from both the superior mesenteric artery and the celiac trunk, the feeding artery supplying the hepatic lobe with lesser tumor burden was selected for embolization to redirect flow, while the catheter was positioned in the artery supplying the lobe with greater tumor burden for infusion. For HCCs with extrahepatic collateral supply, such as from the phrenic or internal thoracic arteries, these feeding vessels were embolized. The embolic agents used lipiodol, followed by gelatin sponge particles. The size of the gelatin sponge particles (available in 150–350, 350–560, and 560–750 μm) was selected based on the diameter of the super-selected feeding artery and the tumor size.Two HAIC drug regimens were utilized: (1) Oxaliplatin-based regimen: Oxaliplatin (100 mg/m2), administered as a 4-hour continuous infusion, followed by raltitrexed (3 mg/m2) as a 1-hour infusion.21 (2) Lobaplatin-based regimen: Lobaplatin (40 mg/m2), administered as a 2-hour continuous infusion, followed by raltitrexed (3 mg/m2) as a 1-hour infusion.Treatments were repeated at 3-week intervals.
Systemic Therapy Administration
Lenvatinib was administered orally at a dose of 12 mg once daily for patients with a body weight ≥ 60 kg, or 8 mg once daily for those weighing < 60 kg. Apatinib was administered at 250 mg once daily, sorafenib at 400 mg twice daily, and donafenib at 200 mg twice daily. Oral TKI therapy was continued uninterrupted before and after each HAIC session. Doses of TKIs were adjusted or temporarily discontinued based on the severity of adverse events, in accordance with established clinical management guidelines. Additionally, all patients received intravenous PD-1 inhibitors at a flat dose of 200 mg every 3 weeks. This systemic combination therapy was initiated either within six weeks before or after the first HAIC procedure and was continued until disease progression, development of unacceptable toxicity, or patient decision to withdraw from treatment.
Follow-Up and Efficacy Assessment
Study participants underwent regular follow-up assessments at our institution. Each visit included a comprehensive review of medical history, physical examination, and laboratory investigations comprising complete blood count, alpha-fetoprotein level, liver and renal function tests, electrolyte panel, thyroid function tests, and prothrombin time. Radiological evaluation consisted of contrast-enhanced triple-phase computed tomography (CT) or magnetic resonance imaging (MRI) of the upper abdomen and non-contrast chest CT.
Following the completion of two cycles of HAIC, follow-up evaluations were scheduled at 6- to 8-week intervals. HAIC treatment was continued until disease progression, unacceptable toxicity, or patient withdrawal of consent, with a maximum of six cycles administered. For patients exhibiting significant tumor regression, eligibility for subsequent therapies—including surgical resection, ablation, external beam radiotherapy, or Iodine-125 seed implantation—was evaluated through multidisciplinary team (MDT) discussion. Conversely, in cases of confirmed disease progression, alternative strategies were considered, such as switching to a second-line tyrosine kinase inhibitor (TKI), administering alternative immune checkpoint inhibitors (eg, targeting PD-L1 or CTLA-4), or enrollment in clinical trials investigating novel therapeutic agents.
Tumor response was assessed based on the best response recorded prior to any subsequent treatment and was independently evaluated by two interventional radiologists according to both Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 and modified RECIST (mRECIST). Any discrepancies were resolved by consensus. During systemic maintenance therapy, follow-up was conducted at 2-month intervals. The objective response rate (ORR) was defined as the proportion of patients achieving a complete or partial response, and the disease control rate (DCR) as the proportion with complete response, partial response, or stable disease. Overall survival (OS) was measured from treatment initiation until death or the last follow-up. Progression-free survival (PFS) was defined as the time from the first treatment to radiological progression, death, or the last follow-up. Adverse events (AEs) were graded according to the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0.
Statistical Analyses
Continuous variables were described as mean ± standard deviation or as median and range, as appropriate. Categorical variables were summarized as frequencies and percentages. Comparisons between groups for categorical variables were performed using the Chi-square test or Fisher’s exact test, as applicable. The Wilcoxon rank-sum test was used for comparing continuous variables or ordinal data between two independent groups.Survival curves were plotted using the Kaplan–Meier method and compared with the Log rank test. Univariate analysis was conducted using Cox proportional hazards models. Variables with a P value ≤ 0.10 in the univariate analysis were included in the multivariate Cox regression model. A two-sided P value < 0.05 was considered statistically significant. All analyses were performed using IBM SPSS Statistics version 29.0 (IBM Corp., Armonk, NY, USA).
Result
Basline Patient Characteristics
A total of 35 patients were included in the final analysis. The baseline clinical characteristics of the patients are summarized in Table 1. The mean age was 52.7 ± 8.3 years, and 7 patients (20.0%) were aged 60 years or older. The majority were male (97.1%, n = 34) and had hepatitis B virus (HBV) infection (97.1%, n = 34). Elevated HBV-DNA levels (≥500 IU/mL) were observed in 19 patients (54.3%). According to liver function assessment, 21 patients (60.0%) were Child–Pugh class A and 14 (40.0%) were class B. Most patients had an Eastern Cooperative Oncology Group performance status (ECOG PS) of 1 (65.7%, n = 23), and 31 (88.6%) were classified as ALBI grade 2. Regarding tumor burden, 19 patients (54.3%) had a maximum tumor diameter ≥10 cm, 20 (57.1%) had ≥4 nodules, and 9 (25.7%) exhibited hepatic vein/inferior vena cava tumor thrombosis. Extrahepatic spread was present in 13 patients (37.1%), and 26 (74.3%) had alpha-fetoprotein (AFP) levels ≥400 ng/mL.
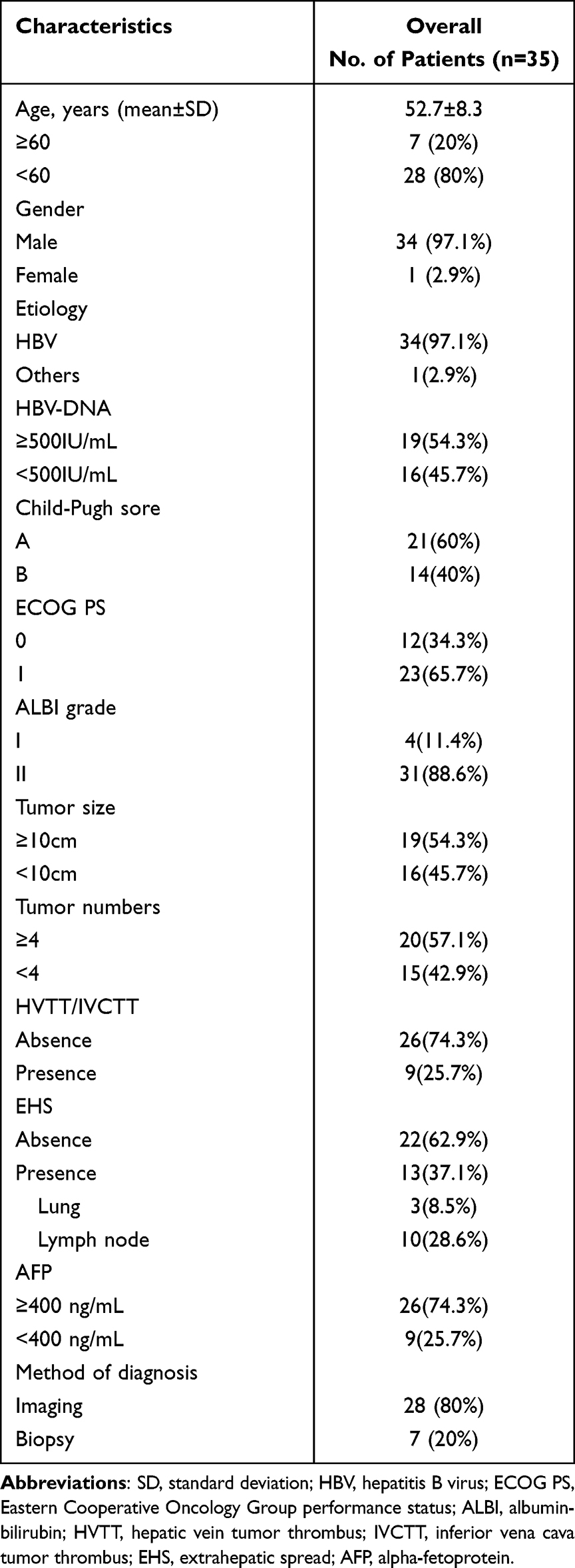 |
Table 1 Baseline Demographic and Clinicopathological Characteristics of the Enrolled Patients (N= 35) |
Treatment Regimens and Follow-Up
Treatment details are presented in Table 2. All patients received combination therapy consisting of a TKI, a PD-1 inhibitor, and HAIC. The most commonly used TKI was lenvatinib (42.9%, n = 15), followed by donafenib (28.6%, n = 10), apatinib (22.9%, n = 8), and sorafenib (5.7%, n = 2). The median duration of TKI treatment was 178 days (interquartile range [IQR], 113–293). Among PD-1 inhibitor, tislelizumab was administered to 12 patients (34.3%), camrelizumab to 11 (31.4%), sintilimab to 11 (31.4%), and pembrolizumab to 1 (2.9%), with a median of 4 cycles (IQR, 3–9) administered per patient. An oxaliplatin-based HAIC regimen was used in 23 patients (65.7%), while a lobaplatin-based regimen was employed in 12 (34.3%), with a median of 4 cycles (IQR, 2–5) delivered. Subsequent-line therapy was received by 17 patients (48.6%). The median follow-up time was 313 days (IQR, 177.5–464.5).
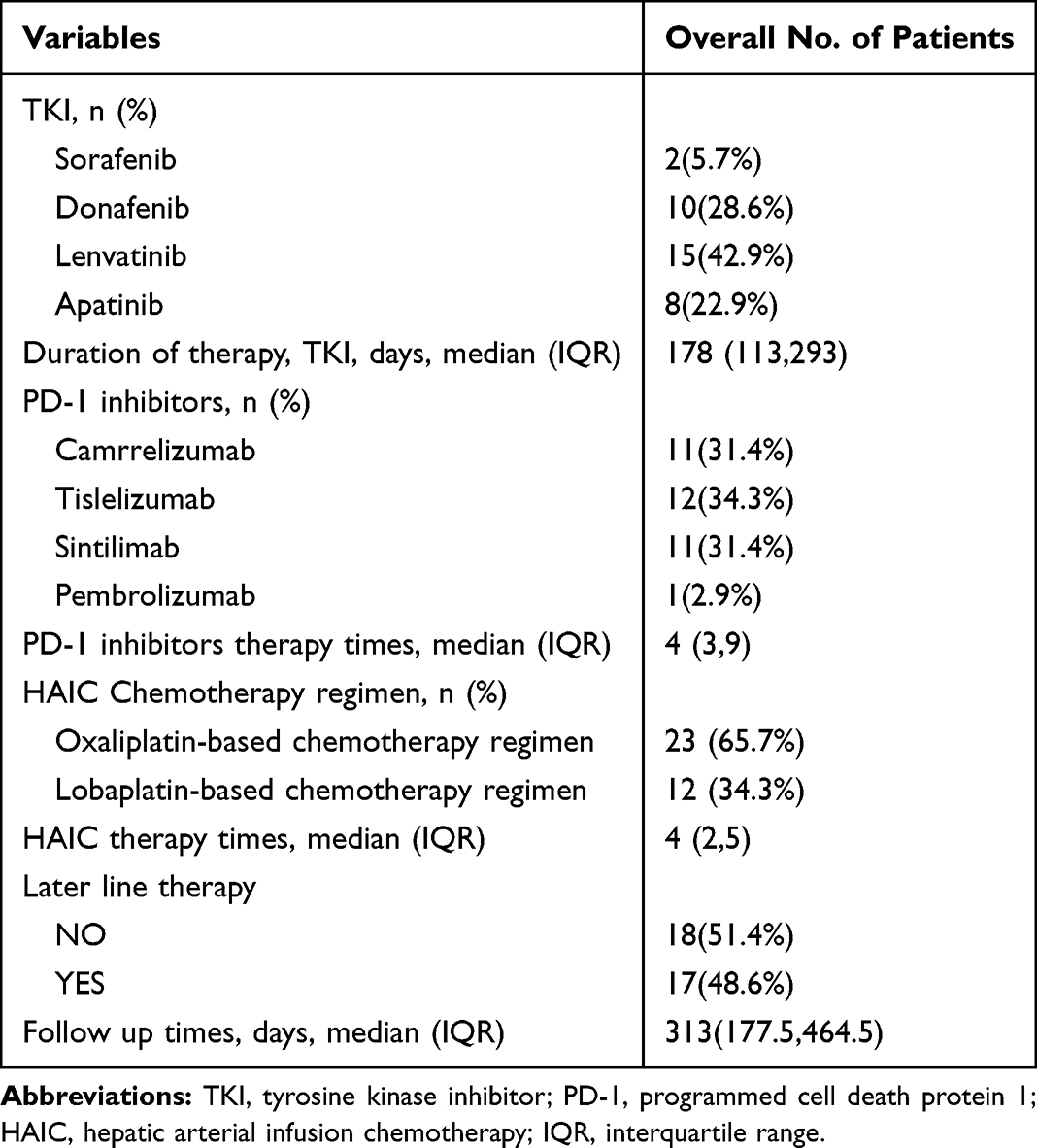 |
Table 2 Treatment Regimens and Follow-Up Characteristics |
Tumor Response
When assessed by mRECIST criteria, ORR was 60.0% (21/35 patients), CR in 5.7% (2 patients) and PR in 54.3% (19 patients) Figure 2. Using RECIST 1.1 criteria, the ORR was 57.2% (20/35 patients), with CR in 2.9% (1 patient) and PR in 54.3% (19 patients) Figure 3. No significant difference in ORR was observed between the two assessment methods (p=0.808). The DCR was identical at 82.9% (29/35 patients) for both criteria (p=1.000). The overall distribution of best response categories (CR, PR, SD, PD) showed no statistically significant variation between mRECIST and RECIST 1.1 classifications (p=0.756) Table 3.
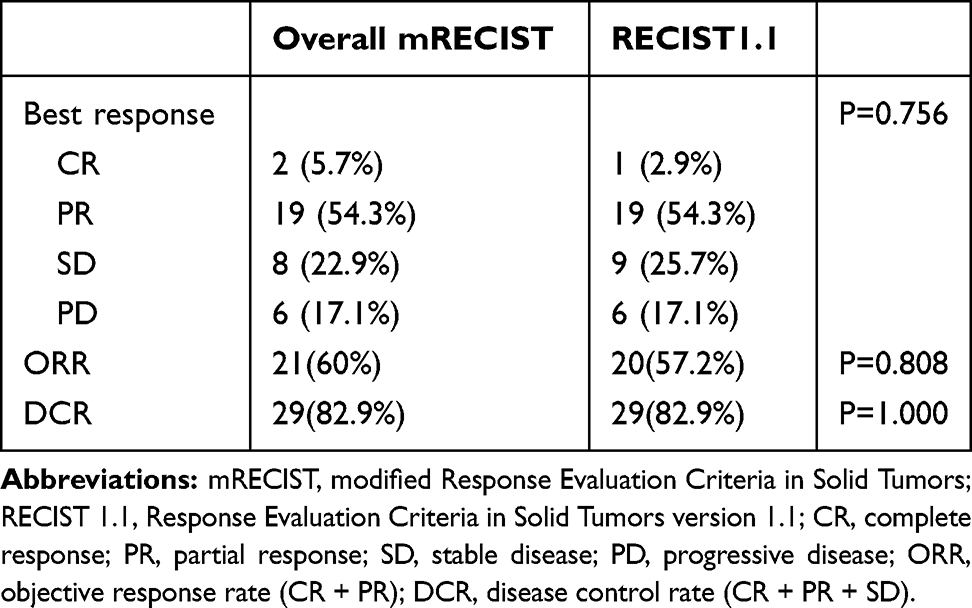 |
Table 3 Tumor Response Assessed per mRECIST and RECIST 1.1 Criteria |
 |
Figure 2 Waterfall Plot Depicting Best Response in Patients Receiving HAIC Combined with TKI and PD-1 Inhibitor Therapy (by mRECIST). Abbreviations: CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease. |
 |
Figure 3 Waterfall Plot Depicting Best Response in Patients Receiving HAIC Combined with TKI and PD-1 Inhibitor Therapy (by RECIST 1.1). Abbreviations: CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease. |
Survival Analysis
The median PFS was 204 days (95% CI: 153.9–254.1) Figure 4. The median overall survival OS was 313 days (95% CI: 257.5–368.5) Figure 5. The 180-, 360-, and 540-day overall survival rates were71.4%, 37.1%, and 17.1%, respectively.
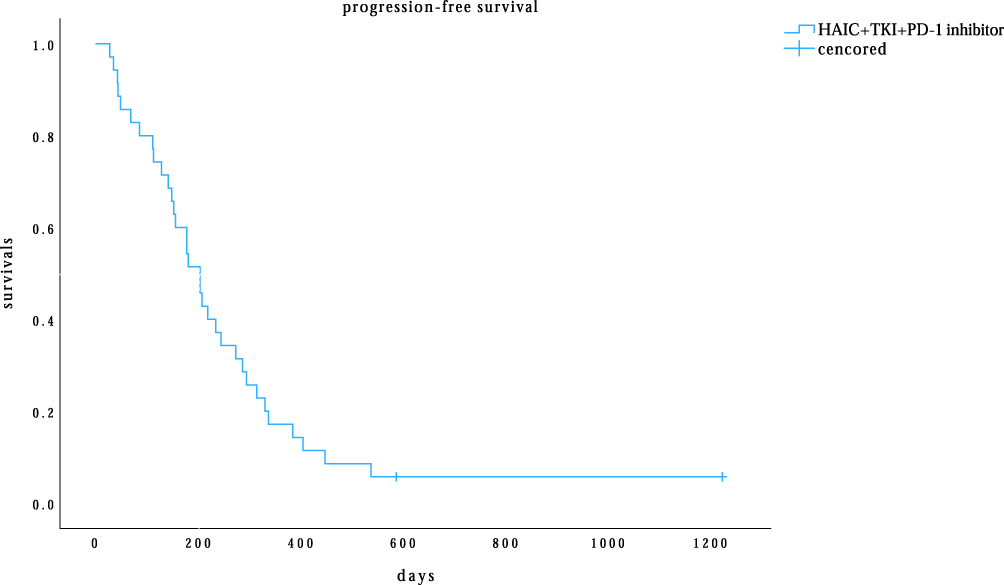 |
Figure 4 Kaplan–Meier curves for progression-free survival (PFS) in patients receiving triple therapy (HAIC plus TKI and PD-1 inhibitor). Abbreviations: HAIC, hepatic arterial infusion chemotherapy; TKI, tyrosine kinase inhibitor; PD-1, programmed death protein 1; PFS, progression-free survival. |
 |
Figure 5 Kaplan–Meier curve for overall survival (OS) in patients treated with HAIC combined with TKI and PD-1 inhibitor. Abbreviations: HAIC, hepatic arterial infusion chemotherapy; TKI, tyrosine kinase inhibitor; PD-1, programmed cell death protein 1; OS, overall survival. |
Prognostic Factor Analysis
For PFS, univariate Cox regression analysis identified HVTT/IVCTT as a significant predictor of reduced PFS (HR: 3.046, 95% CI: 1.239–7.486, p= 0.015). Tumor number ≥4 demonstrated a borderline significant association with worse PFS (HR: 1.946, 95% CI: 0.954–3.970, p = 0.067) and was therefore included in the multivariate model. Multivariate analysis confirmed HVTT/IVCTT as an independent adverse prognostic factor for PFS (HR: 2.860, 95% CI: 1.158–7.062, p = 0.023), while tumor number ≥4 showed a persistent but non-significant trend toward poorer outcomes (HR: 1.838, 95% CI: 0.896–3.770, p = 0.097) Table 4.
 |
Table 4 Univariate and Multivariate Cox Regression Analyses of Factors Associated with Progression-Free Survival (PFS) |
For OS, univariate analysis identified both HVTT/IVCTT (HR: 3.867, 95% CI: 1.560–9.587, p = 0.004) and tumor number ≥4 (HR: 2.625, 95% CI: 1.236–5.576, p = 0.012) as significant predictors of reduced survival. Both factors met the predefined threshold (p ≤ 0.10) for inclusion in the multivariate analysis. Multivariate analysis confirmed HVTT/IVCTT (HR: 3.482, 95% CI: 1.417–8.557, p = 0.007) and tumor number ≥4 (HR: 2.454, 95% CI: 1.150–5.239, p = 0.020) as independent adverse prognostic factors for OS Table 5.
 |
Table 5 Univariate and Multivariate Cox Regression Analyses of Prognostic Factors for Overall Survival (OS) |
Safety Profile
In the cohort receiving combination therapy with HAIC, TKI, and PD-1 inhibitor (n = 35), treatment-related adverse events (TRAEs) were reported in 34 patients (97.1%). The most frequent any-grade TRAEs included elevated aspartate aminotransferase (AST) (77.1%, n = 27), elevated alanine aminotransferase (ALT) (65.7%, n = 23), and thrombocytopenia (37.1%, n = 13). Grade 3 or 4 TRAEs occurred in 16 patients (45.7%). The most common severe toxicities were elevated transaminases (grade 3 AST elevation: 34.3%; grade 3 ALT elevation: 11.4%) and hematological events (grade 3 thrombocytopenia: 5.7%). One case (2.9%) of grade 4 immune-mediated hepatitis was observed. No treatment-related deaths (grade 5) occurred Table 6.
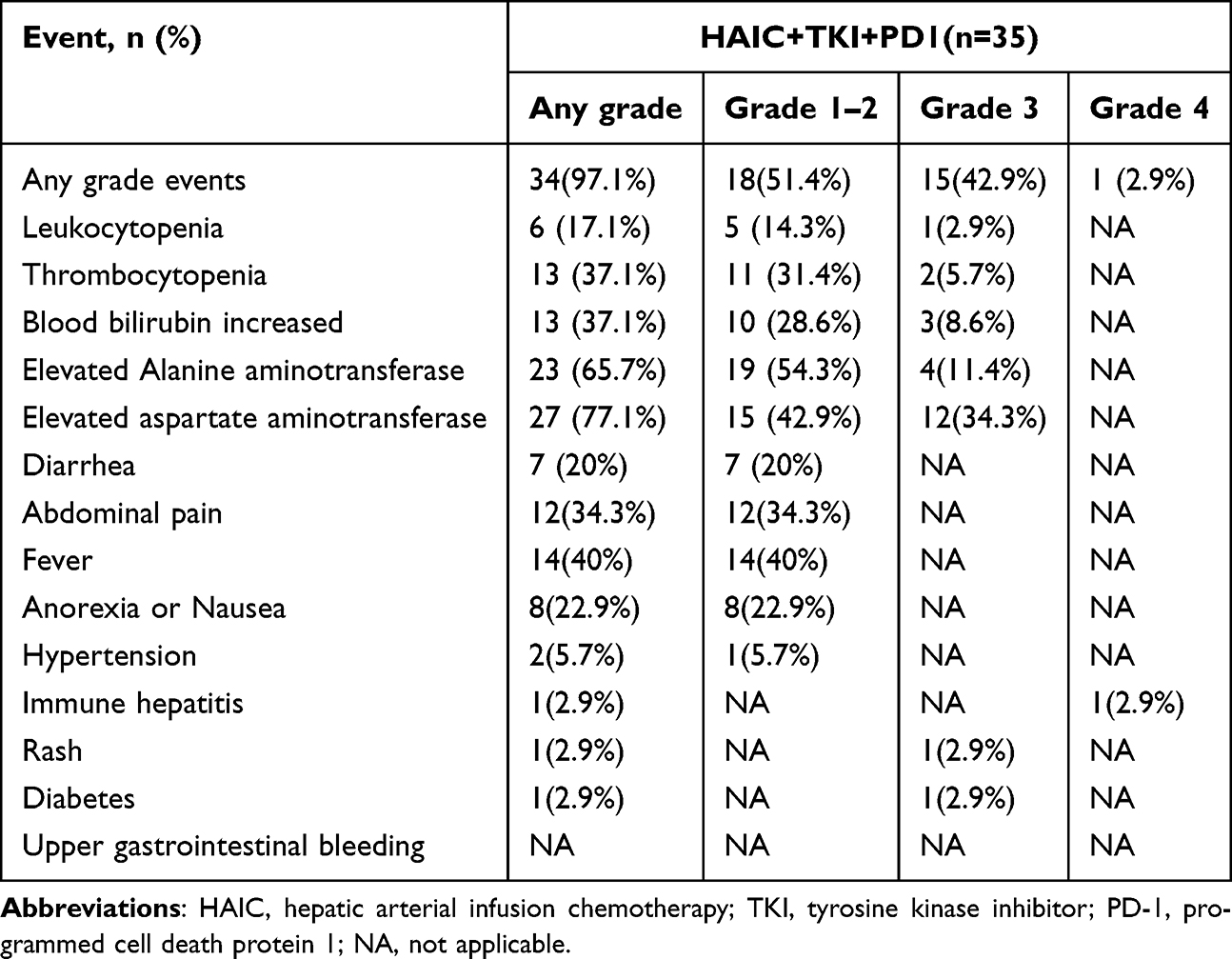 |
Table 6 Treatment-Related Adverse Events in Patients Receiving HAIC Combined with TKI and PD-1 Inhibitor |
Discussion
This retrospective study analyzed 35 patients with HCC complicated by main portal vein tumor thrombus (Vp4) who were treated with a triple therapy combination of HAIC, TKIs, and PD-1 inhibitors. The results demonstrated promising antitumor activity and survival benefits with a manageable safety profile in this population with an otherwise exceedingly poor prognosis.
In this study, the triple therapy yielded ORR as high as 60.0% and 57.2% according to mRECIST and RECIST 1.1 criteria, respectively, and a DCR of 82.9%. This high response rate is notably superior to the efficacy data historically reported for single-agent targeted therapy or TACE in similar advanced HCC populations.3,22 Evidence indicates that adding a PD‑1 inhibitor to combination regimens markedly improves the objective response rate in advanced hepatocellular carcinoma. For high‑risk patients, FOLFOX-based HAIC combined with TKI and a PD‑1 inhibitor achieved an ORR of 57.7% versus 28.9% with TKI plus PD‑1 inhibitor.23 Likewise, in patients with portal vein tumor thrombosis, incorporating the inhibitor into HAIC‑TKI therapy elevated the ORR from 51.3% to 66.3%.24 We postulate that the underlying mechanism is likely attributed to synergistic effects among the three treatment modalities. HAIC delivers high local concentrations of cytotoxic agents, directly targeting the tumor and inducing immunogenic cell death. This process is characterized by the release of tumor antigens, calreticulin (CRT) exposure on the cell surface, and secretion of damage-associated molecular patterns such as HMGB1 and ATP.19 These signals facilitate dendritic cell maturation and promote the activation and infiltration of tumor-specific CD8⁺ T cells. Concurrently, TKIs inhibit angiogenesis and promote vascular normalization, which may enhance intra-tumoral drug delivery, and ameliorate the immunosuppressive tumor microenvironment.25,26 Furthermore, anti-PD-1 therapy reverses T-cell exhaustion and augments pre-existing antitumor immunity. Notably, the combination of antiangiogenic agents with PD-1 blockade has been shown to enhance T-cell function and immune checkpoint activation, resulting in superior antitumor immunity compared to PD-1 inhibition alone.27,28 This multipronged strategy of “local cytotoxicity + vascular normalization + immune activation” likely underlies the high objective response rate observed.
Regarding survival outcomes, the median PFS and OS in this cohort were 204 days and 313 days, respectively. It is noteworthy that these results were achieved in a population with predominantly high-risk features, including main portal vein invasion (Vp4)—which itself carries a median natural history of only 2.7–4 months3—as well as high tumor burden (54.3% with tumors ≥10 cm; 57.1% with ≥4 nodules) and extrahepatic spread (37.1%). Notably, a recent study documented median PFS and OS of only 101 days and 201 days, respectively, with lenvatinib alone in a cohort with Vp4 invasion,29 results which are markedly inferior to those achieved with our combination regimen. Despite these adverse baseline characteristics, our strategy conferred a clinically meaningful survival advantage. These findings align with emerging evidence supporting combination strategies in advanced hepatocellular carcinoma with aggressive features. Long et al30 demonstrated that HAIC combined with TKIs and PD-1 inhibitors significantly improved progression-free survival in patients with hepatocellular carcinoma and high tumor burden or vascular invasion. This is in contrast to the notably prolonged OS (23.2 months) and PFS (6.6 months) reported in the study by Tang et al,31 which employed a combination of HAIC, lenvatinib, and tislelizumab in a patient population with a more favorable liver functional reserve. The comparatively shorter overall survival observed in our study, despite a similar PFS, is likely attributable to the higher proportion of patients with impaired liver function and extrahepatic metastases in our cohort. For patients with portal vein tumor thrombosis in the main trunk (VP3/4), triple therapy with mFOLFOX-HAIC, TKI, and an immune checkpoint inhibitor yielded a median overall survival of 15.8 months. Notably, the cohort included a higher proportion of patients with VP3 disease (23 of 37 patients, 62%), which may contribute to the favorable survival outcome.32
Collectively, these studies—along with the present analysis—suggest that HAIC-based combination regimens may exhibit synergistic efficacy and represent a promising therapeutic alternative for high-risk HCC patients.33 Nevertheless, further validation through larger, prospective studies is warranted to confirm these observations and refine patient selection.
Multivariate Cox regression analysis further confirmed that HVTT/IVCTT and tumor number ≥4 were independent adverse prognostic factors for OS, a finding that aligns with established literature.34,35 The presence of HVTT/IVCTT represents a critical turning point in disease progression, not only signifying aggressive tumor biology but also portending a markedly increased risk of distant metastasis, particularly pulmonary dissemination, due to direct drainage into the systemic circulation.36 This anatomic distinction differentiates it from PVTT and underscores a more dismal prognosis, as it effectively renders the disease a systemic process and traditionally disqualifies patients from potentially curative surgical interventions such as resection or transplantation. Similarly, a tumor number ≥4 is a robust surrogate for extensive intrahepatic tumor burden and signifies a high likelihood of microvascular invasion and intrahepatic metastasis, posing a significant challenge to local-regional control by any modality, including surgery or ablation. The concurrence of these factors delineates a patient subgroup with a particularly aggressive disease phenotype.Nevertheless, within this cohort of patients bearing these high-risk features, our triple therapy regimen still provided a meaningful survival opportunity.
In terms of safety, although the incidence of treatment-related adverse events was high (97.1%), the vast majority were Grade 1–2 and manageable. The incidence of Grade 3–4 TRAEs was 45.7%, primarily comprising elevated transaminases and thrombocytopenia, which is consistent with the known overlapping toxicity profiles of HAIC, TKIs, and immunotherapy. Notably, despite the theoretical concern for upper gastrointestinal bleeding in this high-risk patient population with Vp4 portal vein tumor thrombus, no major bleeding events were observed in our cohort. It is plausible that successful treatment leading to tumor thrombus regression could potentially reduce portal pressure, thereby mitigating the underlying bleeding risk. No unexpected new safety signals were identified. One case of Grade 4 immune-mediated hepatitis improved after appropriate management, and no treatment-related deaths occurred. This indicates that the safety profile of this triple regimen is overall manageable in experienced centers.
This study, however, has several limitations: Firstly, it is a single-center, retrospective study with a limited sample size, which may introduce selection bias; secondly, the specific TKI and PD-1 inhibitors used were not uniform, which, although a reasonable choice in clinical practice, might introduce slight heterogeneity in the outcomes; finally, the lack of a direct comparison with standard treatments (such as sorafenib monotherapy or other dual combinations) limits the strength of the conclusions. Therefore, these findings require further validation in prospective, large sample, randomized controlled trials.
Conclusion
In conclusion, for patients with advanced hepatocellular carcinoma complicated by main portal vein tumor thrombus, the triple therapy combining HAIC, TKI, and a PD-1 inhibitor demonstrated a high objective response rate and encouraging survival benefits, with a manageable safety profile. These results offer a potential new treatment strategy for this patient population with a very poor prognosis. Future efforts should focus on optimizing treatment combinations and sequences, and conducting prospective studies to confirm its efficacy.
Acknowledgments
The authors thank everyone at our institution who helped with this study.
Funding
This work was supported by the National Key R&D Program of China (No. 2023YFC2413500),Joint Funds for the innovation of science and Technology,Fujian province (Grant number: 2023Y9320),Fujian Province Natural Science,Fund Project(2024J011105),Sponsored by Fujian provincial health technology project (grant no. 2024ZD01004),the Special Research Foundation of Fujian Provincial Department of Finance(2024-881#).
Disclosure
The authors declare no competing interests.
References
1. Xia C, Dong X, Li H, et al. Cancer statistics in China and United States, 2022: profiles, trends, and determinants. Chin Med J. 2022;135(5):584–14. doi:10.1097/CM9.0000000000002108
2. Peng Z, Fan W, Zhu B, et al. Lenvatinib combined with transarterial chemoembolization as first-line treatment for advanced hepatocellular carcinoma: a phase iii, randomized clinical trial (LAUNCH). J Clin Oncol. 2023;41(1):117–127. doi:10.1200/JCO.22.00392
3. Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359(4):378–390. doi:10.1056/NEJMoa0708857
4. Ren Z, Xu J, Bai Y, et al. Sintilimab plus a bevacizumab biosimilar (IBI305) versus sorafenib in unresectable hepatocellular carcinoma (ORIENT-32): a randomised, open-label, Phase 2-3 study. Lancet Oncol. 2021;22(7):977–990. doi:10.1016/S1470-2045(21)00252-7
5. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382(20):1894–1905. doi:10.1056/NEJMoa1915745
6. Qin S, Chan SL, Gu S, et al. Camrelizumab plus rivoceranib versus sorafenib as first-line therapy for unresectable hepatocellular carcinoma (CARES-310): a randomised, open-label, international phase 3 study. Lancet. 2023;402(10408):1133–1146. doi:10.1016/S0140-6736(23)00961-3
7. Kelley RK, Sangro B, Harris W, et al. Safety, efficacy, and pharmacodynamics of tremelimumab plus durvalumab for patients with unresectable hepatocellular carcinoma: randomized expansion of a phase i/ii study. J Clin Oncol. 2021;39(27):2991–3001. doi:10.1200/JCO.20.03555
8. Zavaglia C, De Carlis L, Alberti AB, et al. Predictors of long-term survival after liver transplantation for hepatocellular carcinoma. Am J Gastroenterol. 2005;100(12):2708–2716. doi:10.1111/j.1572-0241.2005.00289.x
9. Grazi GL, Cescon M, Ravaioli M, et al. Liver resection for hepatocellular carcinoma in cirrhotics and noncirrhotics. Evaluation of clinicopathologic features and comparison of risk factors for long-term survival and tumour recurrence in a single centre. Aliment Pharmacol Ther. 2003;17(2):119–129. doi:10.1046/j.1365-2036.17.s2.9.x
10. Welland S, Leyh C, Finkelmeier F, et al. Real-world data for lenvatinib in hepatocellular carcinoma (elevator): a retrospective multicenter study. Liver Cancer. 2022;11(3):219–232. doi:10.1159/000521746
11. Finn RS, Galle PR, Ducreux M, et al. Efficacy and safety of atezolizumab plus bevacizumab versus sorafenib in hepatocellular carcinoma with main trunk and/or contralateral portal vein invasion in IMbrave150. Liver Cancer. 2024;13(6):655–668. doi:10.1159/000539897
12. Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 2018;391(10127):1301–1314. doi:10.1016/S0140-6736(18)30010-2
13. Schoniger-Hekele M, Müller C, Kutilek M, et al. Hepatocellular carcinoma in Central Europe: prognostic features and survival. Gut. 2001;48(1):103–109. doi:10.1136/gut.48.1.103
14. Yu W, Liu W, Zhang K, et al. Transarterial interventional therapy combined with tyrosine kinase inhibitors with or without anti-PD-1 antibodies as initial treatment for hepatocellular carcinoma with major portal vein tumor thrombosis: a single-center retrospective study. Cancer Immunol Immunother. 2023;72(11):3609–3619. doi:10.1007/s00262-023-03511-6
15. Zhao M, Guo Z, Zou Y-H, et al. Arterial chemotherapy for hepatocellular carcinoma in China: consensus recommendations. Hepatol Int. 2023;18:4–31. doi:10.1007/s12072-023-10599-6
16. Lyu N, Wang X, Li J-B, et al. Arterial chemotherapy of oxaliplatin plus fluorouracil versus sorafenib in advanced hepatocellular carcinoma: a biomolecular exploratory, randomized, phase iii trial (FOHAIC-1). J Clin Oncol. 2022;40(5):468–480. doi:10.1200/JCO.21.01963
17. Shen L, Cao F, Liu Y, et al. Hepatic artery infusion of FOLFOX chemotherapy plus camrelizumab combined with sorafenib for advanced hepatocellular carcinoma in barcelona clinic liver cancer stage C (Double-IA-001): a Phase II trial. BMC Med. 2025;23(1):275. doi:10.1186/s12916-025-04110-1
18. Zhong S, Yi J, Chen S, et al. Combining immune checkpoint inhibitors and molecular-targeted agents with hepatic arterial infusion chemotherapy for hepatocellular carcinoma with inferior vena cava and/or right atrium tumor thrombus. Hepatol Int. 2025;19(3):560–575. doi:10.1007/s12072-025-10777-8
19. Zuo M, Cao Y, Yang Y, et al. Hepatic arterial infusion chemotherapy plus camrelizumab and apatinib for advanced hepatocellular carcinoma. Hepatol Int. 2024;18(5):1486–1498. doi:10.1007/s12072-024-10690-6
20. Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the American Association for the Study of Liver Diseases. Hepatology. 2018;68(2):723–750. doi:10.1002/hep.29913
21. Chen S, Yuan B, Yu W, et al. Comparison of arterial infusion chemotherapy and chemoembolization for locally advanced hepatocellular carcinoma: a multicenter retrospective study. J Gastrointest Surg. 2022;26(11):2292–2300. doi:10.1007/s11605-022-05421-x
22. Zhang XB, Wang J-H, Yan Z-P, et al. Hepatocellular carcinoma with main portal vein tumor thrombus: treatment with 3-dimensional conformal radiotherapy after portal vein stenting and transarterial chemoembolization. Cancer. 2009;115(6):1245–1252. doi:10.1002/cncr.24139
23. Zuo M, Zheng G, Cao Y, et al. Hepatic arterial chemotherapy infusion combined with tyrosine kinase inhibitors and PD-1 inhibitors for advanced hepatocellular carcinoma with high risk: a propensity score matching study. Int J Surg. 2025;111(1):104–112. doi:10.1097/JS9.0000000000001940
24. Cao F, Wen C, Wang Y, et al. PD-1 inhibitor-augmented HAIC-TKI therapy in hepatocellular carcinoma with portal vein tumor thrombosis: real-world survival benefits, safety, and subgroup-specific efficacy. Front Immunol. 2025;16:1602031. doi:10.3389/fimmu.2025.1602031
25. Une N, Takano-Kasuya M, Kitamura N, et al. The anti-angiogenic agent lenvatinib induces tumor vessel normalization and enhances radiosensitivity in hepatocellular tumors. Med Oncol. 2021;38(6):60. doi:10.1007/s12032-021-01503-z
26. Tzeng HT, Huang YJ. Tumor vasculature as an emerging pharmacological target to promote anti-tumor immunity. Int J Mol Sci. 2023;24(5):4422. doi:10.3390/ijms24054422
27. Sangro B, Kudo M, Erinjeri JP, et al. Durvalumab with or without bevacizumab with transarterial chemoembolisation in hepatocellular carcinoma (EMERALD-1): a multiregional, randomised, double-blind, placebo-controlled, phase 3 study. Lancet. 2025;405(10474):216–232. doi:10.1016/S0140-6736(24)02551-0
28. Sangro B, Chan SL, Kelley RK, et al. Four-year overall survival update from the phase III HIMALAYA study of tremelimumab plus durvalumab in unresectable hepatocellular carcinoma. Ann Oncol. 2024;35(5):448–457. doi:10.1016/j.annonc.2024.02.005
29. Chuma M, Uojima H, Hiraoka A, et al. Analysis of efficacy of lenvatinib treatment in highly advanced hepatocellular carcinoma with tumor thrombus in the main trunk of the portal vein or tumor with more than 50% liver occupation: a multicenter analysis. Hepatol Res. 2021;51(2):201–215. doi:10.1111/hepr.13592
30. Long T, Yang Z, Zeng H, et al. Comparable clinical outcomes between transarterial chemoembolization or hepatic arterial infusion chemotherapy combined with tyrosine kinase inhibitors and pd-1 inhibitors in unresectable hepatocellular carcinoma. J Hepatocell Carcinoma. 2023;10:1849–1859. doi:10.2147/JHC.S436211
31. Tang S, Shi F, Xiao Y, et al. HAIC plus lenvatinib and tislelizumab for advanced hepatocellular carcinoma with Vp4 portal vein invasion. Hepatol Int. 2025;19(1):106–117. doi:10.1007/s12072-024-10762-7
32. Liu Q, Zhang Y, Zhang J, et al. Efficacy and safety of hepatic arterial infusion chemotherapy combined with tyrosine kinase inhibitors and immune checkpoint inhibitors in the treatment of advanced hepatocellular carcinoma with portal vein tumor thrombosis in the main trunk. Front Oncol. 2024;14:1374149. doi:10.3389/fonc.2024.1374149
33. Chang X, Li X, Sun P, et al. HAIC Combined with lenvatinib plus PD-1 versus lenvatinib Plus PD-1 in patients with high-risk advanced HCC: a real-world study. BMC Cancer. 2024;24(1):480. doi:10.1186/s12885-024-12233-6
34. Mahringer-Kunz A, Meyer FI, Hahn F, et al. Hepatic vein tumor thrombosis in patients with hepatocellular carcinoma: prevalence and clinical significance. United Eur Gastroenterol J. 2021;9(5):590–597. doi:10.1002/ueg2.12098
35. Yamakado K, Miyayama S, Hirota S, et al. Subgrouping of intermediate-stage (BCLC stage B) hepatocellular carcinoma based on tumor number and size and Child-Pugh grade correlated with prognosis after transarterial chemoembolization. Jpn J Radiol. 2014;32(5):260–265. doi:10.1007/s11604-014-0298-9
36. Kanda M, Tateishi R, Yoshida H, et al. Extrahepatic metastasis of hepatocellular carcinoma: incidence and risk factors. Liver Int. 2008;28(9):1256–1263. doi:10.1111/j.1478-3231.2008.01864.x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.