Back to Journals » Cancer Management and Research » Volume 18

A Retrospective Study of a Postoperative Inflammation-Based Score for Predicting Disease-Free Survival in Locally Advanced Rectal Cancer After Neoadjuvant Chemoradiotherapy
Authors Yang Q, Li J, Ding L, Feng L, Chen S, Liu Y, Zhou Z
Received 25 November 2025
Accepted for publication 17 February 2026
Published 4 March 2026 Volume 2026:18 579958
DOI https://doi.org/10.2147/CMAR.S579958
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Kattesh Katti
Qiao Yang,1,* Ji Li,1,* Ling Ding,1,* Li Feng,1 Sisi Chen,1 Yong Liu,2 Zili Zhou1
1Department of Gastroenterology, Sichuan Second Hospital of Traditional Chinese Medicine, Chengdu, Sichuan, People’s Republic of China; 2Department of Gastroenterology, West China Hospital of Sichuan University, Chengdu, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zili Zhou, Email [email protected]
Background: Growing research findings highlight the potential of inflammatory markers measured after surgery as prognostic indicators for survival outcomes in rectal carcinoma patients. However, their precise clinical significance remains inadequately explored within the specific population of locally advanced rectal carcinoma (LARC) patients receiving neoadjuvant chemoradiotherapy (NCRT), particularly regarding therapeutic response evaluation and long-term disease progression patterns.
Methods: This investigation enrolled 260 participants diagnosed with LARC who underwent NCRT from 2014 to 2024. The study measured postoperative neutrophil-lymphocyte ratio (NLR) and monocyte-lymphocyte ratio (MLR) through ROC curve analysis to evaluate systemic inflammation. Participants were categorized into three cohorts based on inflammation-based postoperative biomarker score (IPBS): Score 0 (postoperative NLR < 3.21 with MLR < 0.345), Score 2 (NLR > 3.21 and MLR > 0.345), and Score 1 encompassing cases not meeting these thresholds. Survival outcomes were analyzed using Kaplan-Meier methodology stratified by inflammatory marker levels and IPBS classifications. Multivariate Cox regression models were employed to identify prognostic factors influencing OS and DFS.
Results: Initial univariate assessments revealed significant correlations between disease-free survival and several factors including ypTNM staging, histopathological evidence of vascular/lymphatic/perineural invasion, postoperative neutrophil-lymphocyte ratio, and the IPBS system. Subsequent multivariate modeling identified elevated ypTNM classification (HR=2.115, 95% CI:1.114– 4.019, p=0.022) and increased IPBS (HR=1.798, 95% CI:1.049– 3.083, p=0.033) as independent prognostic indicators for reduced DFS. Notably, postoperative NLR values failed to demonstrate statistical significance in multivariate evaluation (HR=1.588, 95% CI:0.910– 2.772, p=0.104).
Conclusion: The composite inflammation-based postoperative biomarker score model demonstrated superior predictive accuracy for DFS outcomes in LARC patients undergoing NCRT compared to isolated biomarker analysis or select histopathological characteristics.
Keywords: rectal cancer, chemoradiotherapy, inflammatory biomarkers, prognosis
Introduction
Research has demonstrated that specific histopathological features exhibit the most significant predictive potential in locally advanced rectal carcinoma (LARC) cases, particularly vascular infiltration, lymphatic involvement, neural sheath invasion, circumferential resection margin compromise, tumor staging, and nodal metastases.1–3 The clinical application of these indicators faces multiple obstacles, such as reliance on procedural expertise during specimen collection and preparation, significant diagnostic discrepancies among pathologists, and difficulties in achieving objective numerical assessments.4 Emerging molecular signatures such as EphA4 expression,5 specific protein profiles,6,7 and microRNA patterns8,9 have shown correlations with clinical prognosis. However, their routine implementation remains constrained by high costs and technical complexity, underscoring the urgent requirement for cost-effective prognostic models that can reliably stratify survival risks in this clinical subgroup.
Recent studies have demonstrated that systemic inflammatory response (SIR) plays a crucial role in cancer pathogenesis, advancement, and metastatic spread.10,11 Hematological indicators including neutrophil-to-lymphocyte ratio (NLR) and monocyte-to-lymphocyte ratio (MLR) have emerged as reliable indicators of SIR.12 Neutrophils and monocytes contribute to a pro-tumorigenic environment, while lymphocytes are crucial for anti-tumor immunity.12,13 Their combination may thus provide a more holistic view of the host inflammatory state than either marker alone. These biomarkers offer practical advantages due to their cost-effective nature and routine availability in clinical settings. Current investigations predominantly concentrate on individual inflammatory parameters (eg, NLR, PLR, LMR) or composite indices like the Systemic Immune-Inflammation Index (SII) or modified Glasgow Prognostic Score (mGPS), yet findings remain inconsistent across different studies. Existing research primarily examines preoperative inflammatory markers. However, the postoperative period—defined here as after surgical resection but prior to adjuvant therapy—may represent a more biologically relevant window. This specific window aims to capture the systemic inflammatory state after tumor burden removal but before potential confounding effects of chemotherapy on hematological parameters (eg, cytopenia), thereby reflecting a more stable, cancer-related host response potentially indicative of residual micrometastatic risk. Evidence for the prognostic value of postoperative inflammatory markers, and particularly for a combined scoring model, in LARC patients receiving NCRT is limited. Consequently, we propose that an integrated scoring model incorporating multiple inflammatory indices might provide enhanced prognostic significance compared to isolated biomarker analysis, with the intended clinical use of identifying high-risk patients post-surgery for intensified surveillance and consideration of adjunctive therapies.
In this study, we developed a novel prognostic evaluation framework integrating postoperative neutrophil-to-lymphocyte ratio (NLR) and monocyte-to-lymphocyte ratio (MLR), designated as the Inflammation-based Postoperative Biomarker Score (IPBS) system. The investigation focused on assessing the clinical significance of this novel scoring system among individuals diagnosed with locally advanced rectal cancer (LARC) who received neoadjuvant chemoradiotherapy (NCRT).
Methods
Patient Cohort
This retrospective analysis examined LARC patients undergoing neoadjuvant chemoradiotherapy followed by total mesorectal excision at West China Hospital’s Gastroenterology Department from March 2014 to December 2024. Cancer staging was performed utilizing the 8th edition TNM classification system.14 The inclusion criteria comprised: 1) histologically verified rectal adenocarcinoma, 2) completion of NCRT protocol, 3) postoperative neutrophil-lymphocyte ratio and monocyte-lymphocyte ratio assessments, and 4) radiologically confirmed locally advanced disease. Exclusion criteria involved non-adenocarcinoma malignancies, active/chronic inflammatory or infectious conditions, hepatic dysfunction, and evidence of distant metastases. Ethical approval for this research was obtained from West China Hospital’s Institutional Review Board in accordance with the principles stated in the Declaration of Helsinki (NO. 2014–1244). This retrospective study was approved by the Ethics Committee/Institutional Review Board of West China Hospital with a waiver of informed consent. The waiver of informed consent was granted because this was a retrospective study involving minimal risk to participants, and obtaining consent was not feasible given the study design. All patient data were anonymized and de-identified prior to analysis to ensure confidentiality. The study was conducted in full compliance with the ethical standards outlined in the Declaration of Helsinki.
Neoadjuvant and Surgical Treatment
The NCRT regimen followed institutional protocol during the study period. All patients received long-course pelvic radiotherapy with a total dose of 45 to 50 Gy delivered in 25 to 28 fractions. Concurrent chemotherapy consisted of capecitabine (825 mg/m2 twice daily 5 d/wk) or CapeOX (oxaliplatin 50 mg/m2 IV weekly and capecitabine 625 mg/m2 twice daily 5d/wk). Surgery was scheduled 8–12 weeks after NCRT completion. The surgical approach (open, laparoscopic, or robotic) was at the surgeon’s discretion. Total mesorectal excision was the standard principle. Pathological assessment of the resection specimen, including ypTNM staging (8th edition AJCC/UICC), tumor regression grade, and status of vascular/lymphatic/perineural invasion and circumferential resection margin (CRM), was performed by dedicated gastrointestinal pathologists following standardized protocols.
Data Collection and Systemic Inflammatory Response Assessment
Blood samples were obtained following surgery but prior to initiating adjuvant treatment, as prior research has indicated that chemotherapy can cause discrepancies in hematological parameters owing to side effects like cytopenia.15,16 Samples were typically drawn during the postoperative hospitalization, prior to discharge and before any planned adjuvant chemotherapy, aiming to capture the baseline systemic inflammatory state after tumor removal.
The neutrophil-to-lymphocyte ratio (NLR) was calculated by dividing the absolute neutrophil count by the absolute lymphocyte count (both measured in cells/µL),16 while the monocyte-to-lymphocyte ratio (MLR) was derived from monocyte count divided by lymphocyte count.15 Elevated ratios of both NLR and MLR signaled an increased inflammatory response. ROC curve analysis identified optimal thresholds for predicting patient survival: scores were categorized as IPBS 0 (NLR <3.21 and MLR <0.345), IPBS 2 (NLR >3.21 and MLR >0.345), with intermediate values classified as IPBS 1.
Follow-Up
Postoperative surveillance followed institutional protocols. Overall survival (OS) was defined as the time from the date of surgery to the date of death from any cause. Disease-free survival (DFS) was defined as the time from surgery to the first event of either locoregional recurrence, distant metastasis, or death from any cause, whichever occurred first. Recurrence was diagnosed based on imaging studies (CT, MRI, or PET-CT) and/or histopathological confirmation.
Postoperative monitoring protocols involved quarterly measurements of serum CEA and CA19-9 biomarkers during the initial three postoperative years, transitioning to semiannual assessments in the subsequent triennium. Thoracoabdominal CT imaging was conducted biannually over a five-year surveillance period. Endoscopic evaluation of the colon occurred at 12 and 36 months following surgical intervention.17 Clinical outcomes were systematically documented in real-time until either recurrence detection or study termination.
Statistical Methodology
Diagnostic thresholds for each biomarker were determined through ROC curve optimization aligned with survival outcomes.18 Survival probabilities (OS and DFS) were graphically represented using Kaplan-Meier survival curves.19 Preliminary risk assessment employed univariate Cox regression modeling to identify prognostic factors influencing survival endpoints.20 Quantitative outcomes were expressed as HR values accompanied by 95% CI ranges. Statistically significant variables (p<0.05) from initial screening underwent multivariable Cox regression analysis.21 To ensure clinical relevance and adjust for established prognostic factors, the following key variables were also forced into the initial multivariable models regardless of their univariable significance: age (as a continuous variable), sex, and ypTNM stage (categorized as 0-I vs II–III). Specifically, Model 1 included established clinicopathological variables (age, sex, ypTNM stage, and relevant invasion patterns) together with the postoperative NLR, but excluded IPBS which aimed to assess whether NLR alone retained prognostic significance after adjusting for key confounders. Model 2 included the same set of clinicopathological variables together with the IPBS, but excluded the separate NLR and MLR variables. This approach prevented multicollinearity, as IPBS itself is derived from NLR and MLR thresholds, and allowed evaluation of the composite score’s independent contribution beyond its components.
Statistical analyses were conducted using SPSS software. Two-tailed statistical tests were employed, with statistical significance defined as P values below 0.05.21 In multivariate analytical procedures, two separate models were developed - one incorporating IPBS and another excluding them - to eliminate potential confounding effects of NLR and LMR on IPBS assessment.
Results
Characteristics of the Study Cohort
Patient demographics and clinical features are summarized in Table 1. The analysis cohort consisted of 260 individuals, with 156 (60.0%) males and 104 (40.0%) females. Pathological staging revealed the following distribution: 54 cases in pT0, 11 in pT1, 60 in ypT2, 122 in ypT3, and 13 in ypT4 stages. Lymph node involvement was identified in 73 patients (28.1%), while 187 (71.9%) showed no nodal metastasis. Vascular invasion occurred in 16 cases (6.2%), lymphatic invasion in 18 (6.9%), perineural invasion in 49 (18.8%), and positive circumferential resection margin in 9 (3.5%). The median age at diagnosis was 57.0 years (IQR 50.0–66.0). Postoperative inflammatory markers demonstrated a median NLR of 3.56 (IQR 2.45–5.39) and MLR of 0.425 (IQR 0.303–0.648). During the observation period, The median follow-up time for surviving patients was 33 months (IQR: 23–49). By the censoring date, no cases of local recurrence were recorded, while 62 patients (23.8%) developed distant metastasis and 44 (16.9%) succumbed to disease progression.
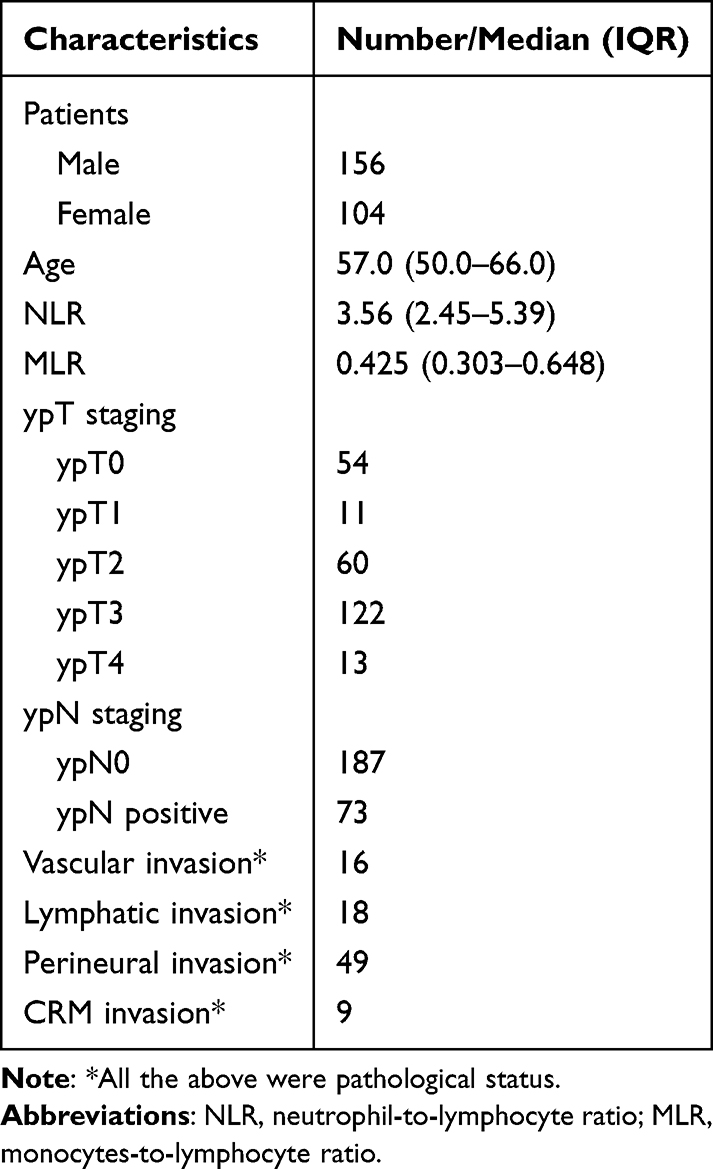 |
Table 1 Postoperative Characteristics of Enrolled RC Patients |
Survival Outcome by K-M Curve
ROC curve analysis identified optimal thresholds for postoperative NLR (3.21) and MLR (0.345). The sensitivity and specificity were (0.69, 0.57) respectively for NLR and (0.75,0.66) respectively for MLR. Figures 1A, 2A and 3A illustrate overall survival (OS) patterns stratified by postoperative NLR, MLR, and IPBS respectively, while Figures 1B, 2B and 3B display disease-free survival (DFS) distributions. Kaplan-Meier analysis revealed no statistically significant differences in OS or DFS outcomes across MLR subgroups. Elevated postoperative NLR levels and higher IPBS emerged as independent predictors for diminished overall and disease-free survival.
 |
Figure 1 Survival outcome by K-M curve of OS and DFS of NLR patients. OS overall survival, DFS disease-free survival, NLR neutrophil-lymphocyte ratio. (A) The overall survival rate of patients per month stratified by NLR. (B) The disease-free survival rate of patients per month stratified by NLR. |
 |
Figure 2 Survival outcome by K-M curve of OS and DFS of MLR patients. OS overall survival, DFS disease-free Survival, MLR monocyte-lymphocyte ratio. (A) The overall survival rate of patients per month stratified by MLR. (B) The disease-free survival rate per month of patients stratified by MLR. |
 |
Figure 3 Survival outcome by K-M curve of OS and DFS of IPBS patients. OS overall survival, DFS disease-free Survival, IPBS inflammatory response biomarker score. (A) The overall survival rate per month of patients stratified by IPBS. (B) The disease-free survival rate per month of patients stratified by IPBS. |
Prognostic Predictors for OS
Single-variable analysis indicated that elevated IPBS, increased postoperative NLR values, histopathological evidence of perineural invasion, lymphatic system infiltration, and advanced ypTNM staging showed associations with worse clinical outcomes. Multivariate modeling identified only advanced ypTNM staging as an independent prognostic indicator (stage II–III versus 0-I, HR=2.495, 95% CI:1.126–5.531, p=0.024) (Detailed data presented in Table 2).
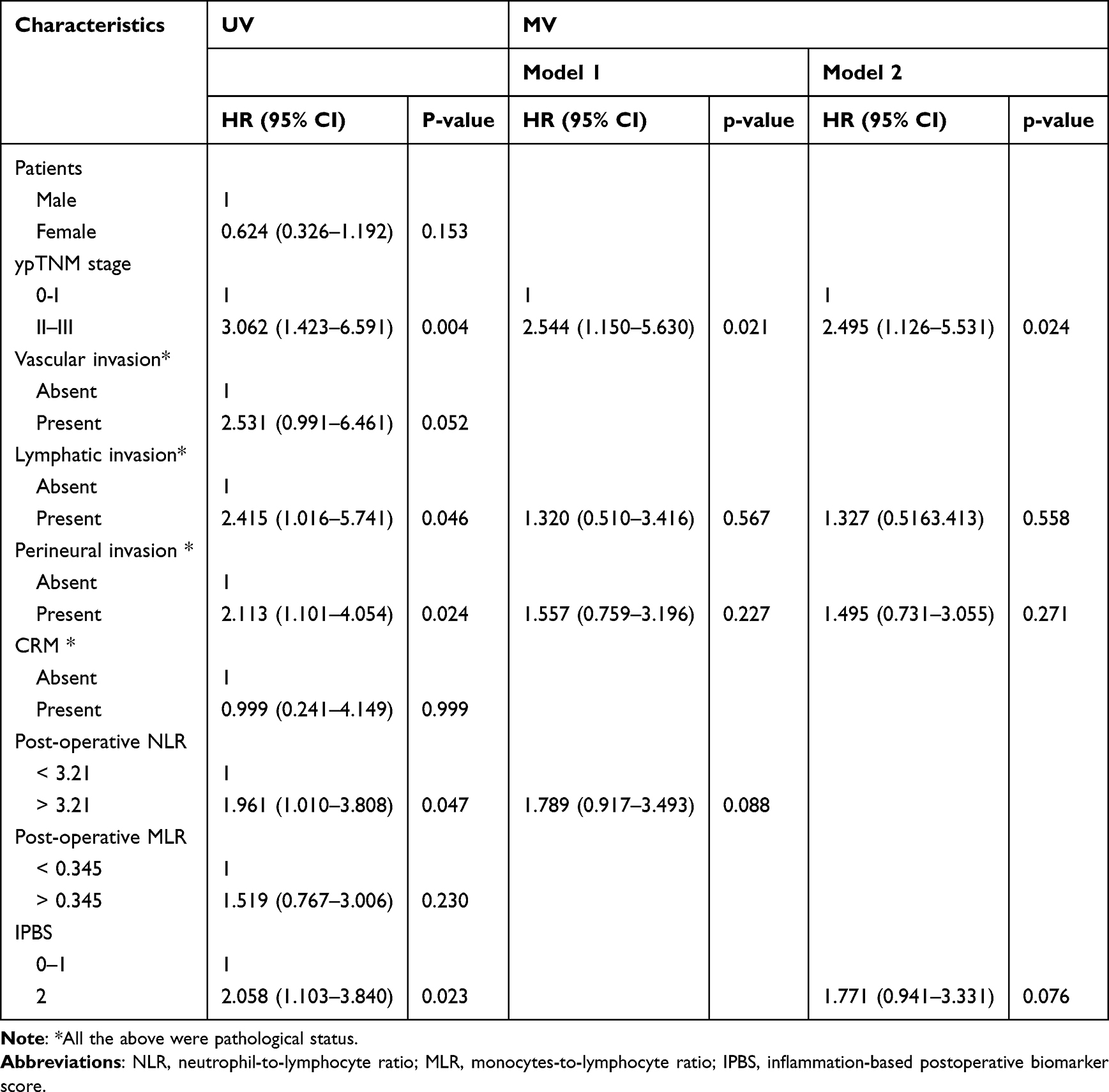 |
Table 2 Univariate and Multivariable Cox Regression Analysis for Overall Survival |
Prognostic Predictors for DFS
In initial univariate assessments, heightened IPBS, postoperative NLR values, and the presence of pathological features such as perineural, lymphatic, and vascular invasion, along with advanced ypTNM staging, emerged as significant predictors of DFS outcomes. Subsequent multivariate modeling revealed that only advanced ypTNM classification (Stage II–III versus 0-I: HR=2.115, 95% CI 1.114–4.019, p=0.022) and elevated IPBS (Score 2 versus 0–1: HR=1.798, 95% CI 1.049–3.083, p=0.033) maintained independent prognostic significance, while postoperative NLR failed to demonstrate statistical significance (HR=1.588, 95% CI 0.910–2.772, p=0.104). Notably, the IPBS system demonstrated superior predictive capacity for DFS compared to established pathological indicators including vascular, lymphatic, and perineural invasion patterns (Comprehensive data detailed in Table 3).
 |
Table 3 Univariate and Multivariable Cox Regression Analysis for Disease-Free Survival |
Discussion
While previous studies have investigated systemic inflammatory indicators following surgery,22–24 our research represents, to the best of our knowledge, the first comprehensive analysis focusing on the predictive significance of integrated IPBS in locally advanced rectal cancer patients undergoing neoadjuvant chemoradiotherapy and curative resection. In our cohort, individual inflammatory prognostic indicators, including the neutrophil-lymphocyte ratio (NLR) and monocyte-lymphocyte ratio (MLR), demonstrated notable associations with patient outcomes in univariate analysis. This finding was corroborated by ROC curve analyses that effectively stratified patients into distinct prognostic categories based on postoperative NLR and MLR measurements. Kaplan-Meier survival curves revealed that heightened postoperative NLR values and the composite IPBS were significantly associated with diminished overall survival (OS) and reduced disease-free survival (DFS) rates. However, multivariate Cox regression modeling provided a more nuanced picture. For OS, only advanced ypTNM stage (II–III vs 0-I) remained an independent prognostic indicator. For DFS, both advanced ypTNM stage and an elevated IPBS score retained independent predictive value, whereas postoperative NLR alone did not. Consequently, our IPBS model demonstrated independent prognostic performance for DFS superior to its individual components and several conventional pathological risk factors in our cohort. This suggests that the IPBS offers a practical advance in postoperative risk stratification for this well-defined patient population.
The study’s outcomes suggest that pharmacological approaches targeting inflammation could be utilized to mitigate the likelihood of disease recurrence among colorectal cancer patients after undergoing radical resection. Contemporary evidence indicates NSAIDs, acetylsalicylic acid, and H2 receptor antagonists demonstrate efficacy in suppressing host inflammatory responses and impeding neoplastic recurrence through distinct biological mechanisms.22–24 Emerging clinical data supports the therapeutic potential of oral aspirin administration as an adjunctive treatment modality in colorectal carcinoma management.25,26 However, precise identification of optimal patient subgroups for these anti-inflammatory therapeutic approaches remains an area requiring further investigation. In breast oncology, NSAID administration has demonstrated particular effectiveness in reducing recurrence rates among patients exhibiting elevated neutrophil-to-lymphocyte ratios.23 In line with this, the present investigation identified through elevated postoperative IPBS a patient subgroup that might, in theory, derive the maximum potential benefit from combined anti-inflammatory therapies and chemotherapy regimens. This specific hypothesis warrants testing in future prospective, interventional studies.
This investigation had several limitations. Firstly, the research utilized a retrospective cohort approach with participants recruited from a single medical center. However, the sample size proved substantial when considering tumor staging and inclusion of patients receiving neoadjuvant therapy. Secondly, surgical variables—including operative approach, resection technique, and anastomotic level—were not routinely documented in the dataset. As these factors may influence postoperative inflammatory responses and oncological outcomes, their absence from the analysis could be considered a constraint. Thirdly, threshold values defining elevated inflammatory states might require institution-specific calibration. Notably, all evaluated inflammatory prognostic markers could be derived from standard hematological parameters, indicating their potential clinical applicability for routine practice. Our findings, while not yet ready for clinical use, highlight the IPBS as a valuable tool to guide future research. It provides a standardized framework for enriching trial populations in studies of postoperative anti-inflammatory therapies and for investigating the biological link between systemic inflammation and micrometastatic risk. Ultimately, integrating this score with molecular and clinicopathological data could advance the development of more sophisticated, multi-factorial prognostic models.
Conclusion
In conclusion, we developed a postoperative inflammation-based scoring system (IPBS) and demonstrated its association with patient outcomes in our cohort. This model showed independent prognostic value for disease-free survival in locally advanced rectal carcinoma patients undergoing preoperative chemoradiation protocols, adding information to established factors such as ypTNM stage, which remained the dominant predictor for overall survival. Further external and prospective validation is required to confirm these findings and assess the score’s utility in routine clinical practice.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Do Canto LM, Barros-Filho MC, Rainho CA, et al. Comprehensive analysis of DNA methylation and prediction of response to neoadjuvanttherapy in locally advanced rectal cancer. Cancers. 2020;12(11):3079. doi:10.3390/cancers12113079
2. Liu X, Wang J, Hu K, et al. Neoadjuvant chemoradiotherapy or radiotherapy in patients aged 75 years or older with locally advanced rectal cancer. J Cancer. 2020;11(12):3536–9. doi:10.7150/jca.41950
3. Yan X, Chen J, Meng Y, et al. RAD18 may function as a predictor of response to preoperative concurrent chemoradiotherapy in patients with locally advanced rectal cancer through caspase‐9‐caspase‐3‐dependent apoptotic pathway. Cancer Med. 2019;8(6):3094–3104. doi:10.1002/cam4.2203
4. Nakhleh RE, Nosé V, Colasacco C, et al. Interpretive diagnostic error reduction in surgical pathology and cytology: guideline from the College of American Pathologists. Arch Pathol Lab Med. 2016;140(1):29–40.
5. Lin CY, Lee YE, Tian YF, et al. High expression of EphA4 predicted lesser degree of tumor regression after neoadjuvant chemoradiotherapy in rectal cancer. J Cancer. 2017;8(6):1089–1096. doi:10.7150/jca.17471
6. Cho EJ, Kim M, Jo D, et al. Immuno-genomic classification of colorectal cancer organoids reveals cancer cells with intrinsic immunogenic properties associated with patient survival. J Exp Clin Cancer Res. 2021;40(1). doi:10.1186/s13046-021-02034-1
7. Chen H-M, Lin -C-C, Chen W-S, et al. Insulin-like growth factor 2 mRNA-binding protein 1 (IGF2BP1) Is a prognostic biomarker and associated with chemotherapy responsiveness in colorectal cancer. Int J Mol Sci. 2021;22(13):6940.
8. Rubio J, Cristóbal I, Santos A, et al. Low MicroRNA-19b expression shows a promising clinical impact in locally advanced rectal cancer. Cancers. 2021;13(6):1456. doi:10.3390/cancers13061456
9. Bjørnetrø T, Redalen KR, Meltzer S, et al. An experimental strategy unveiling exosomal microRNAs 486-5p, 181a-5p and 30d-5p from hypoxic tumour cells as circulating indicators of high-risk rectal cancer. J Extracell Vesicles. 2019;8(1). doi:10.1080/20013078.2019.1567219
10. Jiang Z, Shi Y, Zhao W, et al. Development of an immune-related prognostic index associated with glioblastoma. Front Neurol. 2021;12:610797.
11. Qi W-X, Xiang Y, Zhao S, Chen J. Assessment of systematic inflammatory and nutritional indexes in extensive-stage small-cell lung cancer treated with first-line chemotherapy and atezolizumab. Cancer Immunol Immunother. 2021;70(11):3199–3206. doi:10.1007/s00262-021-02926-3
12. Sato S, Kunisaki C, Takahashi M, et al. High postoperative neutrophil–lymphocyte ratio and low preoperative lymphocyte-monocyte ratio predict poor prognosis in gastric cancer patients receiving gastrectomy with positive lavage cytology: a retrospective cohort study. Langenbecks Arch Surg. 2021;406(7):2295–2303. doi:10.1007/s00423-021-02233-6
13. Luo Q, Yang C, Fu C, Wu W, Wei Y, Zou L. Prognostic role of blood markers in primary central nervous system lymphoma patients treated with high-dose methotrexate-based therapy. Front Oncol. 2021;11:639644.
14. Yu L, Xu T, Zhang L, Zhu Y, Fang H, Zhang H. Tumor deposits should not be ignored in the AJCC TNM staging system for ypN(+) stage rectal cancer with neoadjuvant chemoradiotherapy. J Gastrointestinal Surg. 2020;24(10):2298–2301. doi:10.1007/s11605-020-04675-7
15. Dudani S, Marginean H, Tang PA, et al. Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios as predictive and prognostic markers in patients with locally advanced rectal cancer treated with neoadjuvant chemoradiation. BMC Cancer. 2019;19(1). doi:10.1186/s12885-019-5892-x
16. Patel M, McSorley ST, Park JH, et al. The relationship between right-sided tumour location, tumour microenvironment, systemic inflammation, adjuvant therapy and survival in patients undergoing surgery for colon and rectal cancer. Br J Cancer. 2018;118(5):705–712. doi:10.1038/bjc.2017.441
17. Willett CG. Management of Locoregional Rectal Cancer. J National Compr Cancer Network. 2018;16(5S):617–619. doi:10.6004/jnccn.2018.0037
18. Bantis LE, Tsimikas JV, Chambers GR, Capello M, Hanash S, Feng Z. The length of the receiver operating characteristic curve and the two cutoff Youden index within a robust framework for discovery, evaluation, and cutoff estimation in biomarker studies involving improper receiver operating characteristic curves. Stat Med. 2021;40(7):1767–1789. doi:10.1002/sim.8869
19. Ranstam J, Cook JA. Kaplan–Meier curve. Br J Surg. 2017;104(4):442. doi:10.1002/bjs.10238
20. Goh TS, Lee JS, Il Kim J, et al. Prognostic scoring system for osteosarcoma using network‐regularized high‐dimensional Cox‐regression analysis and potential therapeutic targets. J Cell Physiol. 2019;234(8):13851–13857. doi:10.1002/jcp.28065
21. Li Z, Wang Q, Qiao Y, Wang X, Jin X, Wang A. Incidence and associated predictors of adverse pregnancy outcomes of maternal syphilis in China, 2016–19: a Cox regression analysis. BJOG. 2020;128(6):994–1002. doi:10.1111/1471-0528.16554
22. Ishikawa H, Mutoh M, Sato Y, et al. Chemoprevention with low-dose aspirin, mesalazine, or both in patients with familial adenomatous polyposis without previous colectomy (J-FAPP Study IV): a multicentre, double-blind, randomised, two-by-two factorial design trial. Lancet Gastroenterol Hepatol. 2021;6(6):474–481. doi:10.1016/S2468-1253(21)00018-2
23. Liu J, Sun Y, Liu X, et al. Efficiency of different treatment regimens combining anti-tumor and anti-inflammatory liposomes for metastatic breast cancer. AAPS Pharm Sci Tech. 2020;21(7):259. doi:10.1208/s12249-020-01792-z
24. Tan RZH, Lockart I, Abdel Shaheed C, Danta M. Systematic review with meta-analysis: the effects of non-steroidal anti-inflammatory drugs and anti-platelet therapy on the incidence and recurrence of hepatocellular carcinoma. Aliment Pharmacol Ther. 2021;54(4):356–367. doi:10.1111/apt.16515
25. Farrugia MK, Long MD, Mattson DM, et al. Concurrent aspirin use is associated with improved outcome in rectal cancer patients who undergo chemoradiation therapy. Cancers. 2021;13(2):205. doi:10.3390/cancers13020205
26. Wang B, Huang Y. Effect of aspirin use on neoadjuvant chemoradiotherapy for rectal cancer: a meta-analysis with trial sequential analysis. J Cancer Res Clin Oncol. 2020;146(8):2161–2171. doi:10.1007/s00432-020-03222-w
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Safety and Efficacy of Serplulimab Combined with Neoadjuvant Chemoradiotherapy in High-Risk Locally Advanced Rectal Cancer: A Retrospective Study
Tian M, Zhao M, Jiang L, Liu J, Shen G, Zhang Z, Zhu C, Zhang S, Sun X, Shi Y, Di X
Cancer Management and Research 2025, 17:2931-2938
Published Date: 27 November 2025