Back to Journals » Journal of Pain Research » Volume 14
A Retrospective, Single-Center, Quantitative Analysis of Adverse Events in Patients Undergoing Spinal Stenosis with Neurogenic Claudication Using a Novel Percutaneous Direct Lumbar Decompression Strategy
Authors Pope JE, Deer TR ![]() , Falowski SM
, Falowski SM ![]()
Received 4 February 2021
Accepted for publication 26 May 2021
Published 24 June 2021 Volume 2021:14 Pages 1909—1913
DOI https://doi.org/10.2147/JPR.S304997
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Krishnan Chakravarthy
Jason E Pope,1 Timothy R Deer,2 Steven M Falowski3
1Evolve Restorative Center, Santa Rosa, CA, USA; 2The Spine and Nerve Center of the Virginias, Charleston, WV, USA; 3Neurosurgical Associates of Lancaster, Lancaster, PA, USA
Correspondence: Jason E Pope Email [email protected]
Introduction: Low-back pain with accompanying neurogenic claudication is a common diagnosis in pain and spine centers around the world, with an evolving algorithm of treatment. One option for the treatment of neurogenic claudication by decompressive strategies centers on percutaneous direct decompressive techniques. Although commonly employed in clinical practice, there have been no formal investigations looking at safety of percutaneous direct decompression without the use of an epidurogram and relying on osteal landmarks. The purpose of this study was to investigate the safety of percutaneous direct decompression performed without the use of the epidurogram.
Methods: After an IRB exemption had been obtained from the Western Investigational Review Board, data were retrospectively analyzed from July 2018 to August 2020 on patients that had undergone percutaneous direct decompression using the Mild procedure in a single center by a single physician. Data were analyzed quantitatively for reported complications within 3 months of the procedure, including nerve injury, hematoma, infection, death, or allergic reaction to contrast use.–
Results: Chart review yielded 147 individual patients who had undergone percutaneous direct decompression from July 2018 to August 2020. In this data set, women outnumbered men, with an average age of 76 years, with L4–L5 followed by L3–L4 being the most common levels decompressed. Of the 147 patients was performed, utilizing an epidurogram versus no epidurogram for decompression, with no complications. These data are the first to describe the safety of percutaneous direct lumbar decompression without the use of contrast.
Conclusion: This study strongly suggests the use of an epidurogram is not necessary for the safe decompression of a patient with symptomatic spinal stenosis and neurogenic claudication utilizing percutaneous direct decompression.
Keywords: spinal stenosis, lumbar stenosis, minimally invasive, epidurogram
Introduction
Low-back pain with accompanying neurogenic claudication is a common diagnosis in pain and spine centers around the world, with an evolving algorithm of treatment.1 In the interventional pain community, one option for the treatment of neurogenic claudication by decompressive strategies centers on percutaneous direct decompressive techniques. Up to 85% of spinal canal narrowing is attributed to some contribution of a hypertrophic ligamentum flavum,leading to central stenosis, and minimally invasive direct decompressive treatment debulks hypertrophic ligamentum flavum–relieving pressure caused by stenosis, while leaving no implants behind.2 Thirteen clinical studies and >25 published papers have established the safety and long-term efficacy of percutaneous direct decompression, and a level 1 randomized controlled trial demonstrated similar safety for percutaneous direct decompression and epidural steroid injections.3 Although these data exist, patient selection for treatment candidacy and the procedure itself are evolving.4 Percutaneous direct decompression procedurally has evolved from a dedicated ipsilateral incision and epidurogram to a midline incision with or without the need for an epidurogram. Although this has been employed in clinical practice, there has been no formal investigation of the safety of percutaneous direct decompression without the use of an epidurogram and relying on osteal landmarks. The purpose of this study was to investigate the safety of percutaneous direct decompression performed without the use of an epidurogram, representing the first publication investigating the safety of the direct decompressive strategy without the use of contrast and placement of an epidural for an epidurogram.
Methods
After an IRB exemption had been obtained by the Western Investigational Review Board, data were retrospectively analyzed from July 2018 to August 2020 on patients that had undergone a percutaneous direct decompression using the Mild procedure (Vertos Medical, Aliso Viejo, CA, USA) in a single center by a single physician. The reason for the exemption from the review board was that this was a retrospective chart review with no patient-identifying information for analysis, was of low risk to patients, and patient-data confidentiality complied with the Declaration of Helsinki. Data were analyzed quantitatively for reported complications within 3 months of the procedure, including nerve injury, hematoma, infection, death, or allergic reactions to contrast use. For purposes of analysis, descriptive statistics were used. For calculation of decompression, each level was counted once, regardless of whether it had been treated unilaterally or bilaterally. Similarly, for most common levels, each was counted once, regardless of whether it had been treated unilaterally or bilaterally.
Results
Chart review yielded 147 individual patients who had undergone the percutaneous direct decompression procedure from July 2018 to August 2020. Of these, data had been obtained within 3 months postprocedure to detect complications, with specific queries for infection, nerve injury, bleeding, death, or contrast allergy. Demographic information for these patients that had undergone percutaneous direct decompression for treatment of symptomatic spinal stenosis, defined for the purposes of this report as pain in the back or the leg with standing that improves with sitting or bending forward, is represented in Table 1.
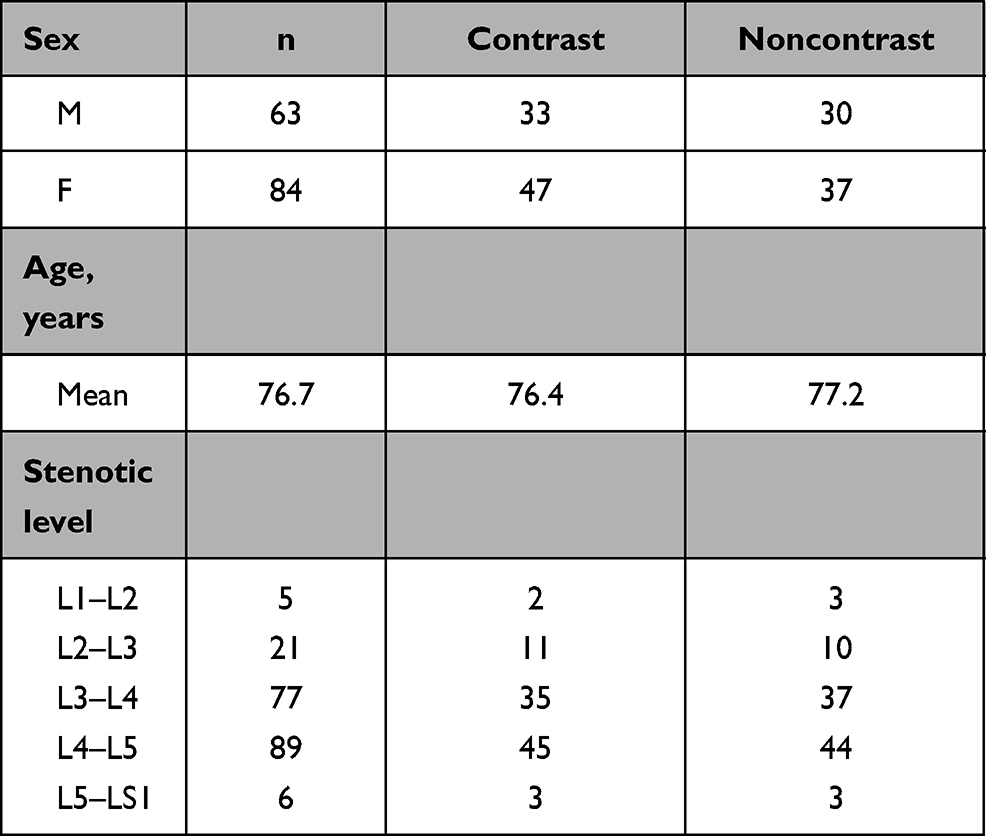 |
Table 1 Demographic information |
We then identified those patients that had undergone percutaneous decompression with the use of an epidurogram (80) compared to those that had undergone the procedure without the use of an epidurogram (67). Data were tabulated based on level decompressed and side of decompression — unilateral versus bilateral. The bilateral percentage represented the likelihood of the level being managed bilaterally, and otherwise it had been performed unilaterally on the symptomatic side.
Complication rates were reviewed, as highlighted in Table 2, investigating the occurrence of nerve injury, hematoma, infection, death, or allergic reaction to contrast during the decompressive procedure. There were no reported complications on the day of the procedure, immediate postoperative period (within the first 2 weeks), or during the 3-month follow-up (±2 weeks) for either the epidurogram or no-epidurogram groups, representing the upper limit of a “global period” for minimally invasive spine procedures.
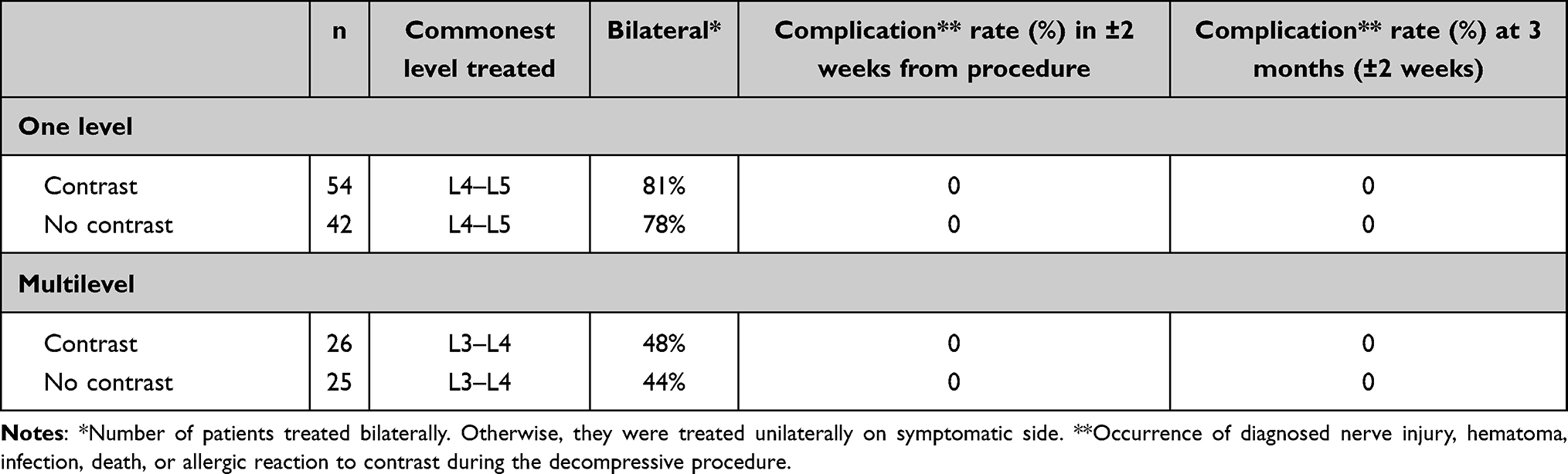 |
Table 2 Treatment strategy, contrast use, and complications |
In this data set, women outnumbered men, with an average age of 76 years, with L4–L5 followed by L3–L4 the most common levels decompressed. The contrast and noncontrast treatment groups were evenly matched on age, sex, stenotic levels, and levels treated. Of the 147 patients, percutaneous direct decompression, as indicated in the lumbar spine from L1 to S1, was performed with no complications. These data are the first to describe the safety of percutaneous direct lumbar decompression without the use of contrast. Interestingly, in this data set, nearly 80% of the single level procedures were performed bilaterally, most often at L4–L5, and two-level decompressions were performed with the most common level being L3–L4, where nearly half were performed bilaterally.
Discussion
The era of minimally invasive decompressive procedures performed by spine surgeons and pain physicians is evolving. With the advent of minimally invasive spine procedures, patients have access to a therapy that may delay or prevent future invasive open surgery for neurogenic claudication and spinal stenosis. Published data suggest that this percutaneous direct decompression therapy has a high rate of success with limited risk.3 For the Mild procedure, a five-point mean numeric pain-rating scale improvement4 with mean ODI responder improvement of 32 points,5 indicating significant pain reduction and functional improvement, has been achieved at 2-year follow-up.
Historically, percutaneous direct decompression was performed by initially placing an epidural at the level or the level above the spinal stenosis.4,5 This allows for production of an epidurogram and outlining the posterior border of the epidural space. The ligamentum flavum, which is decompressed to allow for treatment of the neurogenic claudication from central spinal stenosis with a contribution of least 2.5 mm length of hypertrophy, is posterior and superficial to the epidural space (Figure 1). Further, a contralateral oblique view of the interspinous space allows a working view, where the lamina of the target spinal stenosis level is identified, simplifying decompression and portal placement (Figure 2). This affords clear identification of the lamina and target location for decompression. It has been postulated that this view can be used effectively and safely.
 |
Figure 1 Fluoroscopic lateral (A) and right contralateral oblique view (B) of target level on epidurogram. |
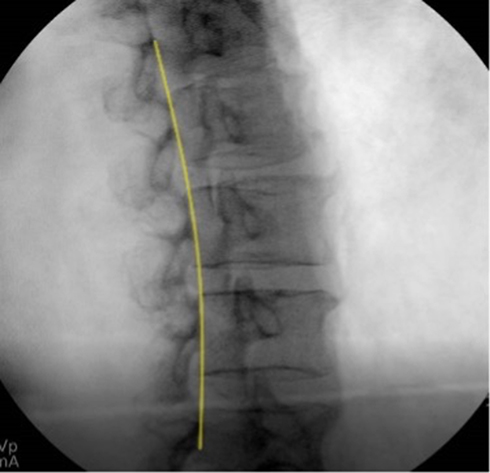 |
Figure 2 Epidural line from contralateral oblique view. |
Additionally, the procedure was further streamlined in both treatment arms by the use of a single midline incision that can be shifted laterally to accommodate the placement of the portal for access to the ligamentum flavum, deep to the ipsilateral lamina, but superficial to the epidural space (Figure 3A–C).
 |
Figure 3 (A) Midline incision. (B) Midline incision shifted to the left. (C) Midline incision shifted to the right. |
This creates an opportunity to move away from the routine use of epidurograms for this procedure. In the MiDAS ENCORE study, the complication rate was 1.3% (two patients) one with intraoperative oozing at the treatment site). Gel foam was administered, and the patient was discharged the same day with no complications. The second patient had postoperative pain possibly related to the Mild procedure that resolved within 3 days of the index procedure.3
As the procedure continues to evolve, this real-world retrospective review suggests that the Mild procedure maintains its safety profile with the no-contrast approach, and should thus continue to be positioned early in the treatment algorithm for patients with neurogenic claudication and ligamentum flavum hypertrophy ≥2.5mm after failure of conservative measures.
Limitations of this study include the retrospective nature of the investigation. Although the MiDAS ENCORE study of 149 patients indicated a reoperation rate of 5.6% at 2-year follow-up6 and an adverse-event rate of 1.3%,3 this single-site study may not translate to a broader application of the percutaneous direct decompressive method using a single incision and absence of an epidurogram. Furthermore, efficacy was not evaluated for either group, as this study was focused on patient safety. Percutaneous decompression–technique variance and efficacy comparisons are under way. Prospective studies need to be performed with a direct comparison of safety and efficacy of the new technique described in this cohort.
Conclusion
This study strongly suggests the use of an epidurogram is not necessary for the safe decompression of a patient with symptomatic spinal stenosis with neurogenic claudication utilizing percutaneous direct decompression.
Acknowledgments
The authors would like to thank Adrian Marquez, Carla Canada, and Eric Bruntlett for their contribution to data collection and statistical analysis in this investigation.
Disclosure
JEP is a consultant for and performs research with Vertos Medical, Vertiflex (Boston Scientific), Aurora Spine, Abbott, Medtronic, Biotronik, Stimgenics, Thermaquil, PainTeq, Spark, Wise, SpineThera, Celeri Health, AIS, Saluda, Nalu, Ethos, Mainstay, and SPR. TRD is a consultant for and has received personal fees from Vertos Medical, Vertiflex (Boston Scientific), Abbott, Flownix, Axonics, Cornerloc, Ethos, Stimgenics, SI Bone, Nevro, Medtronic, PainTeq, SpineThera, Saluda, Mainstay, Nalu, Ethos, and SPR, and has a DRG surgical leads for and a patent issued to Abbott. SMF reports personal fees for consultancy from Vertos, Vertiflex, Boston Scientific, Abbott, CornerLoc, PainTeq, Medtronic, SPR, and Saluda. The authors report no other conflicts of interest in this work.
References
1. Deer TR, Grider JS, Pope JE, et al. The MIST guidelines: the Lumbar Spinal Stenosis Consensus Group guidelines for minimally invasive spine treatment. Pain Pract. 2019;19(3):250–274. doi:10.1111/papr.12744
2. Hansson T, Suzuki N, Hebelka H, Gaulitz A. The narrowing of the lumbar spinal canal during loaded MRI: the effects of the disc and ligamentum flavum. Eur Spine J. 2009;18(5):679–686. doi:10.1007/s00586-009-0919-7
3. Benyamin RM, Staats PS; MiDAS ENCORE Investigators. Mild® is an effective treatment for lumbar spinal stenosis with neurogenic claudication: miDAS ENCORE randomized controlled trial. Pain Physician. 2016;19(4):229–242. doi:10.36076/ppj/2019.19.229
4. Jain S, Deer TR, Sayed D, et al. Minimally invasive lumbar decompression: a review of indications, techniques, efficacy and safety. Pain Manag. 2020;10(5):331–348. doi:10.2217/pmt-2020-0037
5. Stats PS, Benyamin RM, et al. MiDAS ENCORE: Randomized Controlled Clinical Trial Report of 6 month Results. Pain Physician. 2016;(2):25–38.
6. Staats PS, Chafin TB, Golvac S, et al. Long-term safety and efficacy of minimally invasive lumbar decompression procedure for the treatment of lumbar spinal stenosis with neurogenic claudication: 2-year results of MiDAS ENCORE. Reg Anesth Pain Med. 2018;43:789–794. doi:10.1097/AAP.0000000000000868
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.