Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
A Retrospective Evaluation of Setup Errors Associated with Respiratory Motion Management Techniques in Stereotactic Body Radiation Therapy for Hepatic Malignancies
Authors Han JH, He DC, Zhang XY, Zhang Y, Hong J, Shi TT, Zhu ZJ
Received 23 June 2025
Accepted for publication 7 September 2025
Published 20 September 2025 Volume 2025:12 Pages 2139—2147
DOI https://doi.org/10.2147/JHC.S546967
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Mohamed Shaker
Ji-Hua Han,* Dong-Cheng He,* Xiao-Ye Zhang, Yan Zhang, Jun Hong, Ting-Ting Shi, Zhi-Jian Zhu
Department of Radiation Oncology, The Affiliated Huaian No.1 People’s Hospital of Nanjing Medical University, Huai’an, Jiangsu Province, 223300, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhi-Jian Zhu, Department of Radiation Oncology, The Affiliated Huaian No.1 People’s Hospital of Nanjing Medical University, No. 1 Huanghe West Road, Huaiyin District, Huai’an, Jiangsu Province, 223300, People’s Republic of China, Tel +86-517-80872759, Email [email protected]
Objective: This study aimed to evaluate setup errors associated with three respiratory motion management techniques in stereotactic body radiation therapy (SBRT) for individuals with hepatic malignancies.
Methods: A retrospective analysis was conducted on data from 55 individuals with hepatic malignancies who underwent SBRT. Respiratory motion was managed using the Active Breathing Coordinator (ABC) in 11 cases, the BodyFIX system in 6 cases, and a thermoplastic body film combined with an airbag in 38 cases. Cone-beam computed tomography (CBCT) was conducted prior to each treatment session and registered with the reference computed tomography (CT) images acquired during the treatment planning phase to quantify setup errors in three dimensions: left-right (LR), superior-inferior (SI), and anterior-posterior (AP).
Results: In the LR direction, the BodyFIX group had a 1.07 mm lower setup error than the ABC group, and the airbag group showed a 2.13 mm reduction compared to ABC and 1.06 mm compared to BodyFIX. In the SI direction, BodyFIX showed a 4.66 mm reduction and the airbag group a 5.45 mm reduction versus ABC. In the AP direction, reductions were 1.99 mm for BodyFIX and 2.86 mm for the airbag group compared to ABC. All differences were statistically significant. The airbag group also had relatively small planning target volume (PTV) margins.
Conclusion: The airbag-based respiratory motion management technique demonstrated superior positioning accuracy, improved reproducibility, and the potential for PTV margin reduction in SBRT for hepatic malignancies. Further investigations are needed to verify the superiority of this approach in different populations and settings.
Keywords: hepatic malignancies, motion management, PTV margin, setup error
Introduction
Hepatic malignancies are the sixth most commonly diagnosed cancer worldwide and the third leading cause of cancer-related mortality, following lung and colorectal cancers. In 2022, an estimated 865,000 new cases and 757,948 deaths were attributed to hepatic malignancies.1 This category of malignancies encompasses both primary hepatobiliary carcinomas and liver metastases. Metastatic liver involvement is particularly common in individuals with gastrointestinal, thoracic, and breast malignancies, as well as hematological cancers.
Surgical resection remains the standard treatment for hepatic malignancies; however, a significant proportion of individuals are ineligible for surgery due to medical contraindications, advanced liver disease, or inadequate liver function reserve.2 Alternative local therapies include transarterial chemoembolization, radiofrequency ablation, particle implantation, microwave ablation, and stereotactic body radiation therapy (SBRT).3 Among these modalities, SBRT is a non-invasive treatment that has demonstrated high local control rates. Specifically, the 1-year local control rate ranges from 70% to 100%, while the 2-year local control rate ranges from 60% to 90%.4,5
Safe and effective SBRT therapy requires precise patient positioning, accurate treatment planning and implementation, high-quality quality assurance and control, and appropriate management of tumor and organ motion during treatment.6 Given its anatomical location in the upper abdomen, adjacent to the diaphragm, the liver is subject to significant displacement due to respiratory motion. Consequently, implementing effective motion management strategies is critical during SBRT treatment for hepatic malignancies.7
The present study evaluated setup errors associated with three respiratory motion management techniques used in SBRT treatment for hepatic malignancies. Data were collected from 55 individuals with hepatic malignancies who underwent SBRT. Setup errors associated with the Active Breathing Coordinator (ABC),8 the BodyFIX system,9 and the airbag technique were quantified using cone-beam computed tomography (CBCT).
The airbag technique, implemented at this radiotherapy center, integrates a thermoplastic body film with an inflatable airbag to enhance patient immobilization. The airbag is positioned between the upper abdomen and the thermoplastic body film, and an external inflation valve is used to regulate air pressure, thereby applying controlled compression to the upper abdomen to minimize respiratory-induced motion.
As the dose per fraction in SBRT is significantly higher than in conventional radiation therapy, safe and accurate implementation of treatment requires precise definition of the tumor area and effective motion management. This challenge is typically addressed through target volume expansion and the application of various motion-management strategies. The biological effects of SBRT intensify with increasing dose per fraction, necessitating precise determination of planning target volume (PTV) margins to ensure adequate tumor coverage while minimizing radiation exposure to healthy hepatic and gastrointestinal tissues, reducing radiation-induced toxicity, and enabling the delivery of higher therapeutic radiation doses.10 SBRT for hepatic malignancies requires smaller PTV margins compared to conventional radiation therapy. Minimizing geometric uncertainties (internal and external immobilization) is crucial and can be achieved with robust immobilization. This study aimed to quantify setup errors and corresponding PTV margins associated with three different immobilization methods.
Materials and Methods
Study Population
A retrospective analysis was conducted on 55 individuals who underwent SBRT for hepatic malignancies at the radiotherapy center of Huai’an First Hospital between April 2017 and December 2023. Patients were categorized into three groups based on the respiratory motion management technique utilized: the Active Breathing Coordinator (ABC) group (n = 11), the BodyFix group (n=6), and the airbag group (n = 38). The study cohort comprised 36 males and 19 females, with ages ranging from 39 to 80 years (median age: 64 years). Diagnoses consisted of 42 cases of primary liver cancer and 13 cases of liver metastases. Main characteristics of patients and tumors are summarized in Table 1. Treatment was administered at a dose per fraction ranging from 4 to 10 Gy. This study was approved by the Ethics Committee of Huai’an First Hospital.
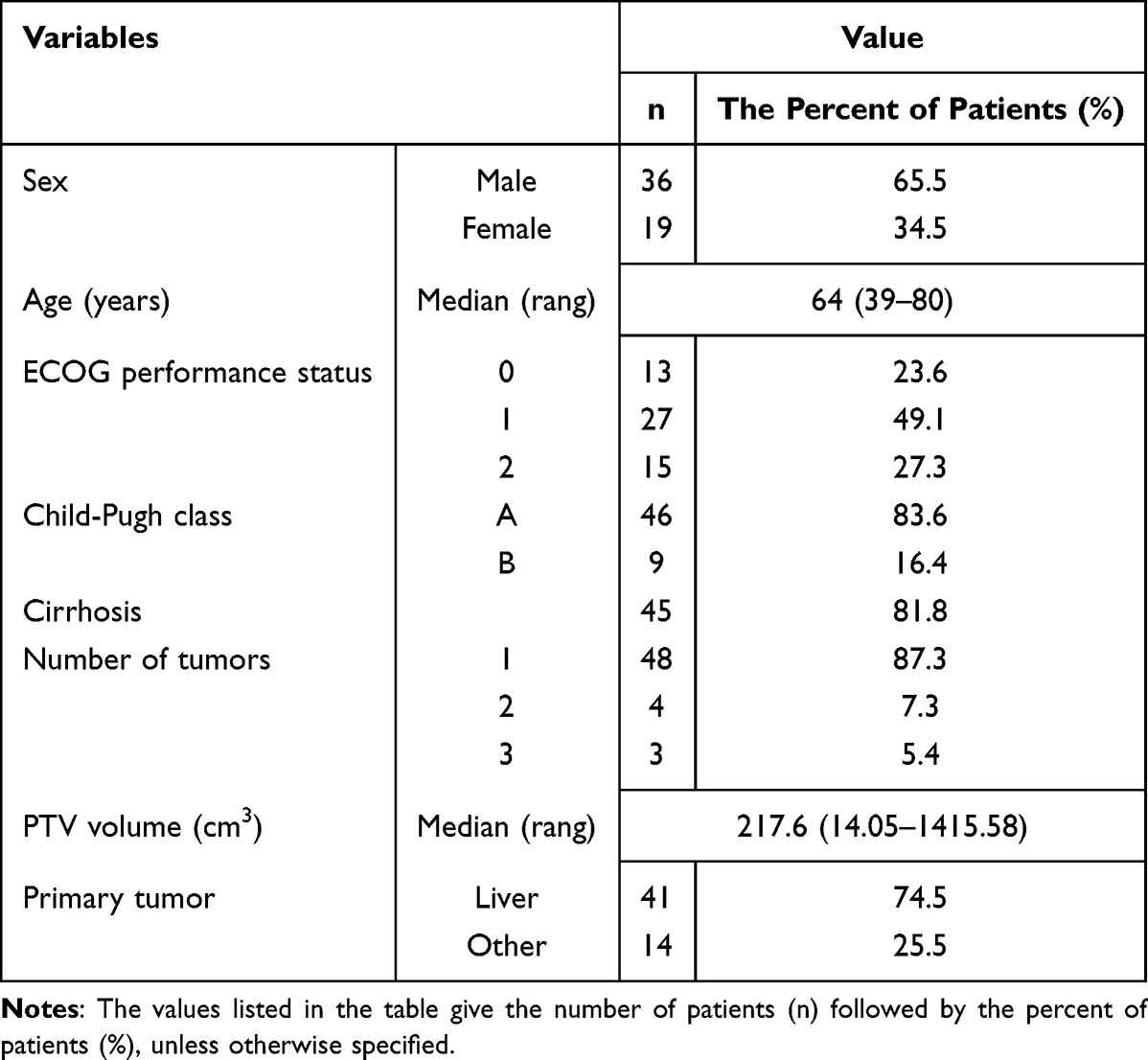 |
Table 1 Patient and Tumor Characteristics |
Respiratory Motion Management
All patients were positioned supine with their arms raised and crossed at the elbows, and their forearms placed above the head. Respiratory motion management was implemented using one of the following three techniques:
- Active Breathing Coordinator (ABC) System: The Deep Inspiration Breath-Hold (DIBH) is the technique we employed to manage respiratory motion. The ABC system is the specific electronic-mechanical system used to achieve, control, and monitor the DIBH state for each patient. The ABC system (Elekta, Atlanta, GA, USA) used in this study was employed to regulate breathing and facilitate DIBH.
- BodyFIX System: The BodyFIX system (Elekta, Atlanta, GA, USA) comprised a full-body vacuum bag without a drape. This system maintained a controlled negative pressure within the chest and abdominal regions, thereby reducing the amplitude of respiratory motion. This technique served as a form of abdominal compression (AC).
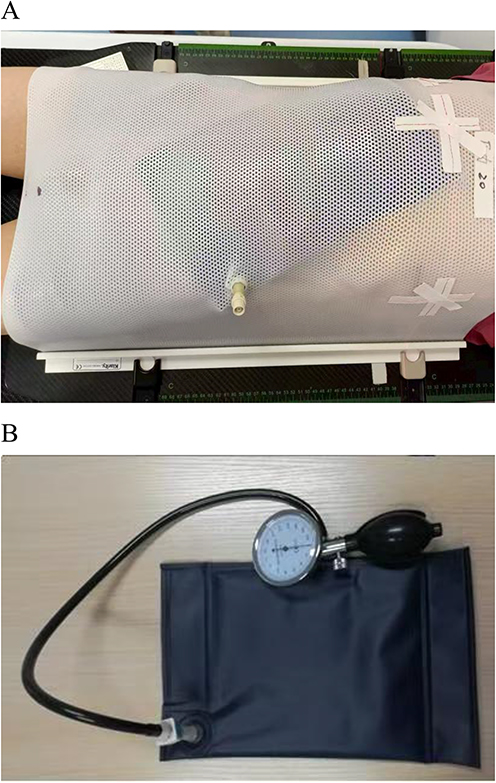
- Thermoplastic Body Film with an Inflatable Airbag (Klarity, Guangzhou, China): This method needs attachment of an uninflated airbag to the skin surface below the xiphoid process of the body, followed by encapsulation with a thermoplastic film, as shown in Figure 1A. A small opening is created in the thermoplastic film to expose the inflation and deflation valves of the airbag. Once the thermoplastic film has fully cooled, the air pump is connected to the inflation valve, and the airbag is inflated to the desired pressure, as shown in Figure 1B. Simultaneously, the airbag pressure is measured using a calibrated gauge. By integrating the thermoplastic film with the inflatable airbag, additional abdominal pressure is applied. The pressure of the airbag can be adjusted via the air pump, effectively suppressing abdominal breathing. The pressurized area of the airbag was positioned in the subxiphoid region. According to Hu et al, four-dimensional computed tomography (4D-CT) imaging demonstrated that applying pressure to the subxiphoid region effectively reduced liver motion.11

Figure 1 (A) shows the patient being fixed with the combination of thermoplastic film and airbag. (B) shows the connection between the airbag and the pressure display inflation pump.
CT Scans
Computed tomography (CT) imaging was performed using a Philips Brilliance Big Bore CT simulator, capturing scans from 5 cm above the diaphragm to the inferior border of the L4 vertebral body, with a slice thickness of 5 mm. The acquired CT images were subsequently transferred to the Monaco 5.1.1 Treatment Planning System (Elekta, Atlanta, GA, USA). Target volume delineation was conducted by senior radiation oncologists, followed by radiotherapy plan development by medical physicists. The finalized CT images, including the delineated target area and treatment plan details, were then transmitted to the X-ray Volume Imaging (XVI) system integrated with the linear accelerator for treatment execution.
Setup Errors and PTV Margins
Prior to each SBRT session, a 3D-CBCT scan was performed. In this study, the ABC system is used to perform a CBCT scan with the patient holding their breath at the end of inhalation. The CBCT scans using the three different fixation methods are all consistent with the treatment. The resulting images are then registered with the planned CT images. Gray-scale registration, in which image alignment is based on the grayscale values corresponding to liver position, was initially applied, followed by manual fine-tuning to optimize the alignment of target areas in the sagittal, coronal, and transverse planes. Setup errors were recorded in the left-right (LR), superior-inferior (SI), and anterior-posterior (AP) directions. A region of interest was used during the registration step. The image registration step conducted by senior specialists with extensive expertise.
Both random and systematic errors were calculated at the individual and population levels using established methodologies.12 Systematic errors (Σ) and random errors (σ) together contribute to the overall setup uncertainty. Specifically, the individual systematic error was calculated as the mean value of all fractional positioning errors for each patient, while the individual random error was quantified by the standard deviation of these fractional errors. The population-level systematic error was then derived as the standard deviation of all individual systematic errors, and the population-level random error was taken as the mean of all individual random errors.13 PTV margins were calculated using the Stroom et al formula: MPTV = 2Σ + 0.7σ.
Statistical Analysis
Data analysis was conducted using SPSS software (version 22, IBM SPSS Statistics). Setup errors for the three immobilization techniques were expressed as mean ± standard deviation (SD). Multiple comparisons were performed using the Tukey’s post-hoc test. A P-value of less than 0.05 indicated statistical significance.
Results
Statistics of Image-Registration Results
A total of 454 pre-treatment CBCT images and corresponding planning CT images were analyzed, including 124 from the ABC group, 54 from the BodyFix group, and 276 from the airbag group. Translational setup errors in the LR, SI, and AP directions were recorded for each CBCT scan, as detailed in Table 2. Among the three groups, the ABC group exhibited the largest setup errors, while the airbag group demonstrated the smallest.
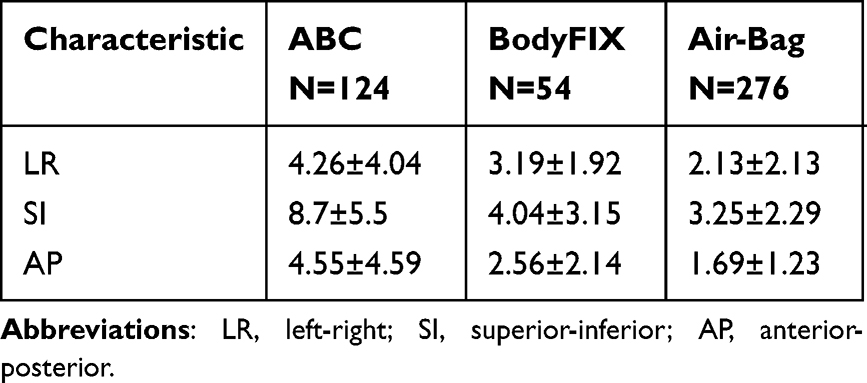 |
Table 2 Description of the Setup Errors in LR, SI and AP Directions of Three Groups (Mean±SD, mm) |
Analysis of Image-Registration Results
The Tukey’s test results for the LR direction, presented in Table 3, indicate that the setup error in the BodyFIX group was significantly reduced by 1.07 mm compared to the ABC group. Additionally, the setup error in the airbag group was reduced by 2.13 mm compared to the ABC group. When comparing the airbag and BodyFIX groups, the setup error in the airbag group was reduced by 1.06 mm. All observed differences in the LR direction were statistically significant.
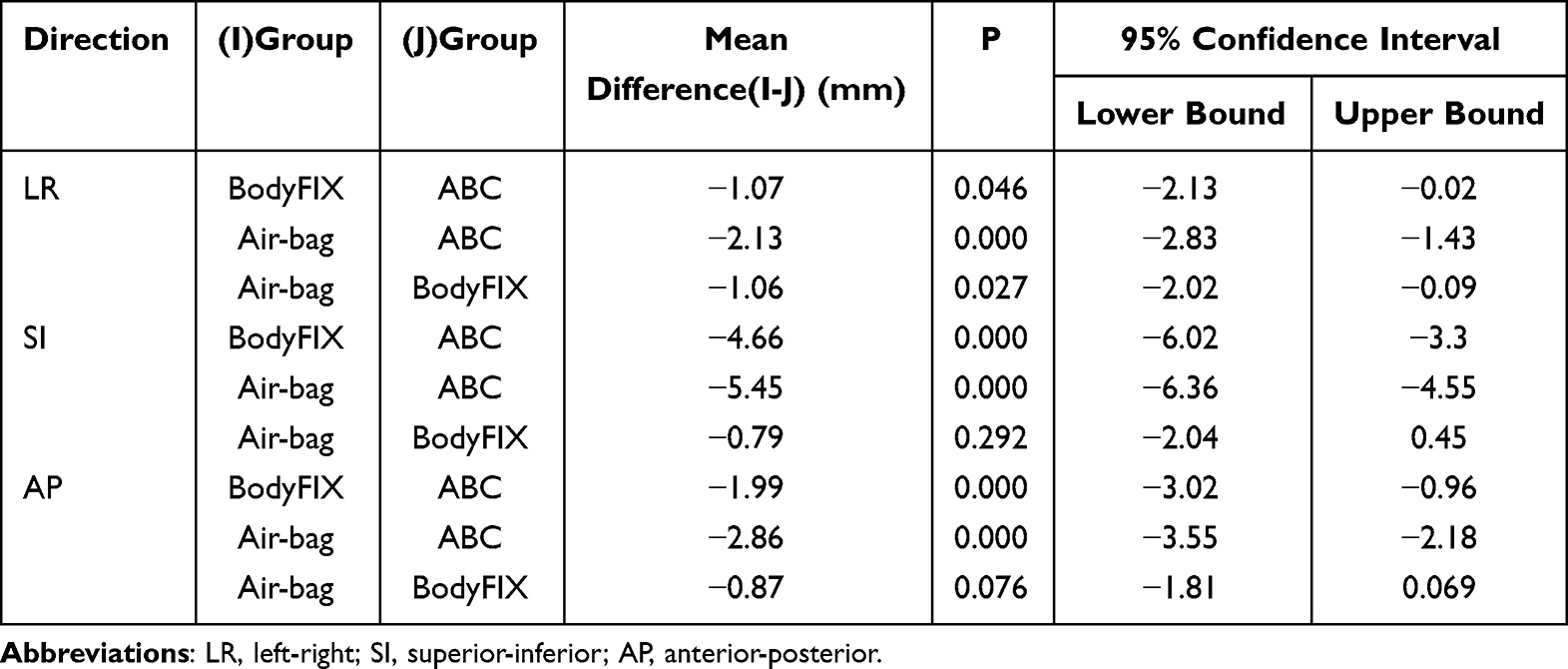 |
Table 3 Comparison Results of Three Groups in the LR, SI and AP Directions |
The Tukey’s test results for the SI direction, summarized in Table 3, demonstrate that the setup error in the BodyFIX group was significantly reduced by 4.66 mm compared to the ABC group. Similarly, the setup error in the airbag group was reduced by 5.45 mm compared to the ABC group, with statistical significance. However, the reduction in setup error between the airbag group and the BodyFIX group was 0.79 mm, which was not statistically significant.
The Tukey’s test results for the AP direction, presented in Table 3, indicate that compared to the ABC group, the setup error in the BodyFIX group was significantly reduced by 1.99 mm. Similarly, the setup error in the airbag group was reduced by 2.86 mm compared to the ABC group, with statistical significance. However, the reduction in setup error between the airbag group and the BodyFIX groups was 0.87 mm, which was not statistically significant.
Analysis of Random Errors, Systematic Errors, and PTV Margins
Table 4 summarizes the total random errors, systematic errors, and corresponding PTV margins for the ABC, BodyFix, and airbag groups, calculated using the previously described formula. The results indicate that errors and PTV margins in the SI direction are greater than those in the LR and AP directions. Among the three groups, the airbag group exhibited the smallest random errors, systematic errors, and PTV margins across all three directions, whereas the ABC group demonstrated the largest values for these parameters.
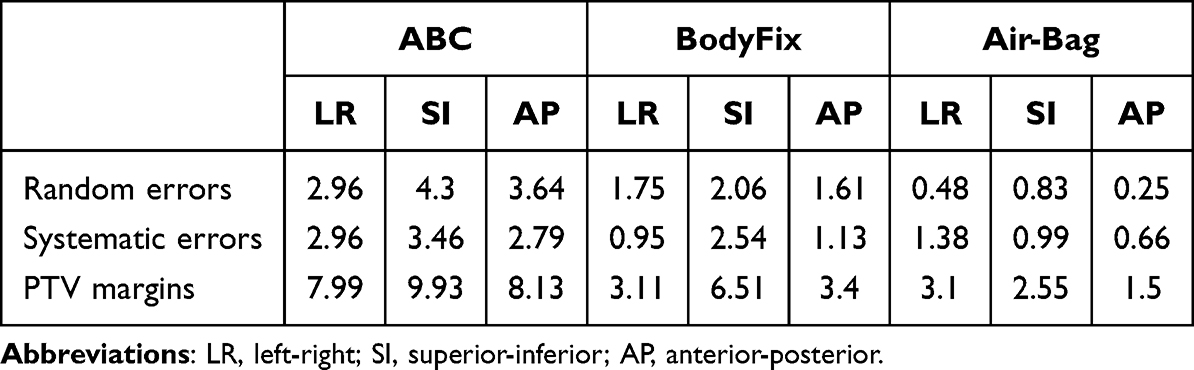 |
Table 4 Analysis of the PTV Margins by Three Groups (mm) |
Discussion
Radiation therapy has traditionally been considered a palliative approach in the local treatment of hepatic malignancies.14 External beam conformal radiation therapy, however, carries a risk of significant toxicity, potentially resulting in radiation-induced liver disease.10 SBRT has demonstrated potential benefits both as a standalone treatment and in combination with other local therapies, achieving tumor control rates comparable to those of standard ablation techniques.15,16 In patients with primary or metastatic hepatic malignancies who are not eligible for surgical intervention, SBRT has been associated with high local control rates,17–19 which may correlate with improved survival outcomes.16,20
Effective motion management and appropriate selection of image-guided radiation therapy play a critical role in optimizing tumor coverage while minimizing irradiation of normal tissues. The present study investigated three respiratory motion management techniques: ABC, BodyFix, and the airbag technique. Among these, ABC utilizes the DIBH method,21 whereas BodyFix and the airbag technique employ AC. The analysis of setup errors, random errors, systematic errors, and PTV margins indicated that, in SBRT for hepatic malignancies, AC-based techniques provided more effective motion control compared to DIBH.
As shown in Table 2, among the three respiratory motion management modes, ABC, BodyFix, and the airbag technique, setup errors in the SI direction were the most significant compared to the other two directions. This finding is likely attributable to respiratory-induced liver motion.22 Although liver movement is anisotropic, displacement predominantly occurs in the SI direction.23–26
In all three directions (LR, SI, and AP), setup errors observed in the ABC group were significantly greater than those in the BodyFIX and airbag groups. Despite pre-treatment assessments and breath-training exercises performed prior to ABC fixation, factors such as stress or anxiety during treatment may necessitate multiple breath-hold attempts after inspiration. Repeated breath-holding can lead to changes in tumor position, thereby reducing treatment accuracy. There are also some patients with poor lung function. They may not be able to cooperate in the training of holding their breath after inhaling.
The extent of liver motion restriction varies based on the degree of AC applied.27 Heinzerling et al demonstrated through 4D-CT imaging that strong AC provided significantly better tumor control movement in the liver compared to moderate AC.6 These findings are consistent with the results of the present study, in which the airbag technique exerted greater pressure on the upper abdomen compared to the BodyFix system, which applied distributed pressure across the chest and abdominal cavity. The findings demonstrated that setup errors in all three directions were smaller in the airbag group compared to the BodyFix group.
Zhong et al28 reported setup errors for liver SBRT using an ABC system, with systematic errors measuring 3.18 mm in the LR direction, 6.80 mm in the SI direction, and 3.05 mm in the AP direction. The corresponding random errors were 3.03 mm in the LR direction, 6.78 mm in the SI direction, and 3.62 mm in the AP direction.
In the present study, both systematic and random errors for liver SBRT using the ABC system were lower compared to those reported by Zhong et al.28 Specifically, systematic errors measured 2.96 mm in the LR direction, 3.46 mm in the SI direction, and 2.79 mm in the AP direction, while the random errors were 2.96 mm, 4.30 mm, and 3.64 mm in these respective directions. These findings suggest improved error control in the current study, which may be attributed to the use of the original ABC system provided by Elekta, whereas a modified version was utilized in the previous study.
Among the three motion management techniques analyzed, the ABC group exhibited the largest setup errors, consistent with the data presented in Table 4. Systematic errors, random errors, and PTV margins were significantly higher in the ABC group compared to the other two groups. The airbag group demonstrated substantial reductions in PTV margins, with decreases of approximately 61% in the LR direction compared to the ABC group, 74% in the SI direction relative to the ABC group (and 61% compared to the BodyFix group), and 82% in the AP direction relative to the ABC group (and 56% compared to the BodyFix group). Precise PTV margins are critical for liver SBRT to ensure adequate target dose coverage while effectively minimizing radiation exposure to the surrounding healthy liver tissue.
Patients utilizing the ABC system are required to undergo pre-training in breathing techniques. Those with compromised pulmonary function are not eligible for its use. The BodyFix system involves applying negative pressure to the entire thoracic and abdominal regions, a process that tends to be more time-consuming. In comparison, the airbag fixation method is straightforward and user-friendly, resulting in higher patient compliance.
This study has several limitations. First, the retrospective design limits the ability to establish causal relationships. Second, unequal group sizes may reduce statistical power and constrain the generalizability of the results. Additionally, intra-fraction motion was not assessed. A more accurate assessment of target position errors and irradiation dose deviations can be achieved by comparing pre- and post-irradiation images.
Tumor location and size may also influence hepatic motion and setup accuracy. As demonstrated by Kitamura et al,29 patients with cirrhosis exhibit significantly greater liver motion than those without, whereas individuals who have undergone partial hepatectomy show significantly reduced motion. Although our institution has conducted preliminary studies on these factors, the limited sample size has prevented conclusive results. Future studies with larger cohorts are warranted to better elucidate the impact of these variables on hepatic motion and positioning accuracy.
Conclusion
This study evaluated three respiratory motion management techniques—ABC, BodyFix, and the airbag technique—in the context of SBRT for hepatic malignancies. The findings indicate that the ABC technique is associated with the largest setup errors, whereas the airbag technique suggests greater positioning accuracy, improved reproducibility, and the potential for PTV margin reduction. Further investigations are warranted to verify the superiority of this approach in different populations and settings.
Abbreviations
SBRT, stereotactic body radiation therapy; ABC, Active Breathing Coordinator; CBCT, cone-beam computed tomography; LR, left-right; SI, superior-inferior; AP, anterior-posterior; TACE, transarterial chemoembolization; RFA, radiofrequency ablation; PTV, planning target volume; DIBH, deep inspiration breath hold; AC, abdominal compression; CT, Computed tomography; XVI, X-ray Volume Imaging; RILD, radiation-induced liver disease; IGRT, image-guided radiation therapy.
Ethics Approval
This study was conducted with approval from the Ethics Committee of the institutional review board of the Affiliated Huaian No.1 People’s Hospital of Nanjing Medical University (Approval No. KY-2025-028-01). This study was conducted in accordance with the declaration of Helsinki.
Consent Statement
All participants provided written informed consent for access to their medical records and anonymized publication prior to their treatment in this retrospective study.
Acknowledgment
The authors thank all members of our radiotherapy Center for their discussion on this project.
Funding
No external funding received to conduct this study.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Dawson LA. Overview: where does radiation therapy fit in the spectrum of liver cancer local-regional therapies? Semin Radiat Oncol. 2011;21(4):241–246. doi:10.1016/j.semradonc.2011.05.009
3. Sharma M, Nano TF, Akkati M, et al. A systematic review and meta-analysis of liver tumor position variability during SBRT using various motion management and IGRT strategies. Radiother Oncol. 2022;166:195–202. doi:10.1016/j.radonc.2021.11.022
4. Blomgren H, Lax I, Näslund I, Svanström R. Stereotactic high dose fraction radiation therapy of extracranial tumors using an accelerator. Clinical experience of the first thirty-one patients. Acta Oncol. 1995;34(6):861–870. doi:10.3109/02841869509127197
5. Méndez Romero A, Wunderink W, Hussain SM, et al. Stereotactic body radiation therapy for primary and metastatic liver tumors: a single institution Phase I-II study. Acta Oncol. 2006;45(7):831–837. doi:10.1080/02841860600897934
6. Heinzerling JH, Anderson JF, Papiez L, et al. Four-dimensional computed tomography scan analysis of tumor and organ motion at varying levels of abdominal compression during stereotactic treatment of lung and liver. Int J Radiat Oncol Biol Phys. 2008;70(5):1571–1578. doi:10.1016/j.ijrobp.2007.12.023
7. Hardcastle N, Gaudreault M, Yeo AU, et al. Selection of motion management in liver stereotactic body radiotherapy and its impact on treatment time. Phys Imaging Radiat Oncol. 2023;25:100407. doi:10.1016/j.phro.2022.12.004
8. McConnell K, Kirby N, Rasmussen K, Gutierrez AN, Papanikolaou N, Stanley D. Variability of breast surface positioning using an active breathing coordinator for a deep inspiration breath hold technique. Cureus. 2021;13(6):e15649. doi:10.7759/cureus.15649
9. Prasad S, Bell LJ, Zwan B, et al. Comparing immobilisation devices in gynaecological external beam radiotherapy: improving inter-fraction reproducibility of pelvic tilt. J Med Radiat Sci. 2024;71:529–539. doi:10.1002/jmrs.804
10. Koay EJ, Owen D, Das P. Radiation-induced liver disease and modern radiotherapy. Semin Radiat Oncol. 2018;28(4):321–331. doi:10.1016/j.semradonc.2018.06.007
11. Hu Y, Zhou YK, Chen YX, Shi SM, Zeng ZC. 4D-CT scans reveal reduced magnitude of respiratory liver motion achieved by different abdominal compression plate positions in patients with intrahepatic tumors undergoing helical tomotherapy. Med Phys. 2016;43(7):4335. doi:10.1118/1.4953190
12. Radiologists, The Royal College Of. On Target: Ensuring Geometric Accuracy in Radiotherapy; 2008.
13. Stroom JC, Heijmen BJ. Geometrical uncertainties, radiotherapy planning margins, and the ICRU-62 report. Radiother Oncol. 2002;64(1):75–83. doi:10.1016/s0167-8140(02)00140-8
14. Wen N, Cai Y, Li F, et al. The clinical management of hepatocellular carcinoma worldwide: a concise review and comparison of current guidelines: 2022 update. Biosci Trends. 2022;16(1):20–30. doi:10.5582/bst.2022.01061
15. Roquette I, Bogart E, Lacornerie T, et al. Stereotactic body radiation therapy for the management of hepatocellular carcinoma: efficacy and safety. Cancers. 2022;14(16):3892. doi:10.3390/cancers14163892
16. Jeong Y, Jung J, Cho B, et al. Stereotactic body radiation therapy using a respiratory-gated volumetric-modulated arc therapy technique for small hepatocellular carcinoma. BMC Cancer. 2018;18(1):416. doi:10.1186/s12885-018-4340-7
17. Schefter TE, Kavanagh BD, Timmerman RD, et al. A Phase I trial of stereotactic body radiation therapy (SBRT) for liver metastases. Int J Radiat Oncol Biol Phys. 2005;62(5):1371–1378. doi:10.1016/j.ijrobp.2005.01.002
18. Wulf J, Hädinger U, Oppitz U, et al. Stereotactic radiotherapy of targets in the lung and liver. Strahlenther Onkol. 2001;177(12):645–655. doi:10.1007/pl00002379
19. Herfarth KK, Debus J, Lohr F, et al. Stereotactic single-dose radiation therapy of liver tumors: results of a phase I/II trial. J Clin Oncol. 2001;19(1):164–170. doi:10.1200/JCO.2001.19.1.164
20. Scorsetti M, Comito T, Cozzi L, et al. The challenge of inoperable hepatocellular carcinoma (HCC): results of a single-institutional experience on stereotactic body radiation therapy (SBRT). J Cancer Res Clin Oncol. 2015;141(7):1301–1309. doi:10.1007/s00432-015-1929-y
21. Dawson LA, Brock KK, Kazanjian S, et al. The reproducibility of organ position using active breathing control (ABC) during liver radiotherapy. Int J Radiat Oncol Biol Phys. 2001;51:1410–1421. doi:10.1016/S0360-3016(01)02653-0
22. Eccles C, Brock KK, Bissonnette JP, Hawkins M, Dawson LA. Reproducibility of liver position using active breathing coordinator for liver cancer radiotherapy. Int J Radiat Oncol Biol Phys. 2006;64:751–759. doi:10.1016/j.ijrobp.2005.05.066
23. Brock KK, Hawkins M, Eccles C, et al. Improving image-guided target localization through deformable registration. Acta Oncol. 2008;47(7):1279–1285. doi:10.1080/02841860802256491
24. Gierga DP, Chen GT, Kung JH, et al. Quantification of respiration-induced abdominal tumor motion and its impact on IMRT dose distributions. Int J Radiat Oncol Biol Phys. 2004;58(5):1584–1595. doi:10.1016/j.ijrobp.2003.09.077
25. Shimizu S, Shirato H, Aoyama H, et al. High-speed magnetic resonance imaging for four-dimensional treatment planning of conformal radiotherapy of moving body tumors. Int J Radiat Oncol Biol Phys. 2000;48(2):471–474. doi:10.1016/s0360-3016(00)00624-6
26. Case RB, Moseley DJ, Sonke JJ, et al. Interfraction and intrafraction changes in amplitude of breathing motion in stereotactic liver radiotherapy. Int J Radiat Oncol Biol Phys. 2010;77(3):918–925. doi:10.1016/j.ijrobp.2009.09.008
27. Chu KY, Cooke R, Van den Heuvel F, Mukherjee S, Hawkins MA. Impact of abdominal compression on setup error and image matching during radical abdominal radiotherapy. Tech Innov Patient Support Radiat Oncol. 2019;12:28–33. doi:10.1016/j.tipsro.2019.11.003
28. Zhong R, Wang J, Jiang X, et al. Hypofraction radiotherapy of liver tumor using cone beam computed tomography guidance combined with active breath control by long breath-holding. Radiother Oncol. 2012;104(3):379–385. doi:10.1016/j.radonc.2011.11.007
29. Kitamura K, Shirato H, Seppenwoolde Y, et al. Tumor location, cirrhosis, and surgical history contribute to tumor movement in the liver, as measured during stereotactic irradiation using a real-time tumor-tracking radiotherapy system. Int J Radiat Oncol Biol Phys. 2003;56(1):221–228. doi:10.1016/s0360-3016(03)00082-8
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.