")
Back to Journals » International Journal of General Medicine » Volume 15
A Retrospective Analysis of the Bacterial Infections, Antibiotic Use, and Mortality Predictors of COVID-19 Patients
Authors Suranadi IW , Sucandra IMAK, Fatmawati NND, Wisnawa ADF
Received 4 January 2022
Accepted for publication 21 March 2022
Published 1 April 2022 Volume 2022:15 Pages 3591—3603
DOI https://doi.org/10.2147/IJGM.S351180
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
I Wayan Suranadi,1 I Made Agus Kresna Sucandra,1 Ni Nengah Dwi Fatmawati,2 Ayu Dilia Febriani Wisnawa3
1Department of Anesthesiology and Intensive Care, Faculty of Medicine, Udayana University, Denpasar, Bali, Indonesia; 2Department of Clinical Microbiology, Faculty of Medicine, Udayana University, Denpasar, Bali, Indonesia; 3Faculty of Medicine, Udayana University, Denpasar, Bali, Indonesia
Correspondence: I Wayan Suranadi, Department of Anesthesiology and Intensive Care, Faculty of Medicine, Udayana University/Sanglah General Hospital, Denpasar, Bali, 80113, Indonesia, Tel +62 812 3846 3838, Email [email protected]
Purpose: This study aimed to investigate the rate and profile of bacterial infections, mortality-associated predictors, and report the most common microorganisms and antibiotic use in coronavirus disease-19 (COVID-19) patients.
Patients and Methods: This study used a retrospective approach to evaluate the bacterial culture, antibiotic use, comorbidities, imaging, and laboratory discoveries of patients with COVID-19 (hospitalized) confirmed by reverse transcription polymerase chain reaction (RT-PCR) between May and December 2020. We have selected 906 COVID-19 positive patients using a consecutive sampling technique and analyzed data using IBM SPSS-22 statistical software. Statistical analysis included univariate, bivariate, and multivariate analysis. It was carried out using multivariable logistic regression analysis to predict the mortality of COVID-19 patients.
Results: A total of 410 patients, which involved 247 males with a mean age of 53.9 years were evaluated. Based on the results, the positive bacterial culture was detected in 18.3% of all patients who sent the culture sample test, representing bacterial infections. The Acinetobacter baumannii was the most commonly identified organism, while the proportion of patients treated with antibiotics was 83.4%. Furthermore, azithromycin was prescribed in the highest number of patients with approximately 44.3% of all antibiotics. The total mortality rate was 39.8% and its ratio was higher in COVID-19 patients with bacterial infections (65.3%, X2 = 25.1, P< 0.001). Patients mortality who used antibiotics were also higher compared to those who did not (89% vs 11%, P< 0.014). Age, length of hospitalization, bacterial infection, shortness of breath, neutrophil-to-lymphocyte ratio (NLR), and diabetes mellitus were also associated predictors to increased hospital mortality (adjusted OR (aOR) 0.382, P< 0.013; aOR 4.265, P< 0.001; aOR 3.720, P< 0.001; aOR 3.889, P< 0.001; aOR 6.839, P< 0.003; aOR 1.844, P< 0.030), respectively.
Conclusion: This study discovered that there is high use of antibiotics amongst COVID-19 patients; however, the bacterial infection rates did not exceed one-fifth of the total patients. Furthermore, older age, bacterial infections, a longer length of hospitalization, diabetes mellitus, shortness of breath, and higher NLR have a significant impact on the mortality of COVID-19 patients.
Keywords: antibiotics, bacterial infections, COVID-19, mortality
Introduction
The novel coronavirus disease-19 (COVID-19) caused by Severe Acute Respiratory Syndrome Coronavirus-2 (SARS-CoV-2) has rapidly become a global health concern.1 There have been around 10 million confirmed cases of COVID-19 and 500,000 reported deaths, leading to a new public health crisis that threatens the healthcare system.2 The average mortality rate in country/territory-specific for COVID-19 cases is expected to fluctuate between 2%–3% globally and to be 0.7–1.3% higher than the previous report.2 In several microbiological studies, viral respiratory infection predisposes patients to bacterial infection, which often has a worse prognosis and severity.3,4 Bacterial infections have been recognized as a common complication of several viral respiratory tract infections and significant causes of morbidity and mortality.3 They can also complicate COVID-19 due to their effects as discovered in the 1918 influenza outbreak and the 2009 H1N1 influenza pandemic.3,5 Recent reports have shown disparities in case frequency and fatality rates of COVID-19 between various states due to several predictors.6 Previous studies showed that approximately 50% of patients who died with COVID-19 had bacterial infections,5,7 which also causes more detrimental outcomes and an increase in the risk of mortality.3,4 However, the impact of the bacterial infection on the poor prognosis of COVID-19 has not been adequately investigated. Therefore, there is a need to clinically study the effects of bacterial infections and predictors of hospital mortality in COVID-19 patients to elucidate and determine their outcomes.
The symptoms are usually fever, cough, sore throat, shortness of breath, fatigue, and malaise. In most people, the clinical manifestations of the disease are mild, while in some (usually the elderly and those with comorbidities), it progresses to pneumonia, acute respiratory distress syndrome (ARDS), and multi-organ failure.8 There is no current evidence of definitive treatment for COVID-19 patients, however, antibiotics are being widely used in most centers for treatment due to the low prevalence of bacterial infection in patients.9 Although several studies used empiric antibiotics for treatment,10–12 there is still a discrepancy in its urgency and benefit. It was also stated that antibiotics are prescribed commonly to COVID-19 patients mainly due to suspected bacterial infection. Meanwhile, it is difficult to distinguish the symptoms of virus infection alone or co-infection with bacterial. There is evidence of the associated inflammatory markers to bacterial infection such as high c-reactive protein (CRP) and several inflammatory blood markers, which appear significantly in COVID-19 patients with bacterial infections.13,14 The disparity between bacterial infection prevalence and antibiotic use has raised concerns about its overuse and subsequent harm related to bacterial resistance.15 The overuse of antibiotics can lead to management failure to treat or prevent infection and antimicrobial resistance, the future consequence of the COVID-19 pandemic.15 Therefore, this study aims to determine the prevalence, profile of bacterial infection, associated predators of mortality, and antibiotics use in hospitalized COVID-19 patients.
Materials and Methods
Data Collection
This study was carried out using a hospital-based retrospective design to review 906 medical records from all hospitalized adult patients with laboratory-confirmed COVID-19 between May and December 2020 by RT-PCR. The samples were collected at Sanglah General Hospital, Denpasar, Bali, Indonesia, as a tertiary hospital from January to August 2021. The samples used were patients with bacterial culture tests and aged 18 years and above, while those excluded were in the outpatients setting (self-isolation) and lack of outcome or incomplete other data such as lack of antibiotics and bacterial culture data, missing laboratory data, etc. Furthermore, pregnant women, patients with malignancy, human immune deficiency virus, and immune deficiency syndromes were excluded due to the expected worst outcomes to avoid the potential confounding effects from their immunocompromised status.16,17 Based on the inclusion and exclusion criteria in Figure 1, a total of 410 patients were included in the final analyzed sample. Current study protocol conformed with the Declaration of Helsinki, national requirements for the conduct of retrospective studies and its following amandments and was approved by Universitas Udayana/Sanglah General Hospital research ethics committee (approval File Number: 2102/UN14.2.2.VII.14/LT/2021). The ethics committee of Sanglah General Hospital of Udayana University waived informed consent because this was a retrospective study. Data confidentiality was ensured by omitting protected health information. Patient data came from the medical record system and were anonymously analyzed to preserve patient privacy.
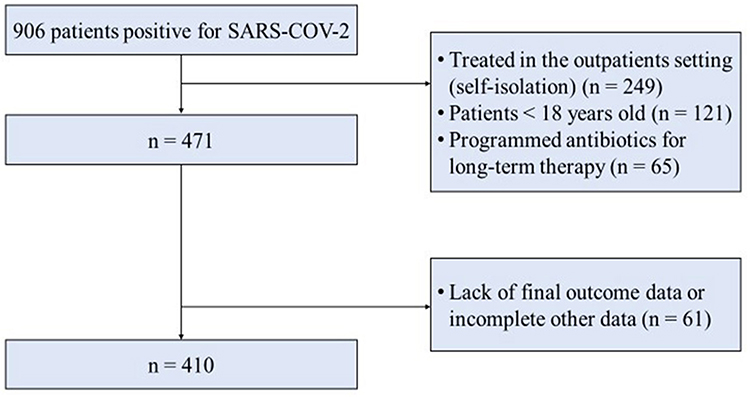 |
Figure 1 Flowchart of inclusion and exclusion. |
The following data were collected from electronic medical records among COVID-19 patients: (1) Demographic characteristics about the age and sex of patients. (2) Clinical data such as clinical symptoms, blood pressure, comorbidities, number of antibiotic use, and radiological assessments. (3) Laboratory discoveries such as white blood cell/WBC, absolute neutrophil count/ANC, absolute lymphocyte count/ALC, neutrophil-to-lymphocyte ratio/NLR, derived neutrophil-to-lymphocyte ratio/d-NLR, lymphocyte-to-monocyte ratio/LMR, platelet-to-lymphocyte ratio/PLR, and c-reactive protein/CRP. (4) The outcome of the COVID-19 disease was determined by the length of hospitalization and death of patients in the hospital. The laboratory results and blood pressure were also defined as single values dated from the first test after admission. The comorbid was assessed based on patient’s admission self-report in their medical record. The types of comorbidities were hypertension, cardiovascular disease such as heart failure, coronary artery disease, diabetes mellitus type 1 and 2, respiratory illness (COPD, asthma), renal disease (chronic kidney disease), and gastrointestinal (hepatitis B/C, cirrhosis, peptic ulcer). Similarly, bacterial infection was also defined as those patients with the positive result of bacterial infection from blood, respiratory, or urine culture results with persistent clinically compatible symptoms during specimen collection in COVID-19 patients. The obtained specimen samples were then examined by microbiologists at our hospital. The outcome of COVID-19 infection was defined as those patients with an outcome following hospital treatment in a certain period such as hospitalization and mortality. The data obtained were inputted into a standard-computerized database and cross-checked.
Statistical Analysis
Subsequently, categorical variables were displayed as frequencies (percentages), while continuous variables were presented as mean (SD, standard deviation) or median (IQR, interquartile range). The univariate analysis of categorical variables was conducted using the Chi-square or Fisher’s exact test, while an independent sample t-test or Mann–Whitney U-test was applied for continuous data. Multivariable logistic regressions were also carried out for the predictors in the bivariate analysis and were used to analyze associated predictors with mortality in COVID-19 patients. The variables from demographics, clinical signs and symptoms, comorbidities, and laboratory data were selected for multivariable analysis using logistic regressions model based on clinical justification and statistical reasoning from bivariate analyses (p<0.25). Odds ratio (OR) with 95% confidence interval (CI) were used to report the association between hospital mortality and exposure to the predictors. The statistical analysis was carried out with SPSS for windows version 22.0 (IBM Corp, Armonk, NY, USA), and P < 0.05 was considered statistically significant.
Results
Demographic and Clinical Characteristics of COVID-19 Patients
A total of 906 patients was identified with a positive COVID-19 test admitted during the study period, where 410 patients who fulfilled the inclusion criteria were included for analysis. Among the studies that reported specific patient characteristics, the mean age was 53.9 years (SD±13.9), with 39.8% females and the systolic per diastolic blood pressure was 110/70 mmHg. Based on clinical symptoms, shortness of breath was the most common symptom affecting approximately 64.1% of all patients, followed by cough (42.9%) and fever (33.4%). The most frequent comorbid in patients were diabetes mellitus (25.4%), renal disease (20.5%), and cardiovascular disease (19.5%). Furthermore, the length of hospitalization ranged from 5–12 days, with 9 days in major. From the available data, 163 (39.8%) of total patients died from the COVID-19, while the bacterial infection was 18.3% (75 of 410 patients) and those received antibiotic treatment were 83.4% (342 of 410 patients).
Rate and Profile of Bacterial Infection in COVID-19 Patients
Based on the results, 75 COVID-19 patients with bacterial infections had a more prolonged hospitalization (10 days; IQR 4–14 days), which was not significantly different. Shortness of breath was statistically different in both the groups, with a high proportion (81.3%) of COVID-19 patients with bacterial infection than 60.3% of patients without infection. In chest x-ray assessment, pulmonary consolidation opacities were the most common discovery in 324 patients (74%), typically bilateral (61.5%). There were 49 patients (65.3%) with bacterial infections who had died, therefore, in-hospital mortality rates were significantly higher compared to those without infection. A significant number of patients (66%) without bacterial infection were discharged from the hospital after recovery from COVID-19. Based on two study groups, the proportion of patients who developed bacterial infection since the detection of COVID-19 until discharge was 18.3% (n=75, p < 0.001). Furthermore, patients receiving antibiotic agents more than or equal to 2 were higher in patients with bacterial infection than those without infection (Table 1).
 |
Table 1 Baseline Characteristics of COVID-19 Patients |
Among the COVID-19 patients, only less than one-fifth of the total patients were tested positive for bacterial infection, where gram-negative bacterial were commonly identified than gram-positive. The leading micro-organisms isolated were Acinetobacter baumannii (n=20 patients, 26.7%), followed by Klebsiella pneumonia (n=18 patients, 24%), and Pseudomonas aeruginosa (n=12 patients, 13%). This showed that several patients can have multiple infections from different types of bacterial (Table 2).
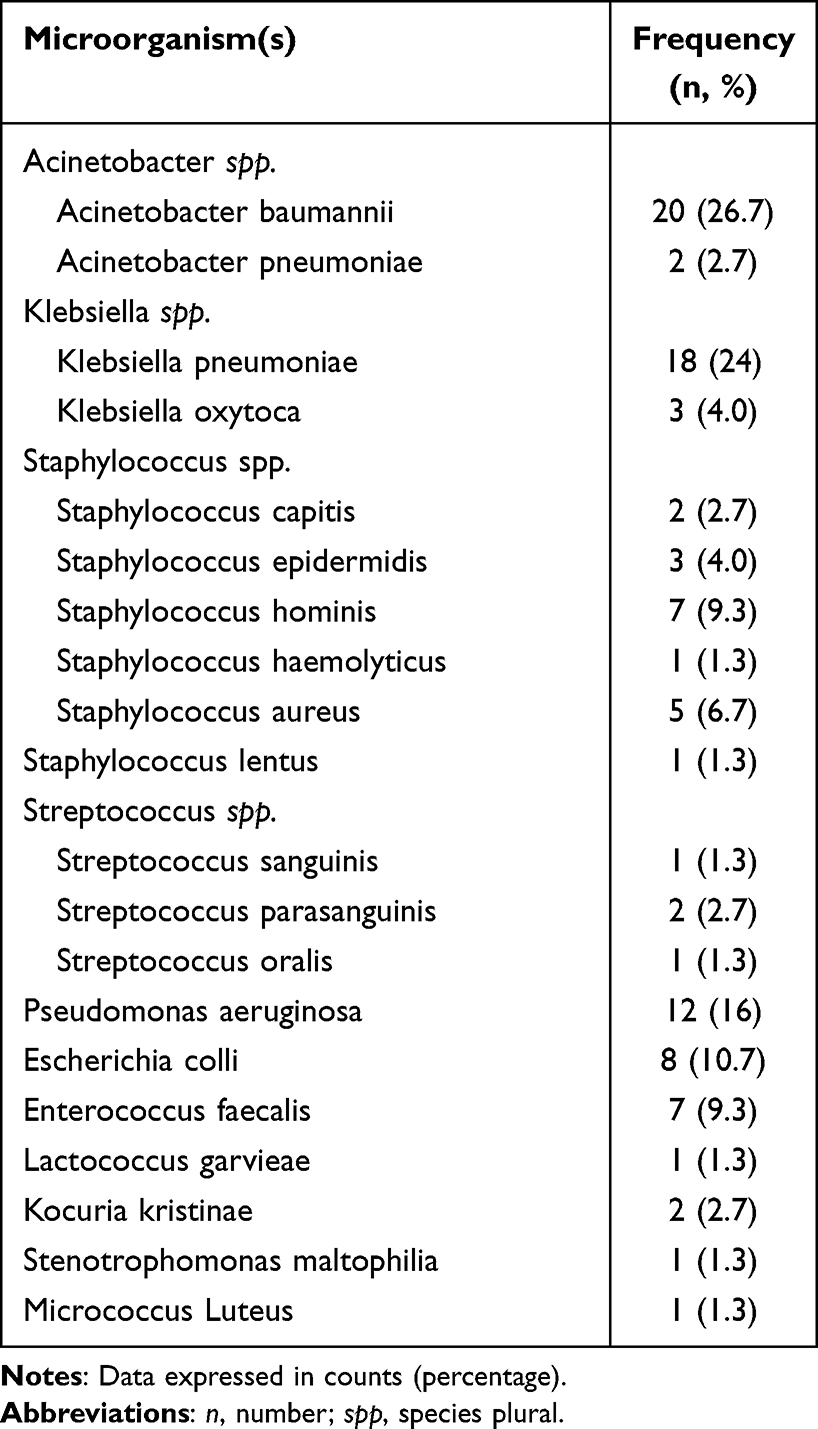 |
Table 2 Bacterial Microorganism(s) Identified of COVID-19 Patients |
Antibiotic Use in COVID-19 Patients
Out of 410 hospitalized patients, a total of 574 antibiotics were prescribed for 342 (83.4%) patients. The median proportion of antibiotics prescribed for each patient was 1 (IQR 1–2), with 5 antibiotics as the highest number. It was discovered that antibiotics were prescribed approximately in 274 (80.1%) for COVID-19 patients without bacterial infection from bacterial culture. Meanwhile, each antibiotic was compared based on the number of antibiotics used during hospitalization to quantify the distribution of prescriptions and show its usage profiles in the COVID-19 setting. The mortality rate comparison between patients who used antibiotics and those without antibiotics was summarized in Figure 2. Most patients had one antibiotic (45.4%), while 38% received a combination of antibiotics. Similarly, for most patients who received antibiotics during treatment, azithromycin (44.3%) was the most frequently prescribed, followed by levofloxacin (41.8%), and ceftriaxone (16.8%) (Figure 3). The results showed that approximately 89% (p=0.014) of all in-hospital patients that died due to COVID-19 received a significant antibiotics treatment compared to those without antibiotics (11%).
 |
Figure 2 Patient-reported outcomes. (A) comparison of patient outcomes between patients who used antibiotics and those without antibiotics (p<0.014). (B) Comparison of patient outcomes based on the number of antibiotics used during hospitalization (p<0.002). Blue dashed line represents significant increasing linear trend of hospital mortality in those with more antibiotics use; Grey dashed line represents significant decreasing linear trend of hospital mortality in those with fewer antibiotics use; %, percentage; n, number. |
 |
Figure 3 The types of antibiotics. (A) The distribution of antibiotics used during hospitalization. (B) Comparison of (B) shows the number of antibiotics during hospitalization based on their types of antibiotics. %, percentage. |
Laboratory Discoveries in COVID-19 Patients
There were similarities in laboratory discoveries between WBC and ANC values in the two groups, where ALC, NLR, d-NLR, PLR, LMR, and CRP were significantly higher in patients with antibiotics treatment. Moreover, all inflammatory markers were significantly elevated, except for WBC and ANC compared to those without antibiotics (Table 3).
 |
Table 3 Comparison of Inflammatory Markers in COVID-19 Patients |
Predictors of Mortality in COVID-19 Patients
Out of 410 patients, 163 (39.8%) died and 247 (60.2%) were discharged alive, meanwhile, the median length of stay in patients who get full recovery in hospital was 10 days (IQR 7–13 days) and in death, it was 6 days (3–11 days). The results of the multivariable analysis are summarized in Table 4. Moreover, age, length of stay, bacterial infection, shortness of breath, NLR, and diabetes mellitus patients were identified as the significant risk factors of in-hospital mortality among COVID-19 patients. Based on observed patients, older age (adjusted OR (aOR), 0.382, 95% CI 0.179–0.818), the longer length of stay (aOR, 4.265; 95% CI 2.551–7.131), higher NLR (aOR, 6.839, 95% CI 1.955–23.922), diabetes mellitus patients (aOR, 1.844, 95% CI 1.063–3.199), and patients with shortness of breath symptom (aOR 3.889; 95% CI 2.187–6.916) were identified as the risk factors of mortality among the COVID-19 patients. It was also discovered that patients with bacterial infection have almost 4 times the odds of death than those without infection after adjusting with other cofounding factors (adjusted OR 3.720; 95% CI 1.992–6.950; P < 0.001).
 |
Table 4 Mortality Predictors of COVID-19 Patients |
Discussion
COVID-19 has been placing significant pressure on global healthcare systems due to the rapid spread of the disease, particularly in resource-limited settings.17 This study is one of the first reports that expected to have crucial implications to describe and analyze some predictors of poor outcomes of COVID-19 patients, a profile of bacterial infections, and provide an overview of the impact of COVID-19 pandemic on antibiotic use and spread of bacterial pathogens. In Indonesia, research on bacterial infections, antibiotics use, and mortality predictors in confirmed patients with COVID-19 are still limited. Furthermore, this research offers additional value as baseline management data and antibiotic administration policy for patients with COVID-19, particularly those with bacterial infections.
This study found that the prevalence of bacterial infection in patients with confirmed COVID-19 was higher in those with more severe clinical symptoms, such as shortness of breath. Bacterial also contributes significantly to worsening the prognosis based on morbidity and mortality. This interesting finding describes how bacterial infection in COVID-19 patients contributes to the severity of the patient’s clinical condition and prognosis. This study documented 18.3% bacterial infections, a higher proportion compared to a study by Langford et al,16 where a pooled prevalence of confirmed bacterial infections was 8.0% (95% CI 6.1–9.9) and systematic review and meta-analysis of 38 studies examined bacterial infections in COVID-19 patients.16–18 Different studies carried out in the United States and several Asian and European countries discovered a highly variable prevalence of bacterial infection in patients diagnosed with COVID-19, ranging between 1% and 50%,19–22 due to the differences in criteria and diagnostic tests used.
The samples used were collected from all patients to identify the etiological agent responsible for the infection with a culture test, identifying 21 different bacteria species. This research also found that nosocomial bacteria dominated the result, thereby requiring more difficult management, similar to the data published in other studies.23,24 This study discovered that Acinetobacter baumannii was the major infecting bacterial pathogen, followed by Klebsiella pneumonia, and Pseudomonas aeruginosa. The species were the most commonly isolated microorganism in hospital-acquired infection since COVID-19 can lead to longer hospitalization, which was consistent with previous studies.25–27 However, there were no fungal superinfection cases recorded as reported by Hughes et al. After collecting the samples for culture, empirical antibiotic treatment was started according to the epidemiology of each institution and current local guidelines.
Based on observation of this study, antibiotics were commonly prescribed in the context of viral infection due to SARS-CoV-2 during the first wave of the COVID-19 pandemic. However, the mortality rate in patients with bacterial infection was higher than in those without bacterial infections, despite receiving more antibiotics. Among the antibiotic use, 17 types of antibiotics were prescribed as monotherapy (45.4%) and in combination (two combinations = 22.7%, more than or equal to three combinations = 15.4%), which were mostly from the “WATCH” and “RESERVE” categories. It was shown that more than half of the total patients received antibiotic treatment with the overall antibiotic prescribing rate, which was 83.4% of patients within the study period. Meanwhile, the antibiotics prescribed were mainly azithromycin (44.3%), levofloxacin (41.8%), ceftriaxone (16,8%), and cefoperazone (14,4%), which is similar to those in other studies. Antibiotic use was widespread, in the absence of bacterial infection. These results exceeded the standard recommended World Health Organization (WHO) value, which is 20–25.4%.28 Therefore, the high percentage of antibiotic prescriptions in the group of patients in the hospital is an aspect that is not in line with other studies, where the percentage of infection was much lower than the prescribed antibiotics. Moreover, the average number of antibiotics for each patient in this study was 1.4, which showed that patients are on at least one prescribed antibiotic, similar to the standard recommended by the WHO, with a limit of 1.6–1.8.28 Related studies demonstrate prolonged duration of antibiotic use despite absence of evidence for bacterial infection.29 The data that showed the prescription pattern of antibiotics in the study area was similar to the 1.29–1.4 antibiotics for each patient reported in studies conducted in Eritrea and Congo, respectively.30,31 The rates of bacterial infection as previously reported were lower, however, a large number of antibiotics were used against bacterial infections that were not properly demonstrated.9,32–34 Therefore, there is a need to examine the syndromic approach of this type of infection and implement programs to rationalize the use of the antibiotics in COVID-19 patients and prevent the increase in its use as well as the consequent impact on the resistance of the nosocomial microbiota.35
Based on multivariate analysis, bacterial infection is still one of the independent predictors of mortality in patients with confirmed COVID-19. This is consistent with the comparative analysis, which found a significant relationship between those infected with the COVID-19 bacterium and clinical severity, increasing markers of inflammation, and prevalence of mortality among patients in the group. In this study, the overall mortality was 39.8% and higher in those who had bacterial infections, which also can be higher when compared with other studies that vary from 12–28%.7,22 Meanwhile, the high mortality rate in this population is due to differences in thresholds for hospitalization in Indonesia and the presence of high-risk factors. It was also discovered that older age, longer length of stay, diabetes mellitus, bacterial infections, shortness of breath, and higher NLR value were the main predictors in the multivariate analysis. According to Yang et al,36 bacterial infection is a predominant inducer of death that can lead to the failure of many organs and systems, and contribute to mortality. In line with previous study,9 bacterial infection is an associated predictor of mortality that is driven by prolonged hospitalization due to severe disease in patients with comorbidities or slower recovery. Similarly, it is possible to develop bacterial infections during treatment to patients, which causes high in-hospital mortality.
Previously, older age has been well-established as an important independent risk factor of mortality in SARS and MERS.37 This study also confirmed that older age (>40 years old) was related to death in patients with COVID-19, similar to others in China and America.7,37 The biomechanism of these results was the age-dependent defects in T-cell and B-cell function and the excess production of type 2 cytokines, which can lead to a deficiency in control of viral replication, prolonged pro-inflammatory responses, and potentially contribute to poor outcomes.38
Patients in this study showed alteration in several inflammatory markers and in NLR value that has been a known indicator of systemic inflammation,39 where a higher NLR value increased the odds of death among all patients, whether clinically as a result of excessive use of antibiotics in patients with COVID-19 or because the patients receiving antibiotics had worse clinical severity than those who did not receive. This occurred due to the biological mechanism, where high NLR indicates an imbalance in the inflammatory response from increased neutrophil and decreased lymphocyte counts. Therefore, further analysis is needed to evaluate these findings specifically in future studies. Meanwhile, compared to other laboratory parameters that predict the prognosis of COVID-19, NLR is more practical for clinical application because it is easily obtained in routine blood tests. In settings with limited resources of this study, high cost is restrictive, NLR remains a simple, accessible, near real-time, and cost-effective biomarker.39
The results from previous studies suggested that diabetes mellitus was related to mortality. In this study, the presence of comorbidity, specifically diabetes mellitus significantly increased the risk of death among the population compared to those without such comorbidities. A recent meta-analysis of 6 studies showed that diabetes mellitus is an associated predictor for mortality in COVID-19 patients. Since the first reports of COVID-19 in Wuhan, high frequencies of hospitalized diabetic patients and those with fatal outcomes have shown that diabetes mellitus is a predictor for poor prognosis and lethality.40 Symptomatology was similar to the previous report, where only the shortness of breath was significantly more frequent in patients who died, associated with the predictor of inpatients mortality. These results were in line with the discoveries of Shi et al41 which showed that shortness of breath was a predictor for death, rather than other symptoms such as fever or cough. Zheng et al42 also reported that shortness of breath indicated the disease deterioration, leading to poor outcomes.
This study has several limitations, including first, the use of a single-center hospital that is not generalized to all hospitals in Indonesia and also the involvement of inpatients, which did not represent an outpatients setting. Second, the protocol of sending cultures through physicians’ discretion is different from other hospitals, therefore, the rates of bacterial infections can not be accurate. Third, many of the positive cultures are from non-sterile sites such as urine and respiratory tract secretions that represent colonization rather than true infection. Since the retrospective study restricted the ability to identify comprehensively, prospective studies are needed for more details.
Conclusion
In conclusion, this study discovered a major use of antibiotics amongst COVID-19 patients, despite the prevalence of bacterial infections that did not exceed one-fifth of total patients. Poor outcomes are higher in patients with bacterial infection. This showed that antibiotics can not offer considerable benefit to a large number of patients. The results showed that older age, the positive result of bacterial infections, the longer length of hospital stays, diabetes mellitus, shortness of breath, and higher NLR value are risk factors for COVID-19 patients, which needs to be Intensively addressed in the management of COVID-19. The importance of physicians to justifying and individualizing antibiotic use of each patient is essential as an approach of antibiotic stewardship to alleviate the adverse impact of COVID-19 pandemic on antimicrobial resistance. Consequently, antibiotic stewardship efforts are crucially needed about reducing unnecessary antibiotic exposure to patients in pandemic situations.
Acknowledgments
We would like to show our highest gratitude to the Committee of Antimicrobial Resistance Control Program in Sanglah General Hospital which provided great assistance and suppport with data collection.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Naming the coronavirus disease (COVID-19) and the virus that causes it; 2020. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it.
2. Cao Y, Hiyoshi A, Montgomery S. COVID-19 case-fatality rate and demographic and socioeconomic influencers: worldwide spatial regression analysis based on country-level data. BMJ Open. 2020;10(11):e043560. doi:10.1136/bmjopen-2020-043560
3. Feldman C, Anderson R. The role of co-infections and secondary infections in patients with COVID-19. Pneumonia. 2021;13(1):5. doi:10.1186/s41479-021-00083-w
4. Arnold FW, Fuqua JL. Viral respiratory infections: a cause of community-acquired pneumonia or a predisposing factor? Curr Opin Pulm Med. 2020;26(3):208–214. doi:10.1097/MCP.0000000000000666
5. Clancy C, Nguyen M. COVID-19, superinfections and antimicrobial development: What can we expect? Clin Infect Dis. 2020;46:1–17.
6. Loomba RS, Aggarwal G, Aggarwal S, et al. Disparities in case frequency and mortality of coronavirus disease 2019 (COVID-19) among various states in the United States. Ann Med. 2021;53(1):151–159. doi:10.1080/07853890.2020.1840620
7. Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054–1062. doi:10.1016/S0140-6736(20)30566-3
8. Singhal T. A review of Coronavirus disease-2019 (COVID-19). Indian J Pediatr. 2020;87(4):281–286. doi:10.1007/s12098-020-03263-6
9. Goncalves Mendes Neto A, Lo KB, Wattoo A, et al. Bacterial infections and patterns of antibiotic use in patients with COVID-19. J Med Virol. 2021;93(3):1489–1495. doi:10.1002/jmv.26441
10. Rawson TM, Moore LSP, Castro-Sanchez E, et al. COVID-19 and the potential long-term impact on antimicrobial resistance. J Antimicrob Chemother. 2020;75(7):1681–1684. doi:10.1093/jac/dkaa194
11. Wang Z, Yang B, Li Q, Wen L, Zhang R. Clinical features of 69 cases with coronavirus disease 2019 in Wuhan, China. Clin Infect Dis. 2020;71(15):769–777. doi:10.1093/cid/ciaa272
12. Du RH, Liu LM, Yin W, et al. Hospitalization and critical care of 109 decedents with COVID-19 pneumonia in Wuhan, China. Ann Am Thorac Soc. 2020;17(7):839–846. doi:10.1513/AnnalsATS.202003-225OC
13. Lansbury L, Lim B, Baskaran V, Lim WS. Co-infections in people with COVID-19: a systematic review and meta-analysis. J Infect. 2020;81(2):266–275. doi:10.1016/j.jinf.2020.05.046
14. Skevaki C, Fragkou PC, Cheng C, Xie M, Renz H. Laboratory characteristics of patients infected with the novel SARS-CoV-2 virus. J Infect. 2020;81(2):205–212. doi:10.1016/j.jinf.2020.06.039
15. Llor C, Bjerrum L. Antimicrobial resistance: risk associated with antibiotic overuse and initiatives to reduce the problem. Ther Adv Drug Saf. 2014;5(6):229–241. doi:10.1177/2042098614554919
16. Langford BJ, So M, Raybardhan S, et al. Bacterial co-infection and secondary infection in patients with COVID-19: a living rapid review and meta-analysis. Clin Microbiol Infect. 2020;26(12):1622–1629. doi:10.1016/j.cmi.2020.07.016
17. Sanche S, Lin YT, Xu C, Romero-Severson E, Hengartner N, Ke R. High contagiousness and rapid spread of severe acute respiratory syndrome coronavirus 2. Emerg Infect Dis. 2020;26(7):1470–1477. doi:10.3201/eid2607.200282
18. Hughes S, Troise O, Donaldson H, Mughal N, Moore LSP. Bacterial and fungal coinfection among hospitalized patients with COVID-19: a retrospective cohort study in a UK secondary-care setting. Clin Microbiol Infect. 2020;26(10):1395–1399. doi:10.1016/j.cmi.2020.06.025
19. Arentz M, Yim E, Klaff L, et al. Characteristics and outcomes of 21 critically ill patients with COVID-19 in Washington State. JAMA. 2020;323(16):1612–1614. doi:10.1001/jama.2020.4326
20. Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395(10223):507–513. doi:10.1016/S0140-6736(20)30211-7
21. Young BE, Ong SWX, Kalimuddin S, et al. Epidemiologic features and clinical course of patients infected with SARS-CoV-2 in Singapore. JAMA. 2020;323(15):1488–1494. doi:10.1001/jama.2020.3204
22. Grasselli G, Zangrillo A, Zanella A, et al. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy Region, Italy. JAMA. 2020;323(16):1574–1581. doi:10.1001/jama.2020.5394
23. Nori P, Cowman K, Chen V, et al. Bacterial and fungal coinfections in COVID-19 patients hospitalized during the New York City pandemic surge. Infect Control Hosp Epidemiol. 2021;42(1):84–88. doi:10.1017/ice.2020.368
24. Zhu X, Ge Y, Wu T, et al. Co-infection with respiratory pathogens among COVID-2019 cases. Virus Res. 2020;285:198005. doi:10.1016/j.virusres.2020.198005
25. Bianco A, Capano MS, Mascaro V, Pileggi C, Pavia M. Prospective surveillance of healthcare-associated infections and patterns of antimicrobial resistance of pathogens in an Italian intensive care unit. Antimicrob Resist Infect Control. 2018;7(1):1–6. doi:10.1186/s13756-018-0337-x
26. Mahendra M, Jayaraj BS, Lokesh KS, et al. Antibiotic prescription, organisms and its resistance pattern in patients admitted to respiratory ICU with respiratory infection in Mysuru. Indian J Crit Care Med. 2018;22(4):223–230. doi:10.4103/ijccm.IJCCM_409_17
27. Moreno-Torres V, de Mendoza C, de la Fuente S, et al.; Puerta de Hierro COVID-19 working group. Bacterial infections in patients hospitalized with COVID-19. Intern Emerg Med. 2021;18:1–8.
28. World Health Organization. How to investigate antimicrobial use in hospitals: selected indicators. World Health Organization; 2012.
29. Townsend L, Hughes G, Kerr C, et al. Bacterial pneumonia coinfection and antimicrobial therapy duration in SARS-CoV-2 (COVID-19) infection. JAC Antimicrob Resist. 2020;2(3):dlaa071. doi:10.1093/jacamr/dlaa071
30. Amaha ND, Berhe YH, Kaushik A. Assessment of inpatient antibiotic use in Halibet National Referral Hospital using WHO indicators: a retrospective study. BMC Res Notes. 2018;11(1):904. doi:10.1186/s13104-018-4000-7
31. Wambale J, Iyamba J, Mathe D, Kavuo S. Takaisi-kikuni point prevalence study of antibiotic use in hospitals in Butembo. Int J Med Sci. 2016;8(12):133–139. doi:10.5897/IJMMS2016.1249
32. Liu C, Wen Y, Wan W, Lei J, Jiang X. Clinical characteristics and antibiotics treatment in suspected bacterial infection patients with COVID-19. Int Immunopharmacol. 2021;90:107157. doi:10.1016/j.intimp.2020.107157
33. Karami Z, Knoop BT, Dofferhoff ASM, et al. Few bacterial co-infections but frequent empiric antibiotic use in the early phase of hospitalized patients with COVID-19: results from a multicentre retrospective cohort study in The Netherlands. Infect Dis. 2021;53(2):102–110. doi:10.1080/23744235.2020.1839672
34. Seaton RA, Gibbons CL, Cooper L, et al. Survey of antibiotic and antifungal prescribing in patients with suspected and confirmed COVID-19 in Scottish hospitals. J Infect. 2020;81(6):952–960. doi:10.1016/j.jinf.2020.09.024
35. Bengoechea JA, Bamford CG. SARS-CoV-2, bacterial co-infections, and AMR: the deadly trio in COVID-19? EMBO Mol Med. 2020;12(7):e12560. doi:10.15252/emmm.202012560
36. Yang X, Yu Y, Xu J, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med. 2020;8(5):475–481. doi:10.1016/S2213-2600(20)30079-5
37. Albitar O, Ballouze R, Ooi JP, Sheikh Ghadzi SM. Risk factors for mortality among COVID‐19 patients. Diabetes Res Clin Pract. 2020;166:108293. doi:10.1016/j.diabres.2020.108293
38. Opal SM, Girard TD, Ely EW. The immunopathogenesis of sepsis in elderly patients. Clin Infect Dis. 2005;41(Supplement 7):S504–S512. doi:10.1086/432007
39. Ponti G, Maccaferri M, Ruini C, Tomasi A, Ozben T. Biomarkers associated with COVID-19 disease progression. Crit Rev Clin Lab Sci. 2020;57(6):389–399. doi:10.1080/10408363.2020.1770685
40. WHO Headquarters. Clinical management Clinical management Living guidance COVID-19. World Heal Organ; 2021. Available from: https://www.who.int/publications/i/item/WHO-2019-nCoV-clinical-2021-1.
41. Shi L, Wang Y, Wang Y, Duan G, Yang H. Dyspnea rather than fever is a risk factor for predicting mortality in patients with COVID-19. J Infect. 2020;81(4):647–679. doi:10.1016/j.jinf.2020.05.013
42. Zheng Z, Peng F, Xu B, et al. Risk factors of critical & mortal COVID-19 cases: a systematic literature review and meta-analysis. J Infect. 2020;81(2):e16–25. doi:10.1016/j.jinf.2020.04.021
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.