Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
A Rehabilitation-Based Multidisciplinary Care Model Reduces Hip Fracture Mortality in Older Adults
Authors Huang CF ![]() , Pan PJ, Chiang YH, Yang SH
, Pan PJ, Chiang YH, Yang SH
Received 26 July 2021
Accepted for publication 22 September 2021
Published 29 September 2021 Volume 2021:14 Pages 2741—2747
DOI https://doi.org/10.2147/JMDH.S331136
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Chun-Feng Huang,1,2 Po-Jung Pan,3 Yi-Hung Chiang,4 Shung-Haur Yang5
1Department of Family Medicine, National Yang Ming Chiao Tung University Hospital, Yilan, Taiwan (R.O.C); 2Department of Leisure Services Management, Chaoyang University of Technology, Taichung, Taiwan (R.O.C); 3Department of Physical Medicine and Rehabilitation, National Yang Ming Chiao Tung University Hospital, Yilan, Taiwan (R.O.C); 4Department of Orthopedics, National Yang Ming Chiao Tung University Hospital, Yilan, Taiwan (R.O.C); 5Department of Surgery, National Yang Ming Chiao Tung University Hospital, Yilan, Taiwan (R.O.C)
Correspondence: Chun-Feng Huang
Department of Family Medicine, National Yang Ming Chiao Tung University Hospital, No. 152, Xinmin Road, Yilan, Yilan County, 26042, Taiwan (R.O.C)
Tel +886-3-932-5192
Fax +886-3-9372119
Email [email protected]
Purpose: In older adults, the one-year mortality rate after experiencing a hip fracture ranges between 8% and 36%. The purpose of this study was to look at the efficacy of rehabilitation-based multidisciplinary care for older individuals who had hip fractures.
Patients and Methods: The study included 185 people (aged 65 and over) with a history of hip fracture surgery between February 2014 and March 2017. A survey was conducted one month and six months following the operation to assess the recovery of 93 individuals who were part of a rehabilitation-based multidisciplinary care program and 92 patients who were getting standard therapy with surgery and unsupervised physical therapy.
Results: Physical activity, gait, balance evaluation, and depression scale ratings all had statistical significance (P < 0.05) after participants received rehabilitation-based care services from multidisciplinary medical professionals. Furthermore, the refracture and one-year mortality rates in this rehabilitation-based multidisciplinary care model were lower than in the groups getting standard therapy.
Conclusion: The research indicates the efficacy of a multidisciplinary rehabilitation strategy provided by a collaborative medical team to older individuals with hip fractures.
Keywords: hip fracture, multidisciplinary care, osteoporosis, rehabilitation
Introduction
Every three seconds, one osteoporotic fracture occurs worldwide. The spine, hip, wrist, and humerus are the most prevalent sites for osteoporotic fractures.1 The risk of fracture rises with age due to bone mass loss and an increased risk of falls. After the age of 50, one-half of women and one-fifth of men experience a fracture.2 Refractures occur in nearly half of all patients with osteoporotic fractures.3,4 Hip fracture is one of the most serious complications of aging, and it is the seventh leading cause of death in older adults.5,6 As a result, patients suffering from hip fractures must take extra care to avoid complications including refractures.
Taiwan has been one of the world’s fastest aging regions.4 Aging causes decreased muscular strength, and a significant decline in balance and gait function; when these factors are combined with bone mass loss due to osteoporosis, the risk of hip fracture from low energy trauma increases even more.7 As a result, the number of individuals in Taiwan with fractures increased by 10% in five years, and more than 675,000 people seek medical attention each year as a result of a fracture.8 Hip fractures in older individuals have become a major public health concern, with the government incurring significant expenses to address the issue.
In Taiwan, four types of fracture treatment approaches for older persons are now used. The first and most prevalent approach is based on traditional care, in which patients with fractures are admitted to the hospital and treated by an orthopedist or orthopedic team, followed by unsupervised physical therapy. The second model is an enhanced conventional paradigm in which geriatric experts and orthopedists collaborate to create therapeutic approaches. Orthopedists offer pre-surgery treatment in the third model, while geriatric specialists provide post-surgery care. Patients with fractures are allocated to a specific fracture ward for older individuals in the fourth model, and care is given by orthopedists who specialize in working with older persons.
Even though different programs, such as the fracture liaison service, have been shown to minimize postoperative mortality and complications in hip fracture patients, a cohesive treatment approach tailored to Asian older hip fracture patients has yet to be developed.9 As a result, we created the Integrated Hip Fracture and Osteoporosis Rehabilitation Program for the Elderly (i-HOPE), a multidisciplinary care paradigm for older patients with hip fractures that emphasizes rehabilitation, osteoporosis therapy, and self-care techniques for improving home settings. The purpose of this study was to assess the risk of falling, the likelihood of refracture, general physical function, and mortality rate in older individuals with hip fractures who received the i-HOPE intervention.
Materials and Methods
Participants in the Study
This retrospective chart study looked at patients who had hip fracture surgery. For eligibility, all patients have been screened. From February 2014 to March 2017, a total of 185 patient records were reviewed. This research comprised individuals over the age of 65 who had no traumatic event and consented to surgery. Figure 1 depicts the enrollment criteria.
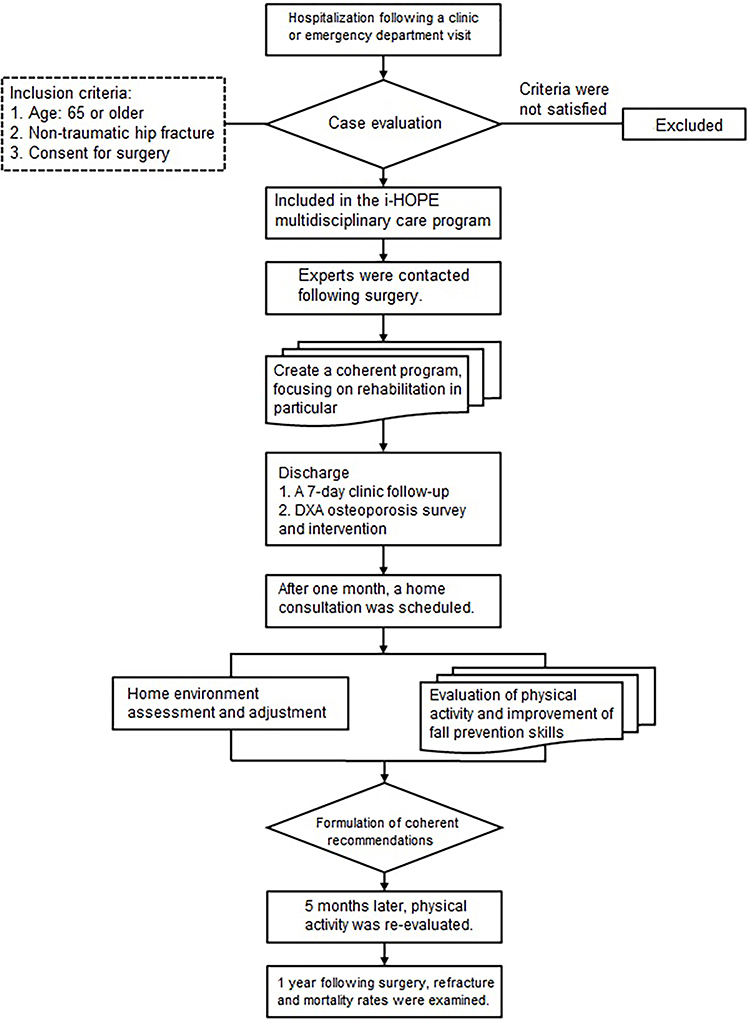 |
Figure 1 Enrollment in the i-HOPE program flowchart. |
Protocol on Intervention
Patients were separated into two groups based on whether they were engaged in the i-HOPE program or were receiving traditional care that included surgery and unsupervised physical therapy. During the hospitalization of i-HOPE program participants, multidisciplinary specialists were engaged to assess the patient and provide a comprehensive proposal immediately after the operation. The physical therapist began a tailored limb strengthening exercise program and walker-assisted ambulation training at the patient’s bedside. The occupational therapist advised each patient and their family on walking aid equipment and home environment changes. The fall prevention technique was emphasized once again during the one-month post-surgery home visit and out-patient department visit six months later, when the geriatric depression scale (GDS), activities of daily living (ADL), instrumental ADL, Elderly Mobility Scale (EMS), and Tinetti Performance Oriented Mobility Assessment (POMA) were used by geriatric specialists to assess each patient’s emotional state, physical activity, gait, and balance abilities.10–13 Furthermore, the medication adherence rate was calculated by summing the number of days the osteoporosis medicine was administered and dividing by the duration of a year.
Ethics
This study was approved by the Institutional Review Board (IRB) of the National Yang-Ming University Hospital (YMUH2016A027) in accordance with the Declaration of Helsinki. The study involves no prospectively collected data so there is no access to patients or opportunity to seek informed consent. A waiver of consent was approved by IRB as re-contacting this number of patients to obtain informed consent would be impracticable. The study is no greater than minimal risk and will have no direct impact on patient’s rights, confidentiality, or clinical care.
Statistical Analysis
To describe the fundamental features, descriptive statistics were utilized. Formal statistical analyses were carried out using IBM SPSS Statistics for Windows, version 22 (IBM Corp., Armonk, N.Y., USA). The difference in response variable change between subjects before and after the i-HOPE program was compared. A generic linear model with adjustments for age, gender, body mass index (BMI), and baseline value for medical conditions was used to evaluate differences between patients who received multidisciplinary care plans and those who did not. The minimum total sample size in this study is 128, with at least 64 subjects for each independent variable, for an effect size of d=0.5, power=0.8, and α=0.05.
Results
When the patients’ baseline characteristics were examined, there was no difference in sex, age, BMI, or medical issues between the individuals receiving multidisciplinary care (n=93) and the control groups receiving traditional care (n=92) (Table 1).
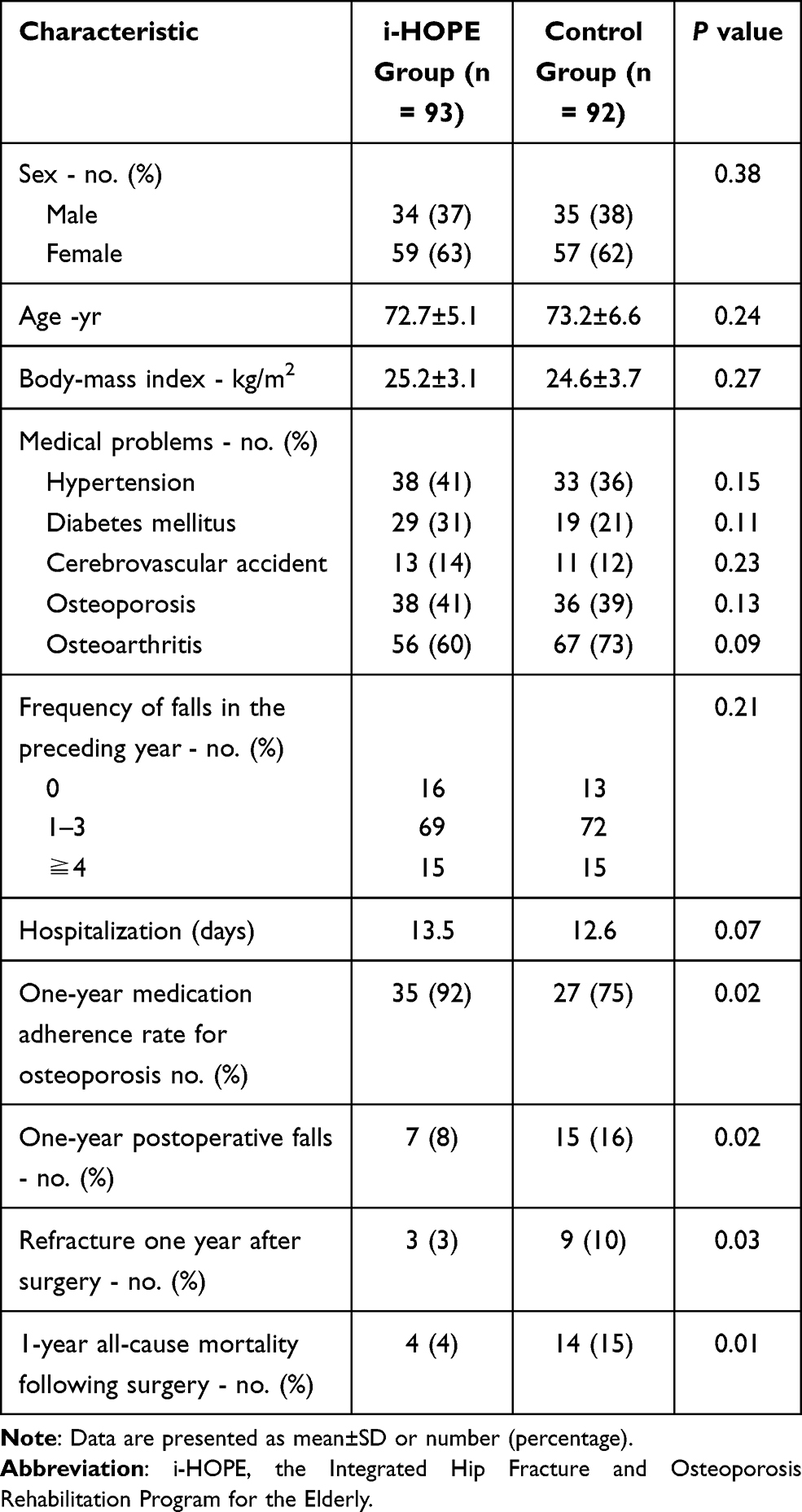 |
Table 1 Characteristics and Outcomes of Individuals Receiving Multidisciplinary Care (I-HOPE) versus the Control Group |
The average age and standard deviation (SD) of patients were 72.9 (6.1) years. Individuals in the i-HOPE program began one month of rehabilitation after the surgery and then continued to actively adjust for a total of six months of rehabilitation over the next five months. When compared to 1-month after surgery, patients who received the following 5-month integrative care services from a multidisciplinary medical team improved significantly in GDS (0.7±1.0 versus 0.9±1.3), ADL (66.6±27.9 versus 42.3±27.8), instrumental ADL (2.2±2.4 versus 1.2±1.6), physical activity (EMS, 12.8±6.0 versus 8.1±4.7), gait, and balance abilities (POMA, 19.1±9.0 versus 10.6±7.2) (Table 2). The incidence of repeated falls, recurrent fractures, and one-year mortality rate were 8%, 3%, and 4%, respectively, substantially lower than the control group receiving traditional treatment (Table 1).
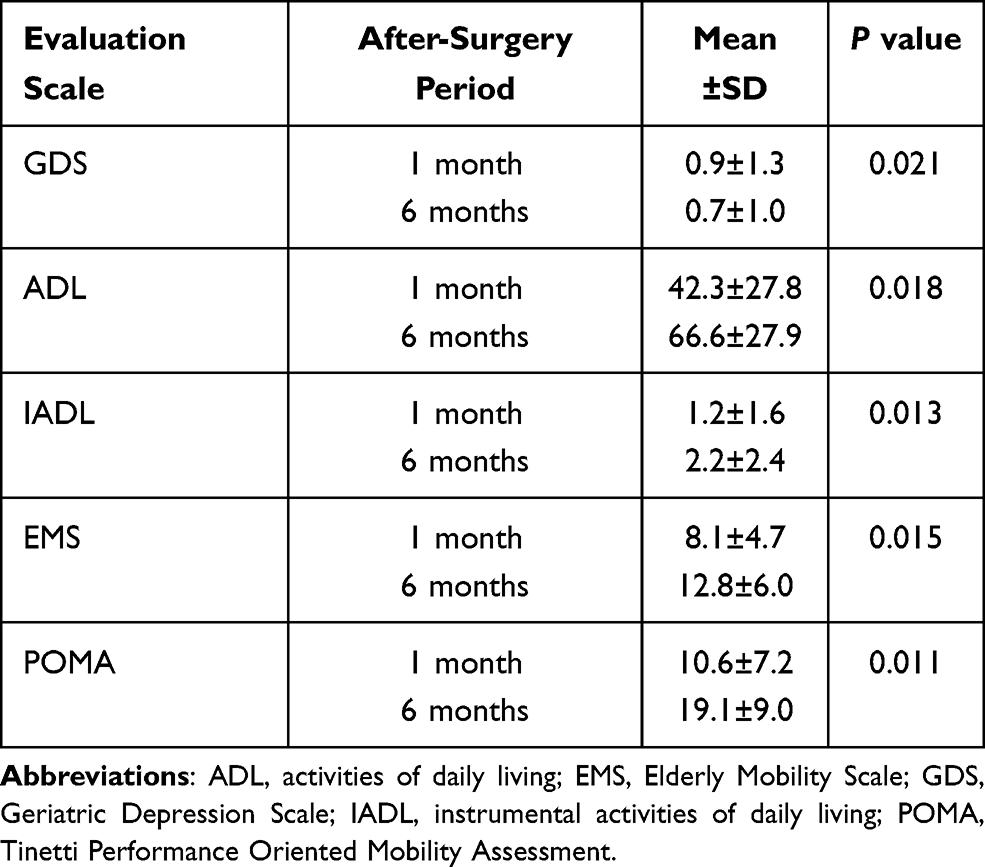 |
Table 2 Changes in Evaluation Scales for Patients Receiving Multidisciplinary Care Following Hip Surgery |
Discussion
Taiwan has one of the highest rates of hip fractures in the Asia-Pacific region and worldwide.14–16 In Taiwan, the mortality rate for patients with a hip fracture one year after surgery is 14.6% (18% for men and 11.2% for women).17 Patients with osteoporosis who have already had hip fractures are two to four times more likely to fracture than those who have not.18 However, prior research has revealed that only around one-third of individuals with fragility fractures receive a thorough examination.19–21 In Taiwan, only around one-quarter of women with hip fractures have their bone mass evaluated, and fewer than one-third are treated for osteoporosis. Individual management and a multidisciplinary integrated care plan involving an orthopedist, gerontologist, endocrinologist, physical therapist, occupational therapist, nutritionist, respiratory therapist, physician assistant, and nurse case manager improved adherence to osteoporosis therapy, reduced the risk of falls and subsequent fractures, and reduced postoperative mortality (Table 3).
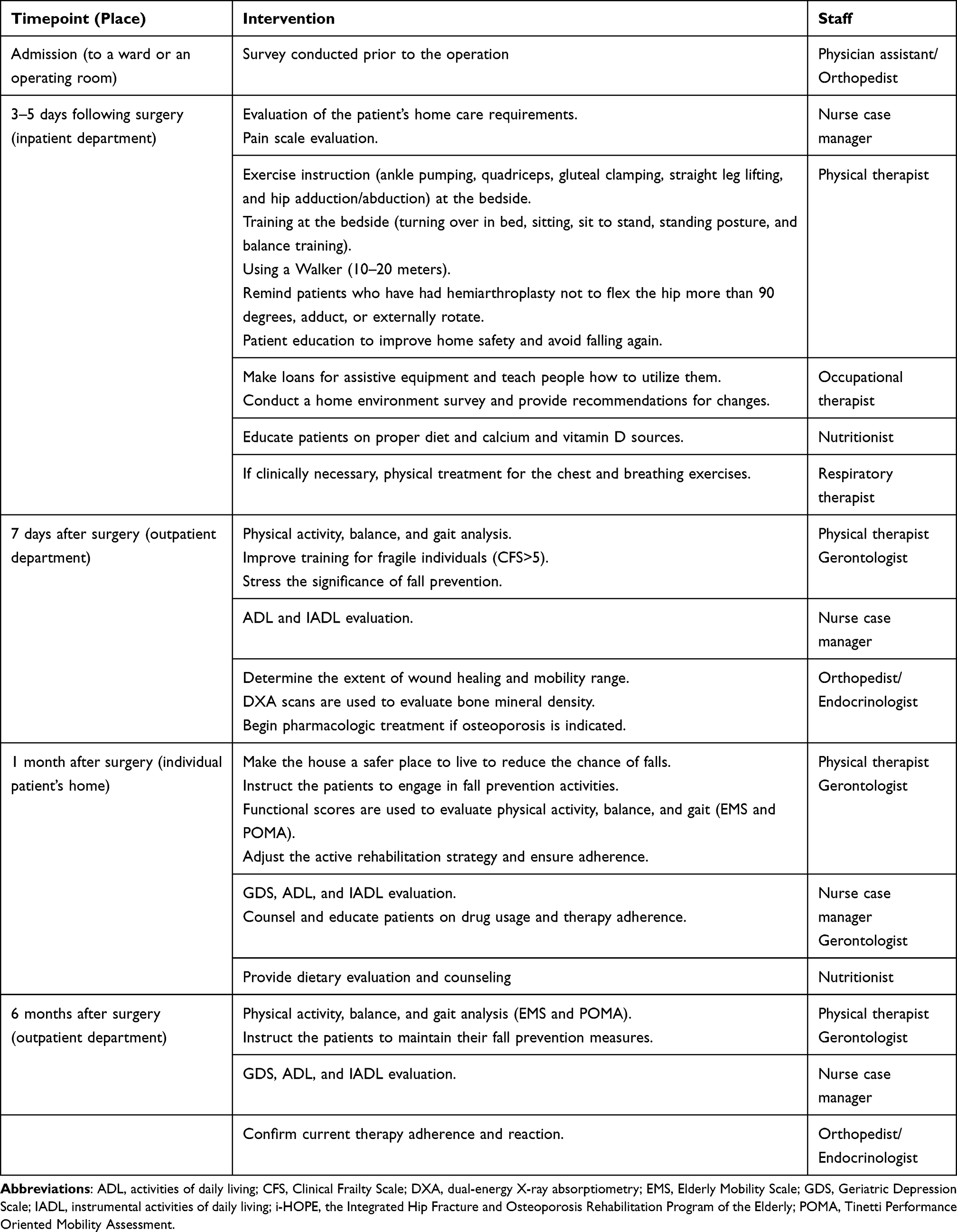 |
Table 3 The I-HOPE Program’s Multidisciplinary Care Profile |
Although educational activities aided in the understanding of patients undergoing hip fracture surgery, the link between education and increased treatment rates was not always clear. Comprehensive treatments, on the other hand, such as these rehabilitation-centered multidisciplinary programs with several experts, were more effective in keeping patients on bone-protecting therapy. As a result, the rates of refracture, falls, and mortality were reduced. Previous research has revealed that 50% of individuals who have hip fracture surgery do not fully restore their pre-operation function.18 In addition to in-hospital acute rehabilitation, many patients require a post-acute care plan that includes continuous active therapy, not only to improve their mobility rapidly but also to successfully regain their functionality.22,23 This is the primary reason why a rehabilitation-based strategy was chosen as the foundation of a multidisciplinary care program to enhance patients’ functional activities following surgery. This study relied heavily on physical and occupational therapists. Physical therapists were in charge of patients’ daily exercise training, while occupational therapists assessed home settings to ensure patients could move safely. During their hospitalization, patients received physical and occupational therapy, which included gait retraining, quadriceps strength training, weight loading exercises, and electrical stimulation of the quadriceps nerves and muscles. The post-surgery rehabilitation regimen includes aerobic and progressive resistance training, muscular strength development, and home rehabilitation.
Furthermore, this rehabilitation-centered cohesive approach would aid in the reduction of care fragmentation. We believe that having a specialized coordinator (nurse case manager) is critical to improving patient identification and supervision (Table 3). A nurse case manager coordinated the home visit intervention following surgery in this supervised program, bringing in additional specialists such as a physical therapist and a nutritionist to provide a complete assessment at home. As predicted, the home visit can assist participants in avoiding additional falls and achieving daily life independence. A handle and a non-slip floor, for example, would be advised to prevent falls in a restroom. A nutritionist might also develop a customized strategy for the elderly to enhance their nutritional condition and avoid postoperative muscle loss. Previous studies discovered that patients with a hip fracture who got structured holistic treatment rather than merely traditional care had a significant reduction in in-hospital mortality, severe comorbidities, and inpatient stay.24–26 Similarly, other studies discovered that the fast-track treatment program, which included preoperative health education, early postoperative feeding, and pain relief methods, as well as oxygen therapy, resulted in a significant reduction in postoperative complications (such as pneumonia, delirium, and urinary tract infections) and mortality rate.27–30
A previous study discovered that the 1-year death rate of patients treated in an elderly hip fracture program is about 21.2%.28 Even while traditional fracture liaison services have the potential to minimize disease burden and associated expenses, there are still logistical problems connected with acquiring sufficient people and material resources. Non-compliance with the care program, for example, or non-adherence to osteoporosis medication, is challenging. Instead, this study’s multidisciplinary care program has been shown to effectively increase medication and rehabilitation adherence in patients with fragility hip fractures. Remarkably, the rehabilitation-based multidisciplinary care model’s considerable improvement in fall rates may have contributed to the significant reduction in refracture rate and mortality rate of participants in the i-HOPE group. To our knowledge, the i-HOPE multidisciplinary care plan is the most successful strategy in Taiwan for reducing refractures and postoperative mortality in patients with fragility hip fractures.
Conclusion
We demonstrated that a multidisciplinary approach with supervised osteoporosis therapy and rehabilitation-based services can improve daily function, lower the risk of recurrent falls and fractures, and significantly reduce postoperative mortality in older patients with a fragility hip fracture.
Acknowledgments
The authors would like to thank Ta-Feng Ho, Cheng-Yu Chang, Tso-Yen Mao, De-Yen Liu, Su-Shun Lo, and Kuan-Hung Lin for their assistance with administrative chores. This study received no particular support from governmental, commercial, or not-for-profit funding organizations.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Harvey NC, McCloskey EV, Mitchell PJ, et al. Mind the (treatment) gap: a global perspective on current and future strategies for prevention of fragility fractures. Osteoporos Int. 2017;28:1507–1529. doi:10.1007/s00198-016-3894-y
2. Curtis EM, van der Velde R, Moon RJ, et al. Epidemiology of fractures in the United Kingdom 1988–2012: variation with age, sex, geography, ethnicity and socioeconomic status. Bone. 2016;87:19–26. doi:10.1016/j.bone.2016.03.006
3. Center JR, Bliuc D, Nguyen TV, Eisman JA. Risk of subsequent fracture after low-trauma fracture in men and women. JAMA. 2007;297(4):387–394. doi:10.1001/jama.297.4.387
4. Hsiao PC, Chen TJ, Li CY, et al. Risk factors and incidence of repeat osteoporotic fractures among the elderly in Taiwan: a population-based cohort study. Medicine. 2015;94(7):e532. doi:10.1097/MD.0000000000000532
5. LeBlanc KE, Muncie HL
6. Yoo JI, Lee YK, Koo KH, Park YJ, Ha YC. Concerns for older adult patients with acute hip fracture. Yonsei Med J. 2018;59:1240–1244. doi:10.3349/ymj.2018.59.10.1240
7. Oliveira A, Vaz C. The role of sarcopenia in the risk of osteoporotic hip fracture. Clin Rheumatol. 2015;34:1673–1680. doi:10.1007/s10067-015-2943-9
8. Shen SH, Huang KC, Tsai YH, et al. Risk analysis for second hip fracture in patients after hip fracture surgery: a nationwide population-based study. J Am Med Dir Assoc. 2014;15:725–731. doi:10.1016/j.jamda.2014.05.010
9. Eekman DA, van Helden SH, Huisman AM, et al. Optimizing fracture prevention: the fracture liaison service, an observational study. Osteoporos Int. 2014;25:701–709. doi:10.1007/s00198-013-2481-8
10. Diem SJ, Harrison SL, Haney E, et al. Depressive symptoms and rates of bone loss at the hip in older men. Osteoporos Int. 2013;24(1):111–119. doi:10.1007/s00198-012-1975-0
11. Perna S, Francis MD, Bologna C, et al. Performance of Edmonton Frail Scale on frailty assessment: its association with multi-dimensional geriatric conditions assessed with specific screening tools. BMC Geriatr. 2017;17(1):2. doi:10.1186/s12877-016-0382-3
12. Smith R. Validation and reliability of the Elderly Mobility Scale. Physiotherapy. 1994;80:744–747. doi:10.1016/S0031-9406(10)60612-8
13. Babiuch AS, Oestervemb K, Lipińska A, et al. Differences in the level of physical fitness and mobility among older women with osteoporosis and healthy women-cross-sectional study. Sci Rep. 2021;11(1):14179. doi:10.1038/s41598-021-93483-3
14. Fernandez MA, Griffin XL, Costa ML. Management of hip fracture. Br Med Bull. 2015;115:165–172. doi:10.1093/bmb/ldv036
15. Kung AW, Fan T, Xu L, Xia WB, Park IH, Kim HS. Factors influencing diagnosis and treatment of osteoporosis after a fragility fracture among postmenopausal women in Asian countries: a retrospective study. BMC Women’s Health. 2013;13:7. doi:10.1186/1472-6874-13-7
16. Kanis JA, Oden A, McCloskey EV, Johansson H, Wahl DA, Cooper C. A systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporos Int. 2012;23:2239–2256. doi:10.1007/s00198-012-1964-3
17. Lin ZZ, Wang JJ, Chung CR. Epidemiology and mortality of hip fracture among patients on dialysis: Taiwan National Cohort Study. Bone. 2014;64:235–239. doi:10.1016/j.bone.2014.04.017
18. Carpintero P, Caeiro JR, Carpintero R, Morales A, Silva S, Mesa M. Complications of hip fractures: a review. World J Orthop. 2014;5:402–411. doi:10.5312/wjo.v5.i4.402
19. Lin YC, Pan WH. Bone mineral density in adults in Taiwan: results of the Nutrition and Health Survey in Taiwan 2005–2008 (NAHSIT 2005–2008). Asia Pac J Clin Nutr. 2011;20:283–291.
20. Barcenilla-Wong AL, Chen JS, March LM. Concern and risk perception of osteoporosis and fracture among post-menopausal Australian women: results from the Global Longitudinal Study of Osteoporosis in Women (GLOW) cohort. Arch Osteoporos. 2013;8:155. doi:10.1007/s11657-013-0155-y
21. Giangregorio L, Thabane L, Cranney A, et al. Osteoporosis knowledge among individuals with recent fragility fracture. Orthop Nurs. 2010;29:99–107. doi:10.1097/NOR.0b013e3181d2436c
22. Gimigliano F, Iolascon G, Riccio I, et al. Post-surgical rehabilitative approach to fragility fractures. Aging Clin Exp Res. 2013;25(Suppl 1):S23–25. doi:10.1007/s40520-013-0094-x
23. Peeters CM, Visser E, Van de Ree CL, Gosens T, Den Oudsten BL, De Vries J. Quality of life after hip fracture in the elderly: a systematic literature review. Injury. 2016;47:1369–1382. doi:10.1016/j.injury.2016.04.018
24. Vidan MT, Sanchez E, Gracia Y, Maranon E, Vaquero J, Serra JA. Causes and effects of surgical delay in patients with hip fracture: a cohort study. Ann Intern Med. 2011;155:226–233. doi:10.7326/0003-4819-155-4-201108160-00006
25. Boddaert J, Cohen-Bittan J, Khiami F. Postoperative admission to a dedicated geriatric unit decreases mortality in elderly patients with hip fracture. PLoS One. 2014;9:e83795. doi:10.1371/journal.pone.0083795
26. Asplin G, Carlsson G, Zidén L, Kjellby-Wendt G. Early coordinated rehabilitation in acute phase after hip fracture - a model for increased patient participation. BMC Geriatr. 2017;17:240. doi:10.1186/s12877-017-0640-z
27. Binder EF, Brown M, Sinacore DR, Steger-May K, Yarasheski KE, Schechtman KB. Effects of extended outpatient rehabilitation after hip fracture: a randomized controlled trial. JAMA. 2004;292:837–846. doi:10.1001/jama.292.7.837
28. Schnell S, Friedman SM, Mendelson DA, Bingham KW, Kates SL. The 1-year mortality of patients treated in a hip fracture program for elders. Geriatr Orthop Surg Rehabil. 2010;1(1):6–14. doi:10.1177/2151458510378105
29. Latham NK, Harris BA, Bean JF, et al. Effect of a home-based exercise program on functional recovery following rehabilitation after hip fracture: a randomized clinical trial. JAMA. 2014;311:700–708. doi:10.1001/jama.2014.469
30. Pedersen SJ, Borgbjerg FM, Schousboe B. A comprehensive hip fracture program reduces complication rates and mortality. J Am Geriatr Soc. 2008;56:1831–1838. doi:10.1111/j.1532-5415.2008.01945.x
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.