Back to Journals » ClinicoEconomics and Outcomes Research » Volume 14
A Real-World Data Study on the Healthcare Resource Use for Uncontrolled Moderate-to-Severe Atopic Dermatitis in Secondary Care in the United Kingdom Prior to the Introduction of Biologic Treatment
Authors Hudson RDA, Ameen M, George SMC, Harwood CA, Weller RB, Lear JT, Rout R, Surendranathan T, Petrovic M, Bewley AP ![]()
Received 15 September 2021
Accepted for publication 19 January 2022
Published 4 April 2022 Volume 2022:14 Pages 167—177
DOI https://doi.org/10.2147/CEOR.S333847
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Giorgio Colombo
Richard DA Hudson,1 Mahreen Ameen,2 Susannah MC George,3 Catherine A Harwood,4,5 Richard B Weller,6,7 John T Lear,8,9 Rajesh Rout,1 Thishi Surendranathan,1 Milos Petrovic,1 Anthony P Bewley4
1Sanofi, Berkshire, UK; 2Royal Free NHS Foundation Trust, London, UK; 3University Hospitals Sussex NHS Foundation Trust, Brighton, UK; 4Barts Health NHS Trust, London, UK; 5QMUL, London, UK; 6NHS Lothian, Edinburgh, UK; 7University of Edinburgh, Edinburgh, UK; 8Salford Royal NHS Foundation Trust, Salford, UK; 9Manchester Academic Health Science Centre, Manchester University, Manchester, UK
Correspondence: Richard DA Hudson, Sanofi, 410 Thames Valley Park Drive, Reading, Berkshire, RG6 1PT, UK, Email [email protected]
Background: Whilst there is international evidence around the high healthcare resource utilization (HRU) associated with atopic dermatitis (AD), there is a lack of published data from the United Kingdom (UK).
Methods: A retrospective, descriptive, observational study was conducted to evaluate the burden of moderate-to-severe AD on the National Health Service (NHS) in an adult UK population treated with traditional standard of care prior to the introduction of biologics. Patients (n=59) were recruited from 6 UK NHS Hospital Trusts and observed over three years.
Results: 707 dermatology clinic visits were recorded over the observation period, amounting to 6.6 visits per patient-year, most commonly for routine check-ups most of which involved dermatology consultants (n=469, 66%). Physicians were the most consulted healthcare professional (n=652, 92%); emollients were the most common treatment (n=80 courses). 174 flares requiring additional medical advice were recorded in total (1.6 per patient-year).
Discussion/Conclusions: Complex treatment pathways for adult patients in the UK with moderate-to-severe AD incur considerable HRU, particularly for those patients non-responsive to systemic therapies with broad immunosuppressant action. Recent advances in biologics-based AD management could possibly have a significant positive impact on HRU through significant reduction in the number of NHS touch points identified in this study.
Keywords: atopic dermatitis, healthcare resource use, observational study
Introduction
Atopic dermatitis (AD) is a chronic and relapsing inflammatory skin disease. Patients with moderate-to-severe AD can develop skin lesions which can encompass a large body surface area and are frequently accompanied by intense pruritus, which leads to sleep deprivation, symptoms of anxiety or depression and a poor quality of life.1 Onset often occurs prior to 6 months of age; 60% of patients develop symptoms before their first birthday2–4 and these may extend into adulthood in up to 80% of cases.5 However, it is also possible for AD to begin in adulthood. Nettis et al, 2020, found key differences in symptoms between child-onset and adult-onset AD patients. The lichenified/exudative flexural dermatitis pattern (often associated with the head, neck or hands) was more common in child-onset patients, whereas the prurigo nodularis pattern was more common in adult-onset patients.6
The overall prevalence of AD in adults varies between 1 and 10%, although AD is estimated to affect 4.4% of adults in the European Union (EU) with 3.5% of those undergoing treatment.7 The chronic nature of the disease means that long-term treatment is often necessary. The typical treatments for AD during the data collection period of this study were emollients and topical corticosteroids.8 However, in recent years, numerous novel therapies have been developed. These include small molecules (eg phosphodiesterase 4 inhibitors and JAK inhibitors), as well as specific monoclonal antibodies like dupilumab and tralokinumab.9
A number of country-specific studies have found a link between the severity of a patient’s AD and their health resource utilization (HRU). For example, an Israeli study,10 reported that patients with AD visited community family practitioner clinics 25% more than the control group and were 12% more likely to be hospitalized (both p<0.0001). Additionally, a Spanish study,11 found that severe AD patients had a significantly higher (p<0.001) mean annual healthcare cost of €2340, versus moderate AD patients (€1572) and mild AD patients (€689). Similar results have also been published in the United States.12
Other studies have also noted that the increased burden on healthcare was not solely related to the treatment costs of AD. Patients with AD had a greater probability of having comorbidities, the treatment of which also place strain on health-care systems. A significant difference in the prevalence of Type 2 immune conditions like allergic rhinitis, conjunctivitis, and urticaria, as well as viral infections, has been reported between AD and matched populations.13 Additionally, AD has been shown to increase risk for cardiovascular disease14 and to negatively impact on AD patients’ quality of life, particularly for those with moderate-to-severe AD.15
While there is strong international evidence around the increased burden on healthcare systems from the HRU associated with AD, there is a lack of research that has been conducted in the United Kingdom (UK). Recent advances in the management of AD16 have significant potential to alleviate burden on the healthcare system and so it is important to establish a baseline with which the HRU benefit of these treatments may be compared. The aim of this study, therefore, was to evaluate the burden of moderate-to-severe AD on the National Health Service (NHS) in patient who are representative of the adult UK population, treated with traditional standard of care before the introduction of biologic therapy.
Patients and Methods
Design
A retrospective, descriptive and observational study was conducted across six secondary and tertiary UK NHS Hospital Trusts (London n=3, Brighton n=1, Edinburgh n=1 Sheffield n=1). These centers provide care to adults with moderate-to-severe AD and were either identified by the study sponsor as centers with an interest in research, or through approach by the National Institute for Health Research (NIHR) Clinical Research Network (CRN) study feasibility service. Due to the observational nature of the study, and the fact no a priori hypothesis was being tested, no formal power calculation was required to determine sample size. The sample size was chosen pragmatically based on estimates of reliability (95% confidence limits) for a mean number of outpatient visits ranging from two to six. A sample size of 60–80 patients was considered sufficient to provide a representative sample of adult patients with moderate-to-severe AD and adequate reliability for quantitative endpoints, whilst recognizing that any rates or proportions would have more limited reliability. Patients who met the eligibility criteria were selected consecutively based on their most recent clinic visit. The study was a real-world observation study, so patients were selected consecutively to reduce the possibility of selection bias. These patients were approached for consent until a maximum of 15 patients per center had been enrolled, or the overall sample required had been reached. All enrolled patients were informed about the purpose of the study.
The observation period was the three years prior to data collection (data collection occurred from August 2017 to December 2017). The data were retrospective, anonymized patient-level data, and were collected by an external researcher, or clinical staff, from electronic and paper-based hospital medical records from the six NHS centers. Only protocol-defined, pre-existing data that were explicitly available from the patient records were recorded. All patients included were known to have a diagnosis of AD, as defined by the Hanifin and Rajka criteria.17 The primary endpoint for the study was health resource utilization (HRU), including metrics, including the duration of hospital admissions (eg for administration of treatment or infection), the interventions and treatment courses, and the healthcare professionals seen during secondary care visits. Secondary endpoints included patient demographics and clinical characteristics, the treatment pathways that they took, and the number and severity of flare episodes (that required medical intervention). A treatment was defined as “a treatment, or combination of treatments, prescribed to a patient on the same date”. A course was defined as “a period of continuous use of a single medicinal product”.
Since data were collected from the date of the patient’s first secondary care dermatology clinic visit (within the three-year observation period), some patients lacked a full three years of data. Patients could enter the study in any of Year 1, Year 2 or Year 3. The eligibility criteria for those patients included in the study is detailed in Table 1. The study targeted male and female patients who were aged at least 21 years and had been referred into secondary or tertiary care at least 12 months prior to enrollment in the study. Patients were eligible to enter the study if they had been diagnosed with moderate-to-severe AD at least 24 months before enrollment and were considered by their healthcare professional to suffer from uncontrolled moderate-to-severe AD on the basis of a previous history of systemic treatment (or intolerance/contraindication to it) which in itself stands as a proxy for severity.
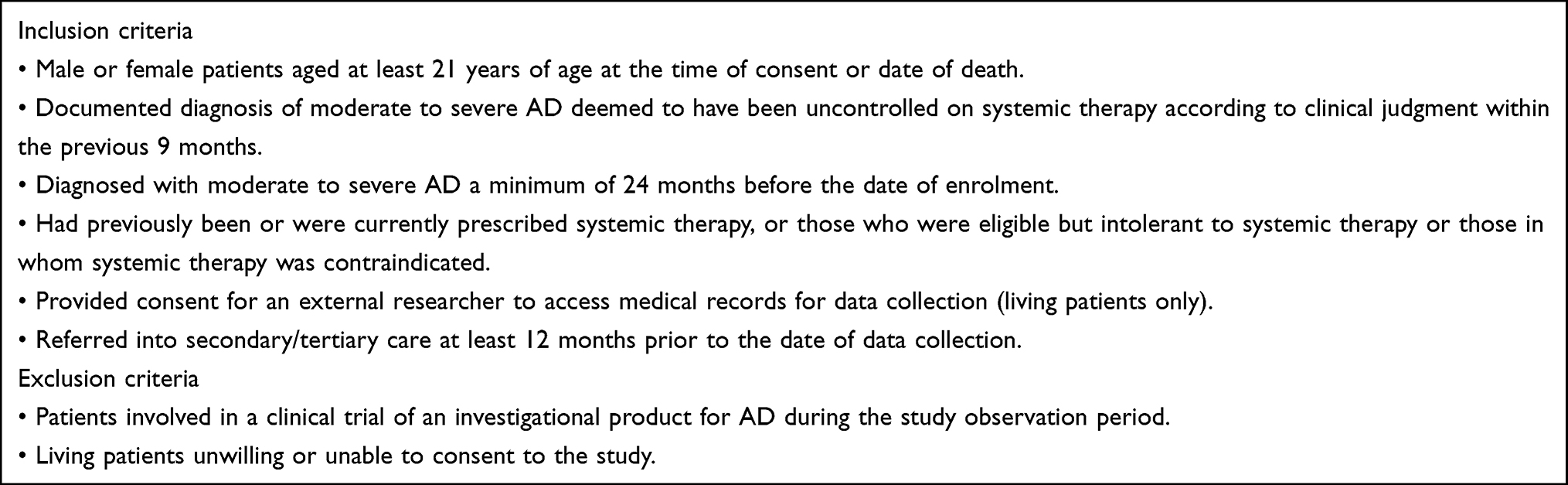 |
Table 1 Eligibility Criteria |
Analysis
If data were missing from medical records, only the available data were used in the analyses with no imputation of missing values except for data on dates. In the case of a missing day, the 15th day of the month was assumed, and in the case of a missing day and month, the 1st of July was assumed. Source data verification (SDV) was conducted by study researchers at each center once a minimum of 50% of data had been collected at that center, and on a 10% random sample of the entire data set to ensure that the data were accurate and of good quality.
Patients were entered into Year 1, Year 2 or Year 3 data depending on the time of their first clinic visit during the observation period, and the summary statistics were calculated on those 12-month periods irrespective of when an individual patient entered the year (ie a patient who visited a clinic for the first time six months into Year 2 had data recorded for Year 2 and Year 3).
Data were analyzed using Stata v14 (StataCorp LLC). Descriptive statistics detailing the socio-demographic characteristics of the sample were generated. The primary endpoint data were presented with descriptive statistics for each variable. These statistics included measures of central tendency like the mean and median, along with the dispersions associated with them like standard deviation and range. These measures were calculated per patient, per year. Where appropriate, 95% confidence intervals were also presented. No sensitivity analyses were conducted on the data.
Results
Sample Characteristics
A total of 97 patients were identified as eligible for the study of whom 66 consented to participate (Table 2). However, 6 patients were subsequently identified as not being eligible to participate. Therefore, a total of 60 patients were included in the sample. 48 of the patients had their first clinic visit in (and so were followed from) Year 1, 11 patients in Year 2 (ie, 59 for Year 2 overall), and 1 in Year 3. The final analysis excluded 1 patient whose first visit was after the start of Year 3, leaving the final number of patients to be 59. Year 1 data were censored for all patients due to incomplete data. Any patients with Year 2 data that were incomplete were also censored for that year. In total, 107 patient years were included in the analysis (Table 2).
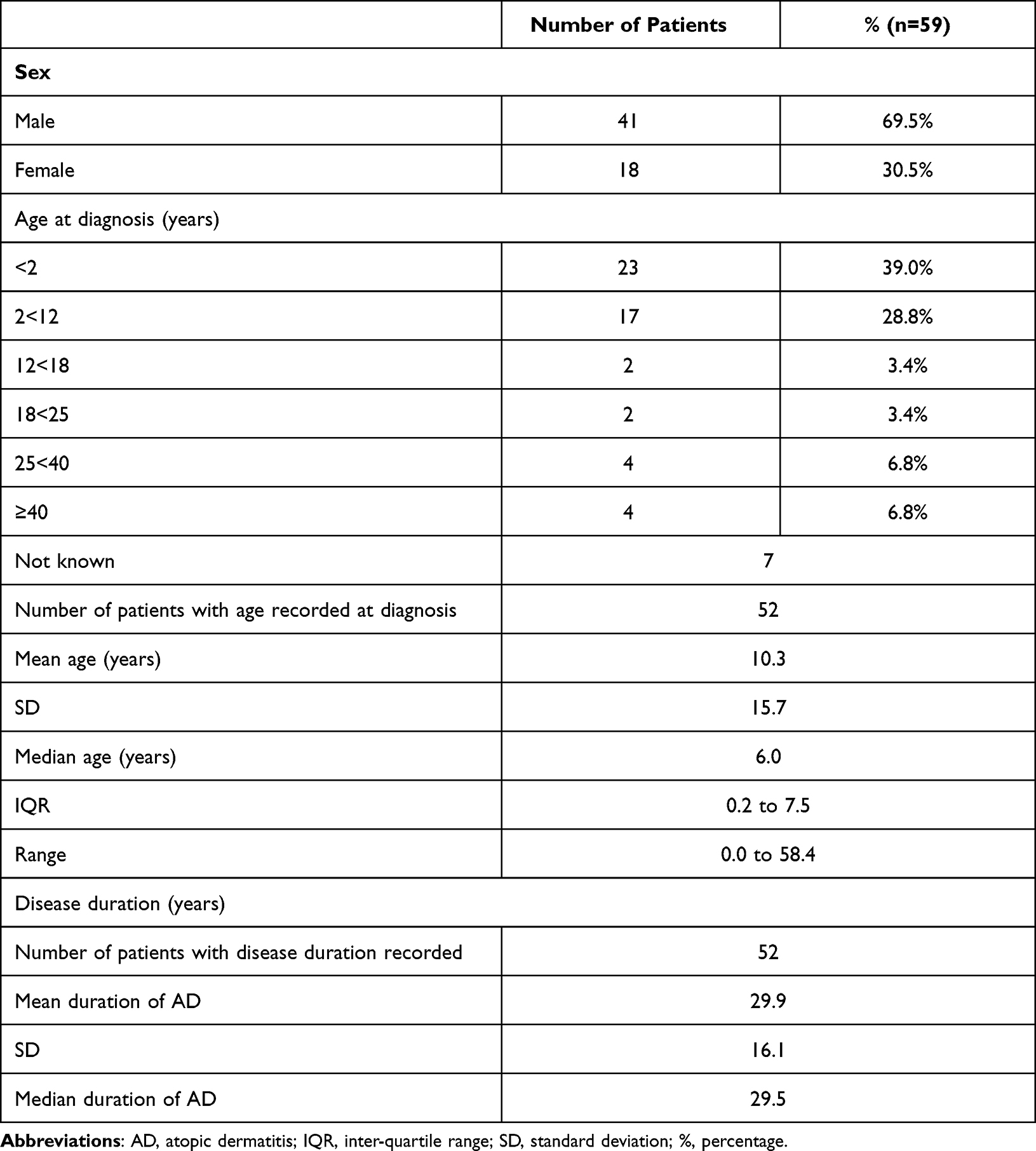 |
Table 2 Sample Characteristics |
The sample was 70% male (n=41) with a mean age of first AD diagnosis of 10.3 years (SD 15.7). Patients had a mean of 1.4 (SD 1.1) comorbidities and 81% of patients (n=48) had at least one comorbidity. Asthma was the most common comorbidity at 61% (n=36) and other comorbidities included seasonal allergies (29%, n=17), food allergies (24%, n=14) and depression (7%, n=4).
The most common, known triggers for AD were infection (25%, n=15), temperature changes (20%, n=12) and stress-emotion (19%, n=11), though “not known” was also recorded for 86% of patients (n=51). Patients were not limited to one single trigger.
Assessments of disease severity/health-related quality of life (HRQoL) recorded at initiation of each category of systemic treatment are summarized in Table 3. Numerous instruments, including the Eczema Area and Severity Index (EASI) and the Dermatology Life Quality Index (DLQI), were used to measure severity. The mean DLQI scores at initiation of each category of systemic treatment ranged between 11.9 and 19.8 points, indicative of moderate-to-severe impact of AD on patients’ lives. The mean EASI scores at initiation of each category of systemic treatment ranged between 12.3 and 33.2 points, indicative of moderate-to-severe AD.18
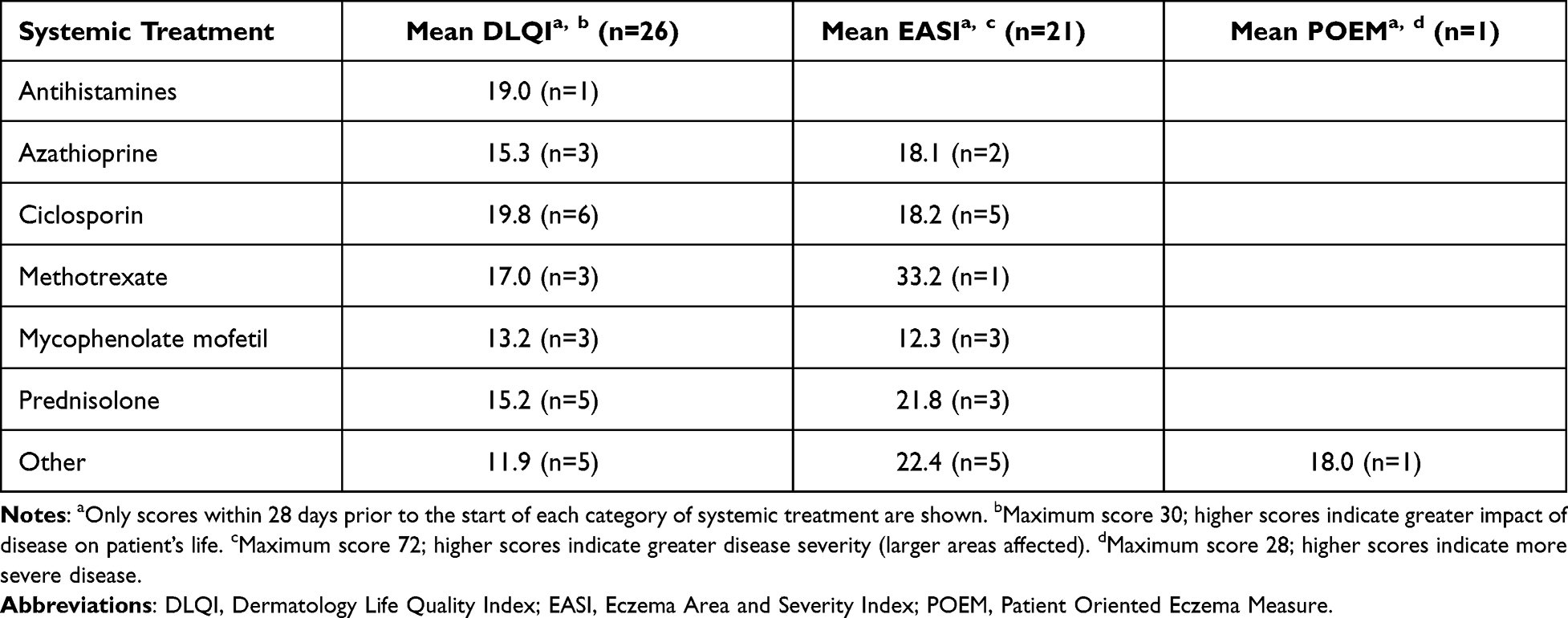 |
Table 3 Distribution of Disease Severity and Health-Related Quality of Life in Patients at Initiation of Each Category of Systemic Treatment |
Employment status was recorded for 32 (53%) patients of the 60-patient sample. 23 patients were recorded as in full time employment, 6 were recorded as unemployed and 3 were recorded as in part time employment. Education status was recorded for 29 (48%) patients of the 60-patient sample. 22 patients were recorded as not in education, 6 were recorded as full-time students and 1 was recorded as a part time student.
Main Results
Resource Use
A total of 707 dermatology clinic visits (including telephone consultations) were recorded during the two-year observation period. This amounted to 6.6 visits per patient-year. The most common reason for a visit to a clinic was a routine check-up, with 66% (n=469) visits being recorded as such. Telephone clinics at 11% (N=81) and telephone clinic patients who did not attend (DNA) at 7% (n=46) were the next most common reasons. At dermatology clinics, physicians were by far the most commonly seen healthcare professional (HCP) by AD patients at 92% (n=652) followed by nurses at 8% (n=59) of visits. Psychologists (n=7) and dieticians (n=2) were both occasionally visited (Table 4).
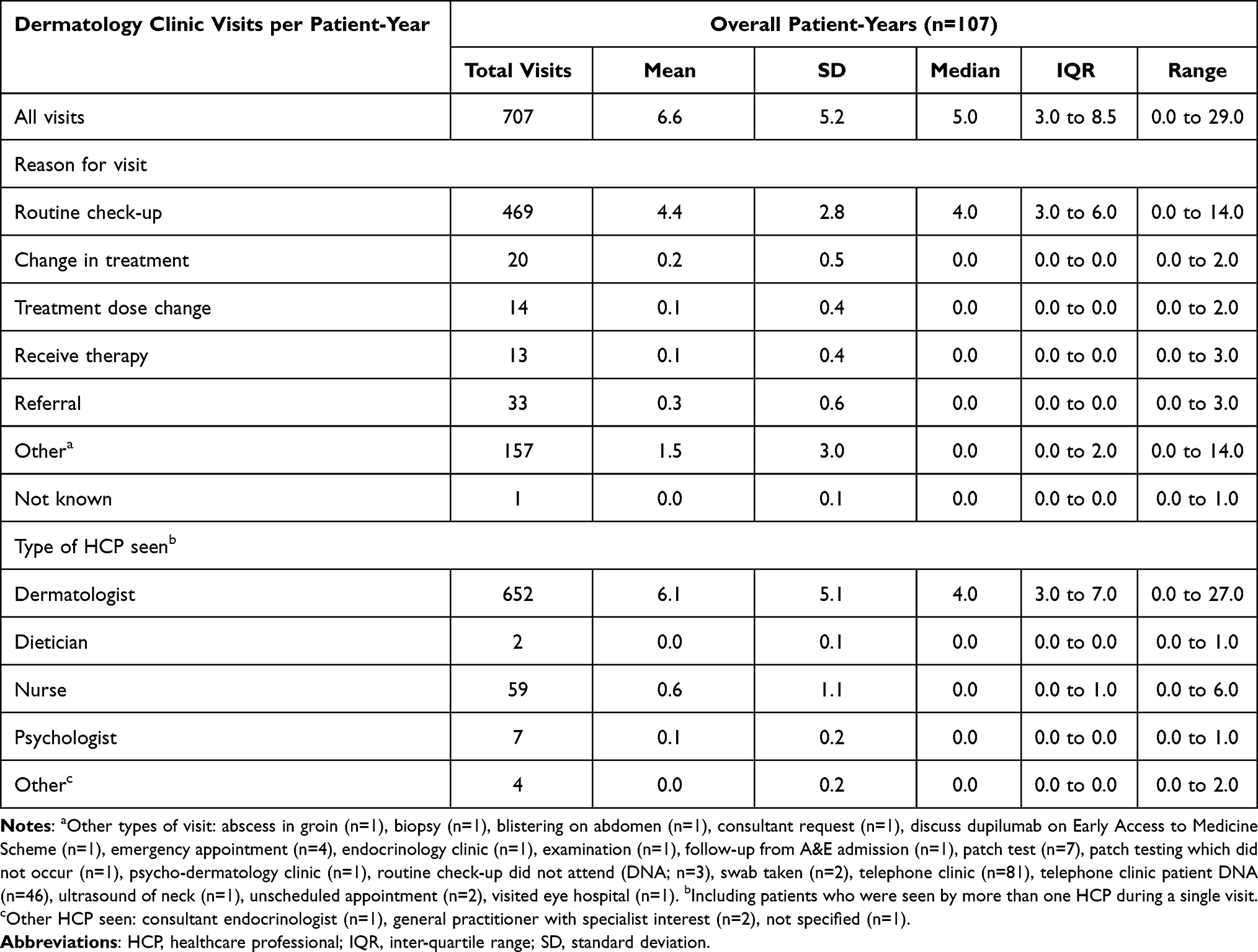 |
Table 4 Number of and Reason for Dermatology Clinic Visits and Type of Healthcare Professional Seen, per Patient-Year |
Over the observation period there were a total of 23 AD-related day case visits recorded across 9 patients, with the most common reason for this being administration of treatment (70%, n=16). Only 10 AD-related A&E attendances were recorded in total, across 8 patients. Four of these visits were due to AD flares (40%) and one due to infection (10%). 13 AD-related inpatient admissions were recorded across 6 patients, for administration of treatment (46%, n=6), infection (31%, n=4) and AD flares (23%, n=3). The mean length of stay for these admissions was 2 days per episode (SD 0.0) for administration of treatment, 11 days per episode (SD 8.3) for infection and 3.3 days per episode (SD 3.2) for AD flares (Table 5).
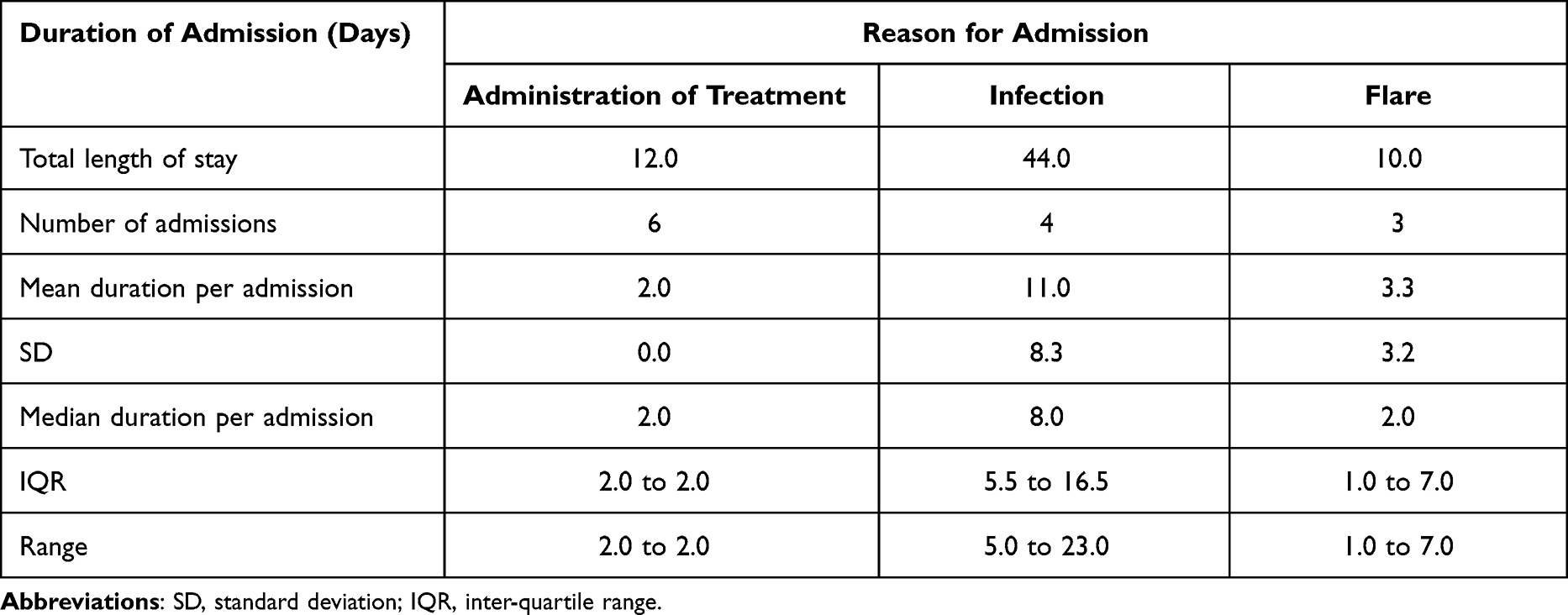 |
Table 5 Length of Stay for Hospital Admissions, by Reason for Admission |
There were 90 investigations recorded during the observation period, 17 (19%) of them were patch tests, 10 (21%) were immunoglobulin E (IgE) levels and 10 (21%) were skin biopsies (Table 6).
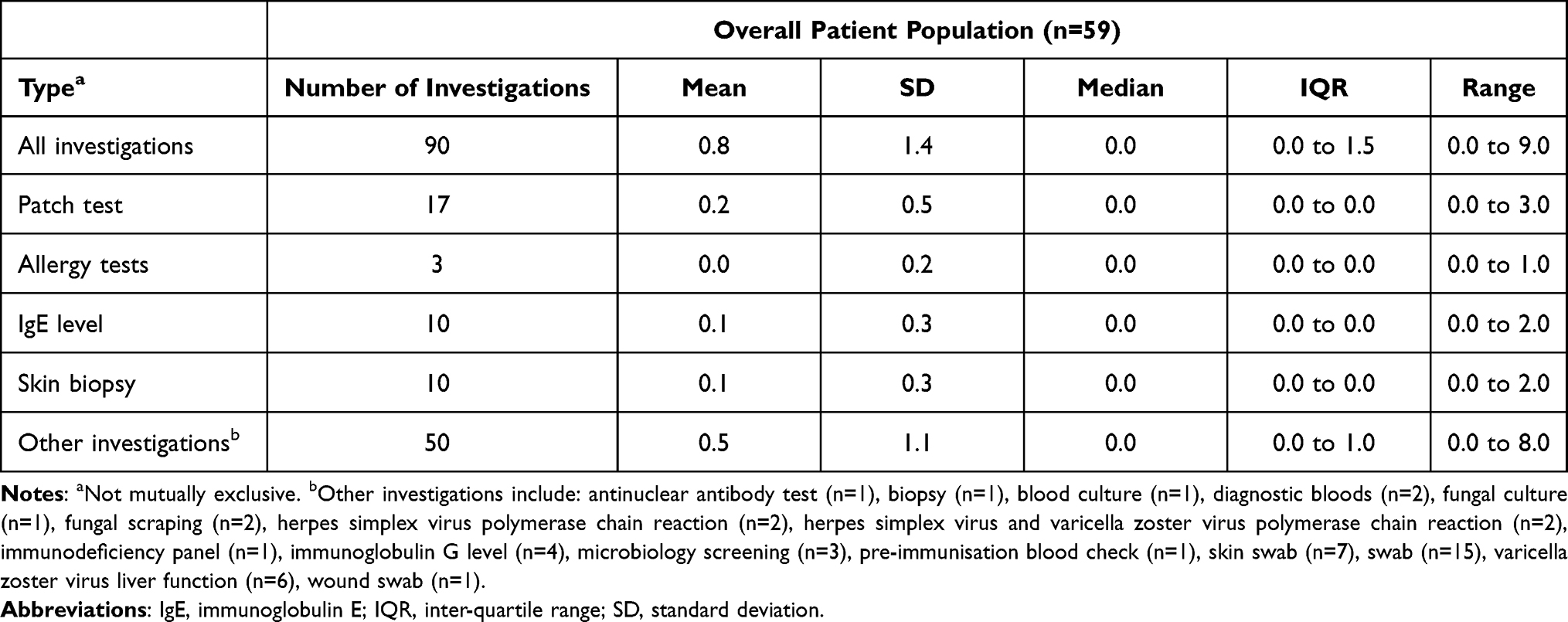 |
Table 6 Number and Type of Investigations per Patient, Years 2–3 |
AD Treatment Pathway
Non-systemic therapies (eg, topical therapies and phototherapy) were the most common treatment during the observation period and were used in 224 treatments during the two years, with a per patient range of 0 to 12 treatments. The most commonly used treatment out of these were emollients, used 80 times (36% of non-systemic treatments), followed by high potency topical corticosteroids and low potency topical corticosteroids, used in 66 (29%) and 37 (17%) treatments respectively.
For systemic therapies, a total of 159 courses were recorded (a course is defined as a period of continuous use of a single medicinal product). The most common of these systemic therapies prescribed was prednisolone, which was used in 45 treatments (courses per patient year) (28% of systemic therapies). Ciclosporin, azathioprine and methotrexate were also commonly used systemic therapies, used in 25 (16%), 18 (11%) and 17 (11%) treatments, respectively. The per patient range was 0 to 8 for systemic therapy treatments, meaning that at least one patient received 8 treatments during their observation period.
There were 6 courses of phototherapy used over the observation period, with narrow band UVB (TL01) used in 5 (83%) of those instances.
Concomitant medications were prescribed in 53 treatments across 37 patients. Vitamins and minerals were used 22 times (42% of concomitant medications) and antihistamines were used 10 times (19%).
58 patients (out of 59) received a new treatment combination (a combination is classified as any treatments initiated from the same date for any given patient) from Year 2 onwards. One patient was initiated on a new combination during Year 1, and so did not start one during Year 2 or 3.
Details of each patient’s sequence of documented treatment combinations (prescription rounds) were recorded. 24 patients were prescribed at least one systemic treatment for their first prescription round and 37 patients were prescribed at least one non-systemic treatment. 5 patients were prescribed at least one concomitant medication. No patients were prescribed phototherapy in their first prescription round, but 3 patients were at their second prescription round.
In general, as prescription rounds went on, the number of patients being prescribed a newly initiated treatment combination reduced; for example, 24 patients were prescribed a total of 26 systemic therapy courses in the first prescription round, but this had reduced to 1 patient with 1 newly initiated systemic therapy course by the tenth prescription round.
Treatment Outcomes
A total of 174 flares (an episode requiring escalation of treatment or seeking additional medical advice)19 were recorded during the patient observation period which is equivalent to 1.6 flares per patient year with a median of 1 flare per patient year. The range was from 0 to 6 flares, indicating that at least one patient had no flares recorded during their observation period. Severity was reported for 52 of the 174 flares (122 flares had an unknown severity). Of these 52, 43 (83%) were severe, 7 (13%) mild and 2 (4%) moderate.
Ciclosporin Combination Therapy
Inclusion criteria stated that patients must have been uncontrolled on systemic therapy according to clinical judgment within the previous 9 months. However due to the paucity of treatments available at the time, at least one course of ciclosporin, an immunosuppressant medication, was recorded to have been given to 21 of the 59 (36%) patients during the two-year observation period. Of these patients, 12 (20%) received ciclosporin in combination with another systemic therapy, and 9 (15%) received ciclosporin as a sole treatment. When used in combination, 8 patients (60%) received ciclosporin in combination with just one other systemic treatment (azathioprine, n=2; methotrexate, n=1; prednisolone, n=1’ other systemic steroid, n=1; other, n=1) while 4 patients (40%) received ciclosporin in combination with two other systemic treatments (methotrexate and mycophenolate mofetil, n=1; azathioprine and prednisolone n=1; prednisolone and other, n=2).
Discussion
The results demonstrate a considerable burden of hospital visits, in particular outpatient visits, in adults with moderate-to-severe AD, with patients attending between 4.4 and 6.8 dermatology clinic visits per year. This amounts to an average of almost 1 visit every 2 months, representing a substantial patient and economic burden. These results are also consistent with results across countries with very different patterns of healthcare provision. A recent real-world study evaluating USA claims data for 10,533 adults with AD, Drucker et al, 2017, reported an additional 6.2 outpatient visits per year in patients with AD compared with age- and sex-matched controls after adjustment for atopic comorbidities.20 The results of the present study are also broadly consistent with the 5.4 hospital visits per year in 380 patients with severe AD and 3.0 hospital visits per year in 2361 patients with moderate AD reported in a Spanish registry study.11 The burden of other hospital visits/admissions in the present study were also broadly consistent with the previous real-world studies, although the number of emergency department visits in the Spanish study was higher than those observed in the present study and the studies from the USA.11,20,21
The wide range of topical and systemic treatments for AD, concomitant medication for AD-related conditions, as well as associated complex treatment patterns observed in this study most likely reflect the difficulty in identifying the most effective and tolerable treatment options for patients with moderate-to-severe AD for long-term use.22–24
Phototherapy was infrequently used in patients included in the present study. This is consistent with available guidance suggesting that phototherapy is more commonly used as first-line therapy after failure of topical therapy and only in the short-term, with systemic therapy more commonly used in patients unresponsive to phototherapy and in those for whom phototherapy is contraindicated.23–26
Prednisolone and ciclosporin were the most commonly used systemic therapies in these patients whilst patients were selected on the basis of failure of systemic therapy according to clinical judgment within the previous 9 months. This may indicate the lack of effective treatments for these patients at the time of data collection. This is consistent with the current recommendations for ciclosporin to be used as the first-line systemic therapy of choice for moderate-to-severe AD by the ETFAD/EADV Eczema Task Force 201522,24 and, and the International Eczema Council/’s consensus statement stating that prednisolone and other systemic corticosteroids should be used only for the short-term treatment of flares or to bridge between different systemic therapies.20,22,24,25 A large number of flares were recorded during the patients’ observation period, despite the complex treatment patterns observed, suggesting a lack of effective treatment options for this group of patients during the study observation period.
Disease severity/HRQoL using EASI, DLQI, EQ-5D or SCORAD questionnaires was infrequently recorded in patients’ medical records, There are a wide variety of different instruments that have been used to assess disease severity/HRQoL in clinical trials and other studies of patients with AD.27 However, some of those tools have poor usability in routine clinical practice because of the time required for completion (eg, the Skindex-29).27,28 This lack of data precluded evaluation of changes in disease severity/HRQoL after changes in treatment and/or dose escalations. However, the limited scores available for EASI and DLQI recorded prior to initiation of different categories of systemic therapy during the patients’ observation period were consistent with expectations for a cohort of patients with moderate-to-severe AD.
This study included 59 adult patients with AD deemed to have been uncontrolled on systemic therapy from six UK centers. Although the majority of centers were located in the South East of England, this is consistent with NICE guidance indicating a regional variation in AD, with the highest rates in the South East and Midlands and lowest rates in Wales and Scotland.29 Therefore, the results of this study can be considered generalizable to the UK population of adult patients with moderate-to-severe AD deemed to have been uncontrolled on systemic therapy.
Furthermore, the similarity in healthcare resource use observed in this study compared with real world studies from the USA and Spain suggest these results will be generalizable to the wider population of adult patients with moderate-to-severe AD deemed to have been uncontrolled on existing systemic therapies with broad immunosuppressant action.
There are a number of potential limitations. As with any retrospective study based on secondary use of data, the interpretation of the results of this study and interpretation of study endpoints depends on the completeness and quality of the source medical records and the reliability of the extraction of data from the medical records. The final number of included patients was one short of the proposed number, which could reduce the viability of the generalizability to the UK population. This limitation is a symptom of the unpredictability in real-world observational studies and was not alleviated by the multi-center nature of the study.
Potentially eligible patients were identified consecutively based on patients attending the most recent clinic visits; it is possible that this may have led to recruitment of patients who attended clinic more often and therefore introduced selection bias that may have led to over-estimation of resource use. The nature of the study objectives and the real-world, observational design meant that identifying patients consecutively proved the most practical solution to reduce selection bias, even if it introduced some bias itself.
Topical treatments in this study were categorized according to the number of different types of topical treatment; this is consistent with recognized difficulties reported in NICE guidance in relation to quantifying patients’ use of topical treatments.29,30 In addition, which HCP has prescribed the topical treatment is unlikely to be recorded if prescribed in primary care, further causing difficulty in the data collection for topical treatments.
Assessments of disease severity/HRQoL were infrequently documented in patients’ medical records; therefore, changes in disease severity/HRQoL after treatment changes and/or dose escalations could not be evaluated.
Summary measures related to resource use in years 1 to 3 were calculated based on 12 months irrespective of the time an individual patient entered the year. Since patients were observed from the first hospital visit until data collection, this is unlikely to influence resource use related to hospital visits as all hospital visits within a year were collected; however, this may have resulted in an underestimation of resource use in relation to treatment and the number of AD flares since data were only collected from the time of the first documented visit within the 3-year study period prior to data collection.
Finally, it should be highlighted that this was study was initiated by a pharmaceutical company. However, ethical issues were mitigated by the fact that the study design was jointly decided upon (ie, was led by the input from the unbiased clinical experts), and that the authors from the study sponsor were not involved in the data selection or analysis. In addition, the interpretation of the data in the paper is the result of joint work of all authors.
Conclusions
The considerable burden of complex treatment pathways including multiple hospital visits reported here for adult patients in the UK with moderate-to-severe AD considered to be unresponsive to broad spectrum systemic therapy prior to the introduction of a biologic treatment is consistent with the limited real-world data available from other countries. Patients were observed to have almost 7 dermatology clinic visits per year. Whilst AD related inpatient admissions were not observed for all patients, those patients with infection related hospital episodes were shown to have a high (n=11) mean number of days per stay. These episodes represent considerable financial and system opportunity costs. It is possible that the recent advances in the management of AD with biologic treatments will have a significant positive impact on the HRU burden that AD places on the system through reduction in the significant number of touch points identified in this study. New therapies may also provide an opportunity to lessen the burden on patients (although disease severity/HRQoL was infrequently formally recorded in patients’ medical records) through, for instance, homecare, less monitoring and self-injection. Indeed, beyond disease related HRQoL impact, the complex and at times unpleasant topical regimens currently prescribed to patients have been shown previously to have a significant impact on HRQoL.31
Ethics Statement
This study was conducted in accordance with the principles laid out by the 18th World Medical Assembly (Helsinki, 1964) and all subsequent amendments.
Acknowledgments
Technical writing support from Adam Smith and Tom Bromilow at York Health Economics Consortium. Study implementation, analysis and reporting by OpenVie. Both were funded by Sanofi.
Funding
This work was supported by Sanofi In accordance with the UK Department of Health Research Governance Framework for Health and Social Care, this study was approved by the NHS Health Research Authority East Midlands–Nottingham 1 Research Ethics Committee (REC reference: 17/EM/0143; protocol DUPILL08674 amendment 1 approval date 26/09/2017). All necessary local Trust approvals were obtained. Eligible patients were all approached for consent before they were included in the study.
Disclosure
Mahreen Ameen has been the principal investigator on clinical trials, consultant or scientific advisor for Regeneron, Sanofi Genzyme, Pfizer, AbbVie, Lea Pharma and Eli Lilly. Catherine A Harwood has had honoraria for speaking, and has consulted for, Almirall, Sanofi, Regeneron, Roche, Merck, Novartis, Leo Pharma, Pellepharm and L’Oreal. Richard Weller has received speaking fees from Leo and served on an advisory board for Almirall. Anthony P Bewley has provided ad-hoc consultancy for AbbVie, Almirall, Eli Lilly, Galderma, Janssen, Leo Pharma, Novartis, Sanofi and UCB. He has also had recent travel grants from AbbVie, Almirall and Leo Pharma. John T Lear has had honoraria for speaking, and has consulted for Almirall, Sanofi, Leo Pharma, Pellepharm, and Mayne Pharma. Richard Hudson, Rajesh Rout, Thishi Surendranathan and Milos Petrovic are employees and/or stockholders of Sanofi. The authors report no other conflicts of interest in this work.
References
1. Simpson EL, Bieber T, Eckert L, et al. Patient burden of moderate to severe atopic dermatitis (AD): Insights from a phase 2b clinical trial of dupilumab in adults. J Am Acad Dermatol. 2016;74(3):491–498. doi:10.1016/j.jaad.2015.10.043
2. Eichenfield LF, Tom WL, Chamlin SL, et al. Guidelines of care for the management of atopic dermatitis: section 1. Diagnosis and assessment of atopic dermatitis. J Am Acad Dermatol. 2014;70(2):338–351. doi:10.1016/j.jaad.2013.10.010
3. Kowalska-Olędzka E, Czarnecka M, Baran A. Epidemiology of atopic dermatitis in Europe. J Drug Assess. 2019;8(1):126–128. doi:10.1080/21556660.2019.1619570
4. NHS. Atopic Eczema; 2019. Available from: https://www.nhs.uk/conditions/atopic-eczema/.
5. Abuabara K, Yu AM, Okhovat J-P, Allen IE, Langan SM. The prevalence of atopic dermatitis beyond childhood: a systematic review and meta-analysis of longitudinal studies. Allergy. 2018;73(3):696–704. doi:10.1111/all.13320
6. Nettis E, Ortoncelli M, Pellacani G, et al. A multicenter study on the prevalence of clinical patterns and clinical phenotypes in adult atopic dermatitis. J Investig Allergol Clin Immunol. 2020;30(6):448–450. doi:10.18176/jiaci.0519
7. Barbarot S, Auziere S, Gadkari A, et al. Epidemiology of atopic dermatitis in adults: results from an international survey. Allergy. 2018;73(6):1284–1293. doi:10.1111/all.13401
8. França K, Lotti T. Complementary medicine and the role of integrative dermatology for the treatment of atopic dermatitis. Dermatol Ther.2017;30(4):e12469–12461.
9. Dattola A, Bennardo L, Silvestri M, Nisticò SP. What’s new in the treatment of atopic dermatitis? Dermatol Ther. 2019;32(2):e12787. doi:10.1111/dth.12787
10. Shalom G, Babaev M, Kridin K, et al. Healthcare service utilization by 116,816 patients with atopic dermatitis in Israel. Acta Derm Venereol. 2019;99(4):370–374. doi:10.2340/00015555-3117
11. Sicras-Mainar A, Navarro-Artieda R, Carrascosa Carrillo JM. Economic impact of atopic dermatitis in adults: a Population-Based Study (IDEA Study). Actas Dermosifiliogr. 2018;109(1):35–46. doi:10.1016/j.ad.2017.09.003
12. Armstrong AW, Huang A, Wang L, et al. Real-world utilization patterns of systemic immunosuppressants among US adult patients with atopic dermatitis. PLoS One. 2019;14(1):e0210517. doi:10.1371/journal.pone.0210517
13. Igarashi A, Fujita H, Arima K, et al. Health-care resource use and current treatment of adult atopic dermatitis patients in Japan: a retrospective claims database analysis. J Dermatol. 2019;46(8):652–661. doi:10.1111/1346-8138.14947
14. Silverwood RJ, Forbes HJ, Abuabara K, et al. Severe and predominantly active atopic eczema in adulthood and long term risk of cardiovascular disease: population based cohort study. BMJ. 2018;361:k1786. doi:10.1136/bmj.k1786
15. Silverberg JI, Gelfand JM, Margolis DJ, et al. Health utility scores of atopic dermatitis in US adults. J Allergy Clin Immunol Pract. 2019;7(4):1246–1252. doi:10.1016/j.jaip.2018.11.043
16. NICE. Dupilumab for treating moderate to severe atopic dermatitis; 2018. Available from: https://www.nice.org.uk/guidance/ta534.
17. Hanifin J, Rajka G. Diagnostic features of atopic dermatitis. Acta Derm Venereol. 1980;22(92):44–47.
18. Leshem YA, Hajar T, Hanifin JM, Simpson EL. What the eczema area and severity index score tells us about the severity of atopic dermatitis: an interpretability study. Br J Dermatol. 2015;172(5):1353–1357. doi:10.1111/bjd.13662
19. Langan SM, Thomas KS, Williams HC. What is meant by a “flare” in atopic dermatitis?: a systematic review and proposal. Arch Dermatol. 2006;142(9):1190–1196. doi:10.1001/archderm.142.9.1190
20. Drucker AM, Qureshi AA, Amand C, et al. Health care resource utilization and costs among adults with atopic dermatitis in the United States: a claims-based analysis. J Allergy Clin Immunol Pract. 2018;6(4):1342–1348. doi:10.1016/j.jaip.2017.10.024
21. Eckert L, Gupta S, Amand C, Gadkari A, Mahajan P, Gelfand JM. The burden of atopic dermatitis in US adults: health care resource utilization data from the 2013 National Health and Wellness Survey. J Am Acad Dermatol. 2018;78(1):54–61. doi:10.1016/j.jaad.2017.08.002
22. Megna M, Napolitano M, Patruno C, et al. Systemic treatment of adult atopic dermatitis: a review. Dermatol Ther. 2017;7(1):1–23. doi:10.1007/s13555-016-0170-1
23. Simpson EL, Bruin-Weller M, Flohr C, et al. When does atopic dermatitis warrant systemic therapy? Recommendations from an expert panel of the International Eczema Council. J Am Acad Dermatol. 2017;77(4):623–633. doi:10.1016/j.jaad.2017.06.042
24. Wollenberg A, Oranje A, Deleuran M, et al. ETFAD/EADV Eczema task force 2015 position paper on diagnosis and treatment of atopic dermatitis in adult and paediatric patients. J Eur Acad Dermatol Venereol. 2016;30(5):729–747. doi:10.1111/jdv.13599
25. Boguniewicz M, Alexis AF, Beck LA, et al. Expert perspectives on management of moderate-to-severe atopic dermatitis: a multidisciplinary consensus addressing current and emerging therapies. J Allergy Clin Immunol Pract. 2017;5(6):1519–1531. doi:10.1016/j.jaip.2017.08.005
26. Taylor K, Swan DJ, Affleck A, Flohr C, Reynolds NJ. Treatment of moderate-to-severe atopic eczema in adults within the U.K.: results of a national survey of dermatologists. Br J Dermatol. 2017;176(6):1617–1623. doi:10.1111/bjd.15235
27. Chernyshov PV, Tomas-Aragones L, Manolache L, et al. Quality of life measurement in atopic dermatitis. Position Paper of the European Academy of Dermatology and Venereology (EADV) task force on quality of life. J Eur Acad Dermatol Venereol. 2017;31(4):576–593. doi:10.1111/jdv.14058
28. Vakharia PP, Cella D, Silverberg JI. Patient-reported outcomes and quality of life measures in atopic dermatitis. Clin Dermatol. 2018;36(5):616–630. doi:10.1016/j.clindermatol.2018.05.011
29. National Institute for Health and Care Excellence. Frequency of application of topical corticosteroids for atopic eczema guidance and guidelines; 2004.
30. National Institute for Health and Care Excellence. Tacrolimus and pimecrolimus for atopic eczema guidance and guidelines; 2004.
31. Retzler J, Smith A, Reaney M, Rout R, Hudson R. Process utilities for topical treatment in atopic dermatitis. Quality Life Res. 2019;28(9):2373–2381. doi:10.1007/s11136-019-02174-0
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.