")
Back to Journals » Infection and Drug Resistance » Volume 16
A Rare Case of a Subcutaneous Abscess Caused by Nocardia cyriacigeorgica in an Immunocompetent Patient
Authors Lv H, Chen M, Ji Y, Pan L, Hong X, Ge Y
Received 28 October 2022
Accepted for publication 6 January 2023
Published 13 January 2023 Volume 2023:16 Pages 263—268
DOI https://doi.org/10.2147/IDR.S395333
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Huoyang Lv,1,* Mengyuan Chen,1,2,* Youqi Ji,1,3,* Liya Pan,4 Xin Hong,1,5 Yumei Ge1– 6
1Department of Clinical Laboratory, Zhejiang Provincial People’s Hospital (Affiliated People’s Hospital, Hangzhou Medical College), Hangzhou, Zhejiang, 310014, People’s Republic of China; 2The Second Clinical Medical College, Zhejiang Chinese Medical University, Hangzhou, Zhejiang, 310053, People’s Republic of China; 3School of Medical Technology and Information Engineering, Zhejiang Chinese Medical University, Hangzhou, Zhejiang, 310053, People’s Republic of China; 4Center for Rehabilitation Medicine, Department of Radiology, Zhejiang Provincial People’s Hospital (Affiliated People’s Hospital, Hangzhou Medical College), Hangzhou, Zhejiang, 310014, People’s Republic of China; 5Department of Green Pharmaceutical Collaborative Innovation Center, School of Pharmacy, Zhejiang University of Technology, Hangzhou, Zhejiang, 310014, People’s Republic of China; 6Key Laboratory of Biomarkers and in vitro Diagnosis Translation of Zhejiang Province, Hangzhou, Zhejiang, 310053, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yumei Ge, Department of Clinical Laboratory, Zhejiang Provincial People’s Hospital (Affiliated People’s Hospital, Hangzhou Medical College), Hangzhou, Zhejiang, 310014, People’s Republic of China, Email [email protected]
Background: Nocardia cyriacigeorgica, which mainly causes pleuropulmonary and disseminated nocardiosis, has been proved to be one of the most common opportunistic pathogens in patients with immunodeficiency, but the cases that cause subcutaneous abscesses in normal individuals are rare and should be paid attention to.
Methods: The clinical data of a patient with cutaneous nocardiosis caused by Nocardia cyriacigeorgica in Zhejiang Provincial People’s Hospital were retrospectively analyzed, including clinical manifestations, laboratory examinations, imaging examinations, medication and prognosis.
Results: Magnetic resonance imaging (MRI) showed that there was a 26 mm × 73 mm abscess under the skin. The pus in the abscess was green. Gram staining showed positive branched rod-shaped and undivided hyphae. After culture, small wrinkle dry white small colonies were observed, and it was identified as Nocardia cyriacigeorgica by MALDI-TOF MS.
Conclusion: We report the first case of a subcutaneous abscess caused by Nocardia cyriacigeorgica in an immunocompetent patient. Compared with cutaneous nocardiosis of which approximately 80% caused by Nocardia brasiliensis invasion, infection of Nocardia cyriacigeorgica is more insidious and latent, the features of the lesions are also unique. For this Nocardia cyriacigeorgica clinical isolate, the tested antibacterial drugs are generally sensitive and have an ideal prognosis after treatment with linezolid and timely debridement.
Keywords: Nocardia cyriacigeorgica, subcutaneous abscess, nocardiosis, matrix-assisted laser desorption ionization-time-of-flight mass spectrometry, MALDI-TOF MS, debridement
Introduction
Nocardia are aerobic saprophytes ubiquitously found in aquatic habitats, decaying organic matter and various soil types.1 Out of more than 100 defined subtypes to date, only approximately 30 of which are significance to human disease.2 Nocardia cyriacigeorgica (N. cyriacigeorgica) is recognized as an emerging pathogenic bacterium commonly manifesting as a localized or systemic infection in the immunocompromised population since it was first described and redefined from the bronchial secretion of a patient with chronic bronchitis in Germany in 2001 by Yassin.3,4 The most typical clinical manifestations of N. cyriacigeorgica are pleuropulmonary and disseminated infection mainly involved in patients with acquired immunodeficiency syndrome (AIDS), corticosteroid maintenance, ongoing malignancy and those with solid organ transplant and hematopoietic stem cell transplant recipients, who are deficient in T cell-mediated immunity.5–10 Nocardiosis caused by N. cyriacigeorgica is rare in immunocompetent hosts, usually acquired by wound infection after invasive surgery and inoculation on damaged skin with festering and scabbing.11 N. cyriacigeorgica-related subcutaneous abscesses are potentially leading to clinical misdiagnosis because they rare in clinical and asymptomatic with insidious manifestations. We reported a case of a subcutaneous abscess caused by N. cyriacigeorgica infection in an immunocompetent individual in order to increase the clinical understanding of the emerging infectious manifestations of N. cyriacigeorgica.
Case Presentation
Clinical Features
A 47-year-old woman was admitted to the hospital due to lumbago with radiating pain of right lower limb, waist distension and numbness for 3 weeks, and the symptoms got worse 4 days ago. After admission, physical examination and medical history examination found no murmur was heard in the auscultation area of each valve, no history of long-term drug use and the abdomen was soft. The right lower limb straight leg elevation test was 50 degrees (+), and the enhancement experiment was not cooperative. The patient’s temperature was normal, and he had no history of hypertension and diabetes. Abnormal elevation of neutrophils (75.6%) and C-reactive protein (CRP) (29.1 mg/L) were indicated by blood routine examination (Table 1).
 |
Table 1 Clinical and Laboratory Indicators of the Patient |
Magnetic Resonance Imaging and Computed Tomography Examination
Magnetic resonance imaging (MRI) of vertebra lumbalis showed lumbar disc herniation in L4/5 and L5/S1, dural sac damage, spinal canal stenosis and lumbar degenerative change. In addition, the size of the subcutaneous abnormal signal focus on the lumbar back was 26 mm × 73 mm, with low signal intensity on T1WI and high signal intensity on T2WI, and the boundary was vague, indicating that it was a subcutaneous abscess (Figure 1A). The chest radiograph showed that the patient’s lungs were normal (Figure 1B).
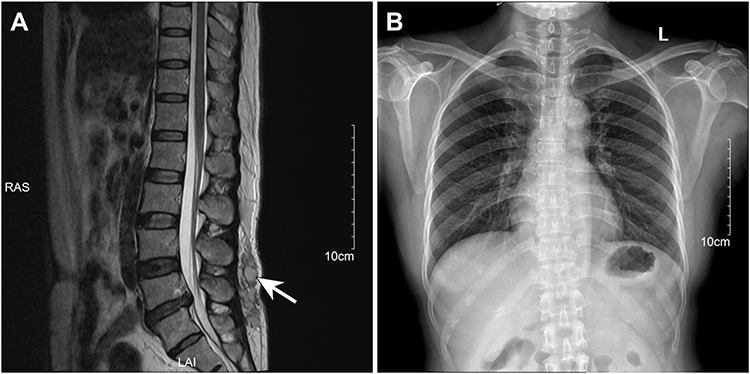 |
Figure 1 Imaging examination. (A) Magnetic resonance imaging (MRI) of vertebra lumbalis showed a 26 mm × 73 mm subcutaneous abscess with low signal intensity on T1WI and high signal intensity on T2WI (arrows). (B) The chest radiograph showed that the patient’s lungs were normal. |
Etiological Examination
Specimen handling and the identification procedures were followed standard laboratory protocols. Gram staining and acid-fast staining were performed on the pus extracted from the abscess, and the observation under the oil microscope showed that it was branching gram-positive rod and partially acid-fast, suggesting that it was likely to belong to Nocardia spp (Figure 2A and B). After the pus was cultured on the blood plate for 3 days, white colonies of different sizes could be seen. The colony was dry or waxy, with wrinkles and particles on its surface (Figure 2C). The colonies were identified by Matrix-assisted laser desorption ionization-time-of-flight mass spectrometry (MALDI-TOF MS) (bioMerieux, France) with 99.9% confidence value as N. cyriacigeorgica (Figure 2D). Kirby–Bauer method (KB) was performed to determine the maximum zone of inhibition (Zoi), and Epsilometer test (E-test) was performed to determine the minimum inhibitory concentration (MIC) value of the isolated N. cyriacigeorgica strain against amoxicillin/clavulanic acid, amikacin, clarithromycin, minocycline, imipenem, linezolid, levofloxacin, ceftriaxone (Table 1). Antibiotic susceptibility results of the N. cyriacigeorgica were judged by the Clinical and Laboratory Standards Institute (CLSI) interpretive breakpoints (CLSI M24: Susceptibility Testing of Mycobacteria, Nocardia spp., and Other Aerobic Actinomycetes). The isolated strain N. cyriacigeorgica was sensitive to the tested antibiotics, except for ceftriaxone (Table 2).
 |
Table 2 Antimicrobial Susceptibility of the Nocardia Cyriacigeorgica by Kirby–Bauer method and Epsilometer Test |
 |
Figure 2 Pathogenic examination. (A) Gram-positive and branching rod-shaped bacterium was observed by Gram staining under oil mirror (×1000 magnification). (B) Acid fast staining showed weak positive mycelia, which proved that it was probably Nocardia spp. (C) Wrinkled, dry and white colonies of different sizes were observed by culture on the blood plate. (D) Matrix-assisted laser desorption ionization-time-of-flight mass spectrometry (MALDI-TOF MS) confirm it was Nocardia cyriacigeorgica. |
Debridement
The patient was treated with vacuum sealing drainage (VSD). The skin tissue was cut open, and the abscess was found under the skin, and the pus was sucked up. The wound was washed with hydrogen peroxide and normal saline, and the wound was filled with VacuSeal. The pus was green, and further pathogenic examination was carried out.
Medication and Prognosis
According to the results of antibiotic sensitivity, the patient took 0.6 g linezolid orally twice a day for antibacterial treatment. After 2 months, the patient’s pain was relieved, and the inflammatory indicators neutrophils (68.4%) and CRP (1.0 mg/L) returned to normal.
Discussion
Nocardiosis has been recognized as an emerging communicable disease with an incidence rate of approximately 500–1000 cases in the United States every year, of which 60% are described in immunocompromised patients and about 10% are cutaneous in nature.12 Approximately 80% of cutaneous nocardiosis are caused by Nocardia brasiliensis13; thus we report the first case of a subcutaneous abscess caused by N. cyriacigeorgica in an immunocompetent patient in this area. Traumatic inoculation of skin by Nocardia brasiliensis progresses to cellulitis, nodules, impetigo, pyoderma, sporotrichosis-like lymphangitis, chronic pyogenic granuloma, multiple fistula or cutaneous involvement in hematogenous dissemination, mainly reported in patients with advanced AIDS and immunocompetent farmers with skin wounds, which were more common in the legs and feet, called mycetoma.14–16 Unlike previously reported cutaneous nocardiosis, which usually infect exposed wounds and cause suppuration, in this case, the patient is immunocompetent and has no skin lesion. Nocardia africana colonies in invaded tissues and pus manifest whitish “sulfur” granules.17 However, in our case, the pus extracted from the N. cyriacigeorgica -related subcutaneous abscess was green, and this pathological phenomenon should be known by more clinical laboratory technicians. Without radioactive or ultrasonic examination, it is difficult to find the presence of the lesions. Compared with cutaneous nocardiosis caused by Nocardia brasiliensis invasion, infection of N. cyriacigeorgica is more insidious and latent.
At present, Nocardia cases that have been reported in detail are limited, the reported average age of patients impacted by Nocardia is 40 years old, and the infection risk of males is higher than females, with an incidence of 3:1.18 In this case, the patient with the subcutaneous abscess caused by N. cyriacigeorgica infection was a 47-year-old woman. Sulfonamides are the first-line antibiotics for treating disseminated nocardiosis and usually combine with amikacin, linezolid or imipenem.19 Most reported N. cyriacigeorgica strains are generally susceptible to sulfonamides, broad-spectrum cephalosporins, amikacin, imipenem, and linezolid but resistant to penicillins, clarithromycin, and ciprofloxacin with the exception of a few strains that have been reported to be susceptible to ciprofloxacin.4,20,21 The isolated strain N. cyriacigeorgica from this patient was sensitive to amoxicillin/clavulanic acid, amikacin, clarithromycin, minocycline, imipenem, linezolid, levofloxacin, except for ceftriaxone in vitro. N. cyriacigeorgica (20.8%, 11/53) were reported in a study of 53 non-repetitive Nocardia isolates collected from 8 tertiary general hospitals of 7 cities in China with a 63.6% (7/11) resistance rate of ciprofloxacin.22 In general, linezolid is still absolutely sensitive to all N. cyriacigeorgica strains.
Conclusion
In conclusion, we report the first case of a subcutaneous abscess caused by N. cyriacigeorgica in an immunocompetent patient. Compared with cutaneous nocardiosis of which approximately 80% caused by Nocardia brasiliensis invasion, infection of N. cyriacigeorgica is more insidious and latent, the features of the lesions are also unique. For this N. cyriacigeorgica clinical isolate, the tested antibacterial drugs are generally sensitive and have an ideal prognosis after treatment with linezolid. Awareness of N. cyriacigeorgica as a distinct pathogenic entity in immunocompetent patients and accurate clinical diagnosis should be emphasized.
Ethics Approval and Consent to Participate
This study was supported by the Ethics Committee of Zhejiang People’s Hospital (Ethics Committee Approval of Biomedical Research Involving Humans, Approval No. 2022JS008) and was carried out in accordance with the ethical standards of the Declaration of Helsinki.
Consent for Publication
Written and informed consent was obtained from the patient for publication of this case report and any accompanying images.
Acknowledgments
We thank all members of the microbiology laboratory of Zhejiang Provincial People’s Hospital for their help in the collection of clinical data and the fitness coach Huang Haotian for his encouragement.
Funding
This study was supported by the New Project of Zhejiang Provincial People’s Hospital entitled “Construction of Rapid Nucleic Acid Detection Platform for Invasive Fungi” (20211214).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Wang H, Zhu Y, Cui Q, et al. Epidemiology and antimicrobial resistance profiles of the Nocardia species in China, 2009 to 2021. Microbiol Spectr. 2022;10(2):e0156021. doi:10.1128/spectrum.01560-21
2. Brown-Elliott BA, Brown JM, Conville PS, et al. Clinical and laboratory features of the Nocardia spp. based on current molecular taxonomy. Clin Microbiol Rev. 2006;19(2):259–282. doi:10.1128/CMR.19.2.259-282.2006
3. Yassin AF, Rainey FA, Steiner U. Nocardia cyriacigeorgici sp. nov. Int J Syst Evol Microbiol. 2001;51(Pt4):1419–1423. doi:10.1099/00207713-51-4-1419
4. Schlaberg R, Huard RC, Della-Latta P. Nocardia cyriacigeorgica, an emerging pathogen in the United States. J Clin Microbiol. 2008;46(1):265–273. doi:10.1128/JCM.00937-07
5. Gabay S, Yakubovsky M, Ben-Ami R, Grossman R. Nocardia cyriacigeorgica brain abscess in a patient on low dose steroids: a case report and review of the literature. BMC Infect Dis. 2022;22(1):635. doi:10.1186/s12879-022-07612-y
6. Alp E, Yildiz O, Aygen B, et al. Disseminated nocardiosis due to unusual species: two case reports. Scand J Infect Dis. 2006;38(6–7):545–548. doi:10.1080/00365540500532860
7. Maraki S, Panagiotaki E, Tsopanidis D, et al. Nocardia cyriacigeorgica pleural empyema in an immunocompromised patient. Diagn Microbiol Infect Dis. 2006;56(3):333–335. doi:10.1016/j.diagmicrobio.2006.05.001
8. Gutiérrez C, Céspedes A, Legarraga P, et al. Infección por Nocardia cyriacigeorgica en paciente con infección por VIH en etapa SIDA. Rev Chilena Infectol. 2020;37(3):322–326. doi:10.4067/s0716-10182020000300322
9. Lin J, Wu XM, Peng MF. Nocardia cyriacigeorgica infection in a patient with pulmonary sequestration: a case report. World J Clin Cases. 2021;9(10):2367–2372. doi:10.12998/wjcc.v9.i10.2367
10. Peng Y, Dong X, Zhu Y, et al. A rare case of pulmonary nocardiosis comorbid with Sjogren’s syndrome. J Clin Lab Anal. 2021;35(9):e23902. doi:10.1002/jcla.23902
11. Oda R, Sekikawa Y, Hongo I. Primary cutaneous Nocardiosis in an immunocompetent patient. Intern Med. 2021;56(4):469–470. doi:10.2169/internalmedicine.56.7810
12. Makadia S, Patel I, Soosaipillai I, et al. First case of Nocardia pseudobrasiliensis causing primary cutaneous nocardiosis in an immunocompetent patient. J Investig Med High Impact Case Rep. 2020;8:2324709620938228. doi:10.1177/2324709620938228
13. Fukuda H, Saotome A, Usami N, et al. Lymphocutaneous type of nocardiosis caused by Nocardia brasiliensis: a case report and review of primary cutaneous nocardiosis caused by N. brasiliensis reported in Japan. J Dermatol. 2008;35(6):346–353. doi:10.1111/j.1346-8138.2008.00482.x
14. Chu L, Xu X, Ran Y. Primary cutaneous nocardiosis caused by Nocardia brasiliensis following a wasp sting. Clin Exp Dermatol. 2017;42(4):416–419. doi:10.1111/ced.13086
15. Maraki S, Chochlidakis S, Nioti E, et al. Primary lymphocutaneous nocardiosis in an immunocompetent patient. Ann Clin Microbiol Antimicrob. 2004;3:24. doi:10.1186/1476-0711-3-24
16. Verma P, Jha A. Mycetoma: reviewing a neglected disease. Clin Exp Dermatol. 2019;44(2):123–129. doi:10.1111/ced.13642
17. de Farias MR, Werner J, Ribeiro MG, et al. Uncommon mandibular osteomyelitis in a cat caused by Nocardia africana. BMC Vet Res. 2012;8:239. doi:10.1186/1746-6148-8-239
18. Centers of Disease Control and Prevention. Risk of infection. Available from: https://www.cdc.gov/nocardiosis/infection/index.html.
19. Margalit I, Lebeaux D, Tishler O, et al. How do I manage nocardiosis? Clin Microbiol Infect. 2021;27:550–558. doi:10.1016/j.cmi.2020.12.019
20. Barnaud G, Deschamps C, Manceron V, et al. Brain abscess caused by Nocardia cyriacigeorgica in a patient with human immunodeficiency virus infection. J Clin Microbiol. 2005;43(9):4895–4897. doi:10.1128/JCM.43.9.4895-4897.2005
21. Yildiz O, Alp E, Tokgoz B, et al. Nocardiosis in a teaching hospital in the Central Anatolia region of Turkey: treatment and outcome. Clin Microbiol Infect. 2005;11(6):495–499. doi:10.1111/j.1469-0691.2005.01145.x
22. Huang L, Chen X, Xu H, et al. Clinical features, identification, antimicrobial resistance patterns of Nocardia species in China: 2009–2017. Diagn Microbiol Infect Dis. 2019;94(2):165–172. doi:10.1016/j.diagmicrobio.2018.12.007
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.