Back to Journals » Nutrition and Dietary Supplements » Volume 18
A Randomized, Triple-Blind, Placebo Controlled, Parallel Virtual Clinical Trial to Investigate the Efficacy of Royal Jelly Supplementation on Upper Respiratory Tract Infections in Healthy Adults
Authors Yumol JL, Kopinč R, Al-Wahsh H, Crowley DC, Guthrie N, Lewis ED, Moulin M
Received 20 January 2026
Accepted for publication 7 June 2026
Published 10 July 2026 Volume 2026:18 597540
DOI https://doi.org/10.2147/NDS.S597540
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ara Kirakosyan
Jenalyn L Yumol,1 Rok Kopinč,2 Huda Al-Wahsh,1 David C Crowley,1 Najla Guthrie,1 Erin D Lewis,1 Marc Moulin1
1KGK Science Inc, London, ON, Canada; 2Medex d.o.o, Ljubljana, Slovenia
Correspondence: Marc Moulin, KGK Science Inc, London, ON, Canada, Email [email protected]
Purpose: To investigate the efficacy of royal jelly (RJ) supplementation compared to placebo on upper respiratory tract infection (URTI) symptoms in healthy adults during the 2024– 2025 North American cold and flu season.
Patients and Methods: One hundred healthy adults aged 18 to 65 years inclusive with at least two self-reported incidences of URTIs in the last 12 months were randomized to RJ supplementation or placebo. Participants underwent a 14-day pre-conditioning period followed by a 84-day study period, for a total of 98 days of supplementation (two capsules daily). The change in frequency, severity, and duration of URTIs from baseline to end of study were assessed using the Wisconsin Upper Respiratory Symptom Survey-24 (WURSS-24). Compliance with study products (RJ or placebo) and adverse events were recorded daily.
Results: RJ supplementation was found to be safe and well tolerated. There was a low incidence of URTIs reported over the study period (32.61% vs. 31.82% without URTI incidence), with no significant differences in the frequency, severity, or duration of URTIs between RJ and placebo supplementation. Post-hoc analyses showed the RJ group reported significantly fewer sick days, as observed from Days 43 to 84 (2.98 vs. 3.98 days), and an overall trend demonstrating fewer reported use of cold and flu medications, when compared to the placebo group. In participants that reported greater symptom severity (n = 32), the RJ group reported significantly lower severity of URTI symptoms as assessed by area under the curve (172.24 vs. 277.46), along with lower severity for individual symptoms including coughs, tiredness, body aches, and scratchy throat, compared to the placebo group.
Conclusion: The low incidence of URTIs over the 84-day study period may have masked potential effects of RJ supplementation on the frequency, severity, and duration of URTIs. However, post hoc results suggested relief of some URTI symptoms in healthy adults who reported more severe symptoms and in younger adults. Further investigation using adequately powered studies is warranted to confirm these findings within targeted groups to understand the role of RJ for supporting immune health.
Keywords: respiratory tract infections, WURSS-24, royal jelly, healthy adults
Introduction
Upper respiratory tract infections (URTIs) are among the most common illnesses with approximately 12.8 billion incidences reported globally in 2021.1 URTIs are transmitted via several routes, such as aerosols, person-to-person contact, or contact with contaminated surfaces. In addition to seasonal trends, the incidence of URTIs is highly influenced by psychosocial factors (eg., sociability/crowding, stress, sleep, smoking, nutrition and exercise) that negatively affect immunologic responses.2 There is a broad range of URTI symptoms varying in severity and duration and include, but are not limited to, nasal congestion, sore throat, muscle pains, cough, and headache.3 URTIs can lead to a reduction in an individual’s quality of life and contribute to a substantial economic burden. In United States, the economic burden of common cold and influenza is approximately $87 billion per year.4,5 While the vast majority of URTIs are self-limited, some can lead to severe complications, such as pneumonia, otitis media, glomerulonephritis, that require medical intervention and further contribute to the healthcare burden. Given the lack of effective preventative options available (eg., vaccinations), current strategies are aimed at providing symptom relief. Use of prescribed (eg., antiviral therapies) or over-the-counter cold and flu medications such as decongestants and analgesics (eg., acetaminophen or nonsteroidal anti-inflammatory drugs) may temporarily alleviate symptoms. However, evidence for the effectiveness of these treatments is limited,6 and warnings and precautions for side effects, toxicity, or drug interactions7 can deter use. Therefore, alternative safe and efficacious strategies to support immune health, such as prevention or reduction in the frequency, severity, and/or duration of URTI symptoms, during cold and flu season are warranted.
The investigational product (IP), Bio Gelee Royale Forte (Medex d.o.o, Ljubljana, Slovenia), contains royal jelly (RJ) which is a secretion of the hypopharyngeal and mandibular glands of nurse bees and used to feed the bee larvae and adult queen bees. RJ is commonly used as a functional food due to its antibacterial, antioxidant, anti-inflammatory, and anti-aging properties.8 Fresh RJ contains 60–70% water, 12–15% proteins, 10–16% total sugar, 3–6% lipids, vitamins, salts, and free amino acids.9 Previous clinical trials conducted in healthy populations have demonstrated beneficial effects of RJ on glucose10,11 and lipid metabolism.12–14 While current evidence suggests RJ may play a role in improving human health, little is known about the effects of RJ for preventing URTIs or mitigating the severity and/or duration of URTI symptoms. The objective of this study is to investigate the efficacy of RJ supplementation compared to placebo on URTIs in healthy adults with self-reported susceptibility to URTIs during the cold and flu season.
Materials and Methods
Ethical and Regulatory Approval
This randomized, triple-blind, placebo controlled, parallel virtual clinical trial was conducted by KGK Science Inc. (London, Ontario, Canada) from October 2024 to April 2025. The trial was registered on ClinicalTrials.gov (Identifier: NCT06573814, August 20, 2024) and reviewed by the Natural and Non-Prescription Health Product Directorate, Health Canada (Ottawa, Ontario), with notice of authorization granted on September 26, 2024. Research ethics board approval was granted on October 4th, 2024, by Advarra (Aurora, Ontario; Pro00080103). Written consent was obtained from all participants prior to participation in the study, and the study was conducted according to the requirements of the International Council for Harmonization of Technical Requirements for Pharmaceuticals for Human Use (ICH) Guidelines for Good Clinical Practice (GCP) and applicable local regulatory guidelines. Consolidated Standards of Reporting Trials (CONSORT) guidelines for randomized controlled trials were also followed.15
Study Design and Population
The current study consisted of a 14-day pre-conditioning period followed by 84 days of supplementation for a total study duration of 98 days (Figure 1). At screening, an electronic informed consent form was provided to the volunteers. Upon agreement, screening assessments included the collection of information regarding eligibility criteria, medical history, demographics, anthropometrics, health status, vaccination status, concomitant therapies, and the number of URTI episodes in the previous 12 months. Using block randomization,16 eligible participants were randomized to receive RJ supplementation or placebo. Participants were instructed to start taking the study product after receiving the shipment for a total of 98 days. If there was an URTI incident between enrollment and Day −14, participants were instructed to start taking the study product three days after resolution of symptoms. Baseline was scheduled based on the confirmed date of receipt and initiation of the study product.
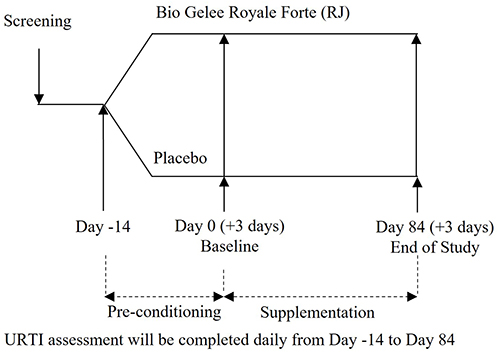 |
Figure 1 Study design. |
Participants were healthy adults aged 18 to 65 years inclusive, with at least two self-reported incidences of URTIs in the last 12 months. All participants were instructed to maintain their current lifestyle, including diet, exercise, supplements/medications, and sleep, as much as possible throughout the study period. Individuals were excluded if they were pregnant, breastfeeding, or planning to become pregnant during the trial, had any allergies or sensitivities to the ingredients of the study products, self-reported allergy to bees or other insects, self-reported autoimmune disease or were immune compromised due to other factors, current or anticipated severe environmental allergies during the study period requiring medication or need for allergy shots, ongoing diagnosis of acute or chronic respiratory illness (eg., asthma, chronic bronchitis, sinusitis, pharyngitis, chronic obstructive pulmonary disease), or any other condition or lifestyle factor, that, in the opinion of the Qualified Investigator, may have adversely affected the participant’s ability to complete the study or its measures or have posed significant risk to the participant. Individuals with current use of prescribed (eg., medications to control immune-related conditions, corticosteroids, cyclosporine, tacrolimus, methotrexate or azathioprine, or antibiotics) and/or over-the-counter medications or supplements (eg., bee products [unless willing to washout], echinacea, zinc, postbiotics, vitamin C, or vitamin D) that could impact the efficacy and/or safety of the IP were also excluded.
Randomization and Blinding
Participants were assigned a randomization code according to the order of the randomization list generated using Greenlight Guru Clinical (Indianapolis, IN). The study products were sealed in identically appearing blister packs and labeled by personnel not involved in the study assessment. The investigators, study personnel, and participants were blinded to the study groups.
Investigational Product and Placebo
Each capsule of the IP contained 334 mg of organic lyophilized RJ (equivalent to 1000 mg of fresh RJ), standardized to minimum 4% 10-hydroxy-2-decenoic acid and a minimum of 1% acetylcholine, two naturally present active ingredients in RJ (Bio Gelee Royale Forte, Medex d.o.o, Ljubljana, Slovenia). The placebo contained rice flour. Both study products were supplied in hydroxypropyl methylcellulose capsules. Participants were instructed to take two capsules each morning on an empty stomach for a total of 98 days, totaling 2000 mg equivalent dose of fresh RJ daily. If a dose was missed, participants were instructed to take the dose approximately two hours after a meal but to not exceed two capsules daily.
Study Outcomes
The primary outcome was the difference between RJ and placebo in frequency, severity (area under the curve [AUC] for total symptom scores), and duration of URTIs from Days 0 to 84, as assessed by the Wisconsin Upper Respiratory Symptom Survey-24 (WURSS-24) questionnaire. The WURSS-24 questionnaire has been validated by Barrett et al and includes questions related to health status, presence and severity of URTI symptoms, symptoms related to allergies, as well as their impact on quality of life.17 Based on this questionnaire, an URTI episode was defined as the appearance of one or more symptoms not attributed to allergies with at least two days of “not sick” in between as defined by Murdoch et al.18 The frequency of URTI was the number of URTI episodes per person. The severity of URTI symptoms was measured by the AUC for daily total symptom scores as well as the average severity of total and individual URTI symptoms. The duration of URTI was the number of days of the URTI episode per person, in which the number of sick days was determined by the number of days scored as any number from 1 (very mild) through 7 (severe) for the question, “How sick do you feel today?”. Not sick was scored as 0.
Secondary outcomes included the difference between RJ and placebo in frequency, severity (AUC, overall and individual average severity of URTI symptom scores), and duration of URTIs from Days −14 to −1 and −14 to 84, as assessed by the WURSS-24 questionnaire; the difference between groups in the overall and individual average severity of URTI symptom scores from Days 0 to 84; as well as the difference between groups in the proportion of participants with URTI incidences, self-reported number of sick days, and use of prescription and non-prescription cold or flu medications from Days −14 to −1, 0 to 84, and −14 to 84.
Safety was assessed based on self-reported AEs. For all AEs, the severity (mild, moderate, or severe) and degree of relationship between the study product and AE (not related, unlikely, possibly, probably, or definitely) were determined by the Qualified Investigator.
A daily study diary was used to complete the WURSS-24 questionnaire, record study product compliance, missed workdays due to URTI, concomitant therapies, and change in health status. Study diaries were reviewed monthly by the investigational staff.
Statistical Analysis
A sample size of 100 participants (50 participants per group) could detect a rate of ≤3.51 for the number of episodes of URTIs and duration of ≤8.75 days of URTI symptoms in the IP group using Poisson regression model with 80% power, 2-sided 5% significance level, and 20% dropout rate. The estimation was obtained assuming participants in the placebo group would experience 4.79 episodes of URTIs over the 84-day study period and duration of 10.7 days of URTI symptoms.19,20 Additionally, a sample size of 100 participants (50 participants per group) could detect a difference of ≥18 in the mean AUC between IP and placebo groups assuming standard deviation equal to 8.41 and 38.92 for IP and placebo groups,19 respectively, using two-sample t-test with 80% power, 2-sided 5% significance level, and 20% dropout rate.
The difference in the frequency and duration of URTI episodes between RJ and placebo groups was assessed using a generalized linear model with log link function (Poisson or negative binomial regression model). The model included the study group as a fixed effect as well as age and/or sex if they are significantly different between groups at baseline. The severity of URTIs was measured by the AUC for daily total symptom scores of the WURSS-24 questionnaire. The difference in the mean AUC for daily WURSS-24 questionnaire total symptom scores between RJ and placebo groups was assessed by t-test if the outcome was normally distributed or by Wilcoxon rank-sum test if the outcome was not normally distributed. AUC was calculated using the trapezoidal area approximation method. The normality assumption was assessed using Q-Q plots. Post-hoc subgroup analysis was performed for Days 0 to 84 in the per-protocol (PP) population based on AUC of symptom severity score (1–100 vs. >100), sex (females vs. males), age (<45 years vs. ≥45 years), and study period (Days 0–42 and Days 43–84).
All statistical analysis were completed using the R Statistical Software Package Version 4.3.2 or newer for Microsoft Windows. P < 0.05 was considered statistically significant, and data are presented at mean ± standard deviation (SD) unless otherwise stated.
Results
A total of 293 volunteers were screened for their participation in the study with 100 eligible participants enrolled and included in the intention-to-treat (ITT) population (Figure 2). Participants were excluded from the PP population due to early termination (n=10), concomitant medication use (n=4) and missing data related to the measurement of the primary outcome (n=1). The PP population consisted of 85 participants (Figure 2).
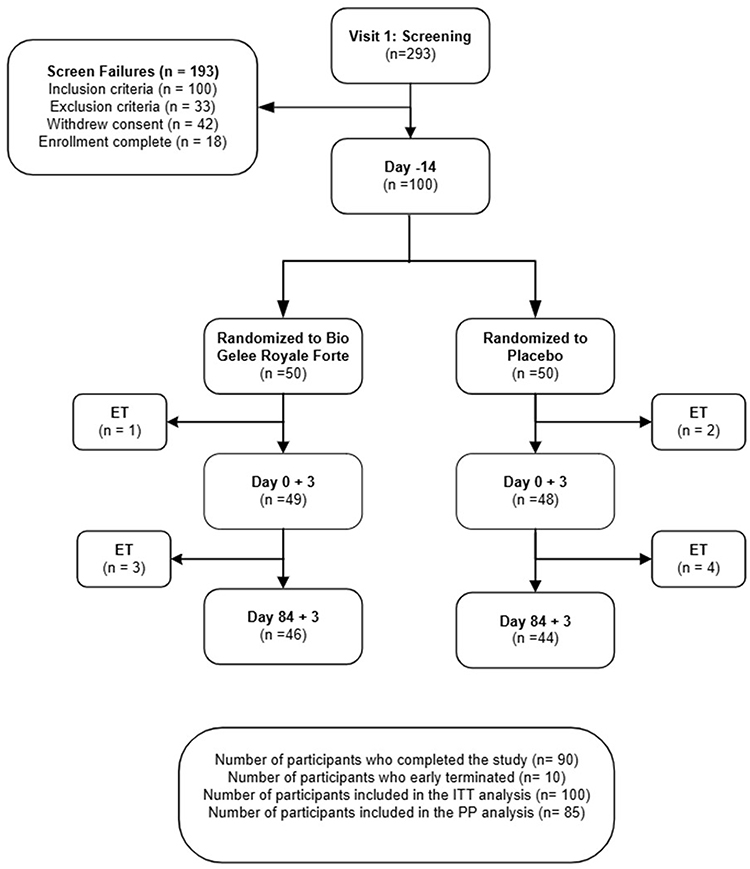 |
Figure 2 Disposition of study participants. Abbreviation: ET, Early Termination. |
Participant demographics (age, sex, race), anthropometrics (height, weight), vaccination status, and use of cold and flu medication were similar between the RJ and placebo groups (Table 1), with no significant differences between groups in either the ITT or PP populations (P ≥ 0.133). The complete sample population consisted of adults between age 20 to 66 years with the majority self-reported female (73%) and Western European White race (52%) (Table 1). Overall, 80% of participants were vaccinated, with no significance between groups at baseline (84% vs. 76%, P = 0.454). Study product compliance (99–101%) was similar between the RJ and placebo groups from Day −14 to Day 84 in the ITT or PP populations (P ≥ 0.879).
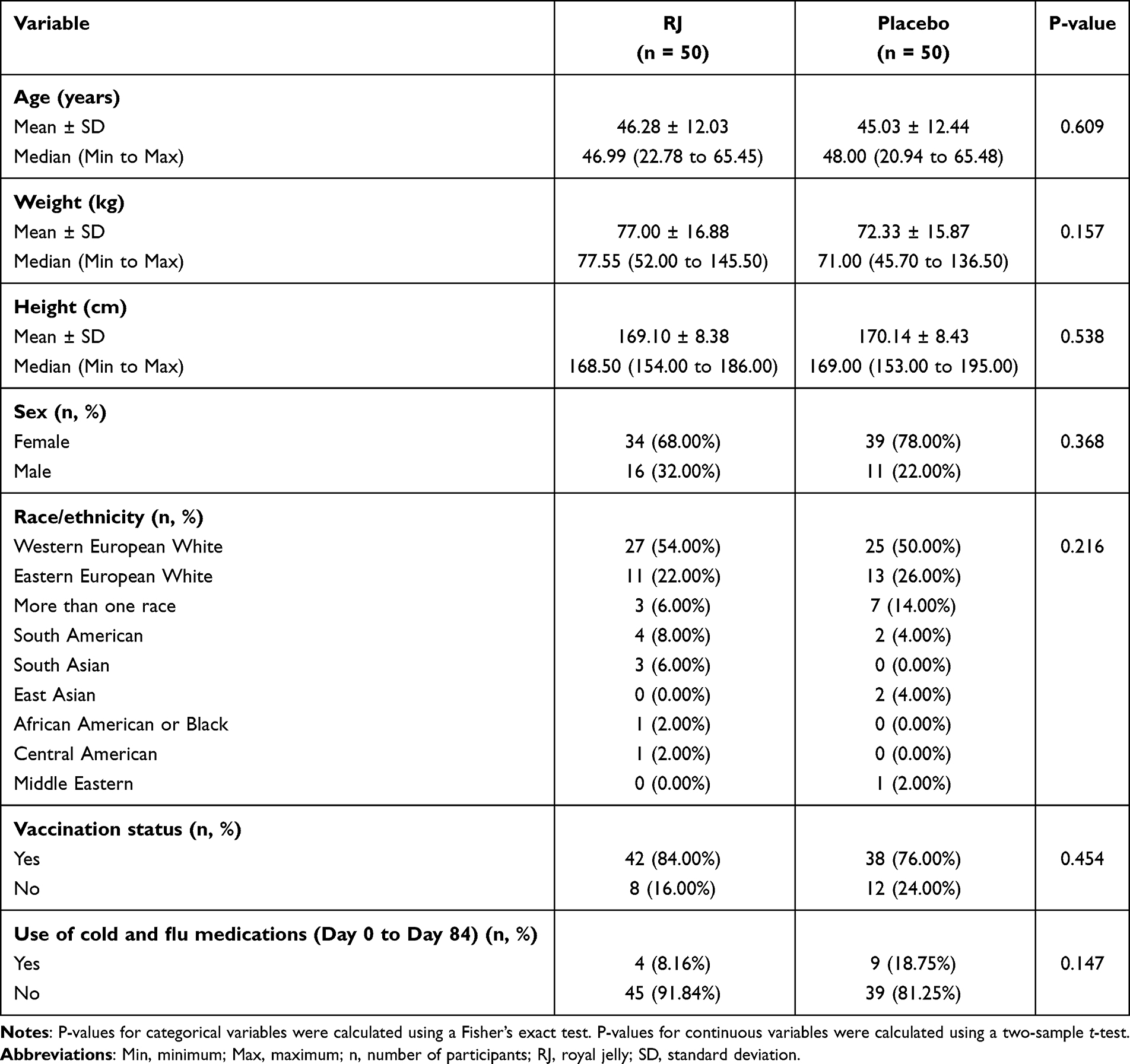 |
Table 1 Demographics of the ITT Population (n=100) |
Safety
Twenty-six post-emergent adverse events (AEs) were reported by 16 participants supplemented with RJ, and 27 AEs were reported by 20 participants taking placebo. Seven AEs were related to gastrointestinal concerns, abdominal discomfort, nausea, or a rash that were deemed possibly related to the study products with three in the RJ group and four in the placebo group. All possibly related AEs were resolved by the end of the study period, except for one incidence of moderate abdominal discomfort reported by a participant taking the placebo. The participant was followed until confirmation that they received consultation by a gastrointestinal specialist. All other AEs reported were deemed not related or unlikely to be related to study product and were resolved by the end of the study period. No serious adverse events were reported.
Frequency of Upper Respiratory Tract Infections
Overall, there was a low incidence of URTIs reported, as 32.61% of participants in the RJ group (n=15) and 31.82% of participants in the placebo group (n=14) did not report any URTIs after the pre-conditioning period (Day 0 to Day 84). Similar proportions were observed in the PP population (33.33% vs. 32.50%). There was no significant difference in the frequency of URTI incidence between the RJ and placebo groups (ITT: 1.30 vs. 1.41, P = 0.670 [Table S1]; PP: 1.27 vs. 1.35, P = 0.737 [Table 2]) from Days 0 to 84, which was also observed from Days −14 to −1 and Days −14 to 84 in the ITT or PP populations (P ≥ 0.663).
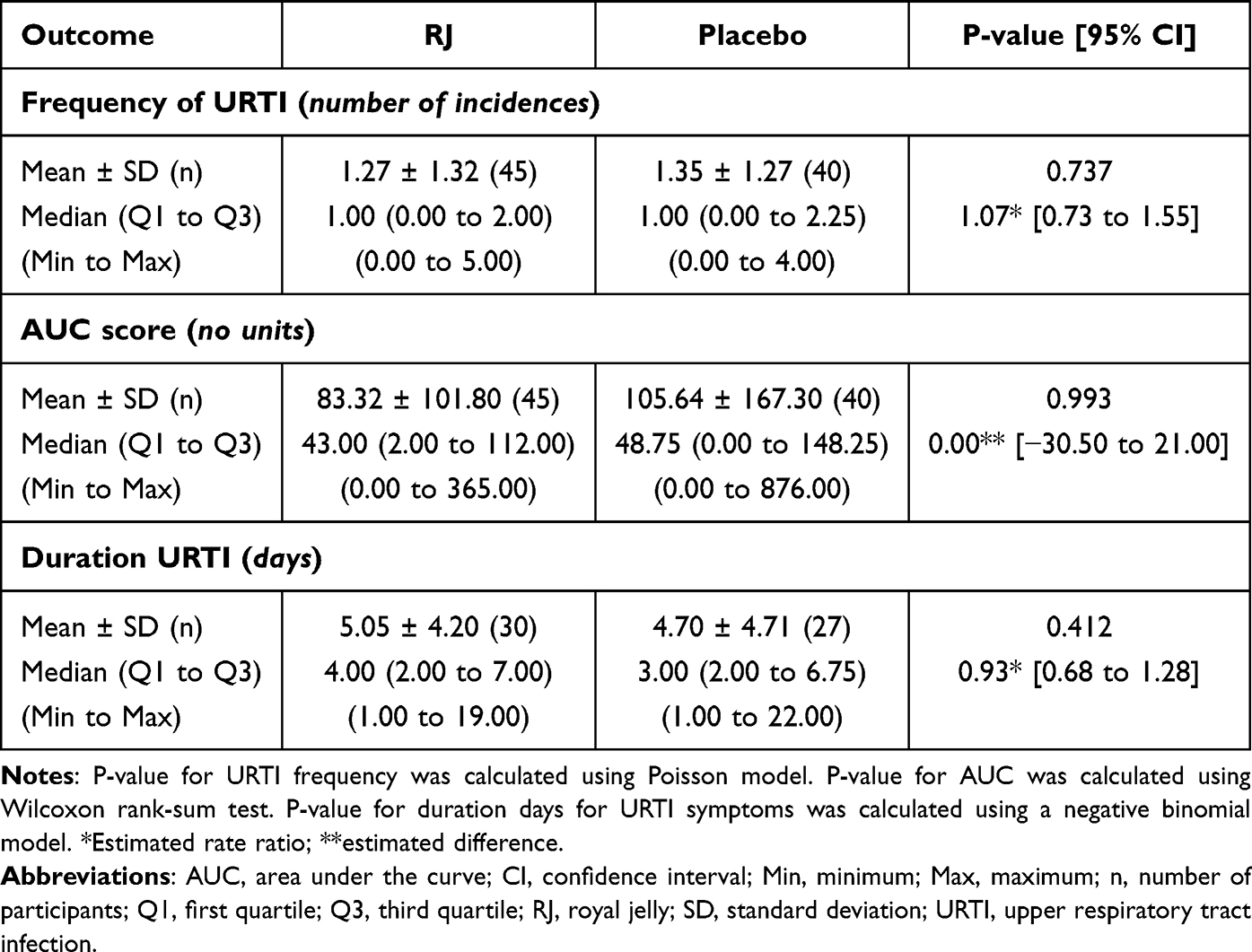 |
Table 2 Frequency, Severity, and Duration of URTIs, as Assessed by the WURSS-24 Questionnaire Over the 84-Day Supplementation Period (Day 0 to 84) for the PP Population (n=85) |
Based on post-hoc subgroup analysis of the PP population, stratified by severity score (AUC 1–100: 1.11 vs. 1.56, P = 0.256; AUC>100: 1.95 vs. 2.23, P = 0.584), age (<45 years: 0.94 vs. 1.56, P = 0.118; ≥45 years: 1.45 vs. 1.21, P = 0.453), sex (females: 1.33 vs. 1.50, P = 0.588; males: 1.13 vs. 0.90, P = 0.576), or study period (Days 0 to 42: 0.76 vs. 0.78, P = 0.919; Days 43 to 84: 0.51 vs. 0.57, P = 0.690), the frequency of URTIs was similar between the RJ and placebo groups.
Severity of Upper Respiratory Tract Infections
For both the ITT and PP populations, the average severity of URTIs did not differ between the RJ and placebo groups (ITT: AUC of 83.24 vs. 109.03, P = 0.994 [Table S1]; PP: AUC of 83.32 vs. 105.64, P = 0.993 [Table 2]). Additionally, no difference in AUC for daily total severity symptom scores was observed between groups from Days −14 to −1 or −14 to 84 (P ≥ 0.778).
Post-hoc subgroup analysis stratified by severity (AUC 1–100 vs. >100) suggested RJ supplementation had greater efficacy for participants with higher reported severity. Of participants with an AUC > 100 (19 participants in the RJ group and 13 participants in the placebo group), the RJ group reported significantly lower severity (AUC of 172.24 vs. 277.46), when compared to the placebo. There was no significant effect of RJ on AUC score when stratified by age (<45 years: 86.72 vs. 159.25, P = 0.132; ≥45 years: 81.45 vs. 69.90, P = 0.757), sex (females: 81.62 vs. 118.47, P = 0.302; males: 86.73 vs. 67.15, P = 0.728), or study period (Days 0 to 42: 52.81 vs. 49.92, P = 0.649; Days 43 to 84: 29.60 vs. 55.17, P = 0.776).
Duration of Upper Respiratory Tract Infections
The mean duration of URTIs was similar between the RJ and placebo groups from Days 0 to 84 (ITT: 4.98 vs. 4.89 days, P = 0.832 [Table S1]; PP: 5.05 vs. 4.70 days, P = 0.412 [Table 2]), as well as Days −14 to −1 and −14 to 84 (P ≥ 0.121). This lack of difference between study groups in the PP population was also observed when stratified by severity (AUC 1–100: 3.65 vs. 2.92, P = 0.379; AUC>100: 5.86 vs. 6.35, P = 0.681), age (<45 years: 4.00 vs. 5.00, P = 0.446; ≥45 years: 5.38 vs. 4.44, P = 0.351), sex (females: 4.46 vs. 4.76, P = 0.731; males: 6.50 vs. 4.44, P = 0.266), or study period (Days 0 to 42: 4.37 vs. 4.15, P = 0.829; Days 43 to 84: 5.10 vs. 5.00, P = 0.936).
Severity of Individual Symptoms
The overall average severity of URTI symptom scores was 0.08 in the RJ group and 0.10 in the placebo group from Days 0 to 84 in both the ITT (P = 0.977) and PP populations (P = 0.982). Individual symptom severity was similar between the RJ and placebo groups in the ITT population (Figure S1). There were no significant differences between groups in total daily severity scores or individual symptom severity from Days −14 to −1 or −14 to 84 (P ≥ 0.129).
Based on subgroup analysis of the PP population, participants supplemented with RJ and an AUC>100 reported a significantly lower overall average severity of URTI symptom scores (0.16 vs. 0.25; Figure 3A), as well as lower severity of coughs (0.21 vs. 0.39), tiredness (0.27 vs 0.42), body aches (0.11 vs. 0.25), and scratchy throat (0.14 vs. 0.32), when compared to the placebo (Figure 3B). In participants <45 years of age, RJ supplementation resulted in significantly lower severity of coughs compared to the placebo group (0.07 vs. 0.26). No significant differences in average severity scores or severity of individual URTI symptoms were observed between study groups in participants aged 45 years or older (P ≥ 0.154), or when stratified by sex (P ≥ 0.136) or study period (P ≥ 0.197) (data not shown).
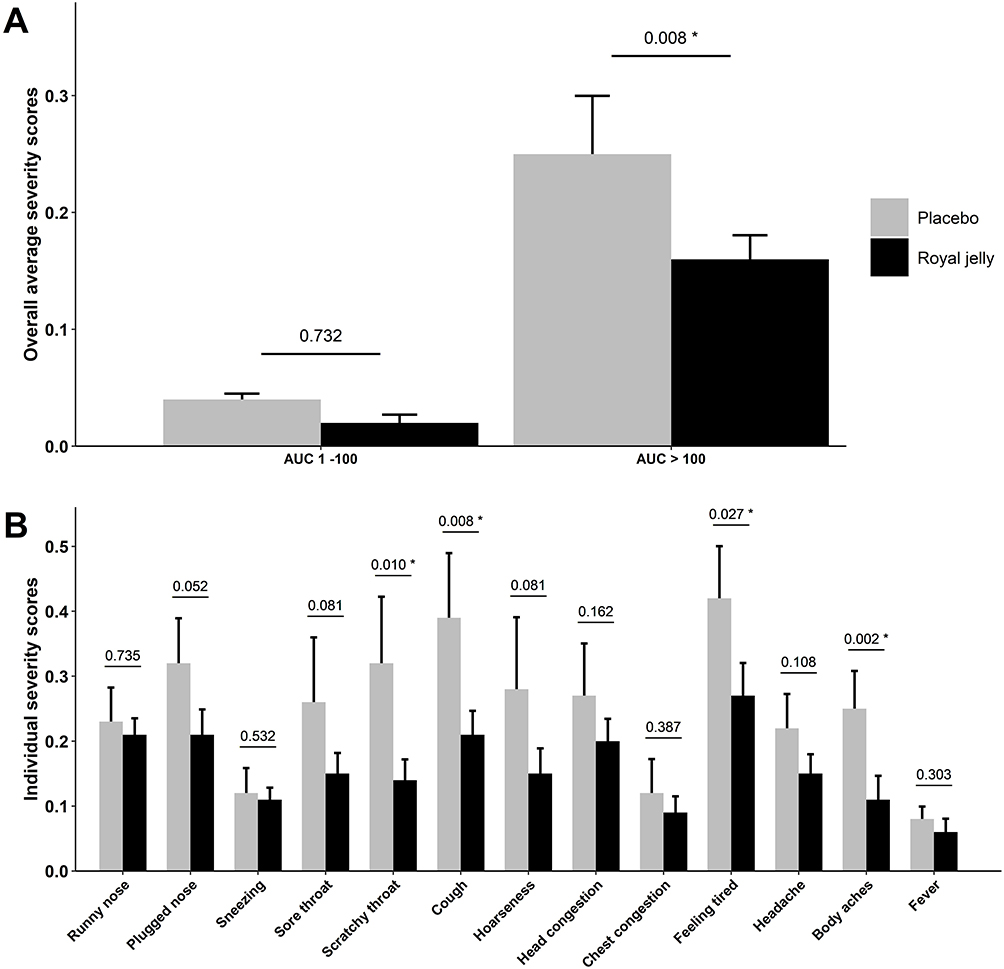 |
Figure 3 (A) Overall average severity score of URTI symptoms of the PP population (n = 85) when stratified by AUC (1–100 vs. >100); and (B) individual symptom severity scores reported by participants with a higher severity of URTI symptoms (AUC >100) (n = 32), as assessed by the WURSS-24 questionnaire; *denotes a significant difference between the RJ and placebo groups. Data are presented as mean ± standard error. |
Number of Sick Days and Use of Cold and Flu Medication
For both groups, the participants “remained well” for majority of the study period. On average, participants reported to be “not sick” on 89.45% of the total study days. Findings from the ITT population showed a trend for fewer sick days in the RJ group, when compared to the placebo group (7.22 vs. 8.34 days, P = 0.056), which is due to the significantly fewer number of sick days reported in the RJ group compared to the placebo group from Day 43 to Day 84 (2.98 vs. 3.98 days, P = 0.011) (Figure 4). No significant difference in the average number of sick days between the RJ and placebo groups was observed in the PP population (7.13 vs. 7.92 days, P = 0.18). The number of sick days was similar between the study groups when stratified by severity (AUC 1–100: 4.39 vs. 5.31, P = 0.470; AUC>100: 12.74 vs. 17.85, P = 0.163), age (<45 years: 5.25 vs. 10.06, P = 0.174; ≥45 years: 8.17 vs. 6.50, P = 0.540), and sex (females: 6.43 vs. 8.73 days, P = 0.384; males: 8.53 vs. 5.50, P = 0.431). No difference in number of sick days was observed from Days −14 to −1 or −14 to 84 in the ITT and PP populations (P ≥ 0.123).
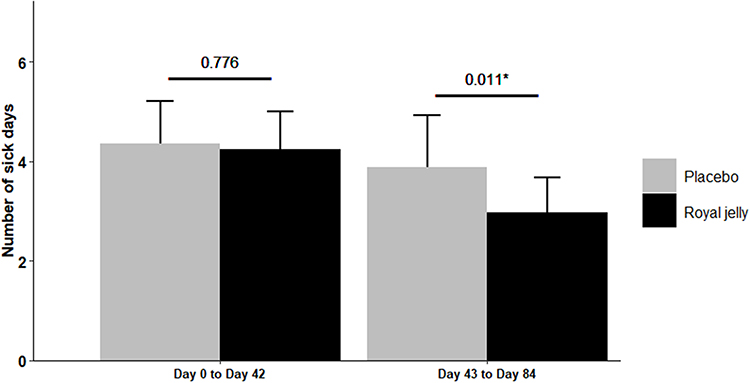 |
Figure 4 Average number of sick days in the ITT population (n=100) from Day 0 to 42 and Day 43 to 84. *Denotes a significant difference between the RJ and placebo groups; data are presented as mean ± standard error. |
Minimal use of prescription or non-prescription cold and flu medication was reported in both the RJ and placebo groups (Table 1). The proportion of participants in the ITT population using cold and flu medication was 8.16% and 18.75% in RJ and placebo groups, respectively (P = 0.147). In the PP population, 6.67% of participants in the RJ group and 15.00% of participants in the placebo group used cold and flu medications (P = 0.295). No difference in use of prescription medication or non-prescription cold and flu medication was observed from Days −14 to −1 or −14 to 84 in the ITT and PP populations (P ≥ 0.388).
Discussion
The safety and efficacy of RJ was investigated in this randomized, triple-blind, placebo-controlled, virtual clinical trial in healthy adults during the 2024–2025 North American cold and flu season. Daily supplementation for 98 days did not result in any serious adverse events, further supporting the safety profile of the study product.21 Given the high rate of compliance with the study product, the capsule form provides several advantages, such as delivering a pure, high potency product and serving as an appealing option for those who may be more selective about food tastes.
In the current study, the low incidence and severity of URTI symptoms reported throughout the study duration may have contributed to masking an observable effect of the study product on the frequency, severity, and duration of URTIs. The frequency of URTIs reported deviates from the trends observed in the respiratory virus surveillance report of influenza activity in Canada.22 When compared to Canadian surveillance report, it would have been expected that the data collection for the current study tracked with the upward trajectory of positive tests for influenza until the peak rate (27.6%) reported around mid- to late-February.22 Though the large proportion of participants remained well throughout the study duration, the notable significant differences in URTI symptoms between the RJ and placebo groups within the subgroup analysis (by severity and age) suggest a promising opportunity to identify differential effects of targeted groups to support the applicability of the findings and inform future directions. In particular, among those with reported higher severity of URTI symptoms and younger adults. Based on the significant reduction in the number of sick days observed in the latter phase of the study (Day 43 to Day 84), but not throughout the first 42 days, the exploratory finding suggests the potential delay in immune response may be of consideration for IP timing, as previously shown by Petelin et al (2019) using a similar dose of RJ.14 In the randomized, double-blind, placebo-controlled trial, RJ supplementation resulted in favorable changes in some antioxidant, anti-inflammatory, and hypolipidemic parameters at 8 weeks, but not at 4 weeks, in overweight adults aged 25 to 50 years.14
The wide spectrum of clinical presentation and time-course of URTIs lends to the importance of identifying strategies for managing URTIs to reduce the burden of infection. Previous studies have shown that the immune response is more engaged with a higher severity of infection. For example, in a sub study of the Southern Hemisphere Influenza Vaccine Efficacy Research and Surveillance (SHIVERS) study, the difference in cytokine profile of patients with mild and severe influenza was investigated in adults.23 Findings demonstrated differing immune response between mild and severe influenza, such as increased amounts of proinflammatory cytokines in more severe cases, compared to mild cases, as well as prolonged inflammation due to a delay in the peripheral immune activation.23 The differences in immune response may help explain the significant reduction in severity of URTI symptoms among those that reported an overall high severity of URTI symptoms, as the efficacy of the study product may have been amplified by a greater and balanced immune response. It is well established that the strength of the immune system is heavily influenced by age.24 In participants under 45 years of age, RJ supplementation demonstrated a significantly lower severity of coughs compared to the placebo group. The lack of significance of the RJ effect in older adults may be related to the lower severity of coughs reported. Of note, gender/sex-related differences in URTIs have been previously explained by differences in innate physiology, with females more susceptible to URTIs.25,26 In the present study, females tended to have a slightly higher frequency of incidence and greater severity of URTI, when compared to males. However, there was no significant sex-specific effect of the RJ supplementation, reinforcing the generalizability for using RJ as a strategy to manage URTI symptoms.
While investigation of potential mechanisms of action was beyond the scope of this trial, the health protective potential of RJ has been attributed to its anti-inflammatory and antioxidative properties that have been demonstrated in vitro, using animal models, and to a lesser extent, in human trials.27 In a recent systematic review and meta-analysis, the effect of RJ on inflammation and oxidative stress was examined in adults over 18 years of age.28 Pooled analysis of six randomized clinical trials demonstrated greater serum total antioxidant capacity and lower serum malondialdehyde, with pronounced effects observed with higher doses of RJ (≥3000 mg per day) and in non-diabetic individuals and those with normal BMI.28 Analysis for serum high sensitivity C-reactive protein could not be performed due to the limited number of eligible trials.28 Supplementation with RJ has also previously been shown to lower markers of low-grade systemic inflammation in overweight people,14 increase anti-inflammatory adipokines and serum total antioxidant potential as well as decrease markers of oxidative stress and inflammation in diabetic patients.29,30 Low-grade systemic inflammation is manifested as chronically elevated basal levels of inflammatory markers, most notable, among others, in people with chronic diseases, elderly, and overweight and obese people.31,32 These are the 3 most representative groups with documented higher risk for complications of URTI, due to dysregulated immune response. By lowering low-grade systemic inflammation, RJ might modulate immune response to URTIs and contribute to lower severity as well as decrease in duration of URTI symptoms and number of sick days, especially in higher risk groups.33,34 Altogether, several results show preliminary evidence of the influence of RJ on intrinsic antioxidant capacity, oxidative stress and immune modulation; but it is recognized that there is a need for trials with larger sample sizes to confirm these findings to help elucidate the mechanisms of action of RJ on immune health.
Interpretation of the study findings should consider the following limitations, including the low incidence and severity of URTIs reported, use of a single study site, and investigation over a single cold and flu season. As previously alluded to, a large proportion of participants remained well throughout the study duration, despite their history of URTI incidences at screening. With significantly fewer sick days among participants consuming the RJ supplementation in the latter phase of the study, compared to the placebo group, there is reason for further investigation of the efficacy of RJ over a longer study duration. The incidence rates in this study were relatively low compared to the ones used to estimate the statistical power, which significantly reduced the anticipated statistical power of this study. A larger sample size may be required to detect clinically meaningful differences under real-world seasonal conditions. Furthermore, to increase the probability of capturing a greater number of incidents and higher severity of URTI symptoms, it may be advantageous for future trials to implement recruitment strategies that span a wide geographical location (eg., multicenter study) and over multiple cold and flu seasons.
Conclusion
In conclusion, RJ supplementation was safe and well tolerated in healthy adults. The low incidence of URTIs over the 84-day study period may have masked potential effects of RJ supplementation on the frequency, severity, and duration of URTIs. However, exploratory findings suggested its potential use for mitigating the severity of some URTI symptoms and decreasing the number of sick days within targeted groups, particularly amongst those reporting a higher severity of symptoms. Further investigation in adequately powered studies is warranted to confirm these findings within targeted groups to understand the role of RJ for supporting immune health, including URTI prevention and relief of related symptom(s). The implications of this research can help provide evidence-based information for determining natural, non-pharmaceutical approaches to managing URTIs in healthy adults.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved on October 4, 2024, by the Institutional Review Board Advarra (Aurora, Ontario; Pro00080103).
Abbreviations
AE, adverse event; AUC, area under the curve; CONSORT, Consolidated Standards of Reporting Trials; ET, Early Termination; GCP, Good Clinical Practice; ICH, International Council for Harmonization of Technical Requirements for Pharmaceuticals for Human Use; IP, investigational product; ITT, intention-to-treat; PP, per protocol; RJ, royal jelly; SD, standard deviation; URTI, upper respiratory tract infection; WURSS-24, Wisconsin Upper Respiratory Symptom Survey-24.
Data Sharing Statement
The data presented in this study is not available due to privacy or ethical restrictions.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research and the APC were funded by Medex d.o.o.
Disclosure
J.Y., D.C., N.G., E.L., and M.M are employed by the company KGK Science Inc. R.K. is employed by the company Medex d.o.o. The authors declare that this study received funding from Medex d.o.o. The funder had no role in the collection, analyses, or interpretation of data.
The investigational product (Bio Gelee Royale Forte; Medex d.o.o, Ljubljana, Slovenia) is commercially available. The authors report no other conflicts of interest in this work.
References
1. Sirota SB, Doxey MC, Dominguez RMV, et al. Global, regional, and national burden of upper respiratory infections and otitis media, 1990–2021: a systematic analysis from the Global Burden of Disease Study 2021. Lancet Infect Dis. 2025;25(1):36–13. doi:10.1016/S1473-3099(24)00430-4
2. Eccles R. Common cold. Front Allergy. 2023;4:1224988. doi:10.3389/falgy.2023.1224988
3. Witek TJ, Ramsey DL, Carr AN, Riker DK. The natural history of community-acquired common colds symptoms assessed over 4-years. Rhinol J. 2015;53(1):81–88. doi:10.4193/Rhino14.149
4. Molinari N-AM, Ortega-Sanchez IR, Messonnier ML, et al. The annual impact of seasonal influenza in the US: measuring disease burden and costs. Vaccine. 2007;25(27):5086–5096. doi:10.1016/j.vaccine.2007.03.046
5. Fendrick AM, Monto AS, Nightengale B, Sarnes M. The economic burden of non–influenza-related viral respiratory tract infection in the United States. Arch Intern Med. 2003;163(4):487–494. doi:10.1001/archinte.163.4.487
6. van Driel ML, Scheire S, Deckx L, Gevaert P, De Sutter A. What treatments are effective for common cold in adults and children? BMJ. 2018;363:k3786. doi:10.1136/bmj.k3786
7. Health Canada. Consumer information for: advil pain & head cold night. 2025. Available from: https://dhpp.hpfb-dgpsa.ca/dhpp/resource/85459/consumer-information.
8. Ahmad S, Campos MG, Fratini F, Altaye SZ, Li J. New insights into the biological and pharmaceutical properties of royal jelly. Int J Mol Sci. 2020;21(2):382. doi:10.3390/ijms21020382
9. Guo J, Wang Z, Chen Y, et al. Active components and biological functions of royal jelly. J Funct Foods. 2021;82:104514. doi:10.1016/j.jff.2021.104514
10. Münstedt K, Bargello M, Hauenschild A. Royal jelly reduces the serum glucose levels in healthy subjects. J Med Food. 2009;12(5):1170–1172. doi:10.1089/jmf.2008.0289
11. Morita H, Ikeda T, Kajita K, et al. Effect of royal jelly ingestion for six months on healthy volunteers. Nutr J. 2012;11(1):77. doi:10.1186/1475-2891-11-77
12. Hadi A, Najafgholizadeh A, Aydenlu ES, et al. Royal jelly is an effective and relatively safe alternative approach to blood lipid modulation: a meta-analysis. J Funct Foods. 2018;41:202–209. doi:10.1016/j.jff.2017.12.005
13. Chiu H-F, Chen B-K, Lu -Y-Y, et al. Hypocholesterolemic efficacy of royal jelly in healthy mild hypercholesterolemic adults. Pharm Biol. 2017;55(1):497–502. doi:10.1080/13880209.2016.1253110
14. Petelin A, Kenig S, Kopinč R, Deželak M, Černelič Bizjak M, Jenko Pražnikar Z. Effects of royal jelly administration on lipid profile, satiety, inflammation, and antioxidant capacity in asymptomatic overweight adults. Evid Based Complement Alternat Med. 2019;2019:1–11. doi:10.1155/2019/4969720
15. Moher D, Hopewell S, Schulz KF, et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. Int J Surg. 2012;10(1):28–55. doi:10.1016/j.ijsu.2011.10.001
16. Efird J. Blocked randomization with randomly selected block sizes. Int J Environ Res Public Health. 2010;8(1):15–20. doi:10.3390/ijerph8010015
17. Barrett B, Brown RL, Mundt MP, et al. Validation of a short form Wisconsin Upper Respiratory Symptom Survey (WURSS-21). Health Qual Life Outcomes. 2009;7(1):76. doi:10.1186/1477-7525-7-76
18. Murdoch DR, Slow S, Chambers ST, et al. Effect of vitamin D 3 supplementation on upper respiratory tract infections in healthy adults. JAMA. 2012;308(13):1333. doi:10.1001/jama.2012.12505
19. Evans M, Falcone PH, Crowley DC, et al. Effect of a Euglena gracilis fermentate on immune function in healthy, active adults: a randomized, double-blind, placebo-controlled trial. Nutrients. 2019;11(12):2926. doi:10.3390/nu11122926
20. Dharsono T, Rudnicka K, Wilhelm M, Schoen C. Effects of yeast (1,3)-(1,6)-beta-glucan on severity of upper respiratory tract infections: a double-blind, randomized, placebo-controlled study in healthy subjects. J Am Coll Nutr. 2019;38(1):40–50. doi:10.1080/07315724.2018.1478339
21. Health Canada. Monograph - Royal Jelly. 2018. Available from: https://webprod.hc-sc.gc.ca/nhpid-bdipsn/atReq?atid=gelee.royal.jelly3&lang=eng.
22. Government of Canada. Canadian respiratory virus surveillance report: overview of key trends in influenza (flu) activity in Canada. 2025. Available from: https://health-infobase.canada.ca/respiratory-virus-surveillance/influenza.html.
23. Wong -S-S, Oshansky CM, Guo X-ZJ, et al. Severe influenza is characterized by prolonged immune activation: results from the SHIVERS COHORT STUDY. J Infect Dis. 2018;217(2):245–256. doi:10.1093/infdis/jix571
24. Yu W, Yu Y, Sun S, et al. Immune alterations with aging: mechanisms and intervention strategies. Nutrients. 2024;16(22):3830. doi:10.3390/nu16223830
25. McClelland EE, Smith JM. Gender specific differences in the immune response to infection. Arch Immunol Ther Exp. 2011;59(3):203–213. doi:10.1007/s00005-011-0124-3
26. Falagas ME, Mourtzoukou EG, Vardakas KZ. Sex differences in the incidence and severity of respiratory tract infections. Respir Med. 2007;101(9):1845–1863. doi:10.1016/j.rmed.2007.04.011
27. Botezan S, Baci G-M, Bagameri L, Pașca C, Dezmirean DS. Current status of the bioactive properties of royal jelly: a comprehensive review with a focus on Its anticancer, anti-inflammatory, and antioxidant effects. Molecules. 2023;28(3):1510. doi:10.3390/molecules28031510
28. Taheri S, Bahari H, Mirzavi F, et al. Effects of royal jelly consumption on inflammation and oxidative stress: a systematic review and meta-analysis of randomized controlled trials. Avicenna J Phytomed. 2024. doi:10.22038/ajp.2024.25139
29. Pourmoradian S, Mahdavi R, Mobasseri M, Faramarzi E, Mobasseri M. Effects of royal jelly supplementation on glycemic control and oxidative stress factors in type 2 diabetic female: a randomized clinical trial. Chin J Integr Med. 2014;20(5):347–352. doi:10.1007/s11655-014-1804-8
30. Maleki V, Jafari-Vayghan H, Saleh-Ghadimi S, Adibian M, Kheirouri S, Alizadeh M. Effects of royal jelly on metabolic variables in diabetes mellitus: a systematic review. Complement Ther Med. 2019;43:20–27. doi:10.1016/j.ctim.2018.12.022
31. Furman D, Campisi J, Verdin E, et al. Chronic inflammation in the etiology of disease across the life span. Nat Med. 2019;25(12):1822–1832. doi:10.1038/s41591-019-0675-0
32. Timar R, Timar B, Degeratu D, Serafinceanu C, Oancea C. Metabolic syndrome, adiponectin and proinflammatory status in patients with type 1 diabetes mellitus. J Int Med Res. 2014;42(5):1131–1138. doi:10.1177/0300060514541829
33. Martono M, Fatmawati F, Mulyanti S. Risk factors associated with the severity of COVID-19. Malays J Med Sci MJMS. 2023;30(3):84–92. doi:10.21315/mjms2023.30.3.7
34. Zsichla L, Müller V. Risk factors of severe COVID-19: a review of host, viral and environmental factors. Viruses. 2023;15(1):175. doi:10.3390/v15010175
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.