Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
A Randomized Controlled Comparative Study of the Three Over-Bed Techniques for Positioning and Repositioning the Lithotomy Position While Using Stirrups
Authors Zhang LL, Luo ZF, Yang GJ
Received 15 September 2023
Accepted for publication 11 December 2023
Published 27 December 2023 Volume 2023:16 Pages 4255—4264
DOI https://doi.org/10.2147/JMDH.S435570
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Ling-Ling Zhang,1,2 Zhi-Fang Luo,2 Guang-Jing Yang1,3
1Hunan University of Chinese Medicine, Hunan, People’s Republic of China; 2Department of Operating Room, Chongqing Traditional Chinese Medicine Hospital, Chongqing, People’s Republic of China; 3Department of Nursing, Chongqing Traditional Chinese Medicine Hospital, Chongqing, People’s Republic of China
Correspondence: Guang-Jing Yang, Department of Nursing, Chongqing Traditional Chinese Medicine Hospital, No. 6, Seven Branch Road, Panxi, Jiangbei District, Chongqing, 400021, People’s Republic of China, Tel +86-15998951588, Email [email protected]
Objective: In this study, the clinical application and efficacy of three different methods for placing and repositioning patients in the lithotomy position over the bed using stirrups were evaluated.
Methods: A total of 240 surgical patients who underwent surgery in Chongqing Traditional Chinese Medicine Hospital between July and November 2022 were selected as study participants. Using envelopes, they were randomly divided into three groups of 80 cases each using a randomization method. The groups included the traditional over-bed method, the postural trolley-assisted over-bed method, and the direct over-bed method. Using the Kruskal–Wallis rank-sum test, analysis of variance, and multiple linear regression equations, the placement time, over-bed repositioning time, and total time of the three methods for placing and repositioning in the lithotomy position supported by stirrups were analyzed statistically. In addition, we investigated and examined the satisfaction of nurses and doctors with the aforementioned techniques.
Results: The placement time, repositioning time, and total time were significantly higher for the traditional over-bed method than for the postural trolley-assisted over-bed method and the direct over-bed method (both P < 0.01). However, there was no statistically significant difference between the postural trolley-assisted over-bed method and the direct over-bed method (P > 0.05). Nurses and doctors reported significantly higher satisfaction with the postural trolley-assisted over-bed method and the direct over-bed method compared to the traditional over-bed method (both P < 0.01). In addition, nurses were more satisfied with the direct over-bed method than the postural trolley-assisted over-bed method (P < 0.05).
Conclusion: The results of this study demonstrate that the direct over-bed method is preferred for positioning and repositioning patients in the lithotomy position with the support of stirrups.
Keywords: lithotomy position, position placement, postural trolley, repositioning over bed, stirrup
Introduction
The lithotomy position is a commonly used position in clinical surgery, and it is often employed in perineal, urethral, and bladder surgeries.1,2 Although this position can provide a wider field of vision, improper placement can increase the risk of various postoperative complications. These complications may include peroneal nerve injury, deep vein thrombosis in the lower extremities, calf compartment syndrome, pain and numbness, and even motor disorders.3,4 With the advancement of medical technology and the increasing focus on the well-being of surgical patients, the lithotomy position with stirrup support is being used more frequently in clinical practice.5 The stirrup provides greater comfort to the patient compared to the traditional lithotomy leg support. Additionally, it reduces the workload for nurses and allows for more precise positioning.6
It takes time and physical strength to reposition the patient in the lithotomy position and move them across the bed. Finding ways to simplify operations and save time and energy is always a goal in clinical work. In this study, we investigated the common methods used for placing and repositioning patients in the lithotomy position in the operating room of a large hospital in Chongqing. We combined the three methods available to determine which method is easier and faster for transferring a patient across the bed.
Data and Methods
General Data
Participants in this study included 240 patients who were admitted to the Chongqing Traditional Chinese Medicine Hospital between July 2022 and November 2022 and underwent elective surgical treatment in the lithotomy position. Participants between the ages of 18 and 65 with no significant cardiopulmonary disease and willingness to participate were eligible for this study. Individuals with a history of lower limb malformation, lower limb dysfunction, or lower limb thrombosis were excluded. Furthermore, those with severe osteoporosis and those who had recently undergone lower extremity surgery accompanied by lower extremity edema or phlebitis were also excluded from the study. In this study, the were used for random grouping in a 1:1:1 ratio. The patients were divided into three groups: the traditional bed-over method, the postural trolley-assisted bed-over method, and the direct bed-over method. Each group consisted of 80 cases. The specific grouping method was as follows: 240 patients to be enrolled were coded as 001–240 according to the enrollment time, and 240 random numbers were intercepted starting from any position in the random number table, and the obtained numbers were sent to 240 patients in turn. Then divide the number of patients by 3, and the group with a remainder of 0 was group A, the group with a remainder of 1 was group B, and the group with a remainder of 2 was group C. The results were put into sealed envelopes. The grouping process was completed by a third party without the participation of the researcher. The grouping envelopes were given to the traveling nurse to open before the operation.
The traditional bed-over method required disassembling and installing the operating bed leg plate in order to place and reposition the bed. The postural trolley-assisted bed transfer method involved the placement and repositioning of the bed with the assistance of a postural trolley. The direct bed-over method entails directly adjusting the foot pedal and support rod to place and reposition the bed. In all three groups, stirrups were utilized for the lithotomy position. Surgery included hysteroscopic surgery, laparoscopic ovarian cyst removal, laparoscopic myomectomy, laparoscopic salpingectomy, laparoscopic total hysterectomy, laparoscopic tubal ligation, laparoscopic right hemicolectomy, transurethral ureteroscope double J-tube insertion or removal, and lithotripsy.
Methods
After entering the operating room, the patients were positioned horizontally on the surgical bed. Their trousers were removed and leg restraints were affixed. The legs of the patients were positioned on the stirrups using the stirrup-type leg supports that were appropriately adjusted to meet the surgical requirements. Following their secure fastening with a fixation belt, the end plate of the bed was subsequently detached, thereby completing the lithotomy position. The patients subsequently transitioned from the lithotomy position to the horizontal supine position after the surgical procedure was completed. This transition is commonly referred to as positional repositioning. The leg restraints were removed and the patients were dressed. The transfer bed was raised to the same height as the surgical bed and secured in place using brakes. The anesthesiologists were advised to support the head and shoulders of the patients, while two additional staff members assisted in turning the patients’ body cautiously. The shoulders and hips were supported by one member of the staff, while the legs were supported by the other, while guiding the movement in the desired direction. After the patients were turned onto their side, the receiving staff member would place a pad underneath the patients, and they would then be gently laid flat and moved onto the transfer bed using the combined efforts of all staff members. The trolley stopper was secured prior to repositioning of the patients from the lithotomy position onto the bed, to ensure stability.
Traditional Over-Bed Method
The foot end of the surgical bed was replaced with the foot plate of the surgical bed. Prior to the surgery, the foot plate of the surgical bed was removed after placing the stirrups in the lithotomy position. The foot plate of the surgical bed was then installed to facilitate postoperative positional repositioning. Then, the stirrups and the leg support clips were removed, to transition the patients to the bed (Figure 1).
 |
Figure 1 Traditional over-bed method. Placement—(A): Install stirrup legs and positioning; (B): Remove the foot plate. Repositioning—(C): Install the foot plate; (D): Flat one’s legs and repositioning; (E): Remove stirrup leg. Transition to the bed—(F): Transition to the bed. |
Postural Trolley-Assisted Over-Bed Method
The postural trolley was used at the foot of the surgical bed. The postural trolley was removed after positioning the patients in the lithotomy position and securing their feet in the stirrups prior to the surgery. After the surgery, the postural trolley was positioned between the two leg supports and securely attached to the surgical bed in order to perform postural repositioning on the bed (Figure 2).
 |
Figure 2 Postural trolley-assisted over-bed method. Placement—(A): Place the postural trolley; (B): Positioning the patients in the lithotomy position; (C): Remove the postural trolley. Repositioning—(D): Place the postural trolley and repositioning; (E): Flat one’s legs. Transition to the bed—(F): Transition to the bed. |
Direct Over-Bed Method
Leg supports of the stirrup variety were utilized at the end of the surgical bed. They were adjusted according to the surgical requirements prior to the surgery. After surgery, the stirrups and the support rod were aligned with the edge of the bed by using the adjusting handle (grip-rotate-release). This enabled the patients’ legs to be aligned and straightened, which facilitated smooth movement across the bed (Figure 3).
 |
Figure 3 Direct over-bed method. Placement—(A): Leg supports of the stirrup variety were utilized at the end of the surgical bed; (B): Positioning. Repositioning—(C): Adjusting handle directly to Reposition; Transition to the bed—(D): Transition to the bed. |
Evaluation Indicators
Time Measurement
A timer was used to record the amount of time required to place and reposition each patient over the bed using the stirrups. The time it takes to successfully position the patient from the horizontal position to the stirrup lithotomy position is called the placement time. Repositioning time is the time required to relocate the patient from the stirrup lithotomy position to the transfer bed after surgery. The total time is the sum of the placement time and the repositioning time.
Evaluation of Satisfaction
Based on the satisfaction evaluation method developed by Li et al,7 combined with the subjective preference of undergraduate doctors and nurses for the placement and repositioning of the three-over-bed method for stirrup lithotomy position, the evaluation was carried out from five aspects: convenience of operation, safety of operation for patients, labor intensity of operation, feasibility of operation, and waiting time for surgery. The researchers collected and evaluated the scores of each item on the postoperative site, and calculated the sum of the scores of each item. Classify more satisfactory and satisfactory as satisfactory (Table 1).
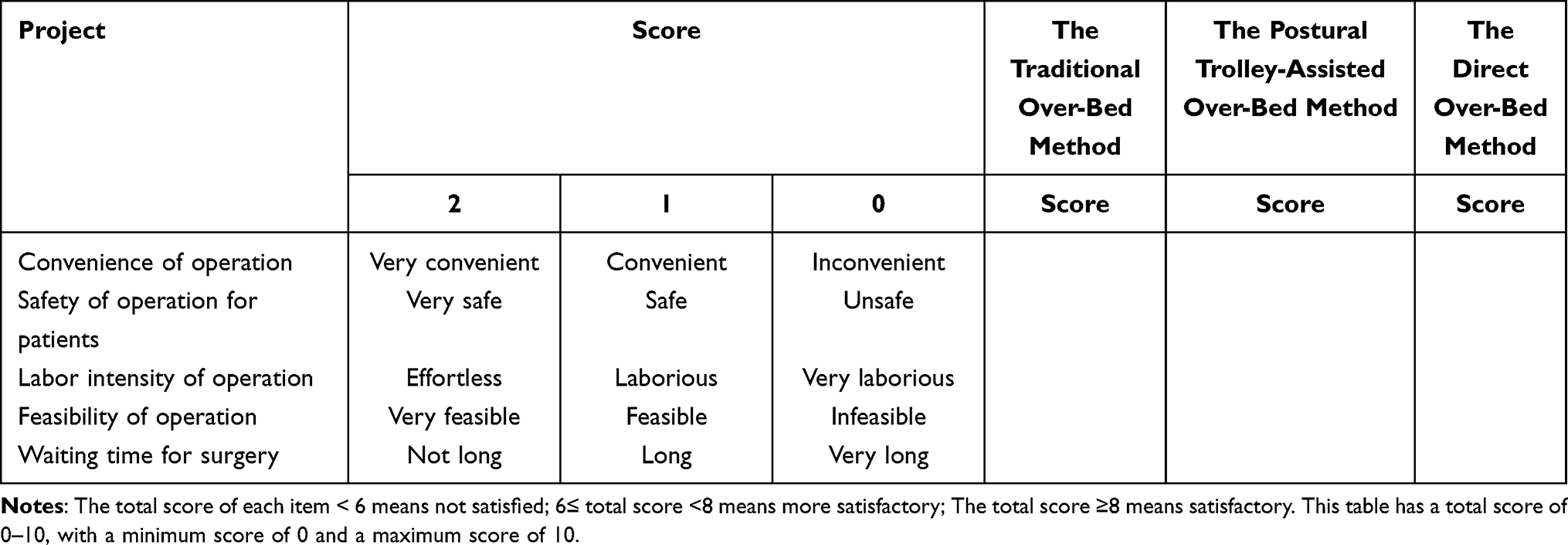 |
Table 1 The Questionnaire of the Placement and Repositioning of the Three-Over-Bed Method for Stirrup Lithotomy Position |
Statistical Methods
SPSS 23.0 statistical software was used for data analysis. The normal distribution of measurement data are expressed as mean ± standard deviation. An analysis of variance (ANOVA) was used to compare multiple groups. Non-normally distributed, variance-independent measurement data are expressed as the median (interquartile range). The Kruskal–Wallis rank-sum test was utilized for inter-group comparisons. Statistical multifactorial analyses were conducted using multivariate linear regression. Counting data were analyzed using the chi-squared test or Fisher’s method. Differences were considered statistically significant at P < 0.05.
Results
General Patient Information
The gender, age, surgical catheter, and body mass index (BMI) of the 240 patients are summarized in Table 2.
 |
Table 2 General Patient Information (n=240) |
Comparison of the General Patient Information Using the Three Over-Bed Methods for the Placement and Repositioning of the Stirrup Lithotomy Position
As indicated in Table 3, there was no statistically significant difference between the three groups of patients in terms of gender, age, surgical catheter, or BMI (P > 0.05).
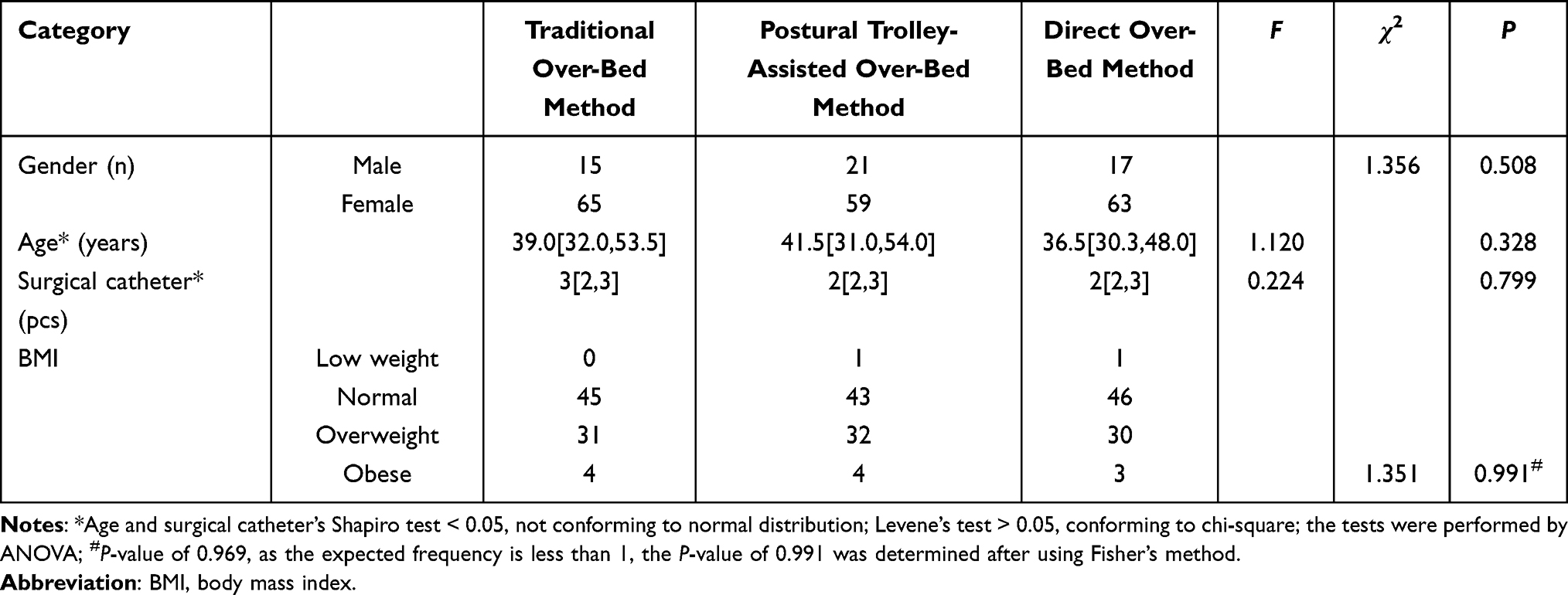 |
Table 3 Comparison of Gender, Age, Surgical Catheters, and BMI Among the Three Groups |
Comparison of the Placement Time, Repositioning Time, and Total Time for the Placement and Repositioning of the Stirrup Lithotomy Position Using the Three Over-Bed Methods
The differences between the three methods in terms of placement time, repositioning time, and total time were statistically significant (all P < 0.01). Using the Dunnett-t two-by-two comparison method, the traditional over-bed method demonstrated significantly longer placement time, repositioning time, and total time compared to both the postural trolley-assisted over-bed method and the direct over-bed method (both P < 0.01). However, there was no statistically significant difference between the postural trolley-assisted over-bed method and the direct over-bed method for placement time, repositioning time, or total time (P > 0.05, as shown in Table 4).
 |
Table 4 Differences Between the Three Methods of Placement Time, Repositioning Time, and Total Time |
Multifactorial Analysis of the Placement Time, Repositioning Time, and Total Time for the Placement and Repositioning of the Stirrup Lithotomy Position Using Three Over-Bed Methods
Sex, age, surgical catheter, and BMI were used as independent variables, while the three methods of placement time, repositioning time, and total time were used as dependent variables. The results of a linear regression analysis indicated that the number of surgical catheters had a significant impact on the repositioning time and total time of the three methods (P < 0.05). These findings are presented in Table 5 and Table 6.
 |
Table 5 Linear Regression Analysis of Reposition Time for the Three Methods |
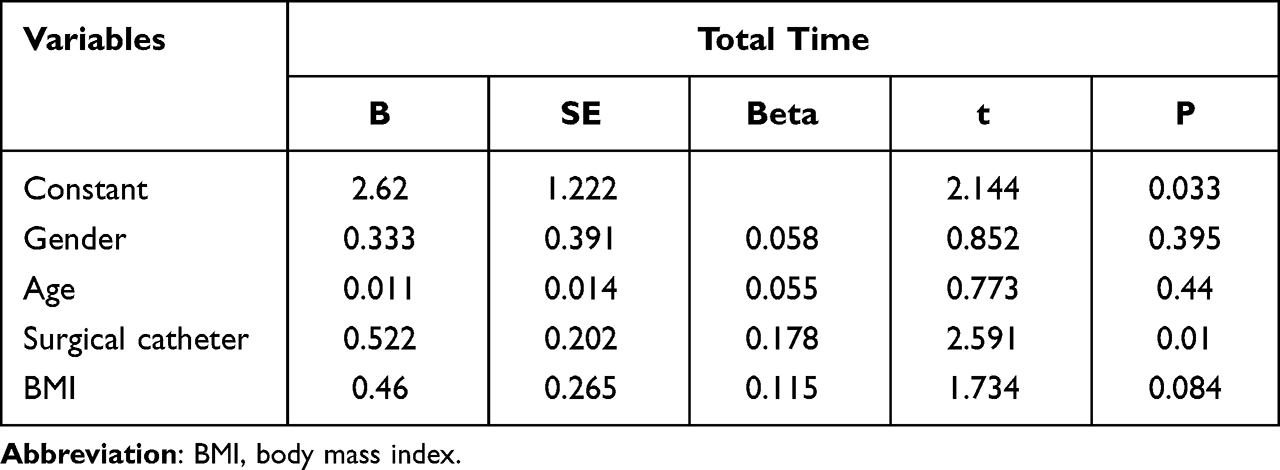 |
Table 6 Linear Regression Analysis of Total Time for the Three Methods |
Satisfaction of Nurses and Doctors with the Three Methods
In this study, 16 nurses and 12 doctors participated. Both nurses and doctors reported higher satisfaction with the postural trolley-assisted over-bed method and the direct over-bed method compared to the traditional over-bed method (both P < 0.01). Furthermore, using the Dunnett-t two-by-two comparison method, it was discovered that nurses were more satisfied with the direct over-bed method than the postural trolley-assisted over-bed method (P < 0.05). These findings are presented in Table 7.
 |
Table 7 Nurse and Physician Satisfaction with the Three Methods |
Discussion
The development of minimally invasive surgery in China is primarily attributable to its ability to minimize trauma and expedite postoperative recovery. Although frequently used in surgical procedures, the lithotomy position carries the potential for various complications, including lower extremity venous thrombosis, nerve damage, and pressure injuries.3,8,9 As a result, the use of stirrups is increasingly favored due to their enhanced safety and convenience.10 Consequently, their application in clinical context is widespread.11 Therefore, enhancing the efficiency of the operating room and accelerating turnaround times are essential for maximizing hospital and social benefits.12 In this study, we aimed to analyze the utilization of three different over-bed methods for the stirrup lithotomy position, adhering to the principles of effective and feasible process development and meticulous control of each step to enhance efficiency. The objective was to determine the approach that clinical staff preferred.
The results of this study revealed that the placement time, repositioning time, and total time for the traditional over-bed method were significantly longer than for the postural trolley-assisted over-bed method and the direct over-bed method (both P < 0.01). However, there were no statistically significant differences between the postural trolley-assisted over-bed method and the direct over-bed method in terms of placement time, repositioning time, or total time (P > 0.05). The results were similar to those of the study by Dong et al.13 The rationale behind this phenomenon could be attributed to the conventional technique of the over-bed method, which requires the use of stirrup-type leg supports and fixation clips, as well as the placement and readjustment of the bed. The aforementioned procedure is characterized by its time-consuming and tedious nature. The postural trolley-assisted over-bed method involves a simple process of adjusting the body position and then removing the postural trolley. Using the handle, the bed can be adjusted to attain the desired body position. The setup process is characterized by its simplicity and efficiency. In all aspects, the traditional method is consequently more time-consuming than the trolley-assisted and direct methods. Although, as short as a few minutes is insignificant for the operation time of several hours, in actual work, efficient and rapid positioning and repositioning can effectively save the time between operations, save the physical energy of medical staff, and greatly improve the satisfaction of medical staff. This is of great benefit to improving work efficiency.
The multifactorial analysis revealed that the number of surgical catheters significantly impacted both the repositioning over-bed time and the total time of the three methods (P < 0.05). In order to minimize the risk of unintended pressure, displacement, or dislodgement, healthcare professionals must organize and identify the names and positions of different catheters. This is essential for maintaining the unobstructed performance of the tubes. Consequently, the repositioning time of the patient was prolonged, resulting in an increase in the total time. Furthermore, in this study, we found that BMI had no significant influence on the repositioning time or total time of the three methods (P > 0.05). This phenomenon may be attributable to the limited representation of underweight and obese individuals within the sample population of this study, thereby potentially influencing the outcomes.
Nurses and doctors were significantly more satisfied with the postural trolley-assisted over-bed method and the direct over-bed method than they were with the traditional over-bed method (both P < 0.01). In addition, nurses were more satisfied with the direct over-bed method compared to the postural trolley-assisted over-bed method (P < 0.05). The rationale behind this phenomenon can be attributed to the following factors: (1) The direct over-bed method provides greater convenience in terms of positioning compared to the traditional over-bed method. This strategy effectively preserves the physical stamina of the nurse diminishes the duration of preoperative waiting, and substantially enhances both work productivity and medical staff satisfaction.14 This technique offers significant benefits in the fields of gynecology and urology, particularly when performing brief surgical procedures. (2) The direct over-bed method has a smaller interval with the trolley in comparison to the postural trolley-assisted over-bed method, allowing for more efficient movement. In addition, it occupies less space in the operating room, which is especially beneficial in small operating rooms.
Conclusion
In conclusion, the stirrup lithotomy position placement and repositioning, as well as the postural trolley-assisted over-bed method and the direct over-bed method, are efficient and easy to use. These methods facilitate the positioning of the surgical table and increase the satisfaction of medical staff, thereby enhancing work efficiency. However, this study has several limitations. For instance, although the satisfaction survey combines the literature and the preference degree of undergraduate medical staff, in general, the reliability and validity verification is needed to better reflect the satisfaction of medical staff. At the same time, the effects of height, weight, and other factors on the time it took for the three groups to cross the bed were not investigated. Furthermore, in this study, the waiting order for receiving patients and surgical methods, among other factors, were not accurately categorized, which could have influenced the results of the three groups. In future research, it is important to investigate the influence of multiple variables on the amount of time required to move the patient over the bed.
Data Sharing Statement
The datasets used or analysed during the current study available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the declaration of Helsinki. This study was conducted with approval from the Ethics Committee of Chongqing traditional Chinese medicine Hospital. A written informed consent was obtained from all participants.
Acknowledgments
We are particularly grateful to all the people who have given us help on our article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
None of the authors have any financial disclosure or conflict of interest.
References
1. Hara K, Kuroda H, Matsuura E, et al. Underbody blankets have a higher heating effect than overbody blankets in lithotomy position endoscopic surgery under general anesthesia: a randomized trial. Surg Endosc. 2022;36(1):670–678. doi:10.1007/s00464-021-08335-y
2. Kumar P, Mishra TS, Sarthak S, Sasmal PK. Lithotomy versus prone position for perianal surgery: a randomized controlled trial. Ann Coloproctol. 2022;38(2):117–123. doi:10.3393/ac.2020.12.16
3. Kajitani R, Minami M, Kubo Y, et al. Intraoperative pressure monitoring of the lower leg for preventing compression-related complications associated with the lithotomy position. Surg Endosc. 2022;36(8):5873–5881. doi:10.1007/s00464-021-08921-0
4. Sajid MS, Shakir AJ, Khatri K, Baig MK. Lithotomy-related neurovascular complications in the lower limbs after colorectal surgery. Colorectal Dis. 2011;13(11):1203–1213. doi:10.1111/j.1463-1318.2010.02314.x
5. Whitis AM, Chen E, Sekhon M, Akella S, Bradley CS, Kowalski JT. Postoperative lower extremity neuropathy with boot stirrups compared with candy cane stirrups. Obstet Gynecol. 2021;137(5):916–923. doi:10.1097/AOG.0000000000004353
6. Gupta A, Meriwether K, Tuller M, et al. Candy cane compared with boot stirrups in vaginal surgery: a randomized controlled trial. Obstet Gynecol. 2020;136(2):333–341. doi:10.1097/AOG.0000000000003954
7. Li XL, Tang JN, Zhu YM, Qin J, Jiang WL. Application of improved ”humanoid” posture in gynecological laparoscopic surgery. J Nurs. 2019;34(7):39–41.
8. Bjøro B, Mykkeltveit I, Rustøen T, Candas Altinbas B, Røise O, Bentsen SB. Intraoperative peripheral nerve injury related to lithotomy positioning with steep Trendelenburg in patients undergoing robotic-assisted laparoscopic surgery - A systematic review. J Adv Nurs. 2020;76(2):490–503. doi:10.1111/jan.14271
9. Hara K, Kuroki T, Kaneko S, et al. Prevention of well-leg compartment syndrome following lengthy medical operations in the lithotomy position. Surg Open Sci. 2020;3:16–21. doi:10.1016/j.sopen.2020.10.001
10. Sze EHM; Sze EHM. An alternate approach to using candy cane stirrups in vaginal surgery. Obstet Gynecol. 2019;133(4):666–668. doi:10.1097/AOG.0000000000003184
11. Negash S, Anberber E, Ayele B, et al. Operating room efficiency in a low resource setting: a pilot study from a large tertiary referral center in Ethiopia. Patient Saf Surg. 2022;16(1):3. doi:10.1186/s13037-021-00314-5
12. Umali MIN, Castillo TR. Efficiency of operating room processes for elective cataract surgeries done by residents in a National University Hospital. Clin Ophthalmol. 2020;14:3527–3533. doi:10.2147/OPTH.S277550
13. Dong D, Shao J. The application of a stirrup posture frame placement and lithotomy position in surgical room posture nursing for patients with giant uterine fibroids. Med theo pract. 2022;35(17):3014–3016.
14. Sun LZ, Guo TT. The application effect of stirrup shaped multifunctional leg rest in laparoscopic endometrial cancer surgery. Chinese And Foreign Medical Research. 2022;20(23):160–164.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.