Back to Journals » Patient Preference and Adherence » Volume 17
A Qualitative Study on Patients’ Views on Hypertension and Antihypertensive Medications
Authors Malkon S, Wettermark B ![]() , Kahan T, Bastholm-Rahmner P, Hasselström J, Qvarnström M
, Kahan T, Bastholm-Rahmner P, Hasselström J, Qvarnström M
Received 8 July 2023
Accepted for publication 26 October 2023
Published 13 December 2023 Volume 2023:17 Pages 3331—3339
DOI https://doi.org/10.2147/PPA.S429638
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Salpe Malkon,1 Björn Wettermark,1 Thomas Kahan,2 Pia Bastholm-Rahmner,3 Jan Hasselström,4 Miriam Qvarnström1
1Department of Pharmacy, Uppsala University, Uppsala, Sweden; 2Karolinska Institutet, Department of Clinical Sciences, Danderyd Hospital, Division of Cardiovascular Medicine, Stockholm, Sweden; 3Department of Laboratory Medicine, Karolinska Institutet, Stockholm, Sweden; 4Department of Neurobiology and Care Sciences and Society, Karolinska Institutet, Stockholm, Sweden
Correspondence: Miriam Qvarnström, Department of Pharmacy, Faculty of Pharmacy, Uppsala University, Box 580, Uppsala, 751 23, Sweden, Email [email protected]
Purpose: Few studies explored what patients initiated on blood pressure medication in primary care think about their disease and their medications. The aim of this study was to gain an understanding of hypertensive patients’ views on and experiences of hypertension and the use of antihypertensive medications.
Methods: A qualitative study based on open-ended questions from a survey on medication adherence, which captured treated hypertensive patients’ perspective on their condition and treatment. Data were collected for 219 patients on antihypertensive medication, ≥ 30 years old, who consulted 25 primary health care centers in Stockholm, Sweden, during 2016. Thematic analysis with both inductive and deductive approach was applied.
Results: We identified 21 codes from the data and grouped them under the World Health Organization’s five dimensions of adherence: condition-, therapy-, health care team and system-, patient-, and socioeconomic-related factors. The analyses revealed that many patients with hypertension have limited knowledge of their disease, are afraid of drug side effects and experience various issues in primary health care that may negatively impact adherence, including short doctor appointments, prescribing without communication and room for improvement in individualization of therapy and a person-centered approach.
Conclusion: Many patients with hypertension have limited understanding of their hypertension and fear of adverse events from their antihypertensive medications. There is also room for improvement in how the patients are managed in primary health care. Interventions should focus on these issues to promote a better blood pressure target achievement.
Plain Language Summary: Few studies have explored what patients initiated on blood pressure medication in primary care think about their disease and their medications.In this study, we analyzed free comments collected from 219 patients responding to a survey on medication adherence. Those who responded used antihypertensive medication, were ≥ 30 years old, and consulted primary health care centers in Stockholm, Sweden.The analyses revealed that many patients with hypertension have limited knowledge of their disease, are afraid of drug side effects and experience various issues in primary health care that may negatively impact adherence, including short doctor appointments, prescribing without communication and room for improvement in individualization of therapy and a person-centered approach.Interventions to promote a better blood pressure treatment would likely benefit from targeting these problems raised by patients.
Keywords: hypertension, antihypertensive treatment, medication adherence, patient perspectives, primary health care, qualitative studies
Introduction
Although guidelines for the management of arterial hypertension emphasize the importance of detection, treatment, and blood pressure control, a majority of patients with hypertension remains uncontrolled.1 This may be explained by a range of barriers related to the patient, the health care provider, or the health care system.2,3 Two major factors contribute to hypertension control in treated patients: Prescription of an adequate number of medications, and patient adherence to the therapy.4 Sadly, many studies show a substantial room for improvement, and many patients discontinue their treatment early after initiation.4,5
Research in medication adherence divides the concept into three different components: initiation (the patient starting to take the first dose of their prescribed medication), implementation (taking the medication in the right time, dose and frequency as intended to the prescription), and persistence (a measure of how long the patient is on treatment, ie, the time from initiation to completion of treatment).6 Adherence can be affected by various factors, and the World Health Organization considers adherence as multidimensional with five themes related to the patient, the condition, socioeconomy, therapy, and the health care team and system.7
There is limited data with a patient perspective on challenges reaching target blood pressures,8 but a recent systematic review reported patients’ symptoms after diagnosis of hypertension, many of which that thought to be related to the patients’ discontinuation of medication.9 To further increase our understanding of patients views on the diagnosis and medication in hypertension, we decided to follow-up on an earlier cross-sectional study from Sweden, were the aim was to observe differences in attitudes towards hypertension and antihypertensive treatment between patients who were and were not persistent to treatment. The former study showed that persistent patients are more aware of hypertension as a chronic disease and of the importance of using antihypertensive medication, as compared to non-persistent patients.10 In addition, non-persistent patients believed that their condition has greater consequences to their life than persistent patients.10 The study also included open-ended questions to the patients on their thoughts about their disease and treatment. The current study applies a qualitative study design using these open-ended questions to assess which experiences and perceptions patients with antihypertensive treatment have about their hypertensive disease and antihypertensive medication. By understanding the views of the patients, we aimed to identify areas for improvement in the management of patients with hypertension, which may be used to target interventions to increase the proportion of patients with hypertension who achieve blood pressure control.
Materials and Methods
Study Design and Population
This was a qualitative study conducted according to the Consolidated Criteria for Reporting Qualitative research (COREQ) guidelines.11 We analyzed open-ended survey questions from a previous cross-sectional study in patients with treated hypertension assessing patients’ perspective on their condition and antihypertensive treatment, as described elsewhere.10 In brief, patients aged ≥ 30 years who had attended one of 25 primary health care centers (PHCC) in the Southwestern greater Stockholm region (Sweden) with a diagnosis of hypertension and who were prescribed antihypertensive medication in 2016 were eligible. The participating PHCC were located in districts of different socioeconomic status, and we believe they were sufficiently different to provide comprehensive views on the subject. A total of 2420 questionnaires were sent out and 711 completed the survey. Among all those who completed the survey, 258 patients also provided answers to open-ended questions and were included in the analysis of the current study.
In the previous study, we used two validated surveys: Brief Illness Perception Questionnaire (Brief IPQ) and Beliefs about Medicines Questionnaire (BMQ).10 BMQ consists of eight questions about the patient’s perception of and attitudes to hypertension with answers distributed by a Likert scale from 0 to 10. At the end of the questionnaire, there was one open-ended question about the patient’s perceptions of high blood pressure. Brief IPQ examined the patients’ attitudes to their antihypertensive treatment and consisted of 22 questions with answers distributed by a Likert scale from 1 to 5. At the end of the questionnaire, there were two open-ended questions, one about the patient’s perceptions of medications in general and the other about the patient’s perceptions of medications prescribed for the patient. These three open ended questions were the basis for the current study. Thematic analysis with both inductive and deductive approach was used to analyze the answers.10
Data Collection
Invitation to participate in the previous study was sent to 69 PHCC whereof 25 agreed to participate. Eligible patients were identified by the electronic medical records of the PHCC. The questionnaires were sent to patients by regular mail and the patients received two reminders, after two and four weeks. The questionnaires could be answered both by regular mail and by internet. The results from the questionnaires were linked to the Swedish Prescribed Drug Register including data on all dispensed drugs12 and subsequently anonymized, as previously described.10
The Regional Ethical Review Board in Stockholm approved of the study (2015/589-31/4), since the study was conducted by Stockholm Region where also Karolinska Institutet is situated, and written consent from all PHCC was obtained. All patients were given separate information about the purpose of the study and consented to participate in the study by responding to the questionnaire, and approved of including the use of their clinical records and their survey responses in the analyses. The patients informed consent included publication of their anonymized responses. Our study complies with the Declaration of Helsinki.
Data Analysis
Thematic analysis was the methodological orientation used to underpin the study which was performed by the authors. Open-ended questions can have a wide variety of answers. By using thematic analysis, the data can be reduced and categorized in a flexible way. The process of the thematic analysis was divided into six phases, according to Braun and Clarke, namely to become familiar with the data, creating codes, to sort the codes connected under an appropriate theme, reviewing themes and achieving an external heterogeneity; to define themes and name them, and finally writing the report and presenting the analysis by showing sufficient data extracts to the reader.13 In this study, the themes were created in a deductive way, using World Health Organization’s 5 dimensions of adherence: 1) condition-related factors, 2) therapy-related factors, 3) health system-related factors, 4) patient-related factors, and 5) socioeconomic factors.7
Details about the entire analysis process are provided in the Supplementary Material.
Results
General
Out of 258 patients who had responded to any of the three open-ended questions, 39 questionnaires were excluded since they contained answers without any relation to the study, (eg people expressing thanks for receiving survey), thus the final number of patients included in the analysis was 219. The study population of responders included 79 men and 137 women (36% vs 63%, 1% unknown), and the number of responders according to country of birth, was 163 (74%) Sweden, 50 (23%) outside Sweden and 6 (3%) were unknown.
Results of the Thematic Analysis
The thematic analysis resulted in a total of 21 different codes, related to each of the five determinants behind medication adherence (Figure 1).
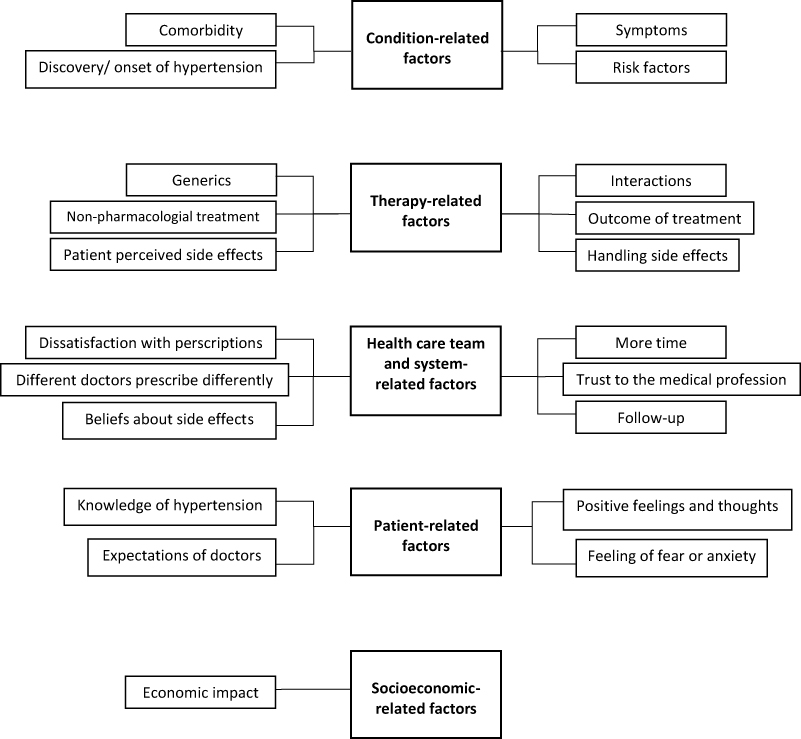 |
Figure 1 Results of the thematic analysis. The five themes are presented in larger boxes with 21 associated codes in smaller boxes. |
Condition-Related Factors
In most cases, the respondents did not notice their hypertension but it was discovered by chance, for example during a visit to the doctor or before an operation.
It came as a surprise - could have been better foreseen and perhaps prevented.
The risk factors for hypertension, which the respondents mentioned in their answers were family history, stress, and increasing age.
My opinion is that too much stress, poor diet and too little exercise creates this. Can of course also be hereditary. Diet and exercise easier to change, but more difficult with stress at work.
While some patients mentioned that they have not had symptoms of hypertension, others referred to headaches, dizziness or fatigue as perceived symptoms. Other symptoms such as tinnitus, impaired sex life, and emotional reactions were raised among the responses.
Did not feel my high blood pressure before it was discovered. I don’t experience any difference at all.
The head felt like a balloon that was about to explode.
Respondents who have other diseases mentioned that doctors prescribed antihypertensive medicines for elevated blood pressure.
[.] Since I’m diabetic, the attending physician believes that antihypertensive medication was appropriate for the sake of safety.
Therapy-Related Factors
The experience of side effects occurred in many respondents. The side effects that were addressed in the answers mainly included dry cough, fatigue and depression.
I have previously tried many blood pressure medications, which I stopped taking due to annoying side effects - extreme fatigue - back pain - depression - reduced sex drive.
Some respondents mentioned that the side effects they have received from antihypertensive medicines have been remedied by changing from one class of drugs to another, or by lowering the dose.
My first blood pressure medication enalapril, I had a severe cough. Switched to losartan and it has worked well. No side effect.
Outcome of the antihypertensive treatment were mentioned among the responses. Some patients believed that the treatment had worked well and lowered their blood pressure. They pointed out that they cannot be without treatment because they feel worse, partly due to symptoms such as headaches and fatigue.
Current medication works well. Therefore, I am motivated to take the medication.
Other respondents, on the other hand, felt that the antihypertensive treatment did not give the desired effect. They did not experience a difference before and during medication.
I would like to get a medicine that lowers my blood pressure. Otherwise, it is pointless to eat drugs, so I do not take so-called blood pressure lowering drugs.
Lifestyle modifications as physical activity, healthy diet and salt reduction occurred among several responses. Some respondents believed that lifestyle modifications are more important than medicine, others saw it as a complement to medicine. It is mentioned that patients may need support regarding lifestyle changes.
My current state of health depends mostly on myself, my lifestyle.
The respondents emphasized the importance of the doctor checking whether the patient’s medicines interact with each other and see the big picture before prescribing.
Drugs are good as long as the prescriber knows how they affect each other.
Opinions about generic medicines were expressed among the survey responses. Some respondents were bothered by the fact that the pharmacy offers other medicines than those prescribed by the doctor. In addition, respondents claimed that it is confusing with all drug name changes and to remember which drug one does not tolerate. One respondent described this as a “jungle” with different manufacturers.
Why does the pharmacy change medicines and not give what the doctor has prescribed???
Health-Care System-Related Factors
Among the respondent’s answers, it appeared that doctor appointments are too short and this is considered to result in unnecessary prescriptions. Patients do not receive information about lifestyle modifications or about the medicines prescribed during the appointment and think that more time is needed.
If doctors had more time for patients, they perhaps would get a greater holistic view of the patient and together reach a different result of the treatment. Time to listen.
Furthermore, the respondents emphasized the importance of the patient being followed up. Patients are willing to go for check-ups and believe that it is as important as getting the medicine itself. Some respondents mentioned that they are followed up annually on their own initiative, while others believed that the follow-up is poor. They expressed that prescription renewal after a phone call is not enough.
Poor follow-up from the primary health care center. I’m not taking the medicine anymore. I check my blood pressure regularly which is now normal.
It appeared among the answers that antihypertensive medications had not been dispensed due to low confidence in doctors. At the same time, several respondents expressed that they trust their doctors since they are aware that the doctors are more competent. Patients take the medications prescribed by their doctor.
I trust the doctors because I lack medical knowledge. Maybe I trust too much. Younger doctors are more committed. I think they are anxious to learn more or they are more afraid of making mistakes. (Am I thinking right?)
It has been pointed out by respondents that doctors are quick to prescribe medicines, especially to the elderly. It is considered that doctors like to prescribe medicines without having formed a clear view about the patient. Respondents mentioned that milder hypertension may not need medication as blood pressure can be normalized with, for example, weight loss.
It is frightening that so many doctors prescribe medication at once, without having examined or investigated the patient properly first. Maybe a doctor should talk and meet the patient first? Prescribe activity, training, support, and conversations with someone who is professional.
The respondents stated that they feel confused due to different doctors prescribing different medicines and doses.
After asking 5-10 different doctors at PHCC, I am very hesitant about whether I should take Enalapril 5 mg or not. Half of doctors say take, the others say don’t. I have chosen not to. I have no idea if the decision is correct?
Patient-Related Factors
The knowledge of hypertension was raised among the answers. Some respondents expressed that they know too little. Other respondents wrote that they know that hypertension is a serious and dangerous disease. They mentioned that it is difficult to feel when the blood pressure is high.
That you can have high blood pressure without feeling it and therefore go with this for a long time.
The respondents were aware that medicines have side effects and this is something they think about often. They expressed their fear of the side effects and wish there were medicines without side effects. Respondents claimed that the side effects outweigh the benefits of the medicine.
The side effects affect more than the blood pressure itself. However, I hope this reduces the risk of stroke
Expectations of doctors were raised among the answers. The respondents mentioned that doctors should inform the patient about the importance of lifestyle modifications, before initiating antihypertensive medication. Doctors were blamed because they did not provide enough information about hypertension and information about side effects. Nor did they do a medication review.
Patients’ drug lists should be reviewed and validated at least once a year. Especially older patients’ lists should be reviewed, as the absorption capacity changes with age.
Fear and anxiety were prevalent among the respondents; anxiety about being diagnosed with hypertension, taking antihypertensive medicines, about side effects and the future.
Worried, a little depressed after the discovery of having high blood pressure. From feeling healthy, I re-evaluated my life. I feel more vulnerable because my life can be more limited by not being able to cope with what I have done before.
Some respondents, on the other hand, expressed that they do not feel anxious since they are satisfied with the antihypertensive treatment. The respondents had a positive mindset and felt grateful for the Swedish healthcare system.
I am lucky to only have the drug amlodipine 5 mg.
Socioeconomic-Related Factors
A few respondents mentioned in their answers that medicines are expensive.
To buy my medicines I have to spend a lot of money - it affects me financially very badly.
Discussion
The aim of this study was to gain an understanding of treated hypertensive patients’ views about and experiences of hypertension, and their use of antihypertensive medications. The main results show that patients with hypertension feel afraid of side effects from medications, have limited knowledge of hypertensive disease, and experience various problems in the management of their blood pressure relating to both lifestyle intervention and medication. All these issues may contribute to failure of reaching target blood pressures.
Under the theme “condition-related factors” patients addressed both modifiable and non-modifiable risk factors. Patients who mentioned family history as a risk factor also wrote that close relatives died in stroke. This suggests a greater understanding of the consequences of hypertension and the importance of treatment, as compared to patients who mention age and stress as risk factors. A greater understanding of the risks associated with hypertension may suggest better adherence to offered therapy, and extend our previous findings.10 These patients may also be more afraid of the consequences of hypertension and thus be more adherent to antihypertensive treatment. Furthermore, several patients claimed they had no symptoms, but their hypertension was discovered by chance during a visit at the doctor for other reasons. Also, patients with no symptoms may not fully understand the severity of hypertension and be less motivated to take medication. Thus, our results underline the importance of regular blood pressure controls also in individuals who do not have a diagnosis of hypertension, as outlined in current guidelines.14
Regarding “therapy-related factors”, respondents claimed they felt confused about, and were not fully aware of, what generic medicines are. The results of this study do not allow us to conclude on how this could affect adherence. However, previous studies have shown that generic substitution in pharmacies (which is a common situation in Sweden) may adversely affect medication adherence in hypertension.15 The majority of patients who mentioned the outcome of their treatment claimed that their blood pressure had become lower. However, some patients did not find the treatment effective. This group of respondents may have been less adherent, as well as those who perceived side effects. This would be consistent with reporting an association between side effects of antihypertensive treatment and medication adherence,16 and findings that although physicians switch antihypertensive treatment due to side effects, uncontrolled blood pressure is the major reason.17 Thus, physicians should actively ask patients about perceived side effects, and changing antihypertensive medication may be a suitable strategy to handle side effects and improve adherence and blood pressure control.
Under the theme “health care team and system-related factors” respondents expressed dissatisfaction with short visits to doctors, which seems to be a main problem for some patients, and with the rapid prescription of medications without obtaining a full evaluation of the patient. In addition, the patients perceived unmotivated differences in prescription patterns between different doctors. Thus, from the perspective of the patient, poor adherence to a person-centered approach by physicians to hypertension management guidelines may exist. These results are in agreement with a reported association between dissatisfaction with health care services and non-adherence.18
The results under the theme “patient-related factors” showed that patients believed that their knowledge about hypertension is limited. This is consistent with results, in which physicians interviewed believe that this affects adherence negatively.19 Our results show that patients have a positive attitude and trust in the competence of doctors, which can contribute to better adherence. However, even more patients felt that their expectations of doctors are not being met. The respondents claimed that physicians did not inform about lifestyle changes, but started treatment by prescribing medications. Guideline recommendations for the treatment of hypertension indicate lifestyle changes to be part of all antihypertensive management.14 Patients in the current study expressed that they felt anxious about medications and afraid of getting side effects, which could affect medication adherence.18 These negative feelings can make patients unwilling to take their medication to obtain blood pressure control.
No “socioeconomic related factors” were highlighted by the respondents, apart from a few comments on drugs costs. This may suggest that patients are reflecting more on themselves and their own treatment than on equal health care. It should also be acknowledged that patent expiries and policy reforms have resulted in comparative low prices for antihypertensives in Sweden.20
The proportions of participants born outside Sweden and of women (23 and 63%, respectively) were greater than for a contemporary treated hypertensive population attending PHCC in Sweden (9 and 53%, respectively).21 This could imply difficulties for those with a foreign origin expressing themselves in Swedish and would be a bias not to answer the open-ended questions. Second, our results could be taken to suggest that women may like to express themselves more than men do, or have a different health-seeking behavior. It is, however, not certain that there are large cultural differences in patient attitudes. A review of 53 qualitative studies on adherence to hypertension treatment showed remarkably similar attitudes across ethnic and geographical groups.22 The overall findings are similar to ours and supports that clinicians in order to improve adherence need a better understanding of patients’ ideas about causality, experiences of symptoms, and concerns about adverse events.
A strength of this study is the varied population concerning gender, age, countries of birth, and comorbidities, representing different PHCC. A heterogeneous population promotes different views and experiences, which appeared among the answers. However, important limitations with this study should be considered. There was sampling bias as a majority of the PHCC invited to participate declined. Non-response bias is another limitation, since not all patients answered the questionnaires, and not all who answered the questionnaires, did answer the open-ended questions. It is important to acknowledge the qualitative nature of data without any aim to quantify certain opinions. Whether patients who did not answer the questionnaires have a more negative attitude towards their medicines and several things to complain about, or the reverse is true, remains to be clarified. Surveys as a method for data collection method have limitations that there are no follow-up questions. In this case, most of the answers were very short and undeveloped. On the other hand, open questions, as used in the current study means that the respondents can write exactly what they want, possibly reflecting what the respondents believe is most important. This adds value in qualitative analyses and meets the purpose of this study.
In conclusion, this study of views and experiences of hypertension and antihypertensive medication from the perspective of the patient show that treated patients with hypertension feel afraid of side effects from medications, have limited knowledge of their disease, and experience problems in the management of hypertension in primary health care (PHC). The latter includes insufficient time during appointments with the doctor, rapid prescription of medications with little advise on lifestyle modifications, and perceived poor adherence by care providers to guideline recommendations on person-centered approaches in the management of hypertension. Such factors potentially associated with non-adherence to medication may be useful for targeted interventions in order to improve the management and control of high blood pressure.
Acknowledgments
We would like to express our thanks to the Regional Drug & Therapeutics Committee in Stockholm, and the participating primary healthcare centers in Southwest Stockholm.
Funding
This work was supported by the Swedish Heart-Lung Foundation (grant number 20160463), Region Stockholm (NSV project, grant number 964603), and Karolinska Institutet Research Foundations (grant number FS-2020:0007).
Disclosure
TK reports research grants to Karolinska Institutet from Medtronic and ReCor Medical; all outside the submitted work. The other authors report no conflicts of interest.
References
1. NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: a pooled analysis of 1201 population-representative studies with 104 million participants. Lancet. 2021;398(10304):957–980. doi:10.1016/S0140-6736(21)01330-1
2. Nieuwlaat R, Schwalm JD, Khatib R, Yusuf S. Why are we failing to implement effective therapies in cardiovascular disease? Eur Heart J. 2013;34(17):1262–1269. doi:10.1093/eurheartj/ehs481
3. Khatib R, Schwalm JD, Yusuf S, et al. Patient and healthcare provider barriers to hypertension awareness, treatment and follow up: a systematic review and meta-analysis of qualitative and quantitative studies. PLoS One. 2014;9(1):e84238. doi:10.1371/journal.pone.0084238
4. Burnier M, Egan BM. Adherence in Hypertension. Circ Res. 2019;124(7):1124–1140. doi:10.1161/CIRCRESAHA.118.313220
5. Qvarnström M, Kahan T, Kieler H, et al. Persistence to antihypertensive drug treatment in Swedish primary healthcare. Eur J Clin Pharmacol. 2013;69:1955–1964. doi:10.1007/s00228-013-1555-z
6. Vrijens B, De Geest S, Hughes DA, et al. ABC Project Team. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. 2012;73:691–705. doi:10.1111/j.1365-2125.2012.04167.x
7. World Health Organization. Adherence to Long-Term Therapies: Evidence for Action. Geneva: World Health Organization. ISBN 92-4-154599-2; 2003.
8. Jolles EP, Padwal RS, Clark AM, Braam B. A qualitative study of patient perspectives about hypertension. International Scholarly Research Notices. 2013;2013:10. doi:10.5402/2013/671691
9. Horne CE, Stayt LC, Schutz LC, et al. Symptom experiences in hypertension: a mixed methods systematic review. J Hypertension. 2023;41(1):1–16. doi:10.1097/HJH.0000000000003306
10. Qvarnström M, Kahan T, Kieler H, Brandt L, Hasselström J, Wettermark B. Medication persistence to antihypertensive drug treatment - a cross-sectional study of attitudes towards hypertension and medication in persistent and non-persistent patients. Blood Press. 2019;28(5):309–316. doi:10.1080/08037051.2019.1627858
11. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
12. Wettermark B, Hammar N, Fored M, et al. The new Swedish Prescribed Drug Register – opportunities for pharmacoepidemiological research and experience from the first six months. Pharmacoepidemiol Drug Saf. 2007;16:726–735. doi:10.1002/pds.1294
13. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3:77–101. doi:10.1191/1478088706qp063oa
14. Williams B, Mancia G, Spiering W, et al. Authors/task force members:. 2018 ESC/ESH guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Cardiology and the European Society of Hypertension. J Hypertens. 2018;36(10):1953–2041. doi:10.1097/HJH.0000000000001940
15. Håkonsen H, Eilertsen M, Borge H, Toverud LE. Generic substitution: additional challenge for adherence in hypertensive patients? Curr Med Res Opin. 2009;25(10):2515–2521. doi:10.1185/03007990903192223
16. Gebreyohannes EA, Bhagavathula AS, Abebe TB, Tefera YG, Abegaz TM. Adverse effects and non-adherence to antihypertensive medications in University of Gondar Comprehensive Specialized Hospital. Clin Hypertens. 2019;25:1. doi:10.1186/s40885-018-0104-6
17. Václavík J, Vysočanová P, Seidlerová J, et al. Reasons for switching antihypertensive medication in general practice: a cross-sectional Czech nationwide survey. Medicine. 2014;93(27):e168. doi:10.1097/MD.0000000000000168
18. Ashoorkhani M, Majdzadeh R, Gholami J, Eftekhar H, Bozorgi A. Understanding non- adherence to treatment in hypertension: a qualitative study. Int J Community Based Nurs Midwifery. 2018;6(4):314–323.
19. Barreto Mda S, Reiners AA, Marcon SS. Knowledge about hypertension and factors associated with the non-adherence to drug therapy. Rev Lat Am Enfermagem. 2014;22(3):491–498. doi:10.1590/0104-1169.3447.2442
20. Wettermark B, Godman B, Neovius M, Hedberg N, Mellgren T-O, Kahan T. Initial effects of a reimbursement restriction to improve the cost-effectiveness of antihypertensive treatment. Health Policy. 2010;94:221–229. doi:10.1016/j.healthpol.2009.09.014
21. Mourtzinis G, Manhem K, Kahan T, et al. Socioeconomic status affects achievement of target blood pressure and cardiovascular outcome in hypertension: contemporary results from the Swedish primary care cardiovascular database. Scand J Prim Health Care. 2021;39:519–526. doi:10.1080/02813432.2021.2004841
22. Marshall IJ, Wolfe CD, McKevitt C. Lay perspectives on hypertension and drug adherence: systematic review of qualitative research. BMJ. 2012;345:e3953.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.