Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 9
A qualitative study of perceptions of determinants of disease burden among young patients with type 1 diabetes and their parents in South India
Authors Verloo H ![]() , Meenakumari M, Abraham J, Malarvizhi G
, Meenakumari M, Abraham J, Malarvizhi G ![]()
Received 14 December 2015
Accepted for publication 9 February 2016
Published 19 May 2016 Volume 2016:9 Pages 169—176
DOI https://doi.org/10.2147/DMSO.S102435
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Henk Verloo,1 Mohan Meenakumari,2 Elizabeth Jean Abraham,3 Gnanam Malarvizhi3
1Department Nursing Sciences, University of Applied Nursing Sciences, La Source, Lausanne, Switzerland; 2Kurinji Hospital, 3PSG College of Nursing, PSG Hospital, Coimbatore, Tamil Nadu, India
Background: Diabetes is a leading threat to public health in India. A huge prevalence of type 1 diabetes among young patients is documented in literature; India is one of the countries with the highest number of new cases per year (10,900), of which 3–4 million face poverty along with diabetes.
Objective: The aim of this study was to explore the perceptions of determinants of the disease burden among young patients with type 1 diabetes and their parents.
Methods: In June 2014, perceptions were collected from eleven young patients and five available parents using the critical incident technique.
Results: Disease burdens associated with the management of type 1 diabetes can vary significantly according to the different social and economic determinants facing each household. Determinants associated with good practices in the management of childhood type 1 diabetes included socioeconomic status, unawareness of health complications, and beliefs about nutrition. Coping strategies applied via lifestyle changes included monitoring glycemia and regular checkups by diabetologists. A general lack of awareness about type 1 diabetes in Indian society, stigmatization, and limited access and systematic barriers to the delivery of optimal health care were all perceived to be factors hindering the successful management of chronic type 1 diabetes by young patients and their parents.
Conclusion: Stigmatization, a lack of therapeutic adherence, and the financial strains placed on families, particularly on poor ones, are critical. More emphasis must be put on the prevention of acute and long-term complications and education.
Keywords: adolescents, adherence, critical incidence technique, India, parents, positive experiences, negative experiences, type 1 diabetes, children
Background
Diabetes is a global public health problem that may be turning into a pandemic chronic disease. By 2030, three-quarters of the world’s 300 million adults with diabetes would live in nonindustrialized countries; almost one-third of these would live in India and in the People’s Republic of China. In 2014, the International Diabetes Federation estimated that 65.1 million Indians were living with different types of diabetes,1 predicting that this would rise up to 79.4 million by 2030.1,2
The incidence of type 1 diabetes continues to increase worldwide, and it has serious short- and long-term implications. Type 1 diabetes is one of the most common pediatric endocrine illnesses. Young patients living with type 1 diabetes – where the pancreatic beta cells that produce insulin are destroyed because of autoimmunity – require regular insulin therapy to survive.3,4 The incidence of type 1 diabetes in young patients is increasing at a rate of 3% per year. In 2006, the International Diabetes Federation estimated that in India there were ~5 million young children, <15 years of age, with type 1 diabetes, and it is one of the countries with the highest estimated number of new cases annually (10,900 new cases/year), of which 3–4 million face poverty along with diabetes.5 It is, therefore, particularly important that population-based prevention strategies for the epidemic rates of obesity and metabolic syndrome in India should be strengthened and effectively implemented.6 Consequences of this life-changing disease is in India still persisting, such as death before diagnosis due to missed diagnosis, poor management because of low awareness and high costs, limited availability of insulin and poor cold chains in rural areas, and limited availability of blood glucose strips.7
Poor care and delayed or no prevention strategies lead to more complications. Due to these inadequacies in the medical care system, the patient and family are trapped in a vicious cycle of increased acute and chronic complications. This provokes further elevating costs, mortality, absenteeism from work and hence decrease in income, employability, and quality of life, further pushing the family into indebtedness and poverty attention to chronic disorders and long-term care.8
The incidence of type 1 diabetes among young patients has increased rapidly, at a rate of 5% per year in preschool children.9 A lack of effective disease management, due to a variety of reasons, means that 1,338 young patients die of diabetes annually in India.10,11 Currently, there is no cure for type 1 diabetes, but, with relatively limited resources, health care systems can save lives by building on the five fundamental requirements for the management of diabetes: 1) availability of food and clean water; 2) availability of insulin; 3) availability of urine/blood testing equipment; 4) prevention of both ketoacidosis and hypoglycemia; and 5) protection against injury.5 Using these five requirements, most short- and long-term complications can be avoided. However, several barriers to putting these requirements into place in India have been documented, such as supplying insulin or urine/blood glucose testing equipment to remote areas.12 Other hindrances include the relatively high cost of insulin and blood glucose monitoring strips, social barriers to accepting insulin injections, and a lack of teams trained to manage type 1 diabetes among young patients.10,12–14 Furthermore, in India, a significant percentage of the population can be overwhelmed by the compounded effects of poverty, malnutrition, and multiple infections including human immunodeficiency virus infection (HIV)/acquired immune deficiency syndrome (AIDS), tuberculosis (TB), and malaria.15
An evidence-based approach to managing type 1 diabetes represents a restraint on the everyday lives of young patients and their families. Young patients and their parents generally lack the coping mechanisms needed to overcome the stress of chronic illness. Psychological morbidity provoking dysfunction in the social, personal, and cognitive domains has been associated with significantly poorer quality of life and general well-being.16,17 Health care providers may, by educating parents on how to appropriately take care of their diabetic child, not only reduce overall health costs but also provide the maximum benefits for the young patient and the parent.16,18,19
Little is currently known, however, about levels of awareness and barriers to care facing young patients with diabetes and their parents.20 The purpose of this qualitative study was to investigate young patients’ perceptions and knowledge of diabetes and its complications, as well as any barriers to care. Specific objectives included assessing the young patients and the available parents’ perceptions of the socioeconomic consequences of diabetes on their family.
Methods
Study design and research population
This study used a community-based participatory research approach.21 Community-based participatory research emphasizes the importance of community members participating in every step of the research process, and it prescribes an equitable partnership between professional and community investigators in all research responsibilities. This emphasizes the importance of coeducation and the rectification of knowledge imbalances between professional and community investigators.22
As a qualitative study, it used the critical incident technique (CIT)23 on eleven young patients with type 1 diabetes, aged between 4 years and 18 years, and their available family members. A critical incident is defined as “any observable human activity that is sufficiently complete in itself to permit inferences and predictions about the person performing the action”.24 The CIT is used to study human experiences based on behaviors shown in precise circumstances.23 Participants were interviewed in the outpatient departments of two periphery district hospitals in the Coimbatore region of the state of Tamil Nadu in South India in June 2014.
Data collection
Interview guidelines were specially prepared for this study, based on a literature review and consultation with a pediatric endocrinologist. The guidelines, using a semi-structured, open-ended questionnaire, were pretested on three young patients living with diabetes, in the presence of their parents. The interview guidelines contained questions on: the family’s socio-demographic characteristics and biography, including the circumstances pertaining to type 1 diabetes; the psychosocial and economic repercussions of the disease on the family; and the family’s knowledge about the disease. The latter section allowed them to give narrative descriptions of their perceptions of the disease. Young patients who felt uncomfortable answering in the presence of their parents were allowed to take the interview separately from them.
All but three interviews took place in a hospital consulting room. It is known that using hospital consulting rooms to conduct interviews may influence participants’ answers.25,26 On the other hand, the interview took place in a safe, confidential space allowing participants to be open and honest with the interviewer. Interviews were carried out by G Malarvizhi who made field notes after each interview. Although the interviews followed a semi-structured format, any interesting or unusual points were investigated in a follow-up interview. Interviews were audio-recorded and lasted between 45 minutes and 1 hour.
Data analysis
The information collected was processed as follows: 1) summaries of interviews were recorded in a digital format; 2) interview content was analyzed by the interviewer to identify positive, negative, or neutral events; and 3) critical incidents were identified, classified, and organized by themes. We used the hierarchical categorization procedure specific to the Flanagan method.23 During the classification of categories, the taxonomy of specific attitudes and the creation of new categories were developed continuously, as proposed by Flanagan method, so that all incidents were classified according to the specificities of the process and the people involved. The participants’ similar and divergent opinions were compared.
Ethics
This study received ethical clearance from the Institutional Human Ethics Committee of PSG Hospital in Peelamedu, Coimbatore, Tamil Nadu. Investigators were bound by obligation to confidentiality, and all the data collected were anonymized, encoded, and kept under lock and key. The results are presented in an agglomerated form, thereby ensuring confidentiality and participants’ anonymity. No participants will be identifiable in future presentations or publications.
Where possible a written parental consent was obtained before any young patients living with diabetes were approached. Parents not able to give written consent were asked to make a ink left thumb print. The young patients’ agreement (assent) to participate was also obtained. Participants were free to withdraw from the study at any time without fear of sanction or prejudice in terms of the subsequent health care services they are entitled to receive. Participants did not receive any compensation for their participation.
Results
Socio-demographic characteristics
A total of eleven young patients with type 1 diabetes, all from different families, and five available parents were interviewed (Table 1).
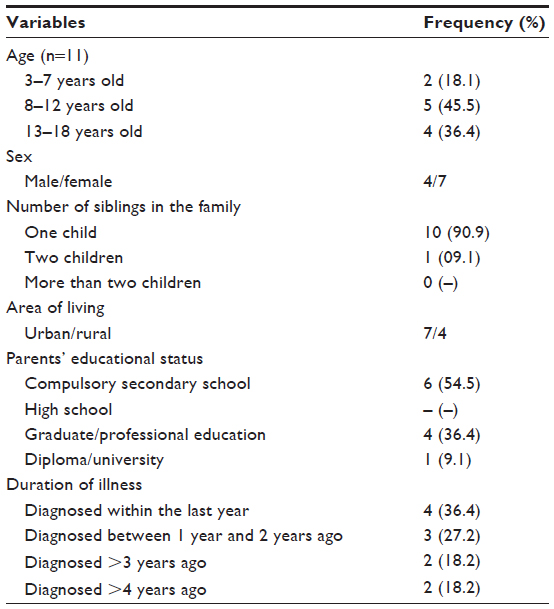 | Table 1 Socio-demographic characteristics of the children interviewed |
Young patients’ and parents’ perceptions of diabetes
Four main themes were observed: experiences of symptoms of diabetes, the impact of diabetes on daily activities, social or cultural acceptance and stigmatization, and the emotional consequences and the quality of life of the young patients with diabetes and their family members. These themes were not mutually exclusive or independent, but rather overlapped and intertwined.
Experience of diabetes symptoms
The typical symptoms of diabetes experienced by most of the young patients were polyuria, polyphagia, sweating, and weight loss. Other common associated symptoms experienced were fever, vomiting, loss of appetite, and tiredness. One 16-year-old girl stated, “I vomited daily and had difficulties breathing for 14 days before they discovered my diabetes.”
One 14-year-old girl said, “I lost weight continuously for 4 months, for no reason, and had headaches also. When I consulted the physician, she told me that I had diabetes.”
One mother stated, “When the disease started, my son lost weight and was suspected of having some vitamin deficiencies and problems with nutrition. He was treated with health tonics and food supplements, but symptoms worsened until he was diagnosed with type 1 diabetes.”
One young patient was admitted to hospital for hyperreactive airway disease; however, during the routine pediatric investigation that followed she was diagnosed with diabetes, despite having had no previous significant symptoms.
Although it is generally accepted that diabetes is a life-changing disease, for most of the young patients and parents, the diagnosis of diabetes was experienced as a relief; after several months of doubt and suspicions about other more lethal diseases (eg, TB or HIV/AIDS), diagnosis was accompanied by a positive feeling.
Impact of diabetes on activities and performance
The majority of the young patients mentioned positive feelings about school performance. Positive narrative incidents mentioned by the young patients included: “My illness does not limit my activities” (7-year-old); “My friends know that I am diabetic, and they are supportive and put no limitations on my activities” (12-year-old); “I am able to perform well in school” (10-year-old).
In response to the open-ended question, “Do you feel that this condition has affected your daily routines, limited your activities, and created a dependency in relation to managing diabetes?” four out of eleven young patients reported that diabetes did not affect their daily routines. However, others reported more negative experiences, such as: “I could not attend school for three years due to my illness. Since I could not afford to take injections daily, I was trying various native treatments. I developed menstrual irregularities” (18-year-old); “I am scared because of my condition and cannot go to school” (7-year-old girl); “I am too shy to confide in my friends about my condition, so I avoid them” (12-year-old boy). One mother mentioned her son’s real ability to manage his diabetes treatment autonomously:
My boy is doing almost everything by himself, except when his leg hurts too much. Then he may ask me to do the insulin injection in his arm. Each time he does the lunchtime injection at school, he notes down the glycemia result and the dose of insulin in a special notebook. I can check it when he comes home.
Social/cultural acceptance and stigmatization
Indian social and health care structures incorporate a number of medical systems working in parallel to Western-style medicine, such as ayurvedic medicine or herbs and homeopathy. These other health professionals also treat patients with diabetes, but some of the mothers reported that such treatments had worsened symptoms. Mothers were often more involved in carrying out treatments for their children, with the fathers working to pay for it.
Young patients and their parents expressed positive and negative experiences in their daily lives with type 1 diabetes. Indian society is characterized by life in families with grandparents and other family members often living in the same home. With regard to grandparents’ interest in and comprehension of the disease, intergenerational relations can at times elicit serious contradicting incidents. One father evoked the following example to illustrate how grandparents are often a source of confusion:
The bigger the family is, the harder it is to stick to the new nutrition plan demanded by diabetes. My family lived on the first floor with our kids, and the grandparents lived on the second floor. Although we tried to have a healthy diet on the first floor, the grandparents didn’t understand why they couldn’t give sweets to their grandchild, and they didn’t want him to be deprived of food. We were finally obliged to leave our home in order to ensure healthy nutrition for our child.
One mother mentioned the positive social engagement of the town of Coimbatore and stated that the social services there hand out for free lunch, soups, and juices to diabetic and other sick young patients.
The general population’s knowledge about type 1 diabetes varies significantly, but is, in most cases, simply lacking. Some perceive it to be a curable disease: one of the young patients was told to “come back to school once the disease has been cured.” Regarding the causes of the disease, people directly responsible for the young patients diagnosed with diabetes often feel guilty and responsible for the situation. Knowledge of type 1 diabetes among the young patients living with it, however, appeared to be more developed. They felt a certain responsibility for their own health and were aware of what they were and were not allowed to eat, recognizing that they could no longer eat sweets and candies like other children do. Older children sometimes even cooked their own meals in order to ensure correct nutrition. Some of them had developed a high level of autonomy and managed their treatment plan very well. They stated feeling no difficulties in their daily lives in society, and although they spoke about initial fears and worries about injections, they were never scared of the disease itself.
In some cases, parents were educated by their young patients: “Through my son’s disease, I now know pretty much everything about it.” Other adults had some knowledge of the disease because their own parents were also living with type 1 diabetes.
Some families were extremely motivated and adapted their nutrition plan around their child, with all family members deciding to stick to the same diet. Indeed, the families mentioned that changing food habits was not a significant burden. Most parents were very proud of their child when they considered them to be mostly autonomous in their treatment management.
Some of the young patients expressed positive feelings about experiencing no problems or stigma at school, from either teachers or classmates. They mentioned how their entourage was ready to support them if they needed any help: “My friends help me a lot” (7-year-old); or “I take my injections in school, and friends and others in school support me” (14-year-old). The degree of knowledge about type 1 diabetes influenced social acceptance and either reinforced or neutralized stigmatization. One older young patient explained everything about diabetes and its treatment to his mother, and this helped him and his family to accept and avoid stigmatization of this chronic disease. Teachers who were aware of the disease did not push the young patients to do activities that should best be avoided by diabetics.
Parents, however, were more likely to evoke negative critical incidents regarding stigmatization. They mentioned that families wanted to hide their child’s disease, “Sometimes even the grandparents don’t know about it,” or explore alternative therapeutic approaches.
It happens even more often in religious families. It seems they have a belief that insulin is something bad and shouldn’t be used. It has to be taken for life. They would prefer to heal the child with alternative Indian treatments, for example, or with homeopathy and ayurvedic therapy. Children are even skeptical about telling other children about their diabetes.
The mother of a 12-year-old girl was upset, saying, “My daughter has to take insulin injections for life. How will I ever get her married? If it came in tablets, nobody would know about her condition.”
Parents also mentioned the obstacles to treatment adherence experienced in schools. Some schools do not allow a “sick child” to attend and do not permit lunchtime insulin injections. Certain parents, therefore, with the intention of keeping the disease hidden, consult a diabetologist in order to seek means of doing without lunchtime insulin injections. Most of the time, parents wish to hide their child’s disease from both the school and teachers. “Teachers don’t want to be responsible for any treatment or complication. Most of the time, they don’t know anything about this chronic disease, they think that the child should stay at home and come back to school as soon as he’s healed.” Another mother was more restrained and expressed a more neutral feeling, saying,
Although some schools don’t accept young patients with diabetes, some teachers are open and ready to accept the young patient after there has been some explanation about the disease and treatment. Other reasons why my child often doesn’t do his injections at school are the facts that he is young and feels embarrassed.
Emotional consequences and impact on quality of life
With regard to questions of adherence and compliance to proposed nutritional plans, we discovered positive incidents among the young patients with diabetes. One 12-year-old boy said, “I cook and eat a wheat-based diet for breakfast, chapattis, lunch with rice, and for dinner wheat dosa and ragi (millet). My grandmother was diabetic. I have seen her following this diet, and I like this food.”
A more nuanced diet was mentioned by the young patients in the following incidents. “I have to restrict my sweets and chocolate, ice cream foods, even though I like them,” one 10-year-old boy said. “I should only eat rice for lunch, and eat more vegetables and fruits.” A 16-year-old adolescent stated, “I eat all types of foods, but I do avoid sweets and tubers.”
Most of the young patients and their parents expressed negative feelings after diabetes was diagnosed, saying, “My parents and I were not aware that I needed to be treated by a diabetologist.” One mother expressed negative feelings about the burdens of diabetes, saying, “Later on, after diagnosis, my child was referred to the pediatric diabetologist. It changed the extended family dynamic, and we could no longer accept every invitation to share meals eating normal food with other family members.” One mother expressed her fear of hypoglycemia, explaining that her quality of life had decreased. “Since they diagnosed my son with type 1 diabetes, he has been on an insulin pump. I fear he may become hypoglycemic, and I am not sleeping well,” she said. One mother said, “My child often fears physical stigmatization and is sometimes demoralized and demotivated by the thought of how his peers will react.”
Discussion and conclusion
This study presents the perceptions of young patients with type 1 diabetes, alongside those of their parents, upon learning the diagnosis of this chronic illness. The positive, negative, and neutral socioeconomic experiences of type 1 diabetes, in the town of Coimbatore in South India, are revealed through illness narratives in relation to the disease.
By using the CIT – a qualitative investigation method – we were able to discover that most of the young patients and their parents clearly understood and were able to report their symptoms. Furthermore, the CIT revealed the burdens that type 1 diabetes imposed on families, highlighting the specific problems related to the disease and how these affected young patients, including the emotional and social impacts it had on their everyday lives. This approach seems appropriate for collecting socially relevant data on the experiences of young patients living with type 1 diabetes and their parents. It corroborates the recent study by Biagetti et al related to celiac disease.27
For most young patients and their parents, the diagnosis of type 1 diabetes proved to be a traumatic experience. The lack of basic information and knowledge about the disease was an important stress factor, and the prevalence of diabetes in Indian society is increasing among children and adults. A large-scale awareness program in media should be considered in order to improve the early recognition of diabetic symptoms and reduce the stigma attached. Informing children about diabetes via school nurses would be an interesting solution; however, in India, health care professionals in schools are limited to certain private institutions. Virmani mentioned that there is a huge need to better understand the use of non-insulin therapies in Indian communities and traditional medicine approaches and the importance of educating communities about insulin and growth disorders in type 1 diabetes.7
Most of the young patients manifested the typical clinical symptoms of type 1 diabetes. In most cases, the relatively late diagnosis of this chronic disease had provoked uncertainty and distress for both children and parents. Despite the difficulties involved in finally obtaining the correct diagnoses, the young patients were doing well to manage both their school activities and their chronic disease. Cues to action were typically symptom related. Most young patients and parents recognized that diet was a key component of diabetes management, but good practices of self-care such as balanced meals and regular physical activity were rare. Based on their lack of initial knowledge and the limited information available, parents and other family members often had difficulty identifying diabetes-related needs. The financial burdens that type 1 diabetes imposes on families are a major determinant in the care pathways that they can take into consideration in relation to good practices. Diabetes puts an important economic burden on most families and influences the care which families themselves can provide to their chronically ill children. The cost of a blood test is INR 15 (USD 0.23). One cartridge of insulin costs about INR 50 (USD 0.77). More advanced treatments, such as an insulin pump, cost about INR 30,000 (USD 462) plus an extra INR 5,000 (USD 77) per month for the insulin. In India, the number of tests a young patient will be able to do each day will probably depend upon the financial resources that the family have to support the medical treatment. The parents mentioned an average monthly cost of approximately INR 4,000 (USD 62). Most Indian families cannot afford these expenses and have no health insurance. Moreover, as soon as a young patient is diagnosed with type 1 diabetes, it becomes almost impossible to get a new health insurance policy for coverage within the Indian health care system: policies exclude people with a chronic disease. Fortunately, most diabetologists will help families to best adapt treatments to match their financial resources. Some parents mentioned that in exceptional cases, employers had offered a financial contribution toward treatment.
Some stigmatization and exclusion were experienced with certain educational institutions, even refusing young patients with type 1 diabetes. This corroborated the findings in the study by Sullivan-Bolyai et al,28 where mothers reported that some day care centers refused to accept their young children with type 1 diabetes. The mothers were informed that their children’s illness-related demands would take time away from others in the day care center.
Siegel et al highlighted the importance to address the social consequences of the Indian diabetes epidemic. Moreover, major societal issues such as fears of marriage as well the negative psychological impact on children’s self-confidence, self-worth, and self-management are been documented.29 Due to the chronic nature of the disease, both young patients and parents perceived a lack of proper access to treatment and the negative impact of diabetes on their quality of life. There is an increasingly strong call coming from within the Indian health care network itself; it backs the view that there is an urgent need to improve the management of type 1 diabetes for the country’s children so as to ensure that “No child should die of diabetes.”
Limitations of the study
This study presents several limitations concerning the collection of the data on critical incidents among young patients <8 years old. Events concerning them were mostly evoked by their parents and were not specifically mentioned by the young patients themselves. Although this could introduce some bias into our results, the overall perceptions of the determinants of disease burden should not be of major importance. The second potential limitation was that participants may not feel fully at ease or may have unpleasant associations with hospital environments. They may also have had an increased association with the interviewer.It may have been preferable to speak to all participants in their homes, only 4 families were interviewed at their homes as they were from different locations. Finally, attention should be given to the transferability of our findings. Extension of our findings in other situations or regions in India should be done with caution.
Acknowledgments
We thank the children and their families for their participation in this study. The authors also thank the nursing students of the PSG College of Nursing, Coimbatore, India, and the Universities of Lausanne (A Godat and M Nikles) and Applied Sciences in Nursing La Source (C Orsino and N Conod) for their contribution to successful data collection. This study was funded by the Canton of Vaud and the University of Applied Nursing Sciences, La Source, Lausanne, Switzerland.
Author contributions
Study concept: HV, GM, EJA, and MM. Data acquisition: HV, GM, and MM. Data analysis and interpretation: HV, GM, EJA, and MM. Manuscript drafting: HV, GM, EJA, and MM. Statistical analysis: HV, GM, and MM. Fundraising: HV, GM, EJA, and MM. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Patterson C, Guariguata L, Dahlquist G, Soltész G, Ogle G, Silink M. Diabetes in the young – a global view and worldwide estimates of numbers of children with type 1 diabetes. Diabetes Res Clin Pract. 2014;103(2):161–175. | |
Das S, Maji D, Majumder PP. Prevalence of diabetes in various habitats of West Bengal, India. J Indian Med Assoc. 2005;103(11):580–584. | |
Bhatia E. Type 1 diabetes mellitus in India. Curr Diab Rep. 2012;12(3):224–226. | |
Raha O, Chowdhury S, Dasgupta S, et al. Approaches in type 1 diabetes research: a status report. Int J Diabetes Dev Ctries. 2009;29(2):85–101. | |
Daneman D. State of the world’s children with diabetes. Pediatr Diabetes. 2009;10(2):120–126. | |
Wasir JS, Misra A. The metabolic syndrome in Asian Indians: impact of nutritional and socio-economic transition in India. Metab Syndr Relat Disord. 2004;2(1):14–23. | |
Virmani A. Growth disorders in type 1 diabetes: an Indian experience. Indian J Endocrinol Metab. 2015;19(suppl 1):S64–S67. | |
Jones KL. World diabetes day 2008: focusing on the children! Indian J Med Res. 2008;128(5):567–569. | |
Shah P, Misra A, Gupta N, et al. Improvement in nutrition-related knowledge and behaviour of urban Asian Indian school children: findings from the ‘Medical education for children/adolescents for realistic prevention of obesity and diabetes and for healthy aGeing’ (MARG) intervention study. Br J Nutr. 2010;104(3):427–436. | |
Bhatia E, Aggarwal A. Insulin therapy for patients with type 1 diabetes. J Assoc Physicians India. 2007;55(suppl):29–34,39–40. | |
Bhatia V, Arya V, Dabadghao P, et al. Etiology and outcome of childhood and adolescent diabetes mellitus in north India. J Pediatr Endocrinol Metab. 2004;17(7):993–999. | |
Zargar AH, Wani AI, Masoodi SR, et al. Causes of mortality in diabetes mellitus: data from a tertiary teaching hospital in India. Postgrad Med J. 2009;85(1003):227–232. | |
Chan JCN. Diabetes in Asia – from understanding to action. Ann Acad Med Singapore. 2008;37(11):903–905. | |
Yadav S, Parakh A. Insulin therapy. Indian Pediatr. 2006;43(10):863–872. | |
Virmani A, Shah P, Setia S, Singh GR. Why must Indian diabetic children continue to have retarded growth? Acta Paediatr. 1995;84(3):354–355. | |
Bhadada S, Grover S, Kumar S, Jaggi S. Psychological impact of type-1 diabetes mellitus on parents: an exploratory study from North India. Int J Diabetes Dev Ctries. 2011;31(3):174–179. | |
Alderman H. The response of child nutrition to changes in income: linking biology with economics. CESifo Econ Stud. 2012;58(2):256–273. | |
Bai PV, Krishnaswami CV, Chellamariappan M, Kumar GV, Subramaniam JR. Glycosuria and diabetes mellitus in children and adolescents in south India. Diabetes Res Clin Pract. 1991;13(1–2):131–135. | |
Balagopal P, Kamalamma N, Patel TG, Misra R. A community-based diabetes prevention and management education program in a rural village in India. Diabetes Care. 2008;31(6):1097–1104. | |
Khan FN, Agne AA, Buttan S, Cherrington AL. Assessing diabetes knowledge and barriers to health services among patients with diabetes: a qualitative study in Delhi, India. Int J Health Promot Educ. 2013;51(6):290–299. | |
Wallerstein NB, Duran B. Using community-based participatory research to address health disparities. Health Promot Pract. 2006;7(3):312–323. | |
Israel BA, Eng E, Schulz AJ, Parker EA. Methods for Community-Based Participatory Research for Health. San Francisco, CA: Wiley; 2013. | |
Flanagan J. The critical incident technique. Psychol Bull. 1954;51(4):327–358. | |
Kemppainen JK. The critical incident technique and nursing care quality research. J Adv Nurs. 2000;32(5):1264–1271. | |
Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. | |
Challenor J, Watts J. ‘It seemed churlish not to’: how living non-directed kidney donors construct their altruism. Health (London). 2014;18(4):388–405. | |
Biagetti C, Naspi G, Catassi C. Health-related quality of life in children with celiac disease: a study based on the critical incident technique. Nutrients. 2013;5(11):4476–4485. | |
Sullivan-Bolyai S, Deatrick J, Gruppuso P, Tamborlane W, Grey M. Constant vigilance: mothers’ work parenting young children with type 1 diabetes. J Pediatr Nurs. 2003;18(1):21–29. | |
Siegel K, Narayan KMV, Kinra S. Finding a policy solution to India’s diabetes epidemic. Health Aff (Millwood). 2008;27(4):1077–1090. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.